")
Back to Journals » Clinical Ophthalmology » Volume 16
Incidence and Characteristics of Orbital Hemorrhages in the United States from 2006 to 2018
Authors Jensen AD , Taneja K , Ahmad MT, Woreta FA , Rajaii F
Received 29 May 2022
Accepted for publication 28 September 2022
Published 12 October 2022 Volume 2022:16 Pages 3369—3380
DOI https://doi.org/10.2147/OPTH.S376447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Adrianna D Jensen,1 Kamil Taneja,1,2 Meleha T Ahmad,1,3 Fasika A Woreta,1 Fatemeh Rajaii1
1Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Renaissance School of Medicine, Stony Brook University, Stony Brook, NY, USA; 3Department of Ophthalmology, University of California San Francisco, San Francisco, CA, USA
Correspondence: Fatemeh Rajaii, Wilmer Eye Institute, Johns Hopkins University School of Medicine, 600 North Wolfe Street, Maumenee 505, Baltimore, MD, 21287, USA, Tel +1-410-955-1112, Fax +1-410-614-9987, Email [email protected]
Purpose: To determine the incidence, characteristics, and costs associated with orbital hemorrhages presenting to US EDs.
Patients and Methods: This was a retrospective, longitudinal study of the Nationwide Emergency Department Sample, 2006 to 2018. Medical records from patients presenting to participating hospital-owned EDs and diagnosed with primary or secondary orbital hemorrhage were examined to determine incidence, demographics, clinical characteristics, mechanism, disposition and related risk factors, and costs.
Results: From 2006 to 2018, an estimated 20,762 US ED visits included an orbital hemorrhage diagnosis. Most primary diagnosis patients were elderly (35%) and male (51%), and incidence increased from 1.1 (95% CI: 0.8– 1.4) to 3.1 per million (95% CI: 2.5– 3.7, p < 0.0001). Fall was the most common mechanism (21.6%), particularly among the elderly (39.9%). Fall-related diagnoses increased from 0.03 (95% CI: − 0.01– 0.07) to 1.0 per million (95% CI: 0.7– 1.3, p < 0.0001), while overall falls increased by only 7%. Assault-related orbital hemorrhage increased from 0.1 (95% CI: 0.0– 0.2) to 0.6 per million (95% CI: 0.4– 0.7, p < 0.0001), while overall assaults decreased by 22%. Annual total ED costs increased from $463,220 (95% CI: 233,993– 692,446) to $6,117,320 (95% CI: 4,665,403– 7,569,237, p < 0.001). Inpatient admission was uncommon (9.0%), but related costs totaled $18.9 million (95% CI: 13.3– 24.5). Odds of admission were lower in fall- and objects-related injuries and higher with certain concurrent injuries.
Conclusion: Orbital hemorrhages are becoming more frequent and costly. A disproportionately large increase in fall- and assault-related diagnoses highlights the need for targeted injury prevention strategies to reduce cost and morbidity.
Keywords: orbital trauma, ocular trauma, epidemiology, cost
Introduction
Most literature on orbital hemorrhage (OH) concentrates on orbital compartment syndrome, which can cause irreversible vision loss after just 100–120 minutes1–3 by decreased perfusion and direct compression.4 Fortunately, the existing literature on OH suggests that this potentially blinding condition occurs relatively infrequently, found in only 0.45–3.6% of orbital fracture and trauma patients.3,5,6 Incidence in post-operative fracture repair has been reported at an even lower rate.7 OHs can also occur spontaneously, generally in patients with predisposing anatomical abnormalities; however, these cases are rare.8 Orbital hemorrhage can be diffuse, either intraconal and/or extraconal, or localized as in subperiosteal hemorrhage. Bleeding diatheses (primary or drug-induced), post-adnexal (blepharoplasty, especially if patient is on anticoagulant or antiplatelet agents) or sinus surgery, and rarely severe Valsalva (eg childbirth) are minor causes of OH.8 In contrast, most OHs occur in male trauma patients, most commonly related to assault, motor vehicle accident, or fall.5,6,9
The present literature on OH is based on either single institution samples or a systematic review of the literature, both of which are inherently limited and subject to bias. We are unaware of previous reports of true national-level investigation in the United States (US) or elsewhere regarding the incidence, characteristics, and cost of orbital hemorrhage diagnoses and could find no references involving a nationwide investigation in a computerized search (PubMed, Google Scholar). Noting the pattern of increasing cost and incidence of orbital fractures,10 there exists a significant chance that the same pattern exists for orbital hemorrhages. Physicians must be aware of the costs incurred by this condition and the factors playing into these costs as the first step in identifying ways to mitigate economic burden in an already overdrawn US healthcare economy. An understanding of OH characteristics and incidence would also help physicians to identify which preventive measures may be most helpful to decrease patient morbidity.
Although eye injuries are often addressed by outpatient ophthalmologists, most eye and orbital injuries are treated first in emergency departments (EDs).11 We utilized a nationally representative sample of ED visits to examine the incidence, characteristics, and cost of OHs presenting to EDs across the US over a 13-year period.
Materials and Methods
Study Design
We conducted a retrospective, longitudinal study using the National Emergency Department Sample (NEDS) to identify all ED visits in the sample from 2006 to 2018 with a diagnosis of OH, which were then examined for main outcome measures of incidence, demographics, clinical characteristics, mechanism, disposition and related risk factors, and cost. International Classification of Diseases [ICD] codes used to isolate these cases are included in Supplementary Table S1 (table detailing ICD codes). External cause of injury codes were used to categorize mechanism of injury and are detailed in Supplementary Table S2 (table detailing cause of injury codes). The Current Procedural Terminology (CPT), ICD-9 procedure, and ICD-10 procedure codes for lateral canthotomy used to ascertain if this procedure was performed are detailed in Supplementary Table S3 (table detailing lateral canthotomy procedure codes). ED cost was defined as the total charge to the patient for the ED visit, whereas inpatient cost was defined as the total of hospital charges for an inpatient stay.
Institutional Review Board approval was obtained prospectively (exempt status given de-identified database, Johns Hopkins Medicine IRB). This study adheres to the tenets of the Declaration of Helsinki and is also in accordance with HIPAA regulations. The NEDS does not contain direct patient identifiers, so informed consent was not required. To maintain adherence with the Healthcare Cost and Utilization Project data user agreement, estimates for any characteristics with 10 or fewer visits are not reported here to maintain patient confidentiality.
Data Set
The Nationwide Emergency Department Sample (NEDS) is the US’ largest all-payer ED database, developed as part of the Healthcare Cost and Utilization Project and sponsored by the US Federal Agency for Healthcare Research and Quality. This database is used to calculate national estimates of ED visits and represents a stratified sample consisting of over 25–30 million ED visits annually from nearly 1000 hospital-owned EDs in the US. To calculate national estimates, sample data are weighted to reflect the portion of all hospital-reported EDs in the AHA Annual Survey Database that they compose. Stratification is based on geographic region, trauma designation, urban versus rural location, teaching status, and hospital control/ownership. Patient characteristics and diagnoses (using ICD-9 from 2006 through September 30, 2015 and ICD-10 from October 1, 2015 onward) are included in the database. The primary diagnosis for an encounter is the diagnosis primarily responsible for presentation to care, while secondary diagnoses are any other accompanying diagnoses. More information can be found at https://www.hcup-us.ahrq.gov/db/nation/neds/nedsdbdocumentation.jsp.
Data Collection and Analysis
National estimates were calculated using NEDS-supplied sampling weights. US Census Bureau data were used to calculate incidence of orbital hemorrhage. Age was grouped into the following categories: children (10 years and younger), adolescents (11–20 years), young adults (21–44 years), adults (45–64 years), and elderly (65 years and older). Descriptive statistics were calculated for hospital characteristics, patient demographics, and concomitant ocular/facial injuries. ED and inpatient charges were inflation-adjusted based on the 2021 US dollar using the Consumer Price Index for Hospital Services from the US Bureau of Labor Statistics. Linear regression was used to estimate trends in incidence and mean ED charge per visit. Univariate and multivariate logistic regression were used to assess factors associated with inpatient admission. Stata version 15 (StataCorp LLC, College Station, Texas, USA) was used for all statistical analyses.
Results
Incidence
Estimated incidence of ED visits with a primary or secondary OH diagnosis increased by more than 4.3-fold from 2.7 per million (95% confidence interval [CI]: 2.2–3.3) in 2006 to 11.8 per million (95% CI: 10.4–13.1, p<0.0001) in 2018. Primary OH diagnoses alone increased about 2.9 times, from 1.1 per million (95% CI: 0.8–1.4) in 2006 to 3.1 per million (95% CI: 2.5–3.7, p<0.0001). Total OH diagnoses increased most precipitously from 2015 to 2016, jumping 74% from 6.0 per million (95% CI: 5.0–7.0) to 10.5 per million (95% CI: 8.9–12.0, p<0.0001). Over the same interval, primary OH diagnoses increased 116% from 1.43 per million (95% CI: 1.1–1.76) to 3.1 per million (95% CI: 2.5–3.7, p<0.0001) (Figure 1A).
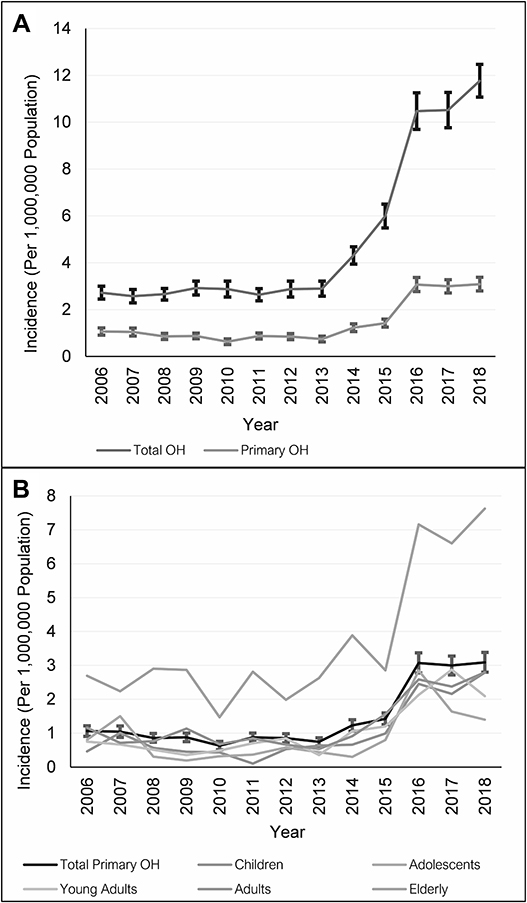 |
Figure 1 Orbital hemorrhage diagnoses in US emergency departments. (A) This plot displays the incidence of emergency department visits with orbital hemorrhage diagnoses (total and primary) from 2006–2018 (with standard error). (B) This plot displays the age-specific incidence of emergency department visits with primary orbital hemorrhage diagnoses from 2006–2018 (with standard error for total incidence). |
All groups but adolescents had a statistically significant increase in age-specific primary OH incidence over the study period (Figure 1B). Primary OH increased about six-fold in children (0.5 [95% CI: 0.0–0.9] to 2.8 per million [95% CI: 1.7–3.9, p<0.0001]), and between two- to three-fold in young adults, adults, and the elderly. There was otherwise a trend toward fewer orbital hemorrhages in January and February in any given year (data not shown), though this did not reach statistical significance.
Demographics
The mean age of OH patients presenting to the ED was 49.2 (standard error = 0.8) years. The elderly made up the largest proportion of OH patients (33.6%) (Table 1). The majority of OH patients were male (51.0%), though elderly patients were predominantly female (64.0%) (Table 1). The most common primary expected payer overall was Medicare, with 85.0% of the elderly covered in this way, though a significant portion of young adults (33.1%) were self-pay (Table 1). These and all demographic results can be examined in Table 1.
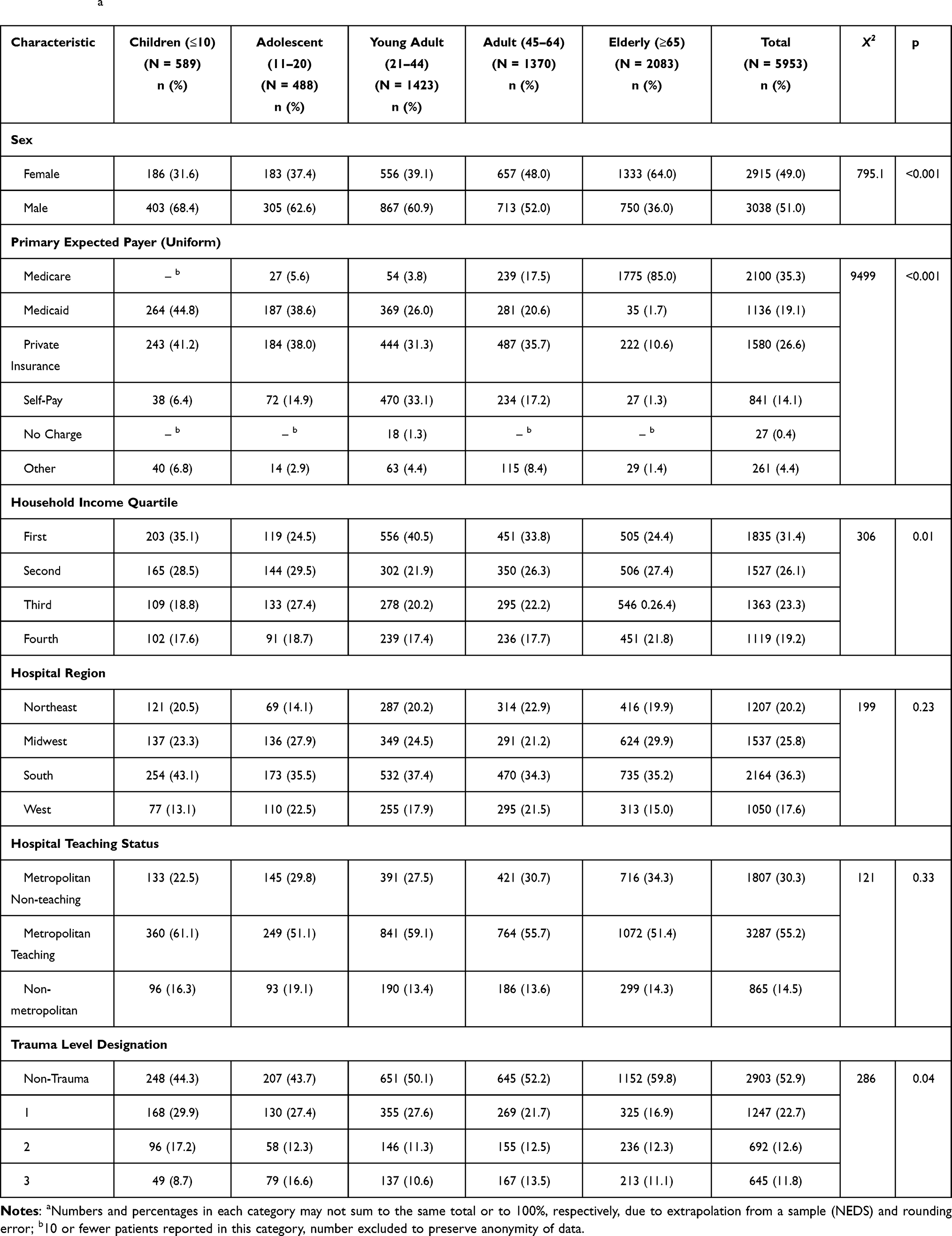 |
Table 1 Demographics of National Emergency Department Sample (NEDS) Patients with Primary Diagnosis of Orbital Hemorrhage 2006 to 2018a |
Mechanism of Injury
The most common overall mechanism of injury reported was fall (21.6%), followed by assault (15.9%). Young adults and the elderly were overwhelmingly injured by assaults (40%) and falls (40%), respectively (Supplementary Figure S1, figure detailing mechanisms of injury across age groups). All examined mechanisms increased in incidence, with fall-related OHs increasing to the greatest extent (Supplementary Figure S2, figure detailing overall incidence of mechanisms of injury). While the incidence of assault-related OHs increased by nearly 7-fold from less than 0.1 (95% CI: 0.0–0.2) to 0.6 per million (95% CI: 0.4–0.7, p<0.0001), fall-related OHs increased by over 34-fold from 0.03 (95% CI: −0.01–0.07) to 1.0 per million (95% CI: 0.7–1.3, p<0.0001) (Figure 2). From 2006 to 2018, overall fall incidence in the NEDS increased by only 7% from 276.6 (95% CI: 264.9–288.3) to 295.0 per 10,000 population (95% CI: 281.1–309.2, p=0.0015). Overall assault incidence decreased by 22% from 43.3 (95% CI: 40.6–46.0) to 33.7 per 10,000 population (95% CI: 31.5–35.9, p<0.001) (Supplementary Figure S3, figure detailing overall assault and fall incidence 2006–2018).
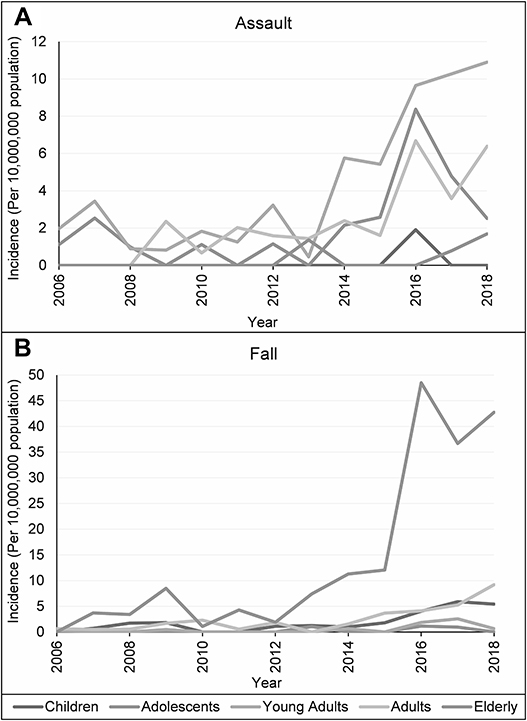 |
Figure 2 Assault- and fall-related orbital hemorrhage diagnoses. This plot displays the age-specific incidence of (A) assault-related and (B) fall-related injury leading to primary orbital hemorrhage from 2006 to 2018. |
Associated Ocular Injuries and Procedures
The most common primary OH-associated ocular injury was contusion (6.3%), with nasal fracture nearly as common in young adults (5.7%) and low vision notable in the elderly (4.0%) (Supplementary Table S4, table detailing most common associated ocular injuries across age groups). Lateral canthotomy was coded in only 3.3% of primary OH cases and 3.8% of total OH cases. However, 20.9% of admitted primary OH cases had undergone lateral canthotomy, and odds of admission increased by over 16-fold if this procedure was performed (Odds Ratio [OR] 16.07, 95% CI: 8.01–32.26).
ED Costs
Total inflation-adjusted ED cost for primary OH cases from 2006 to 2018 was $24.8 million (95% CI: 22.0–27.7), with annual adjusted ED costs increasing over 13-fold from $463,220 (95% CI: 233,993–692,446) to $6,117,320 (95% CI: 4,665,403–7,569,237, p<0.001) (Figure 3A). Mean inflation-adjusted per-visit ED cost increased slightly less than 4-fold, from $1,883 (95% CI: 1,143–2,623) to $6,974 (95% CI: 5,861–8,087, p<0.0001) (Figure 3B).
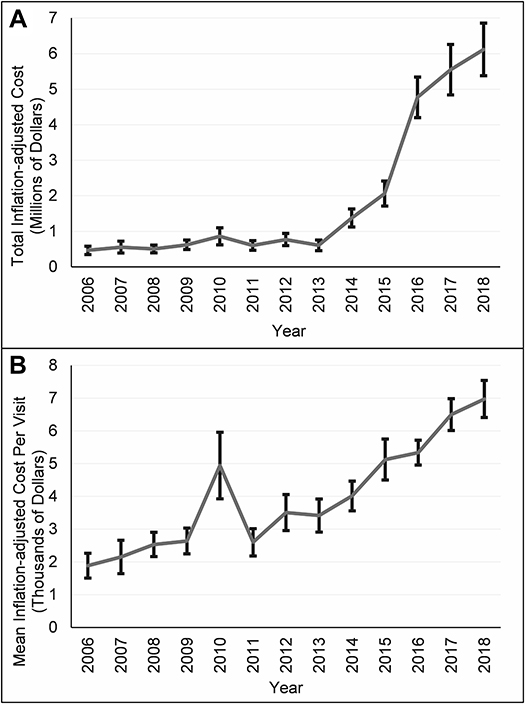 |
Figure 3 Emergency department costs related to orbital hemorrhage diagnoses. (A) This plot displays the estimated total annual inflation-adjusted emergency department costs for visits with a primary orbital hemorrhage diagnosis from 2006 to 2018 (with standard error). (B) This plot displays the mean per-visit inflation-adjusted ED cost for visits with a primary OH diagnosis from 2006 to 2018 (with standard error). |
Disposition and Factors Associated with Admission
The vast majority (80.7%) of primary OH patients were seen in and discharged from the ED (routine disposition). Only 9.0% were admitted to the presenting hospital. Though admission was relatively rare, the total inflation-adjusted inpatient charge for primary OH 2006–2018 was notable at $18.9 million (95% CI: 13.3–24.5), with mean inpatient cost per patient of $35,726 (95% CI: 28,193–43,258).
The largest fraction of admitted patients were elderly, with low admission rates particularly among younger patients (Table 2). Both fall- (OR 0.45, p=0.009) and object-related (OR 0.24, p=0.015) injuries were associated with decreased odds of admission, while long-term anticoagulant or antiplatelet use was associated with increased odds (OR 2.75, p=0.001), as were certain concurrent injuries (Table 2).
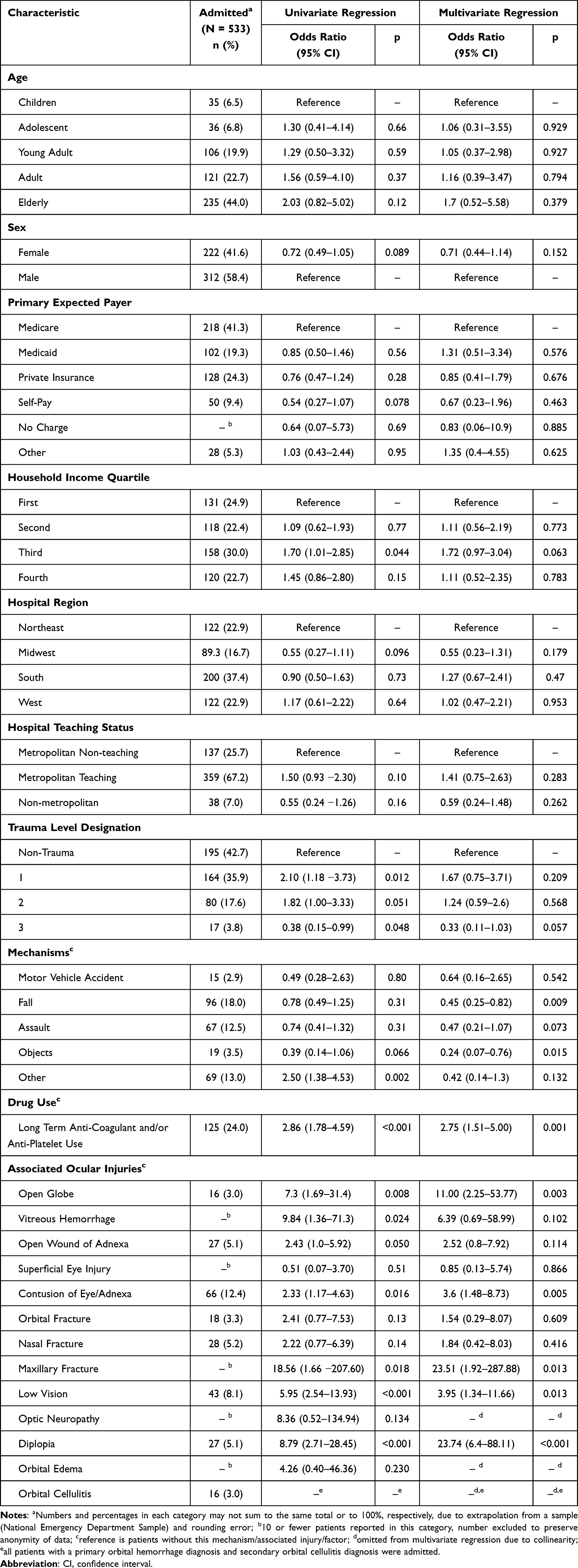 |
Table 2 Risk Factors Associated with Admission in Primary Orbital Hemorrhage |
Discussion
Orbital hemorrhage is a potentially devastating ophthalmic emergency that may require urgent intervention in the rare case of compartment syndrome. Despite its clinical importance, there is little data assessing national epidemiologic trends in OH. Our study used a nationally representative sample to investigate incidence, demographics, clinical characteristics, and economic burden associated with OHs presenting to US EDs from 2006 to 2018. Key findings were a rising incidence of OH, particularly those caused by fall and assault, as well as substantial increases in inflation-adjusted ED costs. A minority of patients with primary OH had secondary injuries, required canthotomy/cantholysis, or warranted hospital admission.
Although incidence and cost of OH visits increased substantially between 2006 and 2018, the greatest increase occurred from 2015 to 2016. This sharp increase coincided with the switch from ICD-9 to ICD-10, which may have induced a shift toward more complete coding, possibly because of greater number and detail of codes in the ICD-10.12 Moreover, seasonality of OH cases, though not statistically significant in our investigation, is consistent with lower volumes of traumatic injuries13 and orbital fractures10 observed in winter months.
Mean cost per primary OH ED visit increased fairly steadily over the study period, exceeding the approximately 68% increase in overall national health expenditures over the same period.14 This relatively greater increase in spending on OH could partly stem from frequent use of imaging in trauma evaluations. The temporary spike in cost per visit in 2010 did not coincide with any major shifts in coding or treatment and remains unexplained. Conversion to ICD-10 did not acutely affect payment per ED visit, consistent with a prior report analyzing effects of this conversion on an outpatient ophthalmology practice.15
The distribution of demographics and mechanisms of injury in our analysis of OH in the NEDS was consistent with data previously reported in patients with OH and orbital fractures.5,6,9,16 In particular, a recent analysis of orbital floor fractures found a high rate of orbital trauma from falls in the elderly, particularly elderly women, and we noted a similar trend.10 This trend is consistent with the higher rate of non-fatal, unintentional falls in elderly women compared to elderly men.17 We also observed a precipitous increase in fall- and assault-related primary OHs. The increase in fall-related primary OHs began prior to conversion from ICD-9 to ICD-10 and was 17 times higher than the 2-fold increase in fall-related orbital floor fractures from 2006 to 2017 noted by Iftikhar et al.10 The rise in fall-related OH was spearheaded by the elderly, though this increase is only partially accounted for by the 34% increase in the US elderly population from 2007 to 2017.18 Fall-related injury, therefore, represents an increasing threat to the elderly,19 perhaps because of increasing lifespans20 and more active lifestyles.21 Comorbid diabetes, heart failure, and/or systemic hypotension in elderly patients increase this threat even further, as these patients would be at a greater risk to develop ocular ischemia as a complication of orbital hemorrhage. As such, fall prevention is an area in particular need of strategies to mitigate injury. Seeing as the elderly are more likely to fall and most likely to be admitted with OH, efforts to decrease falls would cut not only ED costs, but also inpatient costs.
Though the elderly should be a major focus of fall prevention, this age group made up a variable but not growing fraction of the age-specific incidence of fall-related OH throughout the study. Therefore, these injuries are increasing for other age groups as well. Also quite concerning about the rate of increase of fall-related OH is how dramatically it outpaced the rate of increase in incidence of falls in general (only 7%) during the study period, which may be related to known increases in anticoagulant use leading to increased severity of bleeding injuries.22,23 Increasing anticoagulant use may also at least in part explain the much greater increase in fall-related OHs than fractures, as mentioned above. Many investigators have examined possible interventions to reduce falls, including vitamin D supplementation,24 exercise with or without additional education or martial arts training,25,26 interdisciplinary assessment and referral,27 environmental modification,28 addressing physical issues (vision,29 foot care30), and dedicated medication review.31 These methods have individually demonstrated efficacy, but results in meta-analyses are mixed.32,33 Studies on fall prevention are also far from standardized, which remains an area for much needed improvement in future investigations.
Otherwise, assault as an etiology of OH increased nearly 7-fold in incidence from 2006 to 2018, which was out of proportion to changes in assault incidence noted in the literature34,35 and estimated from the NEDS database (22% decrease) over the same period. This disparity may suggest that even if assaults are decreasing, at least a subset of these are becoming more violent. However, increased incidence could otherwise be an artifact of a known increased use of CT imaging in the ED36 or an artifact of more complete coding. As with falls, many groups have examined different programs to reduce violence, especially among youth. Effective methods have included mentorship;37 information sharing programs;38 brief hospital-based interventions;39 case management;40 and pre-school programs providing family support and education.41 Though there is no consensus currently on the best method to prevent youth violence, it appears that more effective strategies in general involve various stakeholders, including youth, community, school, family, etc.42 One group has also demonstrated the likely cost-effectiveness of a hospital-based intervention program, which when combined with our results provides quite an impetus for broad initiation of effective prevention strategies.43
Regarding hospital admission, patients with long-term anticoagulant/antiplatelet use were significantly more likely to be admitted, perhaps because of more severe bleeding, which aligns with past reports of similar rate of bleeding injury for patients regardless of anticoagulant status but a greater mortality from bleeding in the anticoagulated.22 This trend reinforces the importance of fall prevention to decrease healthcare costs, especially as the use of oral anticoagulants has increased.22 Subjects on oral anticoagulants also run an additional risk for prolonged duration of a compartment syndrome, should this severe complication arise, as active orbital bleeding may not stop. The risk of repeat falls should be weighed against the risk of stroke when deciding to continue these medications after a fall,22 and in patients where novel anticoagulant use is clinically appropriate, use of proper doses of dabigatran or apixaban has demonstrated a possibly lower risk for intracranial hemorrhage than warfarin and should be considered.44 Furthermore, certain concomitant injuries were associated with greater odds of admission, which is not surprising as a more severe mechanism necessitating a higher level of care is likely to cause other injuries than just OH. Fall- and object-related primary OHs were less likely to be admitted, which may be the case because patients who fell or were injured by objects in a severe enough manner to be admitted also had other more severe diagnoses than OH that were instead coded as the primary diagnosis.
Moreover, lateral canthotomy was coded at an overall low but variable rate. Prior work has suggested that orbital hemorrhage occurs relatively infrequently, at a rate of 0.45–3.6% in orbital fracture/trauma,3,5,6 of which only a fraction lead to compartment syndrome. As such, it is not surprising that our observed rate of lateral canthotomy is rather low. However, the possibility for underestimation exists in cases in which the anatomic cause of the hemorrhage (for instance, facial fracture) or a more serious nearby injury takes precedence as the primary diagnosis. Regardless, lateral canthotomy significantly increased odds of admission, consistent with greater injury severity one would expect to lead to vision-threatening hemorrhage.
In conclusion, we characterized demographics, cost, and inpatient admission trends in patients presenting to EDs across the US with OH diagnoses, which though it was retrospective allowed for a larger and more broadly representative sample than could likely be organized prospectively on a national level. Strengths of our study include our use of a nationally representative sample over more than a decade and inclusion of both primary and secondary OH diagnoses. Our study is limited by the potential for coding errors or omissions, which could limit our identification of all OH cases. Also, the coding artifact of the ICD-9 to ICD-10 transition is not insignificant, but the increase in orbital hemorrhage incidence over the study period had begun even before this transition and was far more than seen, for instance, with orbital fractures in another examination of the NEDS.10 As such, our conclusions do not appear to be critically limited by coding artifact, and our finding of a rising prevalence of OH emphasizes the continued importance of recognition and treatment of this entity by ophthalmologists and emergency medicine physicians alike. The notable increases in fall- and assault-related OHs, along with exponentially rising costs, further inform public health efforts for the mitigation of facial trauma.
Acknowledgment
The authors would like to acknowledge Joseph Canner, BS, MHS (Baltimore, MD) for his assistance in study inception and IRB procurement.
Disclosure
Fatemeh Rajaii reports being a consultant for, personal fees from, and previous stock ownership in Horizon Therapeutics outside the submitted work. The authors report no other potential conflicts of interest in this work.
References
1. Hayreh S, Weingeist T. Experimental occlusion of the central artery of the retina. IV: retinal tolerance time to acute ischaemia. Br J Ophthalmol. 1980; 64: 818–825. 11 doi:10.1136/bjo.64.11.818
2. Larsen M, Wieslander S Acute orbital compartment syndrome after lateral blow-out fracture effectively relieved by lateral cantholysis. Acta Ophthalmol Scand. 1999; 77(2): 232–233. doi:10.1034/j.1600-0420.1999.770225.x
3. Ballard S, Enzenauer R, O’Donnell T, Fleming J, Risk G, Waite A Emergency lateral canthotomy and cantholysis: a simple procedure to preserve vision from sight threatening orbital hemorrhage. J Spec Oper Med Peer Rev J SOF Med Prof. 2009; 9(3): 26–32. doi:10.55460/1CLD-XJUV
4. Neuhaus RW Orbital complications secondary to endoscopic sinus surgery. Ophthalmology. 1990; 97(11): 1512–1518. doi:10.1016/S0161-6420(90)32383-7
5. Fattahi T, Brewer K, Retana A, Ogledzki M. Incidence of retrobulbar hemorrhage in the emergency department. J Oral Maxillofac Surg. 2014;72(12):2500–2502.
6. Kondoff M, Nassrallah G, Ross M, Deschênes J. Incidence and outcomes of retrobulbar hematoma diagnosed by computed tomography in cases of orbital fracture. Can J Ophthalmol. 2019;54(5):606–610.
7. Ord RA. Post-operative retrobulbar haemorrhage and blindness complicating trauma surgery. Br J Oral Surg. 1981;19(3):202–207.
8. Sullivan TJ, Wright JE. Non-traumatic orbital haemorrhage. Clin Experiment Ophthalmol. 2000;28(1):26–31.
9. Christie B, Block L, Ma Y, Wick A, Afifi A. Retrobulbar hematoma: a systematic review of factors related to outcomes. J Plast Reconstr Aesthet Surg. 2018;71(2):155–161.
10. Iftikhar M, Canner JK, Hall L, Ahmad M, Srikumaran D, Woreta FA Characteristics of orbital floor fractures in the United States from 2006 to 2017. Ophthalmology. 2021; 128(3): 463–470. doi:10.1016/j.ophtha.2020.06.065
11. McGwin G Rate of eye injury in the United States. Arch Ophthalmol. 2005; 123(7): 970. doi:10.1001/archopht.123.7.970
12. National Center for Health Statistics. International classification of diseases, (ICD-10-CM/PCS) Transition - Background. Available from: https://www.cdc.gov/nchs/icd/icd10cm_pcs_background.htm.
13. Bhattacharyya T, Millham FH Relationship between weather and seasonal factors and trauma admission volume at a Level I trauma center. J Trauma Inj Infect Crit Care. 2001; 51(1): 118–122. doi:10.1097/00005373-200107000-00019
14. Centers for Medicare & Medicaid Services. National health expenditure accounts: table 01 National Health expenditures; aggregate and per capita amounts. Available from: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.
15. Hellman JB, Lim M, Leung K, Blount C, Yiu G The impact of conversion to International Classification of Diseases, 10th revision (ICD-10) on an academic ophthalmology practice. Clin Ophthalmol. 2018; 12: 949–956. doi:10.2147/OPTH.S161742
16. MacKinnon CA, David DJ, Cooter RD Blindness and severe visual impairment in facial fractures: an 11 year review. Br J Plast Surg. 2002; 55(1): 1–7. doi:10.1054/bjps.2001.3728
17. Stevens JA Gender differences for non-fatal unintentional fall related injuries among older adults. Inj Prev. 2005; 11(2): 115–119. doi:10.1136/ip.2004.005835
18. Administration for Community Living. 2018 profile of older Americans. Available from: https://acl.gov/sites/default/files/Aging%20and%20Disability%20in%20America/2018OlderAmericansProfile.pdf. Accessed April 21, 2021.
19. Hartholt KA, Stevens JA, Polinder S, van der Cammen TJM, Patka P Increase in fall-related hospitalizations in the United States, 2001–2008. J Trauma Inj Infect Crit Care. 2011; 71(1): 255–258. doi:10.1097/TA.0b013e31821c36e7
20. Vincent GK, Velkoff VA The next four decades: the older population in the United States: 2010 to 2050. Available from: https://www.aarp.org/content/dam/aarp/livable-communities/old-learn/demographics/the-next-four-decades-The-older-population-in-The-united-states-2010-2050-aarp.pdf.
21. Freedman VA, Martin LG, Schoeni RF Recent trends in disability and functioning among older adults in the United States: a systematic review. JAMA. 2002; 288(24): 3137–3146. doi:10.1001/jama.288.24.3137
22. Chiu AS, Jean RA, Fleming M, Pei KY Recurrent falls among elderly patients and the impact of anticoagulation therapy. World J Surg. 2018; 42(12): 3932–3938. doi:10.1007/s00268-018-4728-1
23. Barnes GD, Lucas E, Alexander GC, Goldberger ZD National trends in ambulatory oral anticoagulant use. Am J Med. 2015; 128(12): 1300–5.e2. doi:10.1016/j.amjmed.2015.05.044
24. Smith LM, Gallagher JC, Suiter C Medium doses of daily vitamin D decrease falls and higher doses of daily vitamin D3 increase falls: a randomized clinical trial. J Steroid Biochem Mol Biol. 2017; 173: 317–322. doi:10.1016/j.jsbmb.2017.03.015
25. Smulders E, Weerdesteyn V, Groen BE, et al. Efficacy of a short multidisciplinary falls prevention program for elderly persons with osteoporosis and a fall history: a randomized controlled trial. Arch Phys Med Rehabil. 2010; 91(11): 1705–1711. doi:10.1016/j.apmr.2010.08.004
26. Midha D, Uttam M, Jasim H, Kumar SP Efficacy of education with balance exercise program in improving balance and reducing the fear of falls in elderly: a randomized clinical trial. IJHRS. 2015; 4(1): 27–36. doi:10.5455/ijhrs.000000075
27. Close J, Ellis M, Hooper R, Glucksman E, Jackson S, Swift C Prevention of falls in the elderly trial (PROFET): a randomised controlled trial. Lancet. 1999; 353(9147): 93–97. doi:10.1016/S0140-6736(98)06119-4
28. Tchalla AE, Lachal F, Cardinaud N, et al. Efficacy of simple home-based technologies combined with a monitoring assistive center in decreasing falls in a frail elderly population (results of the Esoppe study). Arch Gerontol Geriatr. 2012; 55(3): 683–689. doi:10.1016/j.archger.2012.05.011
29. Haran MJ, Cameron ID, Ivers RQ, et al. Effect on falls of providing single lens distance vision glasses to multifocal glasses wearers: VISIBLE randomised controlled trial. BMJ. 2010; 340: c2265. may25 1 doi:10.1136/bmj.c2265
30. Spink MJ, Menz HB, Fotoohabadi MR, et al. Effectiveness of a multifaceted podiatry intervention to prevent falls in community dwelling older people with disabling foot pain: randomised controlled trial. BMJ. 2011; 342: d3411. doi:10.1136/bmj.d3411
31. Pit SW, Byles JE, Henry DA, Holt L, Hansen V, Bowman DA A quality use of medicines program for general practitioners and older people: a cluster randomised controlled trial. Med J Aust. 2007; 187(1): 23–30. doi:10.5694/j.1326-5377.2007.tb01110.x
32. Morello RT, Soh SE, Behm K, et al. Multifactorial falls prevention programmes for older adults presenting to the emergency department with a fall: systematic review and meta-analysis. Inj Prev. 2019; 25(6): 557–564. doi:10.1136/injuryprev-2019-043214
33. El-Khoury F, Cassou B, Charles MA, Dargent-Molina P The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: systematic review and meta-analysis of randomised controlled trials. BMJ. 2013; 347: f6234. doi:10.1136/bmj.f6234
34. Truman JL, Langton L. Bureau of Justice Statistics. criminal victimization; 2014. Available from: https://www.bjs.gov/content/pub/pdf/cv14.pdf.
35. Morgan RE, Oudekerk BA. Bureau of justice statistics. Criminal victimization; 2018. Available from: https://www.bjs.gov/content/pub/pdf/cv18.pdf.
36. Bellolio MF, Heien HC, Sangaralingham LR, et al. Increased computed tomography utilization in the emergency department and its association with hospital admission. West J Emerg Med. 2017; 18(5): 835–845. doi:10.5811/westjem.2017.5.34152
37. Jones V, Becote-Jackson M, Parnham T, Lewis Q, Ryan LM. Violence prevention through mentoring for youth with emergency department treated peer assault injuries. J Pediatr. 2021;6:e100064.
38. Florence C, Shepherd J, Brennan I, Simon T Effectiveness of anonymised information sharing and use in health service, police, and local government partnership for preventing violence related injury: experimental study and time series analysis. BMJ. 2011; 342: d3313. doi:10.1136/bmj.d3313
39. Walton MA, Chermack ST, Shope JT, et al. Effects of a brief intervention for reducing violence and alcohol misuse among adolescents: a randomized controlled trial. JAMA. 2010; 304(5): 527–535. doi:10.1001/jama.2010.1066
40. Zun LS, Downey L, Rosen J. The effectiveness of an ED-based violence prevention program. Am J Emerg Med. 2006;24:8–13.
41. Weikart DP, Berrueta-Clement JR, Schweinhart L, Barnett WS, Epstein AS. Changed lives: the effects of the Perry preschool program on youths through age 19. Monographs of the High/Scope educational research foundation, number eight. Ypsilanti, MI: High/Scope Educational Research Foundation; 1984.
42. Mercy JA, Vivolo-Kantor AM. The center for disease control and prevention’s (CDC) youth violence prevention centers: paving the way to prevention. J Prim Prev. 2016;37(2):209–214.
43. Purtle J, Rich LJ, Bloom SL, Rich JA, Corbin TJ. Cost-benefit analysis simulation of a hospital-based violence intervention program. Am J Prev Med. 2015;48(2):162–169.
44. Vinogradova Y, Coupland C, Hill T, Hippisley-Cox J. Risks and benefits of direct oral anticoagulants versus warfarin in a real world setting: cohort study in primary care. BMJ. 2018;362:k2505.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.