")
Back to Journals » Journal of Inflammation Research » Volume 14
Inflammation-Immunity-Nutrition Score: A Novel Prognostic Score for Patients with Resectable Colorectal Cancer
Authors Li XY, Yao S, He YT, Ke SQ, Ma YF, Lu P, Nie SF, Wei SZ, Liang XJ , Liu L
Received 28 May 2021
Accepted for publication 17 August 2021
Published 10 September 2021 Volume 2021:14 Pages 4577—4588
DOI https://doi.org/10.2147/JIR.S322260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Xin-Ying Li,1 Shuang Yao,1 Yang-Ting He,1 Song-Qing Ke,1 Yi-Fei Ma,2 Ping Lu,3 Shao-Fa Nie,1 Shao-Zhong Wei,2 Xin-Jun Liang,3 Li Liu1
1Department of Epidemiology and Biostatistics, The Ministry of Education Key Laboratory of Environment and Health, School of Public Health, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Gastrointestinal Oncology Surgery, Hubei Cancer Hospital, The Seventh Clinical School Affiliated of Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 3Department of Abdominal Oncology, Hubei Cancer Hospital, The Seventh Clinical School Affiliated of Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Li Liu
Department of Epidemiology and Biostatistics, the Ministry of Education Key Laboratory of Environment and Health, School of Public Health, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Tel/Fax +86-27-83693763
Email [email protected]
Xin-Jun Liang
Department of Abdominal Oncology, Hubei Cancer Hospital, The Seventh Clinical School Affiliated of Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Tel/Fax +86-27-87671663
Email [email protected]
Purpose: This study was designed to investigate the prognostic value of the combination of high-sensitivity C-reactive protein, lymphocyte, and albumin in patients with resectable colorectal cancer.
Patients and Methods: Seven-hundred-and-nineteen patients who underwent colorectal cancer resection in Hubei Cancer Hospital were included. Inflammation-Immunity-Nutrition score (0– 6) was constructed based on preoperative high-sensitivity C-reactive protein, lymphocyte, and albumin. Time-dependent receiver operating characteristic curve, decision curve, Kaplan-Meier survival curve, Cox regression, and C-index were conducted to detect the prognostic values of inflammation-immunity-nutrition score. The prognostic values of inflammation-immunity-nutrition score in different subgroups by sex, location of tumor, pathologic stage, and KRAS mutation were also explored. The prognostic performance of inflammation-immunity-nutrition score was further compared with that of other traditional prognostic indicators.
Results: The median follow-up time was 40 months. High inflammation-immunity-nutrition score (> 2 scores) presented worse survival, with the adjusted hazard ratios (95% confidence intervals) of 3.106 (2.202– 4.380) for overall survival and 2.105 (1.604– 2.764) for disease-free survival. Besides, the associations of high inflammation-immunity-nutrition score with overall survival were even stronger in cases with wild type KRAS, with the adjusted hazard ratios (95% confidence intervals) of 4.018 (2.355– 6.854). Considering the AUCs, C-indices, and hazard ratios estimates, inflammation-immunity-nutrition score presented better prognostic performance than high-sensitivity modified Glasgow prognostic score, high-sensitivity C-reactive protein to albumin ratio, prognostic nutrition index, carcinoembryonic antigen, and carbohydrate antigen 19-9 for overall survival.
Conclusion: Inflammation-immunity-nutrition score might serve as a powerful prognostic score in patients with colorectal cancer for overall survival, particularly in patients with wild type KRAS.
Keywords: high-sensitivity C-reactive protein, survival, colorectal cancer, inflammation
Introduction
Colorectal cancer (CRC) is the third most threatening cancer worldwide, with the estimated more than 1.9 million new cases and 935,000 deaths in 2020.1 The statuses of inflammation, immunity, and nutrition of organism have been proposed as potential prognostic factors for CRC. High-sensitivity C-reactive protein (hsCRP), lymphocyte (LYM), and albumin (ALB) are representative indicators of inflammation, immunity, and nutrition status in clinical practice, respectively. HsCRP is an acute phase inflammatory protein that is synthesized in the liver,2,3 and responds as a sensitive but non-specific biomarker for systemic inflammation.4 In addition, lymphocyte counts also reflect the systemic inflammation and immune status.5 ALB could reflect individual’s nutritional status, which is closely related to immune function.6 HsCRP has been reported as a risk factor for cancers, including CRC, as researchers have investigated associations between inflammation and cancer growth.7,8 Serum ALB level was suggested to be a prognostic factor of CRC.9 Infiltration of LYM has been associated with improved prognosis of CRC.10
Prognostic scores derived from the combination of several of C-reactive protein (CRP), hsCRP, LYM, and ALB have been constructed and presented better performance than individual indicators.11–13 The high-sensitivity modified Glasgow Prognostic Score (hs-mGPS: the combination of hsCRP and ALB), hsCRP/ALB, and prognostic nutrition index (PNI: the combination of LYM and ALB) have been proposed as predictors for survival of cancer patients.14–18 A comparative study reported that the prognostic value of Glasgow Prognostic Score (GPS: the combination of CRP and ALB) was better than those of CRP and ALB in patients with hepatocellular carcinoma.19 A multicenter study also found better prognostic performance of PNI than ALB in patients with pancreatic cancer.20
Considering the improved prognostic values of hs-mGPS, hsCRP/ALB, and PNI than individual indicators, we hypothesized that further combination of inflammation, immunity, and nutrition indicators might present even better prognostic performance for CRC. Hence, the current study was aimed to construct a prognostic predictor derived from hsCRP, LYM, and ALB and evaluate its prognostic performance for survival of patients with resectable CRC.
Materials and Methods
Study Population
Between January 2015 and December 2017, 757 patients who underwent CRC tumor operative resection with curative intent in Hubei Cancer Hospital were enrolled. The exclusion criteria of patients were as follows: (1) having history of malignant tumors or concurrent other malignant tumors; (2) unclear pathological TNM stage; (3) having missing information on preoperative hsCRP level, serum ALB level, or LYM counts; (4) preexisting inflammatory conditions, such as active or chronic infection; (5) censoring within 90 days from tumor resection. Finally, 719 patients were included in the study (Figure 1). The study was approved by the Review Board of Hubei Cancer Hospital, and written informed consent was obtained from all patients. This study was conducted in accordance with the Declaration of Helsinki.
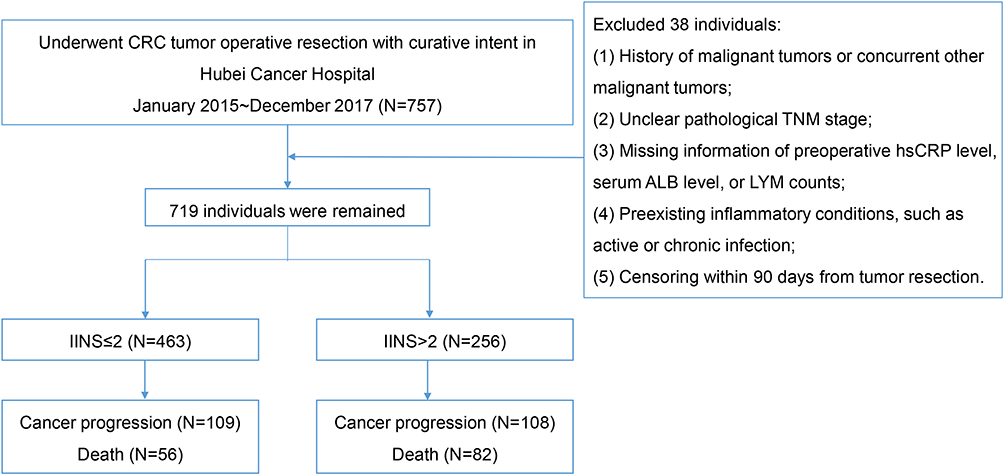 |
Figure 1 The flow chart of the colorectal cancer study population. Abbreviations: CRC, colorectal cancer; hsCRP, high-sensitivity C-reactive protein; ALB, albumin; LYM, lymphocyte; IINS, inflammation-immunity-nutrition score. |
Data Collection
The patients’ clinicopathological characteristics including age, sex, tumor location, histological type, pathological stage, differentiation, circumferential margin, vascular tumor thrombus, Kirsten rat sarcoma viral oncogene homolog (KRAS) status, neoadjuvant therapy, tumor resection information, postoperative adjuvant therapy, and blood indicators were collected from medical records. Blood indicators included carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), hsCRP, LYM, and ALB were measured within 7 days before tumor operative resection. LYM counts were obtained by routine blood tests.21 Pathological stage was confirmed according to the 7th American Joint Committee on Cancer staging. No patient underwent emergency resection. The patients were treated according to the diagnosis and treatment guidelines of the National Health Commission of the People’s Republic of China.
Follow-Up
After tumor resection, we obtained outcomes by reviewing medical records and making follow-up calls every 3–6 months for the first and second years, and then every 6 months for the third to fifth years. The primary outcome was overall survival (OS), and the secondary outcome was disease-free survival (DFS). OS was defined as the interval from the date of tumor diagnosis to the date of death, lost to follow-up, or the end of the follow-up (November 2020), whichever came first. DFS was defined as the interval from the date of tumor diagnosis to the date of death, recurrence or metastasis, loss to follow-up, or the end of the follow-up, whichever came first.
Calculation
We selected the optimum cut-offs for hsCRP, LYM, and ALB using X-tile software version 3.6.1 (https://medicine.yale.edu/lab/rimm/research/software/, Yale University School of Medicine, New Haven, CT) based on the association between each indicator with the patients’ OS.22 Based on 2 cut-offs, hsCRP was divided into 3 groups (score 0: ≤3.22 mg/L, score 1: >3.22 mg/L and ≤73.10 mg/L, score 2: >73.10 mg/L); whereas the classification of LYM and ALB was as follows: LYM (score 0: >1.34×109/L, score 1: >0.89×109/L and ≤1.34×109/L, score 2: ≤0.89×109/L); ALB (score 0: >42.60 g/L, score 1: >36.10 g/L and ≤42.60 g/L, score 2: ≤36.10 g/L). Then, the inflammation-immunity-nutrition score (IINS) was generated by summing the scores of hsCRP, LYM, and ALB. Since the median of IINS was 2 in the study, IINS > 2 was defined as high IINS group. For example, one patient’ preoperative hsCRP, LYM, and ALB values were 208 mg/L, 1.53×109/L, and 38.4 g/L, respectively. Next, the hsCRP, LYM, and ALB scores were 2, 0, and 1, respectively. Then, the IINS was 3 (high IINS).
To compare the performance of IINS with traditional prognostic predictors, we also calculated the scores of CEA, CA19-9, hsCRP/ALB, PNI, and hs-mGPS for each patient. The optimum cut-offs for CEA, CA19-9, hsCRP/ALB, and PNI derived from receiver operating characteristic (ROC) curves are presented as Supplemental Table 1. PNI is calculated by summing ALB value and 5 times of LYM counts. The definition of hs-mGPS is as follows: 0: hsCRP ≤3 mg/L and any levels of ALB concentration; 1: hsCRP >3 mg/L and normal levels of ALB (≥35 g/L); 2: hsCRP >3 mg/L and ALB < 35 g/L.23
Statistical Analysis
Continuous variables were presented as median [interquartile range (IQR)] or mean [standard deviation (SD)]. The Student’s t-test or the Wilcoxon rank sum test was used for comparisons between groups with continuous variables. Categorical variables were expressed by counts and percentages. The chi-square test was used for comparison between groups with categorical variables, and the Fisher's exact test was used when the counts were limited. The area under the curves (AUCs) and Harrell’s concordance indices (C-indices) of the indicators (IINS, hs-mGPS, hsCRP/ALB, PNI, CEA, and CA19-9) were estimated and compared by q values (adjusted P values by Benjamini&Hochberg method). The AUCs and C-indices were calculated based on logistic regression models and Cox regression models, respectively. Therefore, to demonstrate the prognostic performances of indicators well, the AUCs and C-indices were calculated together.24,25 Time-dependent ROC curves, time-AUC curves, decision curve analysis (DCA), Kaplan–Meier survival curves and Log rank tests were used to detect the prognostic performance of IINS. Compared with ordinary ROC curve, time-dependent ROC curve could observe the prognostic performance of indicator at a specific point in time after operation. Furthermore, time-AUC curve could observe the dynamic prognostic performance of indicator at all point in time after operation. Decision curve analysis is conducted to determine the clinical usefulness of the indicator via quantifying the net benefits at different threshold probabilities. Univariate and multivariate Cox proportional hazards regression were applied to detect the associations of individual clinicopathological indicators with OS/DFS by calculating hazard ratios (HRs) and 95% confidence intervals (CIs). The HRs (95% CIs) of IINS in different subgroups by sex, location of tumor, pathologic stage, and KRAS mutation were shown as forest plots.
All statistical tests were two-sided, and P<0.05 was considered statistically significant. Time-dependent ROC curves, time-AUC curves, decision curves, Kaplan–Meier survival curves, C-indices, and forest plots were performed using packages “survivalROC”, “timeROC”, “ggDCA”, “survminer”, “survival”, and “forestplot” of R 3.6.0 (The R Foundation for Statistical Computing, Vienna, Austria), respectively. Other statistical analyses were performed using SAS Statistics software 9.4 (SAS Institute Inc, Cary, North Carolina, USA).
Results
The Characteristics of Included Patients with Colorectal Cancer
The clinicopathologic characteristics of the participants are listed in Table 1. Of the 719 patients included in the study, 427 (59.39%) were men, and the median (IQR) age of all patients was 58 (50–66) years. Among the patients included in the study, 411 (57.16%) were colon cancer and 308 (42.84%) were rectum cancer. A total of 671 patients were non-mucinous adenocarcinoma, accounting for 93.32%. Tumors of pathological stages I, II, III, IV accounted for 126 (17.52%), 224 (31.15%), 263 (36.58%) and 106 (14.74%), respectively. Of the 513 patients detected for KRAS, 150 (29.24%) had mutated KRAS. The patients with high IINS were more likely to have advanced (pathological stage IV: 19.92%) and poorly differentiated (low-differentiation: 18.36%) cancer, higher CA19-9 (mean: 181.53 kU/L) and hsCRP (mean: 64.48 mg/L) levels, but lower ALB (mean: 36.87 g/L) and LYM (mean: 1.22×109/L) levels. The median follow-up time of the study was 40 months. At the end of follow-up, 217 (30.18%) presented cancer progression, and 138 (19.19%) patients died. Patients with high IINS were more likely to present cancer progression (42.19%) and death (32.03%), but lower postoperative radiotherapy rate (5.47%). Patients with rectal cancer were less likely to receive preoperative chemotherapy (3.25%), preoperative radiotherapy (1.62%) and postoperative radiotherapy (4.55%) (Supplemental Table 2).
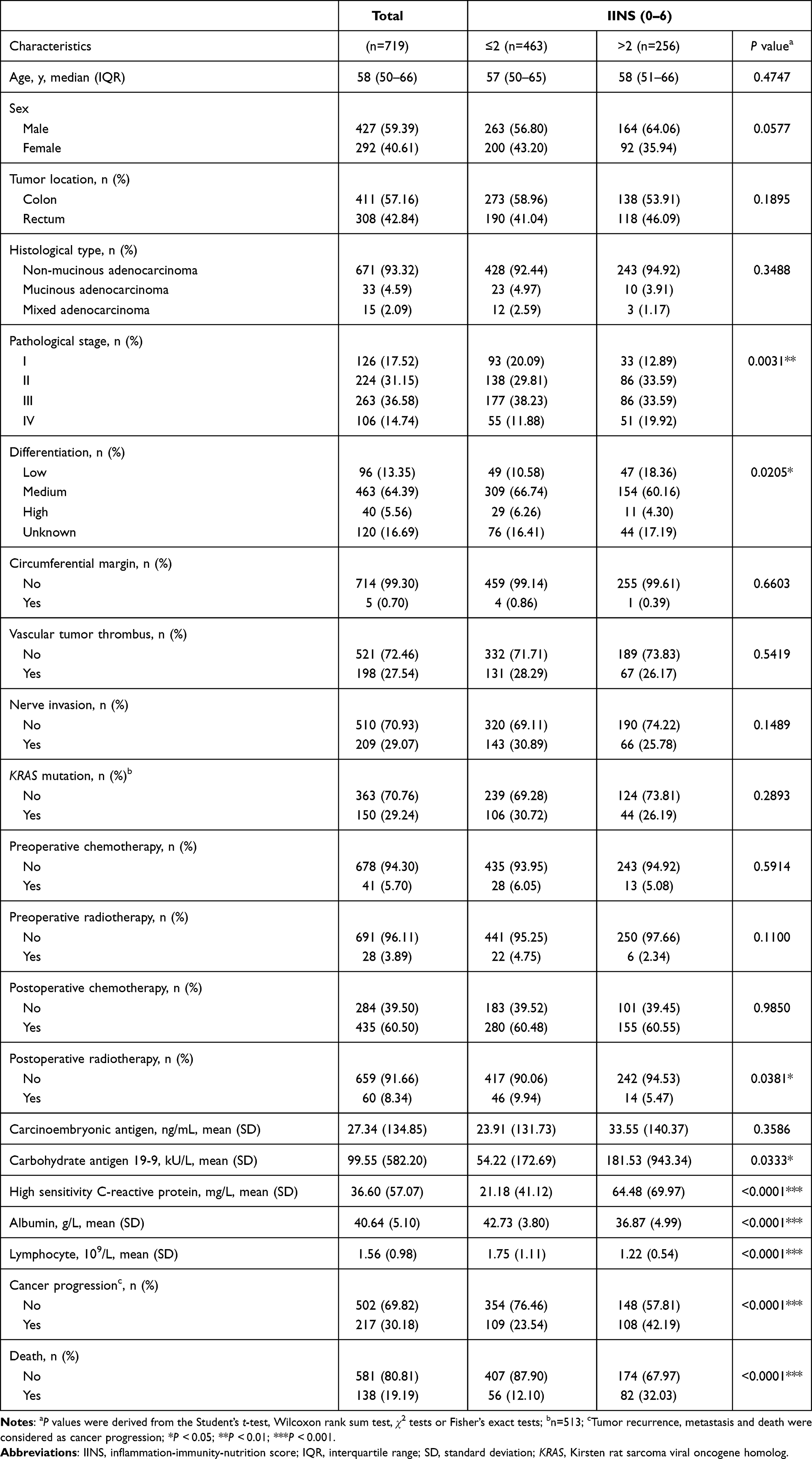 |
Table 1 Characteristics of Patients with Resectable Colorectal Cancer |
Relationships Between Inflammation-Immunity-Nutrition Score and the Prognosis of Patients with Colorectal Cancer
High IINS were associated with worse OS, with the multivariable-adjusted HR (95% CI) of 3.106 (2.202–4.380) (Supplemental Table 3). In addition, the time-dependent ROC curve showed that IINS presented good performance for OS (1-year AUC: 0.762, 2-year AUC: 0.716, 3-year AUC: 0.675) (Figure 2A). Similarly, high IINS presented worse DFS, with the HR (95% CI) of 2.105 (1.604–2.764) after adjusted for covariates of pathological stage, differentiation, vascular tumor thrombus, nerve invasion, and postoperative chemotherapy (Supplemental Table 4). The time-dependent ROC curves (1-year, 2-year, and 3-year) indicated that IINS presented relatively good prognostic value for DFS (Figure 2B). Besides, the AUCs of IINS for OS were relatively stable over time (Figure 2C), and the time-AUC curves of IINS for DFS are plotted as Figure 2D. The decision curves showed that the clinical usefulness of IINS was valuable (Figure 2E and F). The survival curves of IINS are also plotted as Figure 2G and H. In addition, combined with IINS, the prognostic performances of pathological stage for OS (P=0.0030) and DFS (P=0.0006) were improved significantly (Figure 3).
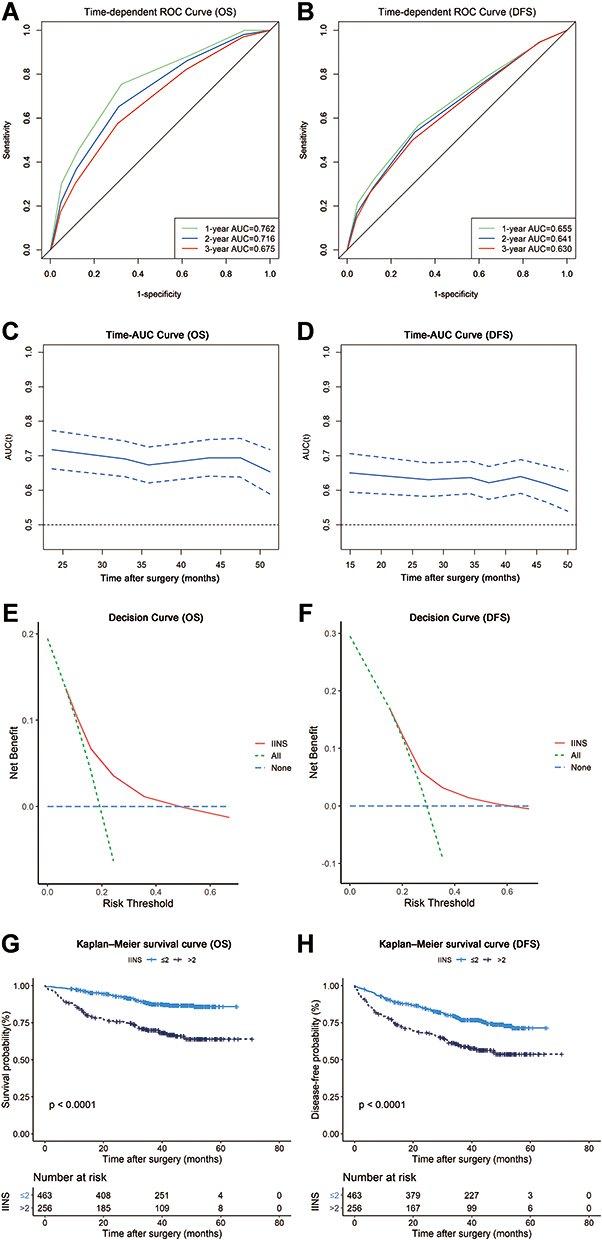 |
Figure 2 The prognostic performance of inflammation-immunity-nutrition score (IINS) in patients with resectable colorectal cancer. (A) The time-dependent ROC curves of IINS for OS; (B) the time-dependent ROC curves of IINS for DFS; (C) the time-AUC curves of IINS for OS; (D) the time-AUC curves of IINS for DFS; (E) the decision analysis curves of IINS for OS; (F) the decision analysis curves of IINS for DFS; (G) the Kaplan–Meier survival curves of IINS for OS; (H) the Kaplan–Meier survival curves of IINS for DFS. Abbreviations: ROC, receiver operating characteristic; OS, overall survival; DFS, disease-free survival; AUC, area under the curve. |
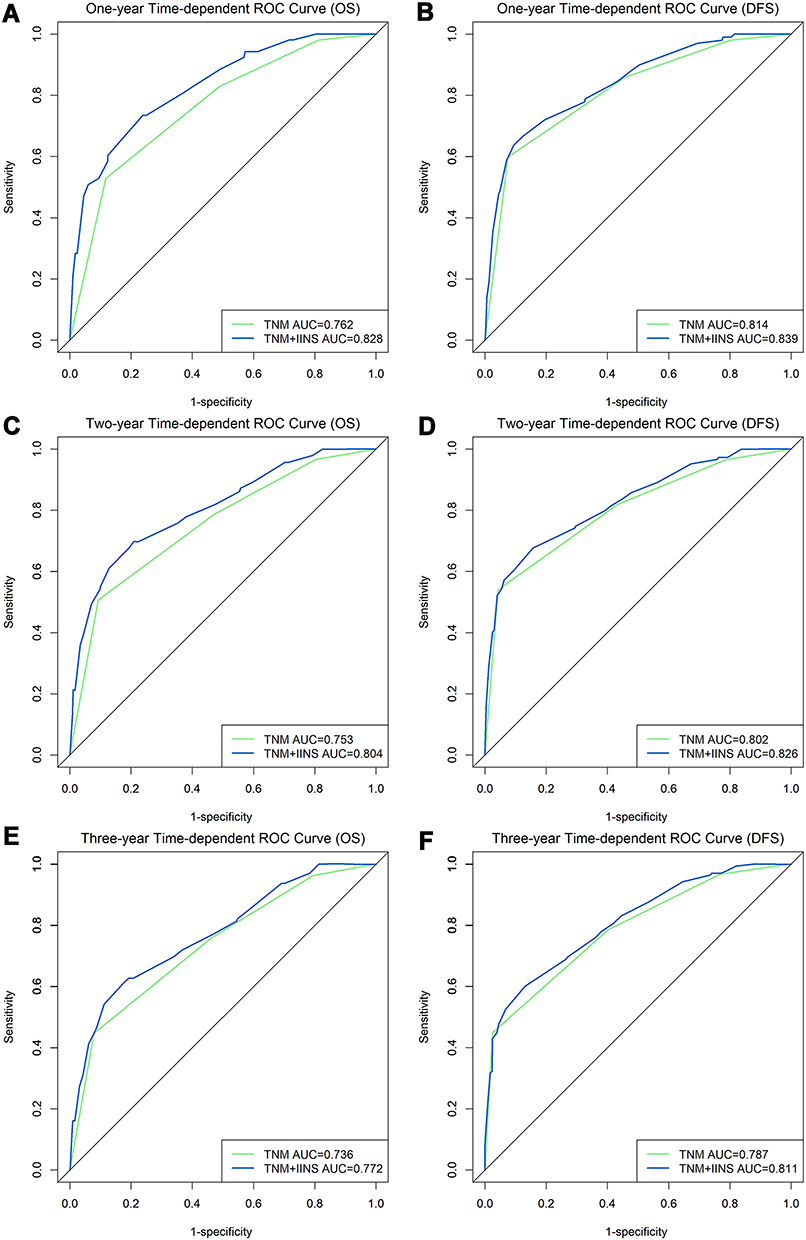 |
Figure 3 The prognostic performance of pathological stage combined with IINS in patients with resectable colorectal cancer. (A) The one-year time-dependent ROC curves for OS; (B) the one-year time-dependent ROC curves for DFS; (C) the two-year time-dependent ROC curves for OS; (D) the two-year time-dependent ROC curves for DFS; (E) the three-year time-dependent ROC curves for OS; (F) the three-year time-dependent ROC curves for DFS. Abbreviations: ROC, receiver operating characteristic; OS, overall survival; DFS, disease-free survival; AUC, area under the curve; IINS, inflammation-immunity-nutrition score. |
Relationships Between Inflammation-Immunity-Nutrition Score and the Prognosis of Patients with Colorectal Cancer in the Subgroups
The associations between IINS and OS presented suggestive heterogeneity according to sex (I2=68.34, P=0.0756) and KRAS status (I2=68.39, P=0.0753). On the contrary, the associations between IINS and OS did not present heterogeneity according to tumor location (I2=0, P=0.5296) and pathologic stage (I2=0, P=0.527). High IINS presented stronger associations with OS in male and patients with wild type (WT) KRAS, with the adjusted HRs (95% CIs) of 4.267 (2.627–6.929) and 4.018 (2.355–6.854), respectively (Figure 4A). The subgroup analysis did not find any heterogeneity for the associations between IINS and DFS by sex, location of tumor, pathologic stage, or KRAS mutation (Figure 4B).
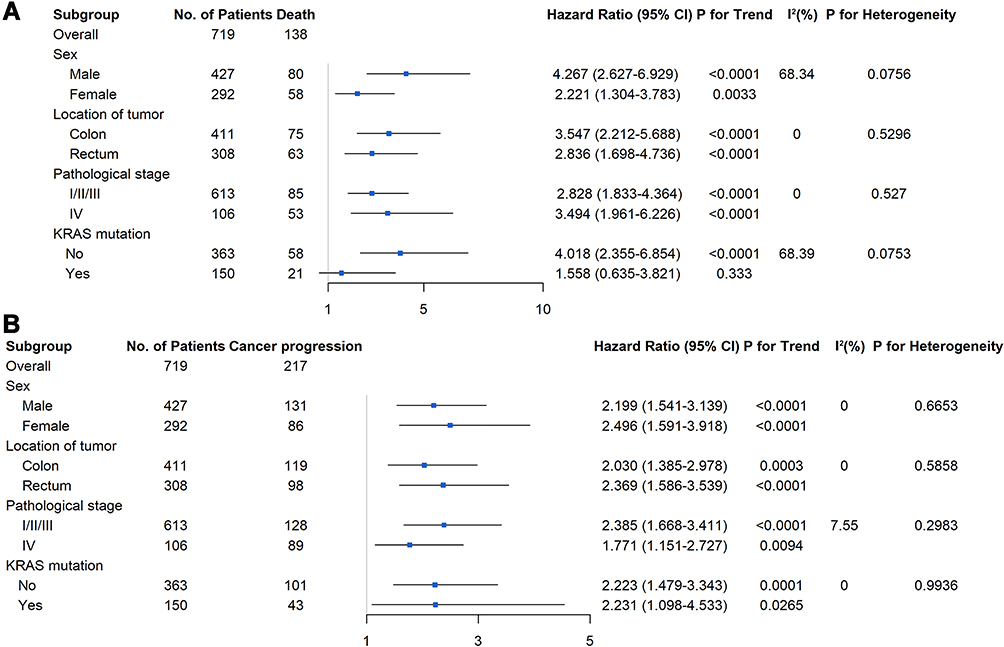 |
Figure 4 The forest plots of the hazard ratios of high inflammation-immunity-nutrition score (IINS) with overall survival (A) and disease-free survival (B) in patients with resectable colorectal cancer. Abbreviations: CI, confidence interval; KRAS, Kirsten rat sarcoma viral oncogene homolog. Notes: Pathological stage, differentiation, and nerve invasion were used as covariates in multivariate Cox regression analysis for overall survival; Pathological stage, differentiation, vascular tumor thrombus, nerve invasion, and postoperative chemotherapy were used as covariates in multivariate Cox regression analysis for disease-free survival. |
Comparing the Prognostic Values of Inflammation-Immunity-Nutrition Score with Other Traditional Indicators
To distinguish the prognostic values of IINS with other traditional indicators including hs-mGPS, hsCRP/ALB, PNI, CEA, and CA19-9, the AUCs (95% CIs), C-indices (95% CIs), and HRs (95% CIs) of the indicators were calculated. IINS presented the best prognostic performance among the indicators for OS (Table 2). The AUC of IINS for OS was higher than that of hs-mGPS (q=0.0001) and hsCRP/ALB (q=0.0005). The C-index of IINS for OS was higher than that of hs-mGPS (q<0.0001), hsCRP/ALB (q=0.0001), and PNI (q<0.0001). In addition, the HR of high IINS was 3.106 (95% CI: 2.202–4.380), which was higher than that of hsCRP/ALB (HR: 1.640; 95% CI: 1.169–2.303; q=0.019), CEA (HR: 1.650; 95% CI: 1.164–2.340; q=0.019), and CA19-9 (HR: 1.457; 95% CI: 1.026–2.069; q=0.013). Differently, the IINS only presented relatively better prognostic performance than hs-mGPS and PNI for DFS (Table 3). The C-index of IINS for DFS was higher than that of hs-mGPS (q=0.027) and PNI (q<0.0001). No difference was found between AUCs and HRs. The survival curves of these indicators are shown in Supplemental Figures 1 and 2. Combined with CEA or CA19-9, the prognostic performances of IINS for OS and DFS were improved significantly (P<0.05) (Supplemental Figure 3).
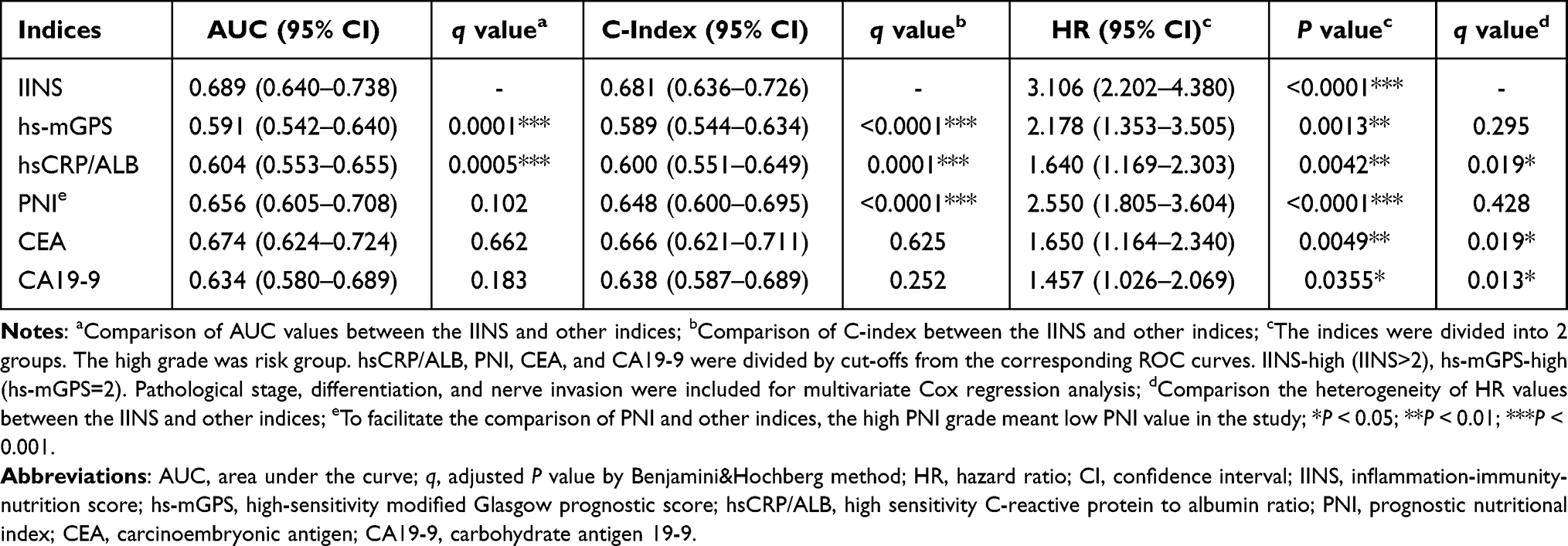 |
Table 2 Comparison of the Prognostic Performance Between the Indices in Overall Survival of Patients with Resectable Colorectal Cancer |
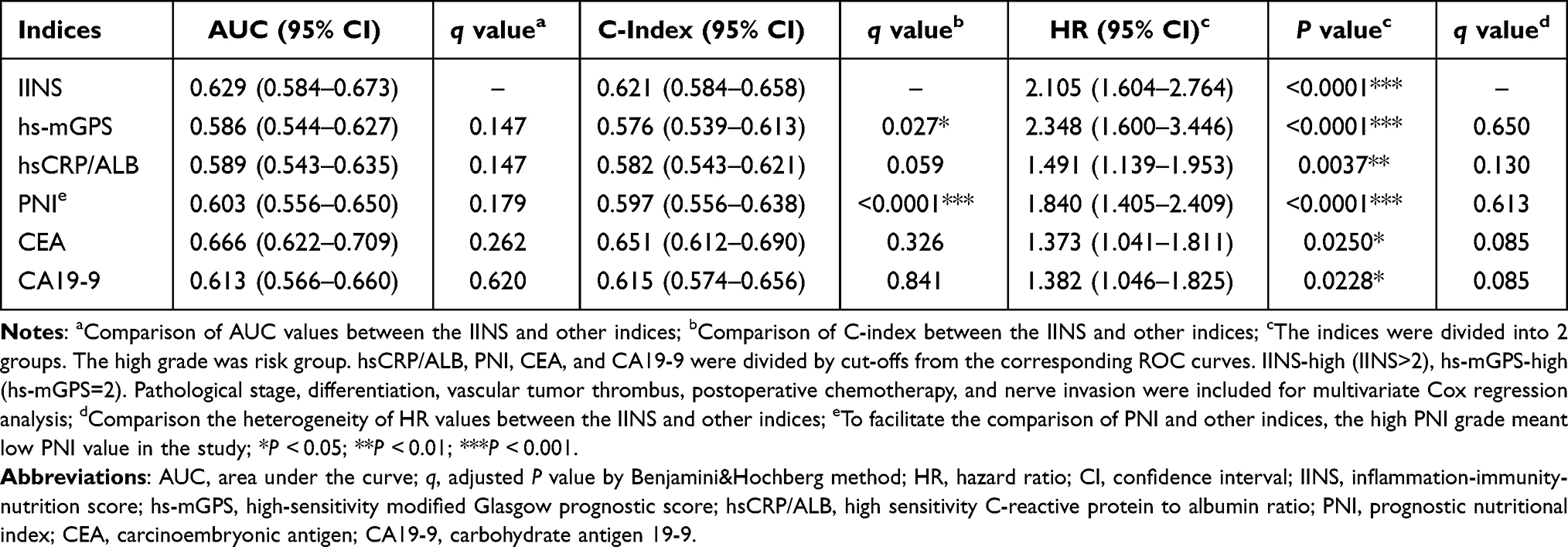 |
Table 3 Comparison of the Prognostic Performance Between the Indices in Disease-Free Survival of Patients with Resectable Colorectal Cancer |
Discussion
We conducted a study to construct a score, IINS, derived from hsCRP, LYM, and ALB, and evaluated its prognostic performance in resectable CRC. High IINS was associated with the worse survival of CRC, with the adjusted HRs of 3.106 and 2.105 for OS and DFS, respectively. Combined with IINS, the prognostic performances of pathological stage for OS and DFS were improved significantly. The associations between high IINS and OS were even stronger in WT KRAS patients (HR=4.018; 95% CI: 2.355–6.854). Further comparison revealed the better prognostic performance of IINS than hs-mGPS, hsCRP/ALB, PNI, CEA, and CA19-9 for OS in the current study.
A study has reported better OS for CRC patients with wild KRAS when compared with those with mutant type.26 In the study, among 363 WT KRAS patients, there were 58 patients dead at the end of follow-up. The HR (95% CI) of high IINS for OS in WT KRAS patients was 4.018 (2.355–6.854), which indicated that IINS showed a stronger correlation with the CRC prognosis in the protective KRAS situation (WT). The associations between IINS and OS/DFS were homogeneous between colon and rectal cancer, which implies the broader practicability of the IINS as a prognostic predictor throughout all colorectal cancer patients.
Previous studies have reported the prognostic values of hs-mGPS, hsCRP/ALB, and PNI in cancers,14–18,27 which were derived from two indicators of hsCRP, LYM, and ALB. To maximize the prognostic performance of these indicators, we combined hsCRP, LYM, and ALB for the first time to construct a new prognostic score, IINS. Consistent with our hypothesis that IINS presented better performance than hs-mGPS, hsCRP/ALB, PNI, CEA, and CA19-9 for OS. High IINS was associated with 3.1-fold risk of death compared with low IINS. A prognostic study reported the relationship between mGPS and CRC outcome, with the HRs of 1.62 (1 vs 0) and 2.67 (2 vs 0) for OS.28 A prognostic study reported that high serum CEA level predicted poor survival, with the HR of 1.661 for OS, which is consistent with our finding.29 Besides, comparable with previous reported AUCs 0.6–0.7 of mGPS, CRP/ALB and PNI for the survival of patients with CRC,30–32 our study revealed the AUCs of 0.591, 0.604 and 0.656 for hs-mGPS, hsCRP/ALB and PNI, which implies the repeatability of our results. Therefore, it is reasonable to infer that the better prognostic performance of IINS (AUC: 0.689; C-index: 0.681) is also valid for OS.
The predominant strength of the current study is that we innovatively constructed IINS based on hsCRP, LYM, and ALB, which presented better performance than some traditional indicators derived from the inflammatory, immune, and nutritional factors. What is more, IINS still showed a stronger correlation with the CRC prognosis in the situation of WT KRAS. Besides, IINS could be used to evaluate the prognosis of patients with CRC as an economical tool, which might guide the adjustment of patients’ follow-up strategies to improve prognosis in the future. Several limitations also exist. First, the sample size in this study was limited. Further studies with large samples were needed to verify the findings. Second, the mechanism of the stronger association between IINS and OS in the situation of WT KRAS needs to be clarified in further studies. Third, although there is few literature on the prognostic performances of hs-mGPS and hsCRP/ALB for colorectal cancer, the cut-offs of both CRP and hsCRP derived from clinical reference value. The repeatability of results (hs-mGPS and hsCRP/ALB) in this study could be observed by the prognostic performances of mGPS and CRP/ALB in other studies.
Conclusion
In conclusion, our study suggests that preoperative IINS present good prognostic performance in resectable CRC for OS, and might serve as a powerful prognostic tool in clinical practice.
Data Sharing Statement
The data sets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We express our appreciations to the participants who contributed to our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China to Shao-Fa Nie (Grant No. 81974491), the National Natural Science Foundation of China to Li Liu (Grant No. 81302491 and No. 82173602), the Health commission of Hubei Province scientific research project to Li Liu (Grant No. WJ2019Q027), the Applied Basic Research Program of Wuhan Science and Technology Bureau to Xin-Jun Liang (Grant No. 2020020601012250), the Foundation of Chinese Society of Clinical Oncology to Xin-Jun Liang (Grant No. CSCO: Y-HS2019-39 and No. CSCO: Y-QL2019-0351), the Health commission of Hubei Province scientific research project to Xin-Jun Liang (Grant No. WJ2021Z001), the National Key R&D Program of China to Shao-Zhong Wei (Grant No. 2017YFC0908200), the Health commission of Hubei Province scientific research project to Shao-Zhong Wei (Grant No. WJ2019H121), and the Hubei Provincial Natural Science Foundation to Shao-Zhong Wei (Grant No. 2019ACA135).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Leuzzi G, Galeone C, Gisabella M, et al. Baseline C-reactive protein level predicts survival of early-stage lung cancer: evidence from a systematic review and meta-analysis. Tumori. 2016;102(5):441–449. doi:10.5301/tj.5000522
3. Murata M. Inflammation and cancer. Environ Health Prev Med. 2018;23(1):50. doi:10.1186/s12199-018-0740-1
4. Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003;107(3):499–511. doi:10.1161/01.CIR.0000052939.59093.45
5. Ostroumov D, Fekete-Drimusz N, Saborowski M, Kühnel F, Woller N. CD4 and CD8 T lymphocyte interplay in controlling tumor growth. Cell Mol Life Sci. 2018;75(4):689–713. doi:10.1007/s00018-017-2686-7
6. Lu J, Xu BB, Zheng ZF, et al. CRP/prealbumin, a novel inflammatory index for predicting recurrence after radical resection in gastric cancer patients: post hoc analysis of a randomized Phase III trial. Gastric Cancer. 2019;22(3):536–545. doi:10.1007/s10120-018-0892-0
7. Li Y, Zhong X, Cheng G, et al. Hs-CRP and all-cause, cardiovascular, and cancer mortality risk: a meta-analysis. Atherosclerosis. 2017;259:75–82. doi:10.1016/j.atherosclerosis.2017.02.003
8. Wilhelmsen M, Christensen IJ, Rasmussen L, et al. Detection of colorectal neoplasia: combination of eight blood-based, cancer-associated protein biomarkers. Int J Cancer. 2017;140(6):1436–1446. doi:10.1002/ijc.30558
9. Wei Y, Xu H, Dai J, et al. Prognostic significance of serum lactic acid, lactate dehydrogenase, and albumin levels in patients with metastatic colorectal cancer. Biomed Res Int. 2018;2018:1804086. doi:10.1155/2018/1804086
10. Zitvogel L, Galluzzi L, Kepp O, Smyth MJ, Kroemer G. Type I interferons in anticancer immunity. Nat Rev Immunol. 2015;15(7):405–414. doi:10.1038/nri3845
11. Bodén S, Myte R, Harbs J, et al. C-reactive protein and future risk of clinical and molecular subtypes of colorectal cancer. Cancer Epidemiol Biomarkers Prev. 2020;29(7):1482–1491. doi:10.1158/1055-9965.EPI-19-1339
12. Ghuman S, Van Hemelrijck M, Garmo H, et al. Serum inflammatory markers and colorectal cancer risk and survival. Br J Cancer. 2017;116(10):1358–1365. doi:10.1038/bjc.2017.96
13. Tokunaga R, Sakamoto Y, Nakagawa S, et al. Comparison of systemic inflammatory and nutritional scores in colorectal cancer patients who underwent potentially curative resection. Int J Clin Oncol. 2017;22(4):740–748. doi:10.1007/s10147-017-1102-5
14. Zheng C, Liu S, Feng J, Zhao X. Prognostic value of inflammation biomarkers for survival of patients with neuroblastoma. Cancer Manag Res. 2020;12:2415–2425. doi:10.2147/CMAR.S245622
15. Nakamura T, Matsumine A, Asanuma K, Matsubara T, Sudo A. The value of the high-sensitivity modified Glasgow prognostic score in predicting the survival of patients with a soft-tissue sarcoma. Bone Joint J. 2015;97-B(6):847–852. doi:10.1302/0301-620X.97B.35098
16. Takeno S, Hashimoto T, Shibata R, et al. The high-sensitivity modified Glasgow prognostic score is superior to the modified Glasgow prognostic score as a prognostic predictor in patients with resectable gastric cancer. Oncology. 2014;87(4):205–214. doi:10.1159/000362601
17. Yang JR, Xu JY, Chen GC, et al. Post-diagnostic C-reactive protein and albumin predict survival in Chinese patients with non-small cell lung cancer: a prospective cohort study. Sci Rep. 2019;9(1):8143. doi:10.1038/s41598-019-44653-x
18. Luvián-Morales J, González-Trejo S, Carrillo JF, et al. Association of the prognostic nutritional index and overall survival in patients with colorectal cancer: a STROBE compliant retrospective cohort study. Cancer Med. 2019;8(7):3379–3388. doi:10.1002/cam4.2212
19. Huang J, Xu L, Luo Y, He F, Zhang Y, Chen M. The inflammation-based scores to predict prognosis of patients with hepatocellular carcinoma after hepatectomy. Med Oncol. 2014;31(4):883. doi:10.1007/s12032-014-0883-x
20. Kobayashi M, Shimodaira S, Nagai K, et al. Prognostic factors related to add-on dendritic cell vaccines on patients with inoperable pancreatic cancer receiving chemotherapy: a multicenter analysis. Cancer Immunol Immunother. 2014;63(8):797–806. doi:10.1007/s00262-014-1554-7
21. Chen JH, Zhai ET, Yuan YJ, et al. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J Gastroenterol. 2017;23(34):6261–6272. doi:10.3748/wjg.v23.i34.6261
22. Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10(21):7252–7259. doi:10.1158/1078-0432.CCR-04-0713
23. Woo Y, Hyung WJ, Obama K, et al. Elevated high-sensitivity C-reactive protein, a marker of advanced stage gastric cancer and postgastrectomy disease recurrence. J Surg Oncol. 2012;105(4):405–409. doi:10.1002/jso.22129
24. Di Stefano AL, Picca A, Saragoussi E, et al. Clinical, molecular, and radiomic profile of gliomas with FGFR3-TACC3 fusions. Neuro Oncol. 2020;22(11):1614–1624. doi:10.1093/neuonc/noaa121
25. Hou X, Wang D, Zuo J, et al. Development and validation of a prognostic nomogram for HIV/AIDS patients who underwent antiretroviral therapy: data from a China population-based cohort. EBioMedicine. 2019;48:414–424. doi:10.1016/j.ebiom.2019.09.031
26. Luo Q, Chen D, Fan X, Fu X, Ma T, Chen D. KRAS and PIK3CA bi-mutations predict a poor prognosis in colorectal cancer patients: a single-site report. Transl Oncol. 2020;13(12):100874. doi:10.1016/j.tranon.2020.100874
27. Zhou ZQ, Pang S, Yu XC, et al. Predictive values of postoperative and dynamic changes of inflammation indexes in survival of patients with resected colorectal cancer. Curr Med Sci. 2018;38(5):798–808. doi:10.1007/s11596-018-1946-6
28. Tsuchihashi K, Ito M, Moriwaki T, et al. Role of predictive value of the modified Glasgow prognostic score for later-line chemotherapy in patients with metastatic colorectal cancer. Clin Colorectal Cancer. 2018;17(4):
29. You W, Sheng N, Yan L, et al. The difference in prognosis of stage II and III colorectal cancer based on preoperative serum tumor markers. J Cancer. 2019;10(16):3757–3766. doi:10.7150/jca.31660
30. Suzuki Y, Okabayashi K, Hasegawa H, et al. Comparison of preoperative inflammation-based prognostic scores in patients with colorectal cancer. Ann Surg. 2018;267(3):
31. Shibutani M, Maeda K, Nagahara H, Iseki Y, Ikeya T, Hirakawa K. Prognostic significance of the preoperative ratio of C-reactive protein to albumin in patients with colorectal cancer. Anticancer Res. 2016;36(3):995–1001.
32. Sato R, Oikawa M, Kakita T, et al. The prognostic value of the prognostic nutritional index and inflammation-based markers in obstructive colorectal cancer. Surg Today. 2020;50(10):1272–1281. doi:10.1007/s00595-020-02007-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.