")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Incidence of Loss to Follow-Up and Its Predictors Among Children with HIV on Antiretroviral Therapy at the University of Gondar Comprehensive Specialized Referral Hospital: A Retrospective Data Analysis
Authors Fisiha Kassa S , Zemene Worku W, Atalell KA, Agegnehu CD
Received 18 July 2020
Accepted for publication 9 September 2020
Published 5 October 2020 Volume 2020:12 Pages 525—533
DOI https://doi.org/10.2147/HIV.S269580
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Selam Fisiha Kassa,1 Workie Zemene Worku,2 Kendalem Asmare Atalell,1 Chilot Desta Agegnehu3
1Department of Pediatrics and Child Health Nursing, School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia; 2Department of Community Health Nursing, School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia; 3School of Nursing College of Medicine and Health Sciences and Comprehensive Specialized Hospital, University of Gondar, Gondar, Ethiopia
Correspondence: Chilot Desta Agegnehu
School of Nursing College of Medicine and Health Sciences and Comprehensive Specialized Hospital, University of Gondar, Gondar, Ethiopia
Tel +251918627403
Email [email protected]
Background: The magnitude of loss to follow-up is high and remains a major public health problem in developing countries. Therefore, the aim of this study determines the incidence rate and predictors of loss to follow-up among children with HIV on ART at the University of Gondar comprehensive specialized referral hospital.
Methods: An institution-based retrospective data analysis was conducted on 361 children with HIV. The simple random sampling technique was used, and data were entered into Epi-info version 7.1 and were exported to Stata version 14 for analysis. The proportional hazard assumption was checked, and Cox regression was fitted. Finally, an adjusted hazard ratio with a 95% CI was computed, and variables with P-value < 0.05 in the multivariable analysis were taken as significant predictors of loss to follow-up.
Results: The overall incidence rate of lost to follow-up was 6.2 events per 100 child-years observations (95% CI: 4.9– 7.7). Children who have got care from their biological parents (AHR 2.6, 95% CI: 1.2– 5.5), WHO clinical stage III/IV (AHR 2.0, 95% CI: 1.1– 3.8), history of regimen substitutions (AHR 1.7, 95% CI: 1.1– 2.9), poor/fair medication adherence (AHR 2.5, 95% CI 1.4– 4.2) and history of TB treatment (AHR 2.7, 95% CI: 1.6– 4.4) were the significant predictors of lost to follow-up.
Conclusion: The incidence rate of loss to follow-up among children was found to be high. Children who have got care from their biological parent, WHO clinical stage III/IV, history of regimen substitution, poor/fair medication adherence, and history of TB treatment were the independent predictors of loss to follow-up. Therefore, strengthening HIV care intervention and addressing these significant predictors is highly recommended in the study setting.
Keywords: ART, children, Gondar, lost to follow-up, the incidence
Background
Globally, 75.7 million people were living with the Human Immunodeficiency Virus (HIV), of them, 1.8 million were children less than 15 years.1 Among those infected children, nearly 53% were initiated by Antiretroviral Therapy (ART) in 2019.1 Antiretroviral therapy restores immune function and reduces HIV-related adverse outcomes.2 However, the effectiveness of Highly-Active Antiretroviral Therapy (HAART) varied a result of various factors.3
Loss To Follow-Up (LTFU) is defined as not taking ART refill for 3 months or longer from the last attendance for a refill and not yet classified as “dead” or “transferred-out”.4 In resource-limited settings, LTFU is one of a common, unfavorable outcome in children with ART.5
Different studies showed that there was a high magnitude of LTFU among children living with HIV. For example, in sub-Saharan Africa estimated that 20–40%,6 in low-income countries the risk of LTFU was found to be 4.1% in Asia, and 21.8% in Western-Africa.7 Besides, the cumulative incidence of LTFU in Ethiopia was 7.7%, 11.8%, and 16.6% at 6, 12, and 24 months, respectively.8 In different articles, various factors were associated with LTFU. Accordingly, being underweight,9,10 age less than 2 years,8–10 advanced WHO staging,7,11–13 low CD4 count,9,11,13 active tuberculosis,9 Incomplete vaccination,14 history of regimen substitution,11 and year of ART initiation7,9,10,13,14 were associated LTFU among children.
LTFU is a major obstacle to achieve 90-90-90 ambitious goals with increased risk of ART failure, morbidity, mortality, and hospitalizations.15–17 Therefore, retention in HIV care is an important public health issue. It improves survival and quality of life among people living with HIV.18 In Ethiopia, over a decade a significant number of HIV-infected children have been successfully enrolled in HIV care and initiated ART. However, retention before and after ART initiation remains a major challenge in the continuum of HIV care.8 Ethiopia is highly affected by HIV epidemics. To achieve 90% of people viral suppression and ends the AIDS epidemic by 2030, continuous, uninterrupted follow-up is very crucial for infected children. Therefore, the aim of this study investigated the incidence and predictors of LTFU among children with HIV on antiretroviral therapy at the University of Gondar comprehensive specialized hospital.
Method
Study Design and Setting
An institution-based retrospective data analysis was conducted from January 2006 to December 2017 at the University of Gondar Comprehensive Specialized Hospital pediatrics ART clinic. It is located in Gondar town. University of Gondar Comprehensive Specialized Hospital is a teaching Hospital, which has been serving for more than five million people in Ethiopia in general and people residing in its surroundings in particular for more than six decades. Apart from other services the hospital started HIV care for both pediatrics and adults in a separate unit since 2005. Various services have been given in its respective departments of these HIV care and treatment centers. Since the hospital starts HIV care and treatment to 2017, more than 9010 adults and 789 pediatric patients were enrolled in HIV care. Currently, about 636 children have active follow-up in this hospital.
Population and Sample
The source population for this study was all children with HIV age less than 15 years who had been on ART at the University of Gondar Comprehensive Specialized Hospital pediatrics ART clinic and the study population was all children with HIV age less than 15 years who had been on ART clinic from January 1st, 2006 to December 30, 2017, were eligible for this study.
Children who had incomplete data or missing potential variables (adherence status, WHO stage, and drug regimen change) were not recorded from their medical charts, not mentioned the status of the child whether dead, LTFU, on follow-up or transfer out were excluded from the study.
We used a survival sample size calculation power approach using Stata 14.1 software with Cox proportional hazard assumptions. The sample size was calculated for the three predictor variables to include WHO staging (HR=2.2), residency (HR=0.4), and ART initiation year (HR=3.3) from a multiregional retrospective cohort study conducted in Ethiopia.10 Accordingly, the minimum sample size was 372 by considering 10% incomplete data.
Variable of the Study
The dependent variable was lost to follow-up whereas the independent variables include child socio-demographic factors (age, sex, year of enrolment, residency, orphanage status), caregiver socio-demographic factors (age, sex, marital status, relationship with a child, educational level, residency, HIV Status, and income), treatment-related factor (ART regimen, OI Prophylaxis (INH & CPT), TB treatment, history of regimen substitution), and clinical characteristics (CD4 count, WHO clinical Staging, baseline functional status, and nutritional status).
LTFU is defined as not taking ART refill for 3 months or longer from the last attendance for a refill and not yet classified as “dead” or “transferred-out”. Time to loss to follow-up is the time interval between the dates of ART initiation to the occurrence of an event. Censored were those children on ART who transferred out to other treatment facilities, recorded as died or active on care during the study period. Adherence to ART was classified into good, fair, and poor according to the percentage of drug dosage calculated from the total monthly dose of ART drugs which is described as Good (≥95% or ≤3 doses missed per month), Fair (85–94% or 4–8 doses missed per month), or Poor (less than 85% or ≥9 doses missed per month).
Data Collection Procedure and Quality Control
Data were collected using a data extraction tool that was adapted from national pediatrics HIV care intake and follow-up care form. Data recording was started from the first day of ART initiation in the regular HIV care in the clinic until the confirmation of a final event in the study period. The data was collected by six bachelor holder ART trained nurses who were working in the three referral hospital. A half-day training was given on the issue of the purpose and scope of the study, on how to use the case recording forms and about the ethical aspects of the study such as how to maintain the confidentiality of the information obtained from the research. Charts were retrieved using the patient’s registration number from the electronic database.
Data Analysis
Data was entered EPI info version 7 and exported to STATA version 14 for recoding and analysis. WHO Anthro-Plus software was used to generate the necessary variables that assess the nutritional status of the child. The Kaplan Meier (KM) failure curve and Log rank test were used to describe the survival experiences of categorical variables. The proportional hazard assumption was checked using a Schoenfield residual test (global test = 0.09). Bi-variable and multivariable Cox proportional hazards regression model was fitted to determine predictors of LTFU. P-value ≤0.25 in the bi-variable analysis was entered into the multivariable cox regression model. The adjusted hazard ratio (AHR) with a 95% confidence interval (CI) was calculated and P-value ≤0.05 in the multivariable Cox regression model was considered as statistically significant predictors of LTFU.
Result
Socio-Demographic Characteristics of Children with HIV
A total of 372 medical records of children on ART from January 2006 to December 2017 were reviewed and from this 361 (97.5%) complete records of children were included and analyzed in the study. Of these, 185 (51.2%) were male and almost half of participants 174 (48.2%) were under five years of age during the time of ART initiation. The median ages of the participants were 66 months with IQR of (33–96) months. The majorities 312 (86.4%) of the children were living with their parents. Three fourth of participant’s primary caregivers 269 (74.5%) were their biological parents (Table 1).
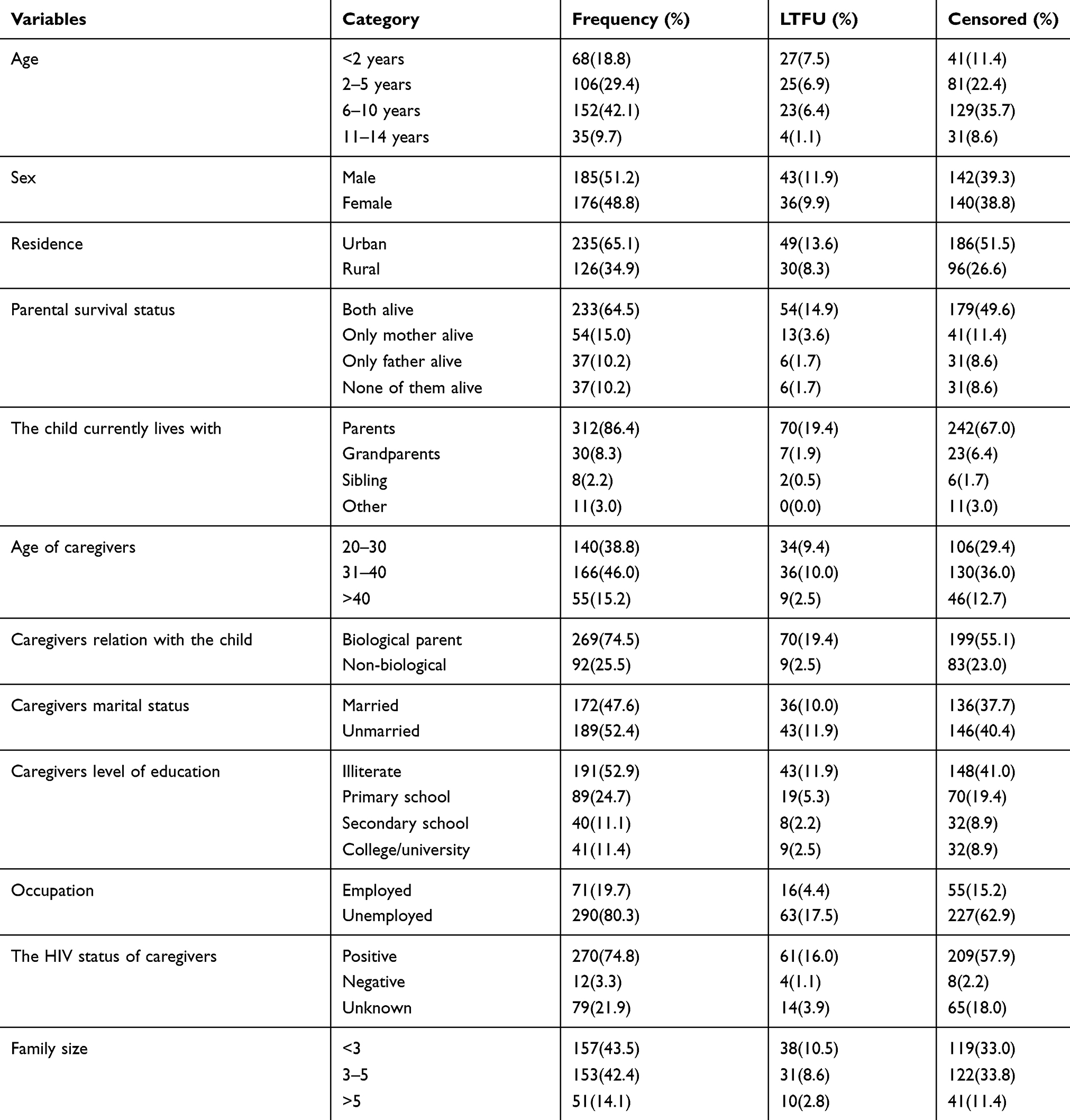 |
Table 1 Socio-Demographic Characteristics of Children Who Were Enrolled on ART at the University of Gondar Comprehensive Specialized Referral Hospitals, from 2006 −2017 (N=361) |
Clinical Characteristics of Children with HIV
Slightly more than half (55.4%) of respondents were in WHO clinical stage 3 and 4 at the time of ART initiation. Almost all, 356 (98.6%) of the patients were taken CPT. However, 283 (78.4%) of the patients developed opportunistic infections. Among the total children, 254 (70.4%) were taken INH. Ninety-seven children (25.9%) had a history of tuberculosis (Table 2).
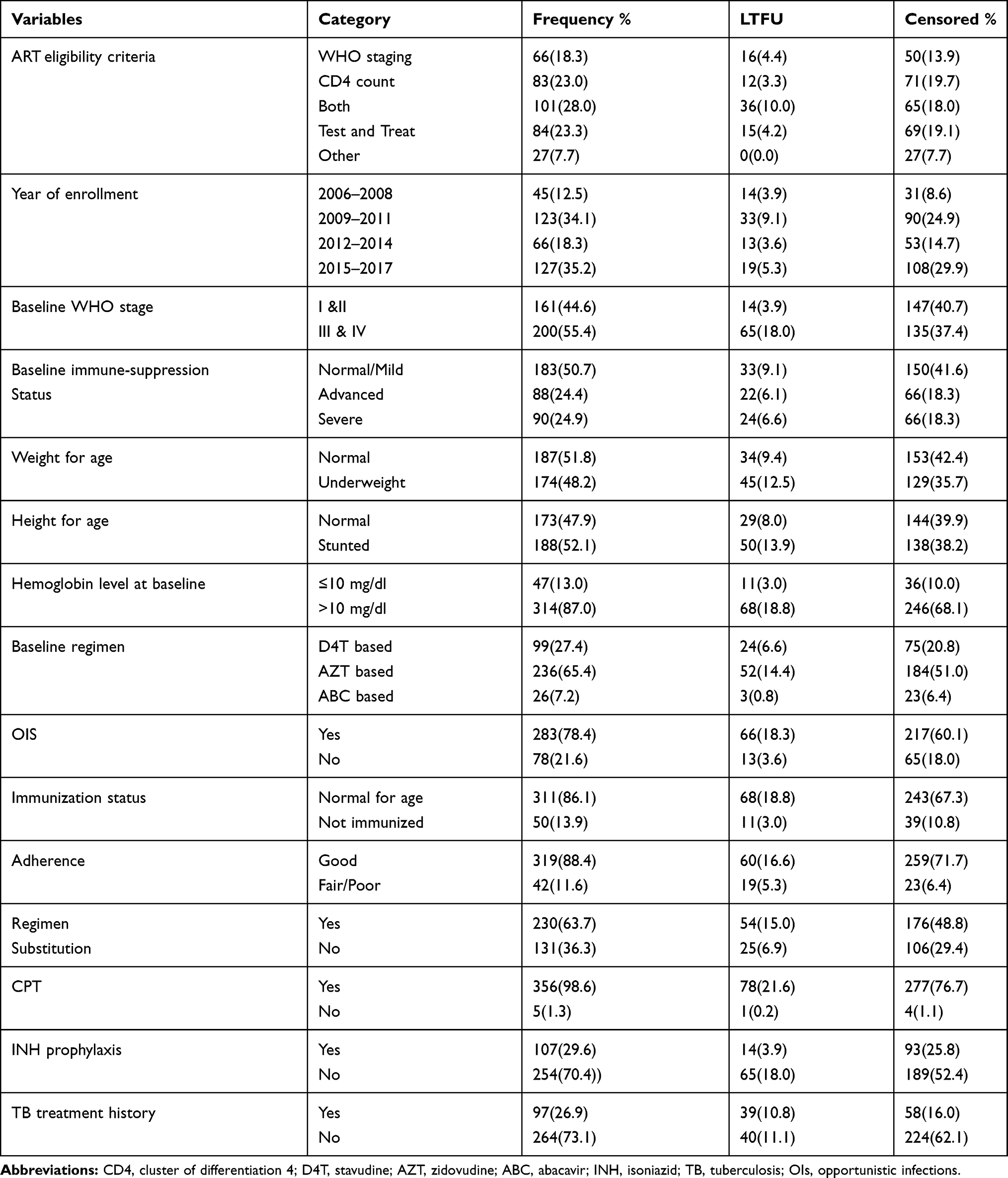 |
Table 2 Clinical Characteristics of Children Who Were Enrolled on ART at the University of Gondar Comprehensive Specialized Referral Hospitals, from 2006 −2017 (N=361) |
The Incidence Rate of Loss to Follow-Up
Three hundred seventy-two (361) children with HIV were followed for different periods with a total of 1280.8 child-year of observations. Patients were followed for a minimum of 3 and a maximum of 127 months. The median follow-up period was 30 (IQR; 14–70) months. The overall proportion of LTFU during the study period was 21.9% with (95% CIs: 17.7–26.3%).
The incidence rate of LTFU among children with HIV was 6.2 with (95% CI: 4.9 −7.7) per 100 Child-Year. The incidence rate was highest in the first six months of the follow-up which is 13.6 (95% CI: 9.1–20.5) per 100 Child-Year. Whereas the incidence rate at 12 and 24 months was 3.3 (95% CI: 1.4–8.0) and 6.1 (95% CI: 4.7–6.2) respectively (Figure 1).
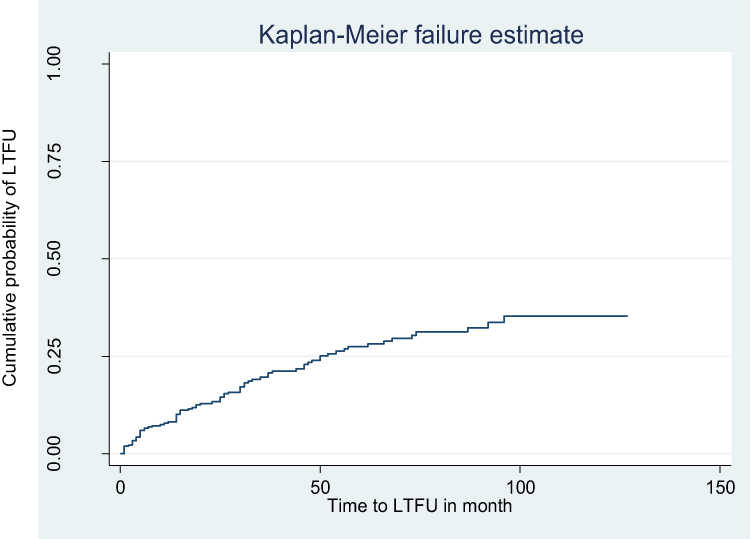 |
Figure 1 Kaplan-Meier failure curve of LTFU probability of children on ART at the University of Gondar Comprehensive specialized hospital, Northwest Ethiopia, from 2006–2017. |
Predictors of Loss to Follow-Up
In the multivariable Cox-regression analysis model, baseline WHO clinical staging, caregiver’s relation to the child, history of regimen substitution, adherence to ARV drugs, and TB treatment history remained were significant predictors of LTFU among children with HIV patients on ART. Children with caregivers of biological parents increase the hazard ratio of LTFU by 2.8 as compared to the non-biological caregiver. Being in WHO clinical stage III/IV (AHR 2.0, 95% CI: 1.1–3.8) was two times more likely to experience LTFU as compared to children with clinical stage I/II. The risk of LTFU was also higher in children with a history of regimen substitution (AHR 1.7, 95% CI: 1.1–2.9) and with poor/fair level of adherence (AHR 2.5, 95% CI 1.4–4.2) as compared to its counterparts. Likewise, children with TB treatment history during the follow-up were at higher risk to LTFU (AHR 2.7, 95% CI: 1.6–4.4) (Table 3).
 |
Table 3 Cox-Regression Analysis of Predictors of LTFU in Children on ART at the University of Gondar Comprehensive Specialized Referral Hospitals, Northwest Ethiopia, from 2006 −2017 (N=361) |
Discussion
LTFU is the major challenge that inhibits the success of anti-retro-viral therapy. The cumulative incidence of LTFU in this study was found to be 6.2 (95% CI: 4.9–7.7%) per 100 Child-Year (CY), which is in line with a multicenter study conducted in Addis Ababa (6.2/100 CY).19 This might be due to the similarity of health care services, treatment protocol, and socio-demographic characteristics. However, the incidence rate of loss to follow-up in this study was lower than a study conducted in Uganda (12.6/100 CY),20 Tanzania (18.2/100 CY),10 and Cote devoir (9.3/100 CY).14 The difference might be due to the study of population differences. In the Uganda study, they have included children on pre-ART. Those children on pre-ART have a higher tendency to be lost from their care. Whereas, the discrepancy with Tanzanian study could be due to the difference in the study design because they used prospective follow-up study design. This might increase the attrition rate that leads to increase LTFU. In the case of Cote devoir, the incidence rate could be increasing due to the difference in the study setting and socio-demographic characteristics of the child.
On the other hand, the incidence rate of loss to follow-up in this study was higher than the Asian study (4.2/100 CY)21 and Kenya (3.29 per 100 CY).16 The difference might be due to the definition of the outcome variable for Asian study. The Asian study defines loss to follow-up as loss of contact for greater than 12 months. Whereas this study defines LTFU as not taking ART refill for 3 months or longer from the last attendance for a refill. The difference in the study design might explain the discrepancy in the finding between this study and a Kenyan study.
The highest loss to follow-up rate (13.6/100 CY) was observed in the first 6 months following ART initiation which was supported by a study conducted in Zimbabwe,22 and South Africa.23 The possible reason could be in the first 6 months ART treatment the likelihood of interrupting ARV drugs and develop ART drug resistance will increase due to drug side effects and non-compliance.24,25 This in turn to increases the pill burden of the children and highly liable to LTFU.
According to the cox multivariable regression model, the caregiver’s relationship with a child, being on WHO clinical stage III/IV, history of regimen substitution, history of TB treatment, and poor/fair level of ART adherence were predictors of LTFU.
Children cared with biological parents were nearly 2.8 at high risk of being the loss to follow-up as compared to children cared with non-biological parents. This finding was supported by a study conducted in South Africa.23 Those mothers may have died during the follow-up period and the other reason could be due to the fear of stigma and discrimination of the biological parents.
Children with an advanced clinical stage (WHO stage III/IV) were nearly two times at high risk of being the loss to follow-up as compared to their counterparts. The advanced clinical-stage can explain the reason for loss to follow-up among children with HIV which was supported by a study conducted in Uganda.26 Since more LFTU could be due to death and patients at an advanced clinical stage are more likely to die due to the side effects of ART with in the first 6 months of ART initiation.27
Children who had regimens substitution were at 1.7 times at higher risk of being LTFU, which is supported by a study conducted in Ethiopia.11 This could be due to adverse drug reaction of the regimen, presences of new TB infection, and treatment failure were some of the reasons mentioned with regimen substitution. The reason, in this case, might be due to fear of adverse drug reactions of a new regimen. The fear of side effects known to be a major cause of defaulter.28 This also leads them to lose faith in the regular medication program.
Children with TB treatment history were 2.7 times at high risk to be lost from the care as compared to their counterparts. The result of this study was supported by a study conducted in Ethiopia.11 This can be justified by the fact that TB is the main opportunistic infection resulting in high mortality and LTFU. Patients generally believe that in history of TB treatment were considered immunocompromised due to pill burden, side effect overlap, and the severity of the illness and which may result in psychological exhaustion.
The study also found that children who had fair/poor adherence to ARV drugs had two and a half times at high risk of being LTFU as compared with children who had good adherence. Disruption in HIV care because of missed appointments can undermine clinical outcomes including assessment of adverse events, ongoing provision of prophylactic medications, clinical and neurodevelopment assessment, and early identification of treatment failure results from LTFU.29 Besides, there might be poor awareness of caregivers about the treatment benefit of antiretroviral drugs and this might lead to give less attention to the regular follow-up of ART schedule.
The limitation of this study since data was collected from secondary sources that use that the routinely collected data from the patient’s medical chart, it lacks to include some of the health care service related predictors and also the psychosocial factor of child and caregiver. Also, some important variables like disclosure status and income were missed due to data incompleteness.
Conclusion
The incidence rate of LTFU among children with HIV was high. Caregivers relationship with a child, being on WHO clinical stage III/IV, history of regimen substitution, TB treatment history, and poor/fair level of adherence were significant predictors of LTFU. Generally, LTFU is the major challenge to achieve a 90-90-90 ambitious goal by 2020 and ends the AIDS epidemic by 2030. This report is very important to monitor the progress of the 90-90-90 ambitious target in Ethiopia. Therefore, to reduce the incidence rate and risk factors of loss to follow-up among children promote families and re-enforcement by counseling and give priority on high-risk groups for better interventions.
Abbreviations
ABC, Abacavir; AHR, Adjusted Hazard Ratio; ART, Antiretroviral Treatment; AIDS, Acquired Immune Deficiency Syndrome; AZT, Zidovudine; CHR, Crude Hazard Ratio; CI, Confidence Level; CD4, Cluster of Differentiation 4; CPT, Cotrimoxazole Preventive Therapy; CY, Child Year; D4T, Stavudine; EFV, Efaveriniz; HIV, Human Immunodeficiency Virus; Hgb, Hemoglobin; IPT, Isoniazid Preventive Therapy; IQR, Inter Quartile Range; LTFU, Loss to Follow-Up; NVP, Nevirapine; OIs, Opportunistic Infections; UNAIDS, United Nations Program on HIV/AIDS; WHO, World Health Organization; 3TC, Lamivudine.
Data Sharing Statement
Based on reasonable requests you can get the data used for the current analysis from the corresponding author.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Ethical Review Committee of the school of Nursing, College of medicine and health sciences, and the University of Gondar with identification number of SN/842/2018. A permission letter was obtained from the University of Gondar comprehensive specialized hospital management, and the HIV care clinic’s focal person. Personal identifiers were not included for the sake of confidentiality. Our study was based on a retrospective review of secondary data from medical records of patients and as this was not a primary study the Ethical Review Committee of the University of Gondar waived the requirement for consent. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgment
We would like to thank the University of Gondar comprehensive specialized hospital for their cooperation and permitting the data access and we would like to give great appreciation for data collectors for their great collaboration and tolerance for this research work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. All authors also have drafted or written, or substantially revised or critically reviewed the article. We have agreed on the journal to which the article will be submitted, reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, agree to take responsibility and be accountable for the contents of the article.
Funding
Financial support was obtained from the University of Gondar. The funding institution or body has no role in any activities of the preparation of the manuscript as well as the decision to publish.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Global H AIDS statistics–2019 fact sheet (2019). 2020.
2. Wube M, Tesfaye A, Hawaze S. Antiretroviral therapy regimen change among HIV/AIDS patients in Nekemt Hospital: a primary care Hospital in Oromia Regional State, Ethiopia. J Appl Pharm Sci. 2013;3(8):36.
3. Abebe N, Alemu K, Asfaw T, Abajobir AA. Predictors of mortality among HIV positive adults on antiretroviral therapy in Debre Markos Referral Hospital, Northwest Ethiopia. J AIDS HIV Res. 2014;6(1):19–27. doi:10.5897/JAHR2013.0275
4. Organization WH. Retention in HIV programs: defining the challenges and identifying solutions: meeting report, 13–15 September 2011. 2012.
5. Brinkhof MW, Dabis F, Myer L, et al. Early loss of HIV-infected patients on potent antiretroviral therapy programs in lower-income countries. Bull World Health Organ. 2008;86:559–567. doi:10.2471/BLT.07.044248
6. Rosen S, Fox MP, Gill CJ. Patient retention in antiretroviral therapy programs in sub-Saharan Africa: a systematic review. PLoS Med. 2007;4(10):e298. doi:10.1371/journal.pmed.0040298
7. Leroy V, Malateste K, Rabie H, et al. Outcomes of antiretroviral therapy in children in Asia and Africa: a comparative analysis of the IeDEA pediatric multiregional collaboration. J Acquir Immune Defic Syndr. 2013;62(2):208. doi:10.1097/QAI.0b013e31827b70bf
8. Melaku Z, Lulseged S, Wang C, et al. Outcomes among HIV‐infected children initiating HIV care and antiretroviral treatment in Ethiopia. Trop Med Int Health. 2017;22(4):474–484. doi:10.1111/tmi.12834
9. Walter J, Molfino L, Moreno V, et al. Long-term outcomes of a pediatric HIV treatment program in Maputo, Mozambique: a cohort study. Glob Health Action. 2015;8(1):26652. doi:10.3402/gha.v8.26652
10. McCormick NM, Nan L, Sando D, et al. Risk factors of loss to follow up among HIV positive pediatric patients in Dar es Salaam, Tanzania. J Acquir Immune Defic Syndr. 2015;70(3):e73. doi:10.1097/QAI.0000000000000782
11. Berheto TM, Haile DB, Mohammed S. Predictors of loss to follow-up in patients living with HIV/AIDS after initiation of antiretroviral therapy. N Am J Med Sci. 2014;6(9):453. doi:10.4103/1947-2714.141636
12. Juergens S, Sawitri AA, Putra IA, Merati P. Predictors of loss to follow up and mortality among children 12 years receiving anti retroviral therapy during the first year at a referral hospital in Bali. Public Health Prev Med Arch. 2016;4:127–133. doi:10.24843/PHPMA.2016.v04.i02.p02
13. Ekouevi DK, Azondekon A, Dicko F, et al. 12-month mortality and loss-to-program in antiretroviral-treated children: the IeDEA pediatric West African database to evaluate AIDS (pWADA), 2000–2008. BMC Public Health. 2011;11(1):519. doi:10.1186/1471-2458-11-519
14. Auld AF, Tuho MZ, Ekra KA, et al. Temporal trends in mortality and loss to follow-up among children enrolled in Cote d’Ivoire’s national antiretroviral therapy program. Pediatr Infect Dis J. 2014;33(11):1134–1140. doi:10.1097/INF.0000000000000457
15. Hogg RS, Heath K, Bangsberg D, Yip B, Press N, O’Shaughnessy MV. Intermittent use of triple-combination therapy is predictive of mortality at baseline and after 1 year of follow-up. AIDS. 2002;16:1051–1058. doi:10.1097/00002030-200205030-00012
16. Saumu WM, Maleche-Obimbo E, Irimu G, Kumar R, Gichuhi C, Karau B. Predictors of loss to follow-up among children attending HIV clinic in a hospital in rural Kenya. Pan Afr Med J. 2019;32. doi:10.11604/pamj.2019.32.216.18310
17. Brinkhof MW, Pujades-Rodriguez M, Egger M. Mortality of patients lost to follow-up in antiretroviral treatment programmes in resource-limited settings: systematic review and meta-analysis. PLoS One. 2009;4(6):e5790. doi:10.1371/journal.pone.0005790
18. Bamidele-Abegunde D. Exploring Predictors of Loss-To-Care Among People Living with HIV. University of Pittsburgh; 2015.
19. Biru M, Hallström I, Lundqvist P, Jerene D. Rates and predictors of attrition among children on antiretroviral therapy in Ethiopia: a prospective cohort study. PLoS One. 2018;13(2):e0189777. doi:10.1371/journal.pone.0189777
20. Massavon W, Lundin R, Costenaro P, et al. Attrition and loss to follow-up among children and adolescents in a community home-based care HIV programme in Uganda. Pediat Therapeut. 2013;3(183):2161–2665.
21. Hansudewechakul R, Sirisanthana V, Kurniati N, et al. Antiretroviral therapy outcomes of HIV-infected children in the TREAT Asia Pediatric HIV observational database. J Acquir Immune Defic Syndr. 2010;55(4):503. doi:10.1097/QAI.0b013e3181f5379a
22. Shroufi A, Gunguwo H, Dixon M, et al. HIV-infected adolescents in southern Africa can achieve good treatment outcomes: results from a retrospective cohort study. AIDS. 2013;27(12):1971. doi:10.1097/QAD.0b013e32836149ea
23. Sengayi M, Dwane N, Marinda E, Sipambo N, Fairlie L, Moultrie H. Predictors of loss to follow-up among children in the first and second years of antiretroviral treatment in Johannesburg, South Africa. Glob Health Action. 2013;6(1):19248. doi:10.3402/gha.v6i0.19248
24. Federal Ministry of Health Ethiopia. National consolidated guidelines for comprehensive HIV prevention, care, and treatment. 2018.
25. O’Brien ME, Clark RA, Besch CL, Myers L, Kissinger P. Patterns and correlates of discontinuation of the initial HAART regimen in an urban outpatient cohort. J Acquir Immune Defic Syndr. 2003;34(4):407–414. doi:10.1097/00126334-200312010-00008
26. Massavon W, Barlow-Mosha L, Mugenyi L, et al. Factors determining survival and retention among HIV-infected children and adolescents in a community home-based care and a facility-based family-centered approach in Kampala, Uganda: a cohort study. Isrn aids. 2014;2014:1–13. doi:10.1155/2014/852489
27. Bhatta L, Klouman E, Deuba K, et al. Survival on antiretroviral treatment among adult HIV-infected patients in Nepal: a retrospective cohort study in far-western Region, 2006–2011. BMC Infect Dis. 2013;13(1):604. doi:10.1186/1471-2334-13-604
28. Deribe K, Hailekiros F, Biadgilign S, Amberbir A, Beyene BK. Defaulters from antiretroviral treatment in Jimma university specialized hospital, Southwest Ethiopia. Trop Med Int Health. 2008;13(3):328–333. doi:10.1111/j.1365-3156.2008.02006.x
29. Geng EH, Nash D, Kambugu A, et al. Retention in care among HIV-infected patients in resource-limited settings: emerging insights and new directions. Curr HIV/AIDS Rep. 2010;7(4):234–244.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.