")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Increased Gestational Weight Gain is Associated with a Higher Risk of Offspring Adiposity Before Five Years of Age: A Population-Based Cohort Study
Authors Zhang S , Li N, Li W, Wang L, Liu E, Zhang T, Dong W, Chen J, Leng J
Received 19 May 2022
Accepted for publication 21 July 2022
Published 8 August 2022 Volume 2022:15 Pages 2353—2363
DOI https://doi.org/10.2147/DMSO.S374427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Shuang Zhang,1,2 Nan Li,1 Weiqin Li,1 Leishen Wang,1 Enqing Liu,1 Tao Zhang,1 Wei Dong,1 Jiujing Chen,2 Junhong Leng1
1Tianjin Women’s and Children’s Health Center, Tianjin, People’s Republic of China; 2NHC Key Laboratory of Hormones and Development, Tianjin Key Laboratory of Metabolic Diseases, Chu Hsien-I Memorial Hospital & Tianjin Institute of Endocrinology, Tianjin Medical University, Tianjin, People’s Republic of China
Correspondence: Junhong Leng, Email [email protected]
Objective: We aim to investigate the influence of weight gain during pregnancy on the risk of offspring adiposity before five years old.
Methods: We retrospectively collected health information from the Tianjin mother-child cohort. Offspring outcome was BMI Z-score and prevalence of childhood adiposity from 0.5– 5 years old. Gestational weight gain was analyzed using continuous and categorical variables evaluated by the IOM guidelines. Multivariate analysis adjusted maternal age, prepregnancy BMI, maternal height, smoking, cesarean section, gestational age at birth, birth weight, birth length, and mode of infant feeding during 0– 6 months.
Results: Gestational weight gain contributed to offspring’s BMI Z-score from 1– 5 years old, and the effect was most obvious in the first half of pregnancy (multivariate analysis, at 1, 2, 2.5, 3, 4, and 5 years of age: β 0.011, 95% CI 0.008– 0.014; β 0.017, 95% CI 0.015– 0.020; β 0.005, 95%CI 0.002-0.008; β 0.018, 95% CI 0.015– 0.021; β 0.014, 95% CI 0.009– 0.020; β 0.013, 95% CI 0.005– 0.021). Excessive weight gain was associated with a higher prevalence of offspring adiposity before five years, even if prepregnancy BMI is normal. Multivariate regression analysis further confirmed that excessive weight gain during the first half of pregnancy significantly increased the risk of childhood obesity at aged one and three (AOR 1.083, 95% CI 1.003– 1.169; AOR 1.158, 95% CI 1.036– 1.293).
Conclusion: Offspring have a higher risk of preschool adiposity when gestational weight gain was excessive during the first half of pregnancy.
Keywords: gestational weight gain, the first half of pregnancy, childhood obesity, retrospective cohort study
Plain Language Summary
- Pregnancy offers an opportunity to break the vicious cycle of obesity between generations.
- Many studies reported the effects of maternal prepregnancy obesity and gestational diabetes on the offspring adiposity while was paid insufficient attention to the gestational weight gain of healthy pregnant women.
- Gestational weight gain, especially during the first half of pregnancy, significantly affects offspring BMI Z-scores at 1–5 years of age.
- Excessive weight gain during the first half of pregnancy increases the prevalence of offspring adiposity before five years old, even if their mother had a normal prepregnancy BMI and did not suffer from diabetes.
- Weight gain during the first half of pregnancy contributed more to the risk of childhood obesity than during the second half of pregnancy.
- Today, most countries and regions carry out gestational diabetes screening in the second trimester, so assessing gestational weight gain in hospitals is convenient and feasible. Identifying inappropriate weight gain in the first half is essential in prenatal care.
Introduction
Obesity has become a significant public health issue in China. Overweight and obesity have increased rapidly in the past four decades, and the latest national prevalence estimates for 2015–2019, based on Chinese criteria, were 3.6% for obesity in children younger than six years, 7.9% for obesity in children and adolescents aged 6–17 years, and 16.4% for obesity in adults (≥18 years).1 Prevalence differed by sex, age group, and geographical location but was substantial in all subpopulations. Children from North China and more-developed areas were more likely to develop obesity.1 The effects of dietary factors and physical inactivity intersect with other individual risk factors such as genetic susceptibility, psychosocial factors, obesogens, and in-utero and early-life exposures have resulted in a rapid increase in overweight and obesity rates among children and adolescents.1,2 Obesity occurred early in life and persisted into adolescence.3,4
The association of maternal weight status with child adiposity does not only appear before pregnancy but also during the postnatal stages. Maternal prepregnancy body mass index (BMI) and gestational weight gain (GWG) are both positively and independently associated with neonatal and infant.5 Other prenatal and early postnatal factors were also related to the development of infant adiposity, including gestational diabetes,6 maternal smoking,7 cesarean delivery,8 preterm birth, and the absence of breastfeeding during the first year of life.9,10 Furthermore, low (<2500 g) or high (>4000 g) birth weight and rapid infant growth were strongly related to increased children’s adiposity.11–13
Pregnancy offers a window of opportunity to program both mothers and offspring.14 Pre-gestational obesity represents a challenge of treatment, and there is new evidence regarding its management, especially regarding adequate weight gain.14 The Institute of Medicine (IOM) guidelines are the most widely used recommendations for weight gain during pregnancy.15 It aims to improve maternal and child health through weight management during pregnancy. At present, many researchers are continuously supplementing and improving it. Since most of its evidence comes from European and American populations, its applicability to Chinese and other Asian people has been a concern.16 Many previous studies report only complications during pregnancy and neonatal outcomes, but few have consistently reported the risk of obesity from birth to preschool. In addition, most studies have focused on the effects of maternal prepregnancy obesity and gestational diabetes on the offspring while paying insufficient attention to healthy pregnant women.
The body composition of mothers changes over the trimesters to support fetal growth. Maternal fat mass is the most variable component of GWG, which mainly contributes to the energy costs of pregnancy and positively correlates with GWG.17 Previous research claims normal-weight women might be more physiologically sensitive to high gestational weight gain than women with obesity.5 However, in a prospective cohort of 146,894 participants, maternal full-term weight gain was positively associated with offspring BMI from women with overweight and obesity, but not in normal-weight mothers.18 More evidence is needed to explore the mechanism of fetal programming related to energy metabolism. When discussing the influence of weight gain during pregnancy on maternal and child health outcomes, we need to consider the specificity of GWG at different trimesters.
We studied a population from North China with a high rate of childhood adiposity. We conducted a maternal-infant cohort from the first trimester of pregnancy and followed it until the offspring were five years old. This study is devoted to observing the influence of weight gain in different stages of pregnancy on offspring adiposity from birth to five years. We focused on healthy pregnant women with normal weight and also reported that with underweight, overweight, and obesity.
Methods
Population and Data Collection
This cohort included singleton pregnant women aged 18–45 who received antenatal care from January to December 2015 in Tianjin, China. We retrospectively collected healthcare records data of mothers and offspring from the Tianjin Women and Children Health Care system. It is a government-administered public health system covering all community populations, and the antenatal care coverage rates of the local pregnant population exceed 95%. All women are registered for healthcare from getting pregnant till delivery, and their children are given health care from birth to six years old. In different phases and examination locations, trained healthcare practitioners conduct the necessary examinations for pregnant women and their children, collect the data, and enter it into an electronic health information system.19
The medical information of pregnant women starts from the first antenatal examination in early pregnancy. Basic information includes age, ethnicity, gravidity, parity, last menstrual period, chronic disease history, family history of diseases, routine prenatal tests (such as height, weight, blood pressure, lab tests of blood and urine, ultrasonography, and gestational diabetes screening), complications during pregnancy, and pregnancy outcomes (delivery modes and labor complications). And children’s information is linked to their mothers. It includes the information about newborns (date of birth, sex, gestational week of birth, birth weight and length, and Apgar score), infancy (weight, recumbent length before 24 months and height from 24 months, head circumference, blood hemoglobin, and feeding modalities), and preschool (weight, height, blood hemoglobin, and blood pressure). The study was approved by the Human Subjects Committee of the Tianjin Women’s and Children’s Health Center. Since this was a retrospective analysis of data routinely collected from health information databases. It does not involve sample collection or touching the participants and has almost no risk to the participants. It is objectively impossible to obtain informed consent from the subject. All participant information was kept confidential and anonymous. The Human Subjects Committee of Tianjin Women’s and Children’s Health Center waived the need for informed consent. This study complies with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (a) singleton pregnancy; (b) aged 18–45 years; (c) mothers did not suffer from diabetes or hypertension in prepregnancy or inter-pregnancy; (d) full-term delivery (gestational age at birth ≥37 weeks and <42 weeks). The exclusion criteria were as follows: (a) intrapartum stillbirth or neonatal death in the first seven days of life; (b) offspring had severe birth defects or other diseases; (c) mother suffered from severe anemia, digestive diseases, or tumors; (d) prenatal care and delivery information are not entirely recorded.
Measurement
Maternal body weight was measured at least three times during pregnancy, including 1) at the initial prenatal visit in the first trimester (baseline weight), 2) at the time of gestational diabetes screening in the second trimester (mid-pregnancy weight), and 3) before delivery in the third trimester (final weight). We adjusted gestational weeks of weight measurement in the analysis. Because the average weight gain during the first trimester was assumed to be 0.5−2kg, it had little impact on BMI classification and GWG calculations.20 We used bodyweight at the first prenatal visit to calculate prepregnancy BMI. BMI was calculated as weight in kilograms divided by squared height in centimeters. Maternal BMI categories were commented the Chinese BMI criteria: underweight (BMI <18.5 kg/m2), normal weight (BMI 18.5–23.9 kg/m2), overweight (BMI 24.0–27.9 kg/m2), and obesity (BMI ≥28.0 kg/m2).21
Total GWG was calculated as follows: (final weight – baseline weight). We defined weight gain during the first half of pregnancy (f-GWG) as GWG before mid-pregnancy weight measurement, and later was defined as weight gain during the second half of pregnancy (s-GWG). According to f-GWG, we divided pregnant women into three categories: insufficient, appropriate, or excessive, based on the IOM’s recommendations. The guidelines recommended rate of weight gain in the second and third trimesters was 0.44−0.58, 0.35−0.50, 0.23−0.33, and 0.17−0.27 kg/week in the underweight, normal weight, overweight, and obesity group.
Offspring’s weight and length/height were measured at birth (<3 days after birth), 0.5 years (6 months and <7 months), 1 year (12 months and <13 months), 1.5 years (18 months and <20 months), 2 years (24 months and <26 months), 2.5 years (30 months and <32 months), 3 years (36 months and <38 months), 4 years (48 months and <50 months), and 5 years (60 months and <62 months). Trained pediatricians collected anthropometric data in the community hospitals, and measurement devices and standards were uniforms.
Birth BMI Z-scores for sex- and gestational age were calculated using our study population means and standard deviations.22 We calculated age- and sex-specific BMI Z-scores from 0.5−5 years old based on the World Health Organization (WHO) child growth references.23 To make the data more useful for comparison and contribute to understanding international standard definitions of overweight and obesity, we used BMI to classify each child as normal, overweight, or with obesity. Normal weight was defined as a BMI less than the 85th percentile for age and sex using the WHO growth reference (<1.035 Z-score), overweight and obesity was described as a BMI ≥85th percentile (≥1.035 Z-score) and a BMI ≥95th percentile (≥1.645 Z-score).23 We defined offspring adiposity as obesity at 0.5, 1, 1.5, 2, 2.5, 3, 4, and 5 years of age.
Term infants were classified as small for gestational age (SGA; <10th percentile) and large for gestational age (LGA; >90th percentile) according to the Chinese neonatal birth weight curve, which was sex- and gestational age-matched with newborns that were appropriate for gestational age (AGA).24 We defined rapid weight gain (RWG) as an increase in BMI Z-score of >0.67 standard deviations (0−6 months).13
Outcome
Offspring outcome was BMI Z-score and prevalence of childhood adiposity from 0.5–5 years old.
Statistical Analysis
IBM SPSS Statistics for Windows (Version 21.0. Armonk, NY: IBM Corp) and GraphPad Prism 8 (San Diego, CA: GraphPad Software) was used for data analysis and figure drawing. Normally distributed continuous variables were presented as means (standard deviations) and were compared between groups using t-test of independent samples or one-way analysis of variance. Categorical variables were presented as frequencies (percentages) and were compared using the Chi-square test. We established linear regression models to analyze the effect of GWG on offspring BMI Z-score. Logistic regression analysis was performed to analyze the effects of GWG on offspring adiposity. A two-tailed P-value of less than 0.05 was considered statistically significant. In the multivariate analysis, we adjusted the confounders including maternal age, prepregnancy BMI, maternal height, smoking, cesarean section, gestational age at birth, birth weight, birth length, mode of infant feeding during 0–6 months (exclusively breastfeeding, mixed feeding, or formula only).
Results
Characteristics of Pregnant Women and Their Offspring
A total of 58,332 mother-child pairs were included in the final analysis (Figure S1). The mean maternal age was 27.95 (SD 4.06) years, and the mean prepregnancy BMI was 22.33 (SD 3.57) kg/m.2 Among them, 6464 (11.1%) were underweight, 36,143 (62.0%) were normal weight, 11,449 (19.6%) were overweight, and 4276 (7.3%) were obesity. The mean gestational age at birth was 39.56 (SD 1.05) weeks. Of the total newborns, 29,898 (51.3%) were male, and 28,434 (48.7%) were female. AGA, SGA and LGA was 48,382 (82.9%), 2979 (5.1%) and 6971 (12.0%), respectively. At 0.5, 1, 1.5, 2, 2.5, 3, 4, and 5 years of age, 49,824 (85.4%), 47,388 (81.2%), 48,401 (83.0%), 47,709 (81.8%), 42,604 (73.0%), 43,948 (75.3%), 15,896 (27.3%), and 9661 (16.6%) children were followed up respectively. Non-participants were mainly 1) moved to another province, 2) overdue health check-ups, and 3) not enrolled in public kindergartens after age three. Table 1 showed that higher prepregnancy BMI was associated with higher maternal age, gravidity, infant birthweight, proportions of multiparity, cesarean delivery, LGA, and BMI Z-score from birth to five years old. It is also related to lower GWG, proportions of education >12 years, first pregnancy conception, SGA, and RWG (P<0.001).
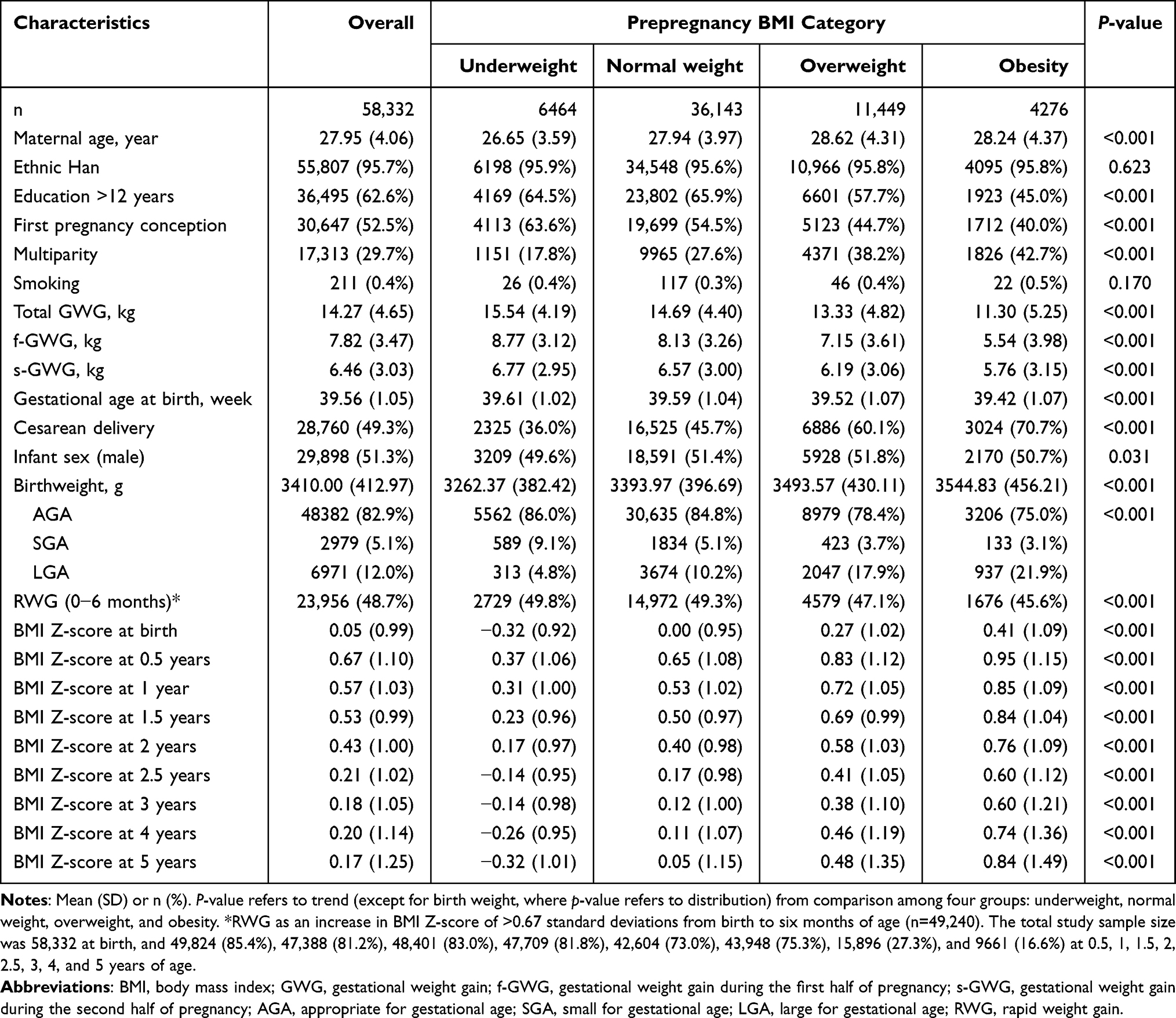 |
Table 1 Characteristics of the Study Population |
Weight Gain and Offspring Body Mass Index-for-Age Z-Score
Linear multivariate regression analysis showed that f-GWG (continuous variable) had significant effects on offspring BMI Z-scores at 1, 2, 2.5, 3, 4, and 5 years of age (β 0.011, 95% CI 0.008–0.014; β 0.017, 95% CI 0.015–0.020; β 0.005, 95% CI 0.002–0.008; β 0.018, 95% CI 0.015–0.021; β 0.014, 95% CI 0.009–0.020; β 0.013, 95% CI 0.005–0.021). The effect was more obvious than total GWG and s-GWG (Table 2).
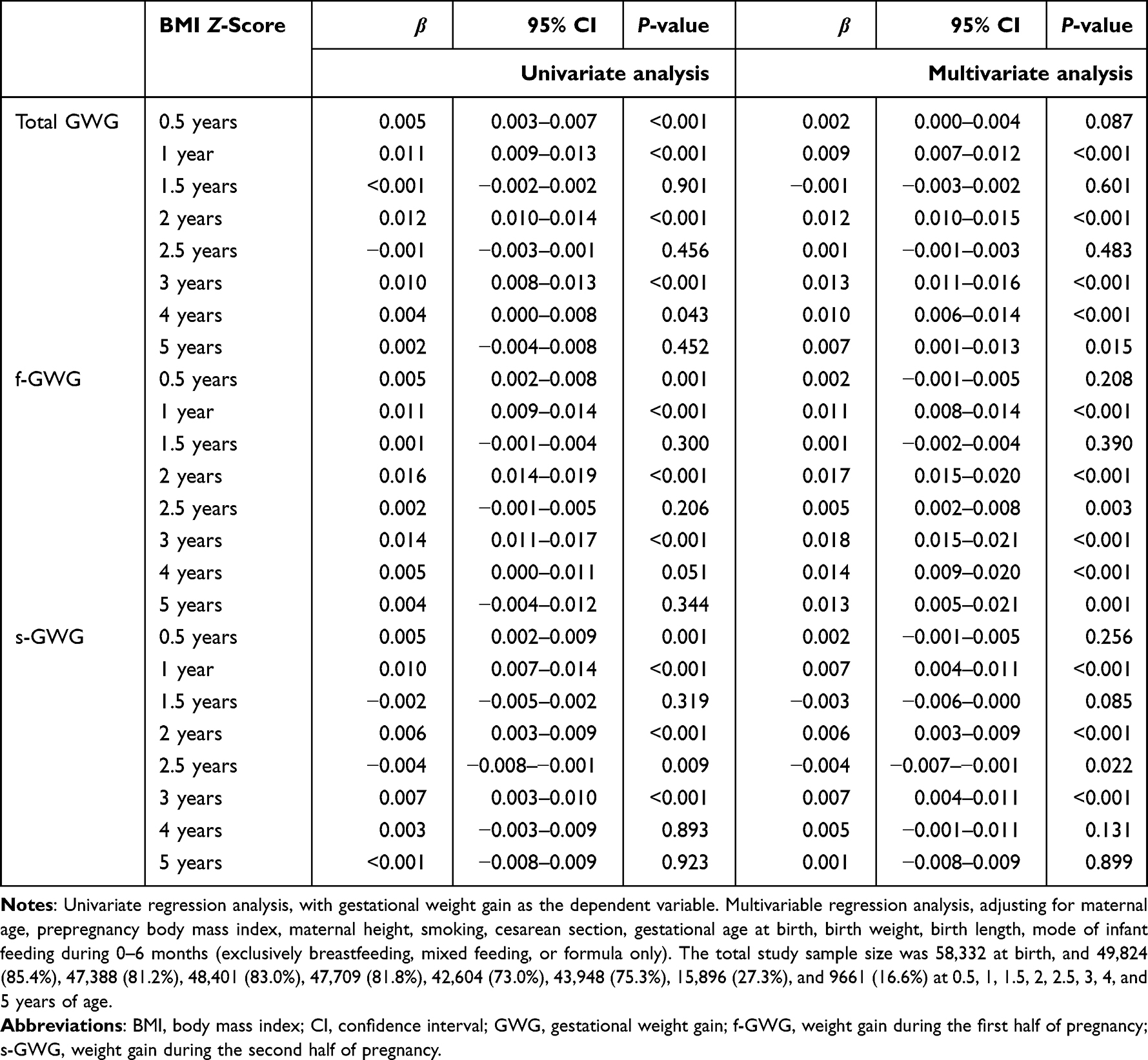 |
Table 2 Linear Regression Analysis of the Effects of Gestational Weight Gain on Offspring BMI Z-Scores |
Weight Gain and Offspring Adiposity
Logistic regression analysis confirmed that maternal weight gain during pregnancy (continuous variable) significantly increased the risk of offspring adiposity (Figure 1). Weight gain during pregnancy greatly affected the risk of offspring adiposity before five years old. The effects of f-GWG on offspring adiposity were more evident than total GWG. We did not observe a significant impact of s-GWG on offspring adiposity at 2–5 years of age. The results indicated that f-GWG and total GWG on childhood adiposity is consistent. The f-GWG has high clinical value for early screening and intervention. Therefore, this study focuses on maternal weight gain in the first half of pregnancy on offspring adiposity.
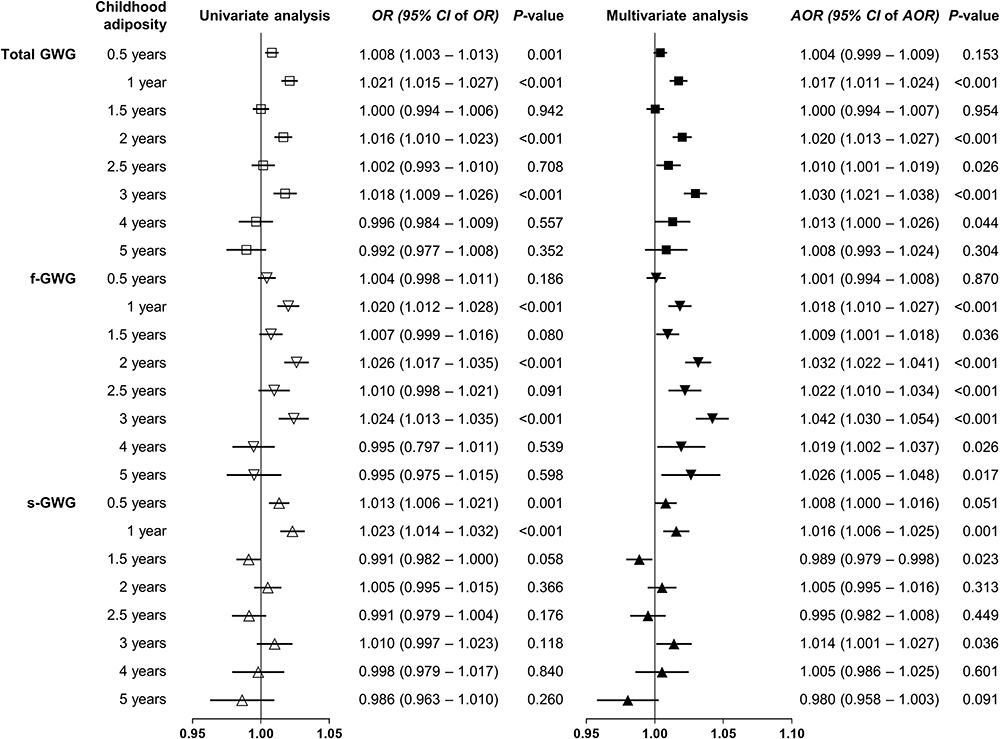 |
Figure 1 Forest plot of odds ratios (95% confidence intervals) for the association of gestational weight gain with offspring adiposity. Abbreviations: OR, odds ratios; CI, confidence interval; GWG, gestational weight gain; f-GWG, weight gain during the first half of pregnancy; s-GWG, weight gain during the second half of pregnancy. Notes: The total study sample size was 58,332 at birth, and 49,824 (85.4%), 47,388 (81.2%), 48,401 (83.0%), 47,709 (81.8%), 42,604 (73.0%), 43,948 (75.3%), 15,896 (27.3%), and 9661 (16.6%) at 0.5, 1, 1.5, 2, 2.5, 3, 4, and 5 years of age. Squares (Total GWG), inverted triangle (weight gain during the first half of pregnancy), and upright triangle (weight gain during the second half of pregnancy) represent the point estimate, and the bars are the 95% confidence intervals. Multivariable regression analysis, adjusting for maternal age, prepregnancy body mass index, maternal height, smoking, cesarean section, gestational age at birth, birth weight, birth length, mode of infant feeding during 0–6 months (exclusively breastfeeding, mixed feeding, or formula only). |
According to maternal f-GWG, we divided all the mother-infant pairs into three categories: insufficient (n=9640), appropriate (n=10,720), and excessive (n=37,972). Figure 2 showed the prevalence of offspring adiposity at 0.5−5 years of age in each f-GWG category and maternal prepregnancy BMI group. In general, the risk of offspring adiposity increased with an increase in maternal prepregnancy BMI. Subgroup analysis showed that insufficient or excessive f-GWG did not affect the prevalence of childhood adiposity in underweight and obesity groups (Table S1). In the normal-weight group, excessive f-GWG was associated with a higher prevalence of childhood adiposity (at 0.5, 1, 1.5, 2, 3, and 5 years of age). A similar significant effect was found in the overweight group when the offspring were 0.5, 1, 1.5, 2, 2.5, and 3 years old.
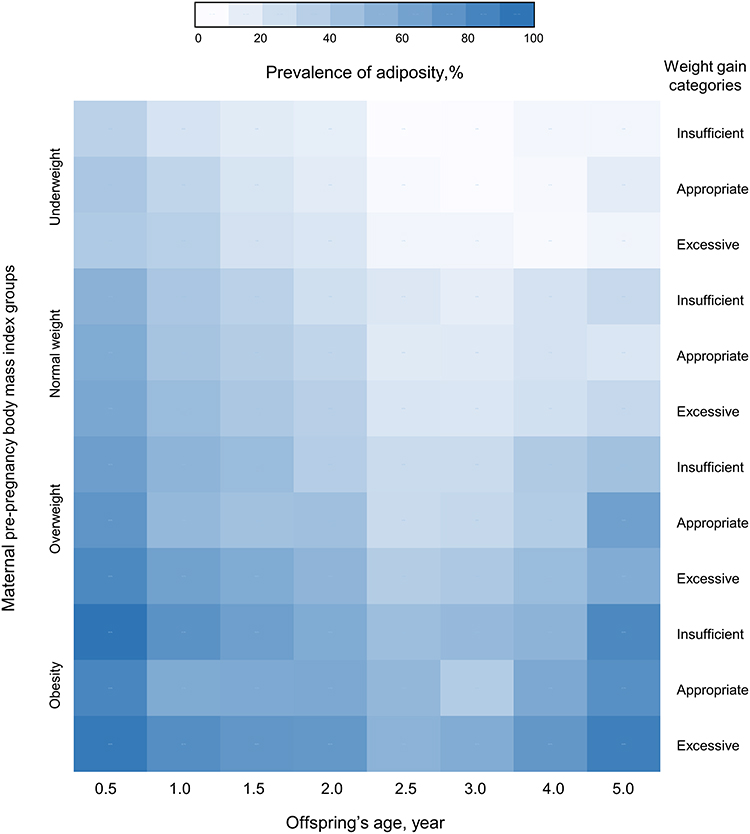 |
Figure 2 Heatmap of the prevalence of offspring adiposity at 0.5−5 years of age. Abbreviations: f-GWG, weight gain during the first half of pregnancy; AGA, appropriate for gestational age. Notes: Values represent the prevalence of offspring adiposity for each body mass index and weight gain category. The total study sample size was 58,332 at birth, and 49,824 (85.4%), 47,388 (81.2%), 48,401 (83.0%), 47,709 (81.8%), 42,604 (73.0%), 43,948 (75.3%), 15,896 (27.3%), and 9661 (16.6%) at 0.5, 1, 1.5, 2, 2.5, 3, 4, and 5 years of age. BMI groups were commented the Chinese BMI criteria, underweight (BMI <18.5 kg/m2), normal weight (BMI 18.5−23.9 kg/m2), overweight (BMI 24.0− 27.9 kg/m2), and obesity (BMI ≥ 28.0 kg/m2). According to the IOM guidelines, participants were divided into three categories based on maternal weight gain during the first half of pregnancy. |
Univariate logistic regression analysis revealed that excessive f-GWG significantly increased the risk of offspring adiposity at 1, 1.5, 2, 2.5, 3, 4, and 5 years of age (all P<0.001) (Table 3). Excessive f-GWG significantly contributed high risk of adiposity at one and three years of age (AOR 1.083, 95% CI 1.003–1.169, P=0.042; AOR 1.158, 95% CI 1.036–1.293, P=0.009) in offspring delivered at term after adjusting for maternal age, prepregnancy BMI, maternal height, smoking, cesarean section, gestational age at birth, birth weight, birth length, mode of infant feeding during 0–6 months (exclusively breastfeeding, mixed feeding, or formula only) in multivariate regression analysis (Table 3).
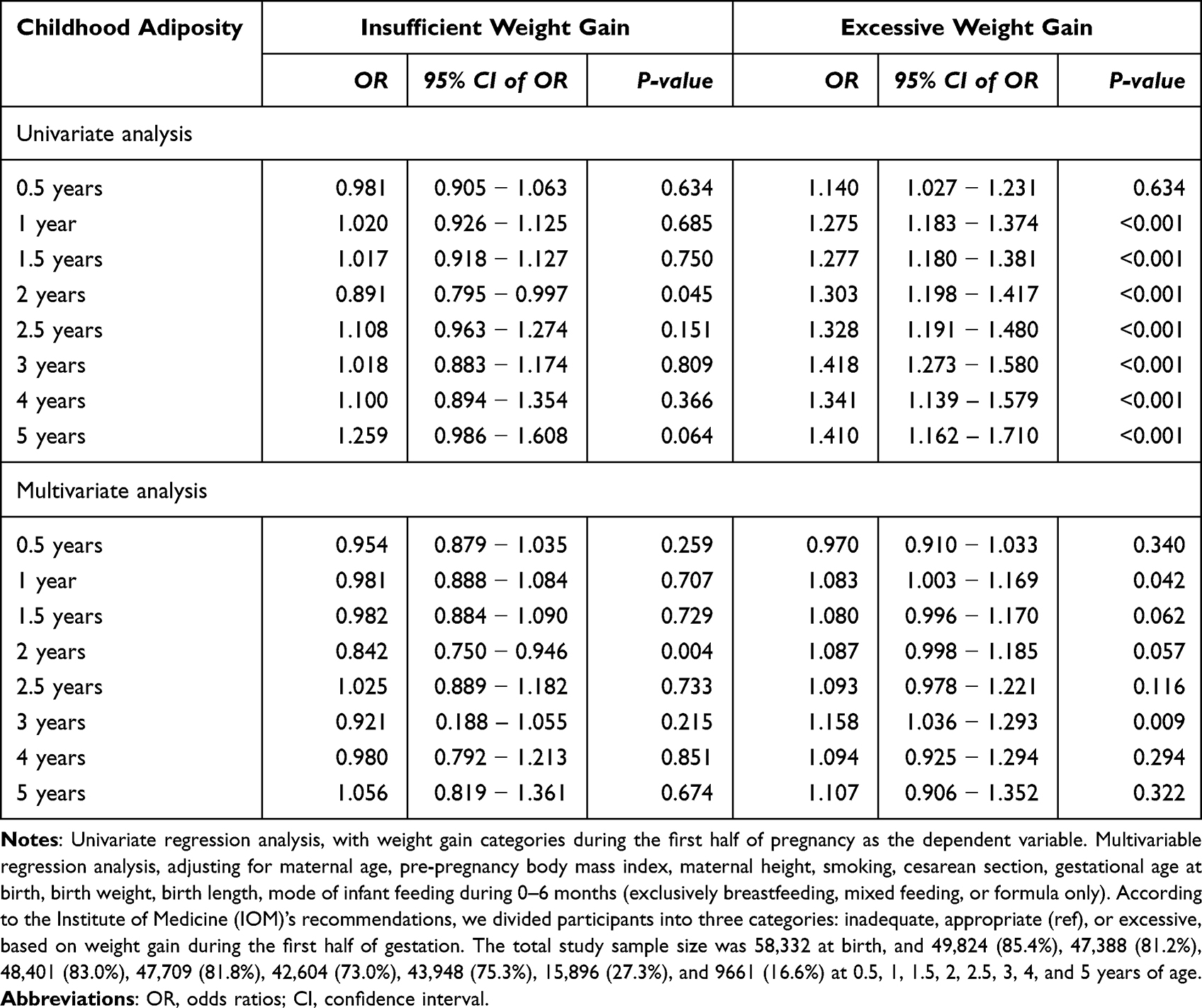 |
Table 3 Odds Ratios and 95% Confidence Intervals for the Effects of Maternal Weight Gain During the First Half of Pregnancy on Offspring Adiposity |
Discussion
This study found that gestational weight gain, especially during the first half of pregnancy, significantly affected the risk of childhood adiposity in offspring.
Maternal prepregnancy obesity and excessive weight gain during pregnancy are important risk factors for various adverse offspring outcomes, including stillbirth, neonatal death, LGA, increased blood pressure, adverse lipids profile, impaired insulin and glucose homeostasis, and obesity.25 It is crucial and urgent to identify early life risk factors for offspring obesity and cardiovascular diseases.26 However, the elements are complex, including intrauterine exposure mechanisms, genetic background, family environment, and lifestyle. Some studies have demonstrated the contribution of weight gain during pregnancy to birth weight.15 The interaction between prepregnancy BMI and GWG on childhood obesity has been a concern. The effects of GWG on childhood adiposity were inconsistent across maternal BMI.27–29 Thus, we fully considered prepregnancy BMI and said the prevalence of childhood obesity in different prepregnancy BMI categories. The results showed that the prevalence of adiposity in offspring at 0.5, 1, 1.5, 2, 3, and 5 years old was higher if their normal-weight mothers gained too much weight during the first half of pregnancy. A similar significant effect was found in the overweight group when the offspring aged 0.5, 1, 1.5, 2, 2.5, and 3 years. However, for mothers underweight or with obesity, weight gain during pregnancy did not contribute to preschool obesity of their offspring.
Earlier studies of intrauterine fat development in human embryos and fetuses have shown five stages in adipose tissue formation.30 Fat tissue differentiates between 14−16 weeks of gestation. During this period, the disturbances of normal adipogenesis may play a role in the etiology of obesity in later life. Fat lobules are the earliest structures to be identified before typical vacuolated fat cells appear. The total number of fat lobules remains approximately constant after the 23rd week. The growth of adipose tissue is determined mainly by increasing the size of the lobules from 23−29 weeks of gestation. These results suggest that 14−23 weeks of pregnancy are sensitive periods in fat lobule development and that disturbances of normal adipogenesis during this period may play a role in the etiology of obesity in later life.30 Early GWG represents a metabolically dysregulated intrauterine environment (ie, lower adiponectin and higher insulin) that could predispose offspring to adiposity and insulin resistance. Low adiponectin in utero may be a pathway through which the first-trimester GWG could program increased adiposity, especially central adiposity. In addition, the second trimester gain matters more for hormones related to growth and adiposity (eg, insulin-like growth factor [IGF]-1, IGF-2, IGFBP-3, and leptin), but the third-trimester GWG was not associated with cord blood hormones.31 We confirmed that GWG (continuous variable) during the first half of pregnancy had significant effects on offspring BMI Z-scores at 1−5 years of age. For each 1kg increase in weight gain during the first half of pregnancy, the offspring’s BMI Z-score increased by 0.013 (95% CI 0.005–0.021) at age five. The effect was more evident than total GWG (β 0.007, 95% CI 0.001–0.013, P=0.015) and s-GWG (β 0.001, 95% CI −0.008–0.009, P=0.899). Furthermore, the results revealed that weight gain during pregnancy significantly affected the risk of offspring adiposity before five years of age. The effects of f-GWG on offspring adiposity were more evident than total GWG. We did not observe a significant impact of s-GWG on offspring adiposity at 2−5 years.
Early identification of inappropriate weight gain during pregnancy is a prerequisite for intervention in the second half of pregnancy. Our population-based mother-child cohort well illustrates it. A previous meta-analysis of multiple randomized controlled trials showed that dietary and physical activity interventions aimed at reducing maternal weight gain during pregnancy might lead to small reductions in gestational weight gain and lower risks of adverse fetal outcomes.32 Therefore, scientific control of weight gain during pregnancy, especially in the first and second trimesters, may contribute to the prevention of childhood adiposity.
Although other studies have demonstrated the significance of weight gain in three trimesters,33 this ideal measurement may be difficult to achieve in a population-wide public health management system. As things stand, most countries and regions carry out gestational diabetes screening in the second trimester, so it is very convenient and feasible to take weight measurements at this time. Therefore, assessing weight gain during the first half of pregnancy has undeniable clinical application value for prenatal care.
There are some limitations to consider in this study. It is a retrospective study and cannot claim a cause-effect relationship between gestational weight gain and obesity in offspring. Further prospective studies are needed to improve our findings. Information on four - and five-year-olds came from public kindergarten health checks, but the information of children who attended private kindergartens or were not enrolled in kindergartens was missing. It led to a sharp decline in follow-up rates and may have weakened the statistical significance of the results.
Conclusion
Offspring have a higher risk of preschool adiposity when gestational weight gain was excessive during the first half of pregnancy.
Abbreviations
BMI, body mass index; GWG, gestational weight gain; IOM, Institute of Medicine; f-GWG, weight gain during the first half of pregnancy; s-GWG, weight gain during the second half of pregnancy; WHO, World Health Organization; SGA, small for gestational age; LGA, large for gestational age; AGA, appropriate for gestational age; RWG, rapid weight gain.
Ethics Approval and Informed Consent
The study was approved by the Human Subjects Committee of the Tianjin Women’s and Children’s Health Center. Since this was a retrospective analysis of data routinely collected from health information databases. It does not involve sample collection or touching the participants and has almost no risk to the participants. It is objectively impossible to obtain informed consent from the subject. All participant information was kept confidential and anonymous. The Human Subjects Committee of Tianjin Women’s and Children’s Health Center waived the need for informed consent. This study complies with the Declaration of Helsinki.
Acknowledgments
The authors sincerely thank the doctors and nurses in the community hospitals involved in collecting medical information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Tianjin Key Medical Discipline (Specialty) Construction Project (grant number: TJYXZDXK-075C).
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9:373–392. doi:10.1016/S2213-8587(21)00045-0
2. Guo Y, Yin X, Wu H, Chai X, Yang X. Trends in overweight and obesity among children and adolescents in China from 1991 to 2015, A meta-analysis. Int J Environ Res Public Health. 2019;16:4656. doi:10.3390/ijerph16234656
3. Geserick M, Vogel M, Gausche R, et al. Acceleration of BMI in early childhood and risk of sustained obesity. N Engl J Med. 2018;379:1303–1312. doi:10.1056/NEJMoa1803527
4. Yoshida S, Kimura T, Noda M, Takeuchi M, Kawakami K. Association of maternal prepregnancy weight and early childhood weight with obesity in adolescence, A population-based longitudinal cohort study in Japan. Pediatr Obes. 2020;15:e12597. doi:10.1111/ijpo.12597
5. Larque E, Labayen I, Flodmark CE, et al. From conception to infancy - early risk factors for childhood obesity. Nat Rev Endocrinol. 2019;15:456–478. doi:10.1038/s41574-019-0219-1
6. Logan KM, Gale C, Hyde MJ, Santhakumaran S, Modi N. Diabetes in pregnancy and infant adiposity, systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2017;102:F65–F72. doi:10.1136/archdischild-2015-309750
7. Oken E, Levitan EB, Gillman MW. Maternal smoking during pregnancy and child overweight, systematic review and meta-analysis. Int J Obes. 2008;32:201–210. doi:10.1038/sj.ijo.0803760
8. Yuan C, Gaskins AJ, Blaine AI, et al. Association between cesarean birth and risk of obesity in offspring in childhood, adolescence, and early adulthood. JAMA Pediatr. 2016;170:e162385. doi:10.1001/jamapediatrics.2016.2385
9. Rogers SL, Blissett J. Breastfeeding duration and its relation to weight gain, eating behaviours and positive maternal feeding practices in infancy. Appetite. 2017;108:399–406. doi:10.1016/j.appet.2016.10.020
10. Ma J, Qiao Y, Zhao P, et al. Breastfeeding and childhood obesity, A 12-country study. Matern Child Nutr. 2020;16:e12984. doi:10.1111/mcn.12984
11. Lai C, Hu Y, He D, et al. U-shaped relationship between birth weight and childhood blood pressure in China. BMC Pediatr. 2019;19:264. doi:10.1186/s12887-019-1638-9
12. Chomtho S, Wells JC, Williams JE, Davies PS, Lucas A, Fewtrell MS. Infant growth and later body composition, evidence from the 4-component model. Am J Clin Nutr. 2008;87:1776–1784. doi:10.1093/ajcn/87.6.1776
13. Li N, Zhang S, Leng JH, et al. Effects of rapid growth in early childhood on metabolic and cardiovascular diseases among preschool-aged children. Asia Pac J Clin Nutr. 2020;29:558–565. doi:10.6133/apjcn.202009_29(3).0015
14. Parrettini S, Caroli A, Torlone E. Nutrition and metabolic adaptations in physiological and complicated pregnancy, focus on obesity and gestational diabetes. Front Endocrinol. 2020;11:611929. doi:10.3389/fendo.2020.611929
15. Rasmussen KM, Yaktine AL. Weight Gain During Pregnancy, Reexamining the Guidelines. Washington (DC): Institute of Medicine (US) and National Research Council (US) Committee; 2009.
16. Voerman E, Santos S, Patro Golab B, et al. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood, An individual participant data meta-analysis. PLoS Med. 2019;16:e1002744. doi:10.1371/journal.pmed.1002744
17. Lederman SA, Paxton A, Heymsfield SB, Wang J, Thornton J, Pierson RN. Body fat and water changes during pregnancy in women with different body weight and weight gain. Obstet Gynecol. 1997;90:483–488. doi:10.1016/s0029-7844(97)00355-4
18. Lawlor DA, Lichtenstein P, Fraser A, Langstrom N. Does maternal weight gain in pregnancy have long-term effects on offspring adiposity? A sibling study in a prospective cohort of 146,894 men from 136,050 families. Am J Clin Nutr. 2011;94:142–148. doi:10.3945/ajcn.110.009324
19. Wang J, Pan L, Liu E, et al. Gestational diabetes and offspring’s growth from birth to 6 years old. Int J Obes. 2019;43:663–672. doi:10.1038/s41366-018-0193-z
20. Rangel Bousquet Carrilho T, Rodrigues Farias D, Rodrigues Farias D, et al. Agreement between self-reported prepregnancy weight and measured first-trimester weight in Brazilian women. BMC Pregnancy Childbirth. 2020;20:734. doi:10.1186/s12884-020-03354-4
21. Zhou BF; Cooperative Meta-Analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults–study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. 2002;15:83–96.
22. Li N, Liu E, Sun S, et al. Birth weight and overweight or obesity risk in children under 3 years in China. Am J Hum Biol. 2014;26:331–336. doi:10.1002/ajhb.22506
23. Group WHOMGRS. WHO child growth standards based on length/height, weight and age. Acta Paediatr Suppl. 2006;450:76–85. doi:10.1111/j.1651-2227.2006.tb02378.x
24. Zhu L, Zhang R, Zhang S, Shi W, Chen C. [Chinese neonatal birth weight curve for different gestational age]中国不同胎龄新生儿出生体重曲线研制. Zhonghua Er Ke Za Zhi中华儿科杂志. 2015;53:97–103. Chinese.
25. Gaillard R. Maternal obesity during pregnancy and cardiovascular development and disease in the offspring. Eur J Epidemiol. 2015;30:1141–1152. doi:10.1007/s10654-015-0085-7
26. Ciccone MM, Scicchitano P, Salerno C, et al. Aorta structural alterations in term neonates, the role of birth and maternal characteristics. Biomed Res Int. 2013;2013:459168. doi:10.1155/2013/459168
27. Diesel JC, Eckhardt CL, Day NL, Brooks MM, Arslanian SA, Bodnar LM. Gestational weight gain and the risk of offspring obesity at 10 and 16 years, a prospective cohort study in low-income women. BJOG. 2015;122:1395–1402. doi:10.1111/1471-0528.13448
28. Montazeri P, Vrijheid M, Martinez D, et al. Maternal metabolic health parameters during pregnancy in relation to early childhood BMI trajectories. Obesity. 2018;26:588–596. doi:10.1002/oby.22095
29. Guo L, Liu J, Ye R, Liu J, Zhuang Z, Ren A. Gestational weight gain and overweight in children aged 3–6 years. J Epidemiol. 2015;25:536–543. doi:10.2188/jea.JE20140149
30. Poissonnet CM, Burdi AR, Bookstein FL. Growth and development of human adipose tissue during early gestation. Early Hum Dev. 1983;8:1–11. doi:10.1016/0378-3782(83)90028-2
31. Rifas-Shiman SL, Fleisch A, Hivert MF, Mantzoros C, Gillman MW, Oken E. First and second trimester gestational weight gains are most strongly associated with cord blood levels of hormones at delivery important for glycemic control and somatic growth. Metabolism. 2017;69:112–119. doi:10.1016/j.metabol.2017.01.019
32. Thangaratinam S, Rogozinska E, Jolly K, et al. Effects of interventions in pregnancy on maternal weight and obstetric outcomes, meta-analysis of randomised evidence. BMJ. 2012;344:e2088. doi:10.1136/bmj.e2088
33. Xiong X, Xia W, Li Y, Xu S, Zhang Y. Associations of gestational weight gain rate during different trimesters with early-childhood body mass index and risk of obesity. Obesity. 2020;28:1941–1950. doi:10.1002/oby.22963
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.