")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Incidence and Predictors of Loss to Follow-Up Among Children Attending ART Clinics in Northeast Ethiopia: A Retrospective Cohort Study
Authors Menshw T, Birhanu S, Gebremaryam T , Yismaw W , Endalamaw A
Received 15 June 2021
Accepted for publication 1 August 2021
Published 11 August 2021 Volume 2021:13 Pages 801—812
DOI https://doi.org/10.2147/HIV.S320601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Tiruye Menshw Snr,1 Shiferaw Birhanu,2 Tigist Gebremaryam,3 Worke Yismaw,1 Aklilu Endalamaw2,4
1Nursing Department, Mettu University, Mettu, Ethiopia; 2Department of Pediatrics and Child Health Nursing, Bahir Dar University, Bahir Dar, Ethiopia; 3Department of Pediatrics and Child Health Nursing, Debre Markos University, Debre Markos, Ethiopia; 4Schools of Public Health, The University of Queensland, Brisbane, Australia
Correspondence: Tiruye Menshw Snr Email [email protected]
Background: It is known that antiretroviral therapy reduces the transmission of human immunodeficiency virus and AIDS-related morbidity. The coverage of HIV drugs is increasing to control further spread of HIV and children living with HIV are the target groups in using these medications. However, loss to follow-up remains a critical challenge among these groups of the population. The aim of this study was therefore to assess the incidence and predictors of loss to follow-up among children attending antiretroviral therapy clinics.
Methods: A ten-year institution-based retrospective cohort study was employed among 448 children enrolled in antiretroviral therapy. Data were entered and cleaned using EpiData version 3.1 and then exported to STATA version 14 for further statistical analysis. The Kaplan–Meier survival curve was used to estimate the survival time and the Log rank test was used to compare the survival time between different categories of the explanatory variables. Multivariable Cox proportional hazards model was fitted to identify predictors of loss to follow-up and p-value < 0.05 was considered statistically significant.
Results: The incidence rate of loss to follow-up was 6.3 per 100 children years of observation. Being male (AHR = 2.1, CI = 1.37, 3.34), aged 1– 5 years (AHR = 1.6, CI = 1.05, 2.46), poor adherence to antiretroviral therapy (AHR = 6.6; CI = 4.11, 10.66), fair adherence to antiretroviral therapy (AHR = 2.2; CI = 1.13, 4.20), regimen was not changed (AHR = 4.1; CI = 2.59, 6.45), World Health Organization stage III and IV (AHR = 2.2; CI = 1.40, 3.33) and height for age <− 2 z score (AHR = 2.2; CI = 1.43, 3.44) were predictors of loss to follow-up.
Conclusion: Nearly seven out of 100 HIV-infected children were lost to follow-up from their link to ART clinics within a one-year follow-up. Non-modifiable demographic characteristics, clinical stage and nutritional status, and ART-related variables were associated with children’s loss to follow-up. Therefore, close monitoring of the “at risk” groups might decrease the rate of loss to follow-up. Improving adherence to antiretroviral therapy and nutritional support are also recommended.
Keywords: incidence, predictors, loss to follow up, Ethiopia
Background
Since the beginning of the epidemic, 74.9 million people have been infected with HIV and 32 million people have died worldwide due to AIDS-related diseases.1 Globally, 37.9 million people were living with HIV by the end of 2018, and 1.7 million were children among HIV cases in the same year.2 More than 1500 children become infected with HIV every day. The vast majority (more than 90%) acquire the infection from their mother, so mother to child transmission is the highest contributing factor to pediatric HIV infections.2,3 Though the burden of the HIV epidemic is varied across countries and regions, an estimated 0.8% of adult populations are living with HIV worldwide which accounts for the significant number of HIV-infected children being adults after few years.3
Sub-Saharan Africa is a region most affected by HIV.4 Ethiopia is one of the Sub-Saharan African countries where it is challenging to decrease HIV across its administrative areas.5 Ethiopian demographic and health survey report showed there is a variation of HIV prevalence among the different settings. Notably, frequently reported in the western part (4.8%) and the capital city, Addis Ababa (3.4%), and lower prevalence existed in the southern (0.4%) and eastern parts (< 0.1%) of the country.6 According to the Ethiopian public health institution report, 45,824 were children among all 691,362 HIV cases by the end of 2019.7
The health sector has prepared to respond to HIV, as one of the targets to halt HIV epidemic by 2030.8 Also, Ethiopia is implementing several strategies to end the HIV epidemic by 2030. These are, by the end of 2020: plan to reduce 70% of new infections and 80% of HIV-related deaths, to enroll 85% of children with HIV in ART, and to achieve the three 95s’ targets; 95% of all people knowing their HIV status, 95% of HIV positive people having access to treatment, and 95% of all people receiving ART will have viral suppression.5,9–11 To achieve this goal, HIV infected patients should be put on HIV medications and loss to follow up (LTFU) after linked to the ART clinic should be prevented by fostering the health care system. Antiretroviral therapy (ART) is essential for children to have a long life by reducing viral load and disease progression.12 Without accessing ART and regular medical supervision, HIV-infected children are more vulnerable to complicated clinical outcomes, including death.13–15
The literature shows that high attrition within PMTCT programs could be due to LTFU rather than mortality. This shows non-retention of mothers in PMTCT programs is another contributor to the loss to follow-up of children within ART care. The quality and effectiveness of PMTCT services should be assessed on the basis of the number of mother-child pairs who are receiving consistent follow-up and antiretroviral treatment, and the number of confirmed HIV-1-negative children born to HIV-1-positive women.16
Loss to follow-up (LTFU) is a critical barrier to HIV care and treatment.17 A significant number of children drop out from the treatment cascade.18 Globally, 14% and 28% of children were LTFU from the treatment cascade at one and two years after starting ART, respectively.13 Similarly, in Sub-Saharan Africa, 20–40% of children with HIV were LTFU.19,20 Children on ART who become LTFU are more at risk of developing drug-resistant viruses than those who remain on ART as a result. Due to this, children’s quality of life might be impaired and their survival time might also be shorter.21,22
Several studies revealed that there was a significant number of children LTFU from their ART clinic. Studies in Asia and Africa showed that 69% of LTFU occurred in the first 3 and 6 months of ART.23 In South Africa, 8.4 per 100 children years of observation and 5 per 100 children per year were LTFU in the first and second years, respectively24 and, in Ethiopia, 6.26 per 100 children per year was documented.25 LTFU could be affected by the complex interplay of self-care, community factors, care delivery, and the drug itself.26 According to data from children at baseline, the variables associated with LTFU from the previous studies were: younger age, lower CD4 cell count during ART initiation, WHO stage III/IV, weight for age ≤ 2, short duration on ART, hemoglobin level <8g/dl, living with non-educated caregiver, and disclosure of HIV status.27–32
To decrease the loss of children from the ART program, several African regions, including Ethiopia, have applied different mechanisms. Offering free ART, decentralization of services, creating awareness using religious or community leaders and other stakeholders, counseling, and phone calls or mobile short message left for a caregiver were applied to retain children in the ART program.33,34
LTFU is a critical barrier complicating clinical outcome in HIV treatment program and identifying whether modifiable or non-modifiable factors were associated with LTFU is fundamental for designing effective patient retention strategy.35 There is limited evidence regarding the predictors of loss to follow-up among children attending ART clinics in Ethiopia. Therefore, we assessed the incidence and predictors of LTFU among children attending ART clinics in the Northeastern parts of Ethiopia.
Methods
Study Setting
The sample was from the Dessie referral hospital, which is a government hospital found in northeast Ethiopia that serves a catchment population of seven million. The hospital is in Dessie town, which is 401 km from the capital city of Addis Ababa. The hospital has been providing ART services for people living with HIV since 1995 Ethiopian calendar, and the ART case team comprises a variety of trained health professionals (four physicians, twelve nurses, three pharmacists, four laboratory technicians, four data clerks, and two ART education adherence counselors). About 1600 ART users were recorded in the last ten years and most of them come to the hospital according to their appointments with their parents. The service given in the ART clinic includes; ART provision, management of cases including: OIs, side effects, nutritional support, counseling and health education. The patients do not pay when they come for ART services because the service is supported by government and NGOs.
Study Design and Period
An institution-based retrospective cohort study was done from February 1 to 27/2020 which included patient charts from January 2010 to January 2020.
Sample Size Determination and Sampling Procedures
For the first objective, a single population formula was used to calculate the sample size by considering the following statistical assumption: P= cumulative incidence of LTFU among children on ART 8.63% study done in Ethiopia.36 Z α/2 = the corresponding Z score of 95% CI, d= margin of error (5%) and in= sample size n= (Z α/2)2*p (1-p) /d2 n= (1.96)2*0. 863(1–0.863)/ (0.05)2= 182. For the second objective, the sample size was determined using Epi info version 7.2 by considering the following predicates: underweight, hemoglobin level and taking cotrimoxazole in a study conducted in Ethiopia.39 With 95% CI, 80% power and ratio of exposed to unexposed 1:1, the highest sample size was 488, so we considered it as a final sample. The medical registration numbers of under-15 year old children who started ART were collected from the database. Then, the computer-generated method was used to select random medical registration numbers.
Data Collection Instrument and Procedure
The data extraction tool was developed from the standardized ART entry and follow-up form of the Ethiopia ministry of health and used by the ART clinic during data collection, which consists of Part-I; social, demographic characteristics of the child and caregiver, part-II; baseline clinical, laboratory and ART related information, part-III; ART treatment and other medication related information and part-IV; patient follow-up information (completed from ART follow-up form) recent results.
First, the patient record was observed and an appropriate data extraction format was prepared in the English version. Data collectors were used and the data collection tool to collect the information from children’s charts. Charts were retrieved using the children’s registration number, which was found in the database in the electronic system, charts with incomplete intake forms were excluded from the study and one data clerk supported by identifying registration number of the charts. Necessary data were extracted by reviewing children’s ART cards. Loss to follow-up was confirmed by reviewing medical registration in the hospital or registration by ART adherence supporters. The data were collected by four experienced personnel with Bachelor of Science degree in nursing who had been trained in comprehensive HIV care and were involved in the HIV care clinic. Ten percent of the sample size charts were checked to ensure consistency of the data extraction tool before starting data collection. One person with Master of Science degree in nursing closely supervised the entire data collection process. One day training was given to both data collectors and supervisor. Data quality was also ensured through designing proper data collection tool and continuous supervision. Codes were given for checklists. All collected data were checked for completeness by data collectors and supervisor every day.
Variables
Socio-Demographic Characteristics
Socio-demographic characteristics included: age of children, sex of children, religion of care giver, relation of caregiver to child, place of delivery, residence, marital status of caregiver, occupation of caregiver, parent status, parent’s HIV status, age of parent/caregiver, and sex of care giver. Clinical and laboratory predictors: WHO stage, CD4 count, hemoglobin level, functional status (for >5 years), developmental status (<5 years) and opportunistic infection, drug side effects, and adherence to ART.
ART and Other Medication Predictors
Prophylaxis (CPTand INH), duration of ART treatment, ART regimen and time to ART initiation). Nutritional predictors: undernourished (wasting, stunting, underweight and thinness).
Operational Definition
Loss to follow-up: child on ART who has not visited the clinic in the past 30 days and more, and not documented as died or transferred out to another ART clinic considered LTFU.37
Transferred out: those who were transferred to other health care facilities.
Event: LTFU of children on ART.
Censored: when children on ART died, were transferred out to other health institution, or continued to attend an ART clinic even after the end of the study.
Duration of ART: the time between ART’s start date and date of the last contact with the health facility during data collection.
Adherence: means taking the right ARV medication, at the right dose, at the right time every day and exactly as prescribed for the rest of your life. Described as good if adherence was ≥95% (1 dose of 30 doses or 2 doses of 60 doses missed), fair if adherence was between 85 to 94% (2 to 4 doses of 30 doses or 4 to 189 doses of 60 doses missed) and poor if adherence was <85% (≥5 doses of 30 doses or ≥10 doses of 60 doses missed).35
Data Analysis
The data were checked for completeness, consistency and then, coded and entered using Epi data version 3.1. Afterward, it was cleaned and analyzed using STATA version 14. Descriptive statistics were computed to determine the frequencies and summary statistics. Anthroplus software was used to generate Z scores to categorize nutritional status by considering weight-for-age, height-for-age, weight-for-height, and body mass index for age. The Kaplan–Meier survival curve was used to estimate survival time after initiation of ART, and the Log rank test was used to compare survival curves of different categorical explanatory variables. The Cox proportional hazard model was used to assess predictors of LTFU. To see the effect of predictors on the time of LTFU, a Bivariate Cox-proportional hazard regression model was fitted for each explanatory variable. Those variables with p-value ≤ 0.25 in the bivariate analysis were fitted to the multivariate Cox-proportional hazard regression model. Cox proportional hazard model assumption was checked using scaled Schoenfeld residual test and graphically with log-log Cox adjusted survival estimate. The model fitness was checked using Cox–snell residuals test. Variables with P-value < 0.05 were considered statistically associated with LTFU.
Ethical Consideration
Ethical approval for the research paper was obtained from the ethical review committee of Bahir Dar University College of medicine and health science and then, a formal letter was written by the department of pediatrics and child health nursing in Dessie referral hospital. After that the letter was taken to Dessie referral hospital’s director and the respective head. And the study was conducted in accordance with the Declaration of Helsinki. During the data collection time, the objective of the study was clearly explained to data collectors and supervisor and the names of children were not written.
Results
Sociodemographic Characteristics of Children on ART
Among 488 children who participated in the study, 52.9% were male. The majority (76%) were of urban residency, and 85.2% were living with their parents. The median age with interquartile range (IQR) of children at the beginning of the follow-up was 8 years (IQR= 6.4) (Table 1).
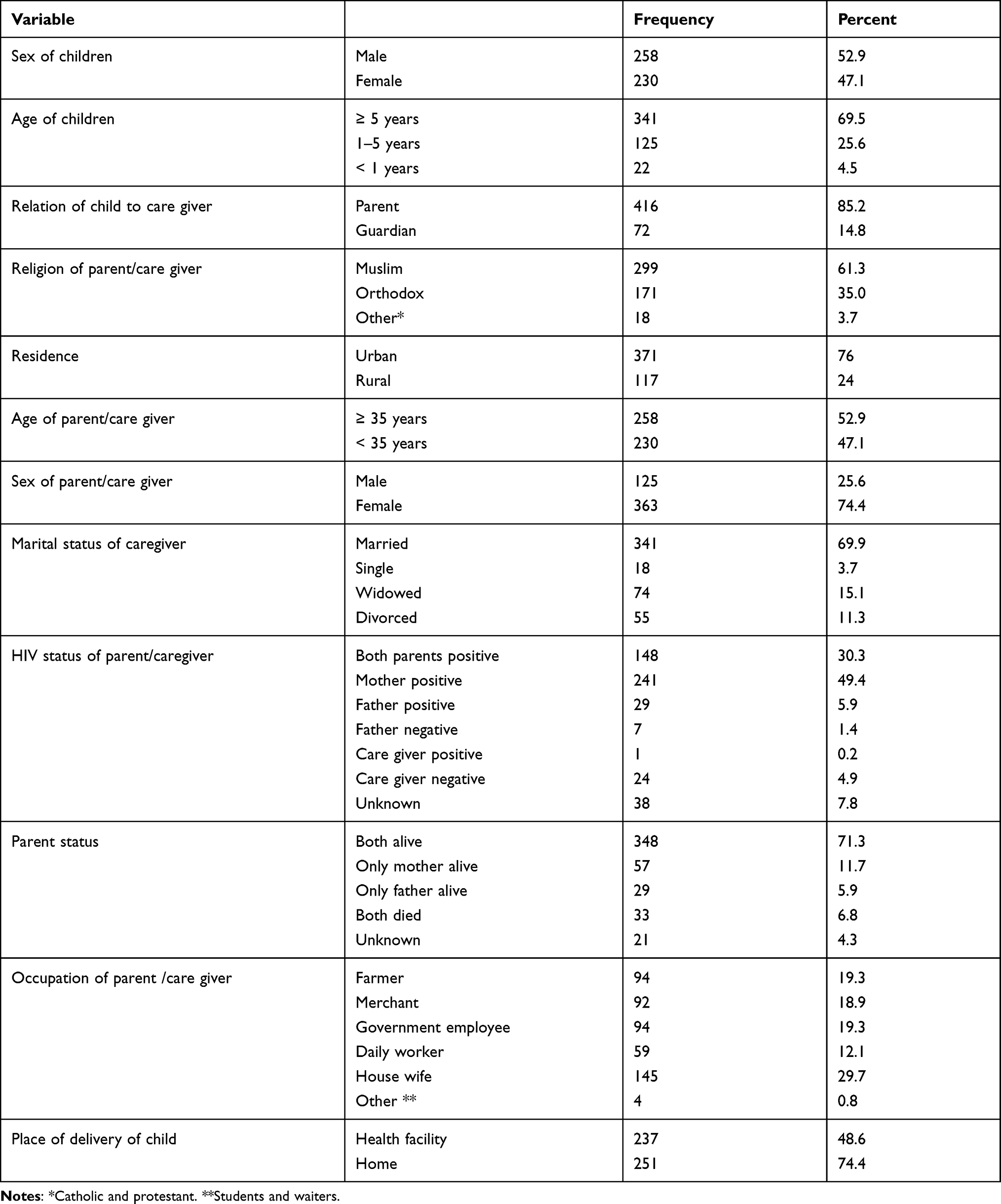 |
Table 1 Baseline Sociodemographic Characteristics of Children on ART in Northeast Ethiopia, 2020 |
Baseline Clinical, Laboratory, and ART Information of Children on ART
During ART initiation, 73.2% of children had opportunistic infections. Nearly half (48.2%) of children were eligible for ART treatment based on the low level of CD4 count (Table 2).
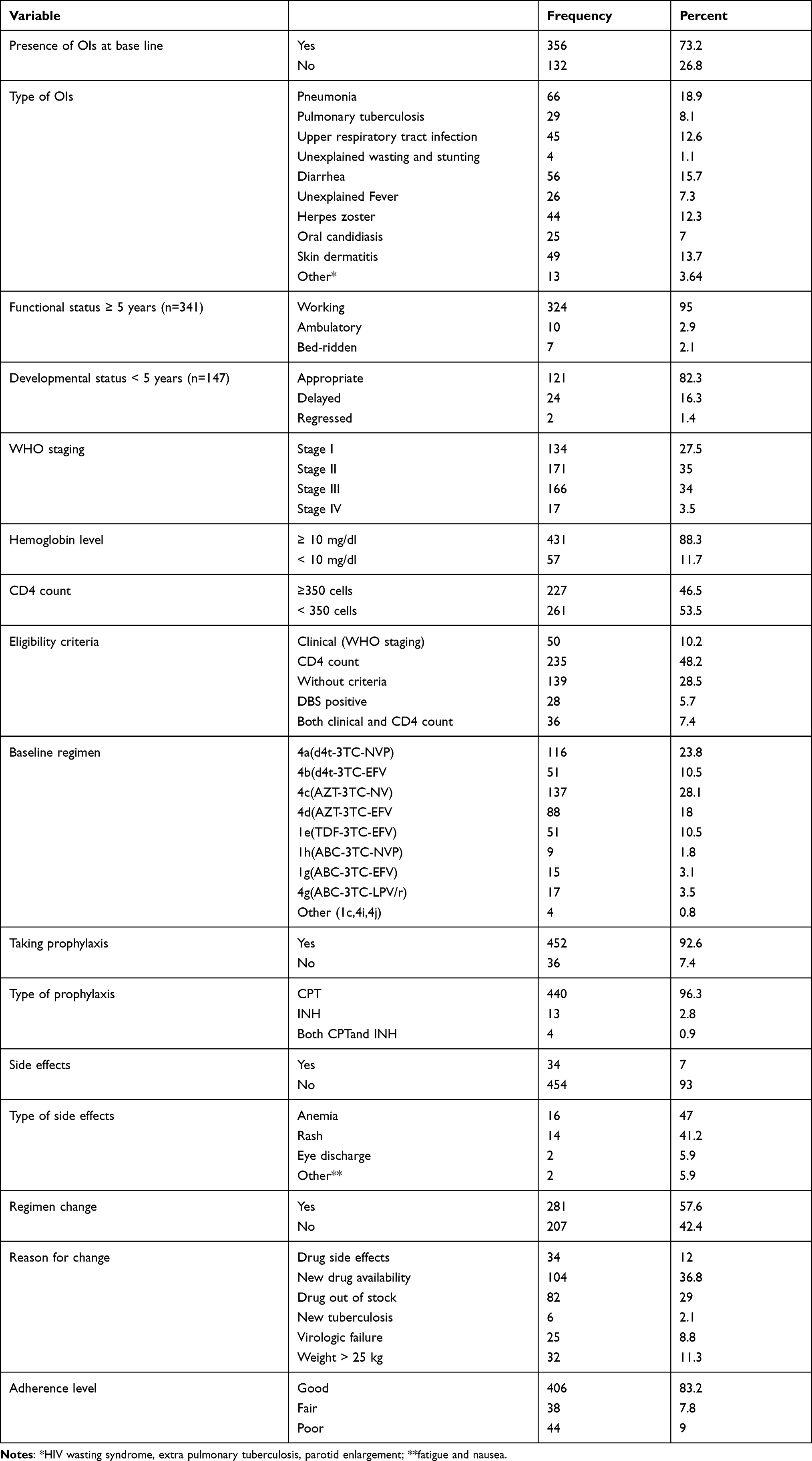 |
Table 2 Baseline Clinical, Laboratory, and ART Information of Children on ART in Northeast Ethiopia, 2020 |
Nutritional Information of Children on ART
From the study participants, 17.2% were stunted (Table 3).
Incidence of Loss to Follow-Up After ART Initiation
Of the 488 children on ART, 61.68% were continuing attending ART clinics at the end of the study; 15.37% were transferred out, and 2.25% died. Using cumulative incidence, 20.7% (95% CI=17.20, 23.80) were LTFU from ART clinic. The overall loss to follow-up incidence density rate (IDR) in the cohort was 6.3 (95% CI = 5.21, 7.77) per 100 children years of observation.
Predictors of Loss to Follow-Up
In the Bivariate analysis, the Cox proportional hazard model showed sex of a child, age of children between 1–5 years, residence, taking prophylaxis, change of regimen, CD4 count, WHO stage, hemoglobin level, adherence level, and height-for-age were statistically significant predictors of loss to follow-up. In the multivariable analysis, sex of a child, age of children between 1–5 years, WHO stage, adherence to ART, height-for-age and regimen change were predictors of loss to follow-up.
Children aged between 1–5 years had an increased hazard of LTFU of 1.6 times (95% CI =1.05, 2.46) compared to those aged ≥ 5 years. Male children were 2.1 (95% CI= 1.37, 3.34) times more prone to be LTFU than females. The hazard of LTFU in children who had WHO stage III and IV was 2.2 (95% CI=1.40, 3.33) times higher than those who had WHO stage I and II. Having poor adherence to ART had 6.6 (95% CI =4.11, 10.66) times increase in hazard to be LTFU among children as compared to good adherence to ART, and also children who had fair adherence to ART were 2.2 (95% CI=1.14,4.20) times more at risk of LTFU compared to those who had good adherence. The hazard of LTFU in children whose nutritional status was stunted (HFA<-2Zscore) was 2.2 (95% CI=1.43, 3.44) times higher than their counterparts. Children whose regimen had not been changed were 4.1 (95% CI = 2.59, 6.45) times more at risk of LTFU as compared to those whose regimen had been changed (Table 4).
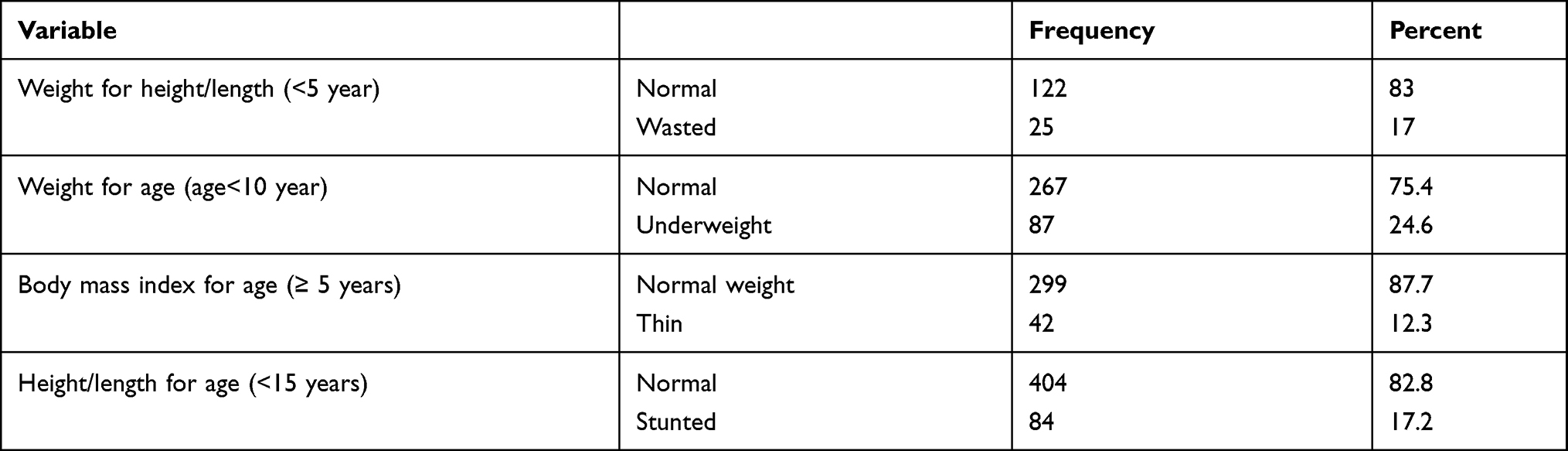 |
Table 3 Nutritional Information of Children on ART in Northeast Ethiopia, 2020 |
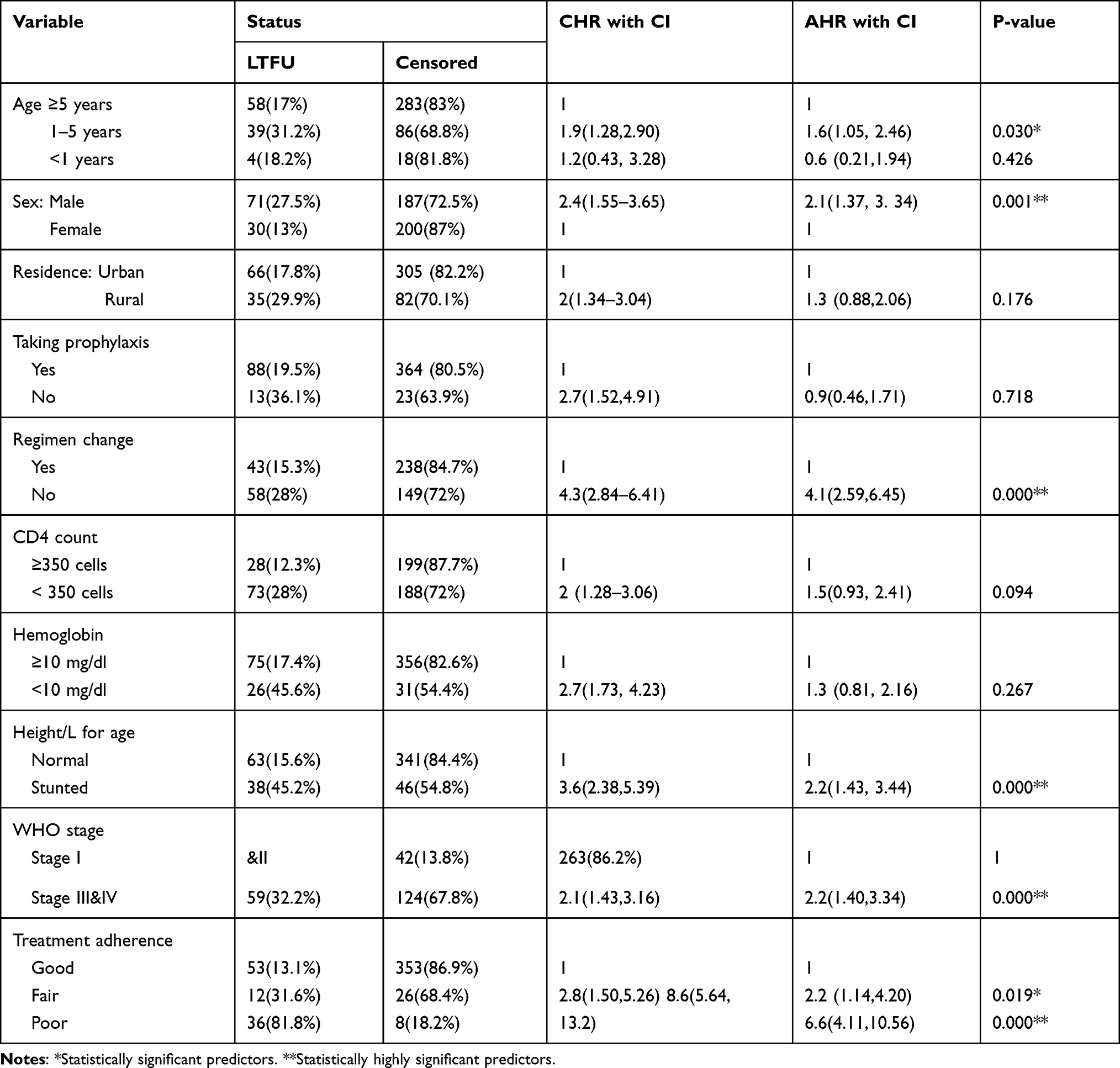 |
Table 4 Cox Regression Analysis for Predictors of Loss to Follow-Up Among Children on ART in Northeast Ethiopia, 2020 |
Discussion
The incidence rate of this study was 6.3 per 100 children years of observation (CI=5.21, 7.77). Upon running the final Cox proportional hazard model, statistically significant predictors for LTFU were male sex, WHO stage III and IV, age between 1–5 years, stunting, poor and fair adherence to ART, and regimen not changed.
The overall incidence rate of this study is in line with the study conducted in Addis Ababa, Ethiopia: 6.26 per 100 children years of observation.25 On the other side, the result of this study is lower than the studies conducted in Tanzania which showed the incidence rate of LTFU was 18.2 per 100 children years of observation, Uganda 12.6 per 100 children years of observation, and in South Africa, 10.8 per 100 children years of observation.29,35,38 This difference might be due to socioeconomic and cultural difference, difference in study time because the government may devise different intervention strategies to alleviate the problem and health care policy. Besides, in Tanzania, the study included both pre-ART initiation and post-ART initiation children and in Uganda, a high presence of orphaned children was found in the study.
On the contrary, the result of this study is higher than studies conducted in Thailand: 2.92 per 100 children years of observation, and India: 4.4 per 100 children years of observation. This difference might be due to sociocultural, economic differences, differences in emphasis given by the government nationally, study setting and access to the service.39,40 The other possible explanation is the presence of more ART service decentralization in India. Additionally, in Thailand there is a difference in study participants, they included children who attended at least 12 months of ART clinic, and study period difference. Plus this, the result of this study is higher than studies conducted in Zimbabwe, 4.92 per 100 children years of observation, and 3.29 per 100 children years of observation in Kenya.13,36,41 This might be due to variation in the implementation of retention in care strategy and also follow-up period difference.
In this study, LTFU before 18 months (with an incidence rate of 6.6 per 100 children years of observation) was higher than LTFU after 18 months of ART initiation (6.1 per 100 children years of observation). This is due to the fact that, at the initial time, they are at risk for immune reconstitution inflammatory syndrome and drug side effects that increase the risk of death.
The incidence rate of loss to follow-up at the first year (6.9 per 100 children years of observation) was higher as compared to the second year (5.9 per 100 children years of observation). This is in line with the study conducted in South Africa.24 This is might be due to health care workers who give repeated counseling for caregivers about the benefit of ART treatment and the consequence of discontinuing. The other possible explanation might be that the government gives attention and creates awareness in the community about the benefit of treatment and decentralization of ART services.
The cumulative incidence of this study was 20.7% (CI=17.20, 23.80). This is in line with the studies conducted in West Africa, 21.8%, Nigeria, 19%, and Ethiopia, 17.9%.21,28,42 However, this result is higher than studies conducted in Asia, 4.1%, Côte d’Ivoire, 9.3%, East Africa, 14%, South Africa, 9%, and Zambia, 16%.21,27 This might be due to economic and sociodemographic differences and variation in the implementation of a retention strategy, accessibility of the service, and weak monitoring and evaluation system of the service. For example, in Zambia, health care workers apply home-to-home visits. On the contrary, the finding of this study is lower than studies conducted in Mozambique, 38.7% and in Adama Ethiopia, 34%.43,44 This might be because in Mozambique, the study was conducted in 10 rural districts and there was a challenge of transportation and poor health care infrastructure. In Adama Ethiopia, the study included both pre-ART initiation and post-ART initiation.
In this study, the hazard of loss to follow up among children between 1–5 years old was 1.6 times higher than children greater or equal to five years old. This is supported by studies conducted in Thailand and Botswana.39,45 It may be because this age group was more at risk for malnutrition and opportunistic infections that increase disease progression rapidly, which indirectly increases loss to follow up.37 This result is inconsistent with a comparative analysis study conducted in Asia and South Africa.21,24
This study showed that being male had 2.1 times increased risk of loss to follow up compared to female. This is consistent with studies conducted in Kenya, South Africa, and Brazil.13,24,32 This is because most (59.4%) males initiate ART at advanced stage of disease. Having advanced clinical stage (WHO stage III and IV) at the time of ART initiation significantly increased the hazard of loss to follow up among children. This is supported by studies conducted in West Africa, Malawi, Uganda, Botswana, and Ethiopia.29,42,45–47 The possible explanation might be that children who initiate ART in the advanced stage have an increased risk of opportunistic infections that cause morbidity and mortality of unregistered deaths. Moreover, children in the advanced stage may develop drug side effects, especially within the first six months and further complicate disease progression.48 On the other hand, this result is inconsistent with studies conducted in South Africa and Kenya.34,37 The possible explanation might be that patients with stage I and II do not feel sick enough to accept restrictive medical care.49 Additionally, in South Africa, children with this stage were asymptomatic, and health care workers might not give as much attention as to those with advanced disease.34
Children whose nutritional status was stunted were more at risk to loss to follow up as compared to those whose nutritional status was normal. This is supported by studies conducted in other parts of African countries.27,31,43 This could be because stunted children may have had poor baseline health and poor ART compliance as compared to normal. HIV by itself affects nutritional status and malnourished children are more affected by HIV and increased disease progression.50,51 Furthermore, stunted children may have had a concomitant opportunistic infection that prevented them from going to the health facility for a refill of drugs and some may have died from such condition.52
Regarding adherence to ART, those with poor adherence had about seven times increased risk of loss to follow up compared to those with good adherence. Also, the risk of LTFU among children who had fair adherence to ART was 2.2 times higher than their counterparts. This is because of the fact that poor/fair adherence increases viral load duplication and decreases drug effectiveness, thus, further suppressing the immune system and increasing opportunistic infection and disease progression.53 The other possible explanation might be that poor medication adherence causes HIV viral resistance and subsequent treatment failure. Moreover, children depend on their caregiver to get their care and due to this, if the child had poor improvement, caregivers might be feeling hopelessness or carelessness and loss from treatment cascade.
Furthermore, children whose regimen was not changed were four times more at risk to loss to follow-up compared to those whose regimen was changed. This might be because most of the old regimens have side effects that cause advanced disease and complications. AZT containing regimen causes anemia that increases the disease progression rapidly.54
As to policy implications, Ethiopia has achieved a remarkable reduction in AIDS-related death in achieving 2020’s national target based on a study report from further analysis of global burden of diseases 2017 data.55 There are no well-organized tracing mechanisms to see the outcome of HIV infected children lost from HIV care clinics. Our study indicates the incidence of LTFU of children on ART. It does not, however, touch on what was happening to those children detached from healthcare follow-up sites.
Conclusion
The incidence rate of loss to follow was high. Age 1–5 years, World Health Organization clinical stage III and IV, poor and fair adherence to ART, regimen not changed, male sex and stunting were at higher risk for loss to follow up. Therefore, close monitoring of the higher risk groups for loss to follow up highlighted in this study could decrease the rate of loss to follow up. Improving the adherence of children to ART and nutritional support for stunted children are recommended.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; ART, Antiretroviral Therapy; HIV, Human Immunodeficiency Virus; LTFU, Lost to Follow UP; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgment
We would like to thank Bahir Dar University College of Medicine and Health sciences. We also thank Dessie referral hospital administration and ART clinic staff for their support.
Author Contributions
All authors contributed to proposal development, data collection, data analysis, drafting or revising the article, have agreed on the journal to which the article is to be submitted, reviewed and agreed on all versions of the article before submission, during revision and agree to take responsibility and be accountable for the contents of the article.
Funding
This research was funded by Bahir Dar University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNAIDS. Fact sheet – world AIDS day; 2019.
2. World Health Organization. Global Health Observatory (GHO) Data; 2019.
3. UNAIDS. Data; 2019.
4. UNAIDS. Miles to Go—Closing Gaps, Breaking Barriers, Righting Injustices; 2018.
5. Office FHAPaC. HIV Prevention in Ethiopia National Road Map 2018–2020; 2018.
6. International. CSACEaI. Ethiopia Demographic and Health Survey HIV Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA; 2016.
7. Institute Eph. HIV related estimate and projection for Ethiopia Addis Ababa; 2017. Available from: https://www.ephi.gov.et/images/pictures/download2009/HIVestimationandprojectionforEthiopia2017.pdf.
8. World Health Organization. Global Health Sector Strategy on Hiv 2016–2021 Towards Ending Aids; 2016.
9. UNAIDS. 90-90-90 an Ambitious Treatment Target to Help End the AIDS Epidemic; 2014.
10. Federal HIV/AIDS Prevention & Control Office E. HIV/AIDS Strategic Plan 2015–2020 in an Investment Case Approach; 2014.
11. Crofts N, Patterson D Police Must Join the Fast Track to End AIDS by 2030. Wiley Online Library; 2016.
12. World Health Organization. HIV/ADIS Department; 2017.
13. Saumu WM, Maleche-Obimbo E, Irimu G, Kumar R, Gichuhi C, Karau B. Predictors of loss to follow-up among children attending HIV clinic in a hospital in rural Kenya. Pan Afr Med J. 2019;32(216). doi:10.11604/pamj.2019.32.216.18310
14. Egger M, Spycher B, Sidle J, Weigel R, Geng E. Correcting mortality for loss to follow-up: a nomogram applied to antiretroviral; 2011.
15. Hønge BL, Jespersen S, Nordentoft PB, et al. Loss to follow-up occurs at all stages in the diagnostic and follow-up period among HIV-infected patients in Guinea-Bissau: a 7-year retrospective cohort study. BMJ Open. 2013;3(10):e003499. doi:10.1136/bmjopen-2013-003499
16. Kalembo FW, Zgambo M. Loss to followup: a major challenge to successful implementation of prevention of mother-to-child transmission of HIV-1 programs in sub-Saharan Africa. Int Sch Res Notices. 2012;2012.
17. McNairy ML, Lamb MR, Carter RJ, et al. Retention of HIV-infected children on antiretroviraltreatment in HIV care and treatment programs in Kenya, Mozambique, Rwanda and Tanzania. J Acquir Immune Defic Syndr. 2012;62(70):81.
18. Weiler G. Global Update on HIV Treatment 2013: Results, Impact and Opportunities. Geneva: World Health Organization; 2013:2017.
19. Brinkhof MWG, Pujades-Rodriguez M, Egger M, Emery S. Mortality of patients lost to follow-up in antiretroviral treatment programmes in resource-limited settings: systematic review and meta-analysis. PLoS One. 2009;4(6):e5790. doi:10.1371/journal.pone.0005790
20. Fox MP, Rosen S. Systematic review of retention of pediatric patients on HIV treatment in low and middle-income countries 2008–2013. Aids. 2015;29(4):493–502. doi:10.1097/QAD.0000000000000559
21. Leroy V, Malateste K, Rabie H, et al. Outcomes of antiretroviral therapy in children in Asia and Africa: a comparative analysis of the IeDEA pediatric multiregional collaboration. J Acquir Immune Defic Syndr. 2013;62(2):208. doi:10.1097/QAI.0b013e31827b70bf
22. Manuel K, Sibhatu IA, Feleke G. HIV case management in Ethiopia: a pragmatic approach to maximizing adherence to long-term treatment and retention in chronic illness care; 2014.
23. Levi J, Raymond A, Pozniak A, Vernazza P, Kohler P, Hill A. Can the UNAIDS 90-90-90target be achieved? A systematic analysis of national HIV treatment cascades. BMJ Glob Health. 2016;1(2):e000010. doi:10.1136/bmjgh-2015-000010
24. Sengayi M, Dwane N, Marinda E, Sipambo N, Fairlie L, Moultrie H. Predictors of loss to follow-up among children in the first and second years of antiretroviral treatment in Johannesburg, South Africa. Glob Health Action. 2013;6(1):19248. doi:10.3402/gha.v6i0.19248
25. Mulatu Biru IH, Lundqvist P, Jerene D. Rates and predictors of attrition among children on antiretroviral therapy in Ethiopia: a prospective cohort study. PLoS One. 2018;13(2):e0189777.
26. Miller CM, Ketlhapile M, Rybasack‐Smith H, Rosen S. Why are antiretroviral treatment patients lost to follow‐up? A qualitative study from South Africa. Trop Med Int Health. 2010;15:48–54. doi:10.1111/j.1365-3156.2010.02514.x
27. Mutanga JN, Mutembo S, Ezeamama AE, et al. Predictors of loss to follow-up among children on long-term antiretroviral therapy in Zambia (2003–2015). BMC Public Health. 2019;19(1):1120. doi:10.1186/s12889-019-7374-0
28. Ojikutu B, Higgins-Biddle M, Greeson D, et al. The association between quality of HIV care, loss to follow-up and mortality in pediatric and adolescent patients receiving antiretroviral therapy in Nigeria. PLoS One. 2014;9(7):e100039. doi:10.1371/journal.pone.0100039
29. Massavon W, Barlow-Mosha L, Mugenyi L, et al. Factors determining survival and retention among HIV-infected children and adolescents in a community home-based care and a facility-based family-centred approach in Kampala, Uganda: a cohort study. Isrn Aids. 2014;2014:1–13. doi:10.1155/2014/852489
30. Ditekemena J, Luhata C, Bonane W, et al. Antiretroviral treatment program retention among HIV-infected children in the Democratic Republic of Congo. PLoS One. 2014;9(12):e113877. doi:10.1371/journal.pone.0113877
31. Auld AF, Tuho MZ, Ekra KA, et al. Temporal trends in mortality and loss to follow-up among children enrolled in Cote d’Ivoire’s national antiretroviral therapy program. Pediatr Infect Dis J. 2014;33(11):1134–1140. doi:10.1097/INF.0000000000000457
32. Da Cruz Gouveia PADC, da Silva GAP, de Fatima Pessoa Militão de Albuque M. Predictors of loss to follow-up among children registered in an HIV prevention mother-to-child transmission cohort study in Pernambuco, Brazil. BMC Public Health. 2014;14(1):1232. doi:10.1186/1471-2458-14-1232
33. Hodgson I, Plummer ML, Konopka SN, et al. A systematic review of individual and contextual factors affecting ART initiation, adherence, and retention for HIV-infected pregnant and postpartum women. PLoS One. 2014;9(11):e111421. doi:10.1371/journal.pone.0111421
34. UNAIDS U, and World Health Organization. The Incredible Journey of the Global Plan Towards the Elimination of New HIV Infections Among Children by 2015 and Keeping Their Mothers Alive; 2016.
35. Chandiwana N, Sawry S, Chersich M, Kachingwe E, Makhathini B, Fairlie L. High loss to follow-up of children on antiretroviral treatment in a primary care HIV clinic in Johannesburg, South Africa. Medicine. 2018;97(29):29. doi:10.1097/MD.0000000000010901
36. Fetene T. Incidence and predictors of lost to follow upamong children on antiretroviral therapy at East and West Gojjam Zone referral hospitals, (2018); 2018.
37. (EMOH) Emoh. National comprehensive HIV prevention, care and treatment training for health care providers; 2018.
38. McCormick NM, Nan L, Sando D, et al. Risk factors of loss to follow up among HIV positive pediatric patients in Dar es Salaam, Tanzania. J Acquir Immune Defic Syndr. 2015;70(3):e73. doi:10.1097/QAI.0000000000000782
39. Teeraananchai S, Kerr SJ, Puthanakit T, et al. Attrition and mortality of children receiving antiretroviral treatment through the universal coverage health program in Thailand. J Pediatr. 2017;188:210–6. e1. doi:10.1016/j.jpeds.2017.05.035
40. Nimkar S, Valvi C, Kadam D, et al. Loss to follow‐up and mortality among HIV‐infected adolescents receiving antiretroviral therapy in Pune, India. HIV Med. 2018;19(6):395–402. doi:10.1111/hiv.12605
41. Kranzer K, Bradley J, Musaazi J, et al. Loss to follow‐up among children and adolescents growing up with HIV infection: age really matters. J Int AIDS Soc. 2017;20(1):21737. doi:10.7448/IAS.20.1.21737
42. Melaku Z, Lulseged S, Wang C, et al. Outcomes among HIV‐infected children initiating HIV care and antiretroviral treatment in Ethiopia. Trop Med Int Health. 2017;22(4):474–484. doi:10.1111/tmi.12834
43. Hagströmer O, Lundstedt L, Balcha TT, Björkman P. Decentralised paediatric HIV care in Ethiopia: a comparison between outcomes of patients managed in health centres and in a hospital clinic. Glob Health Action. 2013;6(1):22274. doi:10.3402/gha.v6i0.22274
44. Vermund SH, Blevins M, Moon TD, et al. Poor clinical outcomes for HIV infected children on antiretroviral therapy in rural Mozambique: need for program quality improvement and community engagement. PLoS One. 2014;9(10):e110116. doi:10.1371/journal.pone.0110116
45. Machine EM, Gillespie SL, Homedes N, et al. Lost to follow-up: failure to engage children in care in the first three months of diagnosis. AIDS Care. 2016;28(11):1402–1410. doi:10.1080/09540121.2016.1179714
46. Weigel R, Estill J, Egger M, et al. Mortality and loss to follow-up in the first year of ART: Malawi national ART programme. AIDS. 2012;26(3):365–373. doi:10.1097/QAD.0b013e32834ed814
47. Ekouevi DK, Azondekon A, Dicko F, et al. 12-month mortality and loss-to-program in antiretroviral-treated children: the IeDEA pediatric West African Database to evaluate AIDS (pWADA), 2000–2008. BMC Public Health. 2011;11(1):519. doi:10.1186/1471-2458-11-519
48. Assemie MA, Muchie KF, Ayele TA. Incidence and predictors of loss to follow up among HIV-infected adults at Pawi General Hospital, northwest Ethiopia: competing risk regression model. BMC Res Notes. 2018;11(1):287. doi:10.1186/s13104-018-3407-5
49. Bikoro B, Oljira L, Gobena T, Erkalo D. Incidence and predictors of loss to follow-up among human immunodeficiency virus-infected adult patients on anti-retroviral therapy at Hadiya zone public hospitals, Southern Ethiopia: a retrospective cohort study. J Public Health. 2020:1–12.
50. Labban L. The implications of HIV/AIDS on the nutritional status and the MNT for its patients. EC Nutr. 2016;3:680–686.
51. Duggal S, Chugh TD, Duggal AK. HIV and malnutrition: effects on immune system. Clin Dev Immunol. 2012;2012:1–8. doi:10.1155/2012/784740
52. Opio D, Semitala FC, Kakeeto A, et al. Loss to follow-up and associated factors among adult people living with HIV at public health facilities in Wakiso district, Uganda: a retrospective cohort study. BMC Health Serv Res. 2019;19(1):628. doi:10.1186/s12913-019-4474-6
53. Holtzman CW, Brady KA, Yehia BR. Retention in care and medication adherence: current challenges to antiretroviral therapy success. Drugs. 2015;75(5):445–454. doi:10.1007/s40265-015-0373-2
54. Gebremedhin KB, Haye TB. Factors associated with anemia among people living with HIV/AIDS taking ART in Ethiopia. Adv Hematol. 2019;2019:1–8. doi:10.1155/2019/9614205
55. Mirkuzie AH, Ali S, Abate E, Worku A, Misganaw A. Progress towards the 2020 fast track HIV/AIDS reduction targets across ages in Ethiopia as compared to neighboring countries using global burden of diseases 2017 data. BMC Public Health. 2021;21(1):1.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.