")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Individualized Surgical Management of Refractory Port-Wine Stains in the Scalp and Face: A Single-Center Retrospective Study and a Discussion of Surgical Strategies
Authors Wang Q, Yong C, Wang M, Cui L, Yuan SM
Received 12 April 2022
Accepted for publication 22 July 2022
Published 3 August 2022 Volume 2022:15 Pages 1527—1535
DOI https://doi.org/10.2147/CCID.S370491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Qian Wang,1 Chen Yong,1 Min Wang,1 Lei Cui,1 Si-Ming Yuan1,2
1Department of Plastic Surgery, Jinling Hospital, Medical School of Nanjing University, Nanjing, 210002, People’s Republic of China; 2Department of Plastic Surgery, Jinling Hospital, Nanjing School of Clinical Medicine, Southern Medical University, Nanjing, 210002, People’s Republic of China
Correspondence: Si-Ming Yuan, Department of Plastic Surgery, Jinling Hospital, Medical School of Nanjing University, Nanjing, 210002, People’s Republic of China, Email [email protected]
Objective: Refractory port-wine stain (PWS) usually contains hypertrophic, nodular lesions or severe scars due to improper treatment, making surgical treatment a necessity. This study aims to introduce our experiences in surgical management of refractory PWSs in the scalp and face.
Methods: From January of 2013 to September of 2018, 25 patients with refractory PWSs in the scalp and face received surgeries in our department. Clinical manifestation of the disease, the surgical procedures and postoperative complications were reviewed. A Visual Analog Scale (VAS) was applied to evaluate the outcomes.
Results: In this study, surgical procedures included serial resection (4 cases), complete resection followed by local flap transplantation (6 cases) or skin grafting (7 cases), and two-staged surgeries using expanded flaps (5 cases) or expanded prefabricated flap (3 cases). All the skin grafts and flaps survived well. Follow-up evaluation with VAS showed that most patients were satisfied with the surgery.
Conclusion: The surgical procedures should depend on the site, area and type of the lesions and patients’ personal requirement. Individualized surgical treatment of refractory PWSs achieved satisfactory results in re-establishing symmetric facial contour and improving the overall appearance.
Keywords: port-wine stain, surgery strategy, scalp and face
Introduction
Port-wine stain (PWS) is a common type of capillary malformation, which has an incidence of 0.3–0.5% in neonates with equal sex distribution.1 Although PWS can be found anywhere in the body, it most frequently occurs in the head and neck. By the age of forties, about two-thirds of the patients will develop darker, hypertrophic, or nodular lesions2 which may significantly influence patients’ appearance and health and increase the difficulty of treatment.
Conventional therapies, including sclerotherapy, cryotherapy, and radiotherapy, have been abandoned due to high incidence of serious complications. Laser therapy, such as pulsed dye laser (PDL) and photodynamic therapy (PDT), is now regarded as the mainstream treatment for PWS. It is reported that PDT can be as effective as 585-nm PDL in treating pink flat lesions in children.3 However, the proportion of complete remission is still less than 20% in PDL therapy.4–6 In addition, 20–30% of PWS lesions are not sensitive or responsive to PDL treatment.7 Although PDT represents a promising alternative to PWS, its limited cure rate (around 30%) and relatively higher incidence of complications such as skin ulceration and scar formation have restricted its wider application.8–10
For refractory PWSs that are ineffective to common therapies and accompanied with severe scars and/or pigmentation due to inappropriate treatment, surgeries are usually the ultimate choice. This study introduced our experiences in the surgical treatment of refractory PWSs in the scalp and face to summarize the common operative techniques and propose individualized surgical strategies.
Methods
General Data
The study was approved by the Ethics Committee of Jinling Hospital (registration number: 2013NZKY-011-01) and the study complies with the Declaration of Helsinki. Informed consent for the treatment and the publication of images was obtained from all the patients, and the diagnosis of PWS was made based on the medical history, clinical manifestation, and physical examination.
Operation Methods
The choice of operation methods was dependent on the site, area, type of the lesions as well as patients’ personal requirement. For lesions in the scalp, skin grafting was the most frequently used procedure. When the lesions were in the face, for small lesions (less than 10% of the face) in covert areas, such as naso-labial groove, serial resection was the first choice. The width of each resection was decided by the tension of surrounding soft tissues. While for small lesions in conspicuous areas, local flaps were applied to achieve better appearance. For extensive lesions involving almost or over half of the face, medium-thickness or full-thickness skin grafts were used to repair the wound regardless of the site of the lesion. For medium size lesions (10%~50% of the face) in areas with high mobility, both local flaps and tissue expansion can be chosen. For medium size lesions that are adjacent to critical facial structures like nose, eyes and lips, tissue expansion was preferred. For medium size lesions in midfacial area (ie, nose, medial cheek, and upper lip), especially in patients with high cosmetic requirement, the expanded prefabricated flap was preferred.
The goal of surgical treatment is to remove pathological tissues to the greatest extent to restore symmetrical facial contour. The shape and function of important organs should be maintained to the maximum extent to achieve the best aesthetic appearance. Preoperative design was established according to the size of the lesions and involvement with the vital organs. Intraoperative injection of tumescent fluid can reduce bleeding and increase the safety of operation. The surgical incision should be made inside the hairline or skin wrinkles. Major vessels, branches of facial nerve, and muscles of expression should be protected with extreme caution. Surgeons are supposed to follow the principles of plastic and aesthetic surgery and use tension-reduced sutures to achieve better cosmetic results.
Follow-Up Assessment
Clinical manifestation, operation procedures, and immediate and late postoperative complications were recorded. Anti-scar therapies were routinely applied for all the patients postoperatively. Patients were followed up every 3 months and the follow-up lasted for 6 months to 24 months with an average time of 8.6 months. Representative photographs were used for cosmetic evaluation. Patients’ satisfaction was evaluated by comparing preoperative and the latest follow-up photographs using modified Visual Analog Scale (VAS) (Table 1). Make-up was allowed when photos were taken.
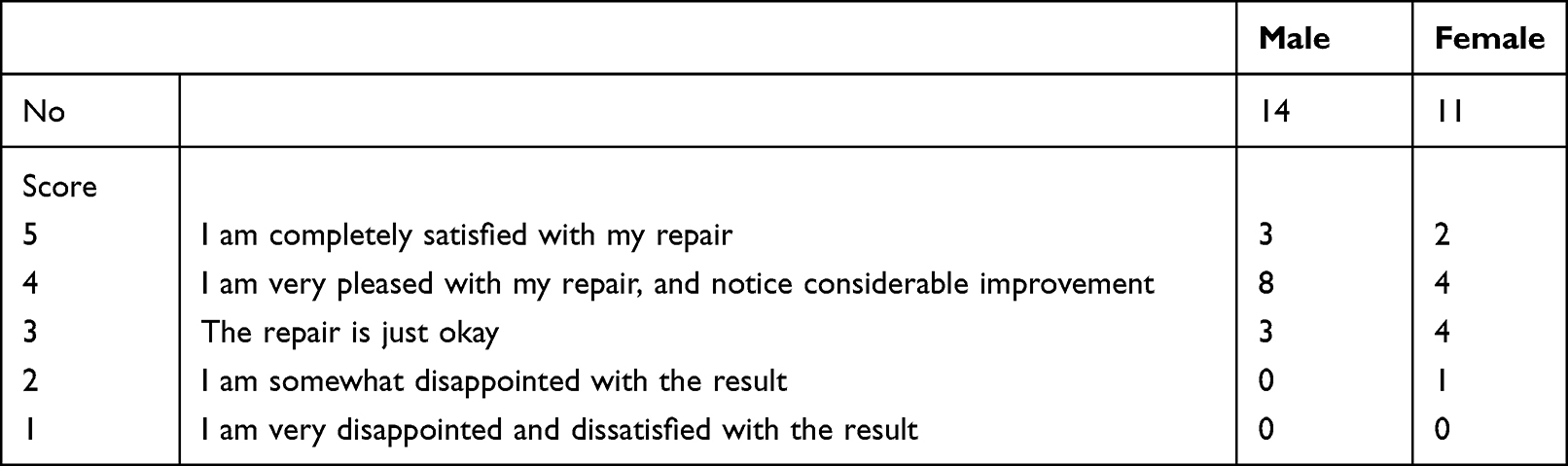 |
Table 1 Evaluation of Cosmetic Results by Modified Visual Analog Scale |
Results
From January of 2013 to September of 2018, 25 patients with refractory PWSs in the scalp and face received surgeries. Eleven of them were male patients and 14 were female. The initial treatment age ranged from 18 to 58 years. Lesion area ranged from 2.5cm2 to 260cm2, some of which might significantly affected the appearance and caused vision and speech dysfunction. The lesions were distributed in the scalp (4 cases), frontal and temporal skin (6 cases), cheeks (7 cases), lips (6 cases), or multiple regions (2 cases). All patients underwent non-surgical treatment before surgery, including pulsed dye laser treatment (15 cases), photodynamic therapy (6 cases), and superficial radiotherapy (4 cases). Previous treatments did not achieve satisfactory therapeutic effects or even resulted in severe complications such as scar hypertrophy and pigmentation. The details can be seen in Table 2. In this study, surgical procedures included serial resection (4 cases), complete resection followed by local flap transplantation (6 cases) or skin grafting (7 cases), and two-staged surgery applying expanded flaps (5 cases) or expanded prefabricated flap (3 cases).
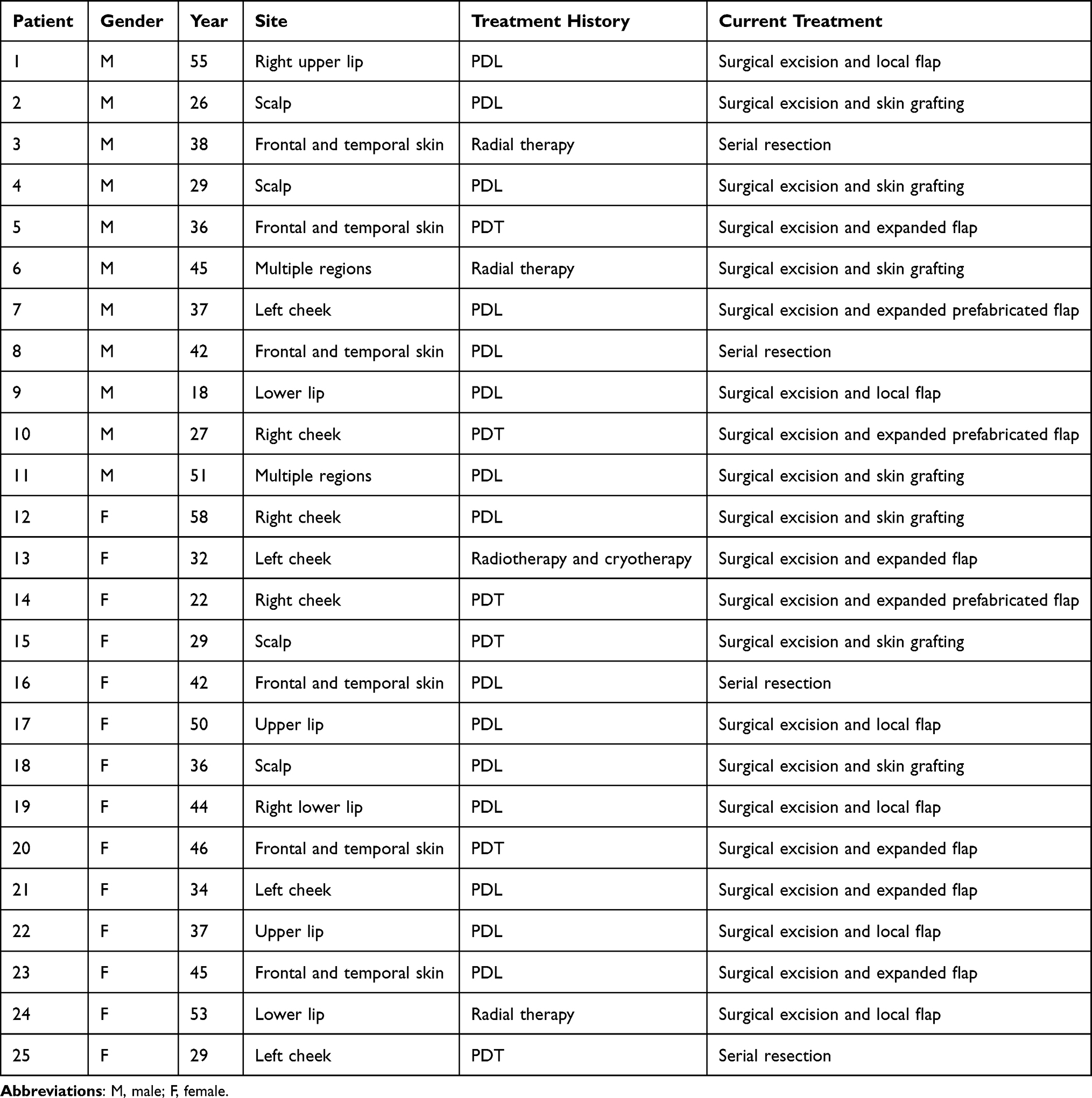 |
Table 2 An Overview of the Cases Included in the Study |
All the patients recovered well after the operations. All skin grafts and flaps survived well. There were no serious complications such as wound dehiscence or hematoma. For patients treated with tissue expanders, no infection, tissue expander exposure or rupture was observed. Partial necrosis at the edge of the skin grafts occurred in three cases, but the wound eventually healed with comprehensive wound management. Flap necrosis did not occur in any case. One case received another surgery to treat scar hypertrophy. Another case underwent skin grafting to treat lower eyelid ectropion caused by scar contracture.
At the end of follow-up, 68% (17 cases) of the patients were satisfied or very satisfied (sores of 4 and 5) with their aesthetic appearance, only one of the female patients was disappointed with cosmetic results (Table 1). Some female patients scored higher after wearing makeup.
Figures 1–4 present three typical cases.
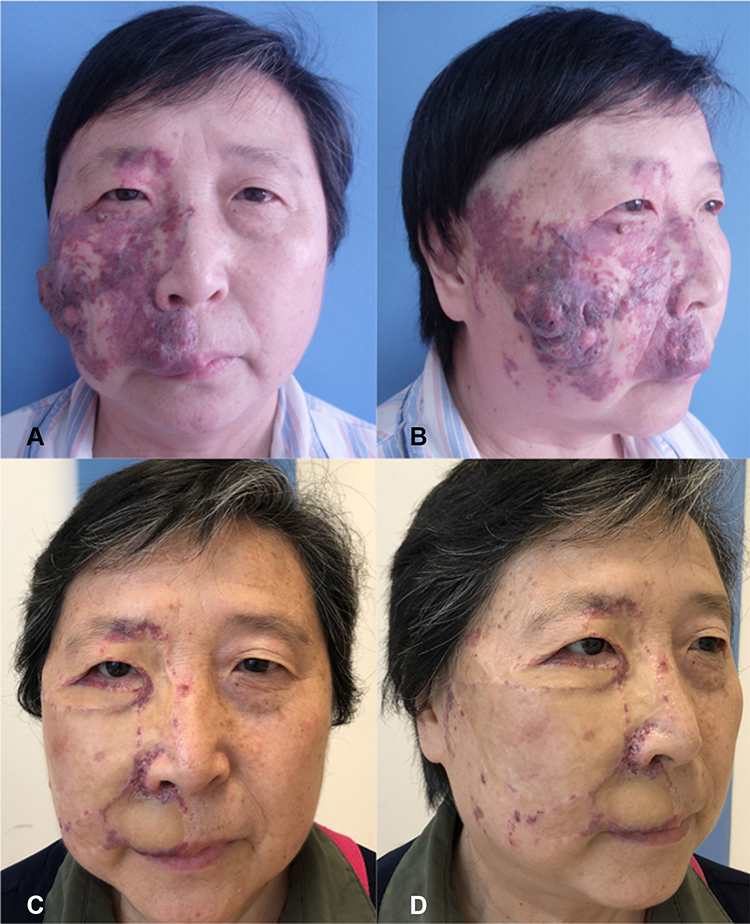 |
Figure 1 Case 1. A 58-year-old female had large area of hypertrophic and nodular PWS in the right face which was resistant to PDL therapy. The majority of the lesions was removed, and medium-thickness skin grafting was used to repair the wound in the first-stage operation. The skin grafts survived well. Eight months later, secondary procedure was performed to relieve lower eyelid ectropion caused by scar contracture. (A and B) Preoperative views. (C and D) Postoperative views three years later. Evaluation result was “very satisfied (score of 5)”. |
 |
Figure 2 Case 2. A 55-year-old male had hypertrophic PWS in the right upper lip which was accompanied by ulceration and infection. The lesions were completely removed, and an abbé flap was used to repair the wound in the first-stage operation. The flap survived well. Two weeks later, secondary procedure was performed to divide the pedicle. (A) The preoperative view. (B) The intraoperative view. (C) One week after the first-stage operation. (D) The flap survived well and was ready to undergo the pedicle division surgery. (E) The flap pedicle was successfully divided. (F–G) Postoperative views three months later. Evaluation result was “very satisfied (score of 5)”. |
 |
Figure 3 Case 3. A 32-year-old female had PWS with obvious scars and pigment anomalies in the left face after superficial radiotherapy and cryotherapy. The tissue expander (rated capacity:100mL) was placed adjacent to the lesion in left cheek in the first-stage surgery. Regular expansion lasted for 93 days with a final capacity of 252mL. The lesion was removed and repaired by the expanded flap in the second-stage operation. The flap survived well. (A and B) Preoperative views. (C and D) Postoperative views one year later. Evaluation result was “very satisfied (score of 5)”. |
 |
Figure 4 Case 4. A 22-year-old female had PWS with obvious scars and pigment anomalies in the right face after photodynamic therapy. Expanded prefabricated flap was used. The right temporoparietal fascial flap was harvested in the first-stage operation and placed under the pre-separated flap in the neck. Rated capacity of the expander was 200 mL. Regular expansion lasted for 114 days with final capacity of 392mL. The expanded prefabricated flap was transferred to the wound through subcutaneous tunnel after the removal of lesion in the second-stage operation. The flap survived well. (A) Preoperative lateral view. (B) Preoperative marking of the frontal and parietal branches of the superficial temporal vessels and operation design. (C) Lateral view before the second-stage operation. (D) Postoperative view with make-up two years later. Evaluation result was “very pleased (score of 4)”. |
Discussion
Port-wine stain (PWS) is a congenital vascular malformation composed of dilated vessels located within the superficial dermal vascular plexus. It frequently occurs in head and neck of infants, especially in areas innervated by the trigeminal nerve, presenting as a pink to red flat macula initially, with no obvious gender difference in the incidence.11,12 The etiology of PWS remains unknown, possibly associated with factors such as abnormal neurovascular distribution and gene mutations including GNAQ, RASA1, and EPHB4 mutations.13–16 Head and neck lesions tend to be darker and undergo hypertrophy or nodule formation over time.17 In a few cases, the lesions can be extremely worsened with grape-like or tumor-like appearance.
Refractory PWSs were characterized by hypertrophic and/or nodular lesions which were often accompanied by severe scar and/or pigmentation and were not responsive to conventional treatment. They are often located in the face and scalp, requiring delicate excision and repair. For individuals diagnosed as refractory PWSs, the appearance can only be effectively improved by surgical management.
Local flaps can be an alternative to wound repair if the incision cannot be sutured directly. If local flaps are not suitable for larger lesions or the patient is reluctant to take the risk of flap necrosis but willing to withstand a longer treatment period, serial resection can be used. For lesions adjacent to crucial facial structures like eyebrows, eyelids, nose, etc., local deformation may occur in the early stage after resection, but often can gradually recover over time. If the risk of obvious deformation after surgery is estimated to be very high, other surgical methods should be considered.
Skin grafting is suitable for patients with extensive or irregular lesions, which involve multiple facial structures like eyebrows, eyelids, lips, and nose. Skin grafting in face requires higher survival rate, lower contractility and less pigmentation, where full-thickness skin grafts are often used to achieve the best cosmetic results. However, hyperpigmentation and scar proliferation in recipient sites is usually inevitable. Therefore, for patients with extensive lesions but lower cosmetic expectations and some elderly patients, this relatively simple, economic and safe surgical procedure is recommended.
Patients with medium size lesions can achieve satisfactory results by tissue expansion. The tissue expander is generally placed below the subcutaneous layer in the cheeks, forehead, cervico-mandibular, or scalp. Tissue expanders should be placed where the appearance and function of important organs can be maintained to the maximum extent. For large lesions that cannot be repaired by single expansion, repeated expansion should be considered. Although tissue expansion compensates for some of the shortcomings of skin grafting, it still has some limitations including longer treatment course, higher requirement for patients’ cooperation, and higher postoperative nursing demands. Therefore, tissue expansion should be considered first only for younger patients with moderate lesions and higher cosmetic requirement.
If the lesions were in midfacial area (nose, medial cheek, and upper lip), it is difficult to provide a flap with reliable blood supply by conventional tissue expansion. Some surgeons use multiple expanded flaps in a single surgery to repair the wound, but the connecting area of different flaps will result in poor appearance. Fortunately, research and clinical practice have shown that expanded prefabricated flaps with superficial temporal vessels transferred to the neck is a feasible method.18 The preoperative marking of the frontal and parietal branch of the superficial temporal vessels should be performed carefully. When the superficial temporal vascular bundle is isolated during operation, the vessel trunk should be cautiously protected to ensure that the arterial blood supply and venous return of the flap are not impaired. The fascial flap was fixed beneath the skin flap in the neck. In this group of patients, no flap necrosis or venous return blockage after operation was observed. The expanded prefabricated flap achieved better cosmetic results. The expansion and prefabrication of a super-thin skin perforator flap can possibly provide a super-thin skin flap that can be used for reconstruction of larger defects, achieving better cosmetic results than traditional prefabricated flaps.19
Overall, the etiology of PWS has not been fully understood and the treatment of PWS is still developing. It has been reported that site-specific pharmaco-laser therapy, which combines conventional laser therapy with the administration of thermosensitive drug delivery system may enhance PWS blanching.20 Also, some research showed that rapamycin can improve the outcomes of PWS as adjunctive therapy.21 These novel therapies can be considered as alternative options.
There are also some limitations of the study. The follow-up time is relatively short. Long-term outcomes needed to be added to evaluate the therapeutic effects in future studies. Also, the details of previous treatment in other hospitals were not accessible and were not included in the study. In addition, only surgeries were applied in these patients. Combined therapies of both surgeries and consequent laser therapies for residual lesions may improve the outcome and should be further studied.
Conclusion
In conclusion, for refractory PWSs in the scalp and face, surgeons should choose appropriate surgery methods according to the site, area, type of the lesion and patients’ preference, among which the area and site being the most critical factor. For small lesions, simple resection, serial resection and local flaps are often applied; for medium size lesions, expanded flaps or expanded prefabricated flaps are better choices; while for extensive lesions involving multiple facial structures, skin grafting is an easy and effective method.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81272989, awarded to Dr. Si-Ming Yuan), “333 Project” of Jiangsu Province, China (No. BRA2020416, awarded to Dr. Si-Ming Yuan), and the Foundation for Key Medical Specialty of Nanjing (SZDZK202001, awarded to Dr. Si-Ming Yuan).
Disclosure
None of the authors declared conflicts of interest.
References
1. Updyke KM, Khachemoune A. Port-wine stains: a focused review on their management. J Drugs Dermatol. 2017;16(11):1145–1151.
2. Galligan ER, Baselga E, Frieden IJ, et al. Characterization of vascular stains associated with high flow. J Am Acad Dermatol. 2021;84(3):654–660. doi:10.1016/j.jaad.2020.06.985
3. Yuan KH, Li Q, Yu WL, et al. Comparison of photodynamic therapy and pulsed dye laser in patients with port wine stain birthmarks: a retrospective analysis. Photodiagnosis Photodyn Ther. 2008;5:50–57. doi:10.1016/j.pdpdt.2007.12.001
4. Han Y, Ying H, Zhang X, et al. Retrospective study of photodynamic therapy for pulsed dye laser-resistant port-wine stains. J Dermatol. 2020;47(4):348–355. doi:10.1111/1346-8138.15238
5. Wang T, Chen D, Yang J, et al. Safety and efficacy of dual-wavelength laser (1064 + 595 nm) for treatment of non-treated port-wine stains. J Eur Acad Dermatol Venereol. 2018;32(2):260–264. doi:10.1111/jdv.14490
6. Li DC, Nong X, Hu ZY, et al. Efficacy and related factors analysis in HMME-PDT in the treatment of port wine stains. Photodiagnosis Photodyn Ther. 2020;29:101649. doi:10.1016/j.pdpdt.2020.101649
7. Mathes EF, Frieden IJ. Early use of laser for port-wine stains: timing, efficacy, and shared decision making. JAMA Dermatol. 2019;155(4):421–423. doi:10.1001/jamadermatol.2018.5189
8. Khalaf AT, Sun Y, Wang F, et al. Photodynamic therapy using HMME for port-wine stains: clinical effectiveness and sonographic appearance. Biomed Res Int. 2020;2020:6030581. doi:10.1155/2020/6030581
9. Gao K, Huang Z, Yuan KH, et al. Side-by-side comparison of photodynamic therapy and pulsed-dye laser treatment of port-wine stain birthmarks. Br J Dermatol. 2013;168(5):1040–1046. doi:10.1111/bjd.12130
10. Zhang Y, Zou X, Chen H, et al. Clinical study on clinical operation and post-treatment reactions of HMME-PDT in treatment of PWS. Photodiagn PhotodynTher. 2017;20:253–256. doi:10.1016/j.pdpdt.2017.09.013
11. van Drooge AM, Beek JF, van der Veen JP, et al. Hypertrophy in port-wine stains: prevalence and patient characteristics in a large patient cohort. J Am Acad Dermatol. 2012;67(6):1214–1219. doi:10.1016/j.jaad.2012.05.027
12. Lee JW, Chung HY, Cerrati EW, et al. The natural history of soft tissue hypertrophy, bony hypertrophy, and nodule formation in patients with untreated head and neck capillary malformations. Dermatol Surg. 2015;41(11):1241–1245. doi:10.1097/DSS.0000000000000525
13. Nguyen V, Hochman M, Mihm MC, et al. The pathogenesis of port wine stain and Sturge weber syndrome: complex interactions between genetic alterations and aberrant MAPK and PI3K activation. Int J Mol Sci. 2019;20(9):2243. doi:10.3390/ijms20092243
14. Ma G, Yu Z, Liu F, et al. Somatic GNAQ mutation in different structures of port-wine macrocheilia. Br J Dermatol. 2018;179(5):1109–1114. doi:10.1111/bjd.16830
15. Cai R, Liu FT, Hua C, et al. A novel RASA1 mutation causing capillary malformation-arteriovenous malformation (CM-AVM): the first genetic clinical report in East Asia. Hereditas. 2018;155:24. doi:10.1186/s41065-018-0062-8
16. Yu JD, Streicher JL, Medne L, et al. EPHB4 mutation implicated in capillary malformation-arteriovenous malformation syndrome: a case report. Pediatr Dermatol. 2017;34(5):e227–230. doi:10.1111/pde.13208
17. Lee JW, Chung HY. Capillary malformations (port wine stains) of the head and neck: natural History, investigations, laser, and surgical management. Otolaryngol Clin North Am. 2018;51(1):197–211. doi:10.1016/j.otc.2017.09.004
18. Pribaz JJ, Fine N, Orgill DP. Flap prefabrication in the head and neck: a 10-year experience. Plast Reconstr Surg. 1999;103(3):808–820. doi:10.1097/00006534-199903000-00006
19. Wang C, Zhang J, Yang S, et al. The clinical application of pre-expanded and prefabricated super-thin skin perforator flap for reconstruction of post-burn neck contracture. Ann Plast Surg. 2016;77(Suppl 1):S49–52. doi:10.1097/SAP.0000000000000711
20. van Raath MI, van Amesfoort JE, Hermann M, et al. Site-specific pharmaco-laser therapy: a novel treatment modality for refractory port wine stains. J Clin Transl Res. 2019;5(1):1–24.
21. Greveling K, Prens EP, van Doorn MB. Treatment of port wine stains using pulsed dye laser, erbium YAG laser, and topical rapamycin (sirolimus)-A randomized controlled trial. Lasers Surg Med. 2017;49(1):104–109. doi:10.1002/lsm.22548
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.