")
Back to Journals » International Medical Case Reports Journal » Volume 14
Incidental Finding of an Aspergillus Pseudoaneurysm in the Ascending Aorta of an Immunocompetent Patient
Authors Ali R, Elhosiny A , Abualnaja S, Baslaim G
Received 1 October 2021
Accepted for publication 2 December 2021
Published 22 December 2021 Volume 2021:14 Pages 843—847
DOI https://doi.org/10.2147/IMCRJ.S340364
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Rola Ali,1– 3 Abdullah Elhosiny,1,2 Seraj Abualnaja,2,4 Ghassan Baslaim2,4
1Department of Internal Medicine, Dr. Soliman Fakeeh Hospital, Jeddah, Kingdom of Saudi Arabia; 2Department of Medicine, Fakeeh College of Medical Sciences, Jeddah, Kingdom of Saudi Arabia; 3Department of Medicine, An-Najah National University, Nablus, West Bank, Palestine; 4Department of Cardiology, Cardiothoracic and Vascular Surgery, Dr. Soliman Fakeeh Hospital, Jeddah, Kingdom of Saudi Arabia
Correspondence: Rola Ali
Department of Internal Medicine, Dr. Soliman Fakeeh Hospital, Jeddah, Kingdom of Saudi Arabia
Tel +970 592192425
Email [email protected]
Abstract: Pseudoaneurysms of the ascending aorta are rare, yet they are life-threatening conditions and usually associated with poor outcomes due to insidious presentation. Many different etiologies have been associated with aortic pseudoaneurysms including; atherosclerosis, infections, connective tissue disorders, and traumatic causes. In addition, aortic pseudoaneurysms have been reported following thoracic surgeries, including aortic valve replacements, aortic dissection repair, and coronary artery bypass grafting. Aspergillus is amongst the infectious etiologies of pseudoaneurysms. Aspergillus species is a ubiquitous mold (fungus) that is mostly harmless but may result in serious illnesses in immunocompromised hosts with hematologic neoplasms, neutropenia, or immunodeficiency syndromes. In this paper, we report a case of an ascending aortic pseudoaneurysm caused by Aspergillus infection. To our knowledge, this is an exceptionally rare case diagnosed incidentally in an immunocompetent patient, who is surgically free and without any pre-existing risk factors.
Keywords: aspergillosis, aorta, pseudoaneurysm
Introduction
Aspergillus species are saprophytic, spore-forming fungi. They usually exist in soil, water and decaying vegetation. Inhalation of the airborne conidia results in a variety of clinical syndromes, ranging from asymptomatic colonization to disseminated infection.1 Invasive Aspergillosis is an opportunistic infection that mainly occurs in immunocompromised individuals.2 Most patients with invasive aspergillosis are neutropenic or have an underlying hematological and immunodeficiency disorders.3 Invasive Aspergillosis can infect virtually any organ, including the aorta, resulting in pseudoaneurysms. Aortic pseudoaneurysms, or false aneurysms, are rare, life-threatening conditions that represent an abnormal outpouching at the site of arterial wall damage. Unlike in true aneurysms, which involve the three layers of the vessel wall, pseudoaneurysms spare the adventitia layer, resulting in leakage of blood and a contained hematoma.4 Aspergillus involvement of the aorta, however, is a rare event, and despite treatment with antifungal therapy and surgery, it can be fatal and usually carries a poor prognosis.2
Most cases of aspergillus aortitis have been reported in patients with a history of cardiothoracic surgery.2 We report a case of mycotic aortic pseudoaneurysm caused by aspergillus, that was diagnosed incidentally in an immunocompetent surgically free patient, and who was treated successfully with antifungal agents following initial surgical debridement and repair.
Case Report
A 45-year-old white male, presented to the clinic for follow-up on a pulmonary embolism episode, which he developed one year ago. A follow-up pulmonary Computed tomography (CT) angiogram was done and showed no evidence of pulmonary embolism, but a new ascending aortic pseudoaneurysm was found with a surrounding hematoma. After reviewing his previous CT scans, it appeared that the patient was misdiagnosed a year ago at the referring hospital as a case of pulmonary embolism and he was started on oral anticoagulation therapy. According to his past medical history with regards to infections, the patient was once hospitalized for uncomplicated Klebsiella community acquired pneumonia, 3 years ago, where he completely recovered after 5 days of a hospital admission. He is not diabetic, hypertensive, nor dyslipidemic. The patient has never had any joint pain, skin rashes, weakness or neurological symptoms, constitutional symptoms, trauma, nor any past surgeries. The patient denied humidity, moisture, or dust in his residential environment. He is an employee at a water desalination company; however, he did not report any water damage, leaks, or malfunction in the workplace. To the patient’s knowledge, no similar symptoms or previous fungal infections were reported by his colleagues and friends, and his family history is unremarkable. He has not traveled in the last 10 years; he is a 14-pack year ex-smoker, and he denied any extra-marital sexual contact.
On physical examination, poor oral hygiene and dental caries were noted. He had a body mass index of 24.2. There was a blood pressure (BP) difference between his upper limbs, measuring 120/83 mmHg on the left and 107/46 mmHg on the right. His pulses were also weaker on the right side of his body compared to his left including both femoral and radial pulses. This pulse asymmetry and difference in BP readings bilaterally raised concerns for a structural vascular problem, preventing smooth blood flow through the vessels, necessitating further evaluation in the patient.
The patient’s laboratory investigations revealed a C-reactive protein of 13 mg/L, procalcitonin of 0.1 ng/mL, and erythrocyte sedimentation rate of 10 mm/hr. The reminder of his laboratory work that included complete blood count, cardiac enzymes, brain natriuretic peptide, renal function tests, liver function tests, and coagulation profile were all within normal limit. Electrocardiogram showed normal sinus rhythm. Further workup for the incidental pseudoaneurysmal finding such as, autoimmune profile (antinuclear antibodies, anti-neutrophilic cytoplasmic antibody, anti-double stranded DNA antibodies, Complement 3, Complement 4), and precipitating infections (human immunodeficiency virus, syphilis testing, blood and urine bacterial and mycological cultures) were all negative.
Imaging workup for the patient included chest x-ray, which revealed increased transverse cardiac diameter, obliterated right cardiophrenic (CP) angle suggesting mild right pleural effusion, and clear left CP angle. The lungs were clear without any nodules or consolidations. Transthoracic and trans-esophageal echocardiograms revealed normal left ventricular systolic function with EF 55%, moderate tricuspid regurgitation, and no valvular vegetation. CT angiography of the brain showed no evidence of aneurysms, vascular malformations, or space occupying lesions. CT angiography of the chest (Figures 1 and 2), however, revealed a focal pseudo aneurysm (2.4×1.5 cm) located in the right anterior wall of the ascending thoracic aorta, 2.5 cm superior to the aortic valve, with the neck of the pseudoaneurysm measuring 1.1 cm. Additionally, there was an associated large anterior mediastinal and intra-pericardial hematoma with pericardial thickening and a mild hemorrhagic pericardial effusion.
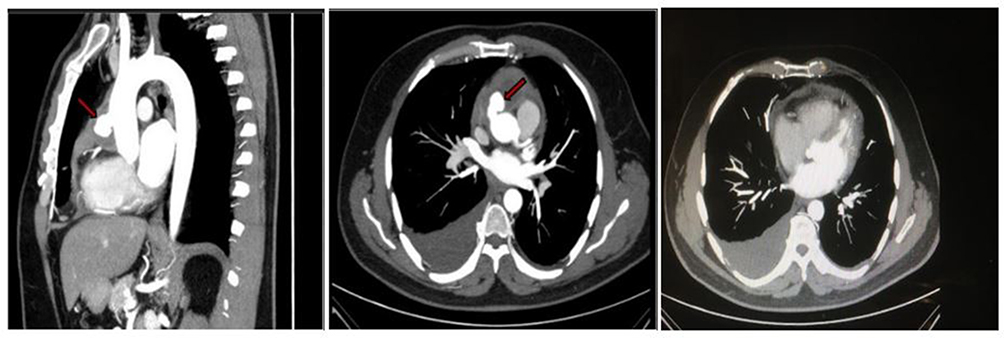 |
Figure 1 CT angiogram of the aorta with contrast revealing the pseudoaneurysm measuring 2.4×1.5 cm (as pointed by the arrow). |
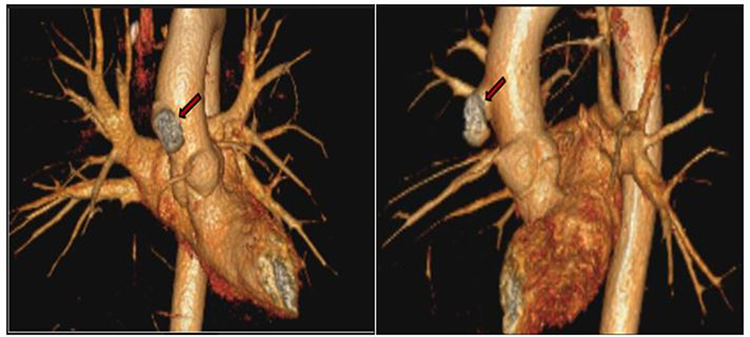 |
Figure 2 3-D CT angiogram of the aorta and its major branches, with arrow pointing towards the pseudoaneurysm. |
The patient was admitted to the hospital to complete the work up, and subsequently he underwent surgical ascending aortic repair and pericardial debridement (Figure 3). Intraoperatively, a thick and adherent pericardium was found without a definite tissue plane. Contained cheesy and hematoma was found over the right ventricle and ascending aorta. The pseudoaneurysmal defect was patched repair using bovine pericardial material. A tissue biopsy was taken and sent for microbiological and histobiological analysis (Figure 4). Hematoxylin and Eosin stain and methenamine silver stain revealed fungal organisms with thin separate hyphae and regular branching, morphologically consistent with Aspergillus species. As revealed in the previous labs and imaging results, the patient had no evidence of disseminated Aspergillosis. The patient’s postoperative course was uneventful, and he was discharged on Voriconazole 200 mg PO bid for a period of 1 year after which he completely improved.
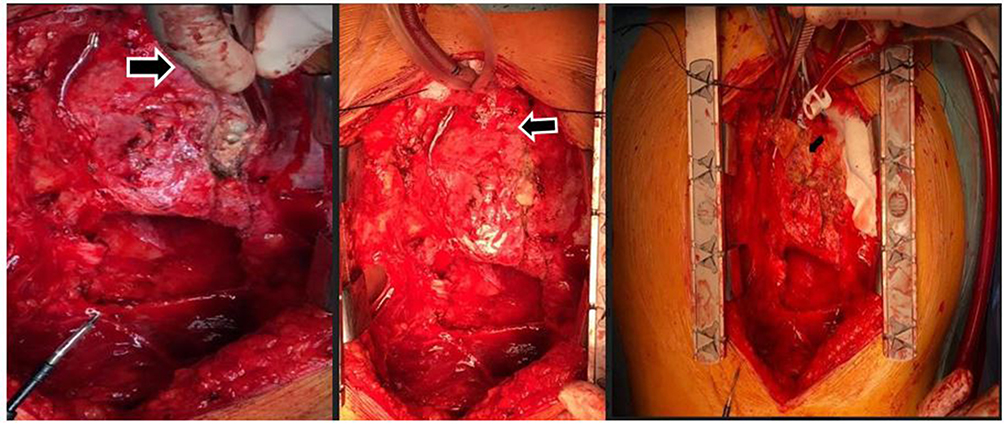 |
Figure 3 Intraoperative view – revealing dense pericardial adhesions, purulent material (indicated by the arrow) over the aortic root and anterior wall of the right ventricle, and ascending aortic pseudoaneurysm. |
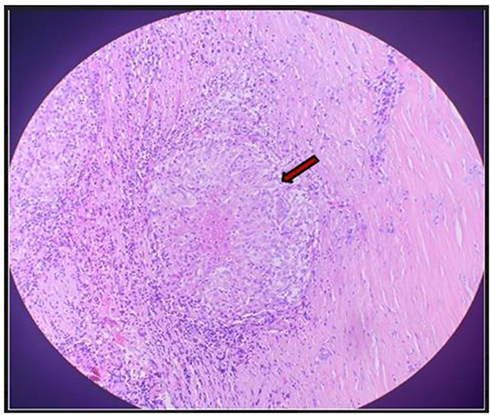 |
Figure 4 Histopathology view of the biopsy revealing necrotic granulomatous lesion (arrow pointing towards the necrotic granuloma) – with multinucleated giant cells surrounding central necrosis. |
Discussion
Pseudoaneurysms, or false aneurysms, of the aorta result from rupture of the intima and media layers of the vessel, and they remain contained by the adventitia and surrounding structures of the mediastinum4 The incidence of ascending aortic pseudoaneurysms is <1%.5 Aortic pseudoaneurysms may occur as a consequence of atherosclerosis,6 infections such as syphilis and tuberculosis, genetic disorders, blunt thoracic trauma,7 or cardiothoracic surgeries.4 It has been reported that aortic pseudoaneurysm has also occurred as a rare complication of pulmonary cancer.8 Although rare, these pseudoaneurysms almost always life-threatening as they result in hemorrhage and other serious complications; thus, timely diagnosis and prompt surgical intervention is necessary.9 Pseudoaneurysms larger than 55 mm in diameter and those associated with sepsis carry a poor prognosis.10
Aspergillosis is an opportunistic infection that mainly affects immunocompromised patients, such as those being treated for leukemia or lymphoma. Its mode of entry into the body is by inhalation as airborne spores, with the primary site of infection usually being the lung. Pulmonary involvement may vary from benign colonization in an immunocompetent host to aspergilloma, allergic bronchopulmonary aspergillosis, or invasive disease in an immunocompromised patient. Involvement of non-pulmonary sites includes: the skin, para-nasal sinuses, and less frequently the central nervous system.1
Aspergillus aortitis, although a rare condition, can occur in transplant patients, those receiving chemotherapy, or in immunocompetent patients following cardiac surgery.11 Our case was particularly exceptional and unusual because the patient was immunocompetent, as his serum immunoglobulin levels were found to be normal during his follow-up, and he has never been on any immunosuppressive medications. In addition, his history is free of any chronic illnesses, hematologic disorders, neutropenia, or previous surgeries. The patient’s condition was probably occupational, acquired from his workplace, given the ubiquitous nature of Aspergillus species in moist environments. The presence of Aspergillus aortitis in our patient has led to speculations, as whether water desalination companies may serve as a transmission route for potentially pathogenic Aspergillus species. Relatively few studies have investigated the presence of fungi in water distribution systems. Although limited knowledge is known about this kind of occupational exposure, it may be a potential health risk that may be worth more attention. His immunocompetent state has likely improved his survival and response to therapy.
Conclusion
In conclusion, we present a case of ascending aortic pseudoaneurysm due to aspergillus infection that was diagnosed incidentally in an immunocompetent and surgically free patient. Survival of patients with Aspergillus aortitis and successful management is dependent on rapid and early diagnosis and aggressive medical treatment and surgical intervention.
Abbreviations
CT, computed tomography; BP, blood pressure; CP, cardiophrenic.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report. As per institutional policy, no IRB is needed.
Disclosure
Dr Seraj Abualnaja's current affiliation is Department of Cardiology, International Medical Center, Jeddah, Kingdom of Saudi Arabia. The authors declare no conflicts of interest.
References
1. Soubani AO, Chandrasekar PH. The clinical spectrum of pulmonary aspergillosis. Chest. 2002;121(6):1988–1999. doi:10.1378/chest.121.6.1988
2. Elmezayen R, Youssef D. Aspergillus aortitis: a case with near-complete occlusion of the brachial artery and large ascending aortic mycotic pseudoaneurysm in an immunocompetent patient. J Bacteriol Mycol Open Access. 2016;3(4):292–295.
3. Watanabe I, Nakayama T, Yamada E, Tsukino M, Hayashi E. Invasive aspergillosis in the aortic arch with infectious Aspergillus lesions in pulmonary bullae. Med Mycol Case Rep. 2015;7:15–19. doi:10.1016/j.mmcr.2014.12.001
4. Garisto JD, Medina A, Williams DB, Carrillo RG. Surgical management of a giant ascending aortic pseudoaneurysm. Tex Heart Inst J. 2010;37(6):710–713.
5. Duraes AR, Schonhofen IS, Freitas CPA, Bitar YDSL. Giant pseudoaneurysm of ascending aorta. J Gen Emerg Med. 2017;3:2.
6. Lee S, Cho SH. Huge ascending aortic pseudoaneurysm caused by a penetrating atherosclerotic ulcer. Circ Cardiovasc Imaging. 2008;1(3):e19–20. doi:10.1161/CIRCIMAGING.108.788133
7. Ozaydin M, Varol E, Altınbaş A, Yavuz T, Ibrişim E. Incidental diagnosis of pseudoaneurysm of the thoracic aorta: an unusual late presentation. SDÜ Tip Fakültesi Dergisi. 2006;13(4):32–34.
8. Lu YQ, Yao F, Shang AD, Pan J. Pseudoaneurysm of the aortic arch: a rare case report of pulmonary cancer complication. Medicine (Baltimore). 2016;95(31):e4457. doi:10.1097/MD.0000000000004457
9. Wang W, Liu X, Lu M. Case-report: endovascular treatment of aortic pseudo-aneurysm caused by Fishbone. J Cardiothorac Surg. 2015;10:94. doi:10.1186/s13019-015-0304-z
10. Aggarwal A, Banga S, Mungee S. Ascending aortic pseudoaneurysm: sleeping giant arises in 3rd decade after surgery. Tex Heart Inst J. 2016;43(4):374–375. doi:10.14503/THIJ-14-4875
11. Rocco JM, Benson MK. Aspergillus aortitis in an immunocompetent patient presenting with acute endophthalmitis. Infect Dis Rep. 2018;10(2):7750. doi:10.4081/idr.2018.7750
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.