")
Back to Journals » Journal of Blood Medicine » Volume 12
Incidence and Risk Factors of Thrombocytopenia in Neonates Admitted with Surgical Disorders to Neonatal Intensive Care Unit of Tikur Anbessa Specialized Hospital: A One-Year Observational Prospective Cohort Study from a Low-Income Country
Authors Abebe Gebreselassie H, Getachew H, Tadesse A, Mammo TN, Kiflu W, Temesgen F, Dejene B
Received 26 May 2021
Accepted for publication 12 July 2021
Published 30 July 2021 Volume 2021:12 Pages 691—697
DOI https://doi.org/10.2147/JBM.S321757
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Hana Abebe Gebreselassie,1 Hanna Getachew,2 Amezene Tadesse,2 Tihitena Negussie Mammo,2 Woubedel Kiflu,2 Fisseha Temesgen,2 Belachew Dejene2
1St. Paul’s Hospital Millennium Medical College, Department of Surgery, Addis Ababa, Ethiopia; 2Addis Ababa University School of Medicine, Department of Surgery, Paediatrics Surgery Unit, Addis Ababa, Ethiopia
Correspondence: Hana Abebe Gebreselassie
St. Paul’s Hospital Millennium Medical Collage, Department of Surgery, 1271 Swaziland Street, Addis Ababa, Ethiopia
Tel +251 913 766 868
Email [email protected]
Background: Thrombocytopenia is one of the most common hematologic disorders affecting neonates admitted to the neonatal intensive care unit. The aim of this study was to determine the incidence and associated risk factors of neonatal thrombocytopenia in neonates admitted with surgical disorders.
Methods: An observational prospective cohort study was conducted and all neonates admitted to neonatal intensive care unit of Tikur Anbessa Specialized Hospital with surgical disorders were included. Data were collected using a checklist and analyzed by SPSS version 23. Chi square test and independent sample t- test were used to assess the association among different variables.
Results: A total of 210 neonates were included in the study, out of which 56.2% were males. The incidence of thrombocytopenia was 55.8%. Among neonates with thrombocytopenia, 90.9% had late onset thrombocytopenia and half were in the severe range (< 50,000/μL). The presence of sepsis (P = 0.000) and atresia (P = 0.000) were found to be significantly associated with the development of thrombocytopenia. The mean non feeding hours were found to be significantly longer for patients with thrombocytopenia (t [199], 5.81, P = 0.000).
Conclusion: The incidence of thrombocytopenia is high in our institution. Prevention methods towards neonatal sepsis should be given due emphasis.
Keywords: thrombocytopenia, incidence, risk factors
Background
Platelets first appear in the human fetus at five weeks post conception and progressively increase in number attaining the normal adult range in the second trimester around 22 weeks of gestation.1,2 Hence, in the neonate thrombocytopenia is defined as a platelet count of less than 150,000/μL similar to adults, which also corresponds to values at or below the fifth percentile.3 The severity of thrombocytopenia can also be graded as follows: mild (a platelet count of 100,000–150,000/μL), moderate (a platelet count of 50,000–100,000 /μL), severe (a platelet count of 30,000–50,000/μL) and very severe (a platelet count of < 30,000/μL).4
Thrombocytopenia in healthy term neonates is uncommon, with a reported incidence of 1–5% and warrants evaluation only in case of a platelet count less than 50,000 per µL, bleeding diathesis, persistent thrombocytopenia, or subsequent worsening of the degree of thrombocytopenia.5–7
Unlike healthy neonates, thrombocytopenia in the setup of neonatal intensive care unit is quite common being one of the most common hematologic disorders with a reported incidence of 18–35%.8–10
Several maternal, perinatal and neonatal factors risk factors are identified for neonatal thrombocytopenia. Maternal factors include age, number of pregnancies, maternal auto immune disease, malignancies, maternal medication including nonsteroidal anti-inflammatory drugs and heparin, and pregnancy-induced hypertensive disorders. Perinatal factors include multiple birth, prematurity, being small for gestational age, and intrauterine growth restriction. Neonatal factors include gender, sepsis, necrotizing enterocolitis (NEC), toxoplasmosis, rubella, cytomegalo virus, and herpes viruses (TORCH) infections, asphyxia, neonatal immunologic disorders, chromosomal disorders and metabolic diseases.11
Based on the timing of development after birth, thrombocytopenia can be classified as early onset (<72hrs of life) and late onset (>72hrs) thrombocytopenia. This classification can possibly indicate the underlying cause for thrombocytopenia as early onset thrombocytopenia is usually considered to be due to antenatal and maternal factors while late onset thrombocytopenia is most likely associated with postnatally acquired infection. Moreover, this classification also helps to predict the course and the severity of thrombocytopenia as early onset thrombocytopenia tends to be mild or moderate in range and resolves spontaneously whereas late onset thrombocytopenia usually tends to be more severe and prolonged.3,12
The clinical consequences of thrombocytopenia can be followed both clinically and with laboratory monitoring by assessing haemostatic function. The main clinical concern for neonates with severe thrombocytopenia is the occurrence of major bleeding especially intracranial hemorrhage into the intraventricular and periventricular space (IVH-PVH). The risk of major IVH-PVH is particularly high in premature neonates with a reported incidence of more than 25%.10,13,14
This study is aimed to generate an objective data about the incidence of thrombocytopenia in neonates admitted to neonatal intensive care unit of Tikur Anbessa Specialized Hospital with surgical disorders. Thrombocytopenia is a common finding in these neonates and is one of the major causes delaying surgical intervention in our institution from our observation. This study has also evaluated the associated risk factors for the development of thrombocytopenia in these neonates so that some preventive and therapeutic measure can be taken before the development of complications. There has been no study done on the incidence and associated risk factors of neonatal thrombocytopenia in the Ethiopian setup so far. Thus, this study will be helpful to understand this common condition better in order to improve the outcome of neonates with this disorder.
Materials and Methods
Study area: Addis Ababa University, School of Health Sciences, Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. This study was conducted in Tikur Anbessa Specialized Hospital which is the largest referral hospital and teaching center in Ethiopia. The paediatric Surgery Unit in this hospital is the major center in the country providing surgical care for neonates and has been the sole center for the country providing neonatal surgical care until recently.
A prospective observational cohort study was conducted to assess the incidence and risk factors associated with neonatal thrombocytopenia. All neonates with surgical disorders who were admitted to NICU of TASH for one-year period (January 1, 2019–December 31, 2019) were included in the study. All neonates were followed daily from their day of admission to discharge or death using various clinical and laboratory parameters.
Data were collected by structured interview and chart review using a checklist developed for the study by the principal investigators. Written informed consent was taken from parents of enrolled neonates and each neonate’s clinical data was kept in confidential manner using a coding system. Ethical clearance for this study was obtained from institutional review board of the Department of Surgery of Addis Ababa University. This study was conducted in accordance with the Declaration of Helsinki.
Data were analyzed using SPSS 23. The association of different variables with regard to the development of thrombocytopenia was tested for significance by chi square analysis and independent samples t-test. Considering a confidence interval of 95%, a P-value of <0.05 was considered significant in all statistical comparisons.
Operational Definitions
Sepsis is defined as systemic inflammatory response to infectious cause and diagnosed based on the following parameters and also a positive acute phase reactant like the c reactive protein.15
Two or more of the following conditions:
- Temperature instability <35°C (101.3°F) or >38.5°C (101.3°F),
- Respiratory dysfunction: Tachypnea >2 SD above the mean for age, Hypoxemia (PaO2< 2 SD above the mean for age),
- Cardiac dysfunction: Tachycardia >2 SD above the mean for age, Delayed capillary refill >3 sec Hypotension >2 SD below the mean for age,
- Perfusion abnormalities: Oliguria (urine output <0.5 mL/kg/hour), Lactic acidosis (elevated plasma lactate and/or arterial pH), altered mental status.
Necrotizing enterocolitis (NEC) is an acquired inflammatory disease that affects the gut of newborns. For this study, The Bell’s criteria was used to define NEC which is graded as follows.16
Stage 1, suspected NEC
- Temperature instability, apnea, bradycardia, lethargy, gastric retention, abdominal distention, emesis, heme-positive or grossly bloody stool, plain abdominal X-ray normal or intestinal dilation.
Stage 2, definite NEC
- Features of stage one plus absent bowel sounds, abdominal tenderness with or without abdominal cellulitis or right lower quadrant mass, ascites, mild metabolic acidosis and thrombocytopenia, plain abdominal X-ray Intestinal dilation, pneumatosis intestinalis.
Stage 3, complicated NEC
- Features of stage 2 plus hypotension, bradycardia, severe apnea, combined respiratory and metabolic acidosis, DIC, and neutropenia, ascites, signs of peritonitis like marked tenderness and abdominal distention, plain abdominal X-ray as stage 2 plus pneumoperitoneum.
Result
A total of 210 neonates who were admitted to the NICU of TASH with surgical diagnosis were included in the study. The neonates were followed from their admission to their discharge day via various clinical parameters and platelet count.
Maternal Characteristics
The mean maternal age was 27.17±4.9 years with a range of 16 to 38 years. Primiparous mothers accounted for 40% of the maternal population. A great majority (96.67%) of the mothers claimed that they had antenatal follow up among whom 9 (4.4%) were diagnosed to have gestational hypertension, 2 (0.96%) type 2 diabetes mellitus, 1 (0.49%) gestational diabetes mellitus and 1 (0.49%) retroviral infection. Among the mothers who were hypertensive, three were taking methyl dopa in the third trimester and one was on magnesium sulphate. The rest of the mothers claimed that they had not taken any medication during pregnancy.
Neonatal Characteristics
Males accounted for more than half of the study population (118; 56.2%). Term neonates constituted the majority (165; 78.6%), preterm neonates accounted for 39 (18.6%). As to the birth weight, 63 (29.9%) of the neonates were underweight, of which 40 (19%) had low birth weight, 20 (9.5%) had very low birth weight and 3 (1.4%) had extremely low birth weight (Figure 1).
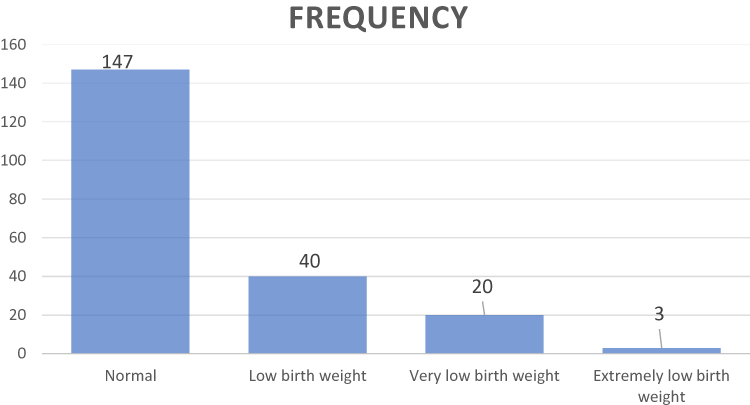 |
Figure 1 Birthweight of the study population. |
Among the neonates, 11 (5.2%) were the result of multiple pregnancies with the majority being twins and one triplet pregnancy. Intrauterine growth restriction was observed in 31 (14.8%) of the neonates. APGAR score was not recorded in the referral paper for 174 (82.9%) of the neonates but the mothers claimed that the neonates had cried immediately after birth.
Perinatal asphyxia was observed in 5 (2.4%) of the neonates all being stage 2. Only one neonate was screened for TORCH infection and the rest were not. A diagnosis of chromosomal abnormality merely based on gross phenotypic characteristics was made in 13 neonates: 11 Down’s syndrome, 1 Patau syndrome and 1 turner/Klippel foli syndrome. NEC was diagnosed in one preterm neonate. The most common admission diagnosis was gastro intestinal atresia accounting for 95 (45.2%) of the cases followed by anorectal malformations 48 (22.9%) (Table 1). The diagnosis of neonatal sepsis was made in 116 (55.2%) of the study population out of which the great majority were of early onset 109 (51.9%) while late onset neonatal sepsis was found in 7 (3.3%) of them.
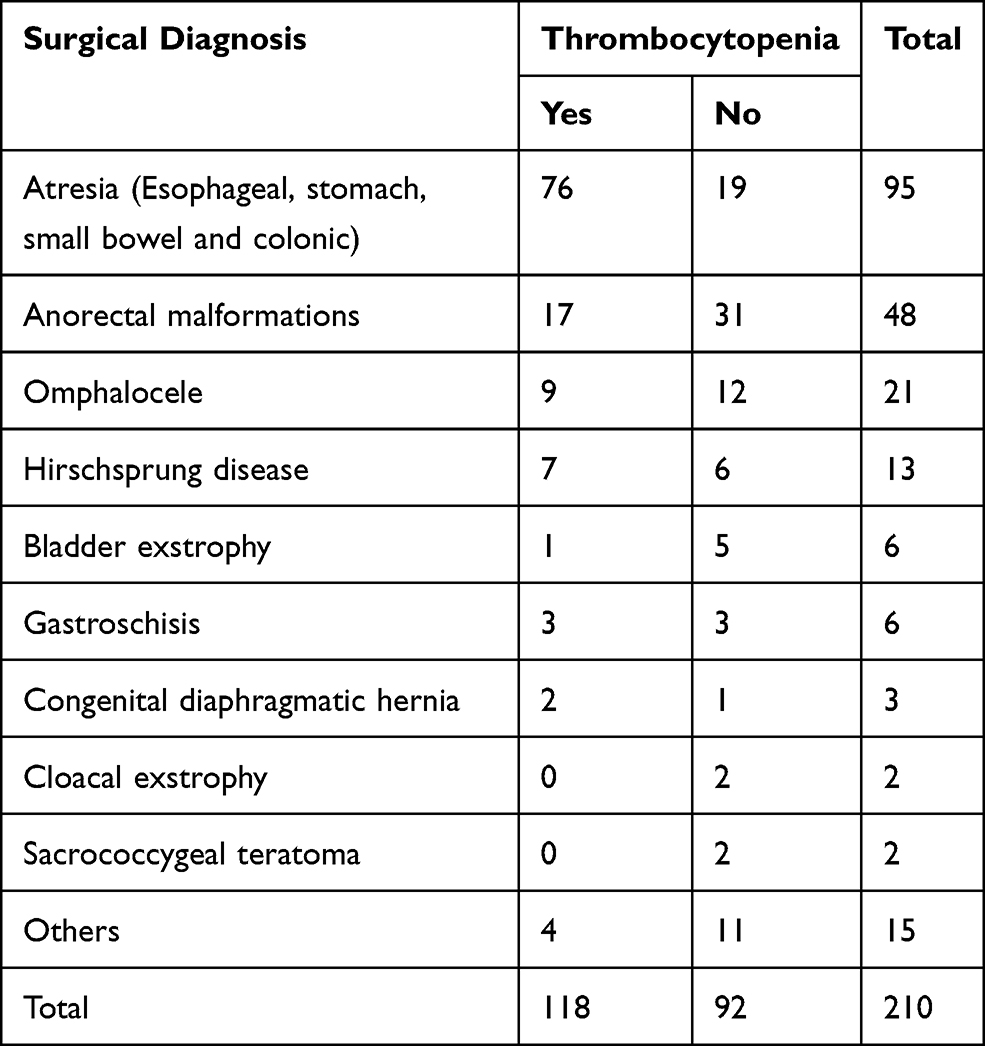 |
Table 1 Admission Diagnosis Versus Thrombocytopenia |
The mean duration of non-feeding (NPO) hours was found to be different in the group of neonates with thrombocytopenia (114.3±119.14 hours) and without thrombocytopenia (33.88±55.07 hours). The duration of intravenous drugs excluding maintenance fluid and electrolytes were compared between neonates with and without thrombocytopenia and found to be longer for the group with thrombocytopenia. The mean duration of hospital stay was 10.2±9.4 days.
Thrombocytopenia
Based on the platelet count determined at admission, 35.2% of the neonates had thrombocytopenia and on their subsequent days of admission, 43 (20.6%) additional neonates were found to be thrombocytopenic making the overall incidence of thrombocytopenia 55.8% in the study period.
Among neonates with thrombocytopenia, a great share of them had a late onset thrombocytopenia (90.9%). As to the degree of thrombocytopenia, 60 (28.4%) had severe, 29 (13.7%) moderate, and 29 (13.7%) mild thrombocytopenia.
Associations
Risk Factors for Thrombocytopenia
A chi square analysis was made considering a confidence interval of 95%, to see the association of the various maternal, perinatal, and neonatal factors with development of thrombocytopenia and the factors which were found to have significant association with the development of thrombocytopenia were sepsis (0.000) and atresia (P = 0.000) (Table 2).
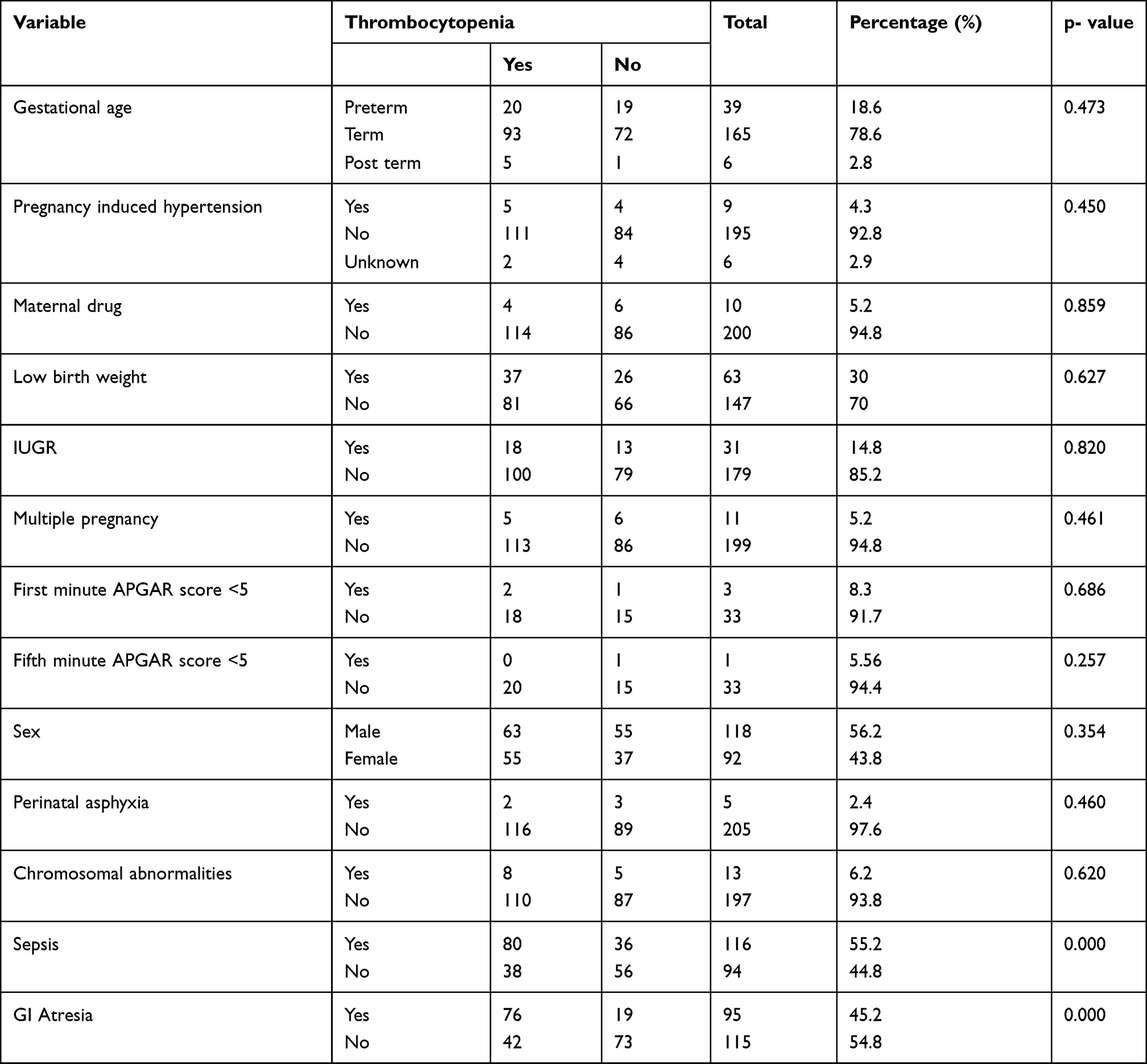 |
Table 2 Percentage and Chi Square Test Result for Various Risk Factors of Thrombocytopenia |
An independent samples t-test was done to compare the difference in the means of the non-feeding (NPO) hours between the group of neonates with and without thrombocytopenia and the difference was found to be statistically significant (t [199], 5.81, P = 0.000).
Discussion
Thrombocytopenia is one of the most common hematologic findings among neonates admitted to NICU with up to 30% of them having a low platelet count detected at some point during their hospital stay. This study is aimed to determine the incidence of this disorder which is commonly observed in our institution. The neonates who were included in this study were those admitted with surgical diagnosis. Thrombocytopenia is one of the factors commonly responsible for delaying surgery and also complicates the post-operative course of such patients. To the best of our knowledge, there is no published literature so far on neonates with surgical diagnosis as a study subject.
The mean maternal age in our study was 27.17±4.9 years, which was comparable to a study from Saudi Arabia in which it was 30±5.5 years.17 The most common maternal comorbidity in our study was pregnancy induced hypertension which was found in 4.4% of the mothers. This figure is significantly lower compared to other reports from India (13.5%), Iran (17.7%), Indonesia (24.3%) and Iran (57.1%).18–21
Male neonates constituted for more than half (56.2%) of our study population which is comparable to a study from Iran (51.3%).19 However, this figure was found to be higher than reports from Indonesia (48.6%) and Nigeria (42.4%) but lower than a study from Saudi Arabia (70.4%).17,20,22 A great majority of our patients were born at term (78.6%) which is comparable to a study from Turkey (73.6%) and Indonesia (85.7%) but significantly higher than that of Iran (34.1%) and Saudi Arabia (51.9).17,20,21,23 Neonates with low birth weight constituted for one fifth of our study population which compares well to a study from Indonesia (20.7%) but higher than a report from Nigeria (13.6%) and significantly lower than India (62.5%).18,20,22
In our study the incidence of thrombocytopenia was found to be 55.8% which is comparable to a report from Nigeria 53% but significantly higher from studies from India (16.7%), Iran (17.9%), Indonesia (12.1%), and the Netherlands (27%).11,19,20,24,25 This difference may be explained by the variability of the types and magnitude of the risk factors involved in the development of thrombocytopenia in each set up. In the great majority (90.9%) of the neonates with thrombocytopenia, the onset was >72 hrs from birth. This figure was significantly higher compared to other studies from Nigeria (15.8%), India (56%), Iran (24.7%), Indonesia (11.8%).18,20–22 This difference may reflect the underlying etiology for thrombocytopenia which was sepsis in our study.
The incidence of severe thrombocytopenia (< 50,000/µL) in our study was 28.6% accounting for half of the cases of thrombocytopenia. This figure was found to be lower than studies from India (37.5%) and Iran (30.5%) but higher compared to that of Nigeria (13.6%), the UK (6%) and the US (2.4%).18,19,22,26,27 This difference may be explained by the difference in the underlying cause of thrombocytopenia.
In our study one of the risk factors that was found to be associated with the development of thrombocytopenia among the various maternal, neonatal and perinatal factors analyzed was sepsis. The incidence of neonatal sepsis in our study was higher compared to two systematic reviews done in Ethiopia.28,29 This association of neonatal sepsis with thrombocytopenia was also present in similar studies from Nigeria, Turkey, India, Iran, Indonesia and Austria.18–20,22,23,30 The other factors like maternal hypertension, prematurity and low birth weight which were found to be significant risk factors for thrombocytopenia in other studies were not significantly associated in our study.
Abbreviations
EOS, early onset sepsis; EOT, early onset thrombocytopenia; IVH, intraventricular haemorrhage; LOS, late onset sepsis; LOT, late onset thrombocytopenia; NEC, necrotizing enterocolitis; NT, neonatal thrombocytopenia; PT, platelet transfusions; NICU, neonatal intensive care unit; TORCH, toxoplasmosis, rubella, cytomegalo virus, herpes simplex virus; TASH, Tikur Anbessa Specialized Hospital.
Funding
Addis Ababa University has granted the funding for this article. We would like to state that the institution has no involvement in any of the steps of this study like in drafting the study design, collection, analysis and interpretation of data, writing of the report and in the decision to submit the paper for publication.
Disclosure
All authors reported no conflicts of interest for this work.
References
1. Sola-Visner M. Platelets in the neonatal period: developmental differences in platelet production,function, and hemostasis and the potential impact of therapies; American Society of Hematology. Hematology. 2012;2012(1):506–511. doi:10.1182/asheducation.V2012.1.506.3798532
2. Ferrer-Marin F, Liu Z-J, Gutti R, Sola-Visner M. Neonatal thrombocytopenia and megakaryocytopoiesis. Semin Hematol. 2010;47(3):281–288. doi:10.1053/j.seminhematol.2010.04.002
3. Roberts I, Murray NA. Neonatal thrombocytopenia: causes and management. Arch Dis Child Fetal Neonatal Ed. 2003;88(5):F359–F364. doi:10.1136/fn.88.5.F359
4. Fernandez CJ. Causes of Neonatal Thrombocytopenia. UpToDate®; 2017:28.
5. Ulusoy E, Tüfekçi Ö, Duman N, Kumral A, Irken G, Ören H. Thrombocytopenia in neonates: causes and outcomes. Ann Hematol. 2013;92(7):961–967. doi:10.1007/s00277-013-1726-0
6. Wong W, Glader B. Approach to the newborn who has thrombocytopenia. NeoReviews. 2004;5(10):e444–e450. doi:10.1542/neo.5-10-e444
7. Sola-Visner M, Saxonhouse MA, Brown RE. Neonatal thrombocytopenia: what we do and don’t know. Early Hum Dev. 2008;84(8):499–506. doi:10.1016/j.earlhumdev.2008.06.004
8. Cremera M, Sallmon H, Kling PJ. Thrombocytopenia and platelet transfusion in the neonate. Semin Fetal Neonatal Med. 2015;1:10–18.
9. Roberts IAG, Murray NA. Neonatal thrombocytopenia: new insights into pathogenesis and implications for clinical management. Curr Opin Pediatr. 2001;13(1):16–21. doi:10.1097/00008480-200102000-00003
10. Antonio DV. Evaluation and management of thrombocytopenic neonates in the intensive care unit. Early Hum Dev. 2014;90(Supplement 2):S51–S55. doi:10.1016/S0378-3782(14)50014-X
11. Roberts I, Stanworth S, Murray NA. Thrombocytopenia in the Neonate. Blood Rev. 2008;22(4):173–186. doi:10.1016/j.blre.2008.03.004
12. Gunnink SF, Vlug R, Fijnvandraat K, van der Bom JG, Stanworth SJ, Lopriore E. Neonatal thrombocytopenia: etiology, management and outcome. Expert Rev Hematol. 2014;7(3):387–395. doi:10.1586/17474086.2014.902301
13. Bonifacio L, Petrova A, Nanjundaswamy S, Mehta R. Thrombocytopenia related neonatal outcome in preterms. Indian J Pediatr. 2007;74(3):269–274. doi:10.1007/s12098-007-0042-x
14. Josephson CD, Su LL, Christensen RD. Platelet transfusion practices among neonatologists in the United States and Canada: results of a survey. PEDIATRICS. 2009;123(1):278–285. doi:10.1542/peds.2007-2850
15. Adams-Chapman I, Stoll BJ. Systemic inflammatory response syndrome. Semin Pediatr Infect Dis. 2001;12(1):5–16. doi:10.1053/spid.2001.19230
16. Sylvester KG, Liu GY, Albanese CT. Necrotizing enterocolitis. In: Coran pediatrics Surgery.
17. Eltawel M, AlHarbi T, AlJamaan K, Alsaif S, Ali Y, Salam M. A prospective study on the incidence and outcomes of neonatal thrombocytopenia at a tertiary care facility in central Saudi Arabia. Adv Neonatal Care. 2018;18(5):E3–E12. doi:10.1097/ANC.0000000000000539
18. Tirupathi K, Swarnkar K, Vagha J. Study of risk factors of neonatal thrombocytopenia. Int J Contemp Pediatr. 2017;4(1):191–196. doi:10.18203/2349-3291.ijcp20164603
19. Khalessi N, Khosravi N, Sanii S. The prevalence and risk factors for neonatal thrombocytopenia among new-borns admitted to intensive care unit of aliasghar children’s hospital. IJBC. 2013;2:41–45.
20. Kusumasari N, Rohsiswatmo R, Gatot D. Incidence and risk factors of neonatal thrombocytopenia: a Preliminary Study. Paediatr Indones. 2010;50(1):31–37.
21. Eslami Z, Lookzadeh M, Noorishadkam M, Hashemi A, Ghilian R, Pirdehghan A. Thrombocytopenia and associated factors in neonates admitted to NICU during years 2010–2011. Iran J Pediatr Hematol Oncol. 2013;3(1):205–215.
22. Jeremiah ZA, Oburu JE. Pattern and prevalence of neonatal thrombocytopenia in Port Harcourt, Nigeria. Arch Pathol Lab Med. 2010;2:27–31. doi:10.2147/PLMI.S9968
23. Oren H, Irken G, Oren B, Olgun N, Özkan H. Assessment of clinical impact and predisposing factors for neonatal thrombocytopenia. Indian J Pediatr. 1994;61(5):551–558. doi:10.1007/BF02751717
24. Gupta AK, Kumari S, Singhal A, Bahl A. Neonatal thrombocytopenia and platelets transfusion. Asian J Transfus Sci. 2012;6(2):161. doi:10.4103/0973-6247.98924
25. von Lindern JS, van den Bruele T, Lopriore E, Walther FJ, Thrombocytopenia in neonates and the risk of intraventricular haemorrhage: a Retrospective Cohort Study. BMC Pediatr. 2011;11(1):16. doi:10.1186/1471-2431-11-16
26. Murray NA, Howarth LJ, Mc Cloy MP, Letsky EA, Roberts IAG. Platelet transfusion in the management of severe thrombocytopenia in neonatal intensive care unit patients. Transf Med. 2002;12(1):35–41. doi:10.1046/j.1365-3148.2002.00343.x
27. Baer VL, Lambert DK, Henry E, Christensen RD. Severe thrombocytopenia in the NICU. Pediatrics. 2009;124(6):e1095–e1100. doi:10.1542/peds.2009-0582
28. Belachew A, Tewabe T. Neonatal sepsis and its association with birth weight and gestational age among admitted neonates in Ethiopia: systematic review and meta-analysis. BMC Pediatr. 2020;20(1):55. doi:10.1186/s12887-020-1949-x
29. Assemie MA, Alene M, Yismaw L, et al. Prevalence of neonatal sepsis in ethiopia: a systematic review and meta-analysis. Int J Pediatr. 2020;2020:9. Article ID 6468492. doi:10.1155/2020/6468492
30. Resch E, Hinkas O, Urlesberger B, Resch B. Neonatal thrombocytopenia—causes and outcomes following platelet transfusions. Eur J Pediatr. 2018;177(7):1045–1052. doi:10.1007/s00431-018-3153-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.