")
Back to Journals » Infection and Drug Resistance » Volume 15
Infection of Severe Fever with Thrombocytopenia Syndrome Virus as a Cause of a Child’s Fever of Unknown Origin: A Case Report
Authors Zhang Y , Huang Y, Xu Y
Received 20 June 2022
Accepted for publication 17 August 2022
Published 26 August 2022 Volume 2022:15 Pages 4871—4875
DOI https://doi.org/10.2147/IDR.S378558
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Yin Zhang, Ying Huang, Yuanhong Xu
Department of Clinical Laboratory, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China
Correspondence: Yuanhong Xu; Ying Huang, Department of Clinical Laboratory, The First Affiliated Hospital of Anhui Medical University, No. 218 Jixi Road, Hefei, People’s Republic of China, Email [email protected]; [email protected]
Background: Severe fever with thrombocytopenia syndrome (SFTS) is a tick-borne disease resulted from SFTSV. It is found in Japan, South Korea, Central, and Eastern China. With the increasing prevalence of SFTS and the rapid spread of the SFTS virus (SFTSV) vector, it is obvious that this virus has pandemic potential and poses an imminent public health concern.
Case Presentation: We depict SFTS in a child from Anhui Province and conduct a review of all reported pediatric cases in China, which is an endemic area for SFTS. From 2011 to 2021, ten SFTS pediatric cases confirmed by RT-PCR were reported, with no child dying. Although SFTS cases in adolescents and children are uncommon, the reported literature showed that clinical symptoms in adolescents and children were milder than in adults.
Conclusion: To better understand this emerging disease, we described the clinical and epidemiological attributes of SFTS. We suggest that the possibility of SFTSV infection in children with seasonal and virus-related acute febrile diseases should be considered in major endemic areas.
Keywords: SFTS, infection, children, Bunyaviridae virus, Dabie bandavirus
Introduction
A fatal viral hemorrhagic fever that is mostly transmitted to humans through tick bites, or contact with infected tissues or blood from infected humans or livestock is severe fever with thrombocytopenia syndrome (SFTS).1
In addition, direct infection of SFTS virus from cat blood or other body fluids to humans has been reported and recognized as a social problem.2,3 Currently, the underlying mechanisms are largely unknown. In 2018, the researchers first revealed the disorder of arginine metabolism caused by SFTSV infection by the metabonomics method. They then found that the decrease of platelet number and T lymphocyte dysfunction is related to the abnormality of arginine metabolism.4 Park et al showed that the B-cell lineage, especially plasma cells, is linked to lethality in SFTSV infections.5
According to previous studies, elderly residents in rural or hilly areas are at a higher risk of infection with SFTSV, and the majority of reported cases of SFTS were in older people.6 Therefore, most studies are based on adult data, and there are little pediatric data available. CHILDREN also could be infected with the SFTS virus; infection in this age group is uncommon. Although SFTSV reports in adolescents and children are uncommon, the literature revealed clinical manifestations that were similar to those in adult patients.7–12
This report aims to evaluate a pediatric case from Anhui Province and the clinical and epidemiological characteristics of SFTS in children in China, from 2011 to 2021.
Cases Presentation
A 3-year-old girl with no underlying disease had a 5-day-long fever with a high temperature of 40.5°C, loss of appetite, and weakness. There were no signs of diarrhea, cough, vomiting, sputum production, myalgias, urinary irritation, or unconsciousness. Her parents claimed that she played on the grass near her grandmother’s house during the Dragon Boat Festival (June 25 to 27), which was held in Lu’an City, Anhui Province, an epidemic area of the SFTSV. Her grandfather died of an SFTSV infection in 2017. She was sent to a community hospital after she developed fever symptoms on July 2. However, her fever did not disappear after the combined treatment of compound paracetamol methamphetamine oral liquid and oseltamivir for 3 days, and she was admitted to the First Affiliated Hospital of Anhui Medical University on July 5 for further treatment.
On admission, the patient had a pulse of 100 beats per minute, a 39.4°C fever, a rate of respiration of 14 breaths per minute, and blood pressure of 110/90 mmHg. Petechiae or ecchymosis was observed, and neurological assessments were negative. Diagnostic assessments revealed leukopenia (1.91 × 109 /L), thrombocytopenia (78 × 109 platelets/L) moderately enhanced lactate dehydrogenase (1620 U/L), aspartate aminotransferase (81 U/L), and alkaline phosphatase (160 U/L) levels (Table 1). The ultrasound results were normal. A chest CT scan revealed an increase in lung markings. Sinus tachycardia was detected on the EKG. Cefoperazone sulbactam sodium and ganciclovir were prescribed for controlling the infection based on his laboratory outcomes and clinical results.
 |
Table 1 Changes of Infection and Immunological Indexes in the Child with SFTS |
Considering the possibility of SFTS virus infection, the child was transferred to the infection department the next day. Vancomycin combined with cefoperazone, sulbactam for anti-infection, ribavirin (0.2 g, once a day for 7 d) combined with gamma globulin (20 g, once a day for 5 d) for anti-virus, and other supportive treatments were implemented as new treatment schemes.
On the third day in the hospital, the patient’s fever subsided, and her general circumstance and symptoms slowly augmented. Three days after being admitted to the hospital, the patient’s WBC and platelet counts had come back to normal. The other laboratory data were normalized over 8 to 21 days.
In addition, other etiological tests were negative, such as cytomegalovirus, EB virus, respiratory virus series, and blood culture. The blood samples on the second day of admission showed positive viral RNA by RT-PCR. The general analysis of urine revealed proteinuria and mild hematuria.
Cases Summary
Three of the ten pediatric patients have tick bites (Table 2), three have had close contact with SFTSV infected family members, and seven have rested and played in grassland.7,10–12
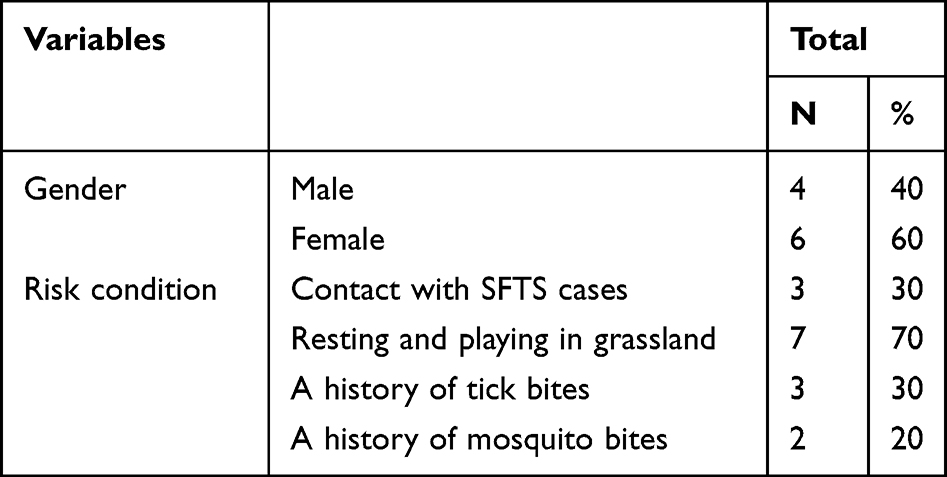 |
Table 2 Demographic and Epidemiological Characteristics of the 10 Cases of SFTS in Children from China, from 2011 to 2022 |
The pediatric patients’ median age was 5.5 (range 2–16) years old, with four males.7,10–12 Three of the patients had experienced tick bites while participating in outdoor activities. Three of them had close contact with SFTSV-infected family members. The pediatric cases were otherwise healthy and did not have any prior co-morbidities. Malaise fever and gastrointestinal syndromes were the most common reasons for hospitalization. This is consistent with the findings from adult patients. There were no signs of cough, dyspnea, consciousness disorder, production of sputum, or myalgias in the pediatric cases. Other common symptoms are seen in adult patients like nausea, diarrhea, petechiae, hematemesis, gingival bleeding, and hematuria, and are rarely seen in these pediatric patients. There were no neurological manifestations in any of the ten pediatric cases (Table 3).
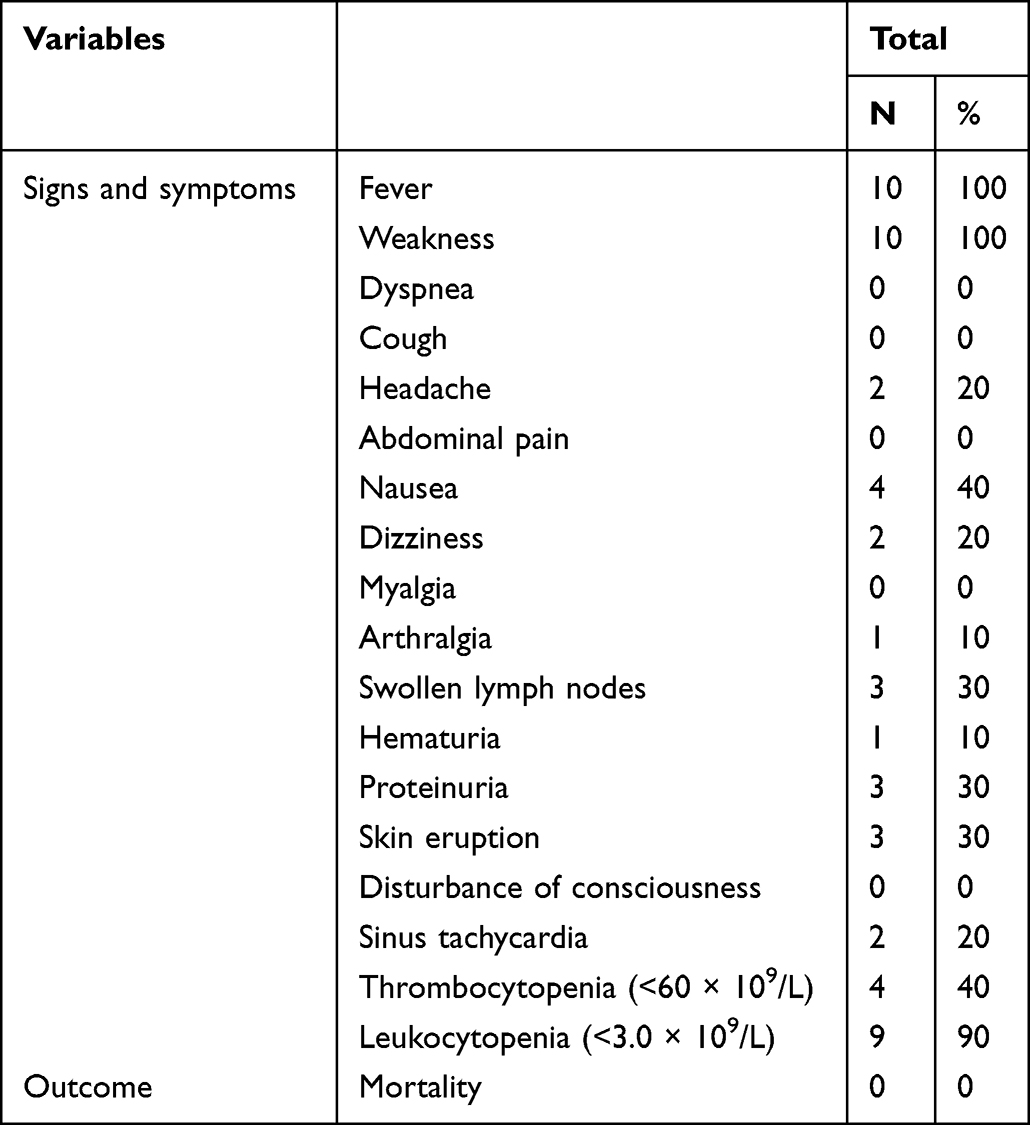 |
Table 3 Clinical and Laboratory Characteristics of the 10 Cases of SFTS in Children from China, from 2011 to 2022 |
In diagnostic assessments, hematological abnormalities at hospital admission into hospital comprised leucopenia (9 cases) and thrombocytopenia (4 cases).
Discussion
Herein, a pediatric case of SFTS in Anhui Province was reported. The patient was effectively processed with a combination of ribavirin, IVIG, and antibiotics, and the clinical manifestation emerged to be less severe compared to an older case.
Ribavirin is an antiviral drug that works against a variety of RNA viruses. It is a nucleoside antimetabolite, a type of drug that prevents viral genetic material from being duplicated.13 Ribavirin has potential activities against Hantaan, flaviviruses, and CCHF.14 Based on the reported literature, it is clear that the evidence for ribavirin’s effectiveness in SFTS patients is conflicting.15 They are not recommended for usage during pregnancy due to their teratogenic and mutagenic properties.16
There are no studies reported that particularly assess the effectiveness of ribavirin in pediatric patients of SFTS. More research is imperative to ascertain the best ribavirin dose, course, and pathway of administration in children suffering from SFTS.
SFTS is a disorder that is capable of affecting any tissue or organ, resulting in a wide range of symptoms. Due to the nonspecific nature of SFTS symptoms, differential diagnoses are complicated to make, and misdiagnoses are common. In areas where SFTS is endemic, must be regarded in the differential diagnosis of pancytopenia, and viral hemorrhagic disease. The differential diagnosis for SFTS encompasses diseases transmitted by the same vector such as Dengue fever, Crimean-Congo hemorrhagic fever (CCHF), typhus, human granulocytic anaplasmosis (HGA), and Lyme disease; however, other zoonoses and non-vector-borne diseases should also be considered, such as Influenza, thrombotic thrombocytopenic purpura (TTP), myelodysplastic syndrome (MDS), and other hematological diseases.17
Pediatric SFTS infection has a milder clinical course than adult SFTS infection and responds well to treatment. This phenomenon led to the hypothesis that children were immune to infection, possibly due to immaturity of the immune system or a lack of other injury risk factors (such as cigarette smoking). In SFTS pediatric case reports, no fatalities have been reported. Because of their proclivity for asymptomatic or mild disease, the incidence of SFTS in children has likely been underestimated.
Tick bites and living in a rural area are two major risk factors for acquiring the virus in children. Without nucleic acid or antibody tests, SFTS is difficult to diagnose. Clinical suspicions on the basis of hematologic abnormalities and symptoms, as well as a background of tick bites or animal contact, are crucial in the diagnosis of SFTS. Tick bites are not always visible, so we need to look into the patient’s animal contact history or outdoor activities.
Currently, there is no effective vaccine for SFTS. Given the disease’s widespread endemicity and high case–fatality rate, an effective anti-SFTS vaccine is needed. This field is expected to progress in the future.
Conclusion
SFTS is not very prevalent among children and with non-specific symptom, and it can be an easy diagnosis to miss. This keeps the attention of health-care providers on the importance of considering this emerging zoonosis as a differential diagnosis in children with fevers of unknown origin. It is necessary to improve regional surveillance of children with acute febrile illnesses, conduct eco-epidemiological studies, and conduct serological research.
Ethical Approval
This study was performed with the approval of the ethics committee of First Affiliated Hospital of Anhui Medical University. All human research was carried out in compliance with the Declaration of Helsinki. Written informed consent was obtained from parent prior to manuscript submission for their personal or clinical details to be published in this study.
Acknowledgments
We thank the anonymous reviewers for constructive comments. We are very grateful to the doctors of department of Infectious Diseases at the First Affiliated Hospital of Anhui Medical University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study had no funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Yu XJ, Liang MF, Zhang SY, et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N Engl J Med. 2011;364(16):1523–1532. doi:10.1056/NEJMoa1010095
2. Park ES, Shimojima M, Nagata N, et al. Severe fever with thrombocytopenia syndrome phlebovirus causes lethal viral hemorrhagic fever in cats. Sci Rep. 2019;9(1):11990. doi:10.1038/s41598-019-48317-8
3. Yamanaka A, Kirino Y, Fujimoto S, et al. Direct transmission of severe fever with thrombocytopenia syndrome virus from domestic cat to veterinary personnel. Emerg Infect Dis. 2020;26(12):2994–2998. doi:10.3201/eid2612.191513
4. Li XK, Lu QB, Chen WW, et al. Arginine deficiency is involved in thrombocytopenia and immunosuppression in severe fever with thrombocytopenia syndrome. Sci Transl Med. 2018;10(459):eaat4162. doi:10.1126/scitranslmed.aat4162
5. Park A, Park SJ, Jung KL, et al. Molecular signatures of inflammatory profile and B-cell function in patients with severe fever with thrombocytopenia syndrome. mBio. 2021;12(1):e02583–e025920. doi:10.1128/mBio.02583-20
6. Ding S, Niu G, Xu X, et al. Age is a critical risk factor for severe fever with thrombocytopenia syndrome. PLoS One. 2014;9(11):e111736. doi:10.1371/journal.pone.0111736
7. Ma T, Sun JM, Chen LF, et al. A pediatric case of severe fever with thrombocytopenia syndrome in Zhejiang Province, China. J Clin Virol. 2015;72:85–87. doi:10.1016/j.jcv.2015.09.006
8. Song TY, Yang EM, Kim CJ, Pediatric A. Case of severe fever with thrombocytopenia syndrome in Korea. J Korean Med Sci. 2017;32(4):704–707. doi:10.3346/jkms.2017.32.4.704
9. Kim JH, Choi YJ, Lee KS, Kim JE, Oh JW, Moon JH. Severe fever with thrombocytopenia syndrome with Q fever coinfection in an 8-year-old girl. Pediatr Infect Dis J. 2021;40(1):e31–e34. doi:10.1097/INF.0000000000002948
10. Wang LY, Cui N, Lu QB, et al. Severe fever with thrombocytopenia syndrome in children: a case report. BMC Infect Dis. 2014;14:366. doi:10.1186/1471-2334-14-366
11. Zhu CH, Xu D, Liu W, Guo D, Ning Q, Chen G. Pediatric huaiyangshan virus infection: a case report with literature review. IDCases. 2017;9:21–24. doi:10.1016/j.idcr.2017.04.017
12. Huang R, Zhou K, Cao L, Liu H, Shan M. Infection caused by tick bites in children: report of three cases and literature review. Chin Gen Pract. 2019;22(32):4011–4014.
13. Mayor J, Engler O, Rothenberger S. Antiviral efficacy of ribavirin and favipiravir against hantaan virus. Microorganisms. 2021;9(6):1306. doi:10.3390/microorganisms9061306
14. Arab-Bafrani Z, Jabbari A, Mostakhdem Hashemi M, Arabzadeh AM, Gilanipour A, Mousavi E. Identification of the crucial parameters regarding the efficacy of ribavirin therapy in Crimean-Congo haemorrhagic fever (CCHF) patients: a systematic review and meta-analysis. J Antimicrob Chemother. 2019;74(12):3432–3439. doi:10.1093/jac/dkz328
15. Liu W, Lu QB, Cui N, et al. Case-fatality ratio and effectiveness of ribavirin therapy among hospitalized patients in China who had severe fever with thrombocytopenia syndrome. Clin Infect Dis. 2013;57(9):1292–1299. doi:10.1093/cid/cit530
16. Sakran R, Frisch A, Elias A, Sliman H, Ammuri H, Kurnik D. Acute and severe ribavirin-associated hyperuricemia and acute kidney injury: an underrecognized adverse effect. Am J Health Syst Pharm. 2021;78(9):794–799. doi:10.1093/ajhp/zxab043
17. Dumic I, Jevtic D, Veselinovic M, et al. Human granulocytic anaplasmosis—a systematic review of published cases. Microorganisms. 2022;10:1433. doi:10.3390/microorganisms10071433
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.