")
Back to Journals » OncoTargets and Therapy » Volume 8
Incidence and clinical characteristics of unexpected uterine sarcoma after hysterectomy and myomectomy for uterine fibroids: a retrospective study of 10,248 cases
Authors Zhao W, Bi F, Li D, Yang Q
Received 23 July 2015
Accepted for publication 30 September 2015
Published 15 October 2015 Volume 2015:8 Pages 2943—2948
DOI https://doi.org/10.2147/OTT.S92978
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr William C. Cho
Wan-Cheng Zhao,1 Fang-Fang Bi,1 Da Li,2 Qing Yang1
1Department of Obstetrics and Gynecology, 2Center of Reproductive Medicine, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China
Background: Uterine fibroids often require a hysterectomy or myomectomy via laparotomy or laparoscopy. Morcellation is often necessary to perform a laparoscopic surgery. The objective of this study is to determine the incidence of unexpected uterine sarcomas (UUSs) after hysterectomy and myomectomy for uterine fibroids and to reduce the occurrence and avoid the morcellation of UUSs by analyzing their characteristics.
Methods: Women who had a hysterectomy or myomectomy for uterine fibroids in Shengjing Hospital of China Medical University between November 2008 and November 2014 were selected for the study, and their clinical characteristics were analyzed.
Results: During the period, 48 UUSs were found in 10,248 cases, and the overall incidence was 0.47%. There was no statistical difference (P=0.449) regarding the incidence (0.50% vs 0.33%) between 42 UUSs in 8,456 cases undergoing laparotomy and six UUSs in 1,792 cases undergoing laparoscopy. Most of the UUSs were stage I (89.58%), which occurred more commonly (56.25%) in women aged 40–49. Abnormal uterine bleeding (39.58%) was the main clinical manifestation. Rapidly growing pelvic masses (12.5%), rich blood flow signals (18.75%), and degeneration of uterine fibroids (18.75%) prompted by ultrasonography may suggest the possibility of UUSs. The margins of most UUSs (93.75%) were regular, which may cause UUSs to be misdiagnosed as uterine fibroids. Fifteen cases underwent magnetic resonance imaging examinations. Approximately 73.33% showed heterogeneous and hypointense signal intensity on T1-weighted images, and 80% showed intermediate-to-high signal intensity on T2-weighted images, with necrosis and hemorrhage in 40% of cases. After contrast administration, 80% presented early heterogeneous enhancement.
Conclusion: The incidence of UUSs after hysterectomy and myomectomy for uterine fibroids was low, and their clinical characteristics are atypical. It is necessary and very critical to make a complete and cautious preoperative evaluation to reduce the occurrence and avoid the morcellation of UUSs.
Keywords: laparoscopy, morcellation, uterine sarcoma, uterine fibroid, hysterectomy, myomectomy
Introduction
Uterine fibroids are one of the most common types of pelvic tumors in women. Various treatments are available for the management of uterine fibroids, such as having a hysterectomy or a myomectomy. The surgical route is shifting from an abdominal to a laparoscopic approach, which confers a more rapid recovery and fewer perioperative complications.1 Morcellation of the specimen is often necessary to perform a laparoscopy.
Uterine sarcoma is a rare, malignant tumor affecting the female genital system that accounts for only 1%–3% of uterine malignancies. The 5-year survival rate is approximately 30%.2,3 The degree of malignancy is high and the prognosis is poor. Inadvertent morcellation of unexpected uterine sarcomas (UUSs) is a surgical risk of laparoscopic hysterectomies and myomectomies. Evidence suggests that morcellation of UUSs potentially upstages the disease, which portends a poor prognosis.4,5 The lack of specific symptoms, signs, or diagnostic techniques for preoperative differentiation from uterine fibroids results in most patients being diagnosed after surgery. If a uterine sarcoma is mistakenly diagnosed as a uterine fibroid and is morcellated via laparoscopy, serious consequences may arise.
The objective of this study is to determine the incidence of UUSs after hysterectomy and myomectomy for uterine fibroids. Until now, few studies have described the characteristics of UUSs in detail. This study is also designed to help reduce the occurrence and avoid the morcellation of UUSs in future by analyzing their characteristics.
Materials and methods
Case selection
This study was approved by the Institutional Review Board at China Medical University, and all subjects provided informed consent. Women who had a hysterectomy or myomectomy for uterine fibroids in Shengjing Hospital of China Medical University between November 2008 and November 2014 were selected for the study. The average patient age was 48.20±7.64 years. Among them, patients who were diagnosed with uterine sarcomas based on postoperative pathology were also selected. Their average age was 47.13±9.48 years. Data analysis was performed to determine the incidence of UUSs. At the same time, the patients were divided into two groups, laparotomy or laparoscopy, and the incidence between them was compared and the impact of morcellation on prognosis was assessed. Finally, we reviewed the patient’s clinical manifestations, laboratory tests, imaging studies, intraoperative findings, surgical pathologic stage, postoperative pathology, and prognosis.
Statistical analysis
Statistical analysis was performed with SPSS 19.0 software (IBM Corporation, Armonk, NY, USA). All results are expressed as the mean ± standard deviation. The Pearson’s chi-square test was used for comparison of percentages between the groups. Statistical significance was assumed at a P<0.05.
Results
Incidence of unexpected uterine sarcomas
During the period, 48 UUSs were found in 10,248 cases, and the overall incidence was 0.47%. Among the 48 patients, open surgery was performed on 42 patients (87.5%), accounting for approximately 0.50% of 8,456 laparotomies. There were six laparoscopies (12.5%), accounting for approximately 0.33% of 1,792 laparoscopies. There was no statistical difference (P=0.449) regarding the incidence of UUSs between laparotomies and laparoscopies.
Among the 8,456 laparotomies, a hysterectomy was performed on 4,250 patients (50.3%), while a myomectomy was performed on 4,206 patients (49.7%). Among the 1,792 laparoscopies, a hysterectomy was performed on 523 patients (29.2%), while a myomectomy was performed on 1,269 patients (70.8%). The number of UUSs diagnosed during a transabdominal hysterectomy or myomectomy was 35 and seven, respectively, accounting for approximately 0.82% (35/4,250) and 0.17% (7/4,206). The number of UUSs diagnosed during a laparoscopic hysterectomy or myomectomy was two and four, respectively, accounting for approximately 0.38% (2/523) and 0.32% (4/1,269). There was no statistical difference (P=0.833) in the incidence of UUSs diagnosed during transabdominal hysterectomy and laparoscopic hysterectomy, and there was no statistical difference (P=0.238) between transabdominal myomectomy and laparoscopic myomectomy. The details of the UUSs are shown in Table 1.
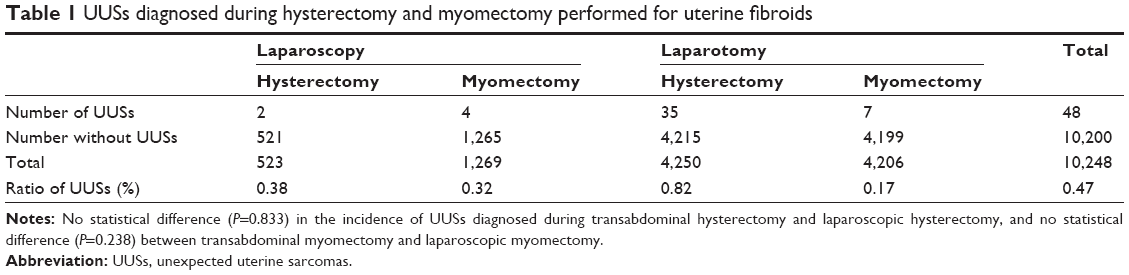 | Table 1 UUSs diagnosed during hysterectomy and myomectomy performed for uterine fibroids |
Clinical data regarding unexpected uterine sarcomas
Ages of the patients with UUSs
The results showed that 27 patients were between 40 and 49 years, comprising the highest proportion (56.25%) of the 48 UUSs. There were only three patients aged over 60, accounting for approximately 6.67%. The number of patients aged 26–39 and 50–59 was seven and eleven, accounting for approximately 14.58% and 22.92%, respectively. Thus, it can be seen that UUSs occurred more commonly in women aged 40–49, but patients aged 26–39 and aged 50–59 cannot be ignored.
Clinical manifestations
The clinical manifestations of uterine sarcomas are nonspecific. Classically, uterine sarcomas are always present as rapidly growing pelvic masses, which may be accompanied by abnormal uterine bleeding and abdominal or pelvic pain.6,7 In our study, 19 UUSs (39.58%) presented with abnormal uterine bleeding (menorrhagia, menostaxis, and irregular uterine bleeding), 16 UUSs (33.33%) presented with no symptoms, six UUSs (12.5%) presented with rapidly growing pelvic masses, five UUSs (10.42%) presented with abdominal or pelvic pain, and two UUSs (4.17%) presented with frequent urination. Abnormal uterine bleeding was the main clinical manifestation, but there were also cases with no symptoms. A rapidly growing pelvic mass may be an indication of uterine sarcoma.
Laboratory tests and imaging studies involving unexpected uterine sarcomas
Of the 48 UUSs, laboratory tests for tumor markers, especially CA-125, were performed on 27 (56.25%). Only five cases had high CA-125 values, ranging from 32.57 to 126.6 mIU/mL, and the average level was 60.94±42.59 mIU/mL. The sensitivity of CA-125 for uterine sarcomas is only 12% and its specificity is poor. We concluded, therefore, that CA-125 contributes minimally to the early diagnosis of uterine sarcoma.
The 48 UUS cases all underwent ultrasonic examinations, and the preoperative ultrasound diagnosis was a uterine fibroid. The diameters of the pelvic mass ranged from 3.2 to 13 cm and the average value was 7.16±2.27 cm. The diameter of the mass in 32 cases (66.67%) was less than 8 cm, in eleven cases (22.92%) from 8 to 10 cm, and only in five (10.41%) were above 10 cm. Among the 48 UUSs, only three cases (6.25%) had irregular margins. The margins of typical uterine sarcomas are mostly nodular, irregular, or ill defined, and the uterus is significantly enlarged, but the size and margins of most UUSs prompted by ultrasonography in this study were atypical, which may cause UUSs to be misdiagnosed as uterine fibroids. Color Doppler flow imaging of nine of the 48 (18.75%) UUSs demonstrated rich blood flow signals, and degeneration of uterine fibroids was found in nine of 48 (18.75%) cases. A rich blood flow signal around a pelvic mass and the degeneration of a uterine fibroid may suggest that more methods are needed to rule out the possibility of a uterine sarcoma.
In our study, 15 out of 48 UUSs (31.25%) were examined by magnetic resonance imaging (MRI). The preoperative MRI diagnoses were uterine fibroids. The diameters ranged from 4.4 to 10.8 cm, and the average value was 7.12±2.27 cm. On the MRI, ten cases (66.67%) appeared as an intramural mass and five cases (33.33%) appeared as a submucosal mass. The margins of 14 cases (93.3%) were regular, and only one case (6.67%) had an irregular margin. The size and margins of most UUSs on the MRI were also atypical. On T1-weighted images, eleven cases (73.33%) showed heterogeneous and hypointense signal intensity, and 12 cases (80%) showed intermediate-to-high signal intensity on T2-weighted images, with a central hyperintensity indicative of extensive necrosis and hemorrhage (six cases, 40%). After contrast administration, 12 cases (80%) presented early heterogeneous enhancement. Of the 15 cases, the MRI diagnosis of six patients (40%) was degenerative uterine fibroids. By comparing the T1 and T2 signals and contrast enhancement, MRI can be used to help distinguish uterine sarcomas from uterine fibroids. When MRI indicated a degenerative uterine fibroid, the possibility of a uterine sarcoma should be strongly considered. This study also showed that it is more difficult to distinguish between benign degenerating uterine fibroids and malignant uterine sarcomas. When the pathology reports were available, the MRI images were reviewed again by the pathologist, but a preoperative MRI diagnosis of a uterine sarcoma still could not be made so easily. In such patients, alternative treatment options should be carefully considered.
Surgical stage, postoperative pathology, and the prognosis of UUSs
According to the postoperative pathology report after the first operation, there were 13 leiomyosarcomas (27.08%), 29 low-grade endometrial stromal sarcomas (ESSs, 60.42%), five undifferentiated endometrial sarcomas (UES, 10.42%), and one adenosarcoma (2.08%). The number of UUSs diagnosed during laparoscopic hysterectomies and myomectomies was two and four, respectively. The details are shown in Table 2. The pathology results are low-grade ESSs. According to the FIGO (International Federation of Gynecology and Obstetrics) 2009 staging for uterine sarcomas, the number of uterine sarcomas for stages I, II, and III after the first operation was 43, one, and four, respectively, thus accounting for approximately 89.58%, 2.08%, and 8.33% of the 48 UUSs. When postoperative pathology was confirmed, ten cases (20.83%) underwent a second operation. Stage I was their first operative stage. Among them, open surgery was performed in five cases (one leiomyosarcomas and four low-grade ESSs). The time interval between the two operations was 7 to 240 days, and the average time interval was 41.9±70.4 days. The time interval was short, and only one case had a time interval >30 days. We suggested that the patient confirm the pathology at another hospital, but she did not attend for personal reasons. A laparoscopic supracervical hysterectomy was the first operation, and morcellation was applied. She underwent a second operation for recurrence after 240 days, and the greater omentum, peritoneum, and mesentery had multiple metastatic lesions. The stage had progressed from stage I to stage III. The result may be related to morcellation, and the patient’s prognosis also decreased. In the remaining nine cases, there was no metastasis, spread, or implanted lesions.
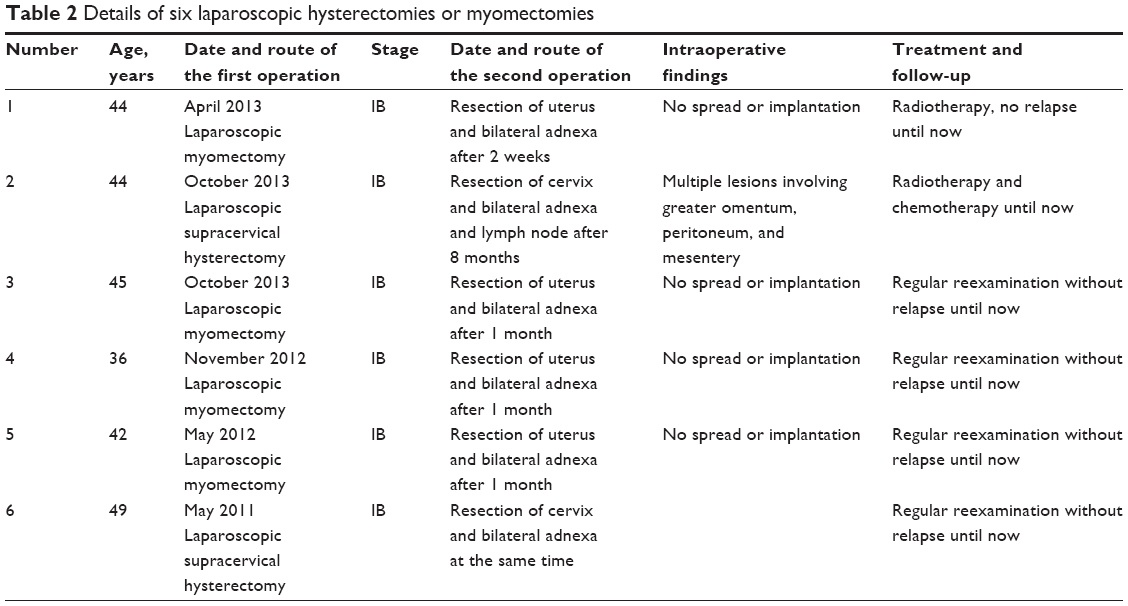 | Table 2 Details of six laparoscopic hysterectomies or myomectomies |
Of the 48 cases, 33 were followed up to make a correct diagnosis, and the number of leiomyosarcoma, ESS, UES, and adenosarcoma was 6, 24, 2, and 1, respectively. The follow-up percentage was 68.75%. The follow-up time was 7–73 months, and the average follow-up time was 30.24±20.11 months. The number of stage I, stage II, and stage III uterine sarcomas was 29, one, and three, respectively. The number of recurrent cases was eight, including seven cases of stage I and one case of stage III. The recurrence rate of stage III (33.33%) was higher than stage I (24.14%), but there was no statistically significant difference (P=0.592) between them. There were 27 laparotomies among the 33 cases, including 18 ESSs (four recurrent cases of stage I, 22.22%), six leiomyosarcomas (two stage I and one stage III recurrent cases), two UESs, and one adenosarcoma. There were six laparoscopies, including one recurrent case (16.67%). There was no statistically significant difference (P=0.634) in the recurrence rates (22.22% vs 16.67%) of stage I ESS between laparotomy and laparoscopy.
Discussion
On April 17, 2014, the US Food and Drug Administration (FDA) issued a safety communication about laparoscopic uterine power morcellation during hysterectomy and myomectomy.8 Laparoscopic power morcellation poses the risk of spreading unsuspected cancerous tissues, most notably uterine sarcomas, beyond the uterus. Based on currently available information, the FDA discourages the use of laparoscopic power morcellation during a hysterectomy or myomectomy for uterine fibroids. George et al9 compared the outcomes between those patients who underwent morcellation or total abdominal hysterectomy as their first surgery for uterine leiomyosarcoma. Intraperitoneal morcellation was associated with a significantly increased risk of abdominal/pelvic recurrences (P=0.001) and with a significantly shorter median recurrence-free survival (10.8 vs 39.6 months; P=0.002). Other studies10–13 have also suggested that the rate of abdominal and pelvic dissemination and pelvic recurrence at 3 months was increased in patients who underwent tumor morcellation, and tumor morcellation was significantly associated with higher stage, poor disease-free survival, and poor overall survival. In this study, one patient underwent a second operation for a recurrence with multiple metastatic lesions after 240 days, which may be the consequence of laparoscopic power morcellation. The tumor stage progressed and may indicate a poor prognosis. The risk of spreading UUSs by laparoscopic power morcellation should thus be given more attention.
A number of studies10,14,15 have reported a poor prognosis for uterine sarcomas closely related to the clinical stage and the method used in the primary operation. In this study, the staging of most UUSs (89.58%) is stage I, which may indicate a good prognosis, but how to make an accurate diagnosis and choose an appropriate treatment is critical. To reduce the occurrence of UUSs and the risk of spreading UUSs by laparoscopic morcellation, the method used for the preoperative diagnosis of a uterine sarcoma is very important. Brohl et al16 found the risk of UUSs varied significantly across age groups, and the risk of uterine sarcoma ranged from a peak of 10.1 cases per 1,000 for patients aged 75–79 years to <1 case per 500 for patients aged <30 years. However, our study found that UUSs occurred more commonly in women aged 40–49. Abnormal uterine bleeding was the main clinical manifestation, and cases with no symptoms cannot be ignored. A rapidly growing pelvic mass may be indicative of a uterine sarcoma. The size and margins of most UUSs as suggested by ultrasonography were atypical, and UUSs can be easily misdiagnosed as uterine fibroids. Attention should be paid to a rich blood flow signal around a pelvic mass and the degeneration of uterine fibroids, and more methods are needed to rule out the possibility of uterine sarcomas. MRI17–19 has an emerging role in the evaluation of pelvic masses. By comparing the localization, surgical margins, T1 and T2 signals, contrast enhancement, and diffusion-weighted imaging, MRI can be very helpful in distinguishing uterine sarcomas from uterine fibroids. In our study, although MRI suggested that the margins of only 6.67% UUSs were irregular, they showed special signal intensity on T1 signals (73.33%), T2 signals (80%), and contrast enhancement (80%). The MRI diagnosis of 40% cases is a degenerative uterine fibroid, which may be strongly indicative of a uterine sarcoma. All of the MRI findings can help us make a correct diagnosis. A preoperative MRI should be recommended. When the pathology reports were available, the pathologist reviewed the MRI images again, but it was still difficult to make a preoperative MRI diagnosis of a uterine sarcoma. This told us that it is more difficult to distinguish between benign degenerating uterine fibroids and malignant uterine sarcomas. Diffusion-weighted imaging and the apparent diffusion coefficient17 may be helpful in distinguishing between the two. Unfortunately, we did not have the data for this. When the malignant potential of a uterine mass is uncertain, alternative treatment options should be carefully considered.
A number of studies20–25 have shown that the incidence of UUSs ranges from 0.09% to 0.49% among women undergoing benign hysterectomy or myomectomy. In this, the incidence of UUSs during hysterectomy and myomectomy performed for uterine fibroids was 0.47%, and there was no statistical difference (P=0.449) in the incidence between laparotomy and laparoscopy (0.50% vs 0.33%). Although the FDA warning should be followed, no tools are available to replace the laparoscopic morcellator. The incidence of UUSs after hysterectomy and myomectomy performed for uterine fibroids is low and there was no statistical significance in recurrence rates (22.22% vs 16.67%, P=0.634) of stage I ESS between laparotomy and laparoscopy. A morcellator may still be used in some situations, such as within a laparoscopic bag.26,27 This technique may reduce the risk of spreading any unsuspected cancerous tissue (created by laparoscopic morcellator) as much as possible. New technologies should be encouraged to limit the dissemination of UUSs as a result of morcellation, while preserving the benefits of minimally invasive surgery.
Conclusion
In conclusion, the incidence of UUSs after hysterectomy and myomectomy for uterine fibroids was low and their clinical characteristics are atypical. It is critical to make a complete and cautious preoperative evaluation to reduce the occurrence and avoid the morcellation of UUSs. Due to the limitations of sample size, further research should be carried out to assess the impact of morcellation on the prognosis of UUSs and summarize the clinical characteristics of UUSs to avoid the risk in future.
Acknowledgments
This work was supported by the Clinical Capability Construction Project for Liaoning Provincial Hospitals (LNCCC-A01-2015), Natural Science Foundation of China (number 81402130), and Doctoral Startup Foundation of Liaoning Province (number 20141045).
Disclosure
The authors report no conflicts of interest in this work.
References
Nieboer TE, Johnson N, Lethaby A, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2009;(3):CD003677. | ||
Sehnal B, Driak D, Kmonickova E, et al. Current classification of malignant tumours in gynecological oncology – part I. Ceska Gynekol. 2011;76(4):279–284. Czech. | ||
Sehnal B, Driak D, Kmonickova E, et al. Current classification of malignant tumours in gynecological oncology – part II. Ceska Gynekol. 2011;76(5):360–366. Czech. | ||
Einstein MH, Barakat RR, Chi DS, et al. Management of uterine malignancy found incidentally after supracervical hysterectomy or uterine morcellation for presumed benign disease. Int J Gynecol Cancer. 2008; 18(5):1065–1070. | ||
Oduyebo T, Rauh-Hain AJ, Meserve EE, et al. The value of re-exploration in patients with inadvertently morcellated uterine sarcoma. Gynecol Oncol. 2014;132(2):360–365. | ||
Seddon BM, Davda R. Uterine sarcomas – recent progress and future challenges. Eur J Radiol. 2011;78(1):30–40. | ||
Wu TI, Yen TC, Lai CH. Clinical presentation and diagnosis of uterine sarcoma, including imaging. Best Pract Res Clin Obstet Gynaecol. 2011;25(6):681–689. | ||
FDA. Laparoscopic Uterine Power Morcellation in Hysterectomy and Myomectomy: FDA Safety Communication. Available from: http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm. Accessed April 17, 2014. | ||
George S, Barysauskas C, Serrano C, et al. Retrospective cohort study evaluating the impact of intraperitoneal morcellation on outcomes of localized uterine leiomyosarcoma. Cancer. 2014;120(20): 3154–3158. | ||
Morice P, Rodriguez A, Rey A, et al. Prognostic value of initial surgical procedure for patients with uterine sarcoma: analysis of 123 patients. Eur J Gynaecol Oncol. 2003;24(3–4):237–240. | ||
Cusido M, Fargas F, Baulies S, et al. Impact of surgery on the evolution of uterine sarcomas. J Minim Invasive Gynecol. 2015;22(6): 1068–1074. | ||
Park JY, Kim DY, Kim JH, Kim YM, Kim YT, Nam JH. The impact of tumor morcellation during surgery on the outcomes of patients with apparently early low-grade endometrial stromal sarcoma of the uterus. Ann Surg Oncol. 2011;18(12):3453–3461. | ||
Park JY, Park SK, Kim DY, et al. The impact of tumor morcellation during surgery on the prognosis of patients with apparently early uterine leiomyosarcoma. Gynecol Oncol. 2011;122(2):255–259. | ||
Gadducci A, Cosio S, Romanini A, Genazzani AR. The management of patients with uterine sarcoma: a debated clinical challenge. Crit Rev Oncol Hematol. 2008;65(2):129–142. | ||
Perri T, Korach J, Sadetzki S, Oberman B, Fridman E, Ben-Baruch G. Uterine leiomyosarcoma: does the primary surgical procedure matter? Int J Gynecol Cancer. 2009;19(2):257–260. | ||
Brohl AS, Li L, Andikyan V, et al. Age-stratified risk of unexpected uterine sarcoma following surgery for presumed benign leiomyoma. Oncologist. 2015;20(4):433–439. | ||
Santos P, Cunha TM. Uterine sarcomas: clinical presentation and MRI features. Diagn Interv Radiol. 2015;21(1):4–9. | ||
Takeuchi M, Matsuzaki K, Harada M. Preliminary observations and clinical value of lipid peak in high-grade uterine sarcomas using in vivo proton MR spectroscopy. Eur Radiol. 2013;23(9):2358–2363. | ||
Thomassin-Naggara I, Dechoux S, Bonneau C, et al. How to differentiate benign from malignant myometrial tumours using MR imaging. Eur Radiol. 2013;23(8):2306–2314. | ||
Wright JD, Tergas AI, Cui R, et al. Use of electric power morcellation and prevalence of underlying cancer in women who undergo myomectomy. JAMA Oncol. 2015;1(1):69–77. | ||
Parker WH, Fu YS, Berek JS. Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet Gynecol. 1994;83(3):414–418. | ||
Takamizawa S, Minakami H, Usui R, et al. Risk of complications and uterine malignancies in women undergoing hysterectomy for presumed benign leiomyomas. Gynecol Obstet Invest. 1999;48(3):193–196. | ||
Theben JU, Schellong AR, Altgassen C, Kelling K, Schneider S, Grosse-Drieling D. Unexpected malignancies after laparoscopic-assisted supracervical hysterectomies (LASH): an analysis of 1,584 LASH cases. Arch Gynecol Obstet. 2013;287(3):455–462. | ||
Zhang J, Zhang J, Dai Y, Zhu L, Lang J, Leng J. Clinical characteristics and management experience of unexpected uterine sarcoma after myomectomy. Int J Gynaecol Obstet. 2015;130(2):195–199. | ||
Graebe K, Garcia-Soto A, Aziz M, et al. Incidental power morcellation of malignancy: a retrospective cohort study. Gynecol Oncol. 2015; 136(2):274–277. | ||
McKenna JB, Kanade T, Choi S, et al. The Sydney contained in bag morcellation technique. J Minim Invasive Gynecol. 2014;21(6): 984–985. | ||
Cholkeri-Singh A, Miller CE. Power morcellation in a specimen bag. J Minim Invasive Gynecol. 2015;22(2):160. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.