")
Back to Journals » Cancer Management and Research » Volume 12
Inflammatory Marker Predicts Outcome of Oral Squamous Cell Carcinoma Receiving Chemo-Radiotherapy
Authors Sun W, Gao M, Hu G, Yuan X
Received 21 August 2020
Accepted for publication 3 November 2020
Published 1 December 2020 Volume 2020:12 Pages 12329—12335
DOI https://doi.org/10.2147/CMAR.S277927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Antonella D'Anneo
Wei Sun,1 Meng Gao,2 Guangyuan Hu,1 Xun Yuan1
1Department of Oncology, Tongji Hospital of Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430020, Hubei, People’s Republic of China; 2Department of Medical Ultrasound, Tongji Hospital of Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430020, Hubei, People’s Republic of China
Correspondence: Xun Yuan
Department of Oncology, Tongji Hospital of Tongji Medical College, Huazhong University of Science and Technology, 1095 Jiefang Avenue, Wuhan 430030, Hubei, People’s Republic of China
Tel +86-027-8366-3406
Fax +86-027-8366-3630
Email [email protected]
Background: Inflammation is involved in the progression of oral squamous cell carcinoma. We therefore postulate that a blood-based inflammatory marker, the neutrophil-to-lymphocyte ratio, could help to predict the prognosis in patients with oral squamous cell carcinoma receiving chemo-radiotherapy, and build a prognostic nomogram.
Methods: In 111 cases of oral squamous cell carcinoma, several baseline variables, including inflammatory markers and lactate dehydrogenase, were measured within the week of chemo-radiotherapy initiation as predictors of mortality and separate risk scores were developed.
Results: Dichotomized neutrophil-to-lymphocyte ratio was found to be associated with AJCC stage (p< 0.001). Patients with oral squamous cell carcinoma with a low neutrophil-to-lymphocyte ratio survived longer than those with a high neutrophil-to-lymphocyte ratio (overall survival HR=2.39, 95% CI 1.24– 4.61, p=0.009). The Harrell’s concordance (C)-statistic of the nomogram was 0.74 and the calibration curve demonstrated the goodness of fit.
Conclusion: The inflammatory marker neutrophil-to-lymphocyte ratio, obtained before chemo-radiotherapy, was an independent factor of survival prediction for oral squamous cell carcinoma. The nomogram incorporating immunological markers could more accurately predict individualized survival probability than the existing models. These findings are significant for the creation of personalized treatment strategies in the clinical setting.
Keywords: nomogram, oral squamous cell carcinoma, LDH, platelet-to-lymphocyte ratio, neutrophil-to-lymphocyte ratio
Introduction
Oral squamous cell carcinoma (OSCC), referring to cancer occurring between the vermillion border of the lips and the junction of the hard and soft palates or the posterior third of the tongue, is a malignancy with high morbidity and mortality, resulting in 177,384 deaths worldwide annually.1 Advanced OSCC is typically treated with multimodal therapy including surgery, radiotherapy and chemotherapy; however, the survival outcome differs considerably among the patients.2 Chemo-radiotherapy (CRT) has been one of the most effective treatment options for patients with resectable or unresectable tumors. The identification of prognostic factors can help improve survival estimation and guide treatment decisions in patients with OSCC. Different clinical and laboratory characteristics have been proposed in the past as being related to prognosis in cancer patients.3–5 However, studies of potentially prognostic variables investigating the mortality of OSCC were inconsistent and varied widely. Inflammation is one of the hallmarks of cancer.6 Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), as inflammation-associated indices, have been evaluated to predict survival for a variety of malignancies.7–9 Lactate dehydrogenase (LDH) is tightly linked to tumor cell load and distant metastasis.10,11 In particular, NLR, PLR and LDH can be obtained from routine blood analysis and have been assessed to be cost-effective biomarkers for cancer survival. Previous studies suggested that preoperative peripheral neutrophil and lymphocyte counts were correlated with survival in oral cancer.12,13 But the prognostic value of inflammatory markers has not been fully elucidated in patients with advanced OSCC undergoing CRT. Thus, it is necessary to assess the available pretreatment parameters in order to develop a prognostic model for the prediction of survival outcomes in OSCC patients. In addition, little evidence has demonstrated the clinical efficacy regarding predictors in OSCC patients undergoing CRT.
Therefore, the present study retrospectively included patients with OSCC who were admitted and treated in our center since 2014, to investigate the predictors of mortality in patients with OSCC and to determine whether NLR is independently correlated with prognosis in OSCC.
Materials and Methods
Patient Selection
The study retrospectively included a total of 111 patients diagnosed with primary OSCC and undergoing CRT in Tongji Hospital of Tongji Medical College, Huazhong University of Science and Technology, between April 2014 and January 2018. Eligible patients were included if they were aged ≥18 years and had a cytologically or histologically confirmed diagnosis of OSCC, while patients with other primary tumors and autoimmune diseases were excluded. Depending on the clinical condition of the patients, patients received radiotherapy or concurrent CRT. Conventional fractionation radiation therapy was administered as 60–66 Gy to the isocenter using intensity-modulated radiation therapy (IMRT), divided over 2 Gy daily fractions, five times a week. Follow-up was typically scheduled for a month after initial treatment, every 3 months within the first 2 years, and every 6 months thereafter.
Data Collection
We collected clinicopathological data, including TNM stage (based on version 7 of the International Association for the Study of TNM staging System), as well as patient’s age, gender and smoking history. The laboratory data, including LDH, neutrophil, platelet and lymphocyte levels, were obtained within the week leading up to CRT. The NLR was calculated as the neutrophil count divided by the lymphocyte count and the PLR was defined as the platelet count divided by the lymphocyte count. Follow-up was performed until January 2020. Outcome variables included overall survival (OS). OS was defined as the date of CRT to the time of death, or the time of last contact. To reduce the potential bias, the five patients who died within a month from the start of initial therapy were excluded from the analysis. The study was granted approval by the Institute Research Medical Ethics Committee of Tongji Hospital of Tongji Medical College, Huazhong University of Science and Technology. All data were collected in accordance with the principles of the Declaration of Helsinki. Using electronic medical records, we searched the information on each patient. Individual patient information was protected and has not been shown. The Ethics Committee waived the need for informed consent for the collection, analysis and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Statistical Analysis
The associations between serum marker level (including LDH, NLR and PLR) and the clinicopathological parameters were evaluated by a Χ2-test. For the univariate analysis, the primary end point was evaluated by the Kaplan–Meier method. Forward stepwise multivariate Cox proportion hazard analysis was conducted to clarify the impact of age, gender, smoking history and TNM stage on OS. Hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) were estimated from the Cox analysis. We also plotted the nomogram to assess the models with the prognostic factors and employed Harrell’s concordance index (C-index) to determine the model’s prognostic accuracy (PA) in the multivariate analysis. The goodness of fit was evaluated by the Akaike information criterion. A two-sided p-value of less than 0.05 was considered significant for all the statistical tests. Data analysis was calculated using the R language, version 4.0.2, with the rms and survival libraries (The R Foundation for Statistical Computing, Vienna, Austria, http://www.r-project.org/).
Results
Patient Characteristics
Clinical characteristics of the 111 patients are detailed in Table 1. Eligible patients were pathologically diagnosed as OSCC. The cohort included 34 (30.6%) females and 48 (43.2%) never-smokers, with an age range of 28–81 years (average 56 years). Of these 111 patients, 29 (26.1%) were diagnosed with cT1–2 stage disease and 82 (73.9%) with cT3–4 stage disease.
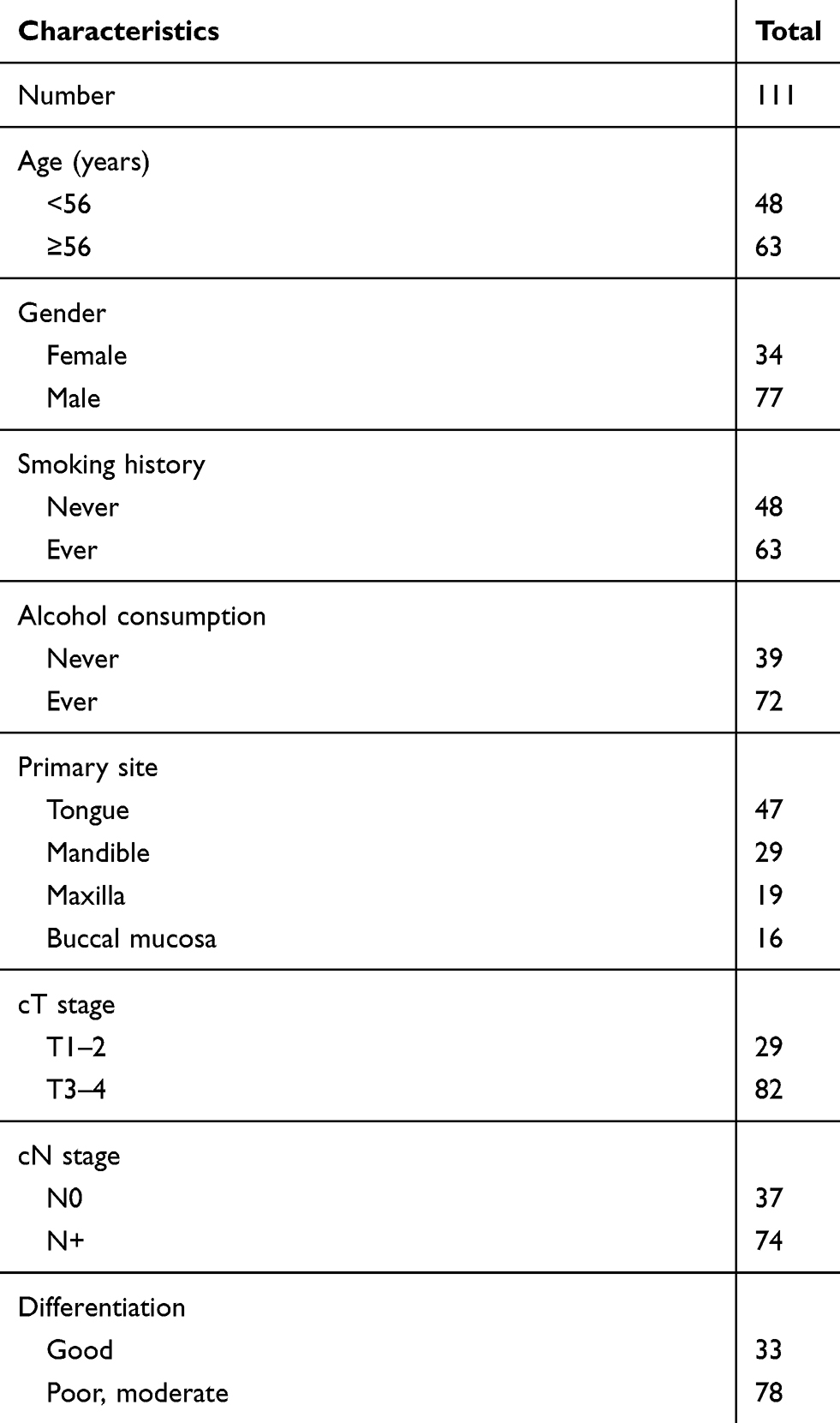 |
Table 1 Clinicopathological Characteristics in 111 patients with OSCC |
Applying clinical criteria set up by the department of laboratory medicine in our institute, we differentiated the serum biomarker LDH as below or above the reference range. The NLR and PLR were dichotomized by the cut-off values of NLR and PLR in survival outcome prediction of OSCC. The best cut-off for NLR (3.1) was defined as the value with the best relative risk coefficient. The area under the curve (AUC) of the dichotomized NLR was calculated in the time-dependent ROC curve. Compared to all other indicators, NLR achieved the largest AUC of 0.66, suggesting that it had the highest predictive value (Supplemental Figure 1).
Survival
To investigate whether the serum markers were associated with the survival outcome of OSCC patients, univariable and multivariate Cox regression analyses for OS were performed (Table 2). The median follow-up period was 38 months (range 4–84 months). During follow-up, tumor progression was observed in 74.8% of patients, with a median time to disease progression of 19 months (2–63 months). Then, 40.1% of patients with disease progression received subsequent chemotherapy. Figure 1 showed the Kaplan–Meier curves for OS, and revealed that inflammatory factors had an obvious impact on the OS of OSCC patients (NLR: HR=2.39, 95% CI 1.24–4.61, p=0.009; PLR: HR=2.13, 95% CI 1.05–4.34, p=0.037), whereas high LDH level was not related to the outcome of OSCC patients.
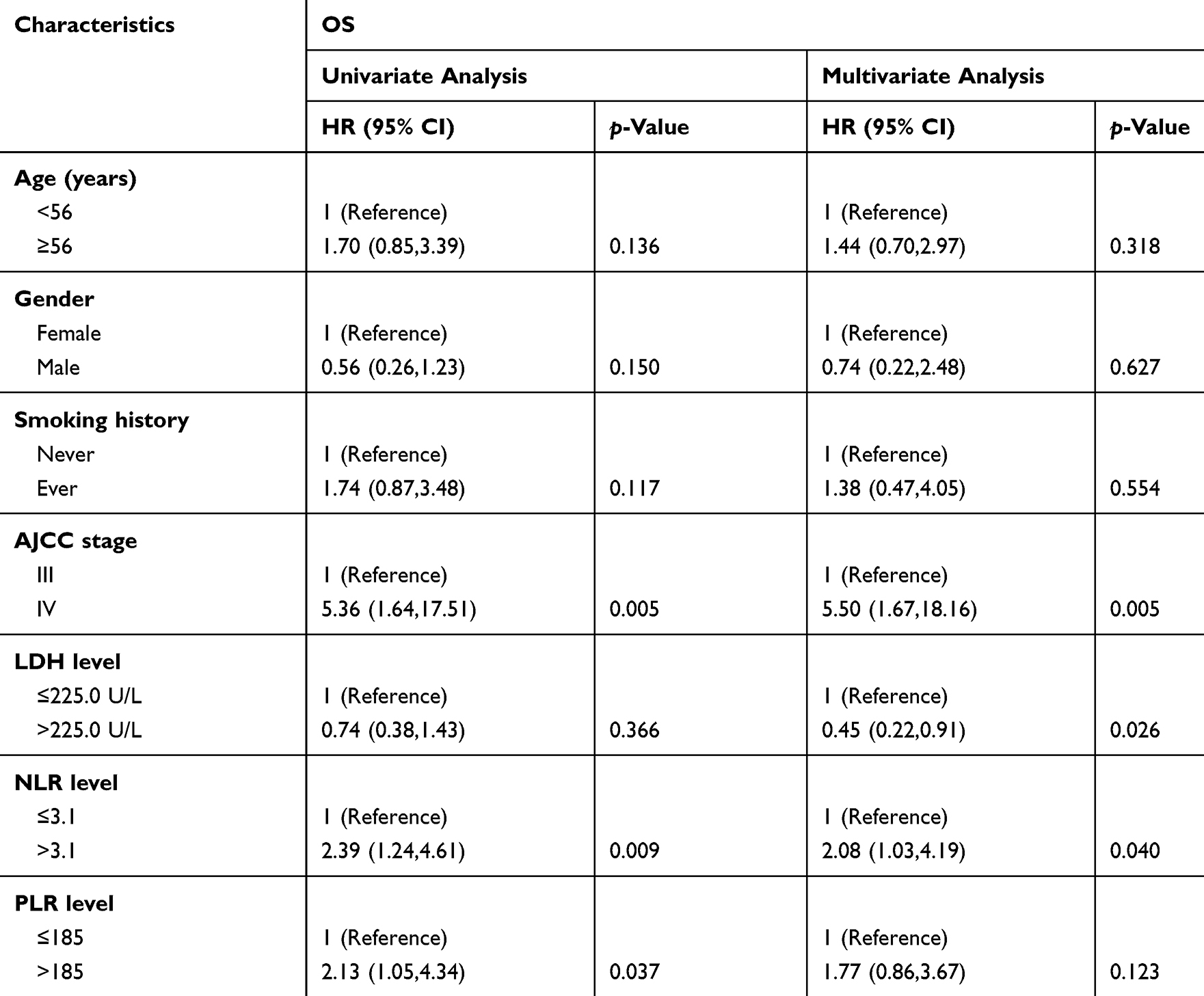 |
Table 2 Univariate and Multivariate Cox Regression Analyses of Multiple Variables for OS in Patients with OSCC (n=111) |
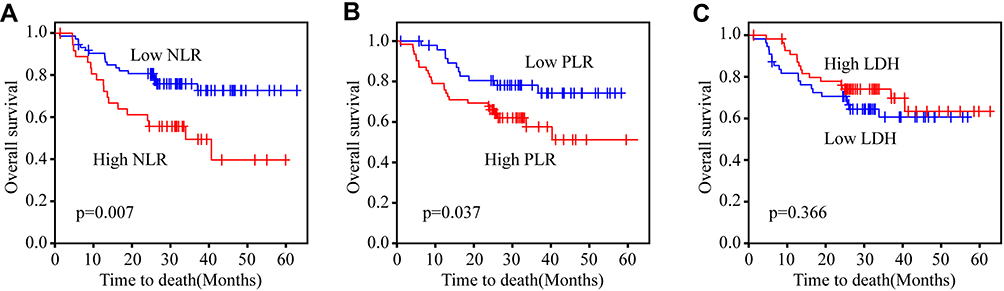 |
Figure 1 Prognosis analysis of serum indicators in OSCC. (A) Kaplan–Meier curve for OS revealed that high NLR was significantly associated with low OS rate in OSCC. (B) Kaplan–Meier curve for OS revealed that high PLR was significantly associated with low OS rate in OSCC. (C) Kaplan–Meier curve for OS revealed that LDH was not associated with OS rate in OSCC. |
To confirm whether NLR was an independent factor influencing outcome, multivariate Cox regression was conducted by the forward LR method. NLR level had a decisive impact on the OS of the patients (HR=2.08, 95% CI 1.03–4.19, p=0.04), which was more distinct than the effect of PLR on their survival. Importantly, we established a nomogram which applied the prognostic factors, including age, sex, smoking history, TNM staging, NLR and PLR, to evaluate the prognostic value of the inflammatory marker in the specific setting of patients (Figure 2). The Harrell’s concordance indices for OS in the clinicopathological multivariate model were 0.721. Notably, the addition of NLR and PLR to the clinicopathological model significantly improved the PA for OS to 0.74. The model displayed moderate levels of discrimination and adequate calibration.
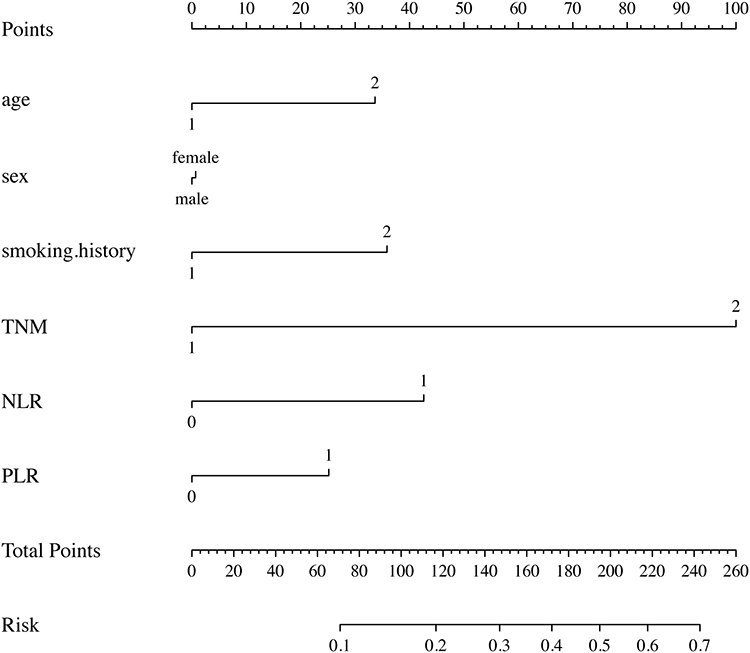 |
Figure 2 Nomogram predicting risk of mortality in OSCC patients. The nomogram is used by adding up the points identified on the points scale for each variable. The total projected on the bottom scale indicates the probability of mortality. |
Discussion
OSCC is the most common malignant tumor in the oral cavity and CRT is the regular treatment for OSCC.2 In recent years, with the development of targeted drugs, the prognosis for patients with OSCC has been extended.14,15 Immune checkpoint inhibitors have also shed light on the treatment of OSCC, and inflammation and immunity have been involved in the development of OSCC.16 However, the immunological characteristics of OSCC are still largely uncovered.
This study evaluated the correlation of pretreatment variables, including LDH and inflammatory markers, with mortality rates among patients with OSCC. The LDH, an enzyme facilitating the formation of lactic acid in the glycolytic pathway, is often used as an indicator to monitor and assess the state of disease in patients. Although LDH was uncovered in a variety of types of tissue damage, as well as in different malignant entities, there is still controversy about the predictive value of NLR, PLR and LDH for patients with OSCC.17–19 In the present study, low levels of NLR and PLR suggested favorable survival outcomes, while LDH was not associated with survival. The NLR was confirmed to be a useful predictive prognostic indicator for OSCC, consistent with previous studies of other kinds of cancer.
Our study indicated that NLR level was associated with AJCC stage. The mechanism behind an inflammation-driven tumorigenesis is not well defined, but our data suggest that tumor stage influences the counts of peripheral neutrophils and lymphocytes, which implies that the lymphocyte-associated immune response may be decreased as the tumor grows. Recent studies have revealed that blood biomarkers have predictive value in the immunotherapy of NSCLC, with higher inflammation, indicating worse survival in patients treated with checkpoint inhibitors.20–22 Whether NLR holds promise as a biomarker for the prediction of immunotherapy efficacy in OSCC is worthy of further study.
The present study developed the first prognostic model for the prediction of survival in OSCC patients undergoing CRT. However, this study has several limitations, including selection bias owing to the retrospective design and short follow-up period, as well as the heterogeneity of clinical parameters (eg, high percentage of men and stage IV patients), which may have resulted in shorter survival times compared with those shown in randomized clinical trials. Nevertheless, we conducted a thorough real-world study that provided preliminary evidence on the potential prognostic predictive value of serum inflammation markers in OSCC, and proposed a hypothesis which should be validated by prospective studies in order to distinguish the most appropriate cut-off for clinical use.
The present study collected data from 111 cases of OSCC, covering a period of 5 years, and indicated that the immunological marker NLR has the potential to be a predictive factor for the mortality of OSCC. Dynamic monitoring of NLR during treatment could be more effective in predicting OSCC prognosis, but we proved that NLR testing before CRT also has a prognostic predictive value for OSCC patients. The predictive value of NLR in immunotherapy is worthy of further evaluation in future clinical trials. Additional prospective studies are required to validate this prognostic model.
Data Sharing Statement
The data are contained within the article and/or its supplementary materials.
Ethics Approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the ethics board of our center (TJ-IRB20190404).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the National Natural Science Foundation of China (Nos. 82003310 and 81904019) and Foundation of Tongji Hospital (No. 2018YJJA02).
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Koyfman SA, Ismaila N, Crook D, et al. Management of the neck in squamous cell carcinoma of the oral cavity and oropharynx: ASCO clinical practice guideline. J Clin Oncol. 2019;37:1753–1774. doi:10.1200/JCO.18.01921
3. Chang CF, Huang PW, Chen JS, et al. Prognostic factors for advanced pancreatic cancer treated with gemcitabine plus S-1: retrospective analysis and development of a prognostic model. Cancers (Basel). 2019;11:57. doi:10.3390/cancers11010057
4. Prelaj A, Ferrara R, Rebuzzi SE, et al. Epsilon: a prognostic score for immunotherapy in advanced non-small-cell lung cancer: a validation cohort. Cancers (Basel). 2019;11(12):1954. doi:10.3390/cancers11121954
5. Sprinzl MF, Kirstein MM, Koch S, et al. Improved prediction of survival by a risk factor-integrating inflammatory score in sorafenib-treated hepatocellular carcinoma. Liver Cancer. 2019;8(5):387–402. doi:10.1159/000492628
6. Taniguchi K, Karin M. NF-B, inflammation, immunity and cancer: coming of age. Nat Rev Immunol. 2018;18:309–324.
7. Bilen MA, Martini DJ, Liu Y, et al. The prognostic and predictive impact of inflammatory biomarkers in patients who have advanced-stage cancer treated with immunotherapy. Cancer. 2019;125(1):127–134. doi:10.1002/cncr.31778
8. Gargiulo P, Dietrich D, Herrmann R, et al. Predicting mortality and adverse events in patients with advanced pancreatic cancer treated with palliative gemcitabine-based chemotherapy in a multicentre phase III randomized clinical trial: the APC-SAKK risk scores. Ther Adv Med Oncol. 2019;11:175883591881835. doi:10.1177/1758835918818351
9. Shi M, Zhao W, Zhou F, et al. Neutrophil or platelet-to-lymphocyte ratios in blood are associated with poor prognosis of pulmonary large cell neuroendocrine carcinoma. Transl Lung Cancer Res. 2020;9(1):45–54.
10. Jantharapattana K, Kotamnivates T, Hirunpat S, Jarumanokul R. Correlation between serum squamous cell carcinoma antigen level and tumor volume in head and neck cancer. ORL. 2018;80:284–289. doi:10.1159/000491494
11. Valvona CJ, Fillmore HL, Nunn PB, Pilkington GJ. The regulation and function of lactate dehydrogenase a: therapeutic potential in brain tumor. Brain Pathol. 2016;26:3–17. doi:10.1111/bpa.12299
12. Diao P, Wu Y, Ge H, et al. Preoperative circulating platelet, neutrophil, and lymphocyte counts predict survival in oral cancer. Oral Dis. 2019;25(4):1057–1066. doi:10.1111/odi.13049
13. Yu W, Dou Y, Wang K, et al. Preoperative neutrophil lymphocyte ratio but not platelet lymphocyte ratio predicts survival and early relapse in patients with oral, pharyngeal, and lip cancer. Head Neck. 2019;41(5):1468–1474. doi:10.1002/hed.25580
14. Gupta P, Singh M, Kumar R, et al. Synthesis and in vitro studies of PLGA-DTX nanoconjugate as potential drug delivery vehicle for oral cancer. Int J Nanomedicine. 2018;13:67–69. doi:10.2147/IJN.S124995
15. Ohnishi Y, Yasui H, Nozaki M, Nakajima M. Molecularly-targeted therapy for the oral cancer stem cells. Jpn Dent Sci Rev. 2018;54:88–103. doi:10.1016/j.jdsr.2017.11.001
16. Pestana RC, Becnel M, Rubin ML, et al. Response rates and survival to systemic therapy after immune checkpoint inhibitor failure in recurrent/metastatic head and neck squamous cell carcinoma. Oral Oncol. 2020;101:104523. doi:10.1016/j.oraloncology.2019.104523
17. Guo G, Wang Y, Zhou Y, et al. Immune cell concentrations among the primary tumor microenvironment in colorectal cancer patients predicted by clinicopathologic characteristics and blood indexes. J Immunother Cancer. 2019;7(1). doi:10.1186/s40425-019-0656-3
18. Ren X, Zhang Y, Lyu Y, et al. Lactate dehydrogenase and serum tumor markers for predicting metastatic status in geriatric patients with lung adenocarcinoma. Cancer Biomarkers. 2019;26(2):139–150. doi:10.3233/CBM-190201
19. Wang Y, Qu X, Kam NW, et al. An inflammation-related nomogram for predicting the survival of patients with non-small cell lung cancer after pulmonary lobectomy. BMC Cancer. 2018;18(1). doi:10.1186/s12885-018-4513-4
20. Amaral SR, Casal Moura M, Carvalho J, Chaves A, Jesus E, Sousa G. 6P Prognostic significance of neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) in non-small cell lung cancer (NSCLC) treated with immune checkpoint inhibitors. Ann Oncol. 2019;30:mdz027–004.
21. Diem S, Schmid S, Krapf M, et al. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer. 2017;111:176–181. doi:10.1016/j.lungcan.2017.07.024
22. Passiglia F, Galvano A, Castiglia M, et al. Monitoring blood biomarkers to predict nivolumab effectiveness in NSCLC patients. Ther Adv Med Oncol. 2019;11:1758835919839928. doi:10.1177/1758835919839928
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.