")
Back to Journals » Cancer Management and Research » Volume 14
Incidence of Mortality and Associated Factors Among Colorectal Cancer Patients at Oncology Units of Northwest Ethiopia: A Retrospective Cohort Study
Authors Tiruneh YM , Beshah DT, Wassie M
Received 15 November 2021
Accepted for publication 4 April 2022
Published 13 April 2022 Volume 2022:14 Pages 1445—1455
DOI https://doi.org/10.2147/CMAR.S349495
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kenan Onel
Yenework Mulu Tiruneh,1 Debrework Tesgera Beshah,1 Mulugeta Wassie2
1Department of Surgical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondor, Ethiopia; 2Department of Medical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondor, Ethiopia
Correspondence: Yenework Mulu Tiruneh, Tel +251967149363, Email [email protected]
Background: Colorectal cancer is one of the commonest types of malignant neoplasm with an estimated 935,000 deaths in 2020 worldwide. In Ethiopia, colorectal cancer is the third most common cancer with an incidence of 8/100,000 person-years. Despite studies related to the burden of colorectal cancer, data of mortality related to colorectal cancer are limited and unknown in the study areas. Therefore, the aim of this study was to assess the incidence of mortality and associated factors among colorectal cancer patients who were followed-up at oncology units of Northwest Amhara hospitals, Ethiopia.
Methods and Materials: A retrospective cohort study was conducted among 367 study participants from January 1, 2017, to December 31, 2020 at oncology units of Northwest Amhara hospitals. Data were entered into EPi-data 4.2.0.0 and transferred to STATA version 14 statistical software for statistical analysis. The Cox regression model was used to identify factors associated with mortality. All variables with P-value < 0.2 during bi-variable analysis were considered for multivariable Cox regression model and level of statistical significance was declared at P value ≤ 0.05.
Results: The overall incidence of colorectal cancer mortality was 22.5 per 100 person-years (95% CI: 18.5, 27.38). Being male [AHR =1.60; 95% CI (1.03, 2.48)], having rural residence [AHR=1.68; 95% CI (1.11, 2.55)], carcinoembryonic antigen level ≥ 5ng/mL [AHR=1.84; 95% CI: (1.02, 3.30)], delay to first health care visit [AHR=1.97; 95% CI (1.19, 3.25)], delay to confirmed diagnosis [AHR=2.45; 95% CI (1.22, 4.90)], and patients who had recurrence after treatment [AHR=1.61;95% CI (1.05, 2.47)] were independently associated with mortality.
Conclusion: Incidence of colorectal cancer mortality was high. Sex, residency, carcinoembryonic antigen level, time to health care visit, time to confirmed diagnosis, and recurrence significantly increased incidence of mortality. Therefore, creating awareness of colorectal cancer and expanding cancer treatment centers could have paramount importance in reducing the burden of mortality.
Keywords: colorectal cancer, incidence, mortality, Ethiopia
Background
Colorectal cancer (CRC) is a malignant tumor of the large intestine that arises from the internal wall of colon and rectum.1 It is the third most common malignant neoplasm in the world and the second most common cause of cancer death, with an estimated 935,000 deaths in 2020;1,2 of which 54.2% occurred in Asia, 26.2% in Europe, and 4.6% in Africa.3
Incidence of mortality among CRC patients differs in countries of the world. From the Global Burden of Cancer Study (GLOBOCAN), mortality was around 11.5 per 100,000 person-years.4 In the United States, the mortality rates were 18.8 and 13.9 per 100,000 person-years from 2002–2005 and 2013–2017 respectively.5,6
Nowadays, African countries suffer from triple burdens such as infectious disease, road traffic accidents, and non-communicable diseases; among non-communicable diseases, cancer is one of the commonest causes of mortality.7 Evidence also found that there was an increased occurrence of CRC mortality among African Americans compared to European Americans8 and Chinese.9 By 2035 the mortality rate of rectal and colon cancer is predicted to be rising by 71.5% and 60.0% respectively.2 CRC mortality increased over time among different countries due to different reasons such as growth and aging of the populations and engaging in risky behaviors and lifestyles.10,11
Even though CRC is treated with endoscopy, surgery, radiation therapy, chemotherapy, and immunotherapy,12,13 mortality related to CRC is increasing over time.7 Lack of a modern specialized treatment system, late presentation,14 and poor awareness of CRC were some of the reasons for increased mortality, especially in developing countries.15
Moreover, factors that increased CRC mortality are; the presence of co-morbid illness, sedentary lifestyle, sex, age, red/processed meat consumption, staging, excessive consumption of alcohol, tobacco smoking, excess body fat, genetic predisposition, and family history of colorectal neoplasia.16–18
The burden of CRC mortality can be minimized through access to health care with high-quality and effective measures of early detection and screening, diagnosis, and treatment.19–21 Moreover, adjustments of diet and lifestyle factors like consumption of calcium, vitamin D, high dietary fiber, dairy products, and increased levels of physical activity, and others can reduce the risk of CRC which in turn reduces mortality related to colorectal cancer.22–25
In Ethiopia, CRC is the third most common cancer in both sexes,26 and it was the leading among males and fourth in females.27 Though there have been different studies conducted in Ethiopia regarding the incidence of colorectal cancer,28–32 studies related to CRC mortality are limited. Therefore, this study aimed to assess the incidence of mortality and its associated factors among colorectal cancer patients at oncology units of Northwest Amhara region hospitals.
Methods and Materials
Study Design, Period and Setting
An institution-based retrospective cohort study was conducted among 367 CRC patients enrolled from January 1, 2017, to December 31, 2020 at oncology units in Northwest Amhara region (University of Gondar Comprehensive Specialized Hospital, UOGCSH) and Bahir Dar Felege Hiwot Referral Hospital, BFHRH), Ethiopia. The two hospitals are the only hospitals where cancer treatment (oncology center) is conducted in North West Ethiopia. UOGCSH is found in Gondar city and located 750 km Northwest of Addis Ababa. UOGCSH serves more than five million people. The hospital has 680 beds and 21 wards for inpatients, emergency and outpatient department (OPD) services. BFHRH is found in Bahir Dar city, 552 km from Addis Ababa, provides in- and outpatient service to 28.5 million people. In the two hospitals, an average of 107 CRC patients are served per year. The oncology units of UOGCSH and BFHRH are providing surgical therapy, chemotherapy, and other supportive care.
Population
All medical records of CRC patients who had follow-up at UOGCSH and BFHRH were included. Incomplete patients’ charts and charts that were not found during data collection period were excluded.
Sample Size Determination, Sampling Procedure, and Study Variables
All CRC patient charts with confirmed diagnosis at oncology units of northwest Amhara hospitals from January 1, 2017-December 31, 2020 were the total sample size. Census sampling procedure was used and the procedure was as follows: first profiles of all CRC patients who had been followed-up from January 1, 2017, to December 31, 2020 at UOGCSH and BFHRH were assessed and 407 CRC patient charts were identified from the registration book. Out of 407 identified medical records, data were collected from 367 patients’ medical records with complete information.
Incidence of colorectal cancer mortality was the outcome variable and socio-demographic characteristics (age at diagnosis, sex, place of residence, religion, marital status, insurance status), clinico-pathological factors (body mass index (BMI), blood group, CEA level, anemic status, co-morbidity, grade at diagnosis, stage at diagnosis, the primary site of the tumor, recurrence of CRC after treatment, and histological type) and treatment-related characteristics (type of intervention provided) were independent variables.
Operational Definitions
Event: the death of colorectal cancer patients.
Censored: patients who survived beyond the end of the follow-up period or patients who were lost to follow-up before the completion of the study.33
Mortality: is the number of deaths occurring in a specified period whereas the mortality rate is the number of deaths per 100,000 persons per year.34
Colorectal cancer: those diagnosed with colon cancer or rectal cancer or both, since both have similar characteristics except for anatomical location.35
Co-morbidity: is the occurrence of any disease (mentioned Charlson co-morbidity index) other than CRC.36
Data Collection Instrument, Quality Assurance, and Collection Procedures
Data were extracted using pre-tested and structured data abstraction sheet which was developed in English language and contained socio-demographic, clinico-pathological, and treatment-related characteristics. The data were collected by two trained MSc students, two BSc nurses who had experience in working in oncology unit, and two MSC supervisors. Training was given to data collectors and supervisors on data collection tools and procedures for one day. The pretest was done on 5% of the total sample size to test its consistency with actual data collection and necessary corrections were done accordingly. Data collectors were supervised closely by the supervisors and principal investigator. The completeness of each abstraction sheet was checked by the principal investigator and supervisors daily and the necessary feedback was offered to the data collectors.
Data Processing and Analysis
Data were entered, coded, cleaned, and checked by Epi-data statistical software version 4.6.0, and analysis was done using STATA Version 14.1 statistical package software. Descriptive statistics of different variables were presented by tables and figures. The Cox regression model was used to identify independent variables associated with the outcome variable. Variables with P-value <0.20 in the bi-variable analysis of Cox regression model were entered into the multivariable Cox proportional hazard model. Hazard ratio (HR) with 95% confidence interval was calculated for the significant predictive variables and statistical significance was considered at P< 0.05.
Ethical Considerations
Ethical clearance was obtained from University of Gondar, College of Medicine and Health Sciences Ethical Review Committee (CMHSERC). An official letter was written to UOGCSH and BFHCSH for permission, and support. Information regarding the purpose of the study, nature of the study, and risk imposed due to involvement presented in the information section of the survey. Informed written consent was not obtained since it relied on chart review. Confidentiality of the information was maintained and the data were recorded anonymously throughout the study. All the processes of research were performed and secured in accordance with the relevant guidelines and regulations of Declaration of Helsinki.
Results
Socio-Demographic Related Characteristics
A total of 407 colorectal cancer patients were diagnosed at UOGCSH and BFHCSH during the study period. Among 407 charts reviewed, a total of 367 individuals participated in the study.
The median age of the participants was 52 years with an interquartile range of 39 to 62 years. One fourth (25.3%) of them were in the age group of less than 40 years of age, and 23.4% were in the age group of 60–69 years. More than half, 55.6%, of colorectal cancer patients were males and from urban (54%) residence. The majority of the participants, (82.2%), were orthodox in religion, and 73% were married. More than half, (58.9%), were not a member of health insurance (Table 1).
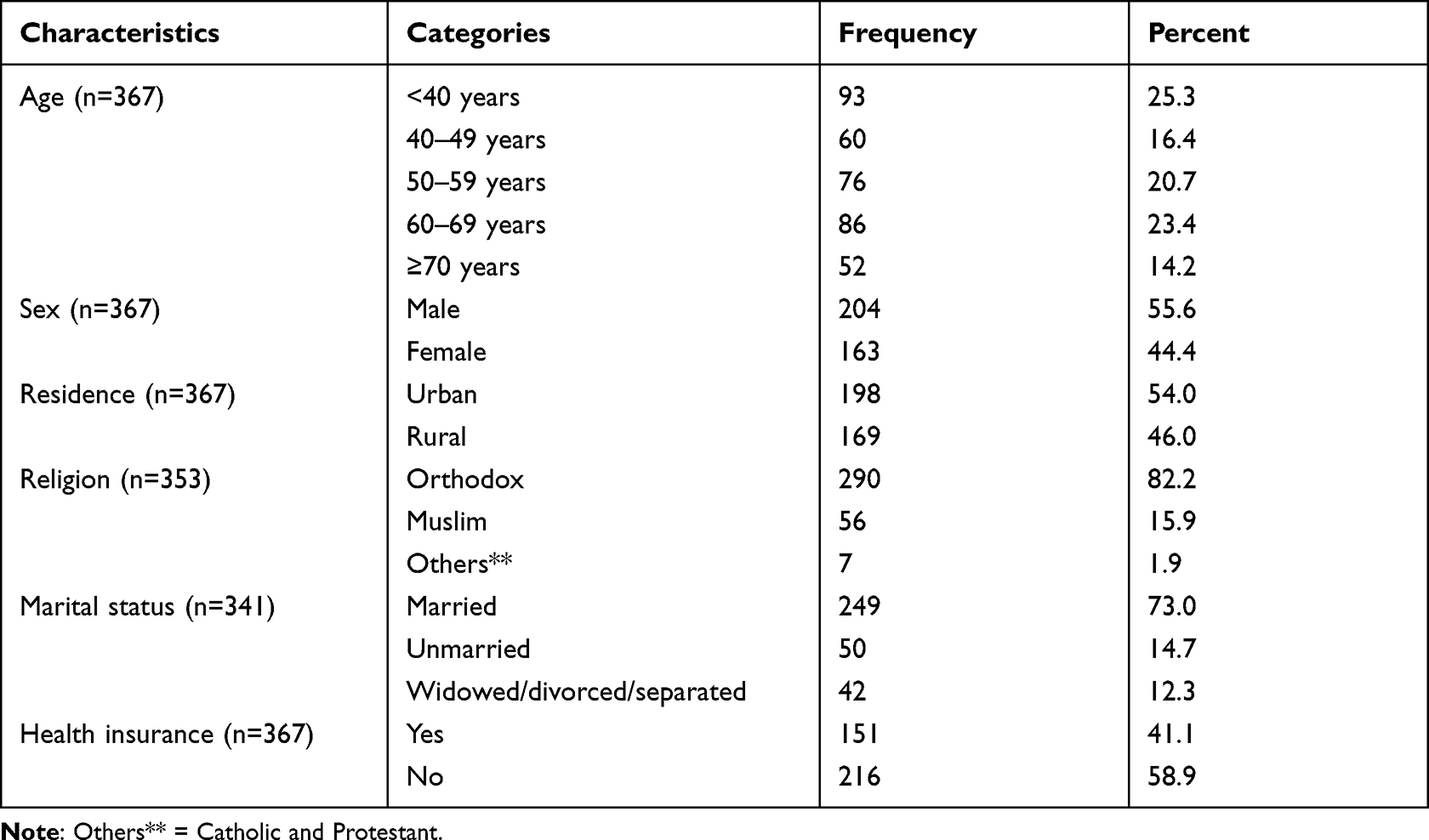 |
Table 1 Socio-Demographic Characteristics of Colorectal Cancer Patients Who Had Follow-Up in Oncology Units of Northwest Amhara, Ethiopia, 2021 |
Clinico-Pathological and Treatment-Related Characteristics
Two thirds of the participants were found in the normal range of body mass index. More than half, 57.7% and 58.9% of them had CEA level of ≥5 ng/mL and had no anemia respectively. Similarly, one fifth of the participants had a co-morbid illness. Based on anatomical site of the tumor, 41.1% was colon cancer. Nearly two thirds, 62.9%, of CRC patients were stage IV at diagnosis and the majority (83.4%) had a histological type adenocarcinoma (Table 2).
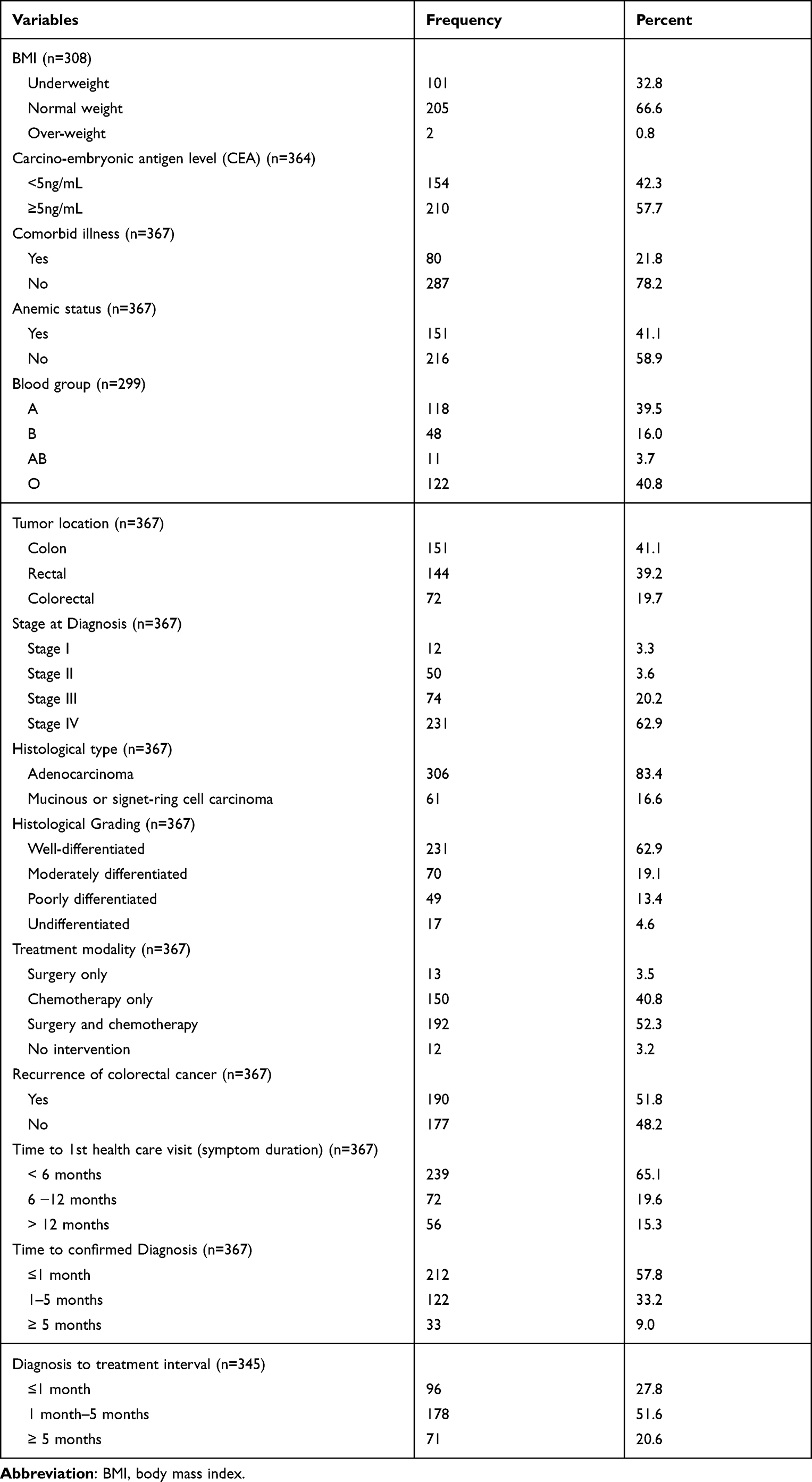 |
Table 2 Clinico-Pathological Characteristics of Colorectal Cancer Patients Who Had Follow-Up in Oncology Units of Northwest Amhara, Ethiopia, 2021 |
Kaplan-Meier Survival Probability
The overall survival probability of CRC patients was 17.96%. The median survival time of the study participants was 30.66 months (95 CI% 28.5, 33.6). The graph showed the probability of colorectal cancer patients who survived during the follow-up time throughout each time interval (diagnosis (0), 10, 20, 30, 40, and 48 months). During the first 35 months, the graph went down gradually which shows the survival probability of CRC patients decreased as time increased and was at steady level during time interval of 35–45 months (Figure 1).
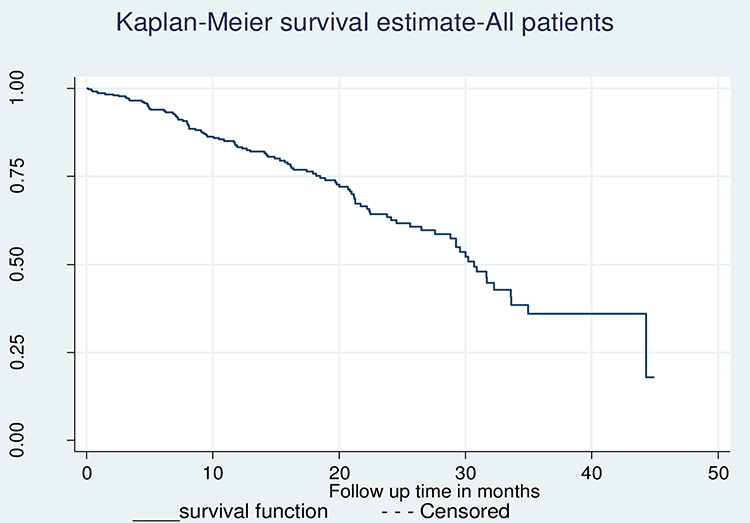 |
Figure 1 Kaplan-Meier estimate of survival probability among colorectal cancer patients who were followed-up at oncology units of Northwest Amhara, Ethiopia, 2021. (n=367). |
Female colorectal cancer patients had higher survival probability compared to males (log rank = 0.0016). Those with CEA level ≥ 5ng/mL had lower survival probability than those with CEA level below 5 ng/mL (log rank test p-value = 0.0013) (Figure 2).
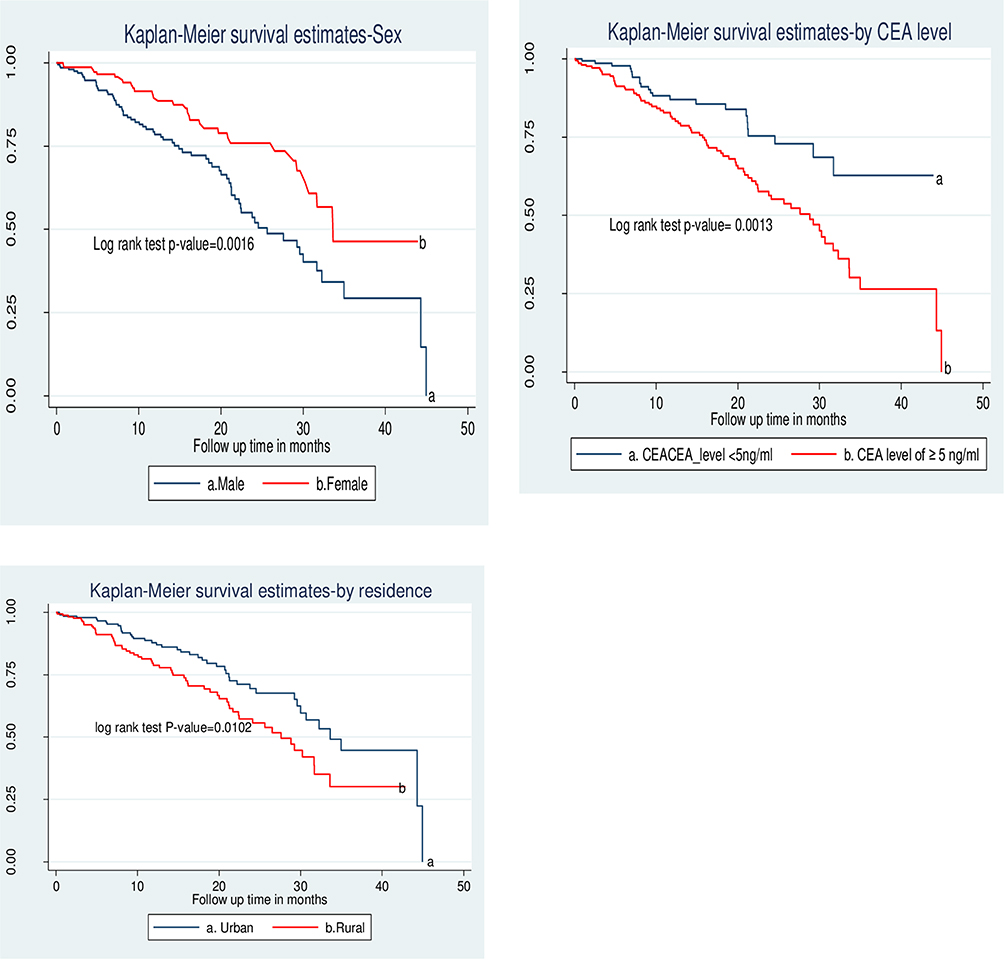 |
Figure 2 Kaplan-Meier survival probability of factors associated with colorectal cancer mortality of patients who were followed-up at oncology unit of Northwest Amhara hospitals, Ethiopia, 2021. |
Incidence of Mortality Among Colorectal Cancer Patients
A total of 367 colorectal patients were followed-up for different time periods ranging from 4 days to 1,348 days, which came to 163,640 days or 448 years total time at risk. The finding showed that 27.52% of deaths occurred within the follow-up period, which makes mortality rate of 22.5 per 100 person-years (95% CI: 18.5, 27.38).
Factors Associated with Mortality Among Colorectal Cancer Patients
Cox regression model was conducted to identify factors of mortality. In the bi-variable Cox- regression model, sex, residence, CEA level, time to 1st health care visit, time to diagnosis, co-morbid illness, stage of tumor at diagnosis, chemotherapy and surgery, recurrence of CRC after treatment, and histologic type were significantly associated with the outcome (p-value < 0.2). Whereas in multivariable Cox-regression, sex, residence, CEA level, time to first health care visit, time to a confirmed diagnosis, and recurrence of CRC after treatment were independently associated with mortality.
The result of the multivariable analysis showed that male colorectal cancer patients had 1.60 [AHR=1.60 (95% CI: 1.03, 2.48)] times higher risk of death as compared to females. Patients whose place of residence was rural had 1.68 [AHR=1.68 (95% CI: 1.11, 2.55)] times higher risk of death as compared to those with urban residence. Patients who had a baseline CEA level of ≥ 5 ng/mL had 1.84 (95% CI: 1.02, 3.30) times higher risk of death than patients with CEA level of <5 ng/mL.
Colorectal cancer patients whose symptoms persisted for more than one year before visiting health care facility had 1.97 times [AHR=1.97 (95% CI: 1.19, 3.25)] higher risk of death compared to those with symptom onset of fewer than six months. Similarly, patients with delayed diagnosis (more than five months) were 2.45 times [AHR= 2.45 (95% CI: 1.22, 4.90)] more likely to die than those diagnosed in less than one month from health care seeking. Moreover, patients who had recurrence after treatment had 1.61 times higher risk of death than those who had no recurrence [AHR=1.61 (95% CI: 1.05, 2.47)] (Table 3).
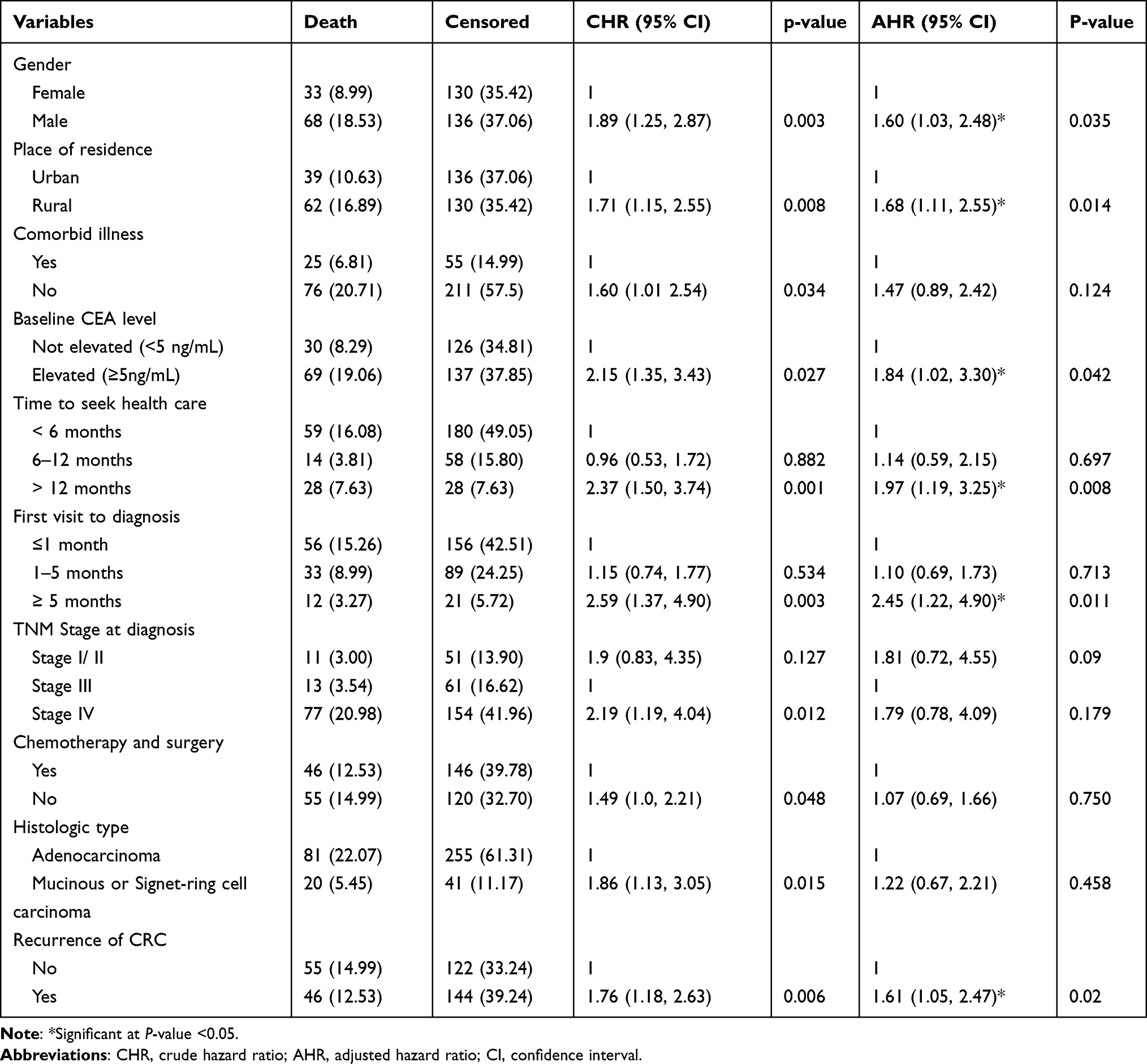 |
Table 3 Factors Associated with Mortality Among Colorectal Cancer Patients Who Had Follow-Up in Northwest Ethiopia, Oncologic Centers, 2021 |
Discussion
The aim of this study was to assess the incidence of mortality and associated factors among colorectal cancer patients at oncology units of Northwest Amhara hospitals, Ethiopia. The finding of the current study is consistent with studies conducted in Black lion Specialized Hospital 20.3,28 and 21.28.30 But higher than studies conducted in Maryland 5.38,37 Singapore 17.3,25 Taiwan 14.9,25 Thailand 8.4,25 China 11.11,38 South Africa 7.6,39 and Zimbabwe 7.27 This difference could be because those countries have a better, healthy lifestyle, accessibility for early detection and screening programs, and effective measures of diagnosis and treatment facility.19–21
The current finding was lower as compared to a study conducted in Kenya (29.4).40 This discrepancy might be due to differences in the population characteristics and study period.
The current finding revealed that male CRC patients had 1.6 times higher risk of death than their counterparts. This is consistent with findings from China.41 This might be because mostly, men are less likely to pay attention to preventive health checkups and screening as compared to women, and delay seeking health care after developing actual symptoms of the disease.42 Moreover, the TP53 tumor suppressor gene among women was predictive of survival after adjuvant chemotherapy which indicates a good response of women to CRC treatment.43
Those coming from rural residences had 1.68 times higher risk of death as compared to those from urban residence. This is in agreement with findings from Iran44 and China.41 The possible reasons could be that those from rural residences have poor health care utilization and present late to health care facilities. Besides, they have a lower budget allocated for health care and transportation costs (45). Moreover, those from rural areas had lower awareness of the disease and faced to access treatment centers. The health care facilities are mainly concentrated in urban areas. As such, the cancer stage at the time of diagnosis becomes more advanced.
Mortality due to colorectal cancer increased as the CEA level increased. The hazard of death was 1.84 times more likely among patients with CEA levels ≥5ng/mL than those who had less than 5ng/mL. This is consistent with studies from Korea.45–47 The possible reason could be that CEA is one of the widely used tumor markers for predicting treatment response, survival, and detecting recurrence in colorectal cancer.48 Another probable reason could be that CEA participates in intracellular adhesion and prevents apoptosis in relation to cell detachment from the extracellular matrix that increases metastasis.49
This study revealed that CRC patients with late presentation to a health care facility (greater than 12 months from the onset of symptoms) were 1.97 times more likely to die than those patients who presented in less than 6 months. This is consistent with a study in Spain (50). This might be because those who presented late had more advanced stage and initiated intervention late. Another probable reason could be not considering rectal bleeding as a problem, resolution of the symptom, and financial issues which makes the disease an untreatable condition that increases the incidence of CRC mortality (51).
Moreover, those with delayed confirmation of diagnosis of more than or equal to five months, had higher risk of death than those diagnosed within a month. This is similar to the study conducted in Taiwan (50). The probable reason could be because the patients wait for a long period of time, the stage of the disease may become worse, which increases mortality (51).
Those patients who had recurrence had higher risk of death than patients with no recurrence. This is similar to the study conducted in the Netherlands (52). This might be due to the patients’ poor adherence to treatment and fear of side effects of chemotherapy drugs. This causes a more advanced stage of CRC.
Strength and Limitation of the Study
This was a multicenter study and included all patients. It investigated a survival function that predicts the probability of death at a given time for the given predictor variables. Censored data were investigated and survival between two groups was compared.
As a limitation, the study was a retrospective follow-up study and depended on medical records not designed for research, which is prone to data incompleteness. Non-registered behavioral related factors such as dietary habits, smoking, alcoholic history, educational status were missed.
Conclusion
The colorectal cancer death rate was high as compared to developed countries based on the GLOBOCAN report. The sex of the patient, place of residence, CEA level, time to health care visit, time to diagnosis, and recurrence after treatment were significantly associated with death. All these factors increased the incidence of mortality among colorectal cancer patients. Therefore, initiating early presentation to health care facilities, decreasing the length of time to diagnosis, and follow-up are important parameters to decrease the incidence of mortality.
Abbreviations
AHR, adjusted hazard ratio; BFCSH, Bahir Dar Felege Hiwot Comprehensive Specialized Hospital; BMI, body mass index, CEA, carcinoembryonic antigen; CHR, crude hazard ratio; CI, confidence interval; CRC, colorectal cancer; GLOBOCAN, Global Burden of Cancer Study; HR, hazard ratio; OR, odds ratio; UOGCSH, University of Gondar Comprehensive Specialized Hospital.
Data Sharing Statement
All relevant data are within the manuscript.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Ethical Review Committee of the school of nursing, college of medicine and health science, University of Gondar. The letter of permission was written from the school of nursing for oncology units of UOGCSH and BFHCSH. Then, the oncology units’ chief administrator was allowed to collect the data from CRC patients’ medical records. The study was conducted without individual informed consent since it relied on chart review. Confidentiality of the information was maintained and the data were recorded anonymously throughout the study.
Acknowledgments
The authors acknowledge the school of Nursing, college of medicine and health science, University of Gondar, University of Gondar Comprehensive Specialized Hospital, Bahir dar Felege Hiwot Hospital, and data collectors.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
2. Araghi M, Soerjomataram I, Jenkins M, et al. Global trends in colorectal cancer mortality: projections to the year 2035. Int J Cancer. 2019;144(12):2992–3000. doi:10.1002/ijc.32055
3. WHO. Colorectal cancer. International agency for research on cancer; 2020. Available from: https://gco.iarc.fr/today/data/factsheets/cancers.
4. Safiri S, Sepanlou SG, Ikuta KS, et al. The global, regional, and national burden of colorectal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2019;4(12):913–933. doi:10.1016/S2468-1253(19)30345-0
5. Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70(3):145–164. doi:10.3322/caac.21601
6. Haggar FA, Boushey RP. Colorectal cancer epidemiology: incidence, mortality, survival, and risk factors. Clin Colon Rectal Surg. 2009;22(4):191. doi:10.1055/s-0029-1242458
7. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. doi:10.3322/caac.21551
8. Wallace K, DeToma A, Lewin DN, et al. Racial differences in stage IV colorectal cancer survival in younger and older patients. Clin Colorectal Cancer. 2017;16(3):178–186. doi:10.1016/j.clcc.2016.11.006
9. Zhang L, Cao F, Zhang G, et al. Trends in and predictions of colorectal cancer incidence and mortality in China from 1990 to 2025. Front Oncol. 2019;9:98. doi:10.3389/fonc.2019.00098
10. Favoriti P, Carbone G, Greco M, et al. Worldwide burden of colorectal cancer: a review. Updates Surg. 2016;68(1):7–11. doi:10.1007/s13304-016-0359-y
11. Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol. 2019;16(12):713–732.
12. Dekker E, Tanis PJ, Vleugels JLA, et al. Colorectal cancer. Lancet. 2019;394(10207):1467–1480. doi:10.1016/S0140-6736(19)32319-0
13. Xie Y-H, Chen Y-X, Fang J-Y, Huang M, Wu M, Zhao X. Comprehensive review of targeted therapy for colorectal cancer. Signal Transduct Target Ther. 2020;5(1):1–30. doi:10.1038/s41392-019-0089-y
14. Chalya PL, Mchembe MD, Mabula JB, et al. Clinicopathological patterns and challenges of management of colorectal cancer in a resource-limited setting: a Tanzanian experience. World J Surg Oncol. 2013;11(1):1–9. doi:10.1186/1477-7819-11-88
15. Hamza A, Argaw Z, Gela D. Awareness of colorectal cancer and associated factors among adult patients in Jimma, South-West Ethiopia. 2020.
16. Baglioni P. The IARC perspective on colorectal cancer screening. N Engl J Med. 2018;379(3):301.
17. Padmanabhan S, Waly MI, Taranikanti V, et al. Modifiable and non-modifiable risk factors for colon and rectal cancer. In: Bioactive Components, Diet and Medical Treatment in Cancer Prevention. Springer; 2018:121–130.
18. Jayasekara H, English DR, Haydon A, et al. Associations of alcohol intake, smoking, physical activity and obesity with survival following colorectal cancer diagnosis by stage, anatomic site and tumor molecular subtype. Int J Cancer. 2018;142(2):238–250. doi:10.1002/ijc.31049
19. Carethers JM, Doubeni CA. Causes of socioeconomic disparities in colorectal cancer and intervention framework and strategies. Gastroenterology. 2020;158(2):354–367. doi:10.1053/j.gastro.2019.10.029
20. Augustus GJ, Ellis NA. Colorectal cancer disparity in African Americans: risk factors and carcinogenic mechanisms. Am J Pathol. 2018;188(2):291–303. doi:10.1016/j.ajpath.2017.07.023
21. López PJT, Albero JS, Rodríguez-Montes JA. Primary and secondary prevention of colorectal cancer. Clinical medicine insights. Gastroenterology. 2014;7:
22. Murphy N, Ward HA, Jenab M, et al. Heterogeneity of colorectal cancer risk factors by anatomical subsite in 10 European countries: a multinational cohort study. Clin Gastroenterol Hepatol. 2019;17(7):1323–1331. e6. doi:10.1016/j.cgh.2018.07.030
23. Rossi M, Usman A, Keshavarzian A, et al. Colorectal cancer and alcohol consumption—populations to molecules. Cancers. 2018;10(2):38. doi:10.3390/cancers10020038
24. Mehrabani D, Almasi-Hashiani A, Moshfeghi K, Khedmati E Survival rate and its predictors in colorectal cancer patients, Southern Iran. Middle East J Sci Res. 2012;12(8):1072–1077.
25. Onyoh EF, Hsu W-F, Chang L-C, et al. The rise of colorectal cancer in Asia: epidemiology, screening, and management. Curr Gastroenterol Rep. 2019;21(8):1–10. doi:10.1007/s11894-019-0703-8
26. Memirie ST, Habtemariam MK, Asefa M, et al. Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data. J Glob Oncol. . 2018;4:1–11.
27. Timotewos G, Solomon A, Mathewos A, et al. First data from a population based cancer registry in Ethiopia. Cancer Epidemiol. 2018;53:93–98. doi:10.1016/j.canep.2018.01.008
28. Atinafu BT, Bulti FA, Demelew TM. Survival status and predictors of mortality among colorectal cancer patients in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia: a retrospective followup study. J Cancer Prev. 2020;25(1):38. doi:10.15430/JCP.2020.25.1.38
29. Memirie ST, Habtemariam MK, Asefa M, et al. Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data. J Glob Oncol. 2018;4:1–11. doi:10.1200/JGO.17.00175
30. Etissa EK, Assefa M, Ayele BT, Chuu C-P. Prognosis of colorectal cancer in Tikur Anbessa Specialized Hospital, the only oncology center in Ethiopia. PLoS One. 2021;16(2):e0246424. doi:10.1371/journal.pone.0246424
31. Deressa BT, Cihoric N, Tefesse E, et al. Multidisciplinary cancer management of colorectal cancer in Tikur Anbessa Specialized Hospital, Ethiopia. J Glob Oncol. 2019;5:1–7. doi:10.1200/JGO.19.00014
32. Tefera B, Assefa M, Abebe B, Rauch D. Patterns of cancer in University of Gondar Hospital: North-West Ethiopia. J Oncol Med Pract. 2016;1:106.
33. Klein JP, Van Houwelingen HC, Ibrahim JG, Scheike TH. Handbook of Survival Analysis. CRC Press; 2016.
34. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
35. American Cancer Society. Colorectal cancer; 2020. Available from: https://www.cancer.org/cancer/colon-rectal-cancer.
36. Glasheen WP, Cordier T, Gumpina R, Haugh G, Davis J, Renda A. Charlson comorbidity index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits. 2019;12(4):188.
37. Schoen RE, Razzak A, Yu KJ, et al. Incidence and mortality of colorectal cancer in individuals with a family history of colorectal cancer. Gastroenterology. 2015;149(6):1438–1445. e1. doi:10.1053/j.gastro.2015.07.055
38. Liu S, Zheng R, Zhang M, et al. Incidence and mortality of colorectal cancer in China, 2011. Chin J Cancer Res. 2015;27(1):22. doi:10.3978/j.issn.1000-9604.2015.02.01
39. Motsuku L, Chen WC, Muchengeti MM, et al. Colorectal cancer incidence and mortality trends by sex and population group in South Africa: 2002–2014. BMC Cancer. 2021;21(1):1–11. doi:10.1186/s12885-021-07853-1
40. Saidi H, Abdihakin M, Njihia B, et al. Clinical outcomes of colorectal cancer in Kenya. Ann Afri Surg. 2011;7. doi:10.4314/aas.v7i1.67029
41. Fang J-Y, Dong H-L, Sang X-J, et al. Colorectal cancer mortality characteristics and predictions in China, 1991–2011. Asian Pacific J Cancer Prev. 2015;16(17):7991–7995. doi:10.7314/APJCP.2015.16.17.7991
42. White A, Ironmonger L, Steele RJC, et al. A review of sex-related differences in colorectal cancer incidence, screening uptake, routes to diagnosis, cancer stage and survival in the UK. BMC Cancer. 2018;18(1):1–11. doi:10.1186/s12885-018-4786-7
43. Kim S-E, Paik HY, Yoon H, et al. Sex-and gender-specific disparities in colorectal cancer risk. World J Gastroenterol. 2015;21(17):5167. doi:10.3748/wjg.v21.i17.5167
44. Semnani S, Noorafkan Z, Aryaie M, et al. Determinants of healthcare utilisation and predictors of outcome in colorectal cancer patients from Northern Iran. Eur J Cancer Care (Engl). 2016;25(2):318–323. doi:10.1111/ecc.12313
45. Lee JH, Lee S-W. The roles of carcinoembryonic antigen in liver metastasis and therapeutic approaches. Gastroenterol Res Pract. 2017;2017:1–11. doi:10.1155/2017/7521987
46. Shen F, Cui J, Hong X, et al. Preoperative serum carcinoembryonic antigen elevation in stage I colon cancer: improved risk of mortality in stage T1 than in stage T2. Int J Colorectal Dis. 2019;34(6):1095–1104. doi:10.1007/s00384-019-03298-y
47. Baqar AR, Wilkins S, Staples M, et al. The role of preoperative CEA in the management of colorectal cancer: a cohort study from two cancer centres. Int J Surg. 2019;64:10–15. doi:10.1016/j.ijsu.2019.02.014
48. Nan J, Li J, Li X, et al. Preoperative serum carcinoembryonic antigen as a marker for predicting the outcome of three cancers. Biomark Cancer. 2017;9:1179299X17690142. doi:10.1177/1179299X17690142
49. Saito G, Sadahiro S, Okada K, et al. Relation between carcinoembryonic antigen levels in colon cancer tissue and serum carcinoembryonic antigen levels at initial surgery and recurrence. Oncology. 2016;91(2):85–89. doi:10.1159/000447062
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.