")
Back to Journals » Clinical Epidemiology » Volume 12
Individual Antidepressants and the Risk of Fractures in Older Adults: A New User Active Comparator Study
Authors Pisa FE, Reinold J , Kollhorst B , Haug U, Schink T
Received 11 July 2019
Accepted for publication 1 April 2020
Published 22 June 2020 Volume 2020:12 Pages 667—678
DOI https://doi.org/10.2147/CLEP.S222888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Vera Ehrenstein
Federica Edith Pisa,1 Jonas Reinold,1 Bianca Kollhorst,2 Ulrike Haug,1,3 Tania Schink1
1Department of Clinical Epidemiology, Leibniz Institute for Prevention Research and Epidemiology – BIPS, Bremen, Germany; 2Department of Biometry and Data Management, Leibniz Institute for Prevention Researchand Epidemiology – BIPS, Bremen, Germany; 3Faculty of Human and Health Sciences, University of Bremen, Bremen, Germany
Correspondence: Tania Schink
Department of Clinical Epidemiology Leibniz Institute for Prevention Research and Epidemiology – BIPS, Achterstrasse 30, Bremen 28359, Germany
Tel +49/421/218-56869
Fax +49/421/218-56821
Email [email protected]
Objective: To determine the risk of hip–pelvis and other non-vertebral fractures in older adults using antidepressants (ADs).
Methods: We conducted a case–control study nested in a cohort of new users of ADs aged ≥ 65 years without prior hip–pelvis or other non-vertebral fractures, identified in the German Pharmacoepidemiological Research Database (GePaRD) during 2005– 2014. Cases were patients first hospitalized for hip–pelvis or other non-vertebral fractures. Up to 100 controls per case were selected using incidence density sampling. AD use was ascertained at index date (ID) based on the supply of last dispensing. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were estimated using conditional logistic regression with current users of mirtazapine as reference (active comparator).
Results: A total of 39,853 cases of hip–pelvis fracture (80% women, median age 81 years) and 31,577 cases of other fractures (84% women, median age 79 years) were matched to > 3 million controls. For hip–pelvis fracture, aORs in current users were about 1.3 with little variation between individual ADs, ranging from 1.33 for citalopram (95% CI 1.27– 1.39) to 1.28 for amitriptyline (1.21– 1.35). For other fractures, the aORs were highest in current users of citalopram (1.50; 1.42– 1.58) and duloxetine (1.54; 1.39– 1.71) and lowest for amitriptyline (1.18; 1.11– 1.26) and trimipramine (1.16; 1.03– 1.29). For all examined ADs, the aORs were higher for other fractures than for hip–pelvis fracture.
Conclusion: The risk of fractures varies between ADs, but for most agents is higher than the risk for mirtazapine. When treating older adults with ADs, prescribers should carefully consider the risk profile of individual ADs regarding fractures, which are a major health problem in this population.
Keywords: antidepressants, fractures, hip fracture, pelvis fracture, older adults, health-care databases, pharmacoepidemiology
Introduction
Antidepressants (ADs) are frequently used in older adults, for example, to treat late-life depression, anxiety disturbance, sleep problems or neuropathic pain.1 The prevalence of AD use in older adults ranges from 15% to up to 30% in different populations.2–6 However, ADs have been consistently associated with an increased risk of fractures in older adults,7–13 in particular with fractures of the hip.13–19 Since fractures are a major health issue in older adults, leading to reduced autonomy and increased short-term mortality, possibilities to reduce the risk of fractures need to be explored. This includes a careful characterization of the safety profile of individual ADs regarding fractures.
However, prior studies mainly focused on differences in risk between AD classes rather than between individual ADs. Meta-analyses of observational studies showed a higher risk for selective serotonin reuptake inhibitors (SSRIs) than for tricyclic antidepressants (TCAs).20–24 For example, the summary risk of hip fracture was increased by 60% to 100% in users of SSRI,22–24 while it was increased by 40% to 70% in users of TCAs;23,24 the risk of any fracture was increased by 70%20,22 for SSRIs and by 40%21,24 for TCAs. These risk patterns were again confirmed by a more recent multi-database study.17
Only two cohort studies have compared the risk of fracture between individual ADs and showed differences in risk within the AD classes. In a French cohort7 of persons aged 65 years or older, the risk of fractures associated with SSRIs was increased twofold for fluoxetine, by 50% for citalopram and by 30% for sertraline and paroxetine. In another cohort of older adults with depression based on a UK primary care database,8 the risk was increased by 80% for venlafaxine, between 70% and 60% for citalopram, fluoxetine, and sertraline, by about 50% for mirtazapine and paroxetine, and by 30% for amitriptyline and escitalopram. However, these studies compared the risk in persons currently using AD with that of persons not currently treated. Moreover, the first study7 evaluated four SSRIs and the second one8 did not evaluate frequently used ADs such as duloxetine.
Improved knowledge of the fracture risk associated with individual ADs is important for clinicians to adequately balance risks and benefits in the decisions of prescribing ADs to older adults and of monitoring treated patients. It ultimately will help to reduce the risk of fractures in this vulnerable population.
We aimed to add knowledge on the risk of individual ADs regarding the risk of hip–pelvis and other non-vertebral fractures in older adults by conducting an active comparator case–control study nested in a cohort of new users of ADs aged ≥65 years without prior hip–pelvis or other non-vertebral fractures.
Methods
Data Source
This study was conducted using the German Pharmacoepidemiological Research Database (GePaRD). GePaRD is based on claims data from four statutory health insurance providers in Germany and currently includes information on about 25 million persons who have been insured with one of the participating providers since 2004 or later. In addition to demographic data, GePaRD contains information on drug dispensations (including Anatomical and Therapeutic Code – ATC, defined daily dose – DDD, strength, packaging size, generic and brand name), outpatient and inpatient services and diagnoses. Per data year, there is information on approximately 17% of the general population and all geographical regions of Germany are represented. In- and outpatient diagnoses are coded according to the International Classification of Diseases, 10th revision, German Modification (ICD-10-GM). GePaRD data are representative of the German general population with respect to age, sex, region of residence and medication dispensations.25,26
The suitability of GePaRD data for pharmacoepidemiological research has been assessed methodologically and by validation studies.25,27,28 GePaRD has been used for various types of pharmacoepidemiological studies including drug utilization studies in the elderly29,30 and studies investigating the risks of antidepressants.27,31-33
Study Design
We conducted a case–control study nested in a cohort of persons aged ≥65 years who initiated the use of an AD (new users) between January 1, 2005 and December 31, 2014 (study period). We applied an active comparator new user design,34 comparing the risk of persons initiating a certain AD to the risk of persons initiating mirtazapine (active comparator) which is frequently used and has been associated with a low risk of hip fractures.35
To be eligible, persons had to be older than 65 years and have at least 12 months of continuous enrollment before cohort entry. Patients entered the cohort at the date of the first AD dispensation after 365 days without such a dispensation (“initiation”). We defined two not mutually exclusive cohorts, one for the outcome hip–pelvis fracture and one for other non-vertebral fractures (the same person could be in both cohorts if he/she experienced both types of fractures during follow-up). We excluded from each cohort persons who experienced the outcome any time before cohort entry. Each person was followed from cohort entry to the date of the first hospitalization for the respective outcome, disenrollment from insurance, end of study period or death, whichever occurred first.
A case was defined as any cohort member (i) hospitalized for a fracture of the hip or pelvis, or (ii) hospitalized for other fractures (excluding hip, pelvis and vertebral fractures). Cases were identified by the main discharge codes (Supplementary Table S1). The day of admission was defined as the index date (ID). We randomly selected up to 100 controls per case using incidence-density sampling36 with matching on sex, age and time in the cohort. Controls were eligible to be selected more than once and could become cases later on during follow-up.36 For controls, the ID was defined as the ID of the corresponding case. Eligible patients hospitalized for any reason at the ID of the case were not at risk of being hospitalized for the outcome and were thus excluded from the set of potential controls (risk-set).36
Exposure Definition
Dispensations of ADs were identified through the ATC code N06A and categorized into the following classes (Table S2): tricyclics (TCAs), selective serotonin reuptake inhibitors (SSRIs), selective serotonin-noradrenaline reuptake inhibitors (SSNRIs), noradrenergic and specific serotonergic antidepressants (NASSAs), noradrenaline reuptake inhibitors (NARIs), monoamine oxidase inhibitors (MAOs), as well as herbal and other ADs.
Treatment episodes were defined based on the estimated supply, as the intended treatment duration and daily dose are not registered. To account for lower dosage and compliance in the elderly, supply was estimated as the dispensed amount of defined daily doses (DDDs) plus 150% of the DDDs.29,37,38 A new dispensation starting during the supply of the previous one marked the start of the new treatment episode. Exposure to ADs was ascertained at ID based on the interval between ID and the end of the most recent prior treatment episode and classified in the following mutually exclusive categories: (i) current use (supply overlapped ID), (ii) recent use (supply ended within 30 days before ID), (iii) past use (supply ended 31 through 90 days before ID) and (iv) remote use (supply ended ≥91 days before ID) (Figure S1). This latter category encompassed use of any AD, while the others were defined separately for selected individual agents. We defined two additional exposure categories: multiple use (encompassing users of two or more ADs within one exposure category) and switching (encompassing current users of an AD with recent use of an AD of a different class).
Covariates and Potential Confounders
We accounted for a wide range of potential confounders, including risk factors of fractures,39–45 co-morbidities (eg, vision disorders, Parkinson´s disease),46,47 co-medications (eg, antipsychotics, antiepileptics, hypnotics and sedatives),48 as well as indicators of life-style habits and of overall health status.
Co-morbidities were ascertained based on inpatient and confirmed outpatient diagnoses occurring (i) any time before ID for chronic diseases and some potentially recurrent conditions, such as syncope and dizziness, (ii) within 6 months before and at ID for acute infectious diseases (eg urinary tract infections or influenza which increase the risk of falling49–51) and (iii) within 1 year before and at ID for co-morbidities that are also proxies of indications, such as depression and anxiety disorder. The use of co-medications was ascertained based on dispensations occurring (i) any time before ID or (ii) within 6 months before and at ID for medications potentially affecting the risk of fractures, such as hypnotics and sedatives. Indicators of lifestyle habits were assessed based on diagnoses and medications related, respectively, to alcohol abuse, illicit drug use, obesity, and smoking, and occurring any time before ID. As indicators of overall health status, frailty and use of health care, we calculated the Charlson Co-morbidity Index,52 the number of different medication classes dispensed within 1 year before ID, nursing home residence (yes/no), and percentage of hospitalized time within 1 year before ID (excluding ID).
Statistical Analysis
Conditional logistic regression was used to estimate matched and confounder-adjusted odds ratios (aORs), with 95% confidence intervals (95% CI), comparing current, recent and past use of each AD with current users of mirtazapine as reference.
In the model, we included all potential confounders (full model) to further reduce the likelihood of residual confounding. Stratified analyses were performed by age (65–74, 75–84 and ≥ 85 years), sex, and prior diagnosis of depression. We performed sensitivity analyses (i) estimating supply based on the dispensed DDDs without any addition and (ii) using remote use of any AD as reference.
Ethics and Approvals
In Germany, the utilisation of health insurance data for scientific research is regulated by the Code of Social Law. All involved health insurance providers as well as the German Federal (Social) Insurance Office and the Senator for Science, Health, and Consumer Protection in Bremen as their responsible authorities approved the use of GePaRD data for this study. Informed consent for studies based on claims data is required by law unless obtaining consent appears unacceptable and would bias results, which was the case in this study. GePaRD does not include any identifying patient data. According to the Ethics Committee of the University of Bremen studies based on GePaRD are exempt from institutional review board review.
Results
The cohort addressing incident hip–pelvis fracture comprised 706,561 new users and the outcome of interest occurred in 39,853 persons (5.6%); of these, 80% were women and median age was 81 years (25–75% percentile 76–86). The cohort addressing other incident fractures comprised 628,780 new users and the outcome of interest occurred in 31,577 persons (5.0%); of these, 84% were women and median age was 79 years (73–84). Each cohort had approximately 2.9 million person-years of observation (hip fracture cohort 2,916,400 person-years; other fracture cohort 2,912,300 person-years).
Compared to respective controls, cases of both hip–pelvis and other fractures were hospitalized for a longer time, more likely used five or more different medications and had conditions potentially affecting the risk (Table 1). For instance, 32.3% of hip–pelvis fracture cases and 23.5% of other fracture cases had dementia vs 19.6% and 16.3% of controls; 48.7% of hip–pelvis cases and 46.8% of other fracture cases had osteoporosis vs 39.3% and 39.1% of controls. Cases were also more likely to have had prior injuries, to use antipsychotics (35.6% of hip–pelvis cases and 29.7% of other fracture cases vs 25.9% and 24.2% of controls, respectively), antiepileptics (11.1% and 10.3% vs 8.2% and 8.1%), and to have a history of alcohol abuse (5.4% and 4.8% vs 2.9% and 3.0%).
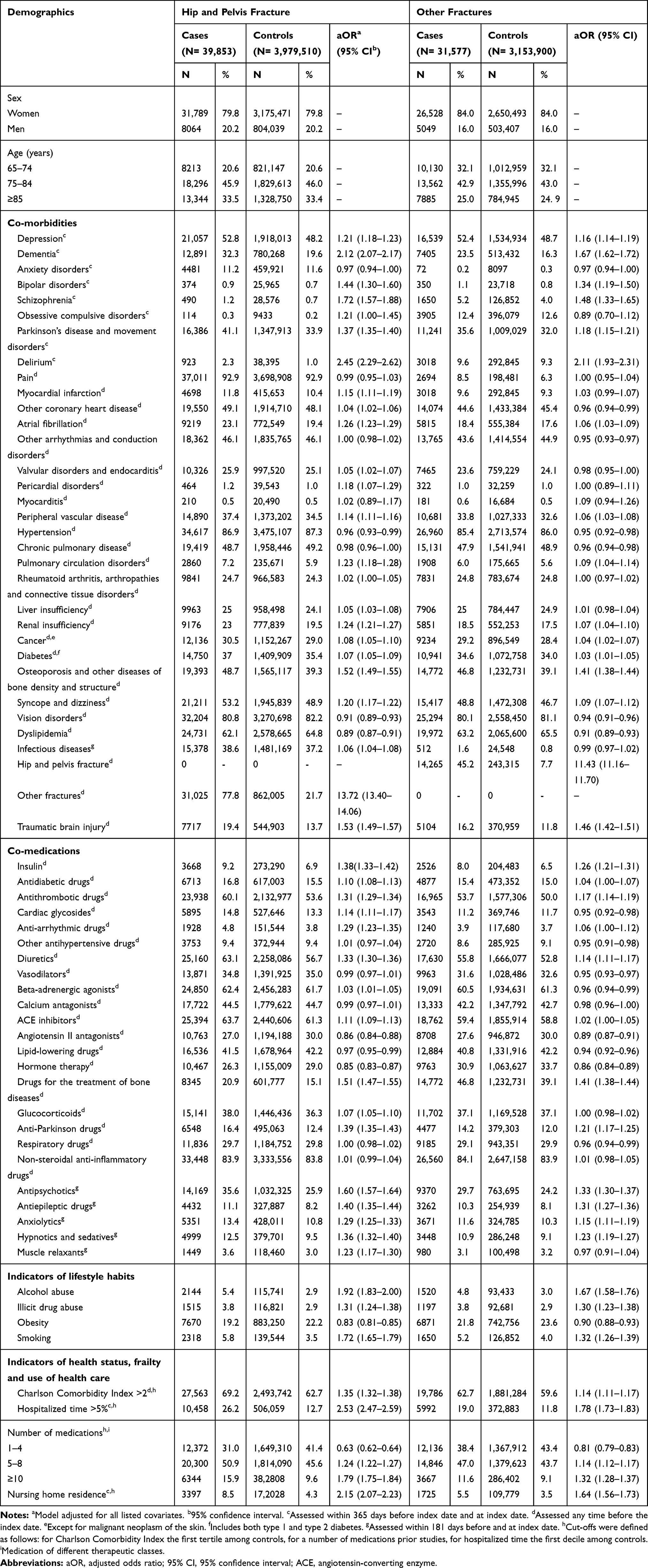 |
Table 1 Characteristics of Cases of Hip and Pelvis Fracture and of Other Fractures and Matched Controls |
Compared with current users of mirtazapine, the aOR of hip–pelvis fracture was increased by about 30% in current users of citalopram, duloxetine, escitalopram, venlafaxine, amitriptyline, and fluoxetine and by 20% for paroxetine (Table 2). The aOR of other fractures was increased by 50% in current users of duloxetine, citalopram, and paroxetine; it was increased by 40% for venlafaxine and escitalopram, and by 30% for sertraline. The aOR was lower for amitriptyline and trimipramine.
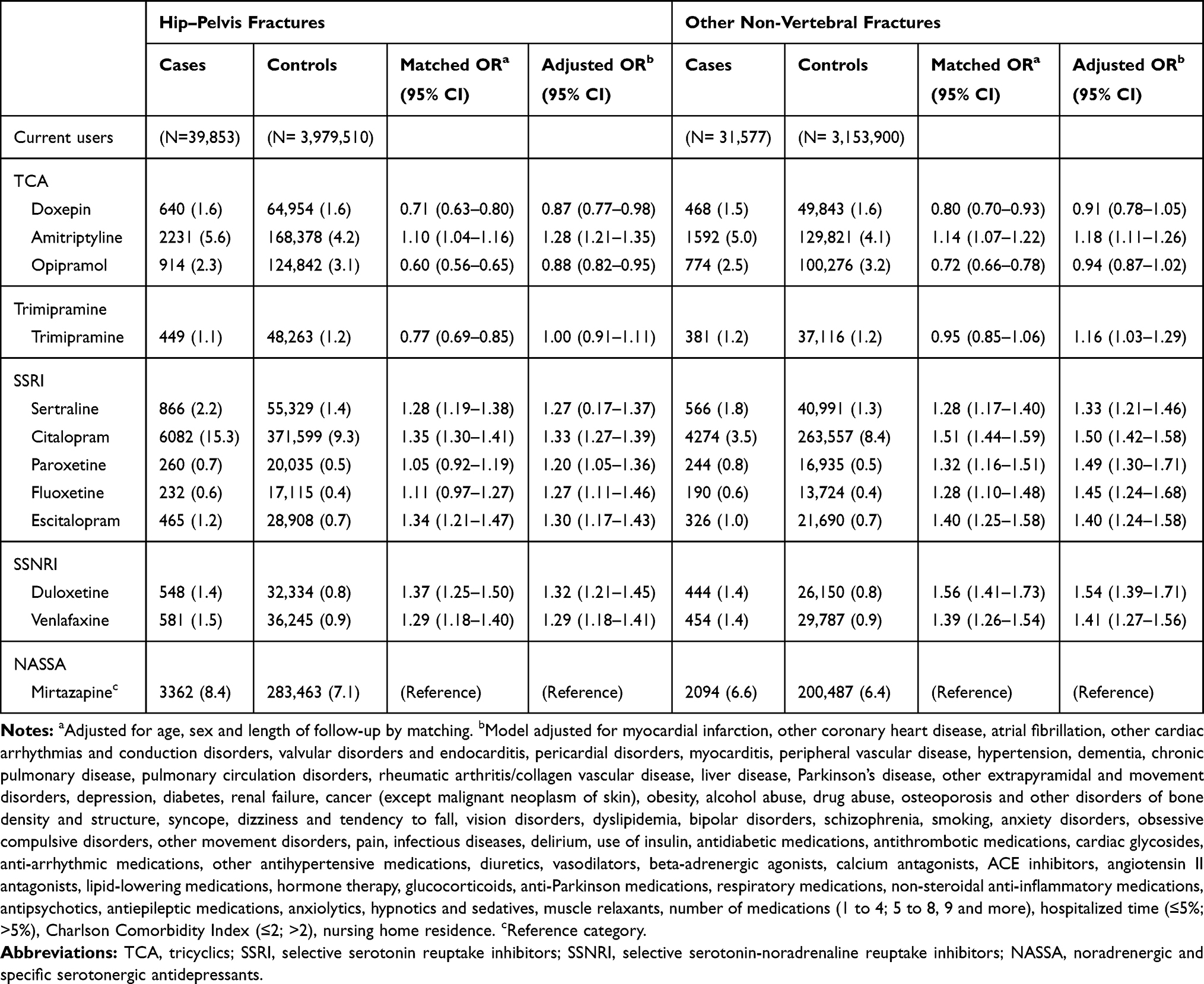 |
Table 2 Odds Ratio (OR), with 95 Confidence Interval (95% CI), of Hip–Pelvis Fracture and Other Non-Vertebral Fractures in Users of Individual Antidepressants (AD) Compared with Current Users of Mirtazapine and with Remote Users of Any AD. Main Analysis (DDDs + 150%) |
The pattern of risk of both hip–pelvis fracture (Figure 1) and other fractures (Figure 2) was similar in persons with and without depression, between men and women (Figures S2 and S3) and across age categories (Figures S4 and S5).
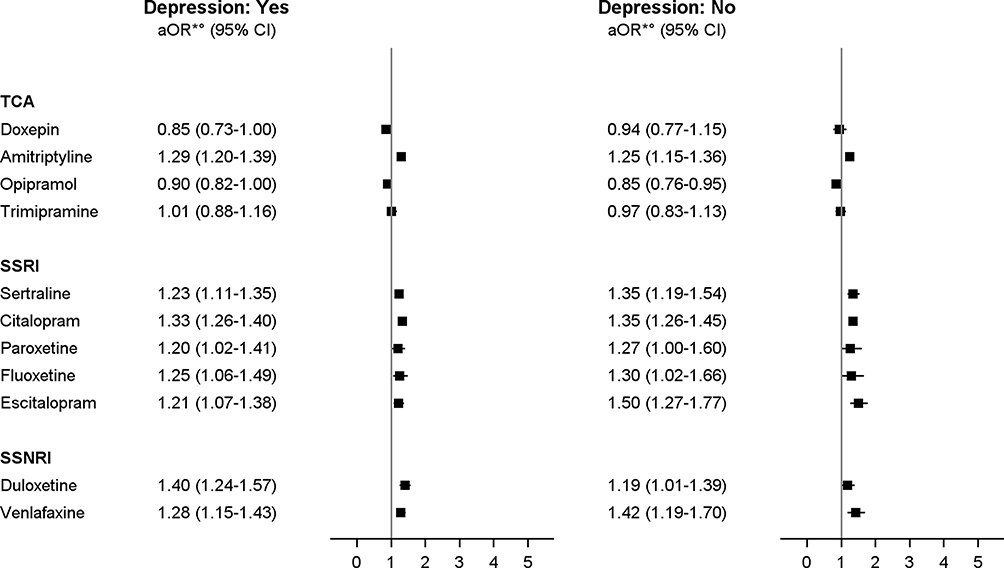 |
Figure 1 Odds ratio (OR) with 95% confidence interval (95% CI) of hip–pelvis fracture in current users of antidepressants (ADs) compared with current users of mirtazapine, by depression. Notes: The model did not converge in the group of age 85 years and above. *Model adjusted for all variables listed in Table 1. Abbreviations: TCA, tricyclics; SSRI, selective serotonin reuptake inhibitors; SSNRI, selective serotonin-noradrenaline reuptake inhibitors; NASSA, noradrenergic and specific serotonergic antidepressants; NARI, noradrenaline reuptake inhibitors; MAO, monoamine oxidase inhibitors. |
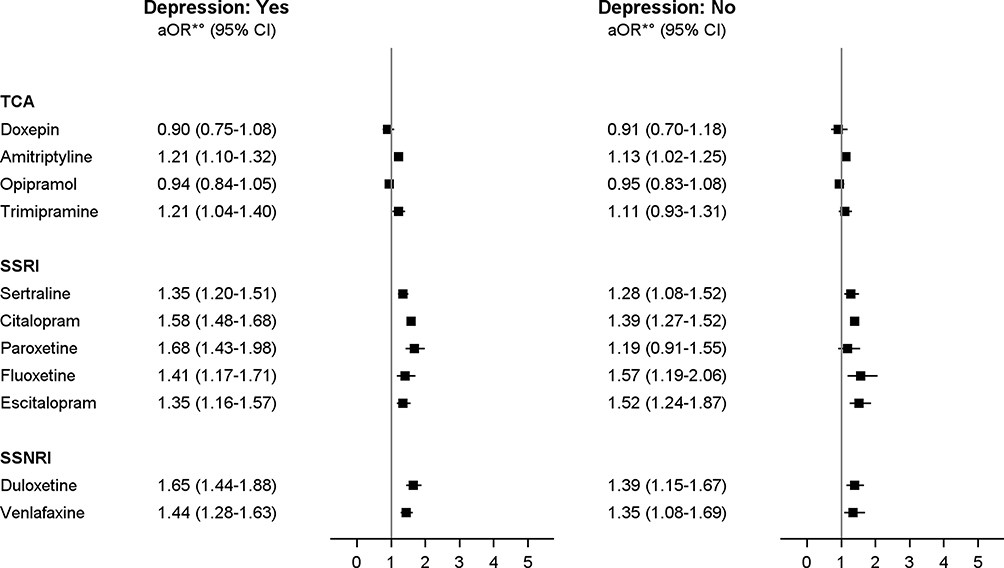 |
Figure 2 Odds ratio (OR) with 95% confidence interval (95% CI) of other non-vertebral fractures in current users of antidepressants (ADs) compared with current users of mirtazapine, by depression. Notes: The model did not converge in the group of age 85 years and above. *Model adjusted for all variables listed in Table 1. Abbreviations: TCA, tricyclics; SSRI, selective serotonin reuptake inhibitors; SSNRI, selective serotonin-noradrenaline reuptake inhibitors; NASSA, noradrenergic and specific serotonergic antidepressants; NARI, noradrenaline reuptake inhibitors; MAO, monoamine oxidase inhibitors. |
Sensitivity analysis using the DDDs without any addition to estimate supply confirmed the results in current users of all examined ADs (Table S3). Using remote users of any AD as a reference, the aORs of both outcomes were higher in current users of almost all the examined ADs, except for the aOR of hip fracture in current users of trimipramine (Table S4).
Discussion
Based on a cohort of more than 700,000 new users, we were able to estimate the risk of hip–pelvis fractures and other non-vertebral fractures in current users of 11 individual ADs, compared with current users of mirtazapine. Accounting for a wide range of co-morbidities, use of co-medications and other potential confounding factors, we found that current users of duloxetine and citalopram had the highest risk, increased by more than 30% for hip–pelvis fracture and by 50% for other fractures. Users of paroxetine had a 50% increased risk of other fractures and a 20% increased risk for hip–pelvis fractures. Among the other examined SSRIs and SSNRI, current users of sertraline, fluoxetine, escitalopram, and venlafaxine had a risk increased by approximately 30% for hip–pelvis fracture and between 30% and 40% for other fractures. Among the examined TCAs, the increase in risk was statistically significant only for amitriptyline (28% for hip–pelvis and 18% for other fractures), and trimipramine (16% for other fractures). The pattern of risk was similar for both hip–pelvis and other fractures, in men and women and across all included age groups, suggesting that the risk was not restricted to specific fractures or sub-populations.
To our knowledge, no study has evaluated the risk of hip fracture associated with individual ADs so far and only two other studies have evaluated the risk of other fractures associated with individual ADs.7,8 The first of these studies conducted among community-dwelling older adults in France7 compared the risk of any fractures of four individual SSRIs compared with never users of any AD. For citalopram and sertraline, this study found a risk of other fractures similar to our study, but a lower risk for fluoxetine and a slightly higher risk for paroxetine. The other study conducted among older adults with depression in the UK8 found that the risk of a composite outcome (encompassing fractures of upper and lower limb, ribs, skull, vertebrae, and pelvis) was increased by 60–70% in users of citalopram, fluoxetine, and sertraline, by about 50% in users of mirtazapine and paroxetine, and by 30% for amitriptyline and escitalopram. Similarly, we found a 50% increased risk for citalopram and paroxetine; amitriptyline also had a lower risk in our study. Conversely, in our cohort venlafaxine was not among the ADs with the highest risk, while in the study by Schneeweiss and Wang it had an 80% increased risk. Additionally, our study provides results for duloxetine, which was not evaluated in that cohort. The lower risks observed in our study might be explained by the different reference. Patients treated with an active comparator are probably more similar than non-users to exposed patients regarding the indication as well as measured and partly unmeasured characteristics (eg severity of depression, cognitive or functional impairment, or frailty). For that reason, using an active comparator is expected to result in less residual confounding, including confounding by indication. In support of this interpretation, one study53 showed that the risk of hip fracture associated with SSRIs decreased, albeit remaining statistically significant, when unmeasured confounding was accounted for.
Indeed, different ADs may have partially different indications and related different dosages. Although depression is the main indication, some ADs are prescribed for anxiety, sleep disturbances (eg mirtazapine, trazodone), or pain (eg amitriptyline), in addition to depression. These indications often overlap, as anxiety, pain and sleep disturbances are commonly associated with depression, particularly in older adults. In addition to using an active comparator, our study extensively adjusted for potential confounders including indications such as depression, other indications (eg anxiety disorders, pain, cancer, rheumatoid arthritis, arthropathies and connective tissue disorders), and medications to treat such indications (anxiolytics, hypnotics and sedatives, non-steroidal anti-inflammatory drugs, muscle relaxants).
It is thus a strength of our study that we used an active comparator design34 and extensively adjusted for potential indications and contraindications as well as co-morbidities, co-medications, indicators of health status and use of health care to reduce possible confounding. Our results did not change when we restricted the analysis to the more homogeneous group of patients with depression, suggesting that residual confounding by indication was small.
Differences between individual ADs regarding the risk of falls and consequences of falls such as fractures7,8 and traumatic brain injuries33 have consistently been reported, but the underlying mechanism is still unclear. Although almost all ADs may cause side effects that increase susceptibility to falls (eg sedation, dizziness, orthostatic hypotension),54 and thus increase the risk of fractures, the intensity of such effects may vary. Considering AD classes, SSRIs generally have less pronounced anticholinergic effects (such as confusion, delirium, and reduced visual acuity) than TCAs, but they can induce sleep disturbances and dizziness.55,56 Differences in fracture-related side effects are poorly characterized, particularly in older adults. In a meta-analysis of randomized controlled trials, examining several individual SSRIs and SSNRIs,57 older patients with major depression treated with duloxetine or venlafaxine reported dizziness three-times more frequently than placebo-treated patients. In patients treated with citalopram, escitalopram, and paroxetine the frequency of dizziness was 45–60% higher, while it was 30% and 10% higher for sertraline. This gradient is compatible with the differences between ADs regarding the risk of fractures observed in our study except for venlafaxine, which showed only an intermediately elevated risk in our study.
Our findings showing a higher risk of fractures associated with SSRIs than with TCAs are also consistent with prior studies.17,20-24 Potential mechanism explaining this difference is unclear; selective prescribing of TCAs to the less frail older adults or those with a lower baseline risk of falling may partially account for this result. Pharmacological properties may partly explain the large difference in risk between individual TCAs observed in our study. For instance, amitriptyline and trimipramine are considered to have relevant sedative, anticholinergic and hypotensive effects, while other TCAs ̶ also with relevant sedative effects ̶ have weaker anticholinergic properties as is the case for doxepin.58 In our study, users of doxepin did not have an increased risk of fractures.
In interpreting our results, limitations due to the nature of secondary data have to be considered including lack of direct information on the intended treatment duration and daily dose as well as on clinical aspects of the fractures (eg radiology confirmation, bone density data). We used elaborate methods to overcome these limitations as much as possible. Assessment of AD use was based on dispensations. On the one hand, this approach has the advantage of reflecting medications actually redeemed at the pharmacy level, contrary to prescriptions or medical records. On the other hand, we had to estimate treatment duration based on the dispensed DDDs but we took into account that dose and compliance are lower in older patients37,59 and further varied these assumptions in sensitivity analyses which supported the robustness of our findings in this regard. The assumptions regarding daily dose were varied uniformly for all study participants; thus, potential differences in dose related to different indications were not examined. However, the results did not change in the more homogeneous group of persons with depression suggesting that differential misclassification of the exposure was small, if there was any.
We defined the outcome as fractures leading to hospitalization, thus focusing on clinically relevant events, and we identified the outcome using hospital main discharge diagnoses. In Germany, hospital main discharge diagnoses are considered to have a high validity since they are based on all information relevant to diagnosis gathered during the in-hospital stay (including imaging results) and are subject to regular inspection. We addressed fractures of hip–pelvis as an outcome because they are the most frequent fractures in old age and in 90% of cases are due to falls,60–62 To comprehensively characterize the risk, we also addressed other non-vertebral fractures as a composite outcome. This encompasses fractures of all sites to capture clinically relevant events with high sensitivity. However, to avoid outcome misclassification, we excluded vertebral fractures because up to two thirds of them remain undiagnosed in older adults.63–65 As fractures of the hip and pelvis usually present with severe pain and inability and need surgery, they are generally accurately diagnosed and coded. This also holds true for other non-vertebral fractures in older patients, since even milder or suspect cases usually undergo diagnostic assessment in order to clarify symptoms and avoid complications due to lack or delay of treatment.
In conclusion, our study showed that the risk of fractures varied between ADs, but for most agents was higher than the risk for mirtazapine. When treating older adults with ADs, prescribers should carefully consider the risk profile of individual ADs regarding the risk of fractures, which are a major health problem in this population.
Disclosure
JR, BK, UH and TS are working at an independent, non-profit research institute, the Leibniz Institute for Prevention Research and Epidemiology – BIPS. Unrelated to this study, BIPS occasionally conducts studies financed by the pharmaceutical industry. Almost exclusively, these are post-authorization safety studies (PASS) requested by health authorities. The design and conduct of these studies, as well as the interpretation and publication, are not influenced by the pharmaceutical industry. At the time of performing the study, writing the manuscript and submission, FEP worked at the Leibniz Institute for Prevention Research and Epidemiology – BIPS. Unrelated to the work presented in this article, she worked from 1st August 2019 to 24th February 2020 at UCB Pharma and since 1st March 2020 she is working at Bayer AG. The authors report no other conflicts of interest in this work.
References
1. Wong J, Motulsky A, Abrahamowicz M, Eguale T, Buckeridge DL, Tamblyn R. Off-label indications for antidepressants in primary care: descriptive study of prescriptions from an indication based electronic prescribing system. BMJ. 2017;356:j603. doi:10.1136/bmj.j603
2. Ufer M, Meyer SA, Junge O, et al. Patterns and prevalence of antidepressant drug use in the German state of Baden-Wuerttemberg: a prescription-based analysis. Pharmacoepidemiol Drug Saf. 2007;16(10):1153–1160. doi:10.1002/pds.1405
3. Abbing-Karahagopian V, Huerta C, Souverein PC, et al. Antidepressant prescribing in five European countries: application of common definitions to assess the prevalence, clinical observations, and methodological implications. Eur J Clin Pharmacol. 2014;70(7):849–857. doi:10.1007/s00228-00014-01676-z
4. Antidepressants in Patterns of Use of Mental Health Services and Prescription Medications; 2011. Available from: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4329.0.00.003~2011~Main%20Features~Antidepressants~10008.
5. Hansen DG, Rosholm JU, Gichangi A, Vach W. Increased use of antidepressants at the end of life: population-based study among people aged 65 years and above. Age Ageing. 2007;36(4):449–454. doi:10.1093/ageing/afm056
6. Moore TJ, Mattison DR. Adult utilization of psychiatric drugs and differences by sex, age, and race. JAMA Intern Med. 2017;177(2):274–275. doi:10.1001/jamainternmed.2016.7507
7. Carriere I, Farre A, Norton J, et al. Patterns of selective serotonin reuptake inhibitor use and risk of falls and fractures in community-dwelling elderly people: the three-city cohort. Osteoporos Int. 2016;27(11):3187–3195. doi:10.1007/s00198-016-3667-7
8. Coupland C, Dhiman P, Morriss R, Arthur A, Barton G, Hippisley-Cox J. Antidepressant use and risk of adverse outcomes in older people: population based cohort study. BMJ. 2011;343(aug02 1):d4551. doi:10.1136/bmj.d4551
9. Richards JB, Papaioannou A, Adachi JD, et al. Effect of selective serotonin reuptake inhibitors on the risk of fracture. Arch Intern Med. 2007;167(2):188–194. doi:10.1001/archinte.167.2.188
10. Ensrud KE, Blackwell T, Mangione CM, et al. Central nervous system active medications and risk for fractures in older women. Arch Intern Med. 2003;163(8):949–957. doi:10.1001/archinte.163.8.949
11. Moura C, Bernatsky S, Abrahamowicz M, et al. Antidepressant use and 10-year incident fracture risk: the population-based Canadian Multicentre Osteoporosis Study (CaMoS). Osteoporos Int. 2014;25(5):1473–1481. doi:10.1007/s00198-014-2649-x
12. Ziere G, Dieleman JP, van der Cammen TJ, Hofman A, Pols HA, Stricker BH. Selective serotonin reuptake inhibiting antidepressants are associated with an increased risk of nonvertebral fractures. J Clin Psychopharmacol. 2008;28(4):411–417. doi:10.1097/JCP.0b013e31817e0ecb
13. Bolton JM, Morin SN, Majumdar SR, et al. Association of mental disorders and related medication use with risk for major osteoporotic fractures. JAMA Psychiatry. 2017;74(6):641–648. doi:10.1001/jamapsychiatry.2017.0449
14. Ray WA. Cyclic antidepressants and the risk of hip fracture. Arch Intern Med. 1991;151(4):754–756. doi:10.1001/archinte.1991.00400040096021
15. Liu B, Anderson G, Mittmann N, To T, Axcell T, Shear N. Use of selective serotonin-reuptake inhibitors or tricyclic antidepressants and risk of hip fractures in elderly people. Lancet. 1998;351(9112):1303–1307. doi:10.1016/S0140-6736(97)09528-7
16. Hubbard R. Exposure to tricyclic and selective serotonin reuptake inhibitor antidepressants and the risk of hip fracture. Am J Epidemiol. 2003;158(1):77–84. doi:10.1093/aje/kwg114
17. Souverein PC, Abbing-Karahagopian V, Martin E, et al. Understanding inconsistency in the results from observational pharmacoepidemiological studies: the case of antidepressant use and risk of hip/femur fractures. Pharmacoepidemiol Drug Saf. 2016;25(Suppl 1):88–102. doi:10.1002/pds.3862
18. Leach MJ, Pratt NL, Roughead EE. Psychoactive medicine use and the risk of hip fracture in older people: a case-crossover study. Pharmacoepidemiol Drug Saf. 2015;24(6):576–582. doi:10.1002/pds.3785
19. Bakken MS, Engeland A, Engesaeter LB, Ranhoff AH, Hunskaar S, Ruths S. Increased risk of hip fracture among older people using antidepressant drugs: data from the Norwegian prescription database and the Norwegian hip fracture registry. Age Ageing. 2013;42(4):514–520. doi:10.1093/ageing/aft009
20. Wu Q, Bencaz AF, Hentz JG, Crowell MD. Selective serotonin reuptake inhibitor treatment and risk of fractures: a meta-analysis of cohort and case-control studies. Osteoporos Int. 2012;23(1):365–375. doi:10.1007/s00198-011-1778-8
21. Wu Q, Qu W, Crowell MD, Hentz JG, Frey KA. Tricyclic antidepressant use and risk of fractures: a meta-analysis of cohort and case-control studies. J Bone Miner Res. 2013;28(4):753–763. doi:10.1002/jbmr.1813
22. Eom CS, Lee HK, Ye S, Park SM, Cho KH. Use of selective serotonin reuptake inhibitors and risk of fracture: a systematic review and meta-analysis. J Bone Miner Res. 2012;27(5):1186–1195. doi:10.1002/jbmr.1554
23. Oderda LH, Young JR, Asche CV, Pepper GA. Psychotropic-related hip fractures: meta-analysis of first-generation and second-generation antidepressant and antipsychotic drugs. Ann Pharmacother. 2012;46(7–8):917–928. doi:10.1345/aph.1Q589
24. Rabenda V, Nicolet D, Beaudart C, Bruyere O, Reginster JY. Relationship between use of antidepressants and risk of fractures: a meta-analysis. Osteoporos Int. 2013;24(1):121–137. doi:10.1007/s00198-012-2015-9
25. Pigeot I, Ahrens W. Establishment of a pharmacoepidemiological database in Germany: methodological potential, scientific value and practical limitations. Pharmacoepidemiol Drug Saf. 2008;17(3):215–223. doi:10.1002/pds.1545
26. Schink T, Garbe E. Representativity of dispensations of non-steroidal anti-inflammatory drugs (NSAIDs) in the German pharmacoepidemiological research database. Pharmacoepidemiol Drug Saf. 2010;19:S294–S294.
27. Garbe E, Kreisel SH, Behr S. Risk of subarachnoid hemorrhage and early case fatality associated with outpatient antithrombotic drug use. Stroke. 2013;44(9):2422–2426. doi:10.1161/STROKEAHA.111.000811
28. Ohlmeier C, Langner I, Garbe E, Riedel O. Validating mortality in the German Pharmacoepidemiological Research Database (GePaRD) against a mortality registry. Pharmacoepidemiol Drug Saf. 2016;25(7):778–784. doi:10.1002/pds.4005
29. Jobski K, Schmedt N, Kollhorst B, Krappweis J, Schink T, Garbe E. Characteristics and drug use patterns of older antidepressant initiators in Germany. Eur J Clin Pharmacol. 2017;73(1):105–113. doi:10.1007/s00228-00016-02145-00227.
30. Schmedt N, Jobski K, Kollhorst B, et al. Treatment patterns and characteristics of older antipsychotic users in Germany. Int Clin Psychopharmacol. 2016;31(3):159–169. doi:10.1097/YIC.0000000000000119
31. Schmedt N, Garbe E. Antipsychotic drug use and the risk of venous thromboembolism in elderly patients with dementia. J Clin Psychopharmacol. 2013;33(6):753–758. doi:10.1097/JCP.0b013e3182a412d5
32. Schroder C, Dorks M, Kollhorst B, et al. Extent and risks of antidepressant off-label use in children and adolescents in Germany between 2004 and 2011. Pharmacoepidemiol Drug Saf. 2017;26(11):1395–1402. doi:10.1002/pds.4289
33. Pisa FE, Reinold J, Kollhorst B, Haug U, Schink T. Antidepressants and the risk of traumatic brain injury in the elderly: differences between individual agents. Clin Epidemiol. 2019;11:185–196. doi:10.2147/CLEP.S173667
34. Lund JL, Richardson DB, Sturmer T. The active comparator, new user study design in pharmacoepidemiology: historical foundations and contemporary application. Curr Epidemiol Rep. 2015;2(4):221–228. doi:10.1007/s40471-015-0053-5
35. Leach MJ, Pratt NL, Roughead EE. The risk of hip fracture due to mirtazapine exposure when switching antidepressants or using other antidepressants as add-on therapy. Drugs Real World Outcomes. 2017;4(4):247–255. doi:10.1007/s40801-017-0120-y
36. Rothman K, Greenland S, Lash C. Case-control studies. In: Rothman K, Greenland S, Lash C, editors. Modern Epidemiology.
37. Gardarsdottir H, Souverein PC, Egberts TC, Heerdink ER. Construction of drug treatment episodes from drug-dispensing histories is influenced by the gap length. J Clin Epidemiol. 2010;63(4):422–427. doi:10.1016/j.jclinepi.2009.07.001
38. Gardarsdottir H, Heerdink ER, Egberts AC. Potential bias in pharmacoepidemiological studies due to the length of the drug free period: a study on antidepressant drug use in adults in the Netherlands. Pharmacoepidemiol Drug Saf. 2006;15(5):338–343. doi:10.1002/pds.1223
39. Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E. Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology. 2010;21(5):658–668. doi:10.1097/EDE.0b013e3181e89905
40. Johnell K, Jonasdottir Bergman G, Fastbom J, Danielsson B, Borg N, Salmi P. Psychotropic drugs and the risk of fall injuries, hospitalisations and mortality among older adults. Int J Geriatr Psychiatr. 2017;32(4):414–420. doi:10.1002/gps.4483
41. Ensrud KE, Blackwell TL, Mangione CM, et al. Central nervous system-active medications and risk for falls in older women. J Am Geriatr Soc. 2002;50(10):1629–1637. doi:10.1046/j.1532-5415.2002.50453.x
42. van Doorn C, Gruber-Baldini AL, Zimmerman S, et al. Dementia as a risk factor for falls and fall injuries among nursing home residents. J Am Geriatr Soc. 2003;51(9):1213–1218. doi:10.1046/j.1532-5415.2003.51404.x
43. Tolppanen A-M, Lavikainen P, Soininen H, Hartikainen S, Kado D. Incident hip fractures among community dwelling persons with Alzheimer’s disease in a Finnish nationwide register-based cohort. PLoS One. 2013;8(3):e59124. doi:10.1371/journal.pone.0059124
44. Park H, Satoh H, Miki A, Urushihara H, Sawada Y. Medications associated with falls in older people: systematic review of publications from a recent 5-year period. Eur J Clin Pharmacol. 2015;71(12):1429–1440. doi:10.1007/s00228-015-1955-3
45. Richardson K, Bennett K, Kenny RA. Polypharmacy including falls risk-increasing medications and subsequent falls in community-dwelling middle-aged and older adults. Age Ageing. 2015;44(1):90–96. doi:10.1093/ageing/afu141
46. Reyes C, Estrada P, Nogues X, et al. The impact of common co-morbidities (as measured using the Charlson index) on hip fracture risk in elderly men: a population-based cohort study. Osteoporos Int. 2014;25(6):1751–1758. doi:10.1007/s00198-014-2682-9
47. Beydoun HA, Beydoun MA, Mishra NK, Rostant OS, Zonderman AB, Eid SM. Comorbid Parkinson’s disease, falls and fractures in the 2010 National Emergency Department Sample. Parkinsonism Relat Disord. 2017;35:30–35. doi:10.1016/j.parkreldis.2016.11.005
48. Koponen M, Taipale H, Lavikainen P, et al. Antipsychotic use and the risk of hip fracture among community-dwelling persons with Alzheimer’s disease. J Clin Psychiatr. 2017;78(3):e257–e263. doi:10.4088/JCP.15m10458
49. McConeghy KW, Lee Y, Zullo AR, et al. Influenza illness and hip fracture hospitalizations in nursing home residents: are they related? J Gerontol a Biol Sci Med Sci. 2017;73(12):1638–1642.
50. Noguchi N, Chan L, Cumming RG, Blyth FM, Naganathan V. A systematic review of the association between lower urinary tract symptoms and falls, injuries, and fractures in community-dwelling older men. Aging Male. 2016;19(3):168–174. doi:10.3109/13685538.2016.1169399
51. Parsons JK, Mougey J, Lambert L, et al. Lower urinary tract symptoms increase the risk of falls in older men. BJU Int. 2009;104(1):63–68. doi:10.1111/j.1464-410X.2008.08317.x
52. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. doi:10.1093/aje/kwq433
53. Schneeweiss S, Wang PS. Association between SSRI use and hip fractures and the effect of residual confounding bias in claims database studies. J Clin Psychopharmacol. 2004;24(6):632–638. doi:10.1097/01.jcp.0000145344.76288.39
54. Aronson JK. Meyler’s Side Effects of Drugs. The International Encyclopedia of Adverse Drug Reactions and Interactions.
55. Darowski A, Chambers SA, Chambers DJ. Antidepressants and falls in the elderly. Drugs Aging. 2009;26(5):381–394. doi:10.2165/00002512-200926050-00002
56. Sultana J, Spina E, Trifiro G. Antidepressant use in the elderly: the role of pharmacodynamics and pharmacokinetics in drug safety. Expert Opin Drug Metab Toxicol. 2015;11(6):883–892. doi:10.1517/17425255.2015.1021684
57. Thorlund K, Druyts E, Wu P, Balijepalli C, Keohane D, Mills E. Comparative efficacy and safety of selective serotonin reuptake inhibitors and serotonin‐norepinephrine reuptake inhibitors in older adults: a network meta‐analysis. J Am Geriatr Soc. 2015;63(5):1002–1009. doi:10.1111/jgs.13395
58. Gillman PK. Tricyclic antidepressant pharmacology and therapeutic drug interactions updated. Br J Pharmacol. 2007;151(6):737–748. doi:10.1038/sj.bjp.0707253
59. Schneeweiss S, Avorn J. A review of uses of health care utilization databases for epidemiologic research on therapeutics. J Clin Epidemiol. 2005;58(4):323–337. doi:10.1016/j.jclinepi.2004.10.012
60. Clement ND, Court-Brown CM. Elderly pelvic fractures: the incidence is increasing and patient demographics can be used to predict the outcome. Eur J Orthop Surg Traumatol. 2014;24(8):1431–1437. doi:10.1007/s00590-014-1439-7
61. Court-Brown CM, McQueen MM. Global forum: fractures in the elderly. J Bone Joint Surg Am. 2016;98(9):e36. doi:10.2106/JBJS.15.00793
62. Seppala LJ, Wermelink A, de Vries M, et al. Fall-risk-increasing drugs: a systematic review and meta-analysis: II. Psychotropics. J Am Med Dir Assoc. 2018;19(4):371e311–371 e317.
63. Fink HA, Milavetz DL, Palermo L, et al. What proportion of incident radiographic vertebral deformities is clinically diagnosed and vice versa? J Bone Miner Res. 2005;20(7):1216–1222. doi:10.1359/JBMR.050314
64. Delmas PD, van de Langerijt L, Watts NB, et al. Underdiagnosis of vertebral fractures is a worldwide problem: the IMPACT study. J Bone Miner Res. 2005;20(4):557–563. doi:10.1359/JBMR.041214
65. Ensrud KE, Blackwell TL, Fink HA, et al. What proportion of incident radiographic vertebral fractures in older men is clinically diagnosed and vice versa: a prospective study. J Bone Miner Res. 2016;31(8):1500–1503. doi:10.1002/jbmr.2831
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.