")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Incidence and Risk Factors of Depressive Symptoms in Chinese College Students
Authors Song Y , Liu Z, Chen H, Guo Q, Huang Y
Received 9 June 2020
Accepted for publication 12 September 2020
Published 23 October 2020 Volume 2020:16 Pages 2449—2457
DOI https://doi.org/10.2147/NDT.S264775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Yuqing Song,1– 3 Zhaorui Liu,1– 3 Hongguang Chen,1– 3 Qi Guo,4 Yueqin Huang1– 3
1Institute of Mental Health, Peking University Sixth Hospital, Beijing 100191, People’s Republic of China; 2Key Laboratory of Mental Health, Ministry of Health, Peking University, Beijing 100191, People’s Republic of China; 3National Clinical Research Center for Mental Disorders, Peking University Sixth Hospital, Beijing 100191, People’s Republic of China; 4School of Basic Medical Sciences, Peking University, Beijing 100191, People’s Republic of China
Correspondence: Yuqing Song; Yueqin Huang Tel +86-010-82806164
Fax +86-010-62026310
Email [email protected] [email protected]
Purpose: Previous surveys have shown an increase in the prevalence of depression among college students. However, knowledge on the incidence and risk factors of depressive symptoms in Chinese college students is limited. The aim of the present study was to determine the two-year cumulative incidence of depressive symptoms in Chinese college freshmen and identified related psychosocial risk factors.
Patients and Methods: A prospective survey was used to examine the cumulative incidence and risk factors of depressive symptoms (as assessed by the Centre for Epidemiological Study-Depression Scale, CES-D) among undergraduate freshmen. Five times (baseline, 5, 12, 17, and 24 months later) of self-reported data were collected from the students.
Results: Of the initial 758 non-depressed respondents at baseline, 235 developed depressive symptoms (CES-D ≥ 16) during the follow-up period. The two-year cumulative incidence was estimated to be 42% and not significantly different between males and females (χ 2=3.138, df =1, p=0.077). Logistic regression model showed that female gender (OR=0.43, 95% CI (0.28– 0.64)), high level of self-esteem (OR=0.67, 95% CI (0.52– 0.86)), and moderate exercise (OR=0.71, 95% CI (0.55– 0.92)) reduced the onset of depressive symptoms; while high levels of baseline anxiety (OR=1.48, 95% CI (1.12– 1.94)), Eysenck Personality Questionnaire-Neuroticism (OR=1.40, 95% CI (1.09– 1.79)), concern over mistakes (OR=1.35,95% CI (1.07– 1.71)), daytime sleepiness (OR=1.28, 95% CI (1.02– 1.60)), mild exercise (OR=1.25, 95% CI (1.01– 1.55)) increased the new onset of depressive symptoms.
Conclusion: The high two-year cumulative incidence indicates that depressive symptoms are an important mental problem in Chinese college students. The present findings on the risk factors of depressive symptoms in Chinese college students may be useful for the design of student health screening and intervention programs.
Keywords: depression, anxiety, risk factor, incidence, college student
Introduction
Given the increasing number of reports on college students’ unsafe sex, binge drinking, depression, and suicide, it is not surprising that college students’ health is a matter of growing concern for researchers.1 Depression affects individuals of all ages. It was reported that the typical age-of-onset of depression is early to mid-20s.2 Although no association between the age-of-onset and depressive subgroups has stood out, earlier age-of-onset patients tend to suffer more severe functional impairment, greater disease burden, and more suicide attempts.3 For college students who are in the critical transition from adolescence to adulthood, the onset of depression is of particular importance.4 In fact, it is becoming one of the main reasons for non-attendance, school dropout, increased suicidal thoughts, and debt crisis.5 Surveys investigating the prevalence of depression in college students have been conducted in some areas. For example, in the United States, it was estimated that 15.6% of undergraduates showed signs of depressive or anxiety disorder.6 Identifying the factors triggering or precipitating depression and understanding the natural course of depression are increasingly crucial public health goals. Over the past several decades, the literature describing risk factors and predictors of major depressive disorders has grown rapidly. A substantial number of studies have demonstrated the influence of stressful life events, personal cognitive styles, family history, and interpersonal and environmental variables on the onset of depression.7–9 A recent study also suggests that childhood sexual abuse has a direct impact on adult mental disorder and suicide.10 However, most of these studies were conducted on adults in Western societies. Little is known about the predictors of depressive disorders in Chinese college students. Due to social and cultural factors, Chinese people have been considered to deny depression and reluctant to admit to emotional distress. However, the influence of western culture and the introduction of depression detection have changed this situation to a certain degree.11 Now Chinese people are more open to affective expression and mental health problems, which is conducive to the identification of depressive symptoms and obtaining accurate data on the incidence rate of depression.
Factors such as parenting style, personality, and stressful life events can be used effectively to strengthen the etiological model of depressive symptoms. We undertook the present study to address several important gaps in the literature. Here, we examined and compared the ability of these psychosocial perspectives to account for subsequent depression as well as new onset of depression in Chinese college students.
Materials and Methods
Setting
First-year students from two of the top universities in Beijing were invited to participate in the survey.
Research Design
We used a prospective longitudinal design, involving five self-report questionnaires to study the incidence rate and risk factors of depressive symptoms in college students.
The cohorts were first year students, who enrolled in the universities in September, and the investigation began from November in the same year. The students were then invited to complete self-rating questionnaires every 5–7 months for the next two years.
Baseline Recruitment and Assessment
Because the academic year in Mainland China starts in September, the initial survey took place in November, two months after students enrolling in college. Investigators and coordinators described the study procedures in detail using leaflets and conducted the paper questionnaire to participating students before or after lectures. Students were volunteered to participate in the investigation and informed that only group data would be reported. To preserve anonymity, tear-off written informed consents were obtained at the baseline stage. Participants received a gift to thank them for their participation each time.
Baseline assessment procedures are described in our previous study.12 In brief, the social-demographic characteristics of the participants, as well as their parents’ socio-economic status, family and personal history of mental disorder, and their drink/drug misuse history were collected at baseline. Depression symptoms were assessed using the Center for Epidemiologic Studies Depression Scale (CES-D), anxiety symptoms were evaluated using the Zung self-rating anxiety scale (SAS), neuroticism level was measured by the brief revised Eysenck Personality Questionnaire-Neuroticism subscale (EPQ-N), and self-esteem was assessed by Rosenberg Self-Esteem Scale (SES). Frost Multidimensional Perfectionism Scale (FMPS) is a self-report measure containing 35 items divided in six subscales: (1) concern over mistakes (COM, 9 items), (2) organization (ORG, 6 items), (3) parental criticism (PC, 4 items), (4) parental expectations (PE, 5 items), (5) personal standards (PS, 7 items), and (6) doubts about actions (DA, 4 items). Egna Minneu av Bardndosnauppforstran (EMBU) was used to assess responders’ memories of perceived parental rearing behavior in childhood. EMBU is composed of 11 different subscales, five assessing the mother’s parenting style and six the father’s. These factors are: (1) Father-Warmth (F-W) and Mother-Warmth (M-W), (2) F-Penalty (F-P) and M-Penalty (M-P), (3) F-Overinvolvement-Overprotection (F-O), and M-Overinvolvement-Overprotection (M-O), (4) F-Favoring (F-F) and M-Favoring (M-F), and (5) F-Rejection (F-R) and M-Rejection (M-R). Participants’ stressful life events were assessed using the Chinese version of the Adolescents Self-Rating Life Events Checklist (ASLEC). Excessive daytime sleepiness was measured with the Epworth Sleepiness Scale (ESS), and physical activity was measured with the Godin Leisure-time exercise questionnaire.
Follow-Up of Subjects and Assessments
After obtaining baseline data on the outcome variables, we collected follow-up data 5, 12, 17, and 24 months after baseline.
The baseline survey was used to select specific classes. Coordinators were then asked to deliver the follow-up questionnaires to the students attending these classes. The last five digits of each student’s University and resident ID numbers, and mother surname were used to identify each student. CES-D, SAS, ASLEC, ESS, and Godin Leisure-time exercise questionnaires were collected at each follow-up times.
This study was approved by the Institutional Review Board (IRB) of the Institute of Mental Health, Peking University and The University of Hongkong. The IRB number is UW06-270T/1295. The study complied with the Declaration of Helsinki.
Data Entry and Quality Control
Data were entered manually using Epidata 3.1. To evaluate completeness and quality, data were subjected to automated checks (eg internal inconsistencies and out-of-range values). The accuracy of coding and entry in the database was checked by re-entering the data of the original 50 records in 5% of the subjects.
Statistical Analysis
All statistical analyses were performed using SPSS 15.0. Statistical significance was measured with 2-sided tests and evaluated at the 0.05 level of significance. The following statistical procedures were used for the data analysis.
Life table is commonly used for survival analysis. Survival/failure analysis study the occurrence of a specific event in a population and the time for such an event to take place. Over a determined period, only a subset of the population will have experienced the events. For these subjects, the length of time until the event occurs can be observed and analyzed. The other subjects are nevertheless informative. Because the measure is a duration, it is possible that for these subjects the time for the event to occur is longer than the duration of the study. Therefore the “end-point” for each subject is either the occurrence of the event under consideration (eg becoming depressed) or no occurrence of the event (censoring). Because some students were lost during follow-up time points, life table methods were used to calculate the two-year cumulative incidence of depressive symptoms in the target population. The analysis was performed using SPSS SURVIVAL LIFE TABLES.
The binary logistic regression analysis was used to determine the prediction of potential risk factors for onset depressive disorders. The strength of the association between predictors and onset depressive symptoms was estimated with odds ratios and 95% confidence intervals. To obtain the most parsimonious set of predictors, we ran a two-step logistic regression analysis with a model first including all socio-demographic predictors. The other predictors with significant results in univariate association tests (baseline subscales of EMBU, EPQ-N, SES, subscales of FMPS, ASLEC, SAS, ESS, week-day nighttime sleep duration and frequency of physical exercise) were then simultaneously entered into the logistic regression model. The analysis was performed using SPSS REGRESSION LOGISTIC.
Results
Descriptive Characters of Students
At the baseline, 1038 first-year students participated in the survey. A total of 758 students showed no depressive symptoms (CES-D < 16), including 391 males with mean age of 18.4±0.90 and 367 females with mean age of 18.1±0.78. Only students without depressive symptoms were followed for the duration of the study.
Cumulative Incidence of Depressive Symptoms
In the current study, “Cumulative Incidence (CI) of new onset depression” was defined as the proportion of participants with new depression symptoms (incident) (CES-D ≥ 16). CES-D scores below 16 at all follow-up times were regarded as negative for depression symptoms. New onset cases were defined by the occurrence of a clinically significant level of depressive symptoms (CES-D ≥ 16) at any follow-up time point. Participants with a clinically significant level of depressive symptoms at more than one follow-up were only regarded as one case.
Of 758 participants, 235 developed clinically significant depressive symptoms during the follow-up period, including 135 males and 100 females. To overcome the loss of participants between follow-ups, the two-year CI was calculated using the life table method. As shown in Table 1, the overall two-year CI was 42%, more specifically 49% for males and 35% for females. The Wilcoxon statistic test showed that the difference between males and females is not significant (χ2=3.138, df =1, p=0.077).
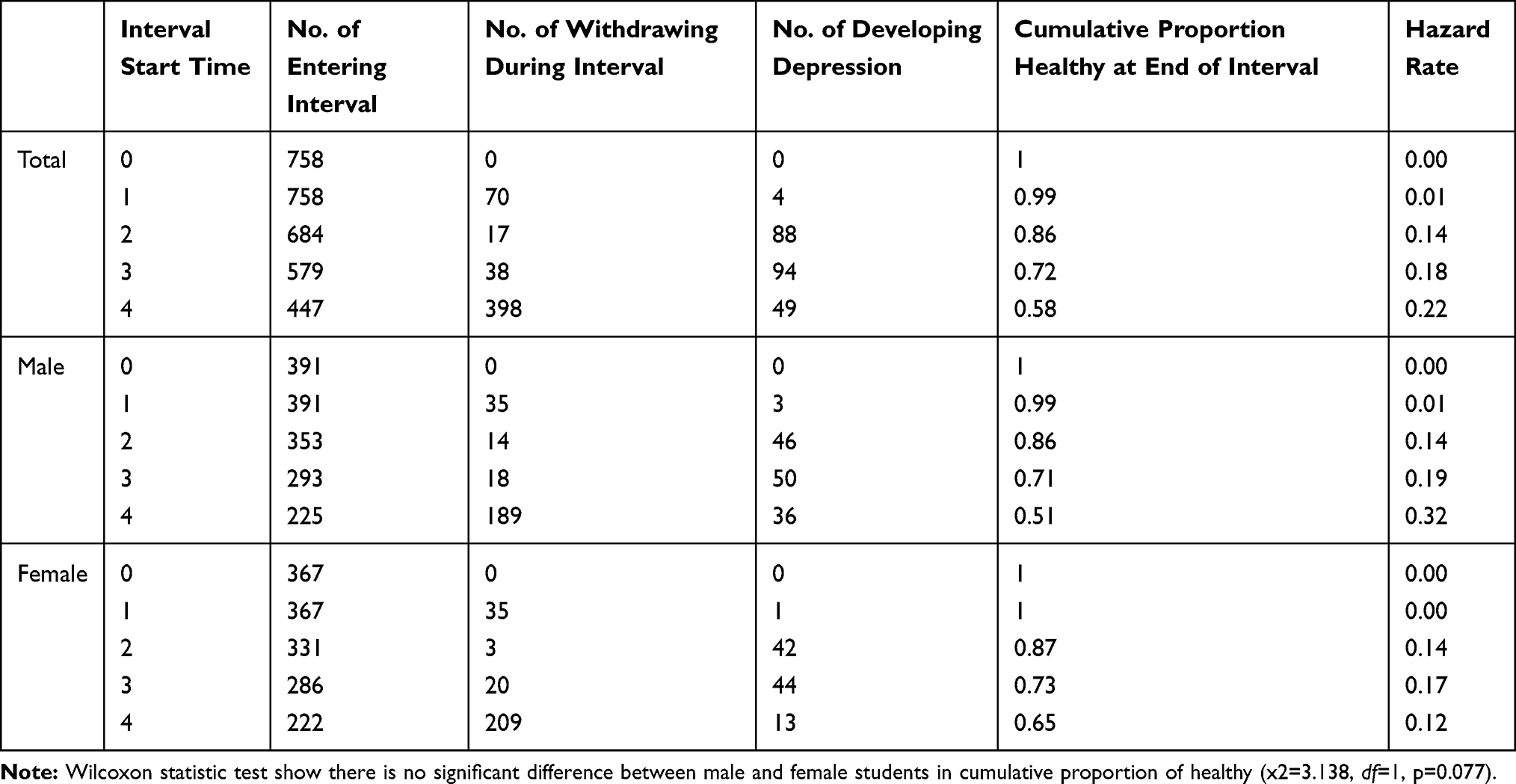 |
Table 1 Life Table of the Cumulative Proportion of No. of Depression at End of Interval |
Predictive Factors for the Onset of Depressive Symptoms
We first compared the baseline EPQ-N, SES, subscales of FMPS and EMBU between participants with new onset depression and without symptoms. The score results of EPQ-N, COM, DA, PD, and PC for students with new onset depression were significantly higher than for students without symptoms. In contrast, SES, ORG, P-W, P-F scores were significantly lower for depressed students compared to students without symptoms (Table 2).
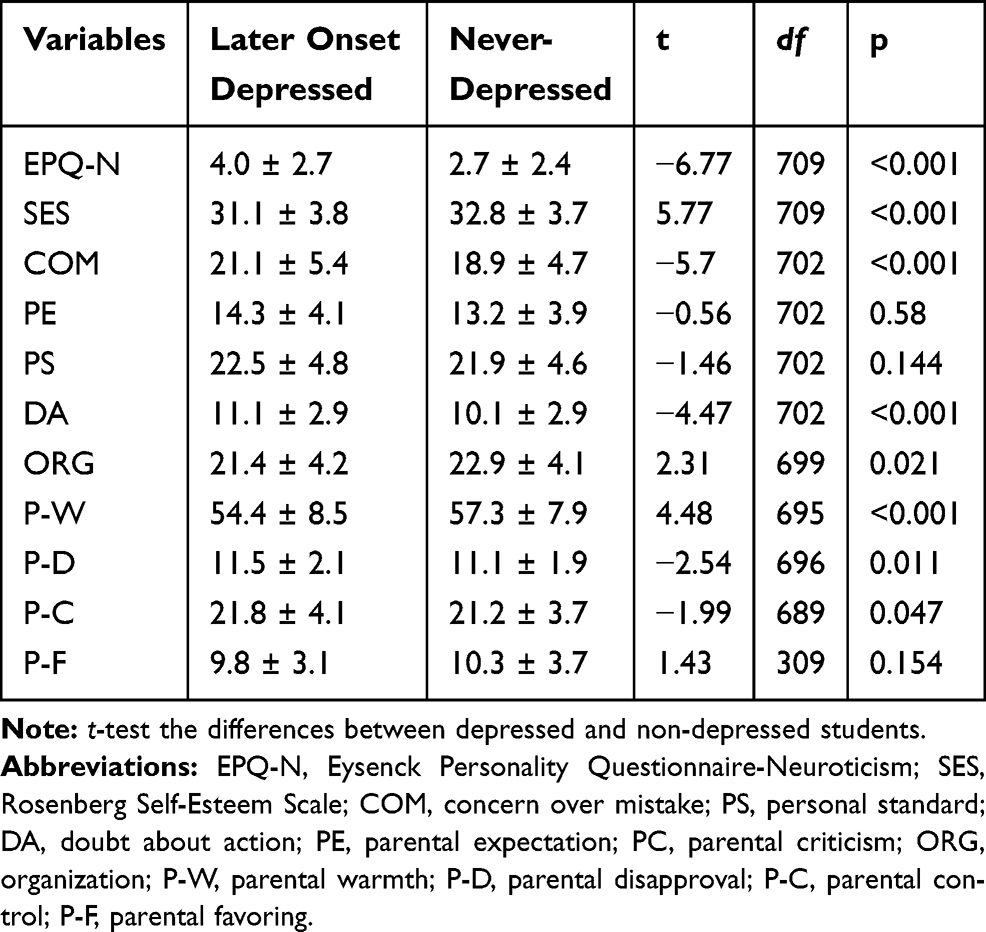 |
Table 2 The Mean Score of Baseline Personality Characteristic and Subscales of Parenting Style Between Later Onset Depressed and Never-Depressed College Freshmen (Mean ± SD) for the Two Years |
Table 3 shows the odd ratios estimate and 95% confidence intervals for each predictor. According to the multivariate model, the test comparing the full model including all predictors and the one constant model showed statistical significance (χ2 (18, N= 658) = 284.58, p < 0.001). This indicates that some predictors were specifically associated with either onset depression or no symptoms. However, only 66.5% of students with onset depression and 85.7% of students without symptoms were correctly predicted, for an overall success rate of 78.4%.
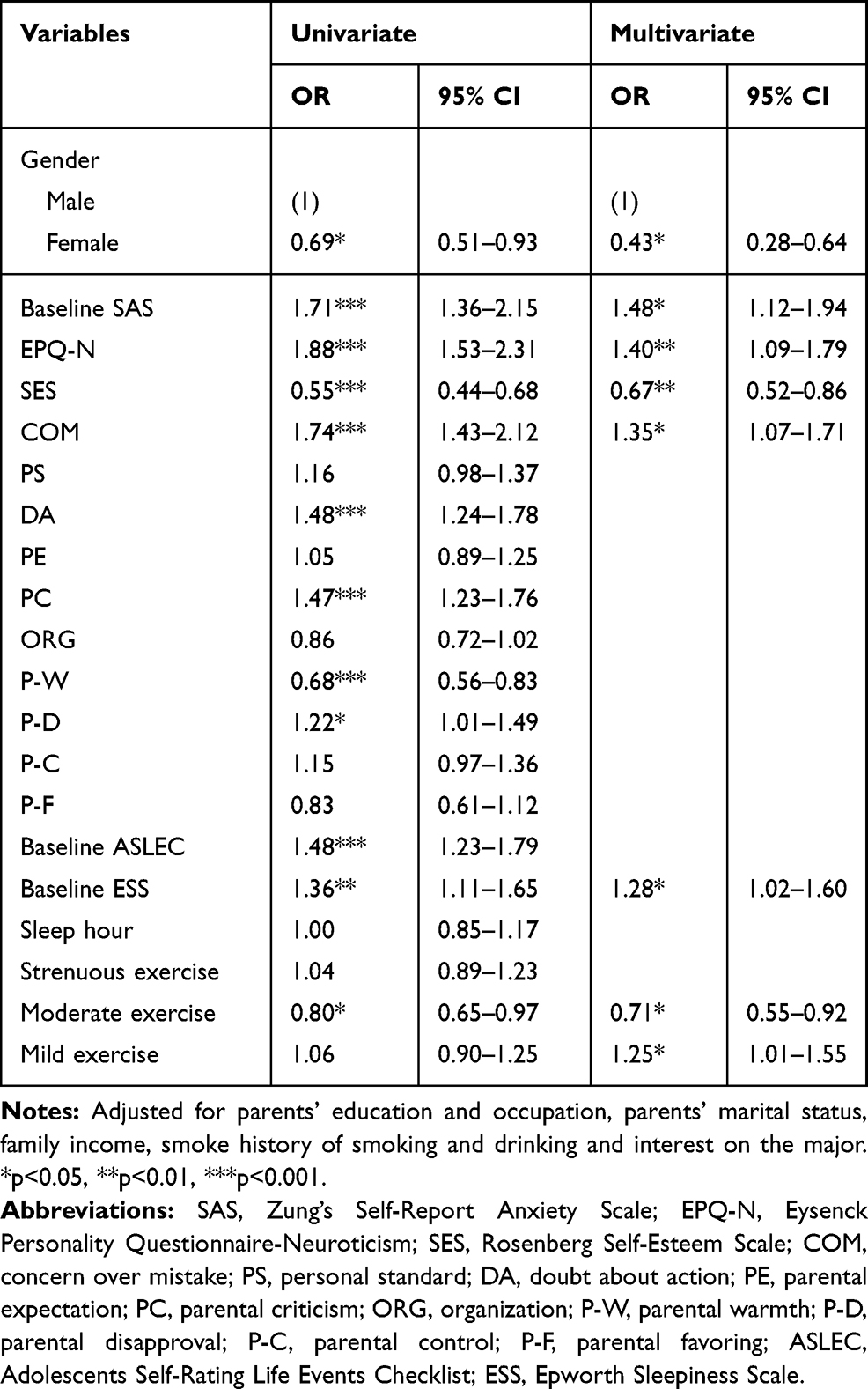 |
Table 3 Crude and Adjusted Odds Ratios with 95% Confidence Intervals (CI) of the Predictors for the Onset of Depressive Symptoms (Forward Method) |
According to the Wald criterion, logistic regression modeling showed that female gender (OR=0.43, 95% CI (0.28–0.64)), high level of SES (OR=0.67, 95% CI (0.52–0.86)) and moderate exercise (OR=0.71, 95% CI (0.55–0.92)) are factors associated with a lower risk of onset depression. In opposite, high level of baseline anxiety (OR=1.48, 95% CI (1.12–1.94)), EPQ-N (OR=1.40, 95% CI (1.09–1.79)), COM (OR=1.35, 95% CI (1.07–1.71)), ESS (OR=1.28, 95% CI (1.02–1.60)), and mild exercise (OR=1.25, 95% CI (1.01–1.55)) are associated with a higher risk of onset depression.
Discussion
High Incidence of Depressive Symptoms in Chinese College Students
In total, 42% of students without depressive symptoms (CES-D<16) at baseline (N=758 total) developed depressive symptoms (CES-D≥ 16) during the 2 years follow-up period. This figure may seem surprisingly high. However, the high incidence of depression in students has already been observed in other previous studies.13–15 For example, the one-year prevalence and incidence rates of DSM-IV major depressive episodes among first-year college students in Japan were 20.7% and 19.8% respectively.14 Another survey among college students in Canada found that elevated distress was significantly higher among students compared to the general population.16 In a meta-analysis by Xian-Yang Lei et al., the overall prevalence of depression among Chinese college students is 23.8%.17 Thus, the results of previous studies evaluating depression in college students already suggested that depressive symptoms may be more prevalent in college students than in the general population.
Psychosocial Risk Factors for the Onset of Depressive Symptoms
The present study examined the predictive effect of psychosocial factors on the onset of depressive symptoms (CES-D ≥16) among college students. Based on our results, baseline anxiety, premorbid neuroticism, concern over mistake, elevated daytime sleepiness, and greater mild physical exercise are factors associated with higher risk of onset depression in Chinese college students. On the other hand, high self-esteem and greater moderate physical exercise are associated with decreased onset of depressive symptoms.
Interestingly, we found that females were at lower risk of depression compared to their male counterparts, suggesting that gender may be an important factor to predict the onset of depressive symptoms in college students: males were 2,3-fold more likely than females to develop depressive symptoms. This result is not consistent with previous findings showing that females are 1–2 times more likely than males to suffer from depression in the general population. These data suggest that the risk of depression may not be inherently associated with the female gender per se. It is possible that the greater prevalence of depression observed in females in the general population is caused by gender-specific adverse factors such as childbirth, single parenthood, and household chores. A previous study has shown that stress associated with marital life, pregnancy, and children18 contributes to depression in females. The influence of gender on the incidence of depression among college students is controversial. In Lei’s study, no significant difference was found in the prevalence of depression between the male and the female students in university.17 There were also studies that found higher level of depression among females than males in late adolescence to early adulthood.19,20 In our study, all female students were single, without children, and lived a relatively simple campus life, which may further protect them from developing depression symptoms. These female students in this special period made them lower depression rate. Due to the influence of traditional ideas, young males are burdened with excessive expectations while they avoid talking about negative emotions, which explains the higher percentage of male students suffering from depression than the females at the same educational level. Our findings are consistent with the latest research report that a growing prevalence of depression was found among male students than females during college.21 Another study investigating the different categories of depressive disorders showed that the female gender was associated with comorbid depression (subjects with lifetime diagnoses of both dysthymia and major depressive disorder), but not major depressive disorder, depressive syndrome, or dysthymia.22
Anxiety is the most reliable factor to predict the occurrence and magnitude of fluctuation of depressive symptoms. Anxiety may lead to subsequent depression through biological, cognitive, or behavioral mechanisms. Chronic anxiety may induce a persistent elevation of the hypothalamus-pituitary-adrenal axis activity and lead to chronically raised cortisol levels and dysregulation of central monoamine and serotonin neurotransmitter systems.23,24 Chronic anxiety may also cause gradual shifts in cognitive processes (eg demoralization or cognitive distortions) or in behavior patterns and social interaction (eg avoidance behaviors that result in critical changes of lifestyle and life events) that lead to an increased risk for onset of depression.25 Wittchen et al. also suggested that individuals with severe anxiety disorders were likely to exhibit persistent avoidance behavior and consequent impairment of psychosocial function, which would lead to a greater risk of developing depressive symptoms.25 In the present study, high level of cumulative anxiety symptoms was a prognostic factor for a subgroup of students with persistently high levels of depressive symptoms.
In the present study, neuroticism was positively associated with the onset and magnitude of fluctuation of depressive symptoms. It suggested neuroticism as a predictor of depressive symptoms. Although neurosis is still vaguely defined, several studies have shown that neurotic individuals are at high risk for depression.26–28 Individuals with high level of neuroticism tend to have negative thoughts in response to setbacks due to their cognitive model, thus having a greater risk of depression.29 Hankin et al. found that high-level neurotic individuals were more likely to develop depressive symptoms when suffered from stress.30 We believe the accumulation of stressful life events in college students increases the risk of depressive symptoms. Moreover, we found that some subscales of perfectionism were associated with baseline and new onset of depressive symptoms; however, when analyzed together with other variables, their predictive power was non-significant. It is noteworthy that neuroticism has a role in the development and maintenance of perfectionism. Perfectionists with neurotic characteristics are more likely to suffer over anxiety, and the accumulated emotional disorder over time leads to more severe neuroticism.31–33
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IIIR), one of the six patients with depression eventually commits suicide.34 Studies have shown that 25.89% of Chinese college students had suicidal ideation.35 The suicide mortality of college students in China has reached 0.2‰, and it has become the leading cause of abnormal death among college students.36 According to a survey of attempted suicide, 29% of them commit suicide because of emotional disorder, and 20% due to neurotic disorder.37 Depression is one of the crucial predictors of suicidal ideation.38 Low self-esteem, which is caused by the increase of stressful life events followed by individual psychological stress, is one of the important factors for depression onset.39 In accordance with literatures, our results showed that high self-esteem was a protective personality character against depression in college students. Studies have shown that social isolation, adverse parenting style, lack of parental acceptance, and experience of trauma during childhood contribute to low self-esteem in adults.40 Overcoming low self-esteem is considered to be essential to mental health.41 Self-esteem enhancement programs have been found not only to increase self-esteem but also to change behavior, personality, emotional functioning, and academic performance in children and adolescents.42 Therefore, the pursuit of healthy self-esteem is crucial for college students to face the many changes and challenges occurring during their college years and beyond.
Stressful life events recorded at baseline were not correlated with the subsequent onset of depression but rather influenced the fluctuation of the symptoms. This is surprising considering that in Kendler’s study, recent stressful life events were the higher risk factors for the onset of depression.43 Lei’s study also showed that stressful life events played a key role in the development of depression.17 This can be explained considering the challenges associated with the measure of stressful life events and chronic difficulties. Their impact on depression may be influenced by a wide range of factors. Thus, the consequences of such events on an individual’s mental health depend mainly on the perceived undesirability, the fear of losing control, the life-threatening nature, and the duration of the event.44 In children, some studies have reported that loss, school, family, and friendship were the only life events associated with depression. In adults, more severe events considered beyond the control of an individual were strongly associated with depression. In this study, the measure of baseline stressful life events includes heterogeneous types of events with different propensities which makes it difficult to link them to the onset of depressive symptoms.
We found that moderate exercise was associated with lower risk of onset of depression, which is in accordance with previous studies that showed the strong correlation between exercise and lower level of depressive symptoms.45,46 Physical exercise, especially moderate-to-intense exercise, has been recognized to have beneficial effects on cognitive function and positive mood due to the increased levels of endorphin and serotonin.47 A similar longitudinal study showed that exercise predicted fewer depressive symptoms at follow-up.48,49 Some randomized controlled trials have reported that exercise training reduces depressive symptoms, with an effect size comparable to that of antidepressant medication.50 A study performed in US and Canadian populations has confirmed that higher levels of physical exercise are associated with lower CES-D scores, especially for people below 40.51 Unlike moderate exercise, mild exercise was positively correlated to the onset of depressive symptoms. It is possible that mild exercise was performed out of necessity rather than as a determined action to get exercise, therefore, its duration could have been perceived as a waste of time preventing studying or even performing more intensive exercise. In addition, the most sedentary students had no other options but to choose “mild” exercise in the questionnaire. For these cases, mild exercise meant no exercise which might explain why the correlation between mild exercise and onset of depressive symptoms was positive.
Inspiration on the Prevention of Depression in College
Although there is no significant correlation between levels of depression and academic achievement,52,53 it is indispensable to establish programs for prevention and intervention of depression among college students. This study may shed some light on the development of mental health programs for students in colleges. The depression level of students increased significantly in the first year of college; thus, it is necessary for schools to screen and track the mental health of freshmen. For the neurotic and maladaptive perfectionism students, psychology service in college should provide timely counseling. Moreover, it is preferred to reduce unnecessary pressure in the school life arrangement and guide students to develop exercise habits and adequate sleep.
Conclusions and Limitations
In summary, our study showed a surprisingly high incidence of depression among college students. There was no significant difference in the two-year cumulative incidence between male and female students, while a lower risk of depression in the females was observed. High level of self-esteem and moderate exercise reduced the onset of depressive symptoms, while neuroticism, anxiety, and lack of exercise increased the new onset of depressive symptoms.
There are limitations in our research. First, the geographical selection is single and the sample size is relatively small, which may affect the representativeness. Second, only questionnaires were conducted on the subjects in the study. Future studies should include more methods, such as interview, to ensure rigorous data and reduce bias. Last, this study lasted for two years, which only revealed the incidence rate of depression after enrolling in college. The fluctuation of depression symptoms in the four years among college students requires further research.
Abbreviations
CES-D, Center for Epidemiologic Studies Depression Scale; SAS, self-rating anxiety scale; EPQ-N, Eysenck Personality Questionnaire-Neuroticism; SES, Self-Esteem Scale; FMPS, Frost Multidimensional Perfectionism Scale; COM, concern over mistakes; ORG, organization; PC, parental criticism; PE, parental expectations; PS, personal standards; DA, doubts about; EMBU, Egna Minneu av Bardndosnauppforstran; F-W, Father-Warmth; M-W, Mother-Warmth; F-P, F-Penalty; M-P, M-Penalty; F-O, F-Overinvolvement-Overprotection; M-O, M-Overinvolvement-Overprotection; F-F, F-Favoring; M-F, M-Favoring; F-R, F-Rejection; M-R, M-Rejection; ASLEC, Adolescents Self-Rating Life Events Checklist; ESS, Epworth Sleepiness Scale; CI, Cumulative Incidence.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board (IRB) of the Institute of Mental Health, Peking University and The University of Hongkong. The IRB number is UW06-270T/1295. The study complied with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sax LJ. Health trends among college freshmen. J Am Coll Health. 1997;45(6):252–262. doi:10.1080/07448481.1997.9936895
2. Kessler RC, Bromet EJ. The epidemiology of depression across cultures. Annu Rev Public Health. 2013;34(1):119–138. doi:10.1146/annurev-publhealth-031912-114409
3. Zisook S, Lesser I, Stewart JW, et al. Effect of age at onset on the course of major depressive disorder. Am J Psychiatry. 2007;164(10):1539–1546. doi:10.1176/appi.ajp.2007.06101757
4. Damico N, Mechling B, Kemppainen J, et al. American college students’ views of depression and utilization of on-campus counseling services. J Am Psychiatr Nurses Assoc. 2016;22(4):302–311. doi:10.1177/1078390316648777
5. Richardson T, Elliott P, Roberts R, et al. A longitudinal study of financial difficulties and mental health in a national sample of British undergraduate students. Community Ment Health J. 2017;53:344–352.
6. Eisenberg D, Gollust SE, Golberstein E, et al. Prevalence and correlates of depression, anxiety, and suicidality among university students. Am J Orthopsychiatry. 2007;77(4):534–542. doi:10.1037/0002-9432.77.4.534
7. Petersen JJ, Paulitsch MA, Hartig J, et al. Factor structure and measurement invariance of the patient health questionnaire-9 for female and male primary care patients with major depression in Germany. J Affect Disord. 2015;170:138–142. doi:10.1016/j.jad.2014.08.053
8. Rodero-Cosano ML, Salinas-Pérez JA, González-Caballero JL, et al. A multi-level analysis of the relationship between spatial clusters of outpatient-treated depression, risk factors and mental health service planning in Catalonia (Spain). J Affect Disord. 2016;201:42–49. doi:10.1016/j.jad.2016.04.024
9. Hammen C. Risk factors for depression: an autobiographical review. Annu Rev Clin Psychol. 2018;14(1):1–28. doi:10.1146/annurev-clinpsy-050817-084811
10. Qin X, Zheng JY, Yin XH, et al. Early life sexual abuse is associated with increased suicide attempts: an update meta-analysis. J Psychiatr Res. 2018;99:129–141. doi:10.1016/j.jpsychires.2018.02.001
11. Parker G, Gladstone G, Chee KT. Depression in the planet’s largest ethnic group: the Chinese. Am J Psychiatry. 2001;158(6):857–864. doi:10.1176/appi.ajp.158.6.857
12. Song Y, Huang Y, Liu D, et al. Depression in college: depressive symptoms and personality factors in Beijing and Hong Kong college freshmen. Compr Psychiatry. 2008;49(5):496–502. doi:10.1016/j.comppsych.2008.02.005
13. Clark DC, Zeldow PB. Vicissitudes of depressed mood during four years of medical school. JAMA. 1988;260(17):2521–2528. doi:10.1001/jama.1988.03410170069036
14. Tomoda A, Mori K, Kimura M, et al. One-year prevalence and incidence of depression among first-year university students in Japan: a preliminary study. Psychiatry Clin Neurosci. 2000;54(5):583–588. doi:10.1046/j.1440-1819.2000.00757.x
15. Wolanin A, Hong E, Marks D, et al. Prevalence of clinically elevated depressive symptoms in college athletes and differences by gender and sport. Br J Sports Med. 2016;50(3):167–171. doi:10.1136/bjsports-2015-095756
16. Adlaf EM, Gliksman L, Demers A, et al. The prevalence of elevated psychological distress among Canadian undergraduates: findings from the 1998 Canadian campus survey. J Am Coll Health. 2001;50(2):67–72. doi:10.1080/07448480109596009
17. Lei XY, Xiao LM, Liu YN, et al. Prevalence of depression among Chinese university students: a meta-analysis. PLoS One. 2016;11(4):e0153454. doi:10.1371/journal.pone.0153454
18. Rosal MC, Ockene IS, Ockene JK, et al. A longitudinal study of students’ depression at one medical school. Acad Med. 1997;72(6):542–546. doi:10.1097/00001888-199706000-00022
19. Mikolajczyk RT, Maxwell AE, El Ansari W, et al. Prevalence of depressive symptoms in university students from Germany, Denmark, Poland and Bulgaria. Soc Psychiatry Psychiatr Epidemiol. 2008;43(2):105–112. doi:10.1007/s00127-007-0282-0
20. Franko DL, Striegel-Moore RH, Bean J, et al. Self-reported symptoms of depression in late adolescence to early adulthood: a comparison of African-American and Caucasian females. J Adolesc Health. 2005;37(6):526–529. doi:10.1016/j.jadohealth.2004.08.028
21. Gao WJ, Ping SQ, Liu XQ. Gender differences in depression, anxiety, and stress among college students: a longitudinal study from China. J Affect Disord. 2019;263.
22. Chen LS, Eaton WW, Gallo JJ, et al. Empirical examination of current depression categories in a population-based study: symptoms, course, and risk factors. Am J Psychiatry. 2000;157(4):573–580. doi:10.1176/appi.ajp.157.4.573
23. Ressler KJ, Nemeroff CB. Role of serotonergic and noradrenergic systems in the pathophysiology of depression and anxiety disorders. Depress Anxiety. 2000;12(Suppl 1):2–19.
24. Risbrough VB, Stein MB. Role of corticotropin releasing factor in anxiety disorders: a translational research perspective. Horm Behav. 2006;50(4):550–561. doi:10.1016/j.yhbeh.2006.06.019
25. Wittchen HU, Kessler RC, Pfister H, et al. Why do people with anxiety disorders become depressed? A prospective-longitudinal community study. Acta Psychiatr Scand Suppl. 2000;102(406):14–23. doi:10.1111/j.0065-1591.2000.acp29-03.x
26. Kendler KS, Kuhn J, Prescott CA. The interrelationship of neuroticism, sex, and stressful life events in the prediction of episodes of major depression. Am J Psychiatry. 2004;161(4):631–636. doi:10.1176/appi.ajp.161.4.631
27. Chien LL, Ko HC, Wu JYW. The five-factor model of personality and depressive symptoms: one-year follow -up. Pers Individ Dif. 2007;43(5):1013–1023. doi:10.1016/j.paid.2007.02.022
28. Hutchinson JG, Williams PG. Neuroticism, daily hassles, and depressive symptoms: an examination of moderating and mediating effects. Pers Individ Dif. 2007;42(7):1367–1378. doi:10.1016/j.paid.2006.10.014
29. Kercher AJ, Rapee RM, Schniering CA. Neurticism, life events and negative thoughts in the development of depression in adolescent girls. J Abnorm Child Psychol. 2009;37(7):903–915. doi:10.1007/s10802-009-9325-1
30. Hankin BL, Abela JRZ. Depression from childhood through adolescence and adulthood. In: Hankin BL, Abela JRZ, editors. Development of Psychopathology: A Vulnerability -Stress Perspective. New York: Sage Publications, Ins; 2005:245–280.
31. Hamachek DE. Psychodynamics of normal and neurotic perfectionism. Psychol J Human Behav. 1978;15:27–33.
32. Paul L. Perfectionism and neuroticism in psychiatric patients and college students. Pers Individ Dif. 1991;12(3):273–279. doi:10.1016/0191-8869(91)90113-P
33. Andrew PH, Thomas C. Multidimensional perfectionism and burnout: a meta-analysis. Pers Soc Psychol Rev. 2015;20:269–288.
34. Volkmar FR. Encyclopedia of Autism Spectrum Disorders. Volkmar FR, eds. New York, NY: Springer; 2013.
35. He H, Yang Y. Path analysis on the influencing factors of suicide ideation among college students in Beijing. Chin J Sch Health. 2015;36:80–83.
36. Liu TS, Xiao SY. The social expression and changes of suicide in the past 60 years in people’s daily.
37. Eitou C, Seisonn R. Psychological education: an emergency treatment strategy in psychiatric department. Clin Psychiatry. 2014;43:763–769.
38. Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016;316(21):2214. doi:10.1001/jama.2016.17324
39. Sowislo JF, Orth U. Does low self-esteem predicts depression and anxiety? A meta-analysis of longitudinal studies. Psychol Bull. 2013;139(1):213–240. doi:10.1037/a0028931
40. Miller L, Warner V, Wickramaratne P, et al. Self-esteem and depression: ten year follow-up of mothers and offspring. J Affect Disord. 1999;52(1–3):41–49. doi:10.1016/S0165-0327(98)00042-1
41. DuBois DL, Flay BR. The healthy pursuit of self-esteem: comment on and alternative to the Crocker and Park (2004) formulation. Psychol Bull. 2004;130(3):415–420. doi:10.1037/0033-2909.130.3.415
42. Haney P, Durlak JA. Changing self-esteem in children and adolescents: a meta-analytic review. J Clin Child Psychol. 1998;27(4):423–433. doi:10.1207/s15374424jccp2704_6
43. Kendler KS, Kessler RC, Neale MC, et al. The prediction of major depression in women: toward an integrated etiologic model. Am J Psychiatry. 1993;150:1139–1148.
44. Bruce ML. Psychosocial risk factors for depressive disorders in late life. Biol Psychiatry. 2002;52(3):175–184. doi:10.1016/S0006-3223(02)01410-5
45. De Moor MH, Beem AL, Stubbe JH, et al. Regular exercise, anxiety, depression and personality: a population-based study. Prev Med. 2006;42(4):273–279. doi:10.1016/j.ypmed.2005.12.002
46. Steptoe A, Butler N. Sports participation and emotional wellbeing in adolescents. Lancet. 1996;347(9018):1789–1792. doi:10.1016/S0140-6736(96)91616-5
47. Qin X, Yih XH, Chan W, et al. Managing childhood and adolescent attention-deficit/hyperactivity disorder (ADHD) with exercise: a systematic review. Complement Ther Med. 2017;34:123–128. doi:10.1016/j.ctim.2017.08.018
48. Brown WJ, Ford JH, Burton NW, et al. Prospective study of physical activity and depressive symptoms in middle-aged women. Am J Prev Med. 2005;29(4):265–272. doi:10.1016/j.amepre.2005.06.009
49. Donna KS, Elizabeth BC, Catherine C. Cross-sectional and prospective study of exercise and depressed mood in the elderly: the Rancho Bernardo study. Am J Epidemiol. 2001;153(6):596–603. doi:10.1093/aje/153.6.596
50. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. 2007;69(7):587–596. doi:10.1097/PSY.0b013e318148c19a
51. Steptoe A, Edwards S, Moses J, et al. The effects of exercise training on mood and perceived coping ability in anxious adults from the general population. J Psychosom Res. 1989;33(5):537–547. doi:10.1016/0022-3999(89)90061-5
52. Yeh YC, Yen CF, Lai CS, et al. Correlations between academic achievement and anxiety and depression in medical students experiencing integrated curriculum reform. Kaohsiung J Med Sci. 2007;23:379–386. doi:10.1016/S0257-5655(07)70001-9
53. Bahmani DS, Faraji R, Faraji P, et al. Depression and loneliness did not affect academic achievement among university students. Eur Psychiatry. 2017;41(S1):S541. doi:10.1016/j.eurpsy.2017.01.750
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.