")
Back to Journals » Infection and Drug Resistance » Volume 10
Incomplete recovery of the fecal flora of hematological patients with neutropenia and repeated fluoroquinolone prophylaxis
Authors Chong Y, Shimoda S, Miyake N, Aoki T, Ito Y, Kamimura T, Shimono N
Received 26 January 2017
Accepted for publication 7 April 2017
Published 27 June 2017 Volume 2017:10 Pages 193—199
DOI https://doi.org/10.2147/IDR.S133333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yong Chong,1 Shinji Shimoda,1 Noriko Miyake,1 Takatoshi Aoki,2 Yoshikiyo Ito,3 Tomohiko Kamimura,2 Nobuyuki Shimono4
1Department of Medicine and Biosystemic Science, Kyushu University Graduate School of Medical Sciences, 2Department of Blood and Marrow Transplantation, Hara-Sanshin Hospital, Fukuoka, 3Department of Internal Medicine, Kyushu University Beppu Hospital, Beppu, 4Center for the Study of Global Infection, Kyushu University Hospital, Fukuoka, Japan
Background: Routine fluoroquinolone prophylaxis in neutropenic patients with hematological malignancies is still controversial, because of antibiotic resistance concerns. The recovery of the fecal microbiota to the initial composition in patients receiving multiple courses of quinolone prophylaxis and repeated chemotherapy has not been evaluated.
Methods: We prospectively examined the changes in the fecal bacterial composition before and after levofloxacin prophylaxis. A sequential observation of bacterial resistance in patients receiving multiple prophylactic courses was also conducted.
Results: In this trial, 68 cases, including (35 with the first course and 33 with the second and subsequent courses) were registered. The disappearance of quinolone-susceptible (QS) Enterobacteriaceae and dominant emergence of quinolone-resistant (QR) coagulase negative staphylococci (CNS) and QR Enterococci were observed after the first prophylaxis. The detection of QS Enterobacteriaceae was recovered before the second and subsequent courses to a level of the initial composition (28/35 samples, 80.0% before the first course vs 23/33 samples, 69.7% before the second and subsequent courses, P=0.41). In contrast, the detection rate of QR CNS and Enterococci significantly increased at the second and subsequent courses, even before prophylaxis (8/35 samples, 22.9% before the first course vs 20/33 samples, 60.6% before the second and subsequent courses, P=0.003). The incomplete recovery of the initial bacterial composition was associated with a prophylactic interval of within 30 days. Of the patients receiving multiple prophylactic courses, six had QR Escherichia coli, including extended-spectrum β-lactamase (ESBL) producers, at the first course, and four (66.3%) of the six patients had persistent detection of QR E. coli at the second course.
Conclusion: In patients receiving multiple courses of prophylactic quinolone, along with a common chemotherapy schedule, newly emergent resistant bacteria could be frequently persistent in their fecal flora.
Keywords: febrile neutropenia, prophylaxis, fluoroquinolone, antibiotic resistance, fecal flora, chemotherapy
Introduction
Febrile neutropenia is one of the most serious adverse events in patients with hematological malignancies and chemotherapy.1 Bacteremia related to febrile neutropenia often increases infection-related morbidity and mortality. The use of antibiotic prophylaxis, particularly fluoroquinolones (quinolones), has been known to have a positive impact on the frequency of febrile episodes, bacteremia, and even infection-related mortality.2–4 The latest guideline issued by the Infectious Diseases Society of America (IDSA) stated that the prophylactic use of quinolones is recommended for high-risk patients in whom chemotherapy-induced neutropenia is expected to last for >7 days.5 However, the emergence of bacterial resistance to antibiotics, especially quinolones, has become a critical concern, and routine prophylactic use has been repeatedly questioned to date.6–10
In our previous study, we prospectively examined the incidence of quinolone-resistant (QR) Escherichia coli isolates recovered from stool cultures before and after levofloxacin prophylaxis in 68 neutropenic patients with hematological malignancies and analyzed the emergence of QR E. coli before and after prophylaxis.11 Patients with hematological malignancies usually receive repeated chemotherapy and, accordingly, repeated quinolone prophylaxis for their neutropenia in many cases. It is not known whether quinolone-susceptible (QS) bacteria in the initial gut flora can be recovered during the administration of multiple courses of prophylactic quinolone. Also, sequential observation of bacterial resistance in patients receiving multiple courses of prophylaxis has not been conducted. In the present study, we used fecal samples collected from the 68 patients who were registered in our previous study to analyze the changes in fecal microbiota before and after quinolone prophylaxis. A significant point of this study was to examine the sequential change of fecal bacterial composition, including the recovery of QS bacteria and persistent detection of QR bacteria, during repeated prophylactic antibiotic exposure. In addition, we examined the detection history of QR E. coli at an individual level.
Methods
Patients and ethics statement
From August 2011 to May 2013, 68 cases were recruited from a single hematological unit with 37 beds at Hara-Sanshin Hospital. The protocol was approved, through the ethics review process, by the Institutional Review Board of the Hara-Sanshin Hospital. Written informed consent was obtained from all registered patients not only for publication of these case details but also to participate in this research. Infection control measures including promotion of hand-washing and isolation procedures were maintained throughout the study.
Enrollment
Inpatients with neutropenia were enrolled in the study. Neutropenia was defined as an absolute neutrophil count of <1,000 cells/mm3 or a neutrophil count with a predicted decrease to <1,000 cells/mm3 during the following 48 hours. Exclusion criteria is shown in our previous report.11 Patients treated for allogeneic hematopoietic stem cell transplantation were excluded from the trial because a confirmative diagnosis of febrile neutropenia is often difficult because of the presence of other causative factors such as graft-versus-host disease and engraftment syndrome. Antimycotic agents were administered for most of the registered neutropenic patients.
Treatment protocol
Antibiotic prophylaxis with levofloxacin (Daiichi Sankyo Co. Ltd., Tokyo, Japan) at a dosage of 500 mg/day was administered to all patients during the study period. Levofloxacin was administered to patients without febrile neutropenia until their neutrophil counts recovered. However, levofloxacin prophylactic treatment was discontinued when the empirical antibiotic therapy for febrile neutropenia was initiated. Febrile neutropenia was defined as: 1) fever, a single axillary temperature of >38.0°C or an axillary temperature >37.5°C lasting 1 hour and 2) neutropenia, defined according to the aforementioned guidelines.
Microbiology
For each patient, 2 stool samples were examined. The first sample was collected before levofloxacin administration, and the second sample after prophylaxis was discontinued. Stool samples were cultured, chiefly using 5% Sheep Blood Agar medium (BD). The species were identified using the Vitek system (bioMerieux Japan Ltd., Tokyo, Japan). Antibiotic susceptibilities were determined by the breakpoints standardized by the Clinical and Laboratory Standards Institute (CLSI).12 The screening and confirmation tests for extended-spectrum β-lactamase (ESBL) were conducted according to the recommendation of the CLSI.12 In addition, β-lactamase producers were confirmed using a Cica β test I/MBL kit (Kanto Chemical Co. Ltd., Tokyo, Japan).
Variables and definitions
Clinical data were collected from medical records to evaluate the related risk factors. The variables obtained from the data of the last course of quinolone prophylaxis, which are associated with the detection of QS and resistant bacteria at the second and subsequent courses, included high-intensity chemotherapy, trimethoprim-sulfamethoxazole (TMP-SMX) prophylaxis, antimicrobial therapy except for quinolone prophylaxis at the last cycle, duration of quinolone prophylaxis at the last cycle, and duration from the final antimicrobial therapy to sample collection. Of the 33 cases with more than two courses of prophylaxis, 23 cases included relatively high-intensity chemotherapy consisting of a standard chemotherapy for acute leukemia (ie, daunorubicin plus cytosine arabinoside) and a salvage chemotherapy for malignant lymphoma, for their last chemotherapy. The remaining 10 cases received relatively low-intensity chemotherapy of CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) or R (rituximab)-CHOP for acute leukemia and malignant lymphoma, for their last chemotherapy. Pneumocystis pneumonia prophylaxis using TMP-SMX was conducted in 18 cases at the last cycle. In the 14 cases of febrile neutropenia at the last cycle, antimicrobial agents recommended for febrile neutropenia, including piperacillin-tazobactam, cefepime, and meropenem, were administered. A protocol for quinolone prophylaxis is mentioned above. The duration of quinolone prophylaxis at the last cycle was examined. The duration from the final antimicrobial therapy to sample collection was defined as the period from the final date of the last quinolone prophylaxis or the last antimicrobial therapy for febrile neutropenia until the date of sample collection before prophylaxis at the second and subsequent courses of prophylaxis.
Statistical analysis
Categorical variables between groups were tested using the Fisher’s exact test. P<0.05 was considered to be statistically significant. All statistical analyses were performed using the JMP Pro software, version 11 (SAS Institute, Inc., Cary, NC, USA).
Results
A total of 68 cases were enrolled (Table 1). Patients receiving multiple courses of quinolone prophylaxis were recruited as a different case for every course. Of the 68 cases, 35 cases were applied for the first cycle of chemotherapy and quinolone prophylaxis. Among the 35 cases, 21 cases were applied for the second cycle. Among the 21 cases, 12 cases were applied for the third and subsequent cycles. Accordingly, a total of 33 cases were applied for the second and subsequent cycles. We focused on the decrease of QS Enterobacteriaceae and the dominant emergence of QR coagulase negative staphylococci (CNS) and QR Enterococcus (QR CNS and Enterococcus) species, as a characteristic of the change of bacterial composition in feces before and after quinolone exposure. The Enterobacteriaceae detected included Escherichia coli, Klebsiella spp., Proteus spp., Citrobacter spp., Enterobacter spp., Morganella morganii, and Raoultella planticola. As shown in Table 1, QS Enterobacteriaceae strains were not detected after the use of quinolones, regardless of the number of cycles. QS Enterobacteriaceae strains were detected in 80% of samples before the first cycle of prophylaxis and ~70% of samples before the second and subsequent prophylactic cycles, resulting in no significant decrease of these bacterial species after repeated quinolone exposure (28/35 samples vs 23/33 samples, P=0.4055). QR CNS and Enterococcus strains were detected in ~20% of samples before the first prophylaxis (Table 1). In contrast, the detection rate of these bacterial strains significantly increased at more than two cycles, even before quinolone exposure (8/35 samples vs 20/33 samples, P=0.0028). In addition, the detection frequency appeared to increase per the number of cycles (52.4% for cycle 2 and 75.0% for cycle >3), although no statistical significance was shown. QR CNS and Enterococcus strains were detected in ~70% of samples after the first prophylaxis, followed by detection in 95.2% of samples for cycle 2 and 100.0% for cycle >3. Vancomycin-resistant Enterococci (VRE) were not isolated in any of the samples.
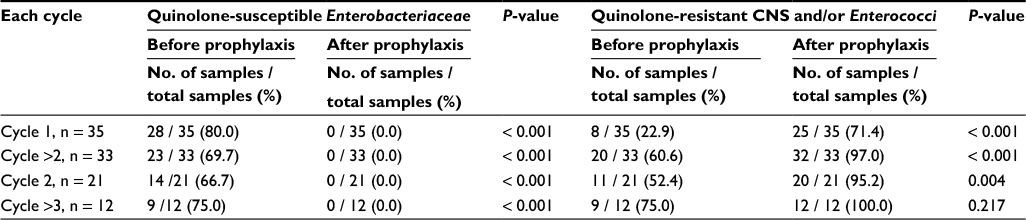 | Table 1 Detection of fluoroquinolone-susceptible and/or resistant bacteria in the fecal flora of hematological patients with neutropenia and repeated quinolone prophylaxis Abbreviation: CNS, coagulase negative staphylococci. |
Of the 33 samples from the cases with more than two courses of prophylaxis, QS Enterobacteriaceae strains and QR CNS and Enterococcus strains were detected before the prophylaxis in 23 and 20 samples, respectively. Next, we examined the predisposing factors for the detection of these bacteria before the prophylaxis of cycle >2 (Table 2). The duration of >31 days from the final antimicrobial use to sample collection was a factor significantly associated with the recovery of QS Enterobacteriaceae strains (P=0.0148). All 10 samples without the detection of QS Enterobacteriaceae strains were collected within 30 days from the final antimicrobial exposure. There were no significant factors associated with the detection of QR CNS and Enterococcus strains. However, these bacterial strains tended to be detected more frequently in the samples collected within 30 days from the final antimicrobial exposure. In fact, the detection frequency significantly decreased when collected after >31 days from the final antimicrobial exposure (16/20 samples vs 4/20 samples, P=0.0004).
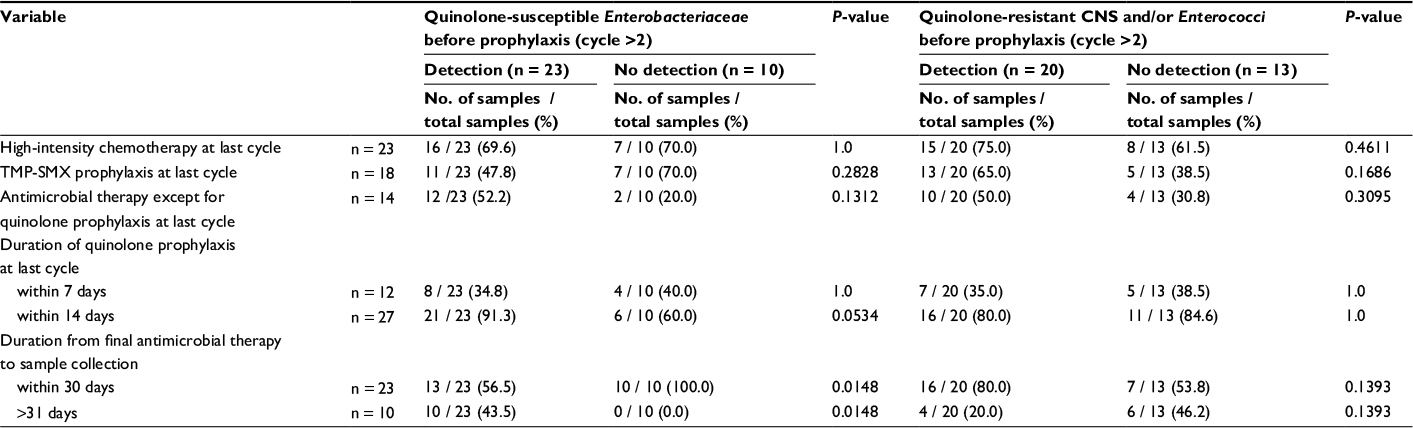 | Table 2 Related factors for the detection of quinolone-susceptible Enterobacteriaceae and quinolone-resistant CNS and/or Enterococci before the prophylaxis of cycle >2 Abbreviations: CNS, coagulase negative staphylococci; TMP-SMX, trimethoprim-sulfamethoxazole. |
Table 3 shows the detection history of QR Enterobacteriaceae strains at an individual level in seven patients receiving quinolone prophylaxis of cycle ≥2. All the QR Enterobacteriaceae strains were E. coli. Of the seven patients, six had QR E. coli, including QR ESBL-producing E. coli, before and/or after the first prophylaxis. Of the six patients, four (registration no. 3 [+4], 14 [+15, 16, and17], 20 [+21], and 37 [+38]) had a persistent detection of QR E. coli before and/or after the second prophylaxis (4/6 patients, 66.3%). In addition, three of the four patients had QR ESBL-producing E. coli. In two patients (registration no. 3 and 20), QR ESBL-producing E. coli isolated at the first prophylaxis were detected before and after the second prophylaxis. In the patient with registration no. 14, QR E. coli which emerged after the first prophylaxis disappeared from the sample after the second prophylaxis, followed by reemergence before the fourth prophylaxis. In the patient with registration no. 37, QR ESBL-producing E. coli isolated before the first prophylaxis were not detected after the first prophylaxis, followed by reemergence before the second prophylaxis.
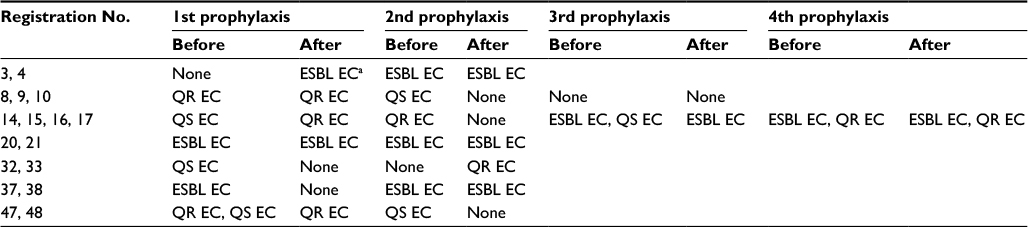 | Table 3 Detection history of fluoroquinolone-resistant and/or ESBL-producing E. coli in the fecal samples from patients with repeated quinolone prophylaxis. Note: aESBL EC strains were all resistant to quinolone. Abbreviations: ESBL, extended-spectrum β-lactamase; EC, Escherichia coli; QR, quinolone-resistant; QS, quinolone-susceptible; ESBL EC, ESBL-producing EC. |
Discussion
In the previous study,11 we concluded that quinolone prophylaxis did not significantly increase QR E. coli, while in the current study, a significant increase in quinolone resistance was observed. Although this appears to be contradictory and confusing, this is due to the evaluation of only E. coli in the previous study, as compared to that of all detected bacteria including CNS and Enterococci in the current study.
The recovery of QS Enterobacteriaceae was seen in ~70% of patients with more than two courses of quinolone prophylaxis (Table 1). In the recent report of de Lastours et al,13 it has been found that 70.8% (34/48 cases) of the cases exhibited reemergence of QS E. coli in the fecal flora after 28 days from final quinolone exposure. In de Lastours et al’s study,13 quinolones were administered to healthy volunteers without chemotherapy. In our study, all but one were subjected to chemotherapy for hematological diseases,11 which is expected to result in mucosal injure in the gut. As shown in Table 2, the intensity of chemotherapy was not associated with the reemergence of QS Enterobacteriaceae. Thus, original Enterobacteriaceae strains in human fecal flora could recover from quinolone exposure, irrespective of chemotherapy. Interestingly, the recovery of QS Enterobacteriaceae tended to be unsuccessful upon initiation of the next course of quinolone prophylaxis within 30 days from final antimicrobial exposure (Table 2).
For many cases in our study, QR CNS and Enterococcus strains persisted and were detected before receipt of more than two courses of quinolone prophylaxis (Table 1). On the contrary, the detection rate of these strains dramatically decreased when antimicrobials were administered at an interval of >31 days (Table 2). These findings mean that patients with hematological malignancies usually experience repeated chemotherapy with an interval of ≤1 month, and accordingly, quinolone prophylaxis also repeats at a similar interval, in many cases. Thus, quinolone prophylaxis for febrile neutropenia might allow QR CNS and Enterococcus strains to be detected in the fecal flora before receipt of more than two courses of prophylaxis. It has been reported by metagenome analysis that the composition of human gut microbiota may not completely recover, even after 6 months, from the initial quinolone exposure.14
In the previous report of this study, we showed the most frequency of 5% in the emergence of QR E. coli after quinolone prophylaxis.11 In contrast, in the studies conducted by European institutes, the detection rates of QR E. coli after quinolone prophylaxis were ~30%.15,16 Quinolone exposure in healthy volunteers also showed the new emergence of QR E. coli at a frequency of ~20% (9/48 cases).13 We have not resolved the mechanism of this difference in detection rates. de Lastours et al demonstrated that quinolone exposure did not induce resistant mutations on the quinolone-resistance-determining region (QRDR) genes (eg, gyrA or parC) of the same E. coli clones.13 The researchers have presumed the two following possibilities based on this result: first, the newly emergent QR E. coli strains after quinolone exposure were present at undetectable levels; and second, the exogenous acquisition of QR E. coli strains occurred. In our study, the footprint of QR E. coli strains at an individual level showed repeated appearance and disappearance in the same gut flora (Table 3). This finding suggests that QR E. coli strains always compete with other bacterial strains in the gut environment, resulting in that the acquisition or loss of dominance in the flora is repeated. This also suggests the possibility that the exogenous transmission of QR E. coli strains occurs during or at the interval of quinolone prophylaxis. Thus, in any case, the most relevant factor for the detection of QR E. coli, including ESBL-producing E. coli, seems to be the level of the endemic spread of QR E. coli. This claim could resolve the question mentioned above. In fact, QR E. coli were detected frequently in the blood isolates after quinolone prophylaxis in the highly endemic area of these bacteria.17,18 The detection rates of ESBL-producing E. coli, most of which are resistant to quinolones, vary across the world.19 The prevalence of ESBL-producing E. coli has been increasing in Japan, not only in the hospitals but also in the community.20,21 Therefore, the emergence of QR E. coli after quinolone prophylaxis may be found more frequently in the other regions of Japan than in our region.
Based on the above-mentioned consideration, the emergence of QR Enterococci after prophylaxis may be also due to the enrichment of the QR Enterococcus subpopulation already present in the initial gut flora. In this case, if VRE are present at undetectable levels in the initial flora, they may be persistently detected by the repeated prophylaxis, as predicted by our study, finally resulting in possible VRE bacteremia. We previously reported that the detection rate of Enterococcus strains in bacteremic isolates was significantly higher in patients with quinolone prophylaxis than in those without prophylaxis.22 Interestingly, the increase of bacteremic VRE isolates after quinolone prophylaxis was also reported from an institute in the United States.23 In the highly endemic areas of VRE, quinolone prophylaxis might affect the detection rates of their bacteremia in patients with febrile neutropenia.
There is a concern that the detection sensitivity of resistant bacteria might be less than ideal in our study. Therefore, a detection sensitivity limit might have affected the results, including the repeated appearance and disappearance of resistant bacteria in the patient’s gut flora.
The emergence of QR bacteria after quinolone prophylaxis for neutropenic patients would depend on the environmental spread of them. The previous colonization of QR bacteria before prophylaxis is also likely attributed to the endemic spread of them. Thus, the spread of resistant bacteria, particularly, QR E. coli including ESBL-producers and QR Enterococci including VRE, as a local factor may influence strategies toward the use of quinolone prophylaxis. Therefore, no conclusion can be made as to whether quinolone prophylaxis should be administered for all patients with neutropenia, from the aspects of the concerns for antibiotic resistance. Continued surveillance for the detection of resistant bacteria in both blood and stool cultures is warranted.
Disclosure
The authors did not receive any funding. The authors report no conflicts of interest in this work.
References
Viscoli C, Castagnola E. Treatment of febrile neutropenia: what is new? Curr Opin Infect Dis. 2002;15:377–382. | ||
Bucaneve G, Micozzi A, Menichetti F, et al. Levofloxacin to prevent bacterial infection in patients with cancer and neutropenia. N Engl J Med. 2005;353:977–987. | ||
Gafter-Gvili A, Fraser A, Paul M, Leibovici L. Meta-analysis: antibiotic prophylaxis reduces mortality in neutropenic patients. Ann Intern Med. 2005;142:979–995. | ||
Leibovici L, Paul M, Cullen M, et al. Antibiotic prophylaxis in neutropenic patients: new evidence, practical decisions. Cancer. 2006;107:1743–1751. | ||
Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2011;52:427–431. | ||
Pascoe J, Steven N. Antibiotics for the prevention of febrile neutropenia. Curr Opin Hematol. 2009;16:48–52. | ||
Cullen M, Baijal S. Prevention of febrile neutropenia: use of prophylactic antibiotics. Br J Cancer. 2009;101 (Suppl 1):S11–S14. | ||
Saito T, Yoshioka S, Iinuma Y, et al. Effects on spectrum and susceptibility patterns of isolates causing bloodstream infection by restriction of fluoroquinolone prophylaxis in a hematology-oncology unit. Eur J Clin Microbiol Infect Dis. 2008;27:209–216. | ||
Sohn BS, Yoon DH, Kim S, et al. The role of prophylactic antimicrobials during autologous stem cell transplantation: a single-center experience. Eur J Clin Microbiol Infect Dis. 2012;31:1653–1661. | ||
Verlinden A, Jansens H, Goossens H, et al. Clinical and microbiological impact of discontinuation of fluoroquinolone prophylaxis in patients with prolonged profound neutropenia. Eur J Haematol. 2014;93:302–308. | ||
Chong Y, Shimoda S, Yakushiji H, et al. Clinical impact of fluoroquinolone-resistant Escherichia coli in the fecal flora of hematological patients with neutropenia and levofloxacin prophylaxis. PLoS One. 2014;9:e85210. | ||
National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Susceptibility Testing. 14th Informational Supplement. Wayne, Pennsylvania: NCCLS; 2004. | ||
de Lastours V, Cambau E, Guillard T, Marcade G, Chau F, Fantin B. Diversity of individual dynamic patterns of emergence of resistance to quinolones in Escherichia coli from the fecal flora of healthy volunteers exposed to ciprofloxacin. J Infect Dis. 2012;206:1399–1406. | ||
Dethlefsen L, Relman DA. Incomplete recovery and individualized responses of the human distal gut microbiota to repeated antibiotic perturbation. Proc Natl Acad Sci U S A. 2011;108 (Suppl 1):4554–4561. | ||
Carratalà J, Fernandez-Sevilla A, Tubau F, Dominguez MÁ, Gudiol F. Emergence of fluoroquinolone-resistant Escherichia coli in fecal flora of cancer patients receiving norfloxacin prophylaxis. Antimicrob Agents Chemother. 1996;40:503–505. | ||
Perea S, Hidalgo M, Arcediano A, et al. Incidence and clinical impact of fluoroquinolone-resistant Escherichia coli in the faecal flora of cancer patients treated with high dose chemotherapy and ciprofloxacin prophylaxis. J Antimicrob Chemother. 1999;44:117–120. | ||
Ng ES-T, Liew Y, Earnest A, Koh LP, Lim S-W, Hsu LY. Audit of fluoroquinolone prophylaxis against chemotherapy-induced febrile neutropenia in a hospital with highly prevalent fluoroquinolone resistance. Leuk Lymphoma. 2011;52:131–133. | ||
Bow EJ. Fluoroquinolones, antimicrobial resistance and neutropenic cancer patients. Curr Opin Infect Dis. 2011;24: 545–553. | ||
Chong Y, Ito Y, Kamimura T. Genetic evolution and clinical impact in extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae. Infect Genet Evol. 2011;11:1499–1504. | ||
Chong Y, Yakushiji H, Ito Y, Kamimura T. Clinical and molecular epidemiology of extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae in a long-term study from Japan. Eur J Clin Microbiol Infect Dis. 2011;30:83–87. | ||
Chong Y, Shimoda S, Yakushiji H, et al. Community spread of extended-spectrum β-lactamase-producing Escherichia coli, Klebsiella pneumoniae and Proteus mirabilis: a long-term study in Japan. J Med Microbiol. 2013;62:1038–1043. | ||
Chong Y, Yakushiji H, Ito Y, Kamimura T. Clinical impact of fluoroquinolone prophylaxis in neutropenic patients with hematological malignancies. Int J Infect Dis. 2011;15:e277–e281. | ||
Craig M, Cumpston AD, Hobbs GR, Devetten MP, Sarwari AR, Ericson SG. The clinical impact of antibacterial prophylaxis and cycling antibiotics for febrile neutropenia in a hematological malignancy and transplantation unit. Bone Marrow Transplant. 2007;39:477–482. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.