")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Increased risk of adverse drug events secondary to bevacizumab treatment in patients with advanced or metastatic breast cancer: a meta-analysis of randomized controlled trials
Received 10 August 2017
Accepted for publication 2 December 2017
Published 4 May 2018 Volume 2018:14 Pages 833—847
DOI https://doi.org/10.2147/TCRM.S148840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Sooyoung Shin,1,2 Yoojin Noh1
1College of Pharmacy, Ajou University, Yeongtong-gu, Suwon, Republic of Korea; 2Research Institute of Pharmaceutical Science and Technology (RIPST), Ajou University, Yeongtong-gu, Suwon, Republic of Korea
Background: Several clinical trials have shown an increased risk of hypertension with bevacizumab when added to chemotherapy in different types of malignancy; however, the risks of other significant adverse events besides hypertension, specifically in breast cancer, have not been completely elucidated. This study was conducted with the aim, primarily, to assess the overall incidence and risk of common toxicities associated with bevacizumab in patients with advanced or metastatic breast cancer and, secondarily, to descriptively review study results concerning a potential correlation between bevacizumab-induced hypertension and its efficacy for breast cancer treatment.
Methods: We carried out a meta-analysis of relevant randomized controlled trials (RCTs) identified from a database search (Cochrane Library and PubMed) and, additionally, by reviewing previous reviews and meta-analyses. Overall incidence rates, odds ratios (ORs), and 95% confidence intervals (CIs) were assessed with the random- or fixed-effect models, depending on the level of heterogeneity across the included trials. The primary clinical outcomes were high-grade adverse events commonly reported with bevacizumab therapy.
Results: We included 6,260 patients with advanced-stage breast cancer from 12 RCTs in the meta-analysis. Five types of high-grade (Grade 3 or 4) adverse drug events were identified as being correlated with bevacizumab treatment versus alternative treatment with statistical significance: hypertension (OR 5.67, 95% CI 3.02–10.65), proteinuria (OR 10.09, 95% CI 4.79–21.27), bleeding (OR 3.45, 95% CI 2.25–5.30), cardiac toxicity (OR 2.15, 95% CI 1.29–3.59), and neutropenic fever (OR 1.51, 95% CI 1.15–2.00). The prognostic value of bevacizumab-induced hypertension for its antitumor efficacy among patients with breast cancer remains controversial, with mixed results presented in the five retrospective studies that were identified from our additional literature search.
Conclusion: The addition of bevacizumab to anticancer therapy was associated with a significant increase in the risk of high-grade adverse events, including hypertension, proteinuria, bleeding, cardiac toxicity, and neutropenic fever among patients with advanced-stage breast cancer. Although several retrospective studies suggested a predictive importance of hypertension secondary to bevacizumab therapy, the role of elevated blood pressure as a prognostic biomarker for its antitumor efficacy remains controversial, and further prospective trials are required to confirm such a correlation.
Keywords: breast cancer, metastatic disease, bevacizumab, adverse events, hypertension, biomarker
Introduction
Breast cancer is the most frequently diagnosed malignancy in women, worldwide. Despite advances in screening and standard treatment, it is still considered one of the predominant causes of cancer-related death in women.1 The development of molecular-targeted therapy in recent years has allowed a significant improvement in survival among patients with metastatic breast cancer. Of the multiple pathophysiologic pathways involved in cancer progression and metastasis, acting against angiogenesis has been under extensive clinical exploration and has yielded a therapeutic target for novel agents commonly referred to as anti-vascular endothelial growth factor (anti-VEGF) inhibitors.2 Bevacizumab was the first anti-VEGF antibody that has been approved for cancer treatment and presently constitutes an important treatment modality for fighting cancer. With promising efficacy results from several clinical trials, its therapeutic horizon has been substantially expanded over the past decades. It is currently indicated for the treatment of multiple types of solid tumors, typically in advanced, relapsed, or metastatic stages. Furthermore, in 2008, the US Food and Drug Administration (FDA) had granted fast-track approval for bevacizumab plus paclitaxel as first-line combination therapy in patients with human epidermal growth factor receptor-2 (HER2)-negative metastatic breast cancer, based on the findings of the E2100 study by Miller et al.3 However, serious treatment-associated toxicities with no improvement in overall survival (OS) have been observed among patients treated with bevacizumab in clinical trials thereafter,4,5 which ultimately resulted in the withdrawal of its indication for metastatic breast cancer by the FDA in 2011. Although the clinical benefit of bevacizumab therapy for metastatic breast cancer has been proved controversial, many experts still regard it as a viable therapeutic strategy for combating advanced-stage cancer. In accordance with such a view, bevacizumab-based doublet chemotherapy continues to be recommended as first-line treatment for HER2-negative metastatic breast cancer – both in the 2017-updated National Comprehensive Cancer Network (NCCN) and European Medicines Agency (EMA) guidelines.
Several meta-analyses have revealed a significant increase in the risk of hypertension among patients treated with bevacizumab for different types of malignancy; however, the risks of other significant adverse events besides hypertension, specifically in patients with breast cancer, have yet to be investigated through meta-analysis. Previous meta-analyses primarily provided insights into patients with metastatic colorectal cancer6 or advanced non-small cell lung cancer (NSCLC)7 due to the large number of randomized controlled trials (RCTs) available for quantitative assessment. As new findings from more recent RCTs pertaining to metastatic breast cancer have been released and the number of patients enrolled in each clinical trial is generally limited, the magnitude of overall risk of encountering adverse events in bevacizumab-treated patients with metastatic breast cancer requires further assurance that also reflects updates from the latest trials. Additionally, although it has been suggested that bevacizumab-induced toxicity – most importantly hypertension – may be used as a prognostic biomarker for patients with cancer, this remains to be confirmed through prospective studies.
This study aimed to conduct a meta-analysis to evaluate the incidence and relative risk of adverse events associated with bevacizumab versus alternative therapy among patients with advanced or metastatic breast cancer. In addition, we descriptively review results from retrospective studies that investigated a potential correlation between bevacizumab-associated hypertension and the therapeutic response to the anticancer activity of the agent.
Methods
Data sources
We first conducted a literature search to identify RCTs of patients with advanced or metastatic breast cancer treated with bevacizumab that evaluated treatment-associated adverse events as safety endpoints. The Cochrane Library and PubMed were searched, without geographical and language restrictions, for articles published between October 2014 and July 2017 with the following pre-specified search strategy: “(bevacizumab OR Avastin) in all fields AND (breast OR breast cancer) in all fields AND (random* OR randomized) in title/abstract. Additional search filters applied were “humans” and “clinical trials”. Secondly, by reviewing previous meta-analyses, we also identified relevant RCTs that enrolled patients with metastatic breast cancer and that contained treatment-associated safety outcomes. The reference lists of collected studies and previous reviews were manually searched for other eligible RCTs that may not have been identified through the initial database search. To undertake the search with efficiency, an initial selection was carried out after screening the title and abstract, followed by a final selection after reviewing the full text of the articles in detail. This study was exempt from ethics committee review and informed consent from study subjects because this meta-analysis was conducted on the basis of published studies extracted from registries.
Study selection and data extraction
Two investigators (SS and YN) independently screened the article titles, abstracts, and, ultimately, full texts to identify RCTs suitable for the pre-established inclusion criteria, which were classified into four categories: 1) only Phase II and Phase III RCTs with placebo-controlled or active-control designs were eligible; 2) patients with advanced or metastatic breast cancer were included; 3) enrolled patients were randomly assigned to bevacizumab or placebo/control treatment in addition to concurrent anticancer therapy; and 4) outcomes must include event or incidence of safety endpoints, such as hypertension, proteinuria, and other toxicities commonly associated with bevacizumab, along with sample size for analysis. In cases where clinical trials with overlapping patient population were encountered, only the final study results were considered for inclusion. Phase II trials with a single-arm scheme and Phase I trials were all excluded due to the absence of comparison arms. Moreover, we carried out an additional search of ClinicalTrials.gov to capture ongoing clinical trials. Two investigators independently extracted data from the trials selected for the meta-analysis using a predefined summary format. Data on study characteristics (study design, control and concurrent treatment, follow-up duration, number of patients, and detailed bevacizumab regimens) and relevant clinical endpoints from the safety profile of each trial were extracted. Any discrepancies of data selection between the two investigators were resolved by consensus. Each safety event in the included studies has been graded one to four in accordance with the National Cancer Institute’s Common Terminology Criteria (CTC) for adverse events (http://ctep.cancer.gov), which defines an adverse event as any unusual clinical finding temporarily associated with medication use, although causality is not required.
Data analysis and statistical methods
For each trial, the incidence of patients experiencing different types of treatment-induced toxicity was calculated, and the 95% CIs were derived. The relative risk of each type of adverse drug events in patients assigned to the bevacizumab group versus those in the alternative therapy group was calculated. ORs and 95% CIs were calculated using the Mantel–Haenszel method, and either the fixed-effect or random-effect model was used depending on the level of heterogeneity among the RCTs included in our meta-analysis. We assessed statistical heterogeneity with chi-square statistics, and inconsistency was quantified with the I2 statistics. P<0.1 and I2>50% signified statistically significant heterogeneity across the included studies. To examine possible causes of heterogeneity, subgroup analyses were conducted by HER2 and hormone receptor status as well as relative bevacizumab dose intensity. A potential dose–event relationship was examined by classifying bevacizumab regimens in individual trials into either a low-dose treatment equivalent to a weekly dose of 2.5 mg/kg or a high-dose treatment equivalent to a weekly dose of 5 mg/kg. All P-values reported in this study are from two-sided tests, which were considered statistically significant when below 0.05. Funnel plots were examined to investigate the existence of publication bias. All statistical analyses were conducted using RevMan Version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) and R software version 3.2.1 (R Foundation for Statistical Computing; www.r-project.org).
Results
Search results and trial characteristics
The study flow diagram of this meta-analysis is displayed in Figure 1. From the database search, we retrieved 150 abstracts; following initial screening, we obtained 56 RCTs for subsequent detailed evaluation. After reviewing each study, 51 studies were excluded. The remaining five RCTs underwent full-text review, and all five studies ultimately fulfilled the inclusion criteria of the meta-analysis. Seven additional relevant RCTs3–5,8–11 were identified by reviewing previous meta-analyses (three meta-analyses incorporated multiple cancer types in their analysis,12–14 and one focused more on efficacy endpoints than safety events in patients with metastatic breast cancer15). Moreover, another RCT was returned through our search in ClinicalTrials.gov, but the study was determined ineligible for inclusion due to the single-arm trial design. In total, 12 RCTs3–5,8–11,16–20 with 6,260 patients were included in the quantitative analyses.
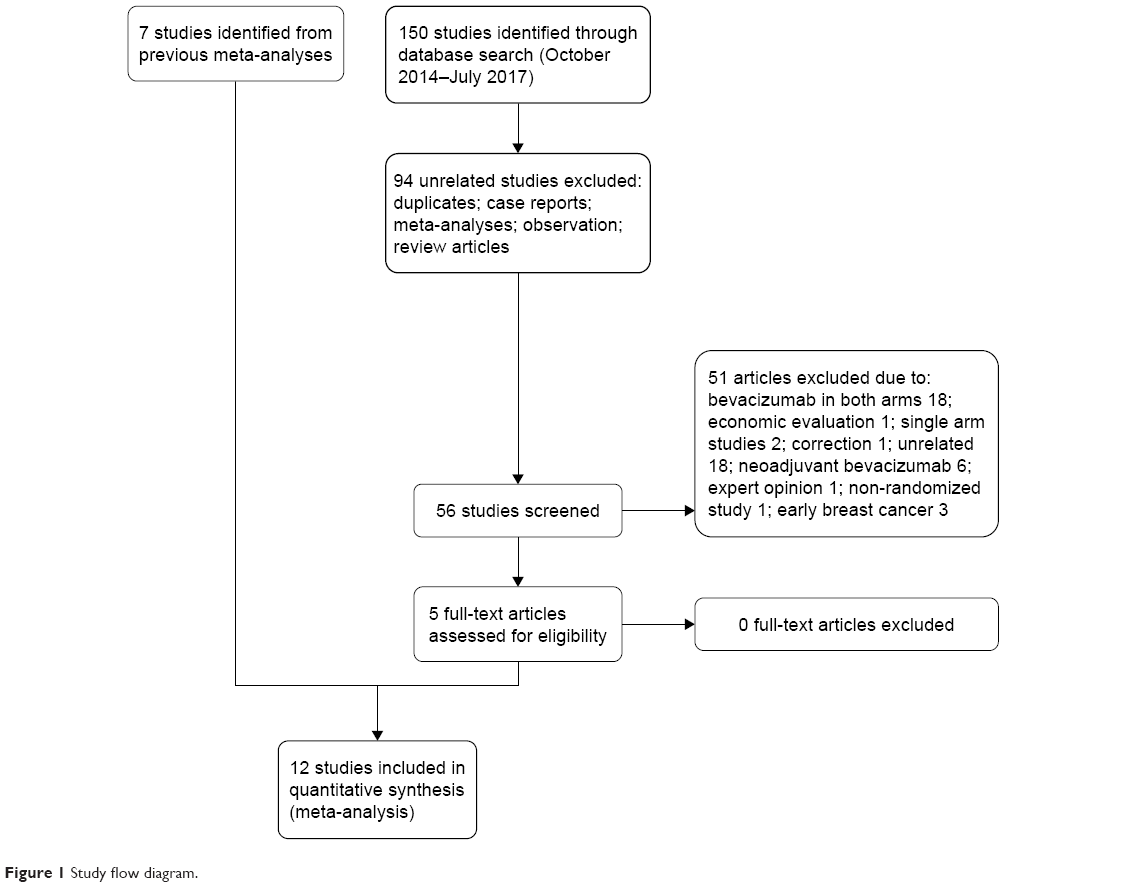 | Figure 1 Study flow diagram. |
A summary of the characteristics of the included studies is displayed in Table 1. The sample sizes of the 12 eligible trials ranged from 185 to 1,237 patients; of the total patient population included in this assessment, 3,621 were enrolled in the bevacizumab arm and 2,639 were in the alternative therapy arm. There were nine Phase III3–5,8,9,11,18–20 and three Phase II trials.10,16,17 Five RCTs were placebo-controlled and double-blinded,5,8,10,16,19 two other RCTs had placebo as controls,4,17 and the remainder of the RCTs had active controls.3,9,11,18,20 Nine RCTs intended to evaluate the therapeutic benefit of the addition of bevacizumab to standard therapy along with treatment-associated adverse events,3–5,8,9,11,18–20 and three RCTs aimed to investigate the treatment effect of new anticancer agents relative to bevacizumab or placebo when administered in combination with standard chemotherapy.10,16,17 The mean age of all subjects was over 50 years in all included studies, and most patients had baseline Eastern Cooperative Oncology Group (ECOG) performance status of between 0 and 1. In 10 trials, participants were predominantly classified as HER2-negative breast cancer (85%–100%),3–5,8,10,16–20 whereas in two trials the percentage of patients with HER2-negative cancer was as low as 8% or unknown.9,11 The majority of patients in 10 RCTs had hormone receptor-positive breast cancer.3–5,8–10,17–20 One trial enrolled only patients with triple-negative breast cancer.16 The meta-analysis was conducted in accordance with PRISMA guidelines.21 Overall, the risk of bias in the included RCTs was considered to be acceptable (Figure 2). The authors assessed there was a high risk of performance bias in six trials (59%)3,9–11,18,20 because of the open-label trial design. Three trials (25%)3,9,11 showed a non-random component in their randomized sequence generation and inadequate concealment of allocations; therefore, they were evaluated as having an unclear risk of selection bias.
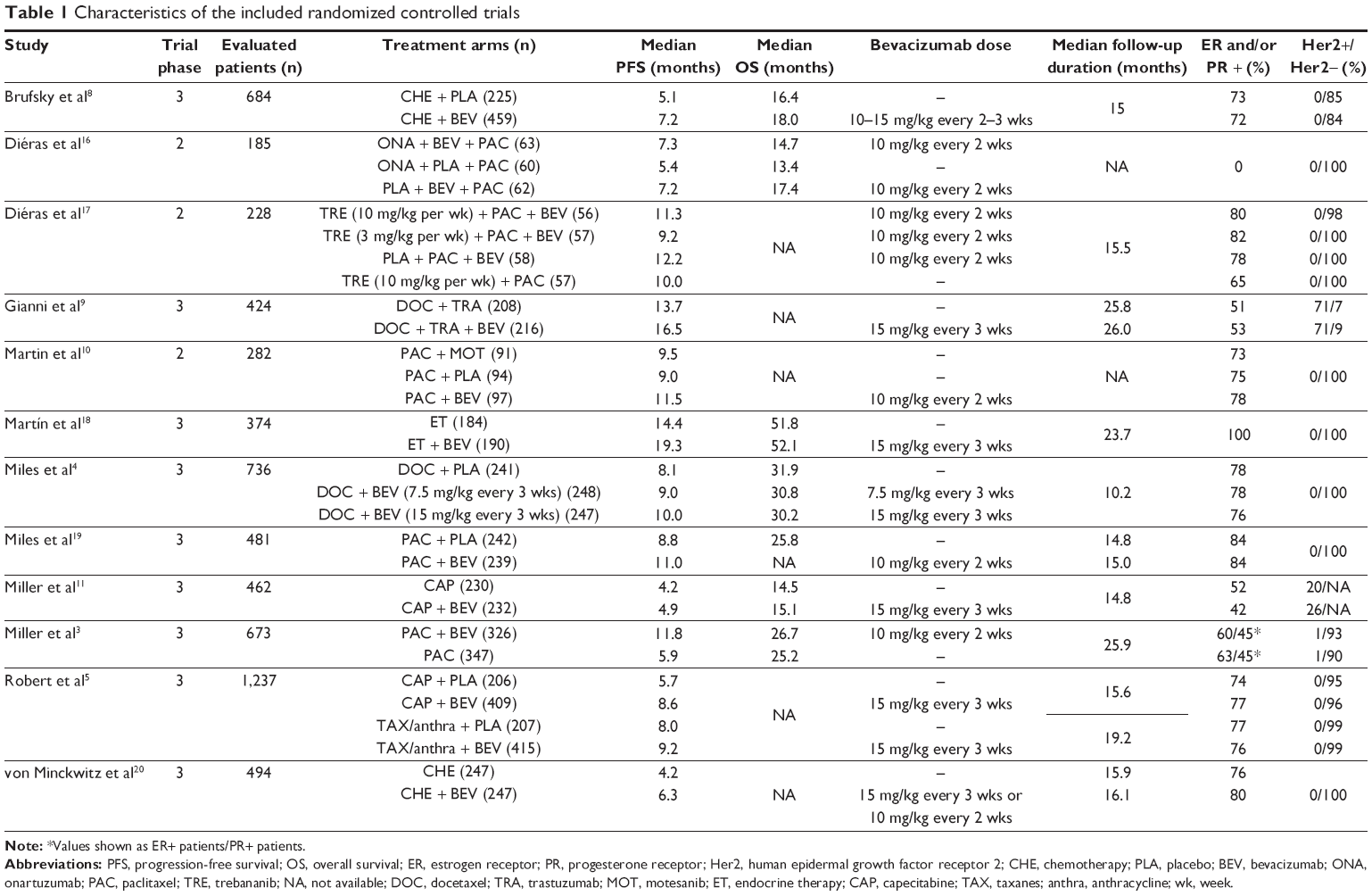 | Table 1 Characteristics of the included randomized controlled trials |
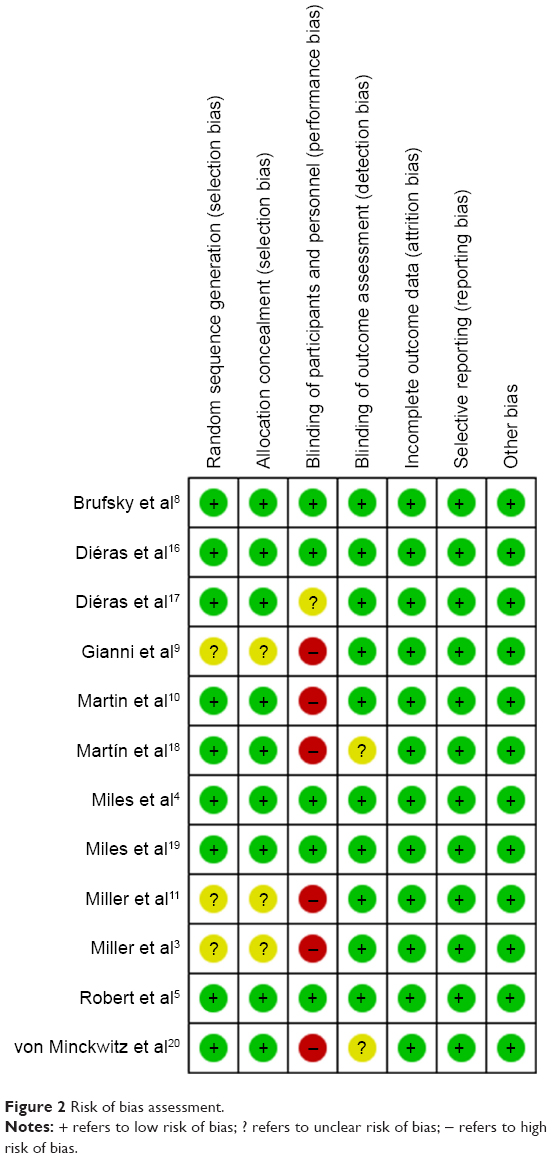 | Figure 2 Risk of bias assessment. |
The rates of treatment-associated toxicities from all RCTs were extracted and categorized for meta-analyses. In this analysis, we only presented the incidence and risk of high-grade (Grade 3 or 4) toxicities in bevacizumab-treated patients due to the following reasons: they are more serious adverse drug events that might have potentially led to life-threatening consequences and could have negatively affected therapy persistence; not all included trials reported on the frequency of Grade 1 or 2 adverse events or all-grade adverse events in their safety-profile section. Five types of adverse drug events were identified as being correlated with bevacizumab treatment with statistical significance: hypertension, proteinuria, bleeding, cardiac toxicity, and neutropenic fever. We obtained a symmetrical, inverted, funnel-shaped distribution with the funnel plot tests, indicating no evidence of significant publication bias was detected in the overall analyses. The risk of selection or information bias was minimized by selecting only prospective RCTs in the assessment.
Relative risk of hypertension
For hypertension, a total of 6,075 patients from 11 trials3–5,8–11,17–20 were included in the analysis. The incidence of Grade 3 or 4 hypertension ranged from 3% to 20%. The overall incidence of high-grade hypertension was 11% (95% CI 9%–15%) with the random-effect model (I2=85%, P<0.01). A meta-analysis of the OR for treatment-induced high-grade hypertension among bevacizumab-treated patients, compared to those who received alternative therapy, was conducted on the basis of the 11 RCTs. The pooled OR for experiencing Grade 3 or 4 hypertension was considerably higher in patients in the bevacizumab arm (5.67, 95% CI 3.02–10.65; P<0.00001; Figure 3). Due to heterogeneity among the included RCTs (I2=72%, P<0.00001), a random-effect model was applied. The pattern of treatment-associated hypertension risk appeared consistent among most trials, except for two comparison pairs in two RCTs4,10 that showed opposite trends.
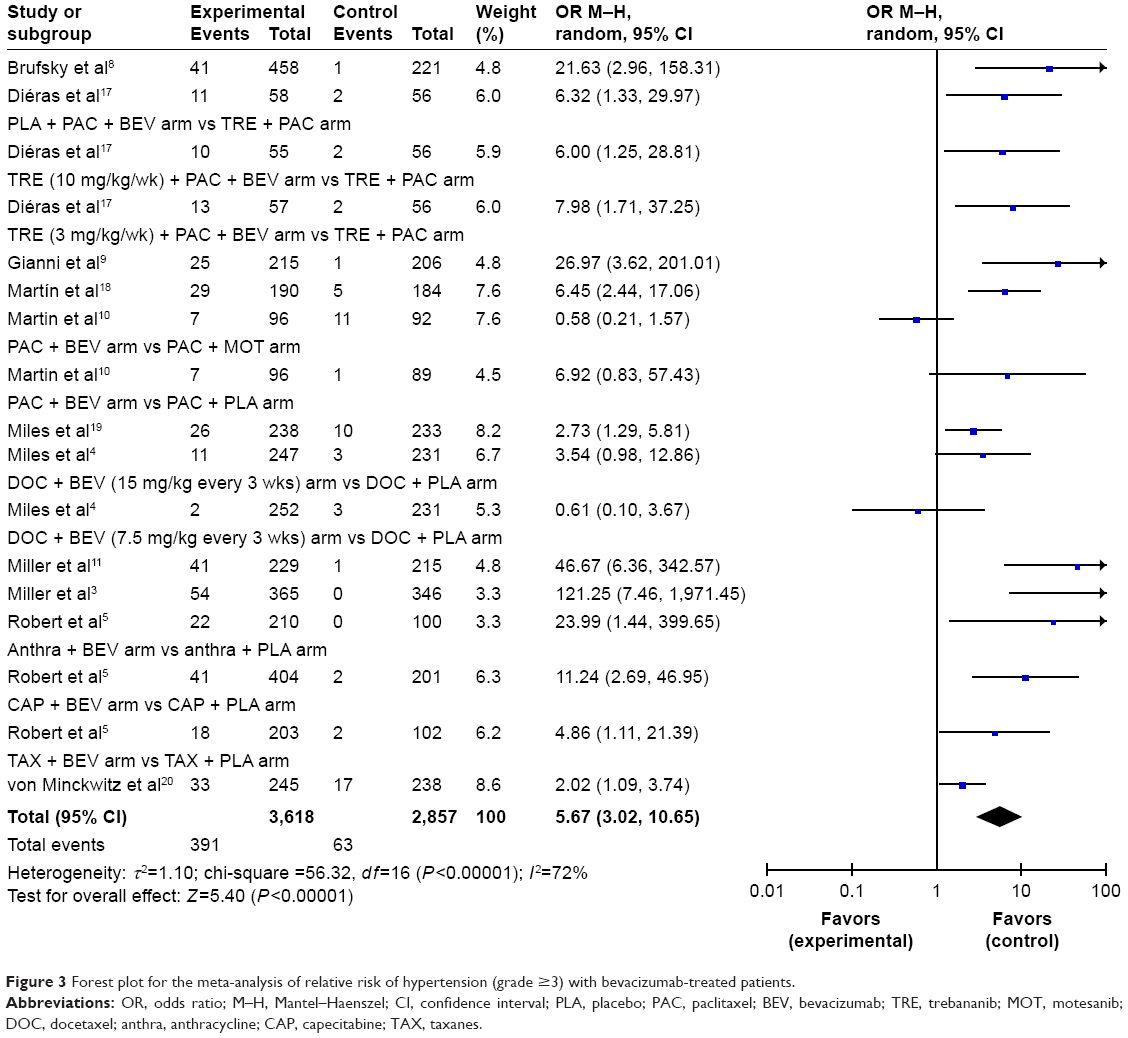 | Figure 3 Forest plot for the meta-analysis of relative risk of hypertension (grade ≥3) with bevacizumab-treated patients. |
For the subgroup analysis, we only included those trials that predominantly enrolled patients with HER2-negative breast cancer (two studies9,11 involving HER2-positive cases were excluded) and found that the overall OR and its statistical significance persisted (OR 4.52, 95% CI 2.47–8.29; P<0.00001). Additionally, we repeated the meta-analysis for sensitivity analysis after excluding the RCT by Miller et al3 – which was associated with the highest OR of 121.25 (95% CI 7.46–1971.45) – and found that the overall risk with statistical significance did not disappear (OR 4.98, 95% CI 2.76–9.00; P<0.00001). To assess a dose–event relationship, bevacizumab regimens in each trial were converted to a weekly dose and categorized into either high-dose bevacizumab (equivalent to 5 mg/kg per week) or low-dose bevacizumab (equivalent to 2.5 mg/kg per week). It was suggested that patients receiving high-dose bevacizumab may be at a higher risk of developing high-grade hypertension than patients treated at a lower dose; however, due to the limited number of RCTs carried out on low-dose bevacizumab, a dose-dependent relationship of bevacizumab on patient blood pressure cannot be confirmed with this analysis.
Relative risk of proteinuria
Concerning proteinuria, nine trials3–5,8,9,11,18–20 with a total of 5,565 patients were included in the analysis. The incidence of high-grade proteinuria ranged from 0.4% to 7%, and the overall incidence of high-grade proteinuria was 3% (95% CI 2%–4%) based on the random-effect model (I2=76%, P<0.01). The OR of high-grade proteinuria between the two treatment groups was calculated, and the pooled OR indicated that patients receiving bevacizumab had a significantly higher risk of experiencing high-grade proteinuria than those who received control treatment, with an OR of 10.09 (95% CI 4.79–21.27, P<0.00001) with the fixed-effect model (I2=0%, P=0.94; Figure 4). Although the incidence of high-grade proteinuria was not as high as that of high-grade hypertension, the magnitude of overall OR for experiencing high-grade proteinuria in patients receiving bevacizumab versus alternative therapy was substantially higher as compared to the OR of high-grade hypertension (10.09 vs 5.67). The greatest OR was obtained from the study by Martín et al18 which was designed to comprise two treatment arms of endocrine therapy plus bevacizumab versus endocrine therapy alone. For sensitivity analysis, we repeated the meta-analysis after excluding the aforementioned study and found that the overall risk with statistical significance did not disappear (OR 9.00, 95% CI 4.14–19.55; P<0.00001).
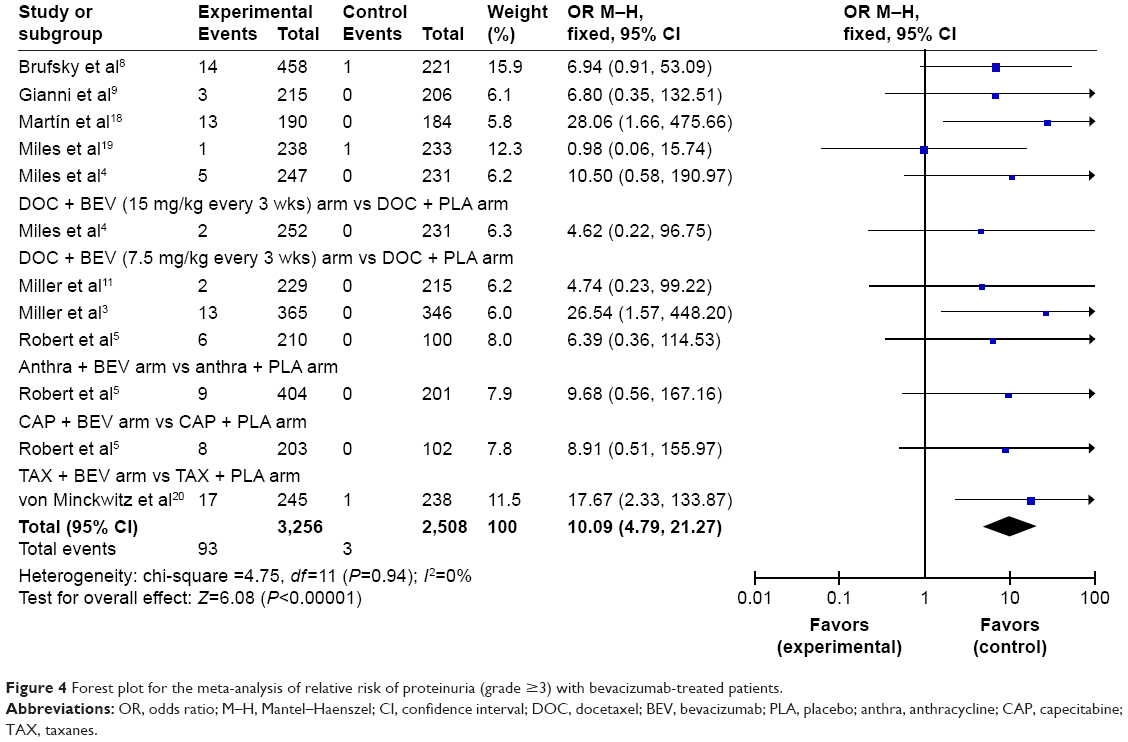 | Figure 4 Forest plot for the meta-analysis of relative risk of proteinuria (grade ≥3) with bevacizumab-treated patients. |
Relative risk of bleeding
Our analysis on bleeding events included 11 trials,3–5,8,9,11,16–20 with a total of 5,978 subjects. The incidence of high-grade bleeding events ranged from 0% to 52%, and the overall incidence of high-grade bleeding was 1% (95% CI 0%–6%) based on the random-effect model (I2=97%, P<0.01). We calculated the OR of high-grade bleeding between the treatment groups, and it revealed that patients undergoing bevacizumab treatment have a substantially increased risk to experience bleeding (OR 3.45; 95% CI 2.25–5.30; Figure 5). For this meta-analysis, the fixed-effect model was used, as no significant heterogeneity was detected among the included RCTs (I2=11%, P<0.00001). The ORs for two comparison pairs were not estimable due to the lack of corresponding events in both treatment arms; therefore, they were not included in the meta-analysis. Notably, most bleeding events (63%) occurred in one trial.16 For sensitivity analysis, we excluded the trial that showed a disproportionately high incidence rate from our meta-analysis and found that the overall risk with statistical significance still persisted (OR 2.07, 95% CI 1.14–3.79; P=0.02).
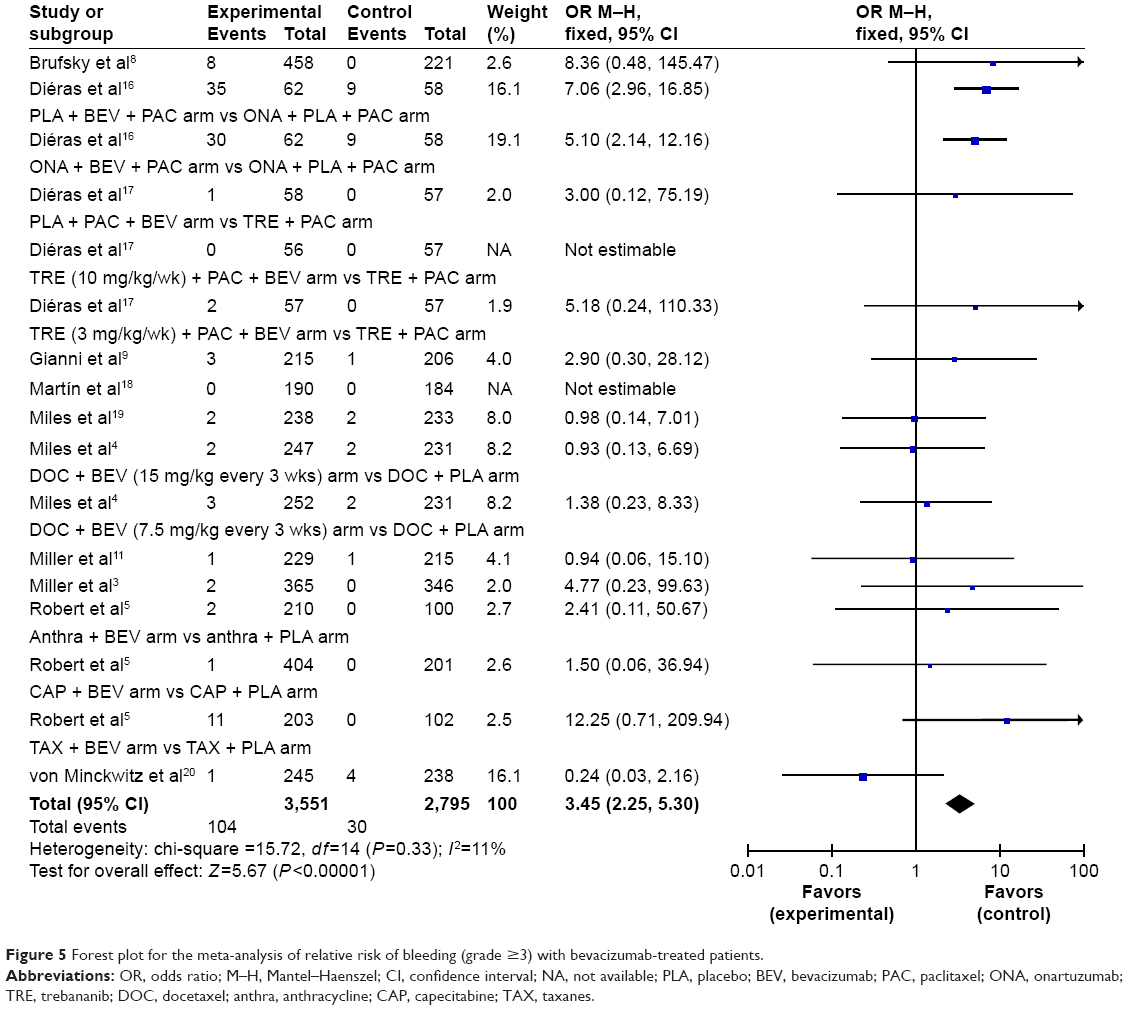 | Figure 5 Forest plot for the meta-analysis of relative risk of bleeding (grade ≥3) with bevacizumab-treated patients. |
Relative risk of cardiac events
The analysis for treatment-induced cardiac toxicity – including congestive heart failure, cardiomyopathy, and left ventricular dysfunction – was conducted on nine RCTs,3–5,8–11,19,20 with a total of 5,473 patients. The incidence of high-grade cardiac toxicity ranged from 0% to 5%, and the overall incidence of high-grade cardiac toxicity was 2% (95% CI 1%–3%) according to the random-effect model (I2=71%, P<0.01). A meta-analysis of the OR for treatment-induced high-grade cardiac toxicity among patients receiving bevacizumab, in comparison with those treated with alternative therapy, was carried out on these nine trials. The overall OR of high-grade cardiac events was 2.15 (95% CI 1.29–3.59, P=0.003) among patients receiving bevacizumab, which was calculated using the fixed-effect model (I2=0%, P=0.76; Figure 6). The ORs for two comparison pairs were not evaluable as there was no event that occurred in both treatment groups; therefore, they were not included in the meta-analysis.
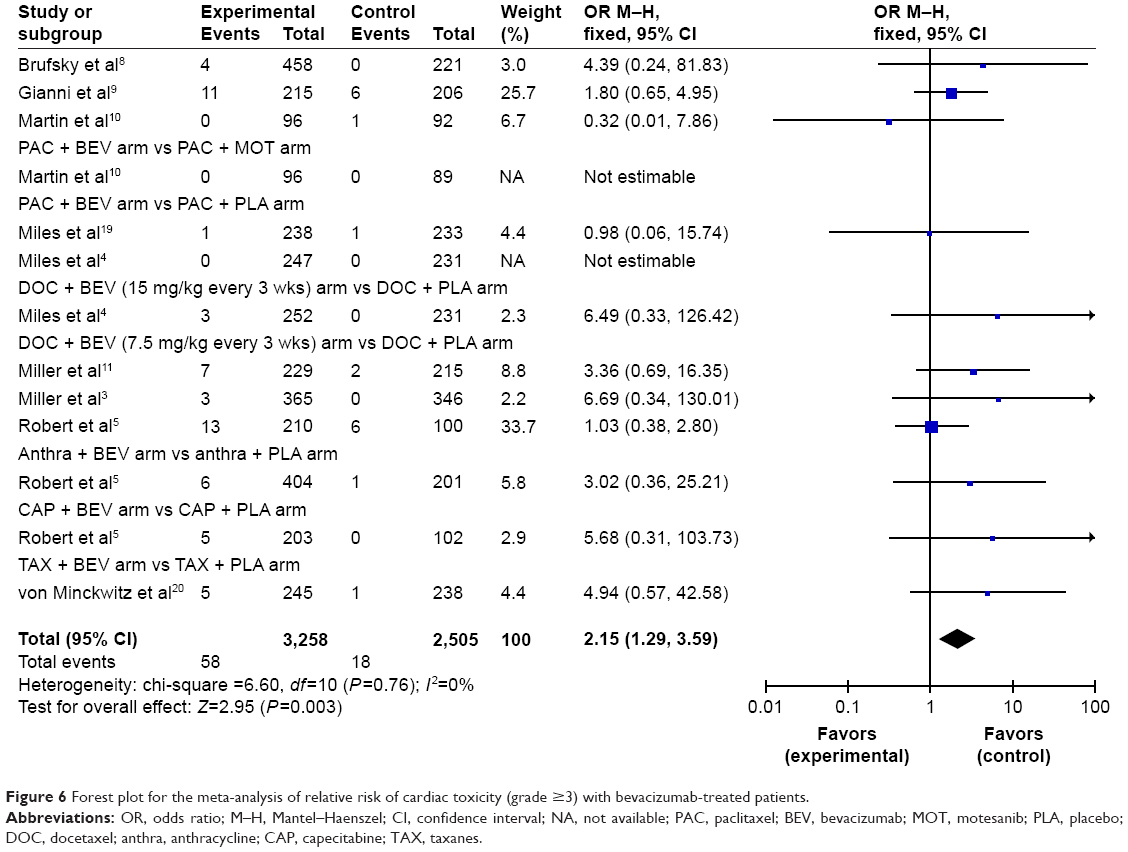 | Figure 6 Forest plot for the meta-analysis of relative risk of cardiac toxicity (grade ≥3) with bevacizumab-treated patients. |
Relative risk of neutropenic fever
Seven RCTs,3–5,8,9,19,20 with a total of 4,729 patients, were included for the analysis concerning neutropenic fever. The incidence of high-grade neutropenic fever ranged from 0.8% to 16%, and the overall incidence of high-grade neutropenic fever was 4% (95% CI 2%–8%) with the random-effect model (I2=95%, P<0.01). We conducted a meta-analysis to calculate the OR of high-grade neutropenic fever between bevacizumab and alternative treatments and found that bevacizumab was associated with a significantly increased risk of developing neutropenic fever in patients with advanced or metastatic breast cancer, with an OR of 1.51 (95% CI, P=0.003) with the fixed-effect model (I2=0%, P=0.48; Figure 7). The OR for one comparison pair was not evaluable owing to the lack of events in both treatment arms; therefore, those studies were not incorporated in the estimation of overall OR.
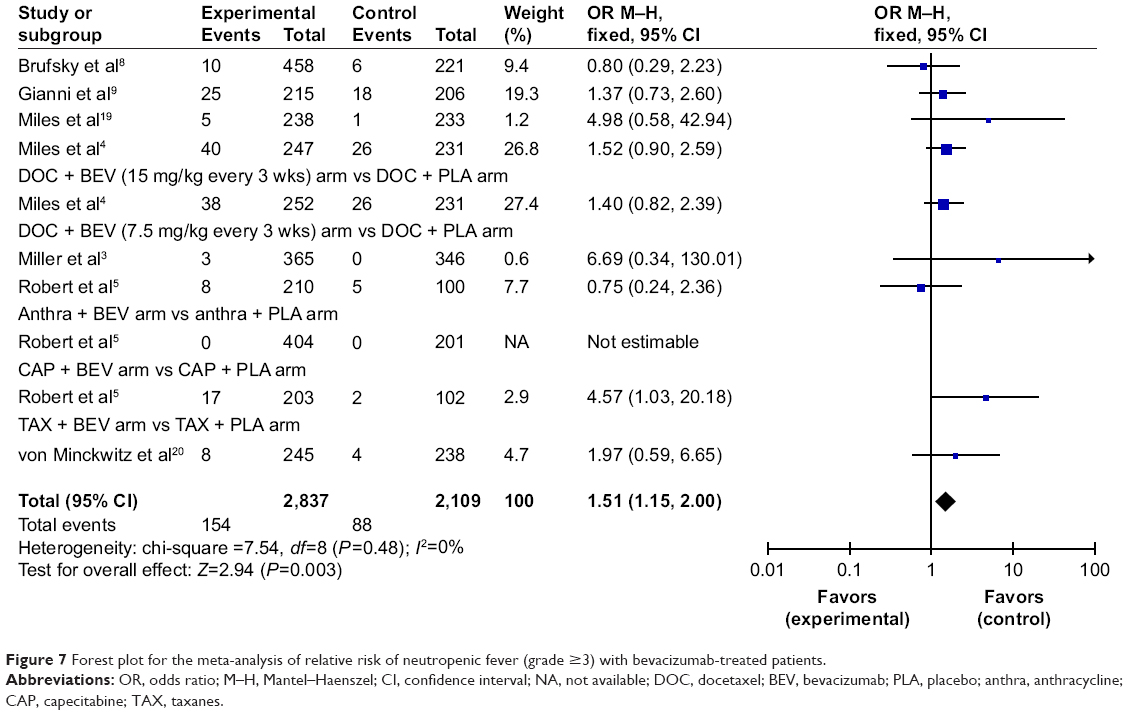 | Figure 7 Forest plot for the meta-analysis of relative risk of neutropenic fever (grade ≥3) with bevacizumab-treated patients. |
Previous study results on hypertension as a prognostic marker for bevacizumab efficacy
Through our additional literature search, we identified five relevant articles22–26 that investigated the potential link between bevacizumab efficacy and hypertension in patients with breast cancer. Important findings from each study are summarized in Table 2. In a genotyping study conducted as a follow-up to the parent E2100 Trial,3 a superior median OS among patients with high-grade hypertension was detected as compared with those with no hypertension (38.7 vs 25.3 months; P=0.002).22 Similarly, a retrospective matched-pair study in 2014 reported that patients with high-grade hypertension had superior survival outcomes in progression-free survival (PFS) times (13.7 vs 6.6 months, HR 0.34, 95% CI 0.23–0.49; P<0.001) as well as in 2-year OS (78% vs 30%, HR 0.20, 95% CI 0.12–0.35; P<0.001).23 Notably, findings from a comprehensive analysis of seven previously conducted Phase III trials were contrary: the randomized, double-blind, placebo-controlled, phase III (RIBBON-1) trial showed a sign of improvement in OS alone with borderline statistical significance (HR 0.62; P=0.0505), whereas the randomized, double-blind, phase III study Avastin And Docetaxel (AVADO) trial revealed no association between hypertension and any of the survival outcomes.24 Furthermore, a study on the subset of patients enrolled in the ATHENA trial reported that no correlation was detected between hypertension and OS.26 Furthermore, in a retrospective cohort study of 2015, hypertension was not predictive of OS in bevacizumab-treated patients with breast cancer.25
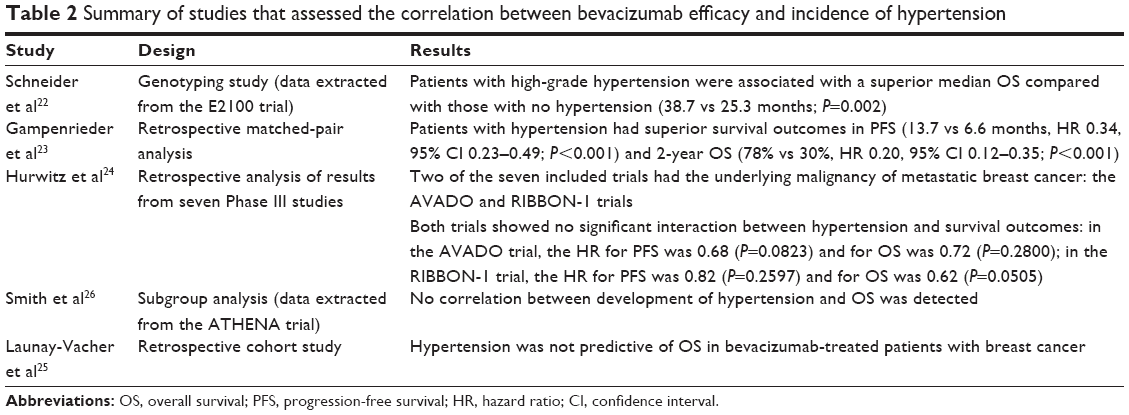 | Table 2 Summary of studies that assessed the correlation between bevacizumab efficacy and incidence of hypertension |
Discussion
The development of antitumor agents selectively targeting the VEGF-promoted angiogenesis pathway has been of paramount interest in cancer research. Bevacizumab – an anti-VEGF antibody – has been validated by extensive clinical investigation as a viable treatment modality for advanced-stage malignancies, including colorectal cancer, NSCLC, renal cancer, glioblastoma, ovarian cancer, and melanoma.27–30 Moreover, in 2008, the FDA gave accelerated approval to bevacizumab for metastatic breast cancer, taking into account the findings from a Phase III trial (E2100) that reported a significant improvement in PFS and objective response rate among patients treated with bevacizumab plus weekly paclitaxel as compared with those treated with paclitaxel alone.3 As its clinical use expanded, however, bevacizumab-induced toxicity reports increased and the lack of therapeutic benefits in terms of OS precipitated controversy over the agent’s indication for metastatic breast cancer.3–5,8,9 In 2011, the FDA ultimately revoked its approval of the indication for the anti-VEGF antibody because recent two Phase III trials4,5 failed to reproduce the efficacy findings of the preceding E2100 trial3 that had originally contributed to the agent attaining the initial licensing for the disease treatment. Although its use has declined since then, clinical practice guidelines still recommend bevacizumab-based chemotherapy as a first-line option for the treatment of metastatic breast cancer. Bevacizumab plus paclitaxel or capecitabine combination therapy is an EMA-approved treatment option for metastatic breast cancer. More importantly, the expert panel of the NCCN recently decided to maintain the current recommendation on the use of bevacizumab plus paclitaxel for HER2-negative metastatic breast cancer in the 2017-updated NCCN guidelines. Moreover, Li et al reported that bevacizumab-based doublet chemotherapy significantly increased PFS in patients with metastatic breast cancer in their 2015 meta-analysis.15 The addition of bevacizumab to chemotherapy appeared tolerable in multiple cancer trials31,32 and, as we have a better understanding of the benefits and risks of bevacizumab, establishing clinical strategies to identify patients who would derive the most therapeutic effects from the anti-VEGF therapy is urgently required.
In this meta-analysis, major adverse events whose risk significantly increased with bevacizumab versus alternative therapy were identified as high-grade toxicities of hypertension, proteinuria, bleeding, cardiac events, and neutropenic fever. The relative risk of the respective high-grade toxicities in bevacizumab-treated patients was highest with proteinuria (OR 10.09, 95% CI 4.79–21.27), followed by hypertension (OR 5.67, 95% CI 3.02–10.65). Notably, high-grade hypertension revealed the highest incidence rate (11%, 95% CI 9%–15%; P<0.01), whereas the incidence rate of proteinuria was merely at 3% (95% CI 2%–4%; P<0.01). Previous meta-analyses conducted thus far included RCTs that enrolled patients with multiple types of malignancy12–14 or those that exclusively enrolled patients with metastatic colorectal cancer alone6 or advanced NSCLC alone.7 These studies typically analyzed the risk of hypertension alone or, rarely, hypertension plus proteinuria in bevacizumab-treated patients with cancer. Our findings with regard hypertension and proteinuria events secondary to bevacizumab use were comparable to those of previous meta-analyses. Interestingly, a meta-analysis by An et al suggested a dose-dependent relationship between hypertension events and exposure to bevacizumab: the relative risks of hypertension in patients with cancer who were treated with bevacizumab at 5 and 2.5 mg/kg per week were 7.17 (95% CI of 3.91–13.13) and 4.11 (95% CI of 2.49–6.78), respectively.12 In our assessment of hypertension risk exclusively among patients with breast cancer, it was not possible to confirm the relationship between dose intensity and frequency of adverse events because of the limited number of trials containing the low-dose bevacizumab intervention that were available for our quantitative analysis. Further, An et al suggested differential risks of hypertension among patients receiving bevacizumab, depending on the type of underlying cancer: patients with breast cancer receiving bevacizumab at 5 mg/kg per week had a highest risk of developing severe hypertension among patients with different types of cancer, with a relative risk of 18.83 (95% CI 2.28–83.15).12 However, of the 19 RCTs included in their meta-analysis, only three trials3,4,11 were on metastatic breast cancer. Although there have been numerous RCTs that investigated the efficacy and safety endpoints of bevacizumab treatment in patients with cancer, to our knowledge no meta-analysis has been conducted thus far with the pre-specified goal to obtain a better understanding toward bevacizumab-induced safety outcomes encompassing other major toxicities besides hypertension, exclusively among patients with advanced-stage breast cancer.
Many of the bevacizumab-associated toxicities are not commonly observed with conventional chemotherapy targeting deoxyribonucleic acid or ribonucleic acid. It has been hypothesized that cardiovascular toxicities of bevacizumab – most importantly hypertension owing to its high incidence rate and prognostic significance among patients encountering such event – are potentially attributable to its unique anti-angiogenetic mechanism of action.27 If inadequately controlled, hypertensive episodes due to bevacizumab may lead to negative consequences, such as treatment discontinuation, serious cardiovascular events, and even patient mortality. Therefore, blood pressure has long been considered the key index for the safe use of the anti-VEGF therapy. The mechanism underlying bevacizumab-triggered hypertension has yet to be thoroughly clarified, but there are several speculations. Inhibition of VEGF due to bevacizumab administration may lead to suppressed synthesis of the vasodilator nitric oxide in endothelial cells, leading to increased vasoconstriction and vascular tone, reduced renal excretion of sodium ion, and, ultimately, elevated blood pressure.13,33 Another possible pathogenesis underlying the hypertensive phenomenon may be related to the extinction of microvascularity: inhibition of VEGF signaling may increase vascular resistance by preventing neovascularization.34 Additionally, an impaired development of the renal glomerulus and elevated intraglomerular pressure secondary to anti-VEGF therapy may contribute to elevated blood pressure.35 Furthermore, recent studies have suggested that anti-VEGF antibody therapy may cause a pre-eclampsia-like phenomenon associated with VEGF dysregulation.36 All of these influences may contribute to increased blood pressure in bevacizumab-treated patients with cancer.
To minimize the risk of serious cardiovascular toxicities, patients on bevacizumab therapy should be under close monitoring for clinical manifestations of common adverse events – most importantly, hypertension. On the bright side, its effects on blood pressure are characterized as being reversible and generally manageable with mainstream antihypertensive strategies.32 It appears that elevated blood pressure secondary to bevacizumab returns to baseline values once the agent is withdrawn.31 Clinicians may need to restrict eligibility for bevacizumab treatment to those patients with controlled blood pressure at baseline before initiating the therapy. Despite the high incidence and risk of hypertension in bevacizumab-treated patients, there are no evidence-based guidelines providing standard measures to manage anti-VEGF-induced hypertension. The British Columbia Cancer Agency indeed recommended thiazide diuretics to be employed as first-line treatment and angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) as second-line agents.27 However, according to the findings from a large number of clinical trials, the antihypertensive benefits appear largely independent of the agents chosen: any of the standard antihypertensive measures, such as thiazide diuretics, beta-blockers, ACE inhibitors, and ARBs, can be employed as monotherapy or in combination to adequately control such treatment-induced hypertension and significantly lower the risk of cardiovascular adverse consequences.37–39 Thus, clinicians may make a clinical judgment by using their expertise and professional discretion in selecting the best therapeutic option for blood pressure control in individual patients.
Hypertension is currently under extensive investigation as a predictive biomarker for the antitumor effectiveness of bevacizumab. To decrease the number needed to treat to attain more therapeutic benefits from bevacizumab while preventing adverse drug events, establishing a prognostic biomarker, which provides preferably a convenient and practical means to employ in clinical practice, for the agent is urgently needed. Many potential biomarkers, including histologic and genetic factors, have undergone extensive clinical investigation, but none are yet validated as a reliable prognostic measure for clinical use.9,22,40,41 The manifestations of hypertension secondary to bevacizumab may signal better clinical responses to the VEGF inhibition therapy. In contrast, absence of blood pressure increase may indicate that a prompt change of therapeutic modality would be beneficial for patient outcomes. Furthermore, titrating bevacizumab dose until blood pressure rises to certain levels in individual patients may be considered to achieve better anticancer activity and improved survival outcomes.42 A positive correlation between treatment-related elevations in blood pressure and therapeutic response to the anti-VEGF agent has been suggested in a series of retrospective studies concerning advanced-stage malignancies of colorectal cancer, NSCLC, and ovarian cancer.6,43–47 With regard to breast cancer, mixed results have been presented in retrospective analyses: some suggested a significant prognostic value of hypertension for bevacizumab efficacy22,23 whereas others showed no significant association between the two.24–26 However, currently available studies are generally retrospective analyses of preexisting health care data or a subset of data from previously conducted clinical trials. Because of the retrospective design, accurate detection of new-onset hypertension could have been challenging because blood pressure measurements were generally done on treatment days only. Therefore, they are not optimally designed to address the following question: can treatment-induced hypertension be used as a simple biomarker for the antitumor efficacy of bevacizumab? The question still remains of paramount clinical importance in cancer research. To date, findings from prior retrospective studies have not been confirmed as yet in well-designed prospective randomized trials with pre-established efficacy and safety endpoints that are specifically designed with the aim to determine the predictive value of hypertension for bevacizumab efficacy.
This meta-analysis has several limitations. First, adverse events in the included RCTs were recorded in accordance to different versions of the CTC for adverse events. Although these versions are generally similar in grading system, discrepancies in the definition of toxicities among studies may have existed. Second, clinical trials evaluating antiangiogenic agents have restricted inclusion criteria for patient enrollment. Only those patients with controlled blood pressure at baseline were eligible for individual trials; therefore, the patients population incorporated in our analysis may not represent real-world patients. Third, an open-label trial design employed in some trials included in our analysis may have increased the risk of performance and detection bias. Lastly, the composition of treatment arms varied, which might have contributed to the clinical heterogeneity across the included trials.
Conclusion
The addition of bevacizumab to anticancer therapy was associated with a significant surge in the risk of high-grade adverse events, including hypertension, proteinuria, bleeding, cardiac toxicity, and neutropenic fever, among patients with advanced or metastatic breast cancer. Close monitoring and effective management of treatment-induced toxicities – most importantly, hypertension – is crucial for those patients receiving bevacizumab in order to prevent significant anti-VEGF-induced adverse consequences. Although several retrospective analyses suggested a prognostic importance of elevated blood pressure secondary to bevacizumab therapy, the role of hypertension as a predictive biomarker for its antitumor efficacy remains controversial, and further prospective clinical trials are urgently needed to confirm such a correlation.
Acknowledgments
This study was supported by the Ajou University Research Fund (grant number S-2017-G0001-00211) and by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Science, ICT & Future Planning (grant number 2017R1C1B5015912).
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30. | ||
Sánchez-Muñoz A, Pérez-Ruiz E, Jiménez B, et al. Targeted therapy of metastatic breast cancer. Clin Transl Oncol. 2009;11(10):643–650. | ||
Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med. 2007;357(26):2666–2676. | ||
Miles DW, Chan A, Dirix LY, et al. Phase III study of bevacizumab plus docetaxel compared with placebo plus docetaxel for the first-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol. 2010;28(20):3239–3247. | ||
Robert NJ, Diéras V, Glaspy J, et al. RIBBON-1: randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or without bevacizumab for first-line treatment of human epidermal growth factor receptor 2-negative, locally recurrent or metastatic breast cancer. J Clin Oncol. 2011;29(10):1252–1260. | ||
Cai J, Ma H, Huang F, et al. Correlation of bevacizumab-induced hypertension and outcomes of metastatic colorectal cancer patients treated with bevacizumab: a systematic review and meta-analysis. World J Surg Oncol. 2013;11:306. | ||
Chen J, Lu Y, Zheng Y. Incidence and risk of hypertension with bevacizumab in non-small-cell lung cancer patients: a meta-analysis of randomized controlled trials. Drug Des Devel Ther. 2015;9:4751–4760. | ||
Brufsky AM, Hurvitz S, Perez E, et al. RIBBON-2: a randomized, double-blind, placebo-controlled, phase III trial evaluating the efficacy and safety of bevacizumab in combination with chemotherapy for second-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol. 2011;29(32):4286–4293. | ||
Gianni L, Romieu GH, Lichinitser M, et al. AVEREL: a randomized phase III trial evaluating bevacizumab in combination with docetaxel and trastuzumab as first-line therapy for HER2-positive locally recurrent/metastatic breast cancer. J Clin Oncol. 2013;31(14):1719–1725. | ||
Martin M, Roche H, Pinter T, et al; TRIO 010 investigators. Motesanib, or open-label bevacizumab, in combination with paclitaxel, as first-line treatment for HER2-negative locally recurrent or metastatic breast cancer: a phase 2, randomised, double-blind, placebo-controlled study. Lancet Oncol. 2011;12(4):369–376. | ||
Miller KD, Chap LI, Holmes FA, et al. Randomized phase III trial of capecitabine compared with bevacizumab plus capecitabine in patients with previously treated metastatic breast cancer. J Clin Oncol. 2005;23(4):792–799. | ||
An MM, Zou Z, Shen H, et al. Incidence and risk of significantly raised blood pressure in cancer patients treated with bevacizumab: an updated meta-analysis. Eur J Clin Pharmacol. 2010;66(8):813–821. | ||
Zhu X, Wu S, Dahut WL, Parikh CR. Risks of proteinuria and hypertension with bevacizumab, an antibody against vascular endothelial growth factor: systematic review and meta-analysis. Am J Kidney Dis. 2007;49(2):186–193. | ||
Ranpura V, Pulipati B, Chu D, Zhu X, Wu S. Increased risk of high-grade hypertension with bevacizumab in cancer patients: a meta-analysis. Am J Hypertens. 2010;23(5):460–468. | ||
Li Q, Yan H, Zhao P, Yang Y, Cao B. Efficacy and safety of bevacizumab combined with chemotherapy for managing metastatic breast cancer: a meta-analysis of randomized controlled trials. Sci Rep. 2015;5:15746. | ||
Diéras V, Campone M, Yardley DA, et al. Randomized, phase II, placebo-controlled trial of onartuzumab and/or bevacizumab in combination with weekly paclitaxel in patients with metastatic triple-negative breast cancer. Ann Oncol. 2015;26(9):1904–1910. | ||
Diéras V, Wildiers H, Jassem J, et al. Trebananib (AMG 386) plus weekly paclitaxel with or without bevacizumab as first-line therapy for HER2-negative locally recurrent or metastatic breast cancer: a phase 2 randomized study. Breast. 2015;24(3):182–190. | ||
Martín M, Loibl S, von Minckwitz G, et al. Phase III trial evaluating the addition of bevacizumab to endocrine therapy as first-line treatment for advanced breast cancer: the letrozole/fulvestrant and avastin (LEA) study. J Clin Oncol. 2015;33(9):1045–1052. | ||
Miles D, Cameron D, Bondarenko I, et al. Bevacizumab plus paclitaxel versus placebo plus paclitaxel as first-line therapy for HER2-negative metastatic breast cancer (MERiDiAN): a double-blind placebo-controlled randomised phase III trial with prospective biomarker evaluation. Eur J Cancer. 2017;70:146–155. | ||
von Minckwitz G, Puglisi F, Cortes J, et al. Bevacizumab plus chemotherapy versus chemotherapy alone as second-line treatment for patients with HER2-negative locally recurrent or metastatic breast cancer after first-line treatment with bevacizumab plus chemotherapy (TANIA): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1269–1278. | ||
Higgins JP, Altman DG, Gøtzsche PC, et al; Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. | ||
Schneider BP, Wang M, Radovich M, et al; ECOG 2100. Association of vascular endothelial growth factor and vascular endothelial growth factor receptor-2 genetic polymorphisms with outcome in a trial of paclitaxel compared with paclitaxel plus bevacizumab in advanced breast cancer: ECOG 2100. J Clin Oncol. 2008;26(28):4672–4678. | ||
Gampenrieder SP, Romeder F, Muß C, et al. Hypertension as a predictive marker for bevacizumab in metastatic breast cancer: results from a retrospective matched-pair analysis. Anticancer Res. 2014;34(1):227–233. | ||
Hurwitz HI, Douglas PS, Middleton JP, et al. Analysis of early hypertension and clinical outcome with bevacizumab: results from seven phase III studies. Oncologist. 2013;18(3):273–280. | ||
Launay-Vacher V, Janus N, Beuzeboc P, et al. Tolérance rénovasculaire du bévacizumab dans le cancer du sein. Valeur pronostique de l’hypertension et de la protéinurie. [Renovascular safety of bevacizumab in breast cancer patients. The prognostic value of hypertension and proteinuria]. Bull Cancer. 2015;102(11):906–914. French [with English abstract]. | ||
Smith I, Pierga JY, Biganzoli L, et al. Final overall survival results and effect of prolonged (≥1 year) first-line bevacizumab-containing therapy for metastatic breast cancer in the ATHENA trial. Breast Cancer Res Treat. 2011;130(1):133–143. | ||
Syrigos KN, Karapanagiotou E, Boura P, Manegold C, Harrington K. Bevacizumab-induced hypertension: pathogenesis and management. BioDrugs. 2011;25(3):159–169. | ||
Giantonio BJ, Catalano PJ, Meropol NJ, et al; Eastern Cooperative Oncology Group Study E3200. Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200. J Clin Oncol. 2007;25(12):1539–1544. | ||
Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–2342. | ||
Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med. 2006;355(24):2542–2550. | ||
Yang JC, Haworth L, Sherry RM, et al. A randomized trial of bevacizumab, an anti-vascular endothelial growth factor antibody, for metastatic renal cancer. N Engl J Med. 2003;349(5):427–434. | ||
Hamilton EP, Blackwell KL. Safety of bevacizumab in patients with metastatic breast cancer. Oncology. 2011;80(5–6):314–325. | ||
Shen BQ, Lee DY, Zioncheck TF. Vascular endothelial growth factor governs endothelial nitric-oxide synthase expression via a KDR/Flk-1 receptor and a protein kinase C signaling pathway. J Biol Chem. 1999;274(46):33057–33063. | ||
Steeghs N, Gelderblom H, Roodt JO, et al. Hypertension and rarefaction during treatment with telatinib, a small molecule angiogenesis inhibitor. Clin Cancer Res. 2008;14(11):3470–3476. | ||
Izzedine H, Rixe O, Billemont B, Baumelou A, Deray G. Angiogenesis inhibitor therapies: focus on kidney toxicity and hypertension. Am J Kidney Dis. 2007;50(2):203–218. | ||
Sugimoto H, Hamano Y, Charytan D, et al. Neutralization of circulating vascular endothelial growth factor (VEGF) by anti-VEGF antibodies and soluble VEGF receptor 1 (sFlt-1) induces proteinuria. J Biol Chem. 2003;278(15):12605–12608. | ||
Izzedine H, Ederhy S, Goldwasser F, et al. Management of hypertension in angiogenesis inhibitor-treated patients. Ann Oncol. 2009;20(5):807–815. | ||
Bottiglieri S, Muluneh B, Sutphin S, Iacovelli L, Adams V. Blood pressure control in patients receiving bevacizumab in an outpatient cancer center. J Oncol Pharm Pract. 2011;17(4):333–338. | ||
Mir O, Coriat R, Ropert S, et al. Treatment of bevacizumab-induced hypertension by amlodipine. Invest New Drugs. 2012;30(2):702–707. | ||
Miles DW, de Haas SL, Dirix LY, et al. Biomarker results from the AVADO phase 3 trial of first-line bevacizumab plus docetaxel for HER2-negative metastatic breast cancer. Br J Cancer. 2013;108(5):1052–1060. | ||
Etienne-Grimaldi MC, Formento P, Degeorges A, et al. Prospective analysis of the impact of VEGF-A gene polymorphisms on the pharmacodynamics of bevacizumab-based therapy in metastatic breast cancer patients. Br J Clin Pharmacol. 2011;71(6):921–928. | ||
Maitland ML, Bakris GL, Black HR, et al; Cardiovascular Toxicities Panel, Convened by the Angiogenesis Task Force of the National Cancer Institute Investigational Drug Steering Committee. Initial assessment, surveillance, and management of blood pressure in patients receiving vascular endothelial growth factor signaling pathway inhibitors. J Natl Cancer Inst. 2010;102(9):596–604. | ||
De Stefano A, Carlomagno C, Pepe S, Bianco R, De Placido S. Bevacizumab-related arterial hypertension as a predictive marker in metastatic colorectal cancer patients. Cancer Chemother Pharmacol. 2011;68(5):1207–1213. | ||
Mir O, Coriat R, Cabanes L, et al. An observational study of bevacizumab-induced hypertension as a clinical biomarker of antitumor activity. Oncologist. 2011;16(9):1325–1332. | ||
Österlund P, Soveri LM, Isoniemi H, Poussa T, Alanko T, Bono P. Hypertension and overall survival in metastatic colorectal cancer patients treated with bevacizumab-containing chemotherapy. Br J Cancer. 2011;104(4):599–604. | ||
Rini BI, Halabi S, Rosenberg JE, et al. Phase III trial of bevacizumab plus interferon alfa versus interferon alfa monotherapy in patients with metastatic renal cell carcinoma: final results of CALGB 90206. J Clin Oncol. 2010;28(13):2137–2143. | ||
Scartozzi M, Galizia E, Chiorrini S, et al. Arterial hypertension correlates with clinical outcome in colorectal cancer patients treated with first-line bevacizumab. Ann Oncol. 2009;20(2):227–230. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.