")
Back to Journals » International Journal of General Medicine » Volume 14
Incidence and Risk Factors of Post-Operative Depression in Patients Undergoing Transurethral Resection of Prostate for Benign Prostatic Hyperplasia
Authors Zhu D, Gao J, Dou X, Peng D, Zhang Y, Zhang X
Received 16 July 2021
Accepted for publication 19 October 2021
Published 9 November 2021 Volume 2021:14 Pages 7961—7969
DOI https://doi.org/10.2147/IJGM.S329817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Daofang Zhu,1 Jingjing Gao,1 Xianming Dou,2 Dangwei Peng,1 Yao Zhang,1 Xiansheng Zhang1
1Department of Urology, The First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China; 2Department of Urology, Anhui No. 2 Provincial People’s Hospital, Heifei, 230041, People’s Republic of China
Correspondence: Xiansheng Zhang Tel +86- 551-62922114
Email [email protected]
Background: Benign prostatic hyperplasia (BPH) is a frequent-occurring disease in middle-aged and elderly men. This work is a prospective study and aims at exploring the incidence of post-operative depression and the potential risk factors of depression in a cohort of patients with BPH in China.
Methods: In this survey, 611 men who underwent transurethral resection of the prostate (TURP) were strictly selected at our institution from January 2016 to August 2019. Zung Self-rating Depression Scale was used for evaluation of depressive symptoms. Sociodemographic, clinical and other data were also collected.
Results: We found that 152/611 (24.9%) patients suffered from different degree of depression at 6 months after TURP, including mild symptoms (20.9%) and moderate/severe symptoms (3.9%). A total of 421 (68.9%) patients developed post-TURP erectile dysfunction (ED). The occurrence of depression was closely associated with marital status, education level, cigarette smoking, alcohol consumption, severity of lower urinary tract symptoms (LUTS), duration of BPH, erectile function, and comorbidities (such as diabetes, dyslipidaemia and bladder stone). The risk factors related to the severity of depression included widowed or single marital status, frequent alcohol consumption, moderate or severe LUTS, longer duration (> 5 years) of BPH, ED, urinary continence, and comorbidities such as diabetes and bladder stone.
Conclusion: Many risk factors are related to the occurrence of depression in patients undergoing TURP. Widowed or single marital status, frequent alcohol consumption, moderate or severe LUTS, longer duration of BPH, ED, urinary incontinence and comorbidities such as diabetes and bladder stone are connected with the increase odds of moderate or severe depressive symptom.
Keywords: benign prostate hyperplasia, BPH, transurethral resection of the prostate, TURP, depression, prevalence rate, risk factors
Introduction
The current Chinese population is aging rapidly, and society is paying more attention to the health of the elderly. Benign prostatic hyperplasia (BPH) is a frequent-occurring disease that eventually causes lower urinary tract symptoms (LUTS) in middle-aged and elderly men.1 A total of 50% of men over 50 and 90% of men over 80 suffer from LUTS/BPH, but these patients usually lose consciousness or do not seek treatment.2,3 Transurethral resection of the prostate (TURP) is a minimally invasive alternative to open prostatectomy for BPH patients. For BPH patients with moderate or severe LUTS who need active treatment or fail or do not want to receive medication, TURP has always been an effective and safe method for the treatment of BPH.4–6
However, merely improving urinary function does not indicate that treatment is beneficial, as more than 20% of patients experience adverse reactions after TURP.7,8 TURP can cause psychological burden like stress, depression, and anxiety, as well as sexual problems such as erection and ejaculation disorders. It is well known that depression adversely affects the life span and overall quality of patients. TURP is an effective treatment for BPH, which can minimize BPH-induced anxiety, depression and psychiatric illness.9 Nonetheless, the risk factors related to depression after TURP is still exist and obscure, and the adverse psychological effects associated with TURP are still unclear. At the same time, there is a lack of understanding about the depression in patients undergoing TURP. It is worth noting that depression is related to a remarkable rise in the number of deaths. Thus, early detection, intervention, and treatment of post-operative depression are vital for high-risk patients.
This work was a prospective study aimed at exploring the incidence of post-operative depression in Chinese BPH patients and identifying its potential risk factors.
Patients and Methods
Patient Cohort
A total of 692 patients with LUTS were recruited in the First Affiliated Hospital of Anhui Medical University from January 2016 to August 2019. These LUTS patients all received TURP and were histologically identified as BPH. All participants were informed and gave written consent. The trials were conducted out according to the Declaration of Helsinki, and authorized by the Ethics Committee of the First Affiliated Hospital of Anhui Medical University.
The urologist discussed the therapeutic schedule with the patients based on the latest examination results and the medical history of patients. In general, surgery was recommended for patients at normal risk. Whether the patient accepts TURP was the result of a joint consultation between the patient and his clinician, while considering the benefits and risks of the therapeutic schedule. All surgical operations were performed by experienced urologists under general anesthesia. The final diagnosis of BPH was dependent on the pathological results after TURP.
Patients were interviewed using a questionnaire covering baseline demographics prior to undergo TURP. All patients were followed up by the same clinician 6 months after the operation. The standardized and structured questionnaire was listed as follows.
Demographic Characteristics
Information on age, education (Nine-year compulsory education system), income (judged by the subjective self-evaluation of patients), occupation, marital status and lifestyle were investigated.
LUTS
The International Prostatic Symptoms Score (IPSS) in the Chinese version was used to evaluate the severity degree of LUTS of patients.10 The IPSS is the total of seven scores, ranging from 0 to 35. LUTS is divided into three groups according to standard cut-points: severe (score ≥ 20), moderate (score 8 to 19) and mild (score ≤ 7).
Self-Rating Depression Scale
The Self-rating Depression Scale (SDS) tool was used to evaluate the depressive symptom of patients.11 According to the Chinese standards,12 a score higher than 53 was considered as depression. Furthermore, the severity of depression was divided into mild (score 53–62), moderate (score 63–72) and severe (score ≥ 72).
International Index of Erectile Function
The International Index of Erectile Function (IIEF-5) questionnaire provided in Chinese containing five questions.13 Score below 22 points were diagnosed as erectile dysfunction (ED).14
For this analysis, exclusion criteria as follows: a history of sexual dysfunction; a former surgery of the bladder, prostate or urethra; urethral stricture; prostate or bladder cancer; chronic urinary tract infection; neurological diseases and psychiatric disorders.15
Statistical Analysis
The data were analyzed using SPSS 21.0 statistical software (IBM, Armonk, NY, USA). Number (constituent ratio) was selected to describe the categorical variables. Chi-square test was used to compare the significant difference between two groups. The Pearson’s correlation was applied to analyze the correlation coefficient. Logistic regression model was utilized to analyze the correlation between the influencing factors and depression. Difference was considered statistically significant at P < 0.05.
Results
Baseline Data Analysis
A total of 692 respondents were enrolled in this study, and we analyzed the data of these patients. According to the preset criteria for inclusion and exclusion, 43 patients were excluded in the first round. According to the postoperative pathological results, 11 cases of prostate cancer and 3 cases of bladder cancer were excluded. There were no death during the operation. During the follow-up period, 6 patients died of causes unrelated to the previous surgery, and 18 patients were lost to follow-up or unable to participate. Finally, 611 samples were remained for analyses (Figure 1). In all samples, most patients were 61–80 years old, accounting for about 78.4% (479) of the total patients. There were 351 (57.4%) respondents who were married or in relationship. A total of 333 (54.5%) patients were current smokers and 208 (34.0%) patients were former smokers. In the meantime, a small number of subjects 133 (21.8%) drank alcohol regularly (Table 1).
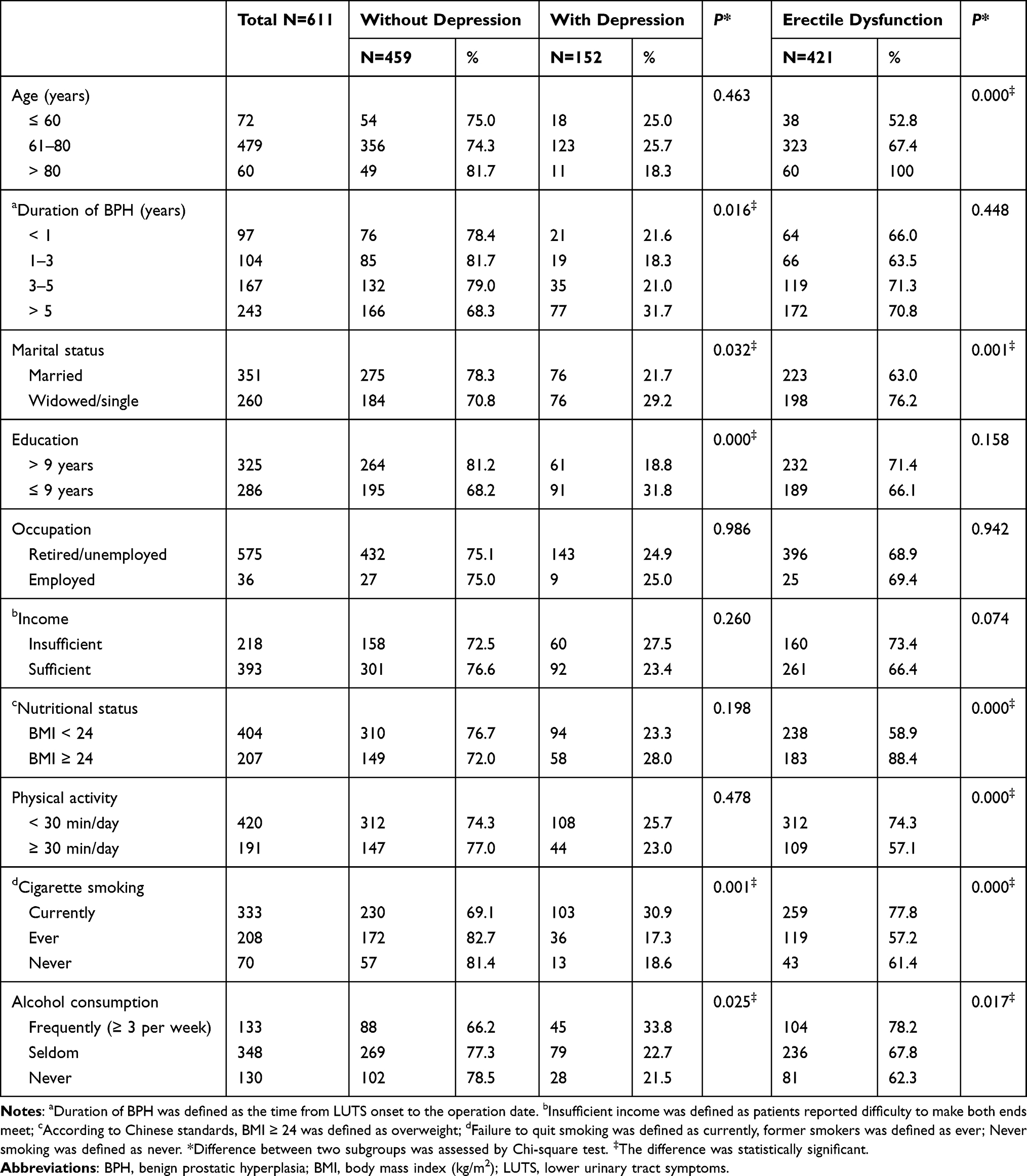 |
Table 1 Frequency of Depression and Erectile Dysfunction in Relation to Baseline Characteristics of 611 Patients |
 |
Figure 1 Flow chart of participant enrolment. |
In addition, 410 (67.1%) respondents had a history of BPH for more than 3 years. After the TURP therapy, 409 (66.9%) patients exhibited mild LUTS, 137 (27.3%) patients had moderate LUTS and 65 (10.7%) patients showed severe LUTS. This study also explored some common comorbidities, and the incidence of these comorbidities was shown as follows: 492 (80.5%) cases of hypertension, 233 (38.1%) cases of dyslipidaemia, 216 (35.4%) cases of coronary artery disease, 179 (29.3%) cases of type 2 diabetes, and 67 (11.0%) cases of bladder stone. At the same time, five patients suffered from persistent urinary incontinence (Table 2). The cause of urinary incontinence is probably urethral sphincter injury caused by surgery.
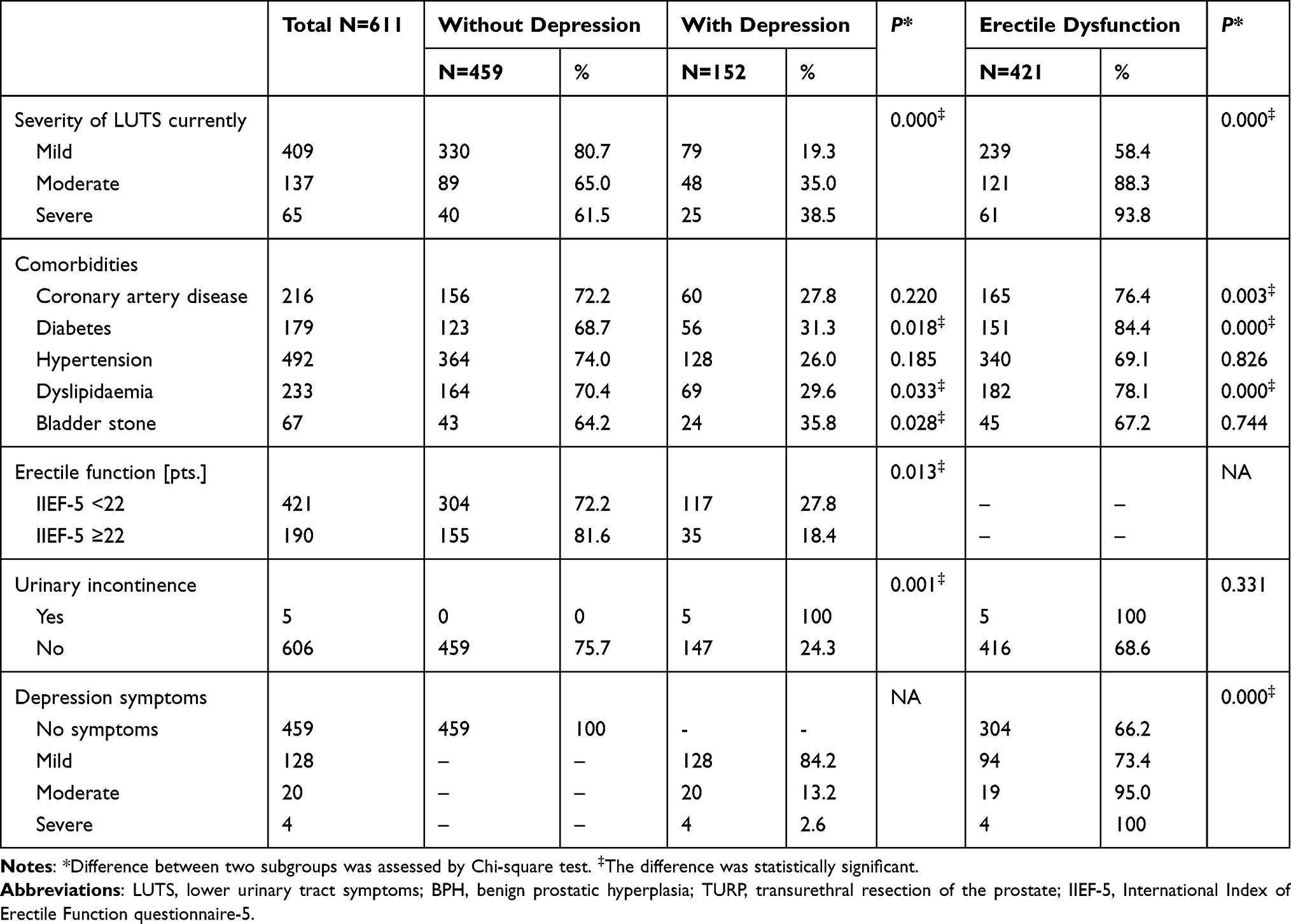 |
Table 2 Severity of LUTS, Coexisting Diseases, Erectile Function and Depression in Patients with BPH at 6 Months After TURP |
ED
The prevalence, demographic data and clinical factors of ED were shown in Tables 2 and 3. In the surveyed population, there were 421 (68.9%) patients developed post-operative ED, while few patients requested treatment. Our results revealed that the incidence of ED was in connection with the increasing age, widowed or single marital status, reduced physical activity (such as sedentary lifestyle), current smoking, frequent drinking, severity of LUTS, comorbidities (such as obesity, diabetes, coronary artery disease, and dyslipidaemia), and the occurrence of depression.
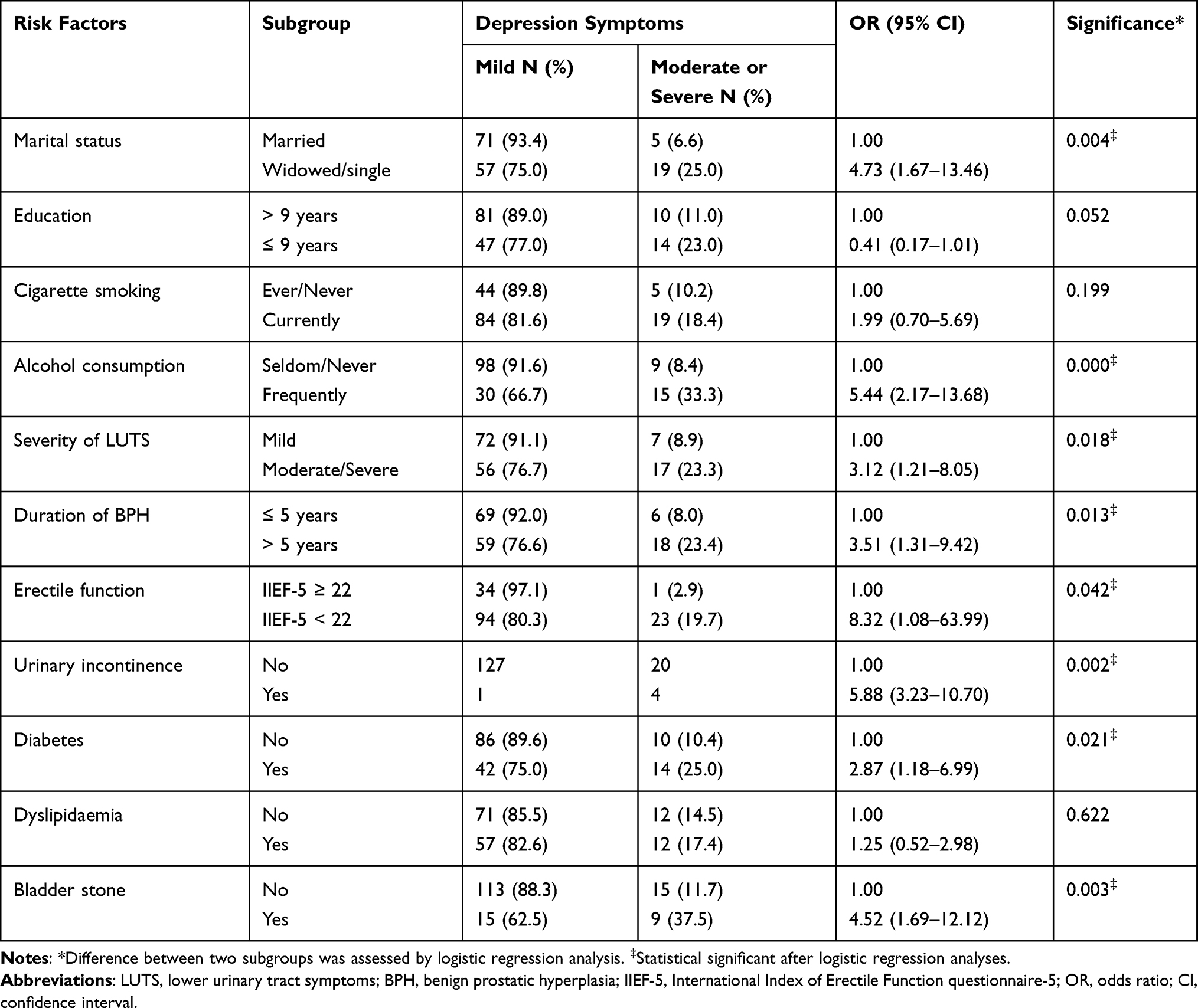 |
Table 3 Risk Factors Revealed by Multiple Logistic Regression for Severity of Depression Symptoms |
Depression Symptoms
According to the SDS, we found that 152 (24.9%) patients with BPH suffered from different degrees of depression 6 months after TURP, including 20.9% of mild Depression symptoms (DSs) and 3.9% of moderate/severe DSs. Moreover, the occurrence of depression was closely associated with marital status, education, smoking, drinking, LUTS, duration of BPH, ED, urinary incontinence and comorbidities (such as diabetes, dyslipidaemia and bladder stone).
According to the logistic regression analysis, we evaluated the risk factors related to depression severity as follows: widowed or single marital status (odds ratio [OR] = 4.73; 95% confidence interval [CI] = 1.67–13.46, P = 0.004), frequent alcohol consumption (OR = 5.44; 95% CI = 2.17–13.68; P < 0.001), moderate or severe LUTS (OR = 3.12; 95% CI =1.21–8.05; P = 0.018), longer duration (> 5 years) of BPH (OR = 3.51; 95% CI = 1.31–9.42; P = 0.013), erectile dysfunction (OR = 8.32; 95% CI = 1.08–63.99; P = 0.042), urinary continence (OR = 5.88; 95% CI = 3.23–10.70; P = 0.002), and comorbidities such as diabetes (OR = 2.87; 95% CI = 1.18–6.99; P = 0.021), bladder stone (OR = 4.52; 95% CI = 1.69–12.12; P = 0.003). Moreover, logistic regression analysis also showed that mild and moderate/severe depression patients had no significant differences in the education, cigarette smoking, and dyslipidaemia.
Discussion
BPH is a common and highly prevalent disease, but it is not life-threatening.16 However, it has been frequently reported that patients with BPH suffered from LUTS, stress, anxiety, depression, and incapacity to complete basic tasks due to the psychological impacts.17–20 Previous studies on BPH patients who undergoing TURP only emphasized the examination of postoperative comorbidities or the technical success of the operation, whereas seldom paid attention to the correlations between TURP treatments for BPH and the adverse psychological effects.
Depression is another common and familiar disease that seriously affects the quality of life. According to data from the National Institute of Mental Health, the prevalence of depression is about 16.5%.20 Due to the serious negative impact of depression on the physical and mental health of patients, it has always been a public health problem that deserves worldwide attention.21 In the present study, we systematically evaluated the incidence of post-operative depression in Chinese men and identified the potential risk factors.
Many studies have demonstrated that BPH/LUTS can increase the likelihood of depression. Coyne et al22 have found that moderate/severe LUTS is significantly associated with an increased risk of depression. Furthermore, another population-based cross-sectional study also has revealed that depression is a common disease in men with LUTS.23 Consistent with the previous findings, we also found that patients with LUTS were more likely to suffer from depression than patients without LUTS. In addition, results of multiple logistic regression analysis indicated that there was significant association between the severity of LUTS and moderate/severe depression after TURP treatment. Obviously, LUTS is a risk factor predicting the occurrence of depression, which means that the negative effects of LUTS may be responsible for the occurrence, development and progression of depression.24 Previous study has reported that post-prostatectomy urinary incontinence may be temporary damage and can be resolved spontaneously.25 Most patients will recover from urinary incontinence within 6 months after surgery. Here, our results confirmed that 5 patients developed persistent incontinence 6 months after surgery. The cause of urinary incontinence was probably urethral sphincter injury caused by surgery. Importantly, urinary incontinence increased the risk of moderate/severe depression. In addition, LUTS can indirectly cause depression through sleep deprivation, because nocturia is one of the major symptoms of LUTS.26
At least 85.5% of depression patients suffer from ED, which is the most common sexual dysfunction after TURP. However, about 83% of men over the age of 50 maintain sexual activity, and thus these patients are more prone to depression and dissatisfaction with post-operative erectile function.27 ED seriously affects the self-esteem of patients, which may lead to the development of depression.28 Consistent with the former studies,29–31 we demonstrated that ED was closely associated with advancing age, widowed or single, obesity (BMI ≥ 24), sedentary lifestyle (physical inactivity), current cigarette smoking, frequent alcohol consumption, moderate or severe LUTS, and comorbidities such as coronary artery disease, diabetes and dyslipidaemia. Patients with moderate/severe LUTS had a significant increased risk of ED and the risk of depression had almost doubled.
At present, both smoking and frequent alcohol consumption are main risk factors that increase the prevalence of depression.32,33 Meanwhile, lack of physical activity and obesity are related to depression.34,35 However, in our study, it was observed that lack of physical activity and obesity had no influence on depression. It should be emphasized that widowed or single men had the higher degree of depression. Many researches have confirmed that widowhood and single men around the world are more likely to suffer from depression.36,37 Whether long-term lack of a sexual partner is the cause of depression is unclear, and further researches are needed.
Urology clinicians should understand that LUTS/BPH and depression are usually comorbid.38 Our results indicated that the prevalence of post-operative depression among in BPH patients was approximately 24.9%. It is very necessary to screen all patients for depression after TURP. The results suggested that interventions may assist patients planning to undergo TURP, especially those who screened for positive risk factors for depression. The post-TURP response for LUTS/BPH may also be improved by combating the potential depression.
Unlike other diseases, the lesions in urology patients are located in the genitourinary tract. During the endoscopic standard procedures, the patient who undergoesndergoes regional anesthesia is awake, and the reproductive organs will be exposed, so that the patient is more likely to show anxiety and stress and other emotions.39 Complementary therapies to decrease the pain and anxiety during endoscopic standard procedures are becoming more popular day by day. These therapies include music, transcutaneous electrical nerve stimulation, acupuncture, and auricular acupressure. The least invasive of these therapies is music. In recent years, music therapy has been widely used in various mental disorders and has a good auxiliary treatment effect on anxiety. Music therapy can improve anxiety and depression, and enhance initiative of patients.40,41 The effect of music as a potential tool for improving the quality of life on anxiety or depression in cancer patients and/or on pain perception in standard procedures for BPH such as endorectal ultrasound or cystoscopy are already recognized several decades ago.42,43 Therefore, music may be used as a complementary therapy to relieve anxiety in patients during the endoscopic standard procedures.
In our study, we integrated multiple factors related to post-operative depression in patients who undergoing TURP. However, we have to acknowledge that there are some limitations in this research. For instance, a minority of patients was involved in our study. Our results may not extend to the whole Chinese male population. Furthermore, there was no patient in control group (other treatment options). Nevertheless, the study was conducted by the research institute in the local community, thereby facilitating consistent follow-up actions. Further studies may clarify the relationship and causality between TURP and post-operative depression.
Conclusion
In summary, many risk factors related to disease courses, lifestyle, even comorbidities are related to the occurrence of depression in patients who undergoing TURP. Especially widowed or single marital status, frequent alcohol consumption, moderate or severe LUTS, longer duration of BPH, ED, urinary incontinence and comorbidities such as diabetes and bladder stone are associated with increased odds of moderate/severe depression.
Funding
This work was supported by the national natural science foundation of China (Grant no. 81571429).
Disclosure
The authors declared no conflicts of interest.
References
1. Berry SJ, Coffey DS, Walsh PC, Ewing LL, Stephen JB. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132(3):474–479. doi:10.1016/S0022-5347(17)49698-4
2. Garraway WM, Lee RJ, Collins GN. High prevalence of benign prostatic hypertrophy in the community. Lancet. 1991;338(8765):469–471. doi:10.1016/0140-6736(91)90543-X
3. Maserejian NN, Chen S, Chiu GR, et al. Treatment status and progression or regression of lower urinary tract symptoms in a general adult population sample. J Urol. 2014;191(1):107–113. doi:10.1016/j.juro.2013.07.005
4. Thomas AW, Cannon A, Bartlett E, Ellis-Jones J, Abrams P. The natural history of lower urinary tract dysfunction in men: the influence of detrusor underactivity on the outcome after transurethral resection of the prostate with a minimum 10-year urodynamic follow-up. BJU Int. 2004;93(6):745–750. doi:10.1111/j.1464-410X.2003.04719.x
5. Ou R, Deng X, Yang W, Wei X, Chen H, Xie K. Transurethral enucleation and resection of the prostate vs transvesical prostatectomy for prostate volumes >80 mL: a prospective randomized study. BJU Int. 2013;112(2):239–245. doi:10.1111/bju.12181
6. Biester K, Skipka G, Jahn R, Buchberger B, Rohde V, Lange S. Systematic review of surgical treatments for benign prostatic hyperplasia and presentation of an approach to investigate therapeutic equivalence (non-inferiority). BJU Int. 2012;109(5):722–730. doi:10.1111/j.1464-410X.2011.10512.x
7. Hakenberg OW, Pinnock CB, Marshall VR. The follow-up of patients with unfavourable early results of transurethral prostatectomy. BJU Int. 1999;84(7):799–804. doi:10.1046/j.1464-410x.1999.00288.x
8. Quek KF, Low WY, Razack AH, Loh CS. The psychological effects of treatments for lower urinary tract symptoms. BJU Int. 2000;86(6):630–633. doi:10.1046/j.1464-410x.2000.00839.x
9. Chan H. The Psychometric Evaluation of the Chinese Version of the International Prostate Symptom Score (IPSS) Hku Thesis Online; 2004.
10. Zhang MY. Manual of Psychiatric Rating Scale (In Chinese). Vol. 1. Hunan Science and Technology Press; 2003.
11. Zung WW. Zung Self Rating Depression Scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1111/j.1464-410X.2009.08438.x
12. Huang YF, Li HJ. Practical Andrology (In Chinese). Vol. 1. Beijing: Science Press; 2009.
13. Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):319–326. doi:10.1038/sj.ijir.3900472
14. Mcvary KT. BPH: epidemiology and comorbidities. Am J Manag Care. 2006;12(5):122–128.
15. Emberton M, Martorana G. BPH: social impact and patient’s perspective. Eur Urol Suppl. 2006;5(20):991–996. doi:10.1016/j.eursup.2006.08.008
16. Quek KF. Factors affecting health-related quality of life among patients with lower urinary tract symptoms. Int J Urol. 2005;12(12):1032–1036. doi:10.1111/j.1442-2042.2005.01198.x
17. Coyne KS, Wein AJ, Tubaro A, et al. The burden of lower urinary tract symptoms: evaluating the effect of LUTS on health-related quality of life, anxiety and depression: EpiLUTS. BJU Int. 2009;103:4–11. doi:10.1111/j.1464-410X.2009.08371.x
18. Milonas D. Significance of operative parameters on outcomes after transurethral resection of the prostate. Medicina. 2010;46(1):24–29. doi:10.3390/medicina46010004
19. Kessler RC, Angermeyer M, Anthony JC, et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the WHO World Mental Health (WMH) Surveys. World Psychiatry. 2007;6(3):168–176.
20. Breyer BN, Kenfield SA, Blaschko SD, Erickson BA. The association of lower urinary tract symptoms, depression and suicidal ideation: data from the 2005–2006 and 2007–2008 National Health and Nutrition Examination Survey. J Urol. 2014;191(5):1333–1339. doi:10.1016/j.juro.2013.12.012
21. Wong SY, Hong A, Leung J, Kwok T, Leung PC, Woo J. Lower urinary tract symptoms and depressive symptoms in elderly men. J Affect Disord. 2006;96(1–2):83–88. doi:10.1016/j.jad.2006.05.013
22. Coyne KS, Kaplan SA, Chapple CR, et al. Risk factors and comorbid conditions associated with lower urinary tract symptoms: EpiLUTS. BJU Int. 2009;103:24–32.
23. Marschall KD. Update on nocturia: the best of rest is sleep. Urology. 2004;64:21–24. doi:10.1016/j.urology.2004.10.072
24. Skalski M, Przydacz M, Sobański J, et al. Coexistence of lower urinary tract symptoms (LUTS) with depressive symptoms in patients suffering from depressive disorders. Psychiatr Pol. 2019;53(4):939–953. doi:10.12740/PP/OnlineFirst/94704
25. Araujo AB, Durante R, Feldman HA, Goldstein I, McKinlay JB. The relationship between depressive symptoms and male erectile dysfunction: cross-sectional results from the Massachusetts Male Aging Study. Psychosom Med. 1998;60(4):458–465. doi:10.1097/00006842-199807000-00011
26. Sullivan ME, Miller MA, Bell CR, et al. Does severity of ischaemic coronary disease correlate with erectile function? Int J Impot Res. 1998;10(2):75. doi:10.1038/sj.ijir.3900347
27. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates results of the Massachusetts Male Aging Study. J Urol. 1994;151(1):54–61. doi:10.1016/S0022-5347(17)34871-1
28. Zohar J, Meiraz D, Maoz B, Durst N. Factors influencing sexual activity after prostatectomy: a prospective study. J Urol. 1976;116(3):332–334. doi:10.1016/S0022-5347(17)58805-9
29. Robertson C, Link CL, Onel E, et al. The impact of lower urinary tract symptoms and comorbidities on quality of life: the BACH and UREPIK studies. BJU Int. 2007;99(2):347–354. doi:10.1111/j.1464-410X.2007.06609.x
30. Coêlho BM, Andrade LH, Guarniero FB, Wang YP. The influence of the comorbidity between depression and alcohol use disorder on suicidal behaviors in the São Paulo Epidemiologic Catchment Area Study, Brazil. Braz J Psychiatry. 2010;32(4):396–408. doi:10.1590/S1516-44462010005000027
31. Boden JM, Fergusson DM. Alcohol and depression. Addiction. 2011;106(5):906–914. doi:10.1111/j.1360-0443.2010.03351.x
32. Yu ZM, Parker L, Dummer TJ. Depressive symptoms, diet quality, physical activity, and body composition among populations in Nova Scotia, Canada: report from the Atlantic Partnership for Tomorrow’s Health. Prev Med. 2014;61:106–113. doi:10.1016/j.ypmed.2013.12.022
33. Olszanecka-Glinianowicz M, Zahorskamarkiewicz B, Kocełak P, et al. Depression in obese persons before starting complex group weight-reduction programme. Int J Soc Psychiatry. 2009;55(5):407–413. doi:10.1177/0020764008095930
34. Rom M, Schatzl G, Swietek N, Rücklinger E, Kratzik C. Lower urinary tract symptoms and depression. BJU Int. 2012;110:E918–921. doi:10.1111/j.1464-410X.2012.11552.x
35. Beiramijam M, Anoosheh M, Mohammadi E. Effect of designed self-care educational program on anxiety, stress, and depression in patients with benign prostatic hyperplasia undergoing prostate surgery. J Chronic Dis. 2013;1(2):55–62.
36. Jadhav A, Weir D. Widowhood and depression in a Cross-National Perspective: evidence from the United States, Europe, Korea, and China. J Gerontol B Psychol Sci Soc Sci. 2018;73(8):e143–e153. doi:10.1093/geronb/gbx021
37. Zhou X, Yan Z, Hesketh T, Therese H. Depression and aggression in never-married men in China: a growing problem. Soc Psychiatry Psychiatr Epidemiol. 2013;48(7):1087–1093. doi:10.1007/s00127-012-0638-y
38. Koh JS, Ko HJ, Wang SM, et al. The relationship between depression, anxiety, somatization, personality and symptoms of lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Psychiatry Investig. 2015;12(2):268–273. doi:10.4306/pi.2015.12.2.268
39. Ou M, Huang C, Wang Y, et al. Depression is a major risk factor for the development of dementia in people with lower urinary tract symptoms: a nationwide population-based study. PLoS One. 2019;14(6):e0217984. doi:10.1371/journal.pone.0217984
40. Roddis J, Tanner M. Music therapy for depression. Res Nurs Health. 2020;43(1):134–136. doi:10.1002/nur.22006
41. Tang Q, Huang Z, Zhou H, Ye P. Effects of music therapy on depression: a meta-analysis of randomized controlled trials. PLoS One. 2020;15(11):e0240862. doi:10.1371/journal.pone.0240862
42. Dell’Atti L. Impact of music on anxiety and pain perception among men undergoing prostate biopsy: synthesis of qualitative literature. Complement Ther Clin Pract. 2021;43:101330. doi:10.1016/j.ctcp.2021.101330
43. Jasemi M, Aazami S, Zabihi R. The effects of music therapy on anxiety and depression of cancer patients. Indian J Palliat Care. 2016;22(4):455–458. doi:10.4103/0973-1075.191823
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.