")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Infantile Eosinophilic Pustular Folliculitis in a Child Aged 7 Years: A Case Report
Authors Shi W , Lu Y , Zhou F, He H, Jiang J , Xue X
Received 20 January 2023
Accepted for publication 14 March 2023
Published 22 March 2023 Volume 2023:16 Pages 717—720
DOI https://doi.org/10.2147/CCID.S404316
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Weikang Shi,1,2,* Yuwen Lu,1,* Fangyan Zhou,1 Huiyi He,3 Jicong Jiang,1 Ximao Xue1
1Department of Dermatology, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China; 2Department of Dermatology, Jinhua Maternal & Child Health Care Hospital, Jinhua, People’s Republic of China; 3Department of Dermatology, Ruian People’s Hospital, Wenzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ximao Xue, Email [email protected]
Abstract: Eosinophilic pustular folliculitis (EPF) is a rare, chronic, itchy, aseptic disease. Although most cases of infantile EPF (I-EPF) are detected in infants, we found that a 7-year-old child with I-EPF, who received treatment with oral azithromycin in combination with topical narrow bound Ultra Violet B light (NB-UVB) irradiation, with no recurrence at follow-up. Our experience with the successful treatment of this patient can provide a reference for more pediatric patients.
Keywords: infantile eosinophilic pustular folliculitis, case report, treatment, dermatopathology
Introduction
Eosinophilic pustular folliculitis (EPF) is a rare, chronic, itchy, aseptic disease.1,2 It is characterized by clustered or circumscribed follicular papules and pustules on an erythematous base, with a central pattern of auto-healing and residual hyperpigmentation. Histopathologically, inflammatory cells (mainly eosinophils) infiltrate the dermis and sebaceous glands of hair follicles and are usually associated with the formation of eosinophilic microabscesses.3
Five cases of infantile EPF (I-EPF) were first reported in 1984 in children aged below 1 year.4 However, it does not just occur in infants. We found a rare case of a 7-year-old child with I-EPF. In this case, we report detailed information about this child and provide the treatment plan. Our experience may help the diagnosis and treatment of related diseases in the future.
Case Presentation
A 7-year-old boy visited the dermatology department of our hospital with recurrent papules and pustules on his scalp, partly fused into patches, and associated with intense itching for 10 months. Topical mometasone furoate cream (Eloson, Bayer Pharmaceuticals), 0.1% tacrolimus ointment (Protopic, Astellas Toyama), and oral cetirizine tablets (Zyrtec, UCB Farchim SA) at 10 mg/d showed no significant improvement. The child denied having fever, aggravation of the lesion after exposure to the sun, or a particular family history.
During dermatological physical examination, multiple papules and pustules of 1–3 mm were observed in the background of erythema of the head, and the occipital lesions were merged into plaques (Figure 1A). Bacterial and fungal cultures of the pustules were negative. The total leukocyte and eosinophil counts were 11.05×109 /L and 0.47×109 /L, respectively, and the percentage of eosinophils was 4.3%. In addition, autoimmune antibodies against syphilis and HIV were negative. Histopathological examination of the pustula revealed mild thickening of the epidermis, eosinophilic pustules in the stratum corneum, eosinophilic infiltration around the sebaceous units of hair follicles, and diffuse eosinophilic and neutrophilic infiltration in the dermis (Figure 1C–E)).
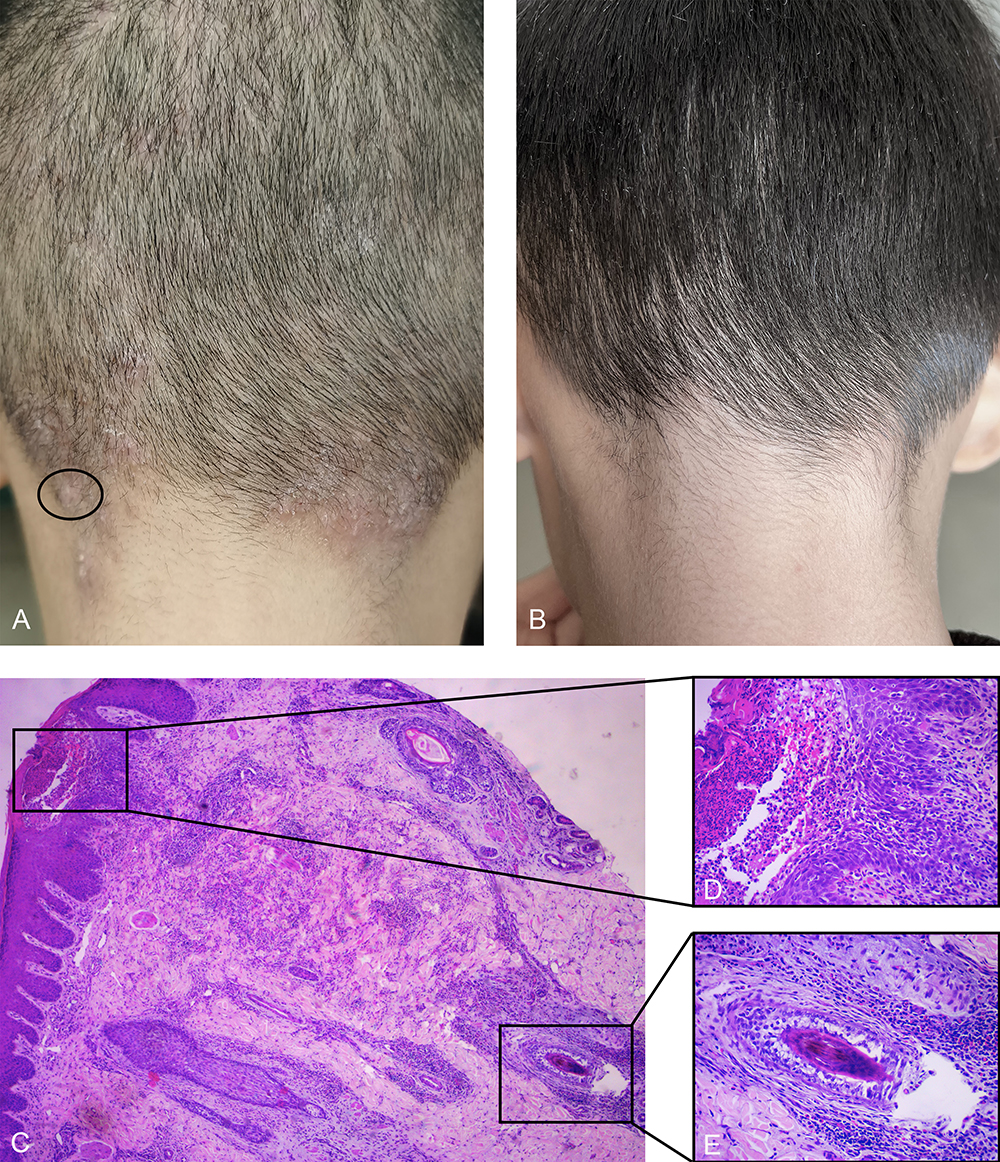 |
Figure 1 (A) At the initial visit, multiple papules, and pustules of 1–3 mm in diameter were detected at the base of the erythema of the head, and the occipital lesions merged into plaques. The black circle was the site of the biopsy. (B) After 3 months of the treatment (during follow-up), no obvious lesion or pigmentation was observed. (C) Mild thickening of the epidermis, eosinophil and neutrophil infiltration around the hair follicle, diffuse eosinophil and neutrophil infiltration in the dermis, and the pustule under the stratum corneum (HE×100). (D) Pustule was found in the stratum corneum (HE×200). (E) Abundant eosinophil infiltration was mentioned around the hair follicle and inside the hair follicle (HE×200). |
Based on the above-mentioned history and examinations, the patient was diagnosed with EPF. Considering the 7-year-old child without response to topical glucocorticoids, we administered oral azithromycin suspension (Zithromax, Pfizer) at 0.2 g/d combined with topical narrow bound Ultra Violet B light (NB-UVB) (ss-09B-10, Shanghai Sigma High-tech) thrice weekly. The initial dose of NB-UVB was 0.2 J/cm2, which was increased by 0.1 J/cm2 for each treatment, with a maximum therapeutic dosage of 1 J/cm2. After 2 weeks of treatment, the lesion began to subside, and the azithromycin suspension was removed. After 4 weeks, the lesions primarily faded, and NB-UVB was administered once weekly. After 2 months, the NB-UVB treatment was stopped. Slight hyperpigmentation occurred during treatment but recovered during follow-up. No recurrence was observed during follow-up (Figure 1B).
Discussion
EPF is a rare, chronic, itchy, and aseptic disease, which was first reported by Ofuji.1,2 According to Nervi et al,5 EPF can be divided into three major types: classical EPF, immunosuppression-associated EPF, and I-EPF. I-EPF shows aseptic papules, similar to classical EPF, but is not characterized by a circular arrangement. It develops primarily on the scalp and occasionally spreads to the face and extremities.6 Although the clinical presentation is different, there are identical pathological features between I-EPF and classical EPF.7
However, I-EPF does not only occur in infants. Nomura et al6 reported 63 patients with I-EPF, aged from a few hours to 9 years (median/mean 0.5/1.3 years), and discovered that most of them occurred within 2 years of age. Furthermore, Hernández-Martín et al8 reviewed 15 patients with I-EPF and found that approximately 70% had onset before 6 months, whereas 5% had their first onset after 14 months. Although our patient was a 7-year-old child, we diagnosed him with I-EPF via clinical presentation, laboratory tests, and histopathological characteristics. However, I-EPF usually lacks specificity and can be similar to certain common diseases, such as acne, fungal infections, and eczema.9 Thus, the pathological examination can be the final method for confirming the diagnosis.7
There are no unified treatments for EPF; however, abundant evidence suggests that the key is the normalization of Th2 immune dysregulation.7 Although indomethacin is the choice of treatment for classical EPF with 84% effectiveness, Nomura et al6 found that indomethacin or other NSAIDs should be avoided in I-EPF. The primary treatments for I-EPF include topical corticosteroids and systemic erythromycin. Second-line treatments include systemic antibiotics and topical 0.03% tacrolimus cream.10 Additionally, UVB is considered the treatment for EPF with minimal side effects. It successfully treated HIV-associated refractory EPF in 1993 and 1998, and no treatment failures were reported in subsequent treatments.11 Apparently, NB-UVB has a higher safety profile and better efficiency than UVB.12 Therefore, we opted for oral azithromycin combined with topical NB-UVB irradiation, and the children responded well without recurrence.
Conclusion
As a rare disease, the diagnosis of EPF should be combined with medical history, laboratory tests, and histopathology. In particular, caution should be exercised when safely diagnosing and administering I-EPF. Our experience with the successful treatment of this patient can provide a reference for pediatric patients for whom topical glucocorticoids are ineffective.
Abbreviations
EPF, eosinophilic pustular folliculitis; I-EPF, infantile eosinophilic pustular folliculitis; NB-UVB, Narrow Bound Ultra Violet B Light.
Ethical Statement
This study was approved by the ethics committee of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, and informed consent was obtained from the guardians of the child in order to publish this case report.
Acknowledgments
We sincerely thank this patient and his parents for providing the permission to share his information.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ise S, Ofuji S. Subcorneal pustular dermatosis; a follicular variant? Arch Dermatol. 1965;92:169–171. doi:10.1001/archderm.92.2.169
2. Ofuji S, Ogino A, Horio T, Oseko T, Uehara M. Eosinophilic pustular folliculitis. Acta Derm Venereol. 1970;50(3):195–203.
3. Sufyan W, Tan K, Wong S, Lee Y. Eosinophilic pustular folliculitis. Arch Pathol Lab Med. 2007;131(10):1598–1601. doi:10.5858/2007-131-1598-epf
4. Lucky A, Esterly N, Heskel N, Krafchik B, Solomon L. Eosinophilic pustular folliculitis in infancy. Pediatr Dermatol. 1984;1(3):202–206. doi:10.1111/j.1525-1470.1984.tb01116.x
5. Nervi S, Schwartz R, Dmochowski M. Eosinophilic pustular folliculitis: a 40 year retrospect. J Am Acad Dermatol. 2006;55(2):285–289. doi:10.1016/j.jaad.2006.02.034
6. Nomura T, Katoh M, Yamamoto Y, Kabashima K, Miyachi Y. Eosinophilic pustular folliculitis: the transition in sex differences and interracial characteristics between 1965 and 2013. J Dermatol. 2015;42(4):343–352. doi:10.1111/1346-8138.12783
7. Nomura T, Katoh M, Yamamoto Y, Miyachi Y, Kabashima K. Eosinophilic pustular folliculitis: a proposal of diagnostic and therapeutic algorithms. J Dermatol. 2016;43(11):1301–1306. doi:10.1111/1346-8138.13359
8. Hernández-Martín Á, Nuño-González A, Colmenero I, Torrelo A. Eosinophilic pustular folliculitis of infancy: a series of 15 cases and review of the literature. J Am Acad Dermatol. 2013;68(1):150–155. doi:10.1016/j.jaad.2012.05.025
9. Fujiyama T, Tokura Y. Clinical and histopathological differential diagnosis of eosinophilic pustular folliculitis. J Dermatol. 2013;40(6):419–423. doi:10.1111/1346-8138.12125
10. Nomura T, Katoh M, Yamamoto Y, Miyachi Y, Kabashima K. Eosinophilic pustular folliculitis: a published work-based comprehensive analysis of therapeutic responsiveness. J Dermatol. 2016;43(8):919–927. doi:10.1111/1346-8138.13287
11. Ellis E, Scheinfeld N. Eosinophilic pustular folliculitis: a comprehensive review of treatment options. Am J Clin Dermatol. 2004;5(3):189–197. doi:10.2165/00128071-200405030-00007
12. Kuwano Y, Watanabe R, Fujimoto M, et al. Treatment of HIV-associated eosinophilic pustular folliculitis with narrow-band UVB. Int J Dermatol. 2006;45(10):1265–1267. doi:10.1111/j.1365-4632.2006.03072.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.