")
Back to Journals » International Journal of General Medicine » Volume 15
Incidence and Epidemiological Characters of Developmental Dysplasia of the Hip in Lianyungang: Based on Ultrasound Screening: A Retrospective Study
Received 8 September 2022
Accepted for publication 7 December 2022
Published 13 December 2022 Volume 2022:15 Pages 8547—8555
DOI https://doi.org/10.2147/IJGM.S389145
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dongsheng Zhu, Hongqi Zhu
Department of Pediatric Orthopedics, The First People’s Hospital of Lianyungang, Lianyungang, 222000, People’s Republic of China
Correspondence: Dongsheng Zhu; Hongqi Zhu, Email [email protected]; [email protected]
Objective: To explore the incidence and epidemiological characteristics of developmental dysplasia of hip (DDH) in Lianyungang and provide a basis for early detection, early diagnosis and early treatment.
Methods: Ultrasound screening was performed on aged 4– 6 weeks to collect the incidence and epidemiological profiles of DDH. Graf hip ultrasound imaging was used for screening. DDH was diagnosed with a classification of ≥IIa−.
Results: Of the 9803 babies, 4999 were boys and 4687 were girls. There were 117 babies diagnosed with DDH, incidence rate of 1.19%. The incidence of DDH rate at left was higher than that at right (0.89%, 87/9803) vs (0.37%, 36/9803) and the difference was statistically significant (P < 0.001). Multivariate logistic regression analysis indicated that female (OR = 5.059, 95% CI: 3.012– 9.109) and first child (OR = 1.871, 95% CI: 1.169– 2.832) were the risk factors of DDH. Due to the small number of relevant cases and the absence of DDH cases, improper swaddling, abnormal amniotic fluid volume and confluent malformation could not be included for statistical comparison.
Conclusion: The incidence of DDH in infants aged 4– 6 weeks in Lianyungang was 1.19% (117/9803). DDH was more prone to occur on the left side. Girl and first-borns were the risk factors of DDH.
Keywords: epidemiology, developmental dysplasia of the hip ultrasound
Introduction
Developmental dysplasia of the hip (DDH) is one of the most common orthopedic hip diseases of the pediatric population. If not diagnosed and treated in time, it leads to hip pain, abnormal walking, and even severe functional impairment in adulthood.1 Therefore, early screening and timely intervention are currently considered the best solutions for DDH prevention and treatment.2 In recent years, with the introduction of ultrasound examinations of the hip and related epidemiological investigations, the examination methods, screening times, and diagnostic criteria used have not been the same.3–6 In China, color Doppler ultrasound was widely used to screen babies younger than 6 months of age for DDH.7 Countries in Asia, such as South Korea, also use this approach.8 A meta-analysis showed an increased risk of DDH in babies born breech, in female, in babies with a positive family history, and in babies with clicking hip at the time of clinical examination.9 Our hospital started Graf hip ultrasound screening method in 2013 and gradually established an early DDH screening network across the city since 2019. In 2021, the hip ultrasound technology, screening time and diagnostic criteria were unified across the city, and the epidemiological characteristics of DDH in Lianyungang district were obtained. The geographical location of Lianyungang in China is shown in (Figure 1).
 |
Figure 1 Geography of Lianyungang in China. |
Materials and Methods
Patients
Babies who received hip ultrasounds from June 2019 to June 2022 at the First People’s Hospital of Lianyungang were selected for the study. Babies were recruited for the current study if they were between 4 and 6 weeks old, able to successfully complete an ultrasound of the hip, and if patient’s guardian was willing to participate in this study and sign a written informed consent. Those with poorly completed medical records, lacking epidemiological data necessary for this work, and who had underwent some kind of prior therapeutic intervention for DDH elsewhere were excluded. The Ethics Committee of the First People’s Hospital of Lianyungang approved all protocols (December 2021; approval no. 20210203).
Ultrasound Examination Methods
Using SIUI color Doppler ultrasound (Apogee 3100) with a 7.5–10.0 MHz linear array probe and infant hip ultrasound examination bed, both hips of the children were examined, standard plane images were obtained, and the α and β angles were measured, then classification was performed according to the measurement results. Among them, α angle is the angle between the line subtended from the ilium and the line of the bony acetabulum, which is mainly used to examine the development of the bony acetabulum; β angle is between the baseline and the cartilaginous roof line that is drawn from the turning point/bony rim (concavity/convexity) through the middle of the labrum (Figure 2).10
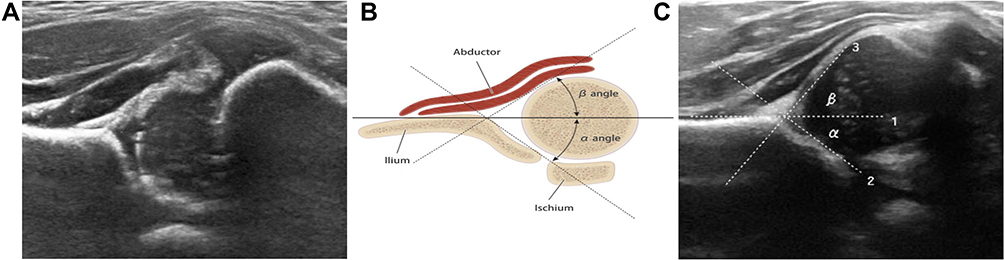 |
Figure 2 α and β angles. (A) Coronal ultrasound image of the Hip; (B) Ultrasound illustrating the measurement technique of the α angle and β angle; (C) Coronal ultrasound image of theα angle and β angle. |
Diagnostic Criteria
Graf classification was used to diagnose DDH, and it was most widely accepted worldwide (Table 1).11 Based on this classification, babies with Type I hip did not require any treatment, whereas babies with Type IIb and higher classification hips required intervention. Management of babies with Type IIa hips remains controversial due to a lack of consensus on whether these hips required treatment, with some authors suggesting that they simply represent physiologically immature hips with a slightly delayed maturation of the bony acetabular roof. Because of IIa− type is a defect in the development of the top of acetabular, so in this study, a diagnosis of DDH was Graf classification ≥IIa− type, including type of IIa−, IIb, IIc, III;, IV and D.
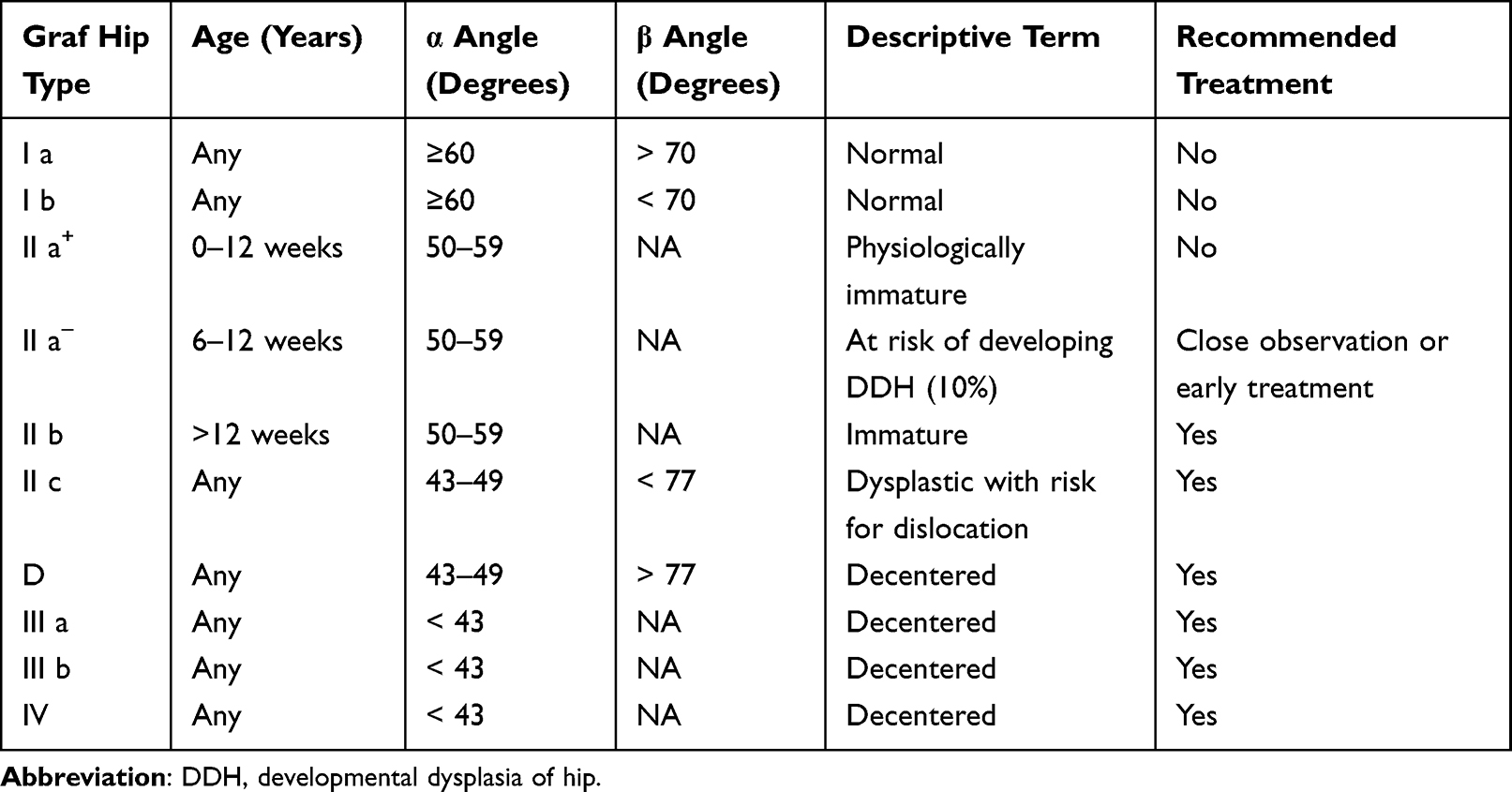 |
Table 1 Ultrasound Classification According to the Graf Method |
Epidemiology Data
A questionnaire on the epidemiological characteristics of DDH was designed (Table 2), which was filled out by the child’s guardian with the help of a nurse, and the data was kept after doctors confirmed that it was correct. In this study, the authors double-checked and obtained the final data according to the inclusion and exclusion criteria.
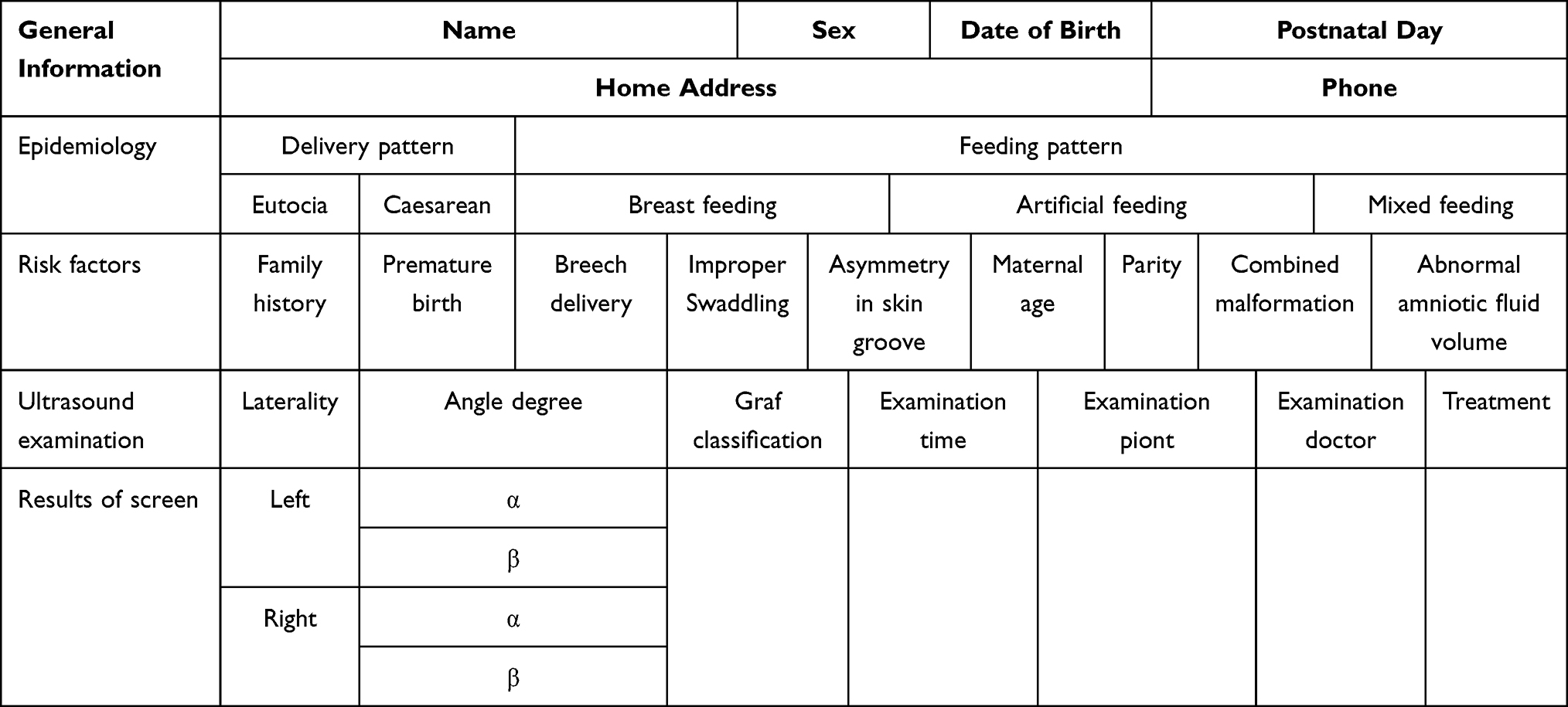 |
Table 2 Child Hip Ultrasound Screening Registry Date |
Identification of Sample Size
Based on our pilot data, the sample size was estimated using the PASS11 software (NCSS, Kaysville, Utah) with a study power of 80% and a significance level of 5%. A minimum of 65 patients was recommended.
Statistical Analysis
Statistical analyses were performed using SPSS 17.0 statistical software (SPSS Inc., Chicago, IL, USA). Pearson’s χ2 and Fisher’s exact tests were performed to assess the categorical variables. The relationship between risk factors and DDH incidence was analyzed using multivariate logistic regression analysis. P < 0.05 was considered to indicate a statistically significant difference.
Results
Between June 2019 and June 2022, a total of 18,932 babies underwent hip ultrasound and filled out the questionnaire at the First People’s Hospital of Lianyungang. According to the inclusion and exclusion criteria, 9803 cases were eventually included. Of these, 4999 were male and 4687 were female. Type I was diagnosed in 8903 cases, type IIa+ in 713 cases, type IIa−in 35 cases, type IIc in 42 cases, type D in 8 cases, type IIIa in 11 cases, type IIIb in 9 cases, and type IV in 14 cases. If the same DDH child had of hip joints of different types on both sides, the type was calculated based on the severe side (Table 3).
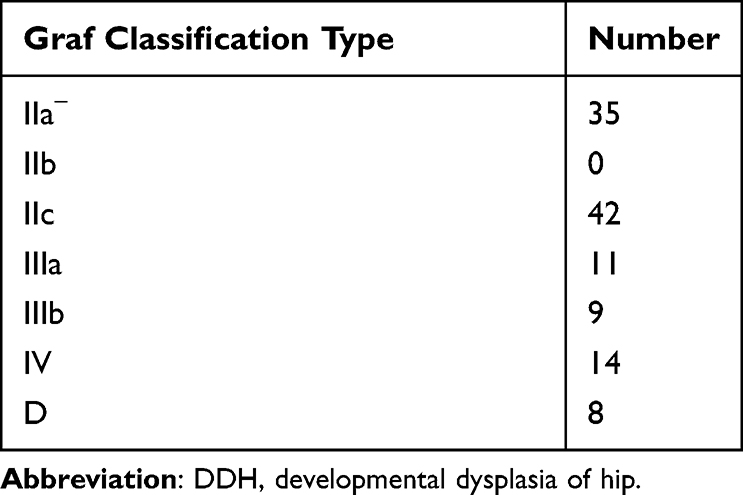 |
Table 3 Graf Classification Type of 117 DDH Cases |
Finally, a total of 117 children were diagnosed with DDH in this study, including 35 cases of type IIa−, 42 cases of type IIb and IIc, and 42 cases of type D, IIIa, IIIb, and IV. The confidence interval (CI) of DDH for the calculated population incidence was 9.8/thousand-13.7/thousand in the city of Lianyungang per year. The incidence of DDH on the left side was 87, higher than that on the right side (P < 0.001); there were 97 female and 20 males (P < 0.001); and there were also 88 first-time births and 29 that were not (P = 0.005); the difference was statistically significant (Table 4). A multivariate logistic regression analysis was performed with the occurrence of DDH as the dependent variable and each risk factor as the independent variable. The results suggest that female (OR = 5.059, 95% CI: 3.012–9.109) and first birth (OR = 1.871, 95% CI: 1.169–2.832) were risk factors for DDH, with no statistical difference between other risk factors including improper swaddling, asymmetry in the skin groove, combined malformation, and abnormal amniotic fluid volume (Table 5) (Figure 3).
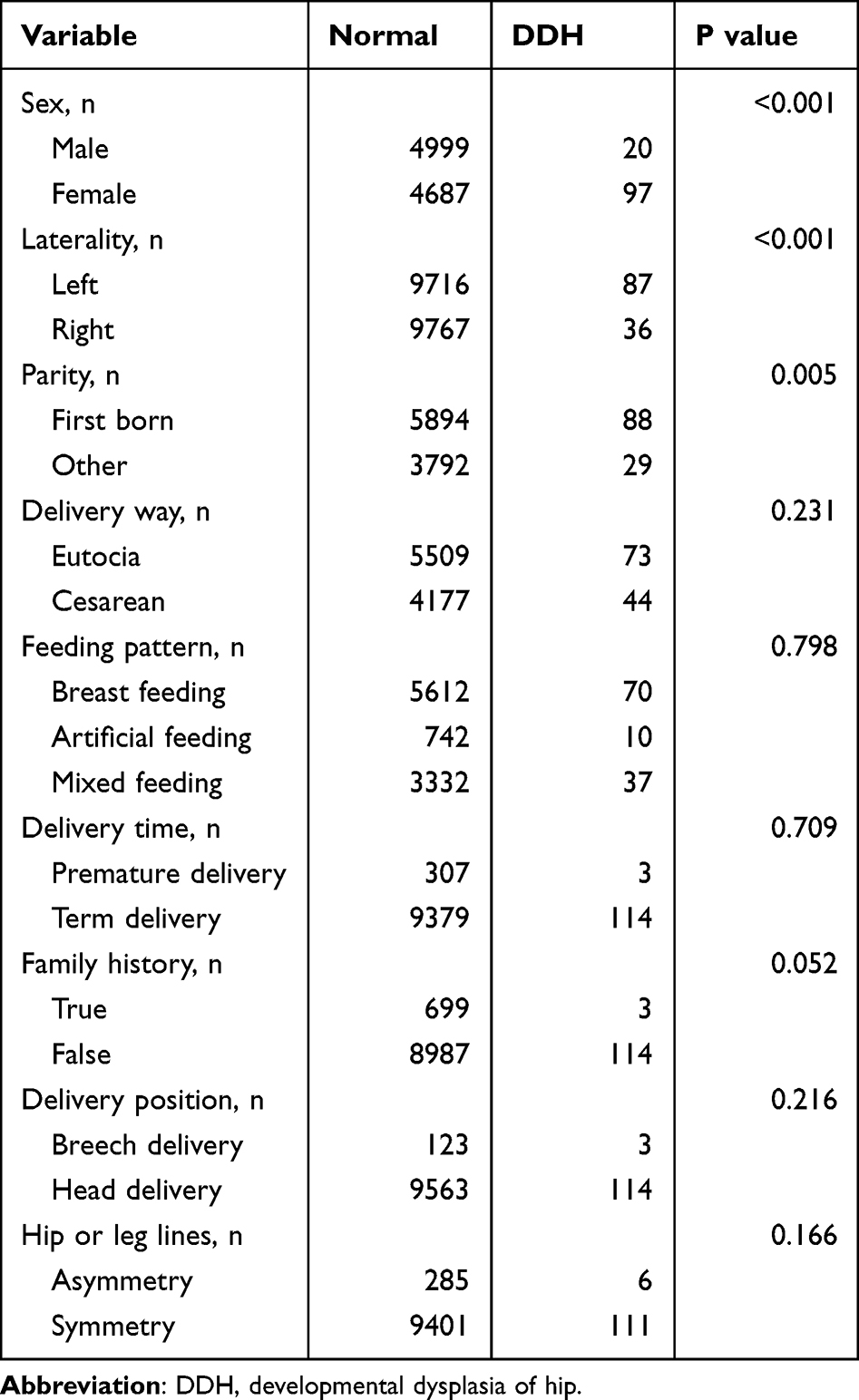 |
Table 4 Patient Characteristic |
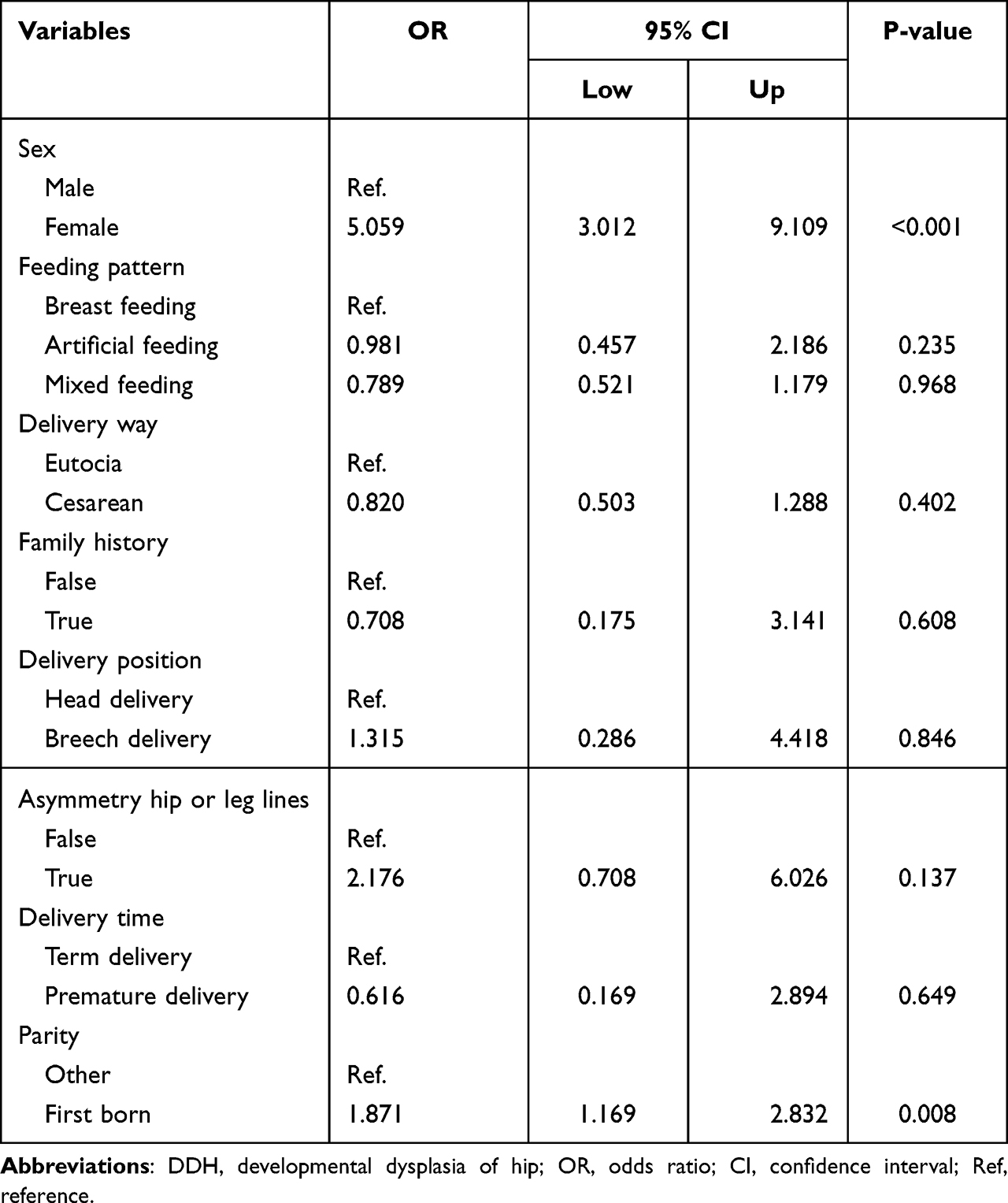 |
Table 5 Logistic Regression Analysis of Risk Factors for DDH |
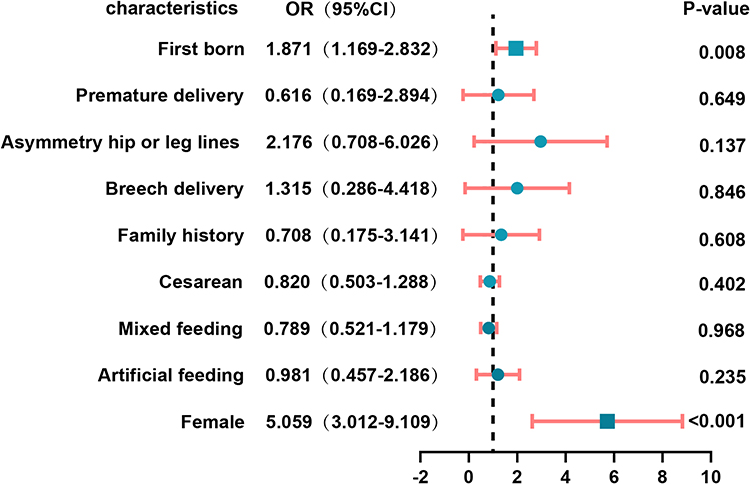 |
Figure 3 Logistic regression analysis of risk factors for DDH. Abbreviations: DDH, developmental dysplasia of hip; Blue circles and the blue squares: odds ratio. |
Discussion
Time for DDH Screening
With the development of ultrasound diagnostics, most cases of DDH can be diagnosed within 6 months of birth, and some countries and regions have adopted hip ultrasound screening for newborns, which has improved the early diagnosis and treatment rates.12 Early screening and intervention can significantly reduce the risk of late surgery in babies with DDH.13 The time of early ultrasound screening is currently debated by scholars. Donnelly believed that 6 weeks after birth was an important time to perform a hip ultrasound examination and recommended two clinical ultrasounds, consisting of the first at birth and the second between the ages of 6 and 10 weeks.14 Gokharman et al also studied the timing of ultrasonography and found that ultrasonography at 8 weeks postpartum was better than those at 4 weeks postpartum, and they suggested that 8 weeks postpartum was the best time for ultrasound screening.15 However, after an extensive review of the literature, the American Academy of Orthopaedic Surgeons currently recommends 4–6 weeks as the optimal screening time,3 so we chose 4–6 weeks as the screening time for this study.
Incidence of DDH and Early Screening and Diagnostic Criteria
Reports of the incidence of DDH vary widely across the world, ranging from 0.15% to 4.45%.13,16–18 In addition to geographic and ethnic factors, this may also be related to the diagnostic methods, timing of testing, diagnostic criteria, and sample size. The incidence of DDH in this study was 1.19%, which is consistent with previous reports.
DDH includes hip dislocation, hip subluxation, and acetabular dysplasia. Early screening should not only detect hip dislocations or subluxations but also focus on finding children with hip dysplasia. In the Graf classification, type IIb and type IIc are typical of acetabular dysplasia, but whether type IIa can be diagnosed as DDH is still debated. Nicola et al argued that even if type IIa was not pathological, it represented potentially a low-grade dysplasia and required a second examination.19 Graf further refined the IIa classification at a later stage. Babies within 6 weeks after birth are divided into type IIa+ and type IIa− according to α angle and the days after birth. Type IIa+ is physiologically immature and does not require intervention, while type IIa− is a defect in the development of the acetabular apex and is recommended for close observation or early treatment.10 A cross-sectional study of Chinese people found a prevalence of DDH of 1.52%,20 which was close to the incidence in this study. This study also had some differences from the previous literature. First, type IIa− was included in the diagnosis of DDH in this study. Second, the screening period in this study was 3–4 weeks after birth, while most other reports were 0–6 months or even later. This may also be responsible for the difference in the final incidence results. Taken together, we believe that early screening and diagnosis of DDH by Graf classification ≥type IIa− may provide a more comprehensive assessment of overall incidence.
DDH Risk Factors
The pathogenesis of DDH is not well understood. Most scholars now agree that that femininity, breech presentation, oligohydramnios, prematurity, and other deformities such as clubfoot or torticollis are risk factors for DDH.21 In recent years, however, there have been reports of a different view. A meta-analysis by Ibrahim et al suggested no association between clubfoot and incidence of DDH.22 Swarup et al suggested that preterm birth was a protective factor against DDH, and that those with higher birth weights were more susceptible to DDH.23 A 10-year survey in the United Kingdom showed that female sex, family history, breech presentation and first birth were the main risk factors for DDH, with pregnancy after 38 weeks also a high-risk factor.24 The results of this study showed that female was a risk factor for DDH, the incidence of DDH in the left hip was higher than that in the right side, and the risk of DDH in the first child was higher than that in the second child and later, which was consistent with most reports. However, in this study, the traditionally important risk factor for breech presentation failed to emerge as a risk factor for DDH occurrence, and two possible reasons for this were analyzed. First, there were 123 cases of breech delivery in this group, of which 108 (88%) for cesarean section. Breech cesarean section may reduce the pathogenic effects of breech presentation, as it avoids the stimulation of the lower limbs during natural delivery. Second, the time node in this study was 4–6 weeks after birth, and babies born partial breech may naturally develop from hip dysplasia at birth to a relatively mature hip. A study from The Children’s Hospital of Philadelphia also confirmed that breech babies had significantly higher spontaneous relief of mild hip instability than non-breech babies.25 As a result, the risk of DDH from breech presentation may decrease with growth, but more samples and longer follow-up are needed to make firm conclusions. In addition, factors such as amniotic fluid volume and combined malformations could not be included in the statistical analysis due to the absence of DDH children in the sample, which may be related to the insufficient overall sample size. However, the present study showed no statistical significance between hip or leg asymmetry, feeding patterns, delivery patterns, prematurity, and DDH incidence. It should be noted that the asymmetry in hip or leg lines is common in pediatric orthopaedic clinics, often causing anxiety among parents, and a good job of popular science is required.
Shortcomings of This Study
First, some parents of children may have misconceptions about specialized medical terms, leading to related errors. Second, the survey period and sample size were still insufficient, and there may be errors or biases. In the future, we intend to build on this work with a longer-term, multi-center, large-sample epidemiological study of DDH on this basis to further improve the quality of early DDH screening and reduce the rates of DDH surgery and disability.
Ethics Approval and Consent to Participate
Written informed consent was provided by guardian of all enrolled babies. This research conformed to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Lianyungang No. 1 People’s Hospital Affiliated to Xuzhou Medical University (December 2021; approval no. 20210203).
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Alves C, Truong WH, Thompson MV, et al. Diagnostic and treatment preferences for developmental dysplasia of the Hip: a survey of EPOS and POSNA members. J Childrens Orthopaedics. 2018;12(3):236–244. doi:10.1302/1863-2548.12.180034
2. Paton RW. Screening in developmental dysplasia of the Hip (DDH). Surgeon. 2017;15(5):290–296.
3. Mulpuri K, Song KM, Gross RH, et al. The American Academy of Orthopaedic Surgeons evidence-based guideline on detection and nonoperative management of pediatric developmental dysplasia of the hip in infants up to six months of age. J Bone Joint Surg Am. 2015;97(20):1717–1718.
4. Shorter D, Hong T, Osborn DA. Cochrane review: screening programmes for developmental dysplasia of the Hip in newborn infants. Evid Based Child Health. 2013;8(1):11–54.
5. Graf R. The diagnosis of congenital Hip-joint dislocation by the ultrasonic Combound treatment. Arch Orthop Trauma Surg. 1980;97(2):117–133.
6. Harcke HT, Clarke NM, Lee MS, Borns PF, MacEwen GD. Examination of the infant Hip with real-time ultrasonography. J Ultrasound Med. 1984;3(3):131–137.
7. Li H, Shu L, Yu J, et al. Using Z-score to optimize population-specific DDH screening: a retrospective study in Hangzhou, China. BMC Musculoskelet Disord. 2021;22(1):344.
8. Kang MS, Han GW, Kam M, Park SS. Clinical significance of asymmetric skin folds in the medial thigh for the infantile screening of developmental dysplasia of the Hip. Pediatr Neonatol. 2019;60(5):570–576.
9. de Hundt M, Vlemmix F, Bais JM, et al. Risk factors for developmental dysplasia of the Hip: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2012;165(1):8–17.
10. Graf R. Hip sonography: background; technique and common mistakes; results; debate and politics; challenges. Hip Int. 2017;27(3):215–219. doi:10.5301/hipint.5000514
11. Vafaee AR, Baghdadi T, Baghdadi A, Jamnani RK. DDH epidemiology revisited: do we need new strategies? Arch Bone Joint Surgery. 2017;5(6):440–442.
12. Westacott DJ, Butler D, Shears E, Cooke SJ, Gaffey A. Universal versus selective ultrasound screening for developmental dysplasia of the Hip: a single-centre retrospective cohort study. J Pediatric Orthopaedics B. 2018;27(5):387–390. doi:10.1097/BPB.0000000000000508
13. McAllister DA, Morling JR, Fischbacher CM, Reidy M, Murray A, Wood R. Enhanced detection services for developmental dysplasia of the Hip in Scottish children, 1997–2013. Arch Dis Child. 2018;103(11):1021–1026.
14. Donnelly KJ, Chan KW, Cosgrove AP. Delayed diagnosis of developmental dysplasia of the Hip in Northern Ireland: can we do better? Bone Joint J. 2015;97-b(11):1572–1576. doi:10.1302/0301-620X.97B11.35286
15. Gokharman FD, Aydin S, Fatihoglu E, Ergun E, Kosar PN. Optimizing the time for developmental dysplasia of the hip screening: earlier or later? Ultrasound Q. 2019;35(2):130–135. doi:10.1097/RUQ.0000000000000348
16. Yang S, Zusman N, Lieberman E, Goldstein RY. Developmental dysplasia of the Hip. Pediatrics. 2019;143(1). doi:10.1542/peds.2018-1147
17. Dezateux C, Rosendahl K. Developmental dysplasia of the Hip. Lancet. 2007;369(9572):1541–1552.
18. Pulik Ł, Płoszka K. Impact of multiple factors on the incidence of developmental dysplasia of the hip: risk assessment tool. Medicina. 2022;58(9):1158.
19. Guindani N, De Pellegrin M. Developmental dysplasia of the Hip screening during the lockdown for COVID-19: experience from Northern Italy. J Children’s Orthopaedics. 2021;15(3):248–254.
20. Tian FD, Zhao DW, Wang W, et al. Prevalence of developmental dysplasia of the hip in Chinese adults: a cross-sectional survey. Chin Med J. 2017;130(11):1261–1268.
21. Schams M, Labruyère R, Zuse A, Walensi M. Diagnosing developmental dysplasia of the Hip using the Graf ultrasound method: risk and protective factor analysis in 11,820 universally screened newborns. Eur J Pediatr. 2017;176(9):1193–1200.
22. Ibrahim T, Riaz M, Hegazy A. The prevalence of developmental dysplasia of the Hip in idiopathic clubfoot: a systematic review and meta-analysis. Int Orthop. 2015;39(7):1371–1378.
23. Swarup I, Penny CL, Dodwell ER. Developmental dysplasia of the Hip: an update on diagnosis and management from birth to 6 months. Curr Opin Pediatr. 2018;30(1):84–92.
24. Woodacre T, Ball T, Cox P. Epidemiology of developmental dysplasia of the Hip within the UK: refining the risk factors. J Childrens Orthopaedics. 2016;10(6):633–642.
25. Sarkissian EJ, Sankar WN, Baldwin K, Flynn JM. Is there a predilection for breech infants to demonstrate spontaneous stabilization of DDH instability? J Pediatr Orthop. 2014;34(5):509–513.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.