")
Back to Journals » Advances in Medical Education and Practice » Volume 8
Increasing medical student exposure to musculoskeletal medicine: the initial impact of the Orthopaedic Surgery and Sports Medicine Interest Group
Authors Mickelson DT, Louie PK, Gundle KR, Farnand AW, Hanel DP
Received 15 April 2017
Accepted for publication 13 June 2017
Published 31 July 2017 Volume 2017:8 Pages 551—558
DOI https://doi.org/10.2147/AMEP.S139701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Dayne T Mickelson,1 Philip K Louie,2 Kenneth R Gundle,3 Alex W Farnand,4 Douglas P Hanel5
1Department of Orthopedic Surgery and Sports Medicine, Duke University, Durham, NC, USA; 2Department of Orthopedic Surgery, Rush University Medical Center, Chicago, IL, USA; 3Department of Orthopedics and Rehabilitation, Oregon Health and Science University, Portland, OR, USA; 4Department of General Surgery, Presence Saint Joseph Hospital – Chicago, Chicago, IL, USA; 5Department of Orthopedic Surgery and Sports Medicine, University of Washington, Harborview Medical Center, Seattle, WA, USA
Purpose: To investigate the impact of the Orthopaedic Surgery and Sports Medicine Interest Group (OSSMIG) on medical student interest and confidence in core musculoskeletal (MSK) concepts through supplemental education and experiences at a single tertiary, academic institution.
Methods: Medical student OSSMIG members at various levels of training were anonymously surveyed at the beginning and end of the 2014–2015 academic year.
Results: Eighteen (N=18) medical student interest group members completed the survey. Significant improvement in their level of training was observed with regard to respondents’ self-assessed competence and confidence in MSK medicine (p<0.05). Additionally, respondents’ attitudes toward exposure and support from the interest group were significantly higher than those provided by the institution (p<0.05). Members believed OSSMIG increased interest in MSK medicine, improved confidence in their ability to perform orthopedics-related physical exams, strengthened mentorship with residents and attendings, and developed a connection with the Department of Orthopedic Surgery and its residents (median “Strongly Agree”, interquartile range one and two scale items).
Conclusion: Since its inception 8 years ago, OSSMIG has been well received and has positively impacted University of Washington School of Medicine students through various interventions. Surgical interest groups should target both the students interested in primary care and surgery. Medical schools can provide additional exposure to MSK medicine by leveraging interest groups that provide early clinical experiences and supplementary instruction.
Keywords: musculoskeletal education, medical education, supplemental experience, student teaching
Introduction
The burden of musculoskeletal (MSK) disorders within the USA and around the world is not reflected in current medical school curriculums.1 MSK diseases affect over half of the USA population and account for over 18% of the 1.3 billion annual health care visits.2,3 However, medical students often lack confidence and knowledge about MSK medicine, especially those pursuing nonorthopedic careers.4–7 Additionally, for students interested in pursuing surgical careers, previous research has demonstrated that early opportunities, clinical exposure, and positive role models have a positive impact.8,9 This is especially true during the preclinical years and third year clerkships, prior to beginning the residency application process.10–12
The University of Washington School of Medicine (UWSOM) has been ranked by the US News and World Report as the No. 1 medical school in the nation for primary care training in 23 of the past 24 years.13 The average number of UWSOM students entering primary care specialties has been over 50% annually.14 The UWSOM required curriculum includes one-quarter of MSK education during the first year, one general surgery rotation, and one elective surgical rotation. With an emphasis on primary care, the majority of this curriculum provides limited exposure to surgical subspecialties.
The Orthopaedic Surgery and Sports Medicine Interest Group (OSSMIG) was established in 2009. Its goals were to provide supplemental education and experiences of core MSK concepts, examinations, and diagnoses; as well as support students interested in applying to orthopedic surgery residency programs. It was proposed that OSSMIG would increase interest in orthopedics and improve medical students’ competency and confidence in MSK medicine, regardless of their chosen career path. The purpose of this study is to assess the OSSMIG through an anonymous survey of its participants.
Materials and methods
Conception and development of OSSMIG
The OSSMIG was established in August 2009 led by junior medical students with support from the orthopedic surgery department and its residents. Founding officers created a constitution and registered with the institution’s Student Activities Office. The constitution outlined five core objectives:
- Provide students additional MSK instruction through lectures and workshops.
- Present students with opportunities to experience the field of orthopedic surgery outside of the classroom.
- Offer students orthopedic research and networking opportunities.
- Support students applying for orthopedic surgery by advising them throughout the process.
- Promote mentoring among medical students, residents, and the attending surgeons.
To improve the quality of mentorship and experiences, OSSMIG cultivated a relationship with the institution’s Department of Orthopedic Surgery and Sports Medicine. This relationship was established through a faculty advisor who oversaw a core group of orthopedic residents interested in educating and mentoring. Residents acted as liaisons by coordinating, teaching, and leading events.
OSSMIG officers sent information to all UWSOM students and presented at the annual interest group fair to engage anyone interested in MSK medicine. An institutional listserv (application that circulates emails to subscribers) was created, allowing leadership to easily communicate with group members. A full-featured, department-supported OSSMIG website (http://www.orthop.washington.edu/?q=ossmig/orthopaedic-surgery-and-sports-medicine-interest-group-ossmig.html) was created, which includes announcements, calendars, and member resources.
Since inception, OSSMIG has developed and maintained a diverse offering of activities, workshops, and services. These extracurricular activities allow students to explore MSK medicine and orthopedic surgery, while receiving guidance and gaining knowledge (Table 1). These events and resources are reviewed and adapted annually for quality improvement.
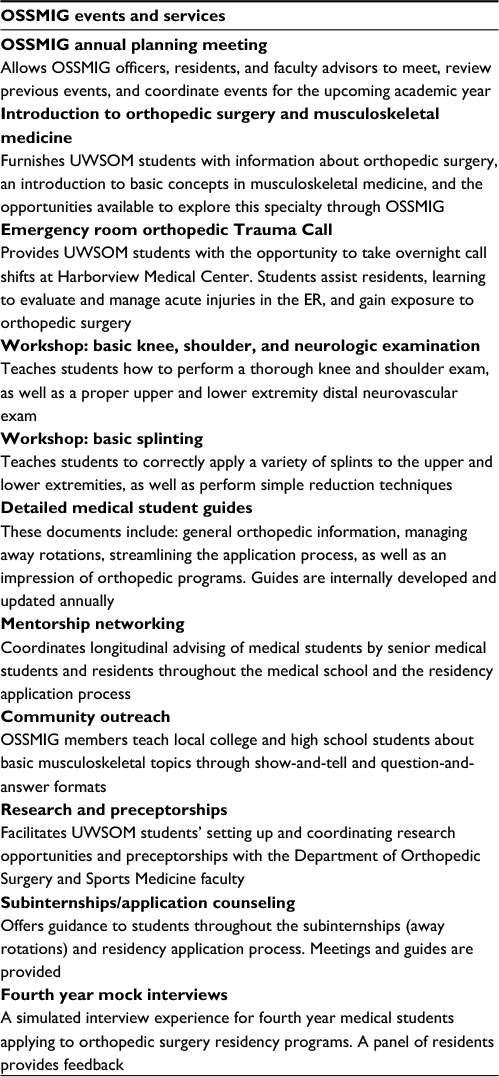 | Table 1 Events and services provided by OSSMIG throughout the academic year Abbreviations: ER, emergency room; OSSMIG, Orthopaedic Surgery and Sports Medicine Interest Group; UWSOM, University of Washington School of Medicine. |
Outcomes
Cross-sectional surveys of OSSMIG members were administered using a secure anonymous institutional online survey system. Surveys were conducted at the beginning and end of each academic year as part of an internal quality assurance and quality improvement process. The survey from the 2014–2015 academic year used a de-identified submission process allowing for blinded data analysis. The institution’s Human Subjects Division reviewed the study and determined it to be exempt from Institutional Review Board approval due to the usage of anonymous surveys and data. Informed consent was provided through the survey platform and verified upon submission of the survey.
At the start of the academic year, members completed a 15-question survey regarding their planned career path, perception of current MSK education, confidence in basic MSK knowledge, and expectations. At the end of the academic year, members completed a 20-question survey inquiring about their satisfaction with OSSMIG, influence on their interests, and comfort with MSK concepts. Answers were provided on a five-point Likert scale.
Statistical analysis
Statistics were performed with R version 3.2.2 (R Core Team, Vienna, Austria) including packages ggplot2, pwr, and plyr. Due to categorical data that did not generally have a normal distribution, nonparametric statistics were utilized. Central tendency is reported by the median and interquartile range (IQR). Differences in paired responses were assessed by the Wilcoxon signed rank test. For unpaired responses, the Wilcoxon rank sum test was used. A p value of <0.05 was considered significant. All analyses were preplanned. A power analysis based on finding a strong effect size estimated that 18 evaluation periods would provide an 80% chance of finding a difference between paired responses, if one exists.6
Results
Membership
For the 2014–2015 academic year, there were 60 active OSSMIG members (6.7% of the student body; 60/900). Membership consists of students interested in pursuing orthopedic surgery (67%), primary care (22%), and undecided students (11%). From 2009 to 2015, OSSMIG membership increased from 20 to 60 students. Membership peaks at the beginning of each academic year and is highest among preclinical students (67% – first and second year students). The 2014–2015 interest group membership survey response rate was 30% (18/60). The 18 interest group member respondents comprising the analysis group had diverse training levels (three first year, five second year, five third year, four fourth year medical students, and one student declining to answer the question). Respondents were queried at the end of the academic year about the overall influence of OSSMIG on their career plans (N=18). These members reported that OSSMIG confirmed their interest in orthopedic surgery (50%), convinced them to pursue orthopedic surgery (17%), influenced them to continue to pursue another specialty (28%), and dissuaded them from pursuing orthopedic surgery (5%).
Self-assessed competence
Two sets of questions compared respondents’ self-assessed competence and confidence for their level of training. When students were asked if they felt competent with MSK anatomy, responses improved from a median of “Neutral” (IQR – one scale item) before the interest group involvement to “Agree” (IQR – zero) afterward. This self-assessment was significant (Wilcoxon signed rank test, p=0.007; Figure 1). When students were asked if they felt competent with basic MSK trauma care, the median answer from pre- to post-interest group involvement shifted from “Disagree” (IQR – 1.75 scale items) to “Agree” (IQR – two scale items), which was significant (Wilcoxon signed rank test, p=0.006; Figure 2).
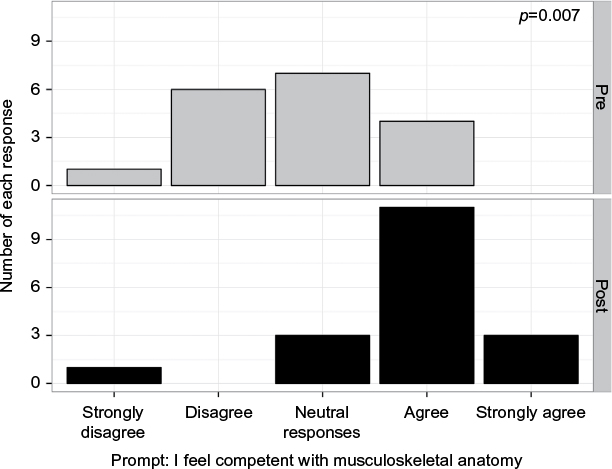 | Figure 1 Medical students’ pre- and post-OSSMIG self-assessed competence with musculoskeletal anatomy. Abbreviation: OSSMIG, Orthopaedic Surgery and Sports Medicine Interest Group. |
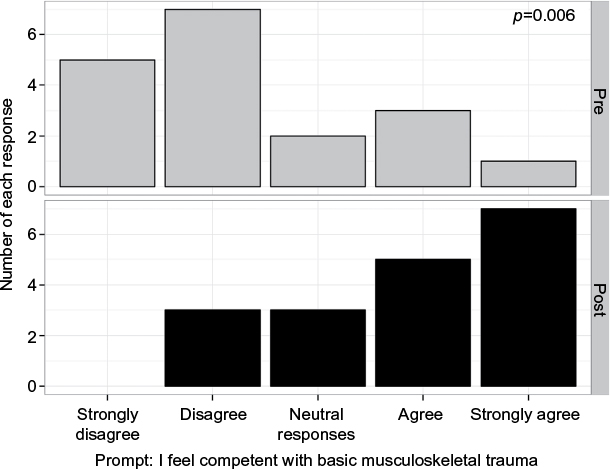 | Figure 2 Medical students’ pre- and post-OSSMIG self-assessed competence with basic musculoskeletal trauma. Abbreviation: OSSMIG, Orthopaedic Surgery and Sports Medicine Interest Group. |
Attitudes of institution vs interest group
Two sets of questions compared respondents’ attitudes regarding exposure and support from their institution and the interest group. When responding to a statement about providing adequate exposure to MSK medicine and the field of orthopedic surgery, the interest group received significantly higher scores (median of “Disagree” vs “Agree”, Wilcoxon rank sum test p=0.009; Figure 3). Similarly, when responding to a statement about providing adequate support to students pursuing a residency in orthopedic surgery, the interest group received significantly more positive responses (median of “Disagree” vs “Agree”, Wilcoxon rank sum test p=0.001; Figure 4).
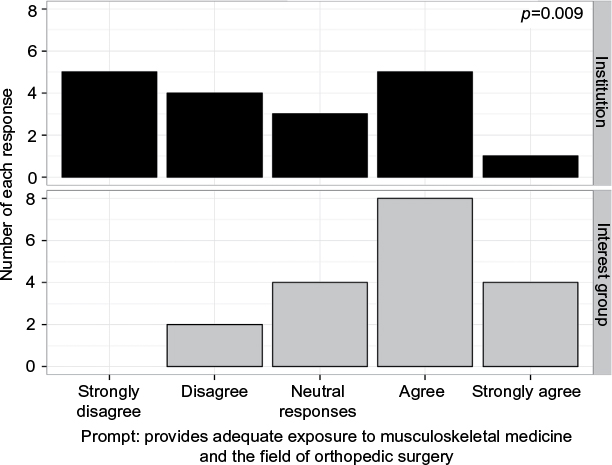 | Figure 3 Medical students’ attitudes toward institutional vs OSSMIG exposure to musculoskeletal medicine and the field of orthopedic surgery. Abbreviation: OSSMIG, Orthopaedic Surgery and Sports Medicine Interest Group. |
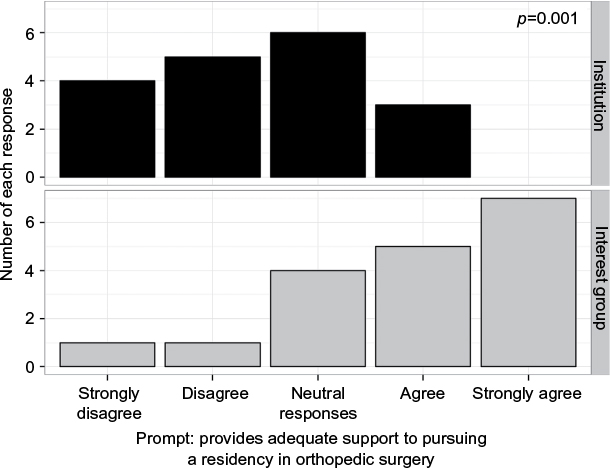 | Figure 4 Medical student attitudes toward institutional vs OSSMIG support to students pursuing a residency in orthopedic surgery. Abbreviation: OSSMIG, Orthopaedic Surgery and Sports Medicine Interest Group. |
Assessment of the interest group
A series of questions asked respondents about their experiences with the interest group. Overall, the results were positive (Figure 5). Respondents tended to find OSSMIG helpful in deciding whether to pursue a career in orthopedics (median “Agree”, IQR two scale items), increasing interest in MSK medicine (median “Agree”, IQR two scale items), improving confidence and ability to perform orthopedics-related physical exams (median “Agree”, IQR two scale items), fostering mentorships with residents and attendings (median “Agree”, IQR one scale item), and feeling more connected with the Department of Orthopedic Surgery and its residents (median “Agree”, IQR 1.25 scale items). The participants strongly recommended other medical schools to have an active orthopedic interest group (median “Strongly Agree”, IQR one scale item).
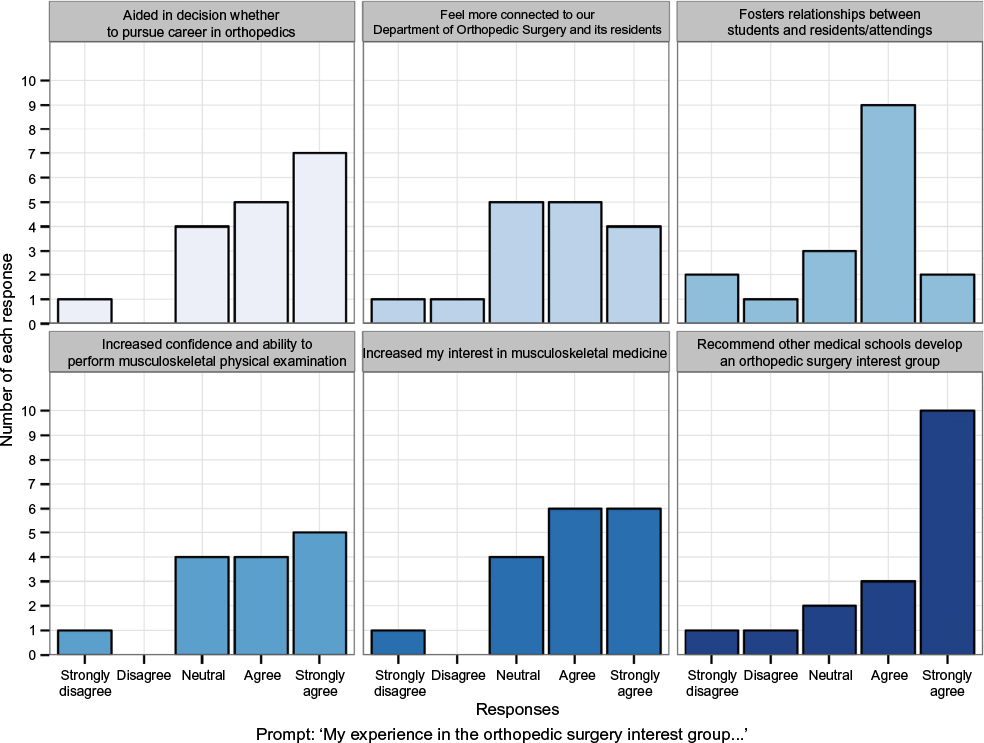 | Figure 5 Medical students’ experiences and attitudes toward OSSMIG. Abbreviation: OSSMIG, Orthopaedic Surgery and Sports Medicine Interest Group. |
Discussion
OSSMIG and MSK medicine education
OSSMIG has evolved over the past 8 years to provide supplementary education, opportunities, and support to UWSOM medical students. Membership increased to over 60 medical students annually, and targets both students interested in pursuing orthopedic surgery (67%) and primary care specialties (22%), but seeking a better understanding of MSK medicine. The group’s greatest impact appears to be the supplemental MSK education, resources, and experiences provided to the medical students outside of the standard UWSOM curriculum. This deficiency of subjective competence with MSK anatomy and basic trauma care was evident in the students surveyed prior to their involvement in OSSMIG (Figures 1 and 2). A lack of exposure to MSK medicine and orthopedics was also reported (Figure 3).
This trend appears to echo a nationwide concern regarding inadequacies in MSK teaching within the medical education landscape.3–7 The literature provides widespread evidence that medical students and residents may not be sufficiently prepared to perform accurate MSK workups and examinations.15–20 When evaluating medical students, Skelley et al observed only 19% assessed obtained a passing score on the competency assessment.18 Similarly, Schmale found that <50% of fourth year medical students at a single institution successfully demonstrated competency in MSK concepts.4
Though MSK complaints continue to be one of the most common reasons people seek medical care annually, a majority of these patients will not be evaluated by an orthopedic surgeon, but rather by primary care physicians (eg, family medicine, rehabilitation, internal medicine, and/or pediatrics).1,2 Deficiency in MSK knowledge appears to be present in these first-line physician fields.19,20 An MSK competency assessment created by Freedman and Bernstein revealed MSK-related knowledge deficiencies in primary care fields.6 When family practice, internal medicine, and pediatric faculty from a single hospital were assessed by Lynch et al, 64 physicians were not able to demonstrate adequate MSK knowledge.20
Although the initiation of an interest group is not necessarily the answer, it provides complementary instruction and unique experiences difficult to provide in a classroom. In orthopedics, dedicated exposure to MSK instruction can improve competence, even in undergraduates.21 Within OSSMIG, those members surveyed demonstrated a positive attitude toward OSSMIG in a number of areas. The year-end query of students’ subjective competency increased in both MSK anatomy (“Neutral” to “Agree”, p=0.007) and basic trauma care (“Disagree” to “Agree”, p=0.006) after involvement in the group’s events (Figures 1 and 2). They believed that OSSMIG increased their interest in MSK medicine and improved their confidence to perform a proficient MSK physical exam (Figure 5). The group was also impactful on students in deciding whether to pursue a career in orthopedics (Figure 5). Respondents reported that OSSMIG provided superior exposure to MSK medicine and the field of orthopedic surgery (Figure 3).
This improved exposure is likely a result of providing the ability for OSSMIG members to explore the “real world” of MSK medicine. During the preclinical years, these students have limited opportunities outside the classroom and sometimes limited exposure inside as well. In fact, the inclusion of MSK education within the medical school classroom curriculum has been associated with a 12% higher rate of application into orthopedic surgery residency programs.22 The Trauma Call experience is an example of one of the OSSMIG programs created to address this deficiency (Table 1). This program has become popular and jointly beneficial – for students, it offers a unique clinical experience and exposure to orthopedics; for the resident, it provides a valuable team member to assist during busy call shifts and the opportunity to teach. These experiences outside the classroom have been shown to help increase student interest.23–26 While the establishment and impact of orthopedic medical student interest groups was not found during review of the literature, general surgery interest groups at other institutions have been described and found to be positively received and demonstrate similar benefits. These general surgery interest groups exhibited positive supplemented surgical education, provided opportunities to improve procedural skills, and increased entrance rates into general surgery residency programs threefold.24,26
It appears that an interest group’s impact is highest when it is welcoming to all students, not just dedicated to assisting those pursuing a specific specialty. For an orthopedic interest group, focusing on unique MSK experiences and supportive MSK education in a supplementary fashion may help strengthen the MSK competence and confidence of those students involved in whatever career path they choose.
Limitations and future direction
This study has a number of limitations. The index surveys were issued as part of the group’s quality assurance and improvement processes and were reviewed retrospectively. These were not designed with a specific research question in mind and serial year data were not available for evaluation. Response rate was only 30%. Members were asked about their confidence in MSK medicine, but no competency assessment tool was administered. No comparison data were available from a control group that was not involved in OSSMIG, so correlations are difficult to infer.
The study was performed at a single institution with a large primary care focus, and thus, the study population may not be representative of other medical schools. Specifically, the MSK curriculum, required clerkships, and established support system can vary between schools. Thus, the impact of a dedicated orthopedic interest group may differ.
Lastly, the entire student body was not queried about the adequacy of MSK instruction. Since those surveyed were only OSSMIG members, responders may have bias toward feeling the instruction provided by the medical school curriculum was inadequate and, thus, actively sought out supplementary instruction.
Future studies will focus on assessing pre- and post-competency using an objective assessment measure and comparing this to a matched group of students who are not involved in the interest group. Additional assessments into the reasoning and motivations of the members who switched their focus from orthopedics to another specialty would be advantageous. A national query to investigate what other medical schools are doing would be helpful to see what is effective and if the findings in this and future studies are transferable.
Conclusion
Education in MSK medicine is inadequate within the USA medical school curricula. In concert with several studies evaluating medical school MSK education, it is recommended that medical schools provide more effective preparation and exposure to this field. This can be accomplished by increasing MSK instruction time, providing early clinical experiences, and integrating supplementary education by means of extracurricular interest groups. Since its inception 8 years ago, OSSMIG has been well received and has positively impacted UWSOM students through various interventions. By welcoming students’ interest in both primary care and surgery, it has expanded their exposure to MSK medicine and increased their subjective competence and confidence.
Maintaining strong student leadership and developing a relationship with the institution’s orthopedic surgery department is crucial to enhance the group’s function. An interest group that provides general MSK instruction to all-comers and supportive guidance to those applying to orthopedic surgery appears most effective. The development of similar interest groups at other schools is encouraged. OSSMIG will continue to refine, strengthen, and build its educational offerings, ultimately furthering student interest and success in orthopedic surgery and primary care MSK medicine.
Disclosure
The authors report no conflicts of interest in this work.
References
Yeh AC, Franko O, Day CS. Impact of clinical electives and residency interest on medical students’ education in musculoskeletal medicine. J Bone Joint Surg Am. 2008;90(2):307–315. | ||
The burden of musculoskeletal diseases in the United States. U.S. Bone and Joint Initiative. Available from: http://www.boneandjointburden.org. Accessed March 1, 2017. | ||
Houston TK, Connors RL, Cutler N, Nidiry MA. A primary care musculoskeletal clinic for residents: successes and sustainability. J Gen Intern Med. 2004;19:524–529. | ||
Schmale GA. More evidence of educational inadequacies in musculoskeletal medicine. Clin Orthop Relat Res. 2005;(437):251–259. | ||
Matzkin E, Smith EL, Freccero D, Richardson AB. Adequacy of education in musculoskeletal medicine. J Bone Joint Surg Am. 2005;87(2):310–314. | ||
Freedman KB, Bernstein J. The adequacy of medical school education in musculoskeletal medicine. J Bone Joint Surg Am. 1998;80(10):1421–1427. | ||
Day CS, Yeh AC, Franko O, Ramirez M, Krupat E. Musculoskeletal medicine: an assessment of the attitudes and knowledge of medical students at Harvard Medical School. Acad Med. 2007;82(5):452–457. | ||
Erzurum VZ, Obermeyer RJ, Fecher A, et al. What influences medical students’ choice of surgical careers. Surgery. 2000;128(2):253–256. | ||
Patel MS, Mowlds DS, Khalsa B, et al. Early intervention to promote medical student interest in surgery and the surgical subspecialties. J Surg Educ. 2013;70(1):81–86. | ||
Pinney SJ, Regan WD. Educating medical students about musculoskeletal problems. Are community needs reflected in the curricula of Canadian medical schools? J Bone Joint Surg Am. 2001;83-A(9):1317–1320. | ||
Tribble C, Kern J, Smith M, DuBose J. The establishment of a surgical interest society for medical students. Am J Surg. 2002;183(6):618–621. | ||
Johnson AL, Sharma J, Chinchilli VM, et al. Why do medical students choose orthopedics as a career? J Bone Joint Surg Am. 2012;94(11):e78. | ||
UW School of Medicine again tops U.S. News rankings. Available from: http://hsnewsbeat.uw.edu/story/uw-school-medicine-again-tops-us-news-rankings. Accessed March 1, 2017. | ||
Ramsey P. University of Washington School of Medicine 2015 report to the Washington State Medical Asssociation. Available from: http://engage.washington.edu/site/DocServer/2015_University_of_Washington_School_of_Medicine_Report_.pdf. Accessed March 1, 2017. | ||
Al-Nammari SS, James BK, Ramachandran M. The inadequacy of musculoskeletal knowledge after foundation training in the United Kingdom. J Bone Joint Surg Br. 2009;91(11):1413–1418. | ||
DiCaprio MR, Covey A, Bernstein J. Curricular requirements for musculoskeletal medicine in American medical schools. J Bone Joint Surg Am. 2003;85–A(3):565–567. | ||
Queally JM, Kiely PD, Shelly MJ, O’Daly BJ, O’Byrne JM, Masterson EL. Deficiencies in the education of musculoskeletal medicine in Ireland. Ir J Med Sci. 2008;177(2):99–105. | ||
Skelley NW, Tanaka MJ, Skelley LM, LaPorte DM. Medical student musculoskeletal education: an institutional survey. J Bone Joint Surg Am. 2012;94(19):e146(1–7). | ||
Comer GC, Liang E, Bishop JA. Lack of proficiency in musculoskeletal medicine among emergency medicine physicians. J Orthop Trauma. 2014;28(4):e85–e87. | ||
Lynch JR, Schmale GA, Schaad DC, Leopold SS. Important demographic variables impact the musculoskeletal knowledge and confidence of academic primary care physicians. J Bone Joint Surg Am. 2006;88(7):1589–1595. | ||
Kelly M, Bennett D, Bruce-Brand R, O’Flynn S, Fleming P. One week with the experts: a short course improves musculoskeletal undergraduate medical education. J Bone Joint Surg Am. 2014;96(5):e39. | ||
Bernstein J, Dicaprio MR, Mehta S. The relationship between required medical school instruction in musculoskeletal medicine and application rates to orthopedic surgery residency programs. J Bone Joint Surg Am. 2004;86–A(10):2335–2338. | ||
Gustafson JD, Rich NM, DeVries WC, McKay PL, Welling DR. A model for a medical school surgery interest group. Mil Med. 2012;177(12):1548–1550. | ||
Li R, Buxey K, Ashrafi A, Drummond KJ. Assessment of the role of a student-led surgical interest group in surgical education. J Surg Educ. 2013;70(1):55–58. | ||
Srinivasa S, Sapre NS. Nurturing of surgical careers by the Wellington Surgical Interest Club. ANZ J Surg. 2009;79(4):227–229. | ||
Salna M, Sia T, Curtis G, Leddy D, Widmann WD. Sustained increased entry of medical students into surgical careers: A student-led approach. J Surg Educ. 2016;73(1):151–156. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.