")
Back to Journals » Infection and Drug Resistance » Volume 14
Inactivation of Clinically Frequently Used Antimicrobial Agents By BacT/ALERT FAN Plus and BACTEC Aerobic and Anaerobic Culture Media in Simulated Blood Cultures: First Comparative Evaluation in China Mainland
Authors Xu X, Wei Q, Wang Z, Yan J, Wang H, Xia Y
Received 3 November 2020
Accepted for publication 22 December 2020
Published 19 January 2021 Volume 2021:14 Pages 163—172
DOI https://doi.org/10.2147/IDR.S290222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiuyu Xu, Qiang Wei, Zhu Wang, Jie Yan, Huijuan Wang, Yun Xia
Department of Laboratory Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Yun Xia
Department of Laboratory Medicine, The First Affiliated Hospital of Chongqing Medical University, No. 1 Youyi Road, Yuzhong District, Chongqing 400016, People’s Republic of China
Tel/Fax +86-23-89012513
Email [email protected]
Purpose: To evaluate the antimicrobial inactivation capabilities of BacT/ALERT (FA Plus and FN Plus) and BACTEC (Plus Aerobic/F and Lytic/10 Anaerobic/F) media.
Patients and Methods: The inactivation capabilities of the commercial blood culture media were compared using 21 microorganism-antimicrobial combinations in simulated adult blood cultures.
Results: BacT/ALERT culture media demonstrated higher detection rates than the BACTEC culture media. The recovery rates of the aerobic bottles were 74/115 (64.3%) for FA Plus bottles and 64/115 (55.7%) for BACTEC Aerobic Plus bottles. The BacT/ALERT FAN Plus culture media exhibited a shorter time to detection (TTD). The TTD of FA Plus media was 14.7 h, 4.85 h shorter than the BACTEC Aerobic media (19.55 h), while the TTDs of FN Plus media and BACTEC Anaerobic media were 16.8 h and 18.4 h, respectively.
Conclusion: BacT/ALERT (FA Plus and FN Plus) media showed relative, but not absolute, advantages, as it had higher detection rates and shorter TTD and thus can be selectively applied to patients with prior use of antimicrobial agents before blood culture samples are taken.
Keywords: antimicrobial inactivation, blood culture, automated system, BacT/ALERT FAN plus media, comparative evaluation
Introduction
Accurate and timely diagnoses of bloodstream infections (BSIs) are crucial for the treatment and prognosis of BSI patients, as well as to decrease the associated high morbidity and mortality.1,2 As the gold standard of BSI detection, blood culture samples should be collected the first time patients are suspected to have sepsis, and before antimicrobial agents are given to improve the detection rate as much as possible. However, antimicrobials are often administered before blood culture samples are collected in the urgent septic conditions. It is reported that nearly half of inpatients are administered with antimicrobials before blood culture samples are collected.3 As a result, the time to detection (TTD) of the commercial automated blood culture systems may be significantly prolonged. Even worse, due to the antimicrobial activity in blood culture samples, microbial growth in blood culture bottles could be undetectable.4
Substances such as resin or charcoal which can absorb antimicrobial agents are added to some commercial blood culture media in order to minimize the inhibition of antimicrobials on microbial growth in blood culture.5 In 2013, BacT/ALERT FA Plus (aerobic) and FN Plus (anaerobic) bottles (bioMérieux) were developed to further improve the detection of microorganisms from sepsis patient samples. Until now, several blood culture simulation studies (involving blood culture bottles injected with whole blood, antimicrobial agents, and microorganisms) have compared the antimicrobial inactivation efficiency of BacT/ALERT FAN Plus media and BACTEC Plus media, including in both anaerobic and aerobic blood culture bottles.6,7 However, since the BacT/ALERT FAN Plus media was only recently approved in the Chinese mainland, data on the performance of antimicrobial agent inactivation of BacT/ALERT FAN Plus media from China mainland is not yet available.
In the present study, we aimed to evaluate the antimicrobial inactivation capabilities of BacT/ALERT FAN Plus media and BACTEC aerobic and anaerobic culture media by measuring the organism detection rate and TTD for several antimicrobial-microorganism combinations in simulated blood cultures. Specifically, the blood antimicrobial concentrations of patients with antimicrobial treatment were mimicked.
Patients and Methods
Ethics Clarification
No ethical review process was required for this simulated blood culture study, as it did not involve any animal or human experiments. In addition, as a simulated study, no specimens, microbial isolates, or any other materials from patients or healthy human bodies were involved. All the materials used in this study, including reference ATCC microorganism strains, antimicrobial agents, and horse blood were commercially available and purchased.
Blood Culture Media and Blood Culture Instrument
Resin-containing BacT/ALERT FA Plus (FA Plus) aerobic bottles, FN Plus (FN Plus) anaerobic bottles, and resin-free BacT/ALERT SA aerobic bottles and SN anaerobic bottles were applied to the automated BacT/ALERT 3D blood culture system. Resin-containing BD BACTEC Aerobic/F Plus (BD Aerobic Plus) bottles and resin-free Lytic/10 Anaerobic/F (BD Lytic/10 Anaerobic) bottles were applied to the automated BD BACTEC FX blood culture system.
Microorganisms
Microorganism species were chosen according to the frequency of recovery from positive blood cultures in our lab, and the following reference ATCC microorganism strains were used: Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, Bacteroides fragilis ATCC 25285, methicillin-susceptible Staphylococcus aureus (MSSA) ATCC 29213, Enterococcus faecalis ATCC 29212, and Candida parapsilosis ATCC 22019. Strains were stored in skim milk and frozen at −80°C until use. Before being spiked into blood culture bottles, strains were subcultured twice on Columbia blood agar plates, and incubated at 37°C overnight. Minimum inhibitory concentrations (MICs) were tested by the Clinical Laboratory Standards Institute (CLSI) broth microdilution method in triplicate, and susceptibility categorization was determined based on the latest CLSI breakpoints (Table 1).8 Colonies from Columbia blood agar plates were suspended in phosphate-buffered saline, and serial dilutions of each organism were prepared to a target concentration of 100 CFU/mL, and 0.1 mL of the final dilutions were plated on the Columbia blood agar plate and incubated at 37°C overnight to verify the CFUs.
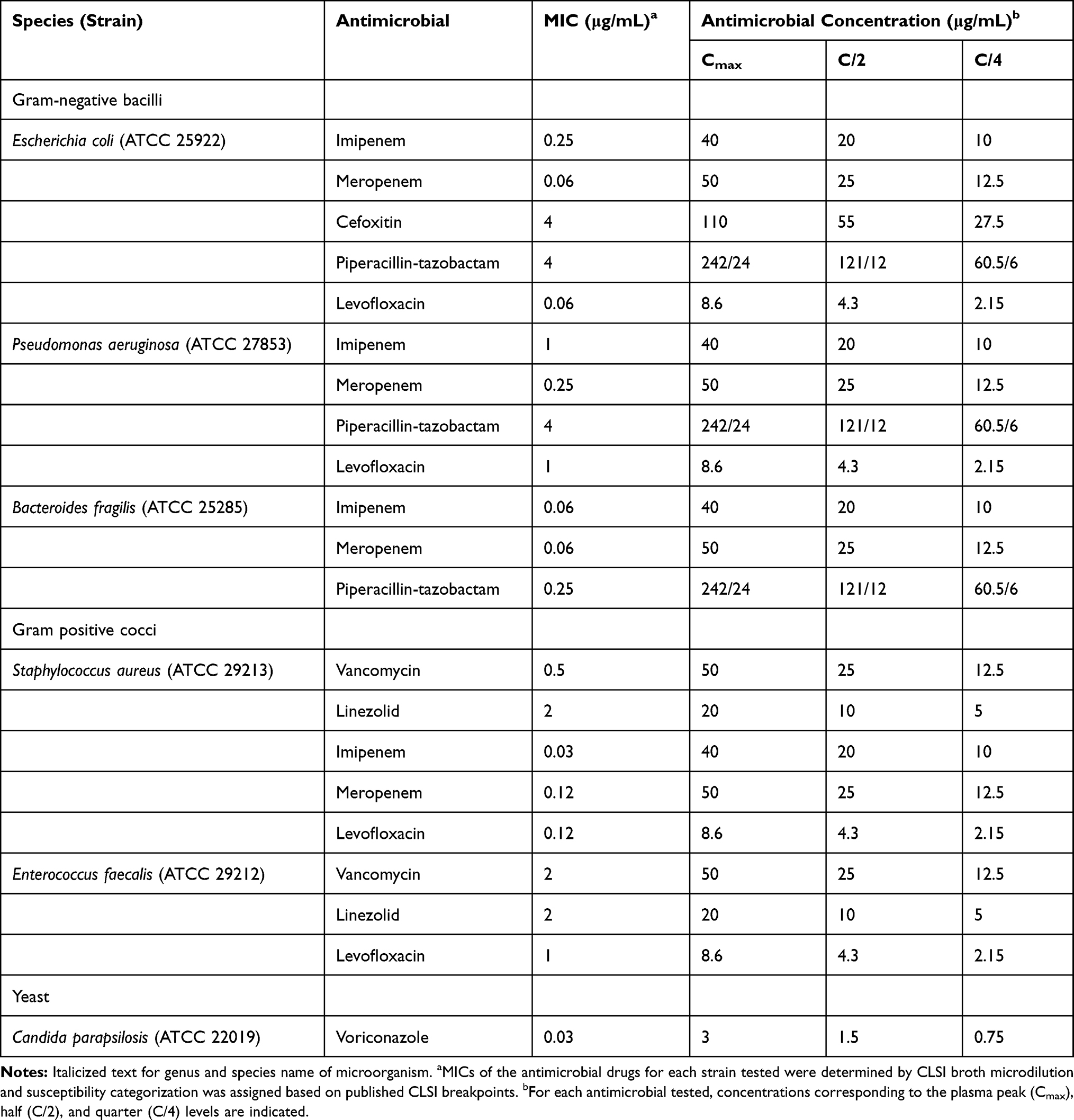 |
Table 1 Microorganism and Antimicrobial Combinations Tested by the Simulated Adult Blood Culture Model |
Antimicrobials
In this study, eight of the most commonly used antimicrobial agents to treat specific blood stream infections were chosen. The commercially available standards of meropenem, imipenem, levofloxacin, cefoxitin, piperacillin-tazobactam, vancomycin, voriconazole (Meilunbio, China), and linezolid (Sigma, USA) were reconstituted according to the manufacturer’s instructions. The peak serum concentration (Cmax), achieved according to standard dosing of the antimicrobial under the condition of a 70-kg adult with normal renal function, was used to simulate patient blood levels (Table 1). If no growth was detected, antimicrobials were then injected at concentrations of C/2 and/or C/4 to obtain positive results in any culture system. Each antimicrobial agent was diluted in sterile water from stock solutions to ensure that 0.3 mL of the dilution contained the desired final antimicrobial concentration of a blood culture bottle.
Blood Culture Preparation
In our simulated blood culture research, each blood culture bottle was spiked with 10 mL of sterile horse blood, 0.3 mL of microbial suspension (described above), and 0.3 mL of antimicrobial agent solution (described above) in turn. For each microorganism-antimicrobial combination, incubations were performed in quintuplicate for each type of blood culture media. Microorganisms were simultaneously spiked into aerobic and anaerobic bottles as pairs, except for P. aeruginosa and C. parapsilosis, which were only evaluated under aerobic conditions, and B. fragilis only tested under anaerobic conditions. To ensure the activities of the antimicrobials tested, for each microorganism-antimicrobial combination, triplicate BacT/ALERT resin-free aerobic and/or anaerobic bottles (SA/SN) were incubated with horse blood, antimicrobial solution at peak serum concentrations and bacterial suspension. In addition, a negative control (containing only horse-blood) and a positive control (antimicrobial-free) were set for each combination. The negative controls were used to confirm the sterility of the spiked horse blood, which were simultaneously incubated on Columbia blood agar plate and incubated at 37°C overnight. Subsequently, the spiked bottles were immediately loaded into the corresponding blood culture instrument and incubated until positive or negative signals were alarmed. A positive signal indicates the signal alarm given by the blood culture instrument when microbial growth was detected in any blood culture bottles loaded in the instrument, whereas a negative signal was observed when no microbial growth was detected up to 5 days (120 h). The negative and positive signals as culture endpoints were used to calculate the time to detection (TTD) of each blood culture bottle. After this, broth from blood culture bottles were subcultured onto Columbia blood agar plates overnight to confirm negative or positive detection as well as to exclude contamination.
Data Analysis and Statistics
Statistical analyses were performed using GraphPad Prism 7. Detection rates between the two culture systems and between aerobic and anaerobic bottles were compared using Fisher’s exact test. Mann–Whitney tests were utilized to analyze the differences in TTD and to compare the mean TTD. When calculating mean TTD, blood culture bottles with no microorganisms recovered within 5 days (120 h) were excluded. A p value of < 0.05 was considered statistically significant.
Results
In this study, we tested 770 BacT/ALERT (FA Plus and FN Plus) and BACTEC (Aerobic/F Plus and Lytic/10 Anaerobic/F) blood culture bottles to evaluate the antimicrobial inactivation functions (Table 1). In general, the detection rate of BacT/ALERT Plus media was 320/385 (83.1%), while that of BACTEC media was 251/385 (65.2%) (p<0.001). Among the antimicrobial-free control bottles, all the microorganisms tested were recovered (340/340). In the presence of antibiotics, 231/430 (53.7%) bottles were declared positive, and the detection rate of BacT/ALERT system was significantly higher than that achieved for the BACTEC system (150/215 [69.8%] versus 81/215 [37.7%]; p<0.001). The detection rate of FA Plus media were higher than that of BD Aerobic Plus bottles; however, the difference was not statistically significant (p=0.22) (Table 2). To ensure the activities of antimicrobials involved, for each microorganism-antimicrobial combination, triplicate BacT/ALERT resin-free aerobic and/or anaerobic bottles (SA/SN) were incubated with horse blood, bacterial suspension and antimicrobial solution at peak serum concentrations, and all showed no microorganism growth (data not shown). Similar to resin-free anaerobic media, the BACTEC Lytic/10 Anaerobic/F media showed 17/80 (21.3%) recovery when evaluated with antimicrobial agents at peak serum concentrations.
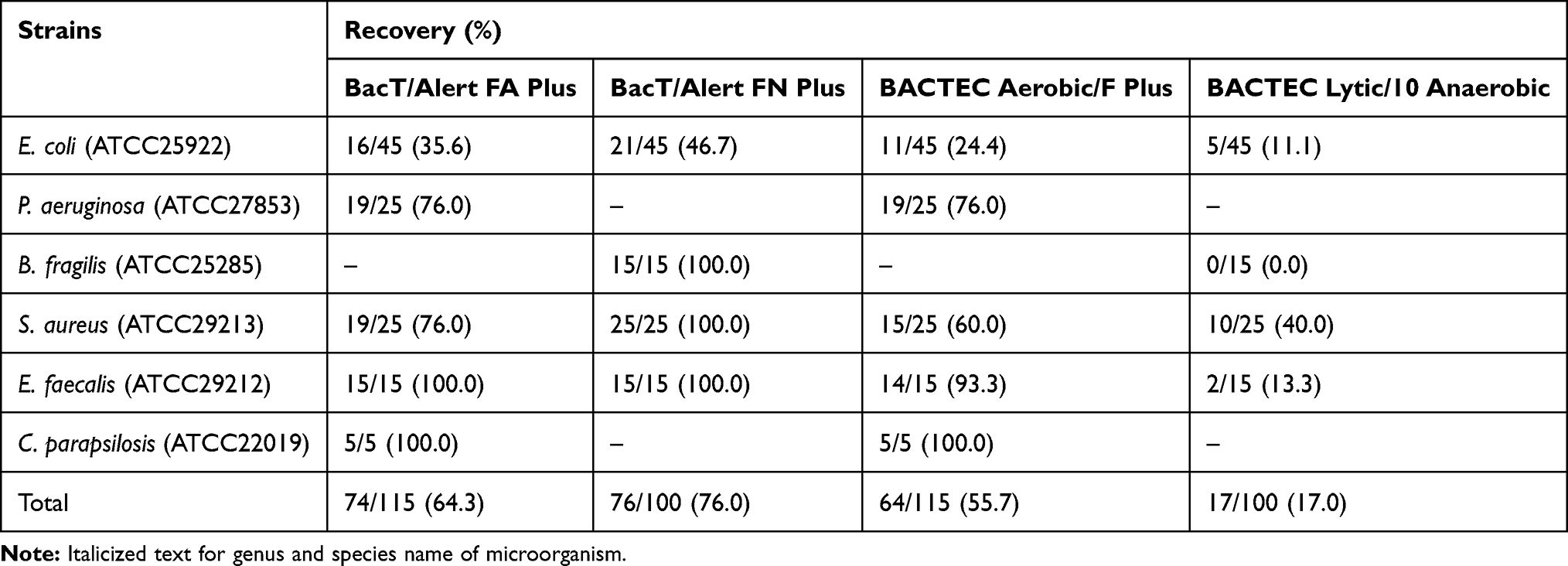 |
Table 2 Recovery in Aerobic (BacT/Alert FA Plus and BACTEC Aerobic/F Plus) or Anaerobic (BacT/Alert FN Plus and BACTEC Lytic/10 Anaerobic) Bottles Containing Antibiotics by Microorganism |
Both culture systems showed complete inactivation of voriconazole tested with C. parapsilosis (Table 4). As shown in Tables 3 and 4, the BacT/ALERT system showed 100% recovery with cefoxitin, piperacillin-tazobactam, vancomycin and linezolid, which were significantly higher than those of the BACTEC system (cefoxitin, p=0.03; piperacillin-tazobactam, p=0.047; vancomycin, p<0.001; linezolid, p=0.047). The lowest detection rates were observed with carbapenems (imipenem and meropenem) in both systems. For imipenem, the recovery rates of the BACTEC and the BacT/ALERT system were 7/40 (17.5%) and 28/40 (70.0%), respectively (p<0.001). Similar lower detection rates with meropenem were also observed in the BACTEC and the BacT/ALERT system (6/55 [10.9%] vs 16/55 [29.1%]) (p=0.03).
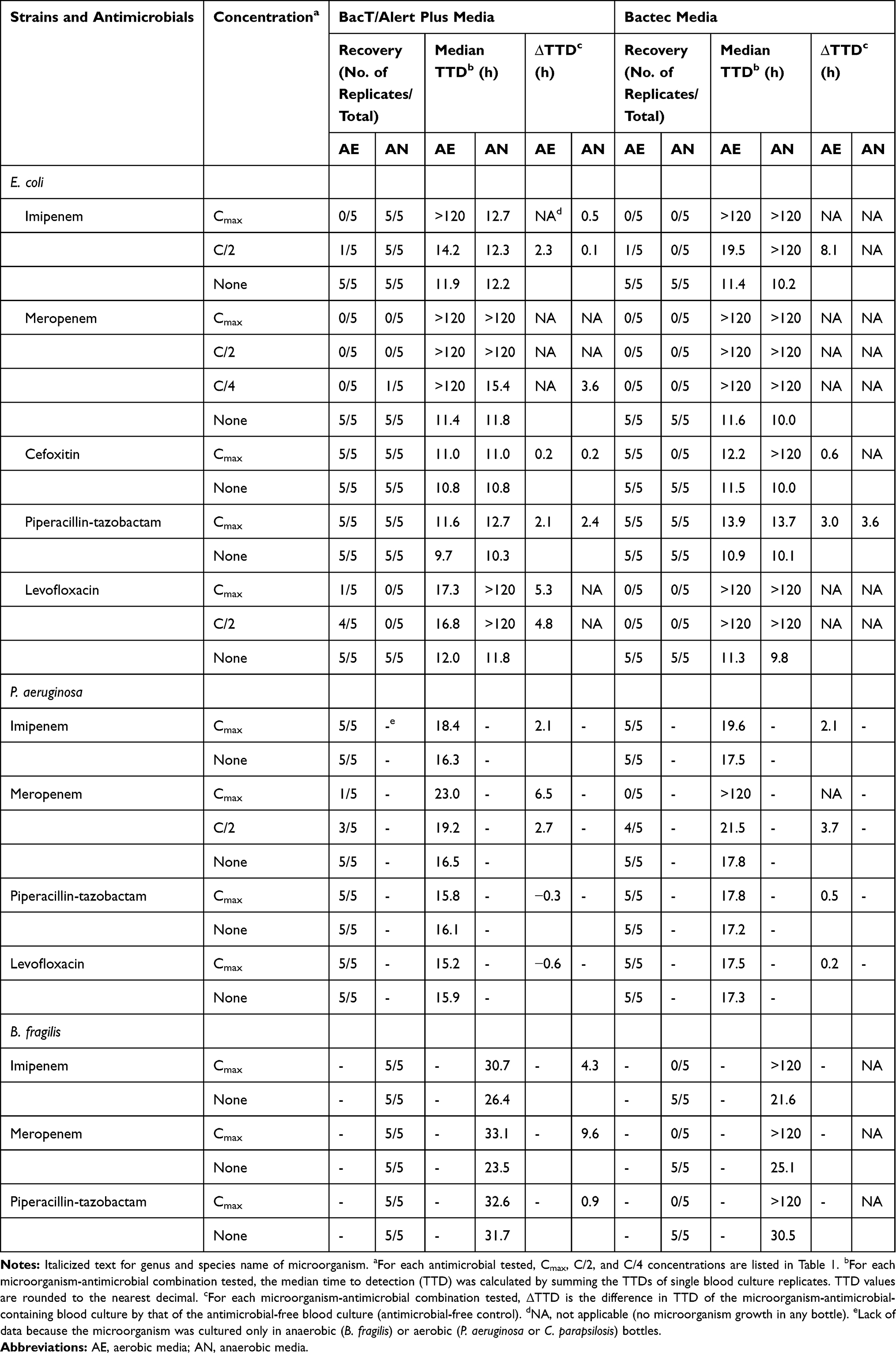 |
Table 3 Times to Detection of Gram-Negative Bacillus Recovered from Resin-Containing BacT/Alert or BACTEC Aerobic (AE) and Anaerobic (AN) Media at Each Antimicrobial Concentration Tested in Blood Culture Quintuplicates |
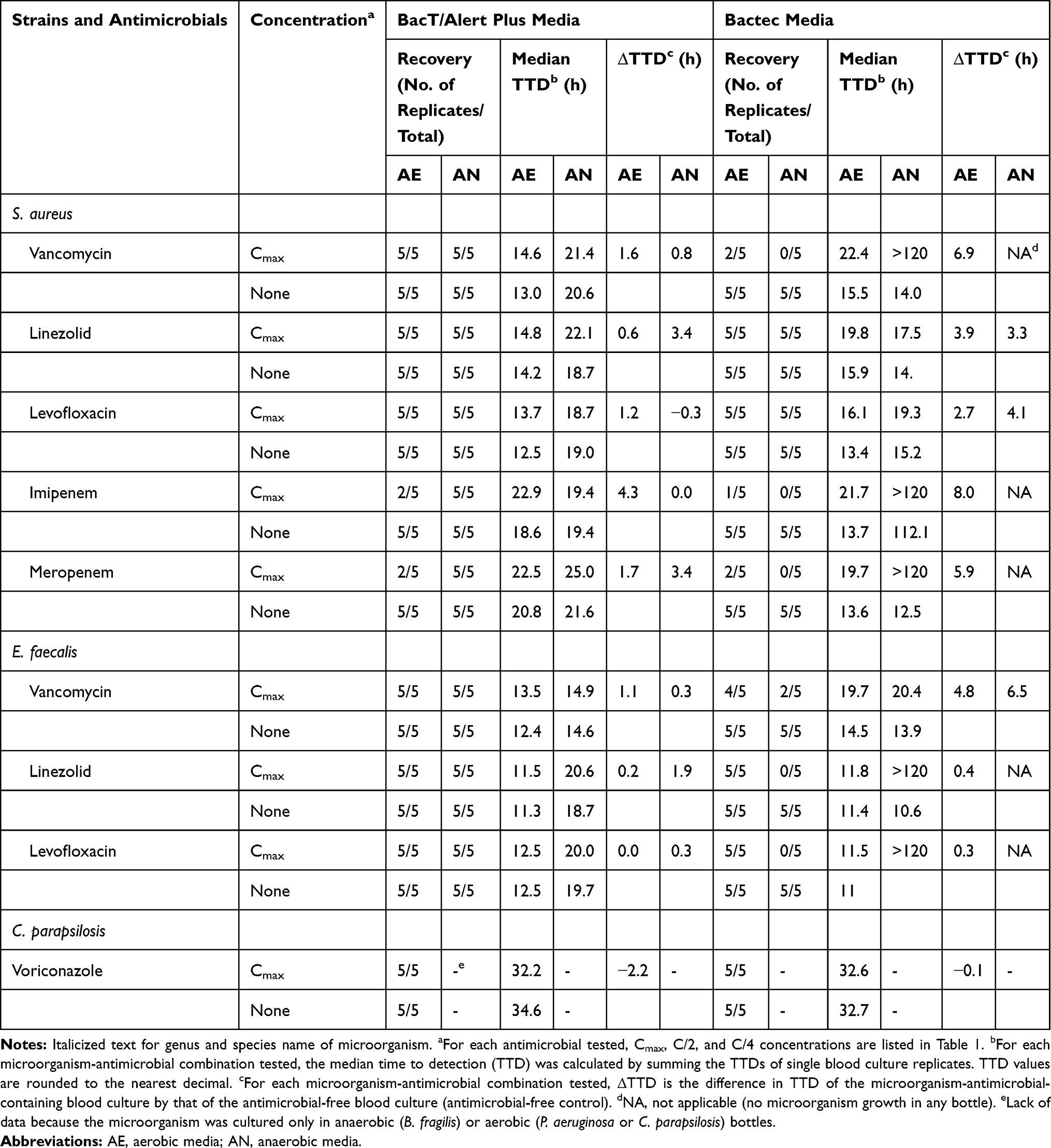 |
Table 4 Times to Detection of Gram-Positive Coccus and Yeast Recovered from Resin-Containing BacT/Alert or BACTEC Aerobic (AE) and Anaerobic (AN) Media at Each Antimicrobial Concentration Tested in Blood Culture Quintuplicates |
A total of 23 microorganism-antimicrobial combinations were found to get organisms recovered in both aerobic culture systems, and shorter TTD in FA Plus culture media than BD Aerobic Plus culture media were found in 16 (69.6%) combinations. For the two anaerobic culture systems, there were 20 microorganism-antimicrobial combinations observed to get organisms recovered, with 15 (75.0%) combinations showing shorter TTD in FN Plus bottles than the corresponding BACTEC anaerobic bottles (Tables 3 and 4). In addition, the TTD of FA Plus bottles (14.70 h) was 4.85 h shorter than that of the BD Aerobic Plus bottles (19.55 h) (p=0.047). Similarly, the TTD of FN Plus bottles was 16.8 h, which was 1.6 h shorter than that of BD Lytic/10 Anaerobic bottles (18.4 h) (p=0.88).
Tables 3 and 4 also summarize the differences in TTDs of the bottles spiked with microorganism-antimicrobial combinations compared with of the antimicrobial-free bottles (ΔTTD).7 For gram-negative bacteria, the highest ΔTTD (≥3 h) was observed for meropenem-E. coli, levofloxacin-E. coli, meropenem-P. aeruginosa, imipenem-B. fragilis, and meropenem-B. fragilis in BacT/ALERT system, and imipenem-E. coli, piperacillin-tazobactam-E. coli, and meropenem-P. aeruginosa in BACTEC system (Table 3). For gram-positive bacteria, the highest ΔTTD (≥3 h) was observed for linezolid-S. aureus, imipenem-S. aureus, and meropenem-S. aureus at the antibiotic Cmax in the BacT/ALERT system, and vancomycin-S. aureus, linezolid-S. aureus, imipenem-S. aureus, meropenem-S. aureus, and vancomycin-E. faecalis at the antibiotic Cmax in the BACTEC system (Table 4). Interestingly, negative ΔTTDs were observed in some microorganism-antimicrobial combinations, especially in voriconazole-C. parapsilosis (−2.2 h) at the antibiotic Cmax in BacT/ALERT FA Plus bottles (Table 4).
Discussion
In our study, significantly higher microorganism recovery rates were observed with the BacT/ALERT FAN Plus media in the presence of antimicrobial agents; however, the difference between the two aerobic blood culture bottles was not statistically significant. When one aerobic bottle and one anaerobic bottle were paired as a set of blood cultures, and microorganisms detected in at least one bottle of a pair are considered to be positive, the BacT/ALERT system showed a more satisfying detection rate. However, the recovery rates of the two systems were both lower than those reported elsewhere,6,7,9 which was probably due to the smaller inoculum (30 CFU/bottle) and susceptible ATCC strains used in our study. It is worth noting that the anaerobic bottles contained different media, which could influence the recovery of many pathogens, especially when exposed to antimicrobial agents.10 In addition, the resin-free BACTEC Lytic/10 Anaerobic/F bottle evaluated here is the only type of BD anaerobic blood culture media approved by the Chinese National Medical Products Administration (NMPA), which to some extent has lead to the relative lower positive rate of BACTEC system. In comparison, the resin-free BacT/ALERT SN anaerobic bottles that functioned to ensure the activities of antimicrobials involved showed 0/48 (0.0%) recovery when evaluated with antimicrobial agents at peak serum concentrations. In this study, besides the peak concentration (Cmax), two other descending concentrations (C/2 and C/4), which were higher than the midpoint (M) and the trough (T) concentrations used in some other studies,10–12 were selected for some antimicrobial-microorganism combinations. Therefore, even in the case that the tested blood culture media showed the best antimicrobial inactivation efficiency, spiked microorganisms could still be recovered in blood culture bottles in the presence of residual active antimicrobial agents (concentrations above the MIC).13
Complete recovery of all microorganisms tested at antimicrobial Cmax was observed in aerobic and anaerobic BacT/ALERT Plus and BACTEC aerobic culture media in at least one replicate, except for levofloxacin, imipenem, and meropenem. Variation in the inactivation of levofloxacin was found, and the difference between the two blood culture systems was not statistically significant. Complete inactivation of levofloxacin at the Cmax was observed in all strains in BacT/ALERT aerobic and anaerobic culture media and BACTEC aerobic culture media, except for E. coli ATCC25922. In the case of E. coli ATCC25922, 20% recovery and 80% recovery were observed at Cmax and C/2, respectively, in BacT/ALERT FA Plus bottles, and no inactivation was observed with BacT/ALERT FN Plus and BACTEC aerobic/anaerobic media. In another comparative evaluation with inoculum of 50–100 CFUs per bottle, complete recoveries of E. coli ATCC25922 incubated with levofloxacin at Cmax and C/2 were observed in BacT/ALERT (FA Plus and FN Plus) and BACTEC (Plus Aerobic/F and Plus Anaerobic/F) culture media.7 This difference in detection rate could be attributed to the lower CFUs used. In addition, in our study, the blood culture simulation model was performed using bottles spiked with horse blood, bacterial suspension, and antibiotic solution. However, in the study mentioned above, antibiotic solution was added prior to bacterial suspension. It has been reported that the concentration of free levofloxacin quickly fell to under the MIC range of E. coli ATCC25922 in BacT/ALERT FA Plus media within 10 min of incubation.14 Thus, the majority of levofloxacin may have been absorbed before bacterial suspension was added.
Carbapenems, in particular meropenem, exhibited the lowest detection rates in our study. There are two reasons for the low detection rates of carbapenems, especially, meropenem. First, according to the manufacture’s instructions, the inhibition of carbapenems in FN Plus media was more significant than that of FA Plus media. Second, the low detection of carbapenems was largely due to the low recovery rate of E. coli ATCC25922; the possible explanation for this is the low MIC and high Cmax/MIC quotient for the strain-antimicrobial combination. In our study, we further evaluated E. coli in the presence of meropenem at a concentration of 1/10 Cmax, and found 100% recovery (median TTD of 15.4 h) in FA Plus and FN Plus bottles. In contrast, no recovery at 1/10 Cmax was observed in the BACTEC (Plus Aerobic/F and Lytic/10 Anaerobic/F) culture media (data not shown).
The overall performance of BacT/ALERT FN Plus media was better than that of FA Plus media, caused by the more powerful antibiotic inactivation of FN Plus media and the difference in oxygen consumption niche of spiked bacteria. However, no statistically significant difference was observed, except for that of S. aureus ATCC29213 (p=0.02). The difference was largely due to the lower recovery rates with carbapenems caused by the weak inhibition of carbapenems by FA Plus media as well as the low MIC and high Cmax/MIC quotient. The presence of voriconazole had no effect on C. parapsilosis detection in two blood culture systems, probably due to the fungistatic effect rather than the fungicidal effect of voriconazole against Candida.15 Therefore, the differences in detection rate among different blood culture systems are supposed to be decided not only by the antibiotic-inactivation ability of the culture media but also by the concentration of the antibiotics, the MICs of the evaluated strains, and the CFUs per bottle.
The first-time detection of positive blood culture in clinical microbiology laboratories is crucial for the treatment and prognosis of patients with sepsis, making TTD a significant parameter to evaluate the performance of commercial automatic blood culture systems. In general, the BacT/ALERT FA Plus and FN Plus bottles demonstrated shorter TTDs than the BACTEC aerobic and anaerobic bottles, respectively. In addition, the difference in the TTDs of aerobic culture media was statistically significant. These results are consistent with a recent study that compared the TTD of the VIRTUO and FX automated blood culture systems.7 It is not clear whether the typical several-hour differences will finally lead to the delay in clinical decision-making in clinical settings. Further prospective clinical studies evaluating the influence of differences in TTD on the initiation or change of antibiotic treatment strategies will be needed.
In terms of ΔTTD, another key parameter to evaluate the antimicrobial-inactivation ability of the automatic blood culture media examined here, delays of at least 3 h compared to positive results in control (antimicrobial-free) blood culture bottles were observed in nine gram-negative bacteria-antibiotic-concentration pairs and ten gram-positive bacteria-antibiotic-concentration pairs, respectively. Among the gram-negative bacteria, six cases (6/9, 66.7%) involved E. coli ATCC25922. Among gram-positive bacteria, seven cases (7/10, 70.0%) involved MSSA. In terms of antibiotics, 9/19 (47.3%) cases involved carbapenems (imipenem and/or meropenem). Moreover, longer ΔTTDs were more frequently observed with BACTEC Plus Aerobic/F media than with FA Plus media. Thus, it is possible that the type and/or species of microorganisms, as well as the interaction between the microorganism and a specific antimicrobial in complex surroundings such as blood culture bottles can to some extent influence the outcome of antimicrobial inactivation.
However, there are still some limitations. First, as simulated blood culture, horse blood was spiked instead of human blood. Second, since the BD BACTEC Plus Anaerobic/F media is not permitted in mainland China, the BACTEC Lytic/10 Anaerobic/F media was evaluated instead with BACTEC Plus Aerobic/F media as pairs. Third, only susceptible ATCC strains were evaluated and resistant clinical isolates were not involved. However, as microorganisms with higher MICs grow faster and more easily in the presence of corresponding antibiotics and clinical isolates with MICs as low as the ATCC strains were not common in our hospital, it is supposed that our study design could well reflect the actual situations in clinical settings. Finally, only limited types and numbers of microorganisms and antimicrobials were evaluated in our study. Further studies with added microbial species/strains and antimicrobial types and further prospective comparative studies with blood culture specimens from patients undergoing antimicrobial treatment will provide more actual information about the capabilities of these commercial automatic blood culture systems for antimicrobial inactivation.
Conclusion
In conclusion, even with the limitations of the simulated study,9 relative but not absolute advantages were observed with BacT/ALERT (FA Plus and FN Plus) media. The majority of the tested broad-spectrum antimicrobial agents under most clinically meaningful concentrations can be effectively inhibited, with the exception of E. coli with meropenem in FA Plus and FN Plus bottles and E. coli with levofloxacin in FN Plus bottles. In addition, shorter TTD was also observed. In order to maximize the chances of recovery for patients who have previously received antimicrobial treatments, BacT/ALERT FAN Plus bottles with a relatively higher cost, can be selectively used. Nevertheless, optimizing the time of blood culture collection just before the next antimicrobials dose and with complete aerobic and anaerobic sets is critical to maximize the efficiency of all blood culture bottles.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grant No. 81572055 and No. 81803110). The funder had no role in the study design, experiments, data collection and analysis, decision to publish, or preparation of the manuscript. We would like to thank Editage (www.editage.cn) for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goto M, Alhasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013;19(6):501–509. doi:10.1111/1469-0691.12195
2. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi:10.1007/s00134-017-4683-6
3. Reddy P. Empiric antibiotic therapy of nosocomial bacterial infections. Am J Ther. 2016;23(4):e982–994. doi:10.1097/MJT.0000000000000042
4. Lamy B, Ferroni A, Henning C, Cattoen C, Laudat P. How to: accreditation of blood cultures’ proceedings. A clinical microbiology approach for adding value to patient care. Clin Microbiol Infect. 2018;24(9):933–934. doi:10.1016/j.cmi.2018.01.011
5. Ziegler R, Johnscher I, Martus P, Lenhardt D, Just HM. Controlled clinical laboratory comparison of two supplemented aerobic and anaerobic media used in automated blood culture systems to detect bloodstream infections. J Clin Microbiol. 1998;36(3):657–661. doi:10.1128/JCM.36.3.657-661.1998
6. Chung Y, Kim IH, Han M, et al. A comparative evaluation of BACT/ALERT FA PLUS and FN PLUS blood culture bottles and BD BACTEC Plus Aerobic and Anaerobic blood culture bottles for antimicrobial neutralization. Eur J Clin Microbiol Infect Dis. 2019;38(12):2229–2233. doi:10.1007/s10096-019-03663-3
7. Menchinelli G, Liotti FM, Giordano L, et al. Efficient inactivation of clinically relevant antimicrobial drug concentrations by BacT/Alert or Bactec resin-containing media in simulated adult blood cultures. Antimicrob Agents Chemother. 2019;63(7):e00420–19. doi:10.1128/AAC.00420-19
8. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
9. Grupper M, Nicolau DP, Aslanzadeh J, Tanner LK, Kuti JL. Effects of clinically meaningful concentrations of antipseudomonal β-lactams on time to detection and organism growth in blood culture bottles. J Clin Microbiol. 2017;55(12):3502–3512. doi:10.1128/JCM.01241-17
10. Chen IH, Nicolau DP, Kuti JL. Effect of clinically meaningful antibiotic concentrations on recovery of Escherichia coli and Klebsiella pneumoniae isolates from anaerobic blood culture bottles with and without antibiotic binding resins. J Clin Microbiol. 2019;57(12):e01344–19. doi:10.1128/JCM.01344-19
11. Flayhart D, Borek AP, Wakefield T, Dick J, Carroll KC. Comparison of BACTEC PLUS blood culture media to BacT/Alert FA blood culture media for detection of bacterial pathogens in samples containing therapeutic levels of antibiotics. J Clin Microbiol. 2007;45(3):816–821. doi:10.1128/JCM.02064-06
12. Miller NS, Rogan D, Orr BL, Whitney D. Comparison of BD Bactec Plus blood culture media to VersaTREK Redox blood culture media for detection of bacterial pathogens in simulated adult blood cultures containing therapeutic concentrations of antibiotics. J Clin Microbiol. 2011;49(4):1624–1627. doi:10.1128/JCM.01958-10
13. Mitteregger D, Barousch W, Nehr M, et al. Neutralization of antimicrobial substances in new BacT/Alert FA and FN Plus blood culture bottles. J Clin Microbiol. 2013;51(5):1534–1540. doi:10.1128/JCM.00103-13
14. Lovern D, Katzin B, Johnson K, et al. Antimicrobial binding and growth kinetics in BacT/ALERT FA Plus and BACTEC Aerobic/F Plus blood culture media. Eur J Clin Microbiol Infect Dis. 2016;35(12):2033–2036. doi:10.1007/s10096-016-2759-9
15. Köck R, Eißing LC, Boschin MG, et al. Evaluation of bactec mycosis IC/F and Plus Aerobic/F blood culture bottles for detection of Candida in the presence of antifungal agents. J Clin Microbiol. 2013;51(11):3683–3687. doi:10.1128/JCM.02048-13
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.