")
Back to Journals » International Journal of Women's Health » Volume 6
Incidence rate of ovarian cancer cases in Saudi Arabia: an observational descriptive epidemiological analysis of data from Saudi Cancer Registry 2001–2008
Authors Alghamdi I , Hussain I, Alghamdi M, Alghamdi M , Dohal A, El-Sheemy M
Received 6 March 2014
Accepted for publication 10 April 2014
Published 25 June 2014 Volume 2014:6 Pages 639—645
DOI https://doi.org/10.2147/IJWH.S63636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Ibrahim G Alghamdi,1,2 Issam I Hussain,1 Mohamed S Alghamdi,3 Mansour M Alghamdi,4 Ahlam A Dohal,4 Mohammed A El-Sheemy5
1School of Life Sciences, University of Lincoln, Brayford Pool, Lincoln, UK; 2Al-Baha University, Kingdom of Saudia Arabia; 3Ministry of Health, General Directorate of Health Affairs, Al-Baha, Kingdom of Saudi Arabia; 4King Fahad Specialist Hospital–Dammam, Kingdom of Saudi Arabia; 5Department of Research and Development, Lincoln Hospital, United Lincolnshire Hospitals, National Health Service Trust, Lincoln, UK
Purpose: This study provides descriptive epidemiological data, such as the percentage of cases diagnosed, crude incidence rate (CIR), and age-standardized incidence rate (ASIR) of ovarian cancer in Saudi Arabia from 2001–2008.
Patients and methods: A retrospective descriptive epidemiological analysis of all ovarian cancer cases recorded in the Saudi Cancer Registry (SCR) from January 2001–December 2008 was performed. The data were analyzed using descriptive statistics, analysis of variance tests, Poisson regression, and simple linear modeling.
Results: A total of 991 ovarian cancer cases were recorded in the SCR from January 2001–December 2008. The region of Riyadh had the highest overall ASIR at 3.3 cases per 100,000 women, followed by the Jouf and Asir regions at 3.13 and 2.96 cases per 100,000 women. However, Hail and Jazan had the lowest rates at 1.4 and 0.6 cases per 100,000 women, respectively. Compared to Jazan, the incidence rate ratio for the number of ovarian cancer cases was significantly higher (P<0.001) in the Makkah region at 6.4 (95% confidence interval [CI]: 4.13–9.83), followed by Riyadh at 6.3 (95% CI: 4.10–9.82), and the eastern region of Saudi Arabia at 4.52 (95% CI: 2.93–6.98). The predicted annual CIR and ASIR for ovarian cancer in Saudi Arabia could be defined by the equations 0.9 + (0.07× years) and 1.71 + (0.09× years), respectively.
Conclusion: We observed a slight increase in the CIRs and ASIRs for ovarian cancer in Saudi Arabia from 2001–2008. Riyadh, Jouf, and Asir had the highest overall ASIR, while Jazan and Hail had the lowest rates. Makkah, Riyadh, and the eastern region of Saudi Arabia had the highest incidence rate ratio for the number of ovarian cancer cases. Further analytical studies are required to determine the potential risk factors of ovarian cancer among Saudi women.
Keywords: cancer epidemiology, ovarian cancer, Saudi Cancer Registry, incidence rate
Introduction
Ovarian cancer is the eighth most common type of cancer among women in the world. Furthermore, it is the seventh leading cause of cancer-related mortality with a severe impact on socioeconomic and community health, globally.1–4 Compared to other types of gynecologic malignancies, ovarian cancer has the highest mortality rate in developed countries worldwide.5–7 The American Cancer Society estimated that 22,240 women were going to be diagnosed with ovarian cancer in the US in 2013, while the number of ovarian cancer-related deaths was estimated to be 14,230.8 Moreover, ovarian cancer was estimated to account for 3% of all cancers among women. Currently, the lifetime risk of developing ovarian cancer is approximately 1 in 72, while the lifetime risk of dying from ovarian cancer is approximately 1 in 100.8
The International Agency for Research on Cancer estimated that the age-standardized incidence rate (ASIR) and the age-standardized mortality rate for ovarian cancer in Saudi Arabia in 2012 was 3.4 per 100,000 women and 2.5 per 100,000 women, respectively.9 Furthermore, the registry of the King Faisal Specialist Hospital and Research Centre (2011) recorded 1510 cases of ovarian cancer with admission to the hospital from 1975–2011.10 In 2008, data from the Saudi Cancer Registry (SCR) suggested that ovarian cancer ranked seventh in cancer incidence among Saudi women.11 The ASIR of ovarian cancer in Saudi Arabia is low in comparison with other countries in the Arabian Gulf. For example, in 2012, the reported ASIR of ovarian cancer for Oman, United Arab Emirates, Kuwait, Qatar, and Bahrain was 10.2, 6.4, 4.7, 4.6, and 4.4 per 100,000 women, respectively.9
Despite a lack of data on the geographic distribution of ovarian cancer among women in Saudi Arabia, we aimed to investigate and describe the crude incidence rate (CIR) and ASIR of ovarian cancer cases by providing an observational descriptive epidemiological analysis of cancer of the ovary while considering spatial/temporal distribution of recorded cases in the SCR from 2001–2008.12
Materials and methods
A retrospective descriptive epidemiological study of the ovarian cancer cases and diagnosed in Saudi Arabia from January 2001–December 2008 was performed. The data of reports regarding cancer incidence in Saudi Arabia are publicly available and easily accessible to be downloaded from the website of SCR. The main mission of SCR is to gather, register, and provide high standard data for cancer incidence stratified by region, age group, and year of diagnosis. Furthermore, the published reports by SCR would be available to policy makers, cancer researchers, treating physician, cancer control, and prevention programs. Therefore, no ethical approval was required for this observational descriptive epidemiological study. The data source for this study was the SCR, a population-based registry established in 1992 by the Ministry of Health of Saudi Arabia. The data cannot be obtained directly from the SCR, but it is published in reports. However, no data was available from 1994–2000 and the latest published report of the SCR was available in 2008.
Since 2001, the SCR has been providing reports on the patterns of cancers in Saudi Arabia with the primary objective of defining the population-based incidence of the disease. Currently, there are comprehensive reports for each of the 13 administrative regions of Saudi Arabia. Each report discusses the number and percentage of cases diagnosed, the CIR, and the ASIR (adjusted by region and year of diagnosis) of cancer from 2001–2008. The current study utilized the SCR reports to gather all the information on ovarian cancer with the aim of presenting the descriptive epidemiology of ovarian cancer in Saudi Arabia.
Data were analyzed using the Statistical Package for the Social Sciences version 20.0 (IBM Corporation, Armonk, NY, USA). The descriptive analysis of the epidemiological data of ovarian cancer was performed by calculating the overall percentage of ovarian cancer cases, CIR, and the ASIR adjusted by the age group, region, or year of diagnosis. The analysis of variance (ANOVA) test was performed to determine the effect of the geographical area and the year of diagnosis on CIR and ASIR.13 Simple linear regression was used separately with an independent variable (year of diagnosis) to predict the annual CIR and the ASIR of ovarian cancer among Saudi women.14 In addition, the Poisson regression was conducted to calculate the incidence rate ratio (IRR) of ovarian cancer cases for each region of Saudi Arabia.
Results
A total of 991 ovarian cancer cases were recorded in the SCR from January 2001–December 2008. The percentage of women diagnosed with ovarian cancer increased slightly from 2001–2008. Figure 1A and B shows that there were 101 new ovarian cancer cases in 2001 (3.7% of all cancer cases diagnosed in women; 95% confidence interval [CI]: 1.7%–5.7%) and 96 in 2002. This indicates a 0.4% decline in cases. By 2005, 136 ovarian cancer cases were reported, corresponding to a 0.2% increase. The number of ovarian cancer cases diagnosed annually remained slightly high, but the percentages were stable in 2005 and 2008 at 3.5%.
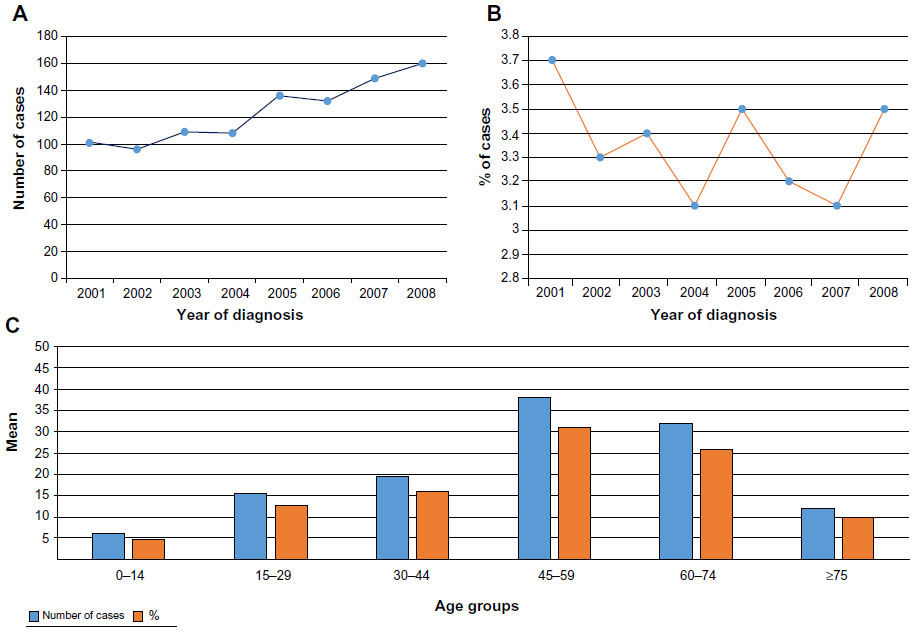 | Figure 1 Number and percentage of ovarian cancer cases (A and B) in Saudi Arabia from 2001–2008. Overall number and percentage of ovarian cancer cases’ distribution by age group (C) in Saudi Arabia from 2001–2008. |
The average number and percentage of ovarian cancer cases diagnosed from 2001–2008, adjusted by age group, was calculated using the data from the SCR (Table 1 and Figure 1C). Women aged 45–59 years were most frequently diagnosed with ovarian cancer followed by those aged 60–74 years, representing 31% (38 cases) and 26.0% (33 cases) of the total number of ovarian cancer cases. In contrast, the younger (0–44 years) and older (75 years and over) groups recorded the lowest overall number and percentage of cases.
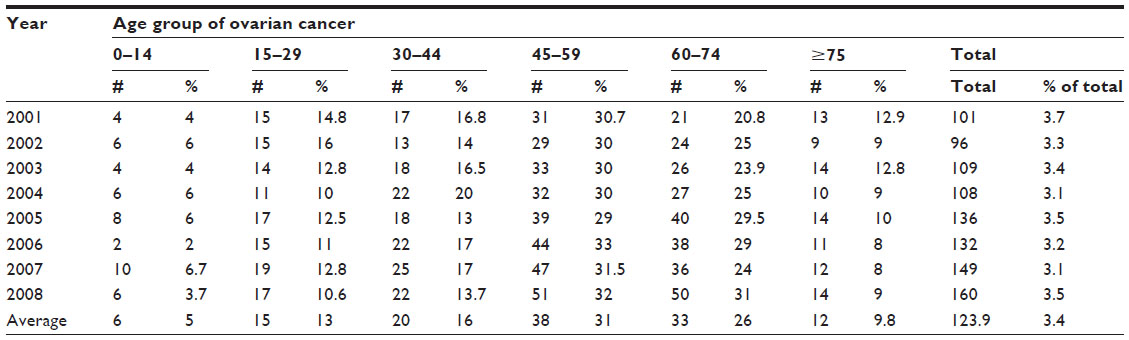 | Table 1 Ovarian cancer cases distribution by age group in Saudi Arabia from 2001–2008 |
The CIRs per 100,000 women, adjusted for the year of diagnosis, indicated a steady increase in ovarian cancer cases in Saudi Arabia from 2001–2008. As shown in Table 2 and Figure 2A, a CIR of 1.3 (95% CI: 0.6–2.0) ovarian cancer cases per 100,000 women was estimated in 2001; and a CIR of 1.8 (95% CI: 0.9–2.7) cases per 100,000 women in 2008. The latter CIR was the highest rate observed, but it was not statistically significantly different compared to the other years (F[7, 96]=0.106; P>0.05). Linear regression analysis suggested that the annual increase of CIR for ovarian cancer in Saudi Arabia can be predicted by the equation 0.9 + (0.07× years), which indicates that the CIR of ovarian cancer increased on average by 0.9 cases per 100,000 Saudi women per year.
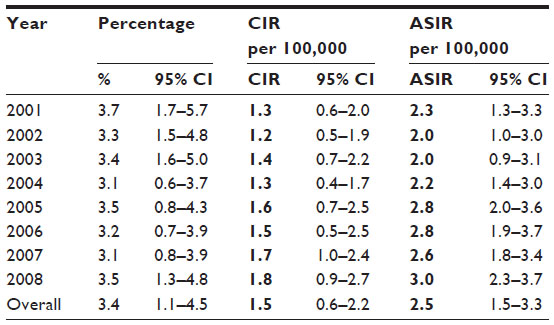 | Table 2 CI for %, CIR, and ASIR of ovarian cancer cases in Saudi Arabia from 2001–2008 |
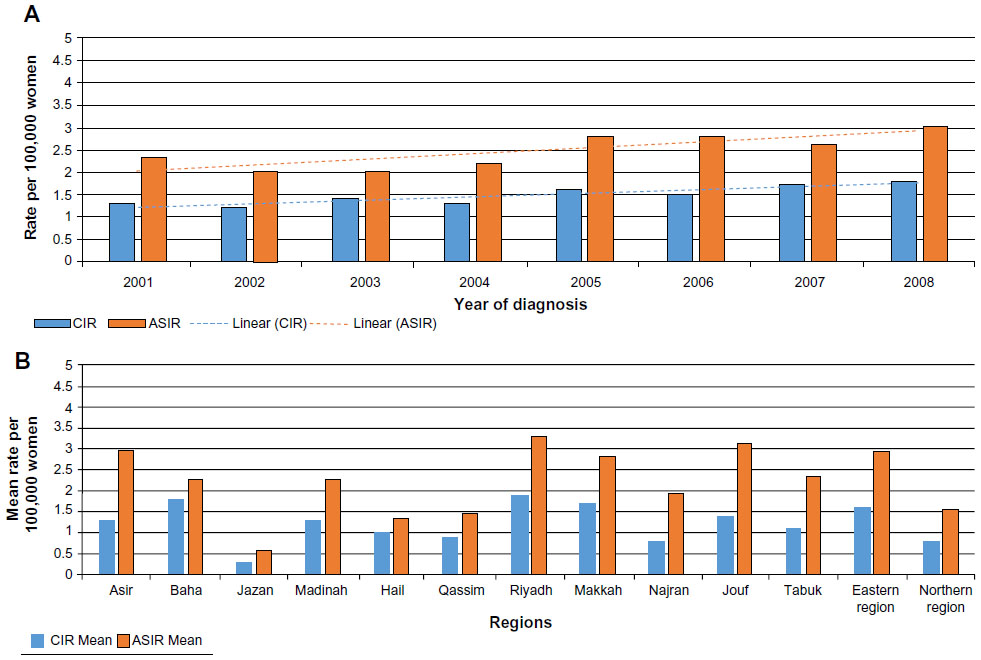 | Figure 2 CIR and ASIR of ovarian cancer cases (A) in Saudi Arabia from 2001–2008. Overall CIR and ASIR of ovarian cancer cases’ distribution by region (B) in Saudi Arabia from 2001–2008. |
Table 3 and Figure 2B show the overall CIR of ovarian cancer per 100,000 women, adjusted for the region of Saudi Arabia from 2001–2008. The region of Riyadh had the highest overall CIR for ovarian cancer at 1.9 (95% CI: 1.6–2.2) cases per 100,000 women, followed by the regions of Baha and Makkah at 1.8 (95% CI: 1.0–2.6) and 1.7 (95% CI: 1.4–3.0) cases per 100,000 women, respectively. The ANOVA test revealed that the incidence rates of ovarian cancer were significantly higher for these three regions compared to the other regions of Saudi Arabia (F[12, 91]=4.988; P<0.001). Furthermore, Jazan (95% CI: 0.1–0.5), Najran (95% CI: 0.3–1.3), and the northern region of Saudi Arabia (95% CI: 0.3–1.3) had the lowest average CIRs for ovarian cancer at 0.3, 0.8, and 0.8 cases per 100,000 women, respectively.
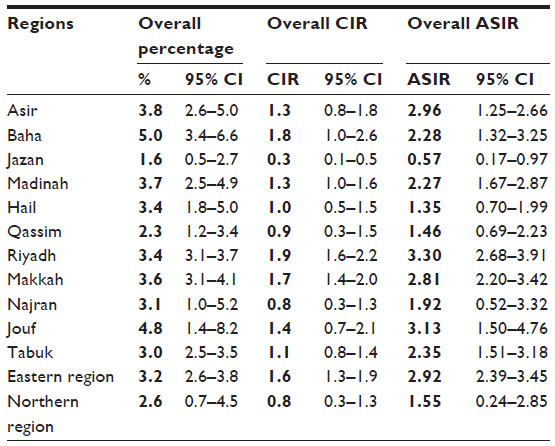 | Table 3 CI for overall percentage, CIR, and ASIR of ovarian cancer cases in the regions of Saudi Arabia from 2001–2008 |
The overall ASIRs per 100,000 women were calculated for all of the SCR reports on the basis of (Segi) world standard for intermediate-age populations (Table 4). This standard can be used in the direct method of standardization to calculate the ASIR. It allows to control the confounding effects of age when making a comparison between populations with different age structures.15,16 Therefore, the ASIR of ovarian cancer per 100,000 women, adjusted for the year of diagnosis in Saudi Arabia, from 2001–2008, is displayed in Table 2 and Figure 2A. The SCR reports indicated a slight increase in the number of cases of ovarian cancer diagnosed from 2001–2008, with the highest ASIR of three cases per 100,000 women recorded in 2008 (95% CI: 2.3–3.7). Linear regression showed that the annual increase in ASIR of ovarian cancer in Saudi Arabia can be predicted by the equation 1.71 + (0.09× years), which suggests that the ASIR of ovarian cancer increased by a predicted average of 0.09 cases per 100,000 women per year. Furthermore, Riyadh had the highest overall ASIR for ovarian cancer at 3.3 (95% CI: 2.68–3.91) cases per 100,000 women, followed by Jouf and Asir at 3.13 (95% CI: 1.5–4.76) and 2.96 (95% CI: 1.25–2.66) cases per 100,000 women, respectively (Table 3 and Figure 2B). The ANOVA test indicated that the ASIRs of ovarian cancer were significantly higher for these three regions compared to other provinces of Saudi Arabia (F[12, 91]=4.100; P<0.001). Furthermore, Jazan, Najran, and the northern region of Saudi Arabia had the lowest average ASIRs for ovarian cancer at: 0.3 (95% CI: 0.1–0.5); 0.8 (95% CI: 0.3–1.3); and 0.8 (95% CI: 0.3–1.3) cases per 100,000 women, respectively.
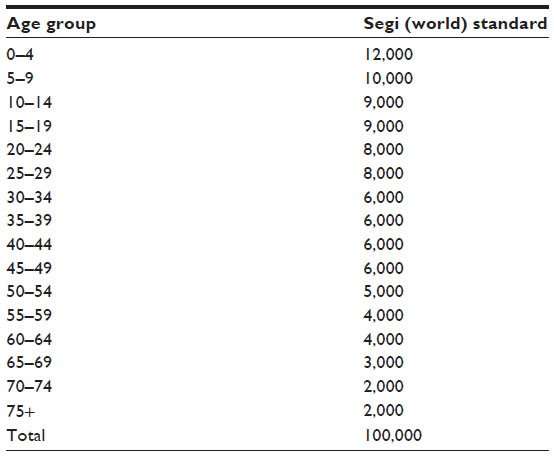 | Table 4 Segi (world) standard for making comparisons with intermediate-age population (Segi, 1960) |
The Poisson regression was conducted to calculate the IRR of ovarian cancer cases for the different regions of Saudi Arabia. The model was statistically significant (LRχ2[15]=850.6; P<0.001). As shown in Table 5, Jazan was used as the reference region for comparing the other provinces of Saudi Arabia. The IRRs were significantly higher (P<0.001) for Makkah at 6.4 (95% CI, 4.12–9.83), Riyadh at 6.3 (95% CI, 4.10–9.82), and the eastern region of Saudi Arabia at 4.52 (95% CI, 2.93–6.98).
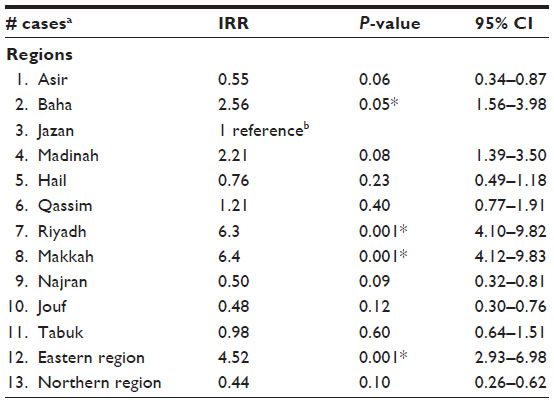 | Table 5 Poisson regression model to calculate the IRR and check if there is an effect due to geographical area |
The differences in the CIRs and ASIRs between 2001–2008 were calculated to investigate the pattern of ovarian cancer in the different regions of Saudi Arabia (Table 6). The greatest changes in percentages and rates were observed in the region of Baha (6.4%; CIR, 2.9; ASIR, 3.6). However, the CIR and ASIR for all regions, with the exception of Baha, were under the predicted values based on the equations for the linear regression, ie, 0.9 + (0.07×8 years) = 1.46 per 100,000 women for the CIR and 2.43 + (0.09×8 years) = 2.43 per 100,000 women for the ASIR. The smallest changes in the CIR and ASIR were observed in the regions of Najran (−5.8%, −1.3 CIR, −4.1 ASIR), and Hail (−2.9%; CIR, −0.5; ASIR, −1.1). The percentage of ovarian cancer cases decreased by 5.8% and 2.9% in Najran and Hail, respectively. Furthermore, in the Najran region the CIR and ASIR decreased by 1.3 and 4.1 cases per 100,000 women, respectively; whereas, in the Hail region the CIR decreased by 0.5 case and the ASIR decreased by 1.1 cases per 100,000 women. However, these data indicate downtrending rates for both regions from 2001–2008.
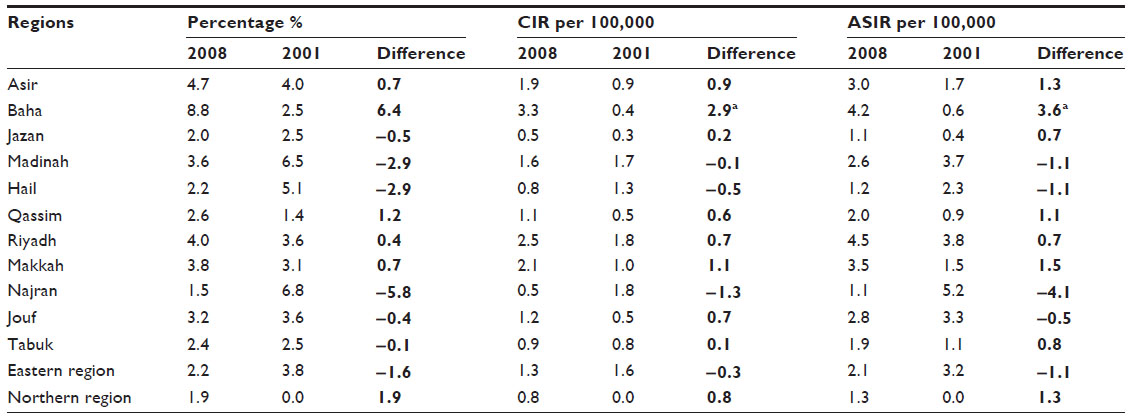 | Table 6 Differences in the percentage, CIR, and ASIR of ovarian cancer cases in the regions of Saudi Arabia from 2001–2008 |
Discussion
Ovarian cancer is an important malignancy in women with regards to its incidence and mortality. The current study focused on the CIR and ASIR of ovarian cancer in different regions of Saudi Arabia from 2001–2008. To the best of our knowledge, this is the first geographical descriptive epidemiological study of ovarian cancer cases in Saudi Arabia. It presents the pattern and the trend of the disease from 2001–2008. In addition, this study provides an important explanation for the observed trend, thereby highlighting the significance of this disease.
The results indicated that the regions of Riyadh, Jouf, and Asir had the highest overall ASIRs for ovarian cancer in Saudi Arabia from 2001–2008; however, the overall ASIRs of these regions did not increase above the expected levels. In contrast, the regions of Jazan and Hail had the lowest overall ASIRs of ovarian cancer in Saudi Arabia from 2001–2008. Women >44 years of age were the most affected by ovarian cancer in the different provinces of Saudi Arabia. Furthermore, the Poisson regression showed that the IRR of ovarian cancer cases in the regions of Riyadh and Makkah was more than six times higher than the reference region of Jazan.
This study also reported the changes in the percentage of ovarian cancer cases diagnosed, CIR, and ASIR from 2001–2008. The Baha region had the largest differences in CIR and ASIR, which were both higher than their predicted values for the years 2001–2008. These differences in rates suggest that, from 2001–2008, more women in the region of Baha were affected by ovarian cancer than predicted. In contrast, the rates of ovarian cancer decreased in the regions of Najran and Hail. These regions reported the lowest changes in the respective study outcomes, with a downtrend observed in the CIR and ASIR from 2001–2008.
However, with the exception of the SCR reports, only limited information was available on the incidence of ovarian cancer in Saudi Arabia. This study intended to explore the real pattern of ovarian cancer in different regions of Saudi Arabia from 2001–2008. The findings of this study may be useful for researchers and decision makers in the field of medicine and health care administration in Saudi Arabia as they can provide opportunities for generating hypotheses about the potential risk factors of ovarian cancer in the highest affected regions. Furthermore, the findings can be utilized to conduct analytical epidemiological studies that aim to identify the relationship between exposure and disease.13 The availability of data from the SCR reports can also encourage further descriptive epidemiological studies of other types of cancers among the Saudi population.
Conclusion
The epidemiological analysis of the reports by the SCR, from 2001–2008, revealed that the CIR and ASIR of ovarian cancer were increasing slightly. The regions of Riyadh, Jouf, and Asir had the highest overall ASIR in Saudi Arabia, while Jazan and Hail recorded the lowest rates. The IRR of ovarian cancer cases indicated a concern in the number of ovarian cancer cases diagnosed in certain regions, such as Makkah, Riyadh, and the eastern region of Saudi Arabia. Moreover, the region of Baha documented the greatest changes in CIR and ASIR from 2001–2008, while the regions of Najran and Hail reported the lowest. Nonetheless, further analytical studies are required to determine and to explore the potential risk factors of ovarian cancer in Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
Ferlay J, Shine H, Bray F, Forman D, Mathers C, Parkin D. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–2917. | |
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. | |
Bast RC, Hennessy B, Mills GB. The biology of ovarian cancer: new opportunities for translation. Nat Rev Cancer. 2009;9(6):415–428. | |
Kusumbe AP, Bapat SA. Ovarian stem cell biology and the emergence of ovarian cancer stem cells. In: Cancer Stem Cells. 2008:95–110. | |
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60(5):277–300. | |
Holschneider CH, Berek JS. Ovarian cancer: epidemiology, biology, and prognostic factors. Semin Surg Oncol. 2000;19(1):3–10. | |
Klint A, Tryggvadóttir L, Bray F, et al. Trends in the survival of patients diagnosed with cancer in female genital organs in the Nordic countries 1964–2003 followed up to the end of 2006. Acta Oncol. 2010;49(5):632–643. | |
American Cancer Society. Global Cancer Facts and Figures. 2nd ed. Atlanta: American Cancer Society; 2012. Available from: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-027766.pdf. Accessed January 1, 2014. | |
GLOBOCAN (IARC). Section of Cancer Information; 2008. Available from: http://globocan.iarc.fr/ia/World/atlas.html. Accessed September 21, 2013. | |
King Faisal Specialist Hospital and Research Centre. Tumor Registry Annual Report; 2011. Available from: http://www.kfshrc.edu.sa/oncology/ Tumor%202011%20New%206%20Final.pdf. Accessed June 9, 2014. | |
Saudi Cancer Registry. Cancer Incidence Report in Saudi Arabia. Ministry of Health; 2008. Available from http://www.scr.org.sa/files/file/1eo1lhvt_compressPdf.pdf. Accessed June 9, 2014. | |
Friis RH, Sellers TA. Epidemiology for Public Health Practice. 4th ed. Sudbury, MA: Jones and Bartlett; 2009. | |
McHugh ML. Multiple comparison analysis testing in ANOVA. Biochem Med (Zagreb). 2011;21(3):203–209. | |
Tabatabai MA, Eby WM, Li H, Bae S, Singh KP. TELBS robust linear regression method. Open Access Medical Statistics. 2012;2:65–84. | |
Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age Standardization of Rates: a New WHO Standard. Geneva: World Health Organization; 2001. Available from: http://www.who.int/healthinfo/paper31.pdf. Accessed January 20, 2014. | |
Doll R, Payne PM, Waterhouse JAH. Cancer incidence in five countries. International Union Against Cancer. Berlin: Springer-Verlag; 1966. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.