")
Back to Journals » Clinical Ophthalmology » Volume 13
Incidence and prevalence of vitreomacular traction with and without macular hole in Germany
Authors Menzler J, Neubauer AS, Haritoglou C, Jackson TL
Received 25 September 2018
Accepted for publication 14 November 2018
Published 15 January 2019 Volume 2019:13 Pages 177—188
DOI https://doi.org/10.2147/OPTH.S188704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jacob Menzler,1 Aljoscha Steffen Neubauer,1,2 Christos Haritoglou,3 Timothy L Jackson4
1Institute for Health- and Pharmacoeconomics/Neubauer Consult, Munich, Germany; 2Private practice, Munich, Germany; 3Herzog Carl Theodor Eye Hospital, Munich, Germany; 4Department of Ophthalmology, Faculty of Life Course Sciences and Medicine, King’s College London, London, UK
Purpose: Symptomatic vitreomacular adhesion (sVMA) comprises vitreomacular traction (VMT) and stage 1 and 2 full-thickness macular holes (MHs) associated with vitreomacular adhesion (VMA). We aimed to estimate the incidence and prevalence of sVMA in Germany.
Materials and methods: A systematic literature review was conducted to identify the incidence and prevalence of sVMA based on international epidemiologic studies, weighted for study size and then averaged across eligible studies. A second systematic review aimed to estimate the proportion of vitrectomy undertaken for sVMA in Germany. This was combined with the reported number of vitrectomies in Germany in 2016 to estimate the number of patients undergoing vitrectomy for sVMA.
Results: The prevalence of sVMA is 1,365 per 100,000 population, with an incidence of 6.96 per 100,000 per year. For Germany, this translates to 1,119,300 cases, with 5,700 new cases reported annually. Analyzing the national hospital statistics, ~2,300 patients undergo vitrectomy due to sVMA in Germany each year, of which about 1,700 patients have VMT.
Conclusion: Incidence figures, driven by patients presenting to clinic, are much lower than expected based on population-based studies, suggesting that many patients with sVMA exist outside of the clinic system.
Keywords: epidemiology, vitreous body, vitreous pathology, vitreous adhesion, vitreous detachment, pars plana vitrectomy
Introduction
As part of normal aging, the vitreous body liquefies and usually starts to separate from the posterior retina, described as posterior vitreous detachment. Incomplete separation at the macula is described as vitreomacular adhesion (VMA), which is not, in itself, pathological and is, by definition, not associated with morphological alterations of the retina or functional loss. In contrast, if residual, focal, vitreomacular tractional (VMT) forces lead to a distortion of retinal tissue, visual symptoms may occur. This condition is described as VMT (syndrome). In the course of VMT, the development of a full-thickness macular hole (MH) may be observed. In the literature, VMT, with or without MH, is often referred to as symptomatic VMA (sVMA).
Structural changes are usually best seen using optical coherence tomography (OCT) and are characterized by retinal distortion, intraretinal cysts, and foveal elevation. Full-thickness MHs may retain vitreous traction, or this may subsequently pull free. Both VMT and MH may resolve spontaneously, although this becomes increasingly unlikely with increasing size or longer duration of an MH.1
Symptoms of sVMA typically include metamorphopsia and decreased distance and reading visual acuity,2 although some patients describe significant symptoms despite relatively well-preserved retinal structures. The indication of treatment of sVMA is usually based on the patients’ complaints and function, and includes watchful waiting in less-pronounced cases, an intravitreal injection of a vitreolytic agent (ocriplasmin), or pars plana vitrectomy (PPV).1,3
While the epidemiology of MHs is relatively well documented, this is not always broken down by MH stage or the presence or absence of vitreous adhesion. Therefore, combined with incomplete epidemiological data on VMT, the overall epidemiological burden of sVMA is unclear. To address this uncertainty, Jackson et al completed a systematic review regarding the epidemiology of sVMA,4 which was published 5 years ago. One may hypothesize that since then, figures may have changed due to an aging population and, even more important, higher-resolution OCT imaging being available. Based on the developments of high-resolution imaging, the staging of these conditions was revisited and new classification systems for sVMA and MHs have been suggested.1,2,5 However, for the present investigation, we used the MH classification published by the American Academy of Ophthalmology (AAO).1 Given this background, we aimed to update Jackson’s analysis using international published data and then combine this with German vitrectomy data in order to estimate the burden of sVMA in Germany.
Materials and methods
Two systematic literature searches were conducted using the EMBASE and Medline databases and the Ovid interface. The first literature search targeted all eligible epidemiologic studies concerned with VMT and idiopathic MHs. The second collected all available data on MH staging and surgery in Germany. For the number of vitrectomies due to MH, we analyzed hospital data from the German national hospital reimbursement data.6
Search for epidemiologic studies on VMT
In the first search, we used the following search terms in all search fields: vitreomacular traction, vitreoretinal traction, VMT, VMTS (vitreomacular traction syndrome), vitreomacular adhesion, vitreoretinal adhesion, VMA, vitreous AND macula AND separation, vitreous detachment, retinal detachment, macular detachment, macular hole, MH, retinal Hole, full-thickness macular hole, macular foramen and FTMH.
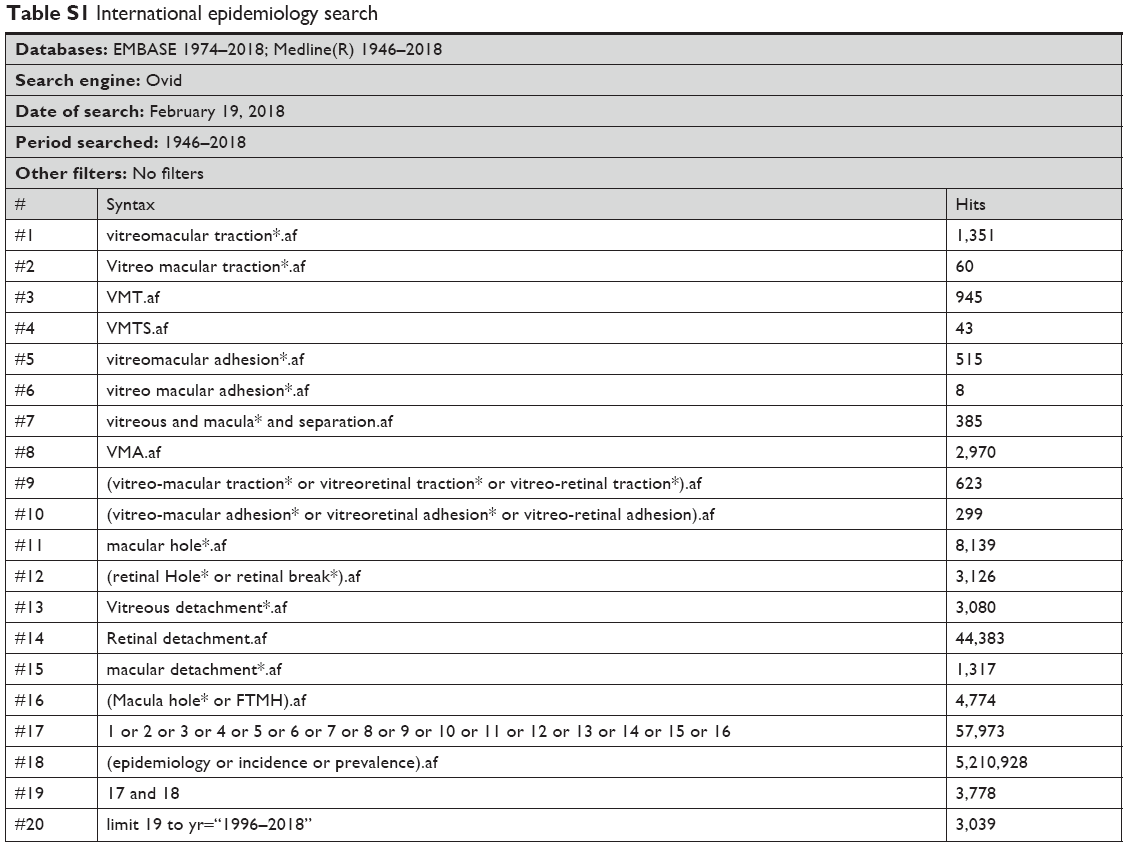
To filter for epidemiologic literature, we used the term “Epidemiology[MeSH:NoExp] OR Incidence[Title/abstract] OR Prevalence[Title/abstract] OR Epidemiology[Title/abstract]” as proposed by Orphan.net.7 The details of the search strategies are shown in Table S1.
The search was conducted on February 19, 2018, by JM and AN, who independently sorted the articles and extracted the data. Differences were solved by discussion. To be included in the study, articles had to meet the inclusion and exclusion criteria listed in Table 1.
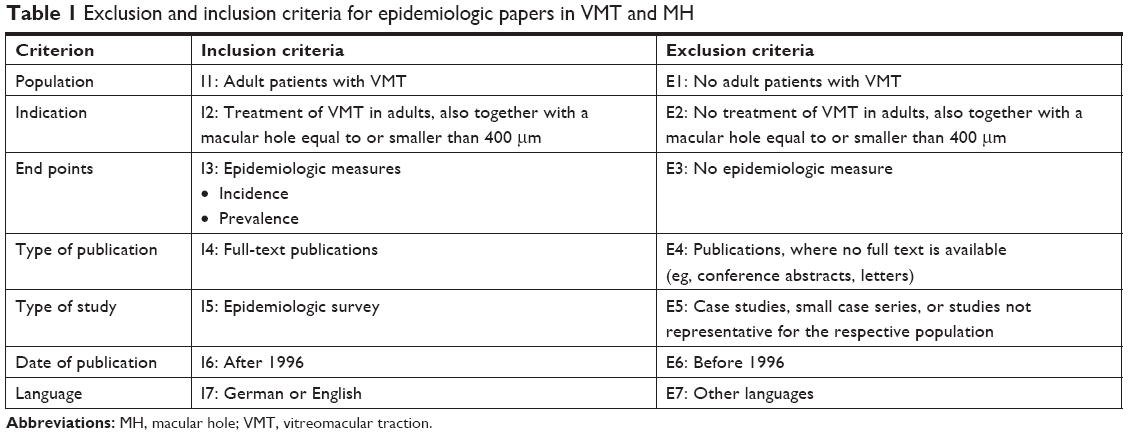 | Table 1 Exclusion and inclusion criteria for epidemiologic papers in VMT and MH |
MH stages in German vitrectomy patients
In the second search, we applied the following disease terms in all search fields: vitreomacular traction, vitreoretinal traction, VMT, VMTS, vitreomacular adhesion, vitreoretinal adhesion, macular hole, MH, Retinal Hole, full-thickness macular hole, macular foramen and FTMH. Defining the intervention, we used the terms “vitrectomy OR PPV OR pars plana OR surgery OR operation” in all fields and combined both searches using the AND operator.
The resulting set of articles was condensed by searching for the term “German” in all search fields. The search was conducted on February 19, 2018, by JM and AN, who independently selected the articles and extracted the data. Differences were resolved by discussion. The articles were sorted based on the inclusion and exclusion criteria listed in Table 2. Search strategies are shown in detail in Table S2.
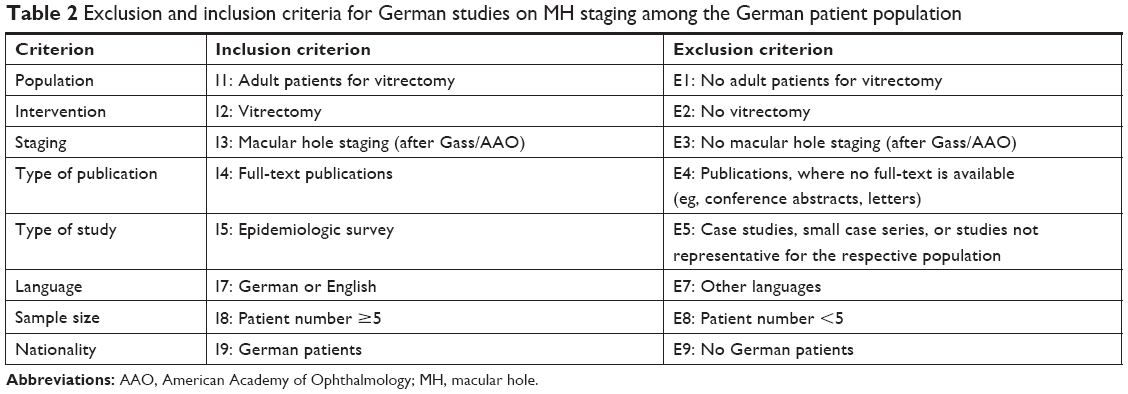 | Table 2 Exclusion and inclusion criteria for German studies on MH staging among the German patient population |
Number of vitrectomies due to an MH in Germany
We determined the number of PPVs in Germany in 2016 for a VMT using data from the Institut für das Entgeltsystem im Krankenhaus (InEK), the institute that facilitates reimbursement to hospitals. InEK collects all codes used by hospitals for billing of medical services.6 The codes used were ICD-10, Diagnosis Related Groups (DRG), and Operationen und Prozedurenschlüssel (OPS), all version 2016.
We filtered the data set for patients with the DRG codes C03A, C03B, or C03C indicating a retinal surgery. Two subsets were created using either the ICD-10 codes for macular pathology, H35.3 and H35.8, that include the diagnoses of VMT and MH, or the OPS codes for retinal surgery including macular manipulation 5-158.0, 5-158.1, 5-158.2, 5-158.4, 5-158.x, 5-158.y. The OPS codes included all relevant PPVs.8 Finally, we searched for patient numbers emerging in both DRG code subsets, created using either the ICD-10 codes or the OPS codes. Those patients matching both criteria (diagnosis defined by ICD and procedure defined by OPS) were assumed to have undergone vitrectomy due to an MH, VMT, and/or epiretinal membrane as well as some less-frequent macular diseases. Distribution of MH stages from the systematic literature research was applied to derive numbers for stage 1 and 2 MH.
Results
VMT prevalence and incidence in population-based studies
The systematic literature search for international epidemiologic studies resulted in 3,039 articles. This included 1,409 duplicates that were identified by review of the title and abstract and then removed. The abstract and title search resulted in 43 articles for full-text screening, of which 12 met the eligibility and were included (Table 1). Figure 1 shows the flowchart of the systematic literature search.
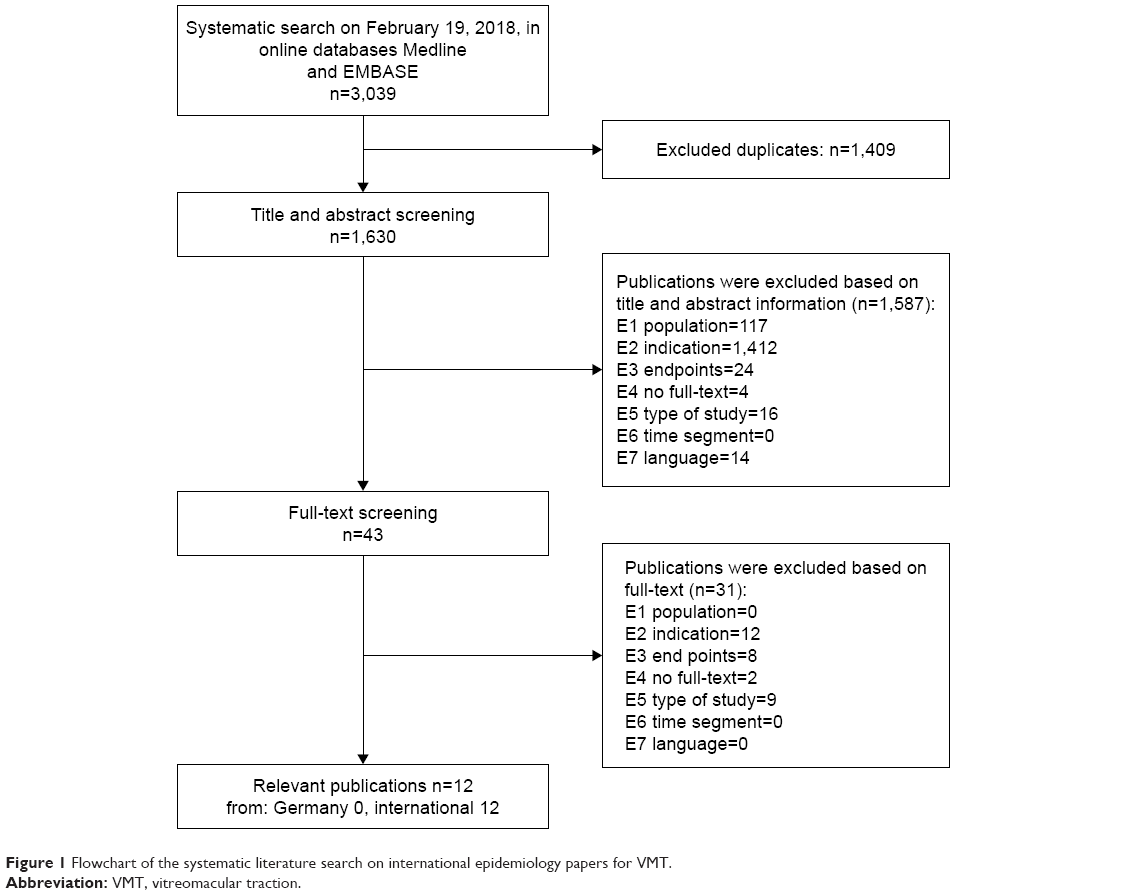 | Figure 1 Flowchart of the systematic literature search on international epidemiology papers for VMT. |
Seven publications reported epidemiologic data on VMT and five on MH. Study details are shown in Table 3, listing design, population, sample size, diagnostic methods, and epidemiologic measures. With the exception of three studies,9–11 all used OCT to diagnose VMT or MH. In most studies, the MH stage was not reported according to the current AAO classification.1
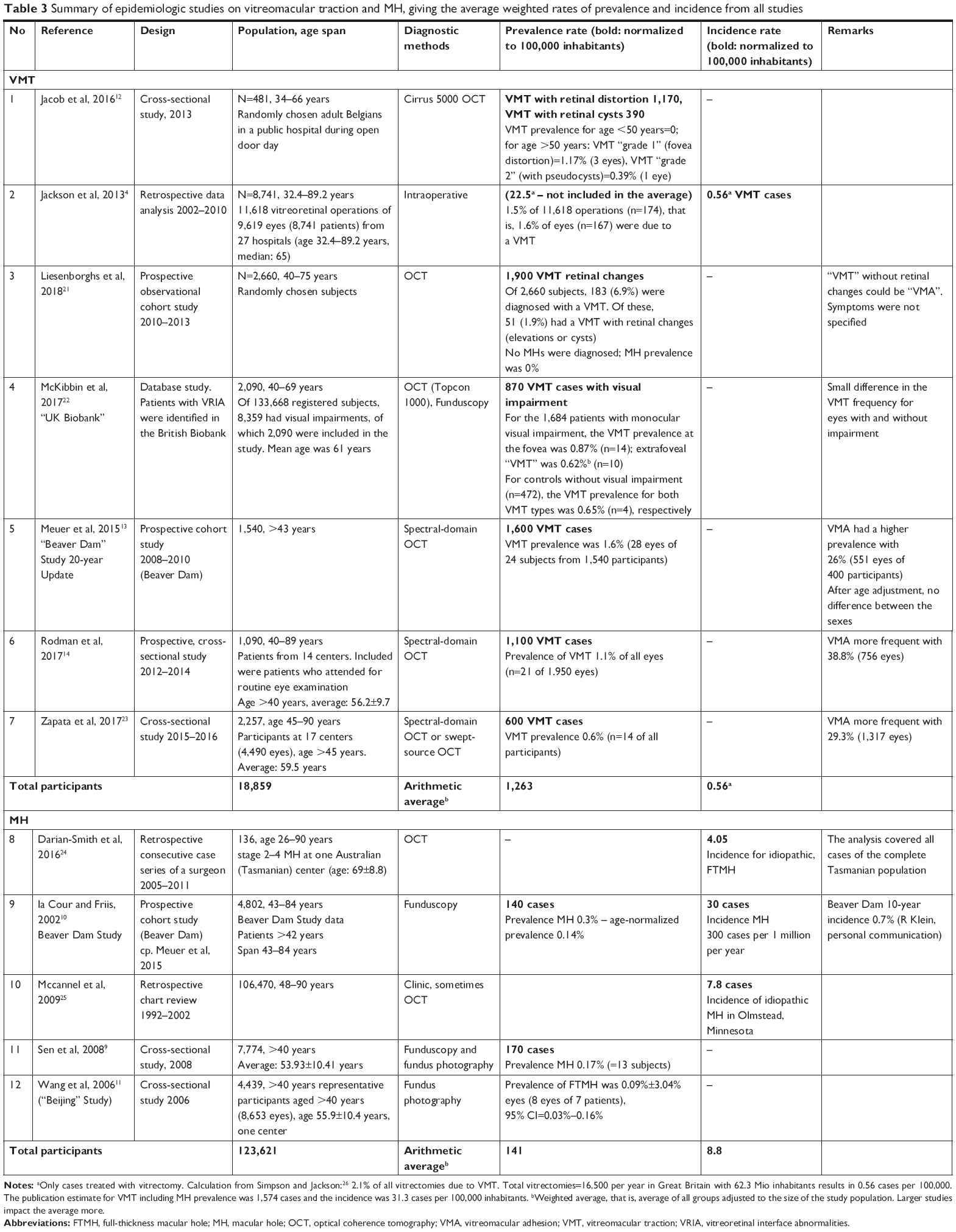 | Table 3 Summary of epidemiologic studies on vitreomacular traction and MH, giving the average weighted rates of prevalence and incidence from all studies |
All studies included quite large population samples, with varying estimates of VMT prevalence that are summarized in Table 3. The incidence rate was estimated in only one study.4 For MH, both rates were estimated by at least three publications (Table 1). From the given rates, we calculated the arithmetic average (Table 3).
For VMT, we calculated from seven studies with a total of 18,859 participants (age range: 32–90 years) an average prevalence of 1.263 cases per 100,000. The incidence rate was reported by only one study with 0.56 cases per 100,000.4 Averaging the data of five studies with a total of 123,621 participants (age range: 26–90 years), we calculated an average prevalence for MH of 141 cases per 100,000 and an average annual incidence of 8.8 cases per 100,000.
We then aimed to refine these incidence and prevalence figures to consider just the subpopulation which had sVMA, namely, VMT with or without MH (Table 4). All patients with a diagnosis of VMT were included, while those patients diagnosed with an MH only (72.8%) had a concomitant VMT according to Jackson’s review of the literature.4 Therefore, the incidence and prevalence rates for MH were reduced to 72.8% of their reported values in Table 4 to capture only those MHs with coexisting VMT. The resulting prevalence rate, including all cases of VMT plus all MH cases with coexisting VMT, was 1.365 cases per 100,000 inhabitants with an incidence rate of 6.96 new cases per 100,000 inhabitants per year. Applied to the German population of roughly 82 million, every year, about 5,700 new cases of sVMA would be observed. From the literature, a prevalent pool of 1,119,300 patients is calculated.
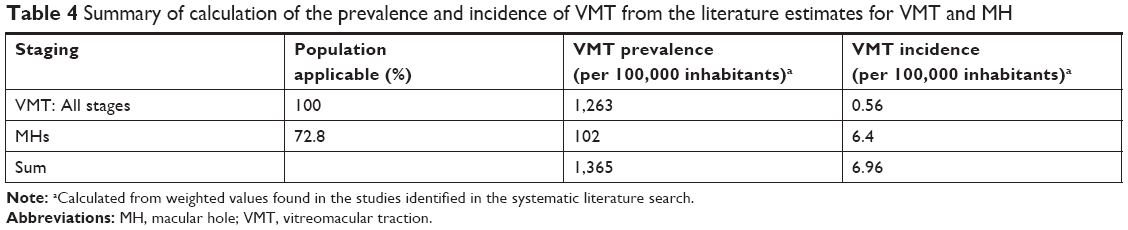 | Table 4 Summary of calculation of the prevalence and incidence of VMT from the literature estimates for VMT and MH |
MH stages in German vitrectomy patients
The literature search about MH stage rates in Germany resulted in 719 hits containing 159 duplicates. From these, 31 articles (Table 3) were included. Figure 2 shows the flowchart of the systematic literature search.
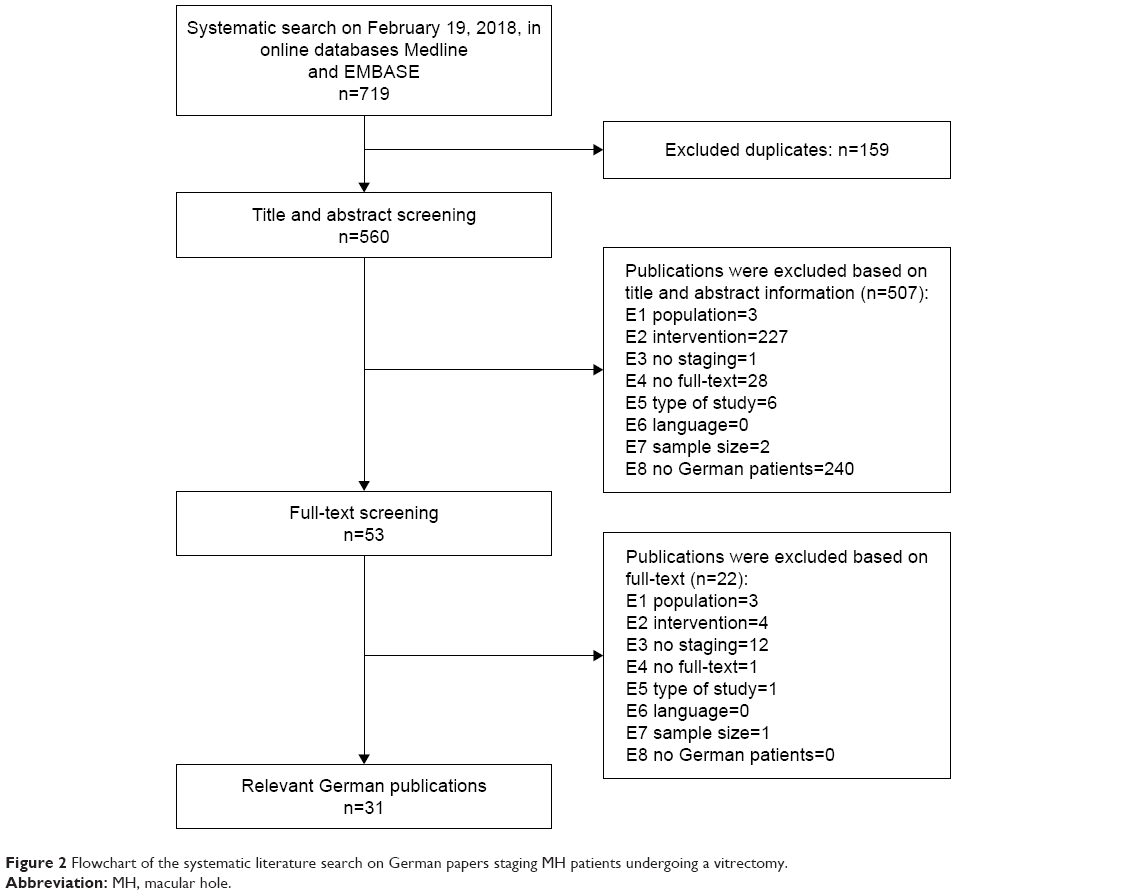 | Figure 2 Flowchart of the systematic literature search on German papers staging MH patients undergoing a vitrectomy. |
To estimate the surgical numbers for Germany based on real-world clinical data, we first made a literature search to determine the MH stage distribution of patients in Germany who underwent a PPV. Included studies are listed in Table 5, indicating sample size and staging distribution. For evaluation, we pooled the patients of stages 3 and 4 and calculated the weighted average.
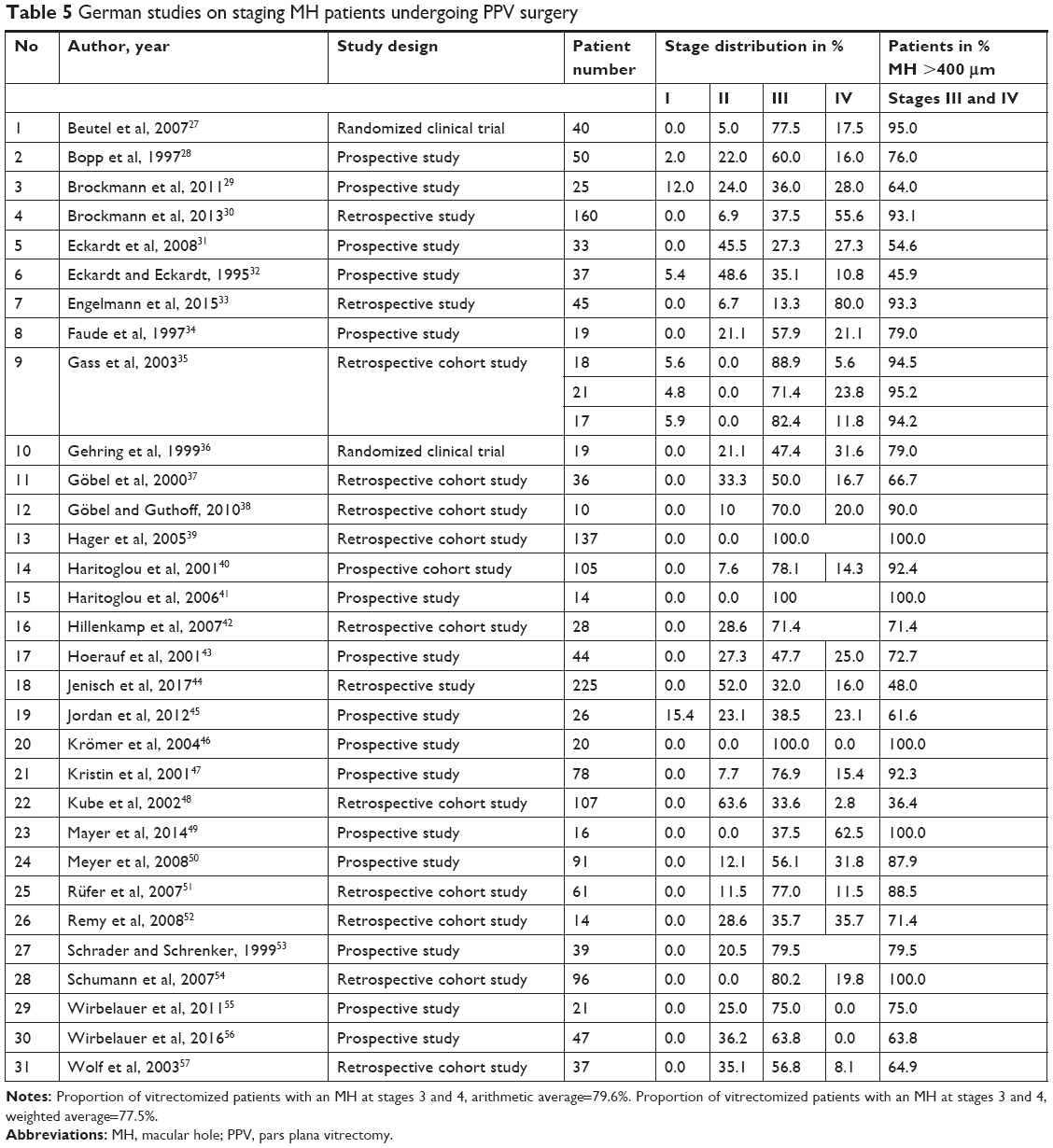 | Table 5 German studies on staging MH patients undergoing PPV surgery |
About 77% of all patients receiving a PPV for MHs in Germany had a stage 3 or 4 MH. Therefore, 23% had a stage 1 or 2 MH, including VMT.
Estimation of German VMT patients based on hospital surgery statistics
According to the INEK data, 52,223 patients underwent retinal surgery in Germany in 2016 and 34,314 of these underwent a PPV base on OPS codes. Of the 52,223 patients, about 15,878 had ICD-10 codes H35.3 or H35.8, indicating any macular changes, including VMT and MH, but also including patients with surgery for other macular changes such as epiretinal membrane. Selecting patients in the overlap of the ICD-10 and OPS subgroups resulted in a sample of 9,941 patients. This group most likely included patients who underwent a PPV for MH or VMT, but due to nonspecific codes with the ICD-10 and OPS, it is likely that it also included patients with other macular diseases, in particular, epiretinal membrane.
Applying the stage distribution given in the literature (Table 5) to these 9,941 patients, 7,655 patients had a stage 3 or 4 MH and 2,287 patients had an sVMA, that is, stage 1 or 2 MH and/or a VMT. Considering that not all MHs show concomitant VMT, only 72.8% of patients with MH had concomitant VMT,4 the numbers for stage 1 or 2 MHs and a VMT reduced to 1,665 vitrectomies for patients with VMT or MH stages 1 or 2 with VMT in Germany.
Discussion
In the present work, we estimated the incidence and prevalence of VMT, with and without MH, based on 12 large international studies. We found a prevalence of 1,365 cases per 100,000 population and an incidence rate of 6.96 new cases per 100,000 population per year.
There is an apparent discrepancy between the incidence and prevalence rates, in that the prevalence is more than expected based on incident cases. There may be several reasons for this difference. First, the rate of spontaneous resolution of VMT (with or without MH) could be higher than previously assumed, and thus, only a small proportion of lesions that exist in the population-based studies (which drives our prevalence rates) progress to eye clinics/hospitals (which drives our incidence rates). This is possible as our understanding of the natural history of VMT and MH is largely based on clinical data, whereas the natural history of those outside of a clinic/hospital environment may differ. The use of OCT may also enable us to detect lesions much earlier than in previous studies, and earlier lesions might be more likely to resolve. Perhaps, the most likely explanation is that population-based studies may pick up asymptomatic cases that do not progress to intervention, unlike studies based on patients presenting to clinic or surgery.12–14 More epidemiologic studies are needed to determine the sVMA incidence rates.15
Given the existing uncertainties of results from the systematic literature review, we aimed to further validate our results with other data sources: As one validation step, we considered the number of MH patients predicted by the literature with an incidence rate for MHs of 8.8 patients per 100,000 adult inhabitants (Table 1), suggesting ~7,200 new MH patients for Germany per year. This is in good accordance with 2016 German vitrectomy statistics, which suggest that 9,941 patients received surgery for MH or VMT – a figure that potentially also includes patients with other macular diseases, in particular, epiretinal membrane.
As another validation step, we considered a large vitreoretinal database study in the UK,4 which reported that 40.2% of PPVs with macular manipulation were for MH. For the 34,314 German PPV patients with macular manipulation, the pool of MH patients would be 13,795, which is also in good accordance with the OPS/ICD filtered data figure of 15,878 patients. The same UK database study found that 14.2% of PPVs with macular manipulation were for VMT, suggesting that for Germany, 2,255 of the 15,878 vitrectomy patients with macular manipulation had VMT. These results are also concordant.
Weaknesses of this study include a reliance on certain assumptions. First, the AAO classification system describes stage 3 MHs (which we excluded) as those ≥400 μm in diameter with vitreomacular separation, but it is possible that some MHs >400 μm still had persisting VMA. Also, clinicians may have applied the classification systems variably, as more than one has evolved over time.1,3,16 Further, the measurement of MHs and their classification may be subject to significant interobserver variability. The clinical statistic reflects in-patient settings with vitrectomy only, while intravitreal gas or air injections are documented by several case series as the possible out-patient therapy for sVMA.17–20
Conclusion
While our estimated incidence of VMT (with and without MH) in Germany relies on a number of untested assumptions, it, nonetheless, shows that sVMA is an important disease affecting a large number of individuals, many of whom may be undiagnosed or exist outside of the clinic system.
Disclosure
AN: consultant for Alimera, Santen, OD-OS, Contracare, Santhera, Thrombogenics/Oxurion. TJ: former consultant to Thrombogenics and Advisor to Alcon; the employer receives site payments for participants enrolled into clinical trials sponsored by Alcon. The authors report no other conflicts of interest in this work.
References
American Academy of Ophthalmology (AAO). Preferred practice pattern® guidelines. Idiopathic macular hole; 2017. Available from: https://www.aao.org/preferred-practice-pattern/idiopathic-macular-hole-ppp-updated-2017. Accessed May 3, 2018. | ||
Duker JS, Kaiser PK, Binder S, et al. The international vitreomacular traction study group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120(12):2611–2619. | ||
Steel DH, Lotery AJ. Idiopathic vitreomacular traction and macular hole: a comprehensive review of pathophysiology, diagnosis, and treatment. Eye (Lond). 2013;27(Suppl 1):S1–S21. | ||
Jackson TL, Donachie PH, Sparrow JM, Johnston RL. United Kingdom National ophthalmology database study of vitreoretinal surgery: report 1; case mix, complications, and cataract. Eye (Lond). 2013;27(5):644–651. | ||
Steel DH, Downey L, Greiner K, et al. The design and validation of an optical coherence tomography-based classification system for focal vitreomacular traction. Eye (Lond). 2016;30(2):314–324; quiz 325. | ||
Institut für das Entgeldsystem im Krankenhaus (InEK) [webpage on the Internet]. G-DRG-browser 2016_2017; 2016. Available from: https://www.g-drg.de/Datenbrowser_und_Begleitforschung/Datenveroeffentlichung_gem._21_KHEntgG/G-DRG-Browser_2016_2017. Accessed May 11, 2018. | ||
Orphanet Report Series. Prevalence and incidence of rare diseases: bibliographic data; 2016. Available from: https://www.orpha.net/orphacom/cahiers/docs/GB/Prevalence_of_rare_diseases_by_alphabetical_list.pdf. Accessed May 3, 2018. | ||
Deutsches Institut für Medizinische Information und Dokumentation (DIMDI) [webpage on the Internet]. Operationen- und Prozedurenschlüssel – Version 2018; 2018. Available from: https://www.dimdi.de/static/de/klassi/ops/kodesuche/onlinefassungen/opshtml2018/index.htm. Accessed May 11, 2018. | ||
Sen P, Bhargava A, Vijaya L, George R. Prevalence of idiopathic macular hole in adult rural and urban South Indian population. Clin Exp Ophthalmol. 2008;36(3):257–260. | ||
la Cour M, Friis J. Macular holes: classification, epidemiology, natural history and treatment. Acta Ophthalmol Scand. 2002;80(6):579–587. | ||
Wang S, Xu L, Jonas JB. Prevalence of full-thickness macular holes in urban and rural adult Chinese: the Beijing Eye Study. Am J Ophthalmol. 2006;141(3):589–591. | ||
Jacob J, Stalmans P. Prevalence of vitreoretinal interface abnormalities as detected by spectral-domain optical coherence tomography. Ophthalmologica. 2016;236(2):81–87. | ||
Meuer SM, Myers CE, Klein BE, et al. The epidemiology of vitreoretinal interface abnormalities as detected by spectral-domain optical coherence tomography: the Beaver Dam eye study. Ophthalmology. 2015;122(4):787–795. | ||
Rodman JA, Shechtman D, Sutton BM, Pizzimenti JJ, Bittner AK. Prevalence of vitreomacular adhesion in patients without maculopathy older than 40 years. Retina. 2018;38(10):2056–2063. | ||
Dimopoulos S, Bartz-Schmidt KU, Gelisken F, Januschowski K, Ziemssen F. Rate and timing of spontaneous resolution in a vitreomacular traction group: should the role of watchful waiting be re-evaluated as an alternative to ocriplasmin therapy? Br J Ophthalmol. 2015;99(3):350–353. | ||
Gass JD. Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol. 1995;119(6):752–759. | ||
Chan CK, Crosson JN, Mein CE, Daher N. Pneumatic vitreolysis for relief of vitreomacular traction. Retina. 2017;37(10):1820–1831. | ||
Chan CK, Wessels IF, Friedrichsen EJ. Treatment of idiopathic macular holes by induced posterior vitreous detachment. Ophthalmology. 1995;102(5):757–767. | ||
Day S, Martinez JA, Nixon PA, et al. Intravitreal sulfur hexafluoride injection for the treatment of vitreomacular traction syndrome. Retina. 2016;36(4):733–737. | ||
Steinle NC, Dhoot DS, Quezada Ruiz C, et al. Treatment of vitreomacular traction with intravitreal perfluoropropane (c3f8) injection. Retina. 2017;37(4):643–650. | ||
Liesenborghs I, De Clerck EEB, Berendschot TTJM, et al. Prevalence of optical coherence tomography detected vitreomacular interface disorders: the Maastricht Study. Acta Ophthalmol. 2018;96(7):729–736. | ||
McKibbin M, Farragher T, Shickle D. Vitreoretinal interface abnormalities in middle-aged adults with visual impairment in the UK Biobank study: prevalence, impact on visual acuity and associations. BMJ Open Ophthalmol. 2017;1(1):e000057. | ||
Zapata MA, Figueroa MS, Esteban González E, et al. Prevalence of vitreoretinal interface abnormalities on spectral-domain OCT in healthy participants over 45 years of age. Ophthalmol Retina. 2017;1(3):249–254. | ||
Darian-Smith E, Howie AR, Allen PL, Vote BJ. Tasmanian macular hole study: whole population-based incidence of full thickness macular hole. Clin Exp Ophthalmol. 2016;44(9):812–816. | ||
McCannel CA, Ensminger JL, Diehl NN, Hodge DN. Population-based incidence of macular holes. Ophthalmology. 2009;116(7):1366–1369. | ||
Simpson ARH, Jackson TL. The epidemiology of vitreo-macular interface diseases. In: Girach A, de Smet M, editors. Diseases of the Vitreo-Macular Interface. Essentials in Ophthalmology. Berlin, Heidelberg: Springer; 2014. | ||
Beutel J, Dahmen G, Ziegler A, Hoerauf H. Internal limiting membrane peeling with indocyanine green or trypan blue in macular hole surgery: a randomized trial. Arch Ophthalmol. 2007;125(3):326–332. | ||
Bopp S, Lucke K, Hille U. Peripheral visual field loss after vitreous surgery for macular holes. Graefes Arch Clin Exp Ophthalmol. 1997;235(6):362–371. | ||
Brockmann T, Steger C, Westermann M, et al. Ultrastructure of the membrana limitans interna after dye-assisted membrane peeling. Ophthalmologica. 2011;226(4):228–233. | ||
Brockmann T, Steger C, Weger M, Wedrich A, Haas A. Risk assessment of idiopathic macular holes undergoing vitrectomy with dye-assisted internal limiting membrane peeling. Retina. 2013;33(6):1132–1136. | ||
Eckardt C, Eckert T, Eckardt U, Porkert U, Gesser C. Macular hole surgery with air tamponade and optical coherence tomography-based duration of face-down positioning. Retina. 2008;28(8):1087–1096. | ||
Eckardt U, Eckardt C. [Binocular vision in cases of idiopathic macular hole: pre- and postoperative findings]. Ophthalmologe. 1995;92(5):626–630. German. | ||
Engelmann K, Sievert U, Hölig K, et al. [Effect of autologous platelet concentrates on the anatomical and functional outcome of late stage macular hole surgery: a retrospective analysis]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2015;58(11–12):1289–1298. German. | ||
Faude F, Edel E, Dannhauer M, Petzel C, Meier P, Wiedemann P. [Autologous thrombocyte administration in treatment of idiopathic macular foramen]. Ophthalmologe. 1997;94(12):877–881. German. | ||
Gass CA, Haritoglou C, Schaumberger M, Kampik A. Functional outcome of macular hole surgery with and without indocyanine green-assisted peeling of the internal limiting membrane. Graefes Arch Clin Exp Ophthalmol. 2003;241(9):716–720. | ||
Gehring S, Hoerauf H, Laqua H, Kirchner H, Klüter H. Preparation of autologous platelets for the ophthalmologic treatment of macular holes. Transfusion. 1999;39(2):144–148. | ||
Göbel W, Schrader WF, Schrenker M, Klink T. [Findings of optical coherence tomography (OPT) before and after macular hole surgery]. Ophthalmologe. 2000;97(4):251–256. German. | ||
Göbel W, Guthoff R. [Morphology of macular holes after pars plana vitrectomy with silicone oil endotamponade: a pilot study with high resolution Fourier domain OCT (Cirrus OCT)]. Ophthalmologe. 2010;107(5):452–459. German. | ||
Hager A, Ehrich S, Wiegand W. [Anatomical and functional results after elective macular surgery]. Ophthalmologe. 2005;102(6):597–602. German. | ||
Haritoglou C, Gass CA, Schaumberger M, Ehrt O, Gandorfer A, Kampik A. Macular changes after peeling of the internal limiting membrane in macular hole surgery. Am J Ophthalmol. 2001;132(3):363–368. | ||
Haritoglou C, Schumann R, Reiniger I, et al. Evaluation of the internal limiting membrane after conventional peeling during macular hole surgery. Retina. 2006;26(1):21–24. | ||
Hillenkamp J, Kraus J, Framme C, et al. Retreatment of full-thickness macular hole: predictive value of optical coherence tomography. Br J Ophthalmol. 2007;91(11):1445–1449. | ||
Hoerauf H, Klüter H, Joachimmeyer E, et al. Results of vitrectomy and the no-touch-technique using autologous adjuvants in macular hole treatment. Int Ophthalmol. 2001;24(3):151–159. | ||
Jenisch TM, Zeman F, Koller M, Märker DA, Helbig H, Herrmann WA. Macular hole surgery: an analysis of risk factors for the anatomical and functional outcomes with a special emphasis on the experience of the surgeon. Clin Ophthalmol. 2017;11:1127–1134. | ||
Jordan F, Jentsch S, Augsten R, Strobel J, Dawczynski J. [Study on the time course of macular pigment density measurement in patients with a macular hole – clinical course and impact of surgery]. Klin Monbl Augenheilkd. 2012;229(11):1124–1129. German. | ||
Krömer I, Lommatzsch A, Pauleikhoff D. [Retinal ICG-accumulation after ILM-staining during macular hole surgery?] Ophthalmologe. 2004;101(6):604–607. German. | ||
Kristin N, Ehrt O, Gass CA, Haritoglou C, Kampik A. [Preoperative scanning laser ophthalmoscope: findings in idiopathic macular foramen]. Ophthalmologe. 2001;98(11):1060–1064. German. | ||
Kube T, Hermel M, Dahlke C, Hutschenreuter G, Schrage N, Kirchhof B. [Macular hole surgery: experience with autologous platelet concentrate and indocyanine green-assisted internal limiting membrane peeling]. Klin Monbl Augenheilkd. 2002;219(12):883–888. German. | ||
Mayer WJ, Reznicek L, Neubauer AS, Wolf A, Kampik A, Haritoglou C. [Functional and morphological correlations in macular hole surgery]. Klin Monbl Augenheilkd. 2014;231(1):54–60. German. | ||
Meyer CH, Schmidt JC, Mennel S, et al. [Anatomical and functional results after macular hole surgery]. Klin Monbl Augenheilkd. 2008;225(3):220–226. German. | ||
Rüfer F, Frimpong-Boateng A, Bunse A, Roider J. [Comparison of ILM peeling with and without the use of indocyanine green. Functional results for idiopathic macular hole after pars plana vitrectomy]. Ophthalmologe. 2007;104(1):54–59. German. | ||
Remy M, Thaler S, Schumann RG, et al. An in vivo evaluation of brilliant blue G in animals and humans. Br J Ophthalmol. 2008;92(8):1142–1147. | ||
Schrader WF, Schrenker M. Can the functional outcome in macular hole surgery be improved by internal limiting membrane maculorhexis? Klin Oczna. 1999;101(3):169–173. | ||
Schumann RG, Schaumberger MM, Rohleder M, Haritoglou C, Kampik A, Gandorfer A. [The primary objective in macular hole surgery. Ultrastructural features of the vitreomacular interface]. Ophthalmologe. 2007;104(9):783–789. German. | ||
Wirbelauer C, Häberle H, Pham DT. [Clinical experience with brilliant blue G staining of the retinal surface]. Klin Monbl Augenheilkd. 2011;228(1):62–65. German | ||
Wirbelauer C, Kolarov D, Just A. [Influence of macular hole width on visual acuity, endotamponade and closure rate]. Klin Monbl Augenheilkd. 2016;233(12):1362–1366. German. | ||
Wolf S, Reichel MB, Wiedemann P, Schnurrbusch UEK. Clinical findings in macular hole surgery with indocyanine green-assisted peeling of the internal limiting membrane. Graefes Arch Clin Exp Ophthalmol. 2003;241(7):589–592. |
Supplementary materials
 | Table S1 International epidemiology search |
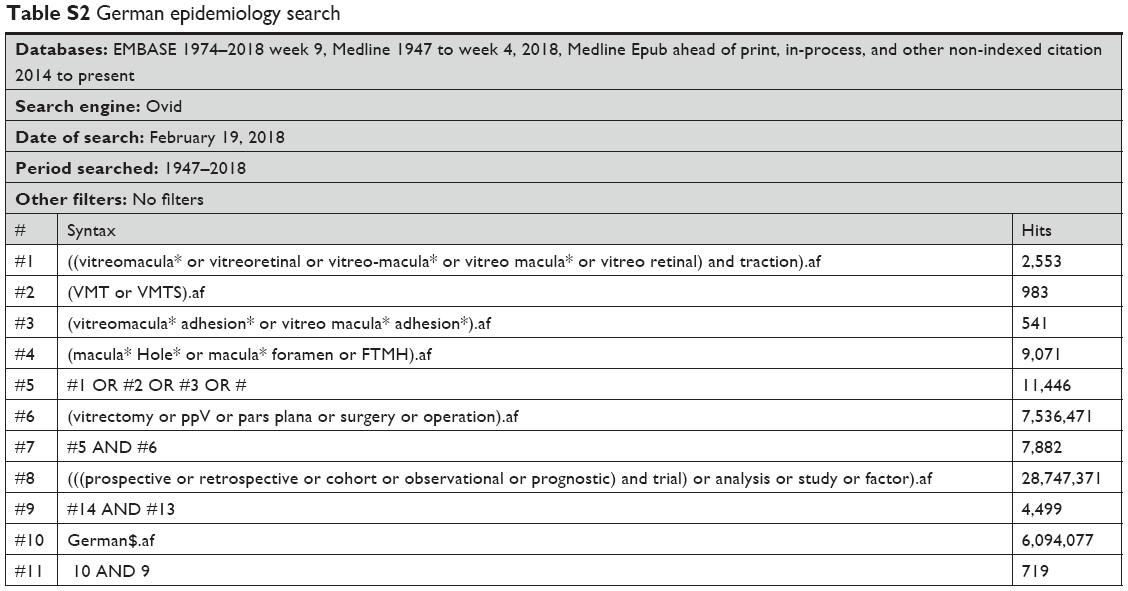 | Table S2 German epidemiology search |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.