")
Back to Journals » Infection and Drug Resistance » Volume 12
In vitro activity of newer antimicrobials against penicillin non-susceptible strains of Streptococcus pneumoniae
Authors Hipp M, Burckhardt I
Received 24 January 2019
Accepted for publication 24 April 2019
Published 1 July 2019 Volume 2019:12 Pages 1889—1893
DOI https://doi.org/10.2147/IDR.S202789
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Marlene Hipp, Irene Burckhardt
Department for Infectious Diseases, Microbiology and Hygiene, University Hospital of Heidelberg, Heidelberg, Germany
Background: Since the first isolation of Streptococcus pneumoniae with low penicillin susceptibility in the 1960s, resistant strains have spread over the globe, causing substantial problems in the treatment of pneumococcal infections. However, in Germany, rates of non-susceptibility are still below 5%.
Methods: Since 2009 clinical pneumococcal strains have been collected at the Center for Infectious Diseases, Heidelberg University Hospital, Germany. In this study, 56 of these strains were chosen due to their decreased penicillin susceptibility (minimal inhibitory concentration (MIC)≥0.12 μg/mL). Sixteen of these strains even showed an MIC of ≥2 μg/mL. We examined the in vitro activity of newer antimicrobials known to be active against Gram-positive bacteria. For this purpose MICs of ceftaroline, ceftobiprole, dalbavancin, delafloxacin, eravacycline, tedizolid, and telavancin were determined and evaluated.
Results: All of the 7 antimicrobial agents inhibited pneumococcal growth at concentrations of 0.5 μg/mL or lower. Currently, clinical breakpoints are only available for two substances, ceftaroline and ceftobiprole. According to these breakpoints, all MICs were below the susceptibility breakpoint; however, there was a correlation between high penicillin MICs (≥2 μg/mL) and MICs near the ceftaroline and ceftobiprole susceptibility breakpoint. The other agents showed very promising effects against all tested strains with the lowest MIC90 of 0.002 μg/mL for telavancin.
Conclusion: Consequently, this study demonstrates the promising in vitro activity of newer antimicrobials against penicillin non-susceptible strains of S. pneumoniae.
Keywords: Streptococcus pneumoniae, penicillin resistance, susceptibility testing
Introduction
Increasing antimicrobial resistance in Streptococcus pneumoniae (pneumococcus) is a major problem in treating pneumococcal infections. While therapy is becoming more difficult, S. pneumoniae is still responsible for millions of deaths worldwide every year by causing severe illnesses like pneumonia, meningitis, and sepsis.1 Successful treatment with penicillin was impaired by the emergence of penicillin non-susceptible strains in the 1960s and 1970s.2 Additionally, some strains acquired resistance mechanisms against erythromycin, macrolides, and quinolones. Emergence of resistance was shown to be correlated to the usage of antibiotics.3,4
The European Committee on Antimicrobial Susceptibility Testing (EUCAST) determined the clinical breakpoint for penicillin-susceptible pneumococci at 0.06 µg/mL.5 Isolates with minimal inhibitory concentrations (MIC) above this breakpoint are considered penicillin non-susceptible S. pneumoniae (PNSP). In meningitis cases, resistance to penicillin is characterized as a MIC of >0.06 µg/mL. There is no intermediate category for strains causing meningitis. In non-meningitis cases, resistance is characterized as a MIC of >2 µg/mL. Non-meningitis strains with MICs of >0.06 µg/mL and ≤2 µg/mL are considered to be intermediate. The prevalence of PNSP isolates depends strongly on the country of isolation. Within Europe, the proportion of PNSP ranges from 0.2% in Belgium to 45.5% in Cyprus. In Germany, roughly 5% of pneumococcal isolates are penicillin non-susceptible.6
In this study, the activity of newly developed antimicrobial agents against clinical PNSP strains was examined. All antimicrobials are reported to show activity against Gram-positive bacteria. Eravacycline, a new tetracycline, was chosen due to reports about its activity against Gram-positive bacteria, including PNSP.7 Further, two cephalosporins approved for pneumococcal disease, ceftaroline and ceftobiprole, were selected. Eventually, four antimicrobial agents were examined, representing different classes of antibiotics: glycopeptides (dalbavancin, telavancin), oxazolidinone (tedizolid) and fluoroquinolone (delafloxacin). All these four are in use against skin and skin structure infections due to resistant Gram-positive bacteria, mainly methicillin-resistant Staphylococcus aureus.8–11
The purpose of the study was to determine the MIC distribution of the newer antimicrobial agents against clinical PNSP isolates. In prospect, this could lead to treatment alternatives for patients with diseases caused by penicillin non-susceptible pneumococci.
Materials and methods
Bacterial isolates
For this study, 56 penicillin non-susceptible strains of Streptococcus pneumoniae were examined. Strains had been isolated from different patient specimens at the Heidelberg University Hospital in Germany between February 2009 and December 2016. Among them, 27 strains originated from respiratory material, 14 were invasive pneumococcal strains (blood n=12; pleural empyema n=1; aortic tissue n=1) and 15 strains originated from other material (nose swab n=7; urine n=5; conjunctiva swab n=1; other swab n=1; bile punctate n=1). Species identification was performed by bile and optochin susceptibility as well as mass spectrometry performed with a Bruker microflex MALDI-TOF MS. Serotyping was performed only for invasive strains at the National Reference Laboratory for Streptococci in Aachen, Germany (NRCS) with the Quellung reaction. Invasive strains included serotype 19A (n=5), 15A (n=3), 19F (n=2), 23B (n=2), 12F (n=1), and 6A (n=1). Isolates were stored in skim milk at −80°C until further testing. Penicillin susceptibility was initially determined by agar diffusion with oxacillin disks (1 mg). In the case of resistance (diameter <20 mm), MICs were determined by broth microdilution with VITEK2 using AST-P576 or AST-ST03 panels (bioMérieux, Marcy l’Etoile/France). All MICs for penicillin of the tested pneumococci were equal to or higher than 0.12 µg/mL and laid above the susceptibility breakpoint of 0.06 µg/µL as defined by EUCAST.5 Sixteen of 56 strains showed MIC values for penicillin equal to or higher than 2 µg/mL and were designated resistant. The VITEK AST panels could not distinguish between 2 µg/mL and >2 µg/mL for penicillin. Fourteen of these 16 resistant strains additionally exhibited an intermediate susceptibility to cefotaxime with MICs between 0.75 µg/mL and 1.0 µg/mL, while all other strains were fully susceptible to cefotaxime (MIC≤0.5 µg/mL). Forty of 56 strains were designated as intermediately resistant against penicillin. For comprehensive data on the test strains, see Tables S1 and S2.
Media and culture conditions
Strains were cultured on BD Columbia Agar with 5% Sheep Blood (Becton Dickinson GmbH, Heidelberg/Germany). For MIC determination using E-Test, Mueller Hinton agar +5% horse blood +20 mg/L ß-NAD (MHF) (bioMérieux, Marcy l’Etoile/France) was used. Agar plates were stored as recommended by the manufacturer. Cultures were incubated for 18±2 h at 36±1°C and 5% CO2.
Antimicrobial susceptibility testing
In vitro antimicrobial activities of 7 agents against 56 PNSP isolates were examined. For this purpose, MICs of the bacterial strains were determined using MIC Test Strips (Liofilchem S.r.l., Roseto, Italy). Testing was executed as specified by the manufacturer. With the test strips, MICs between 0.002 µg/mL and 32 µg/mL could be evaluated. Seven antimicrobials were tested: ceftaroline (Allergan, Dublin, Ireland), ceftobiprole (Basilea Pharmaceutica, Basel, Switzerland), dalbavancin (Durata Therapeutics Holding, Morristown, NJ, USA), delafloxacin (Melinta Therapeutics, New Haven, CT, USA), eravacycline (Tetraphase Pharmaceuticals, Watertown, NY, USA), tedizolid (Merck Sharp & Dohme Corp., Kenilworth, NJ, USA) and telavancin (Astellas Pharma US, Chūō, Japan). Out of these 7 antimicrobials, EUCAST clinical breakpoints for S. pneumoniae are currently available only for ceftaroline (0.25 µg/mL) and ceftobiprole (0.5 µg/mL).5 The Clinical and Laboratory Standards Institute (CLSI) defines the susceptibility breakpoint for ceftaroline and S. pneumoniae at 0.5 µg/mL.12 For MIC interpretation EUCAST breakpoints were used; however, using CLSI breakpoints would not have affected the interpretation of the results.
Results
With a MIC range of 0.008 to 0.19 µg/mL, all strains were tested susceptible for ceftaroline (breakpoint of 0.25 µg/mL) (Table 1). In the same way, ceftobiprole, having a range of 0.012 to 0.5 µg/mL and a breakpoint of 0.5 µg/mL, also showed a sufficient activity against all tested pneumococci.
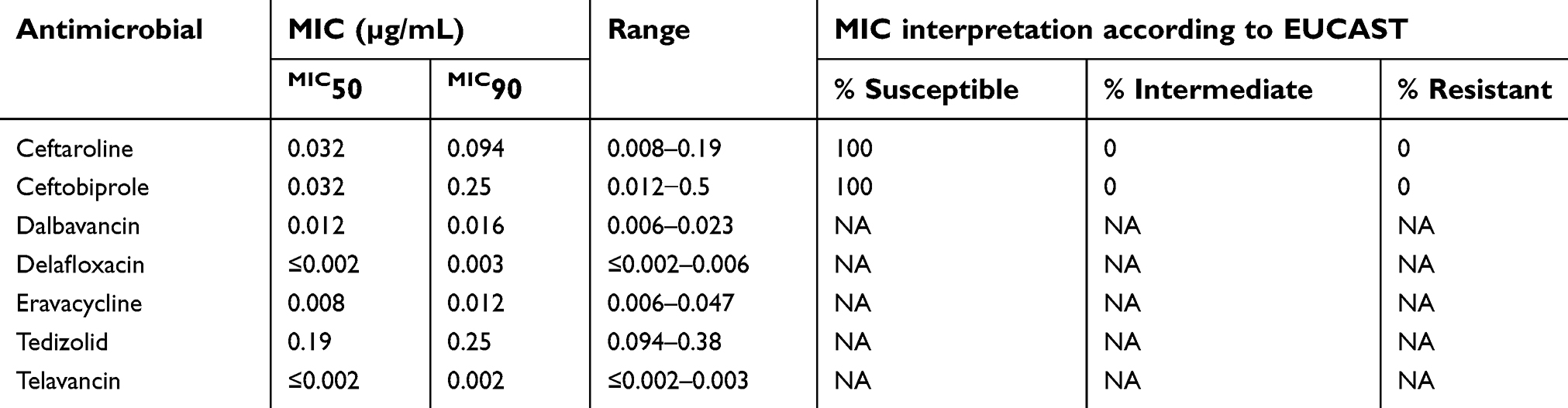 |
Table 1 In vitro activity of different antimicrobial agents against 56 penicillin non-susceptible pneumococcal isolates. |
However, while both agents caused an inhibition of 50% of the strains at concentrations of 0.032 µg/mL, MICs close to the susceptibility breakpoints were necessary to inhibit 90% of the strains. MIC90 of ceftaroline was determined as 0.094 µg/mL. Ceftobiprole had a MIC90 of 0.25 µg/mL and a wide distribution of inhibitory concentrations. Roughly 5% of the strains showed a MIC for ceftobiprole identically to the clinical breakpoint of 0.5 µg/mL (Table 2). Noticeably, most of the strains with higher MICs for ceftobiprole and ceftaroline were strains with very high penicillin and cefotaxime MICs.
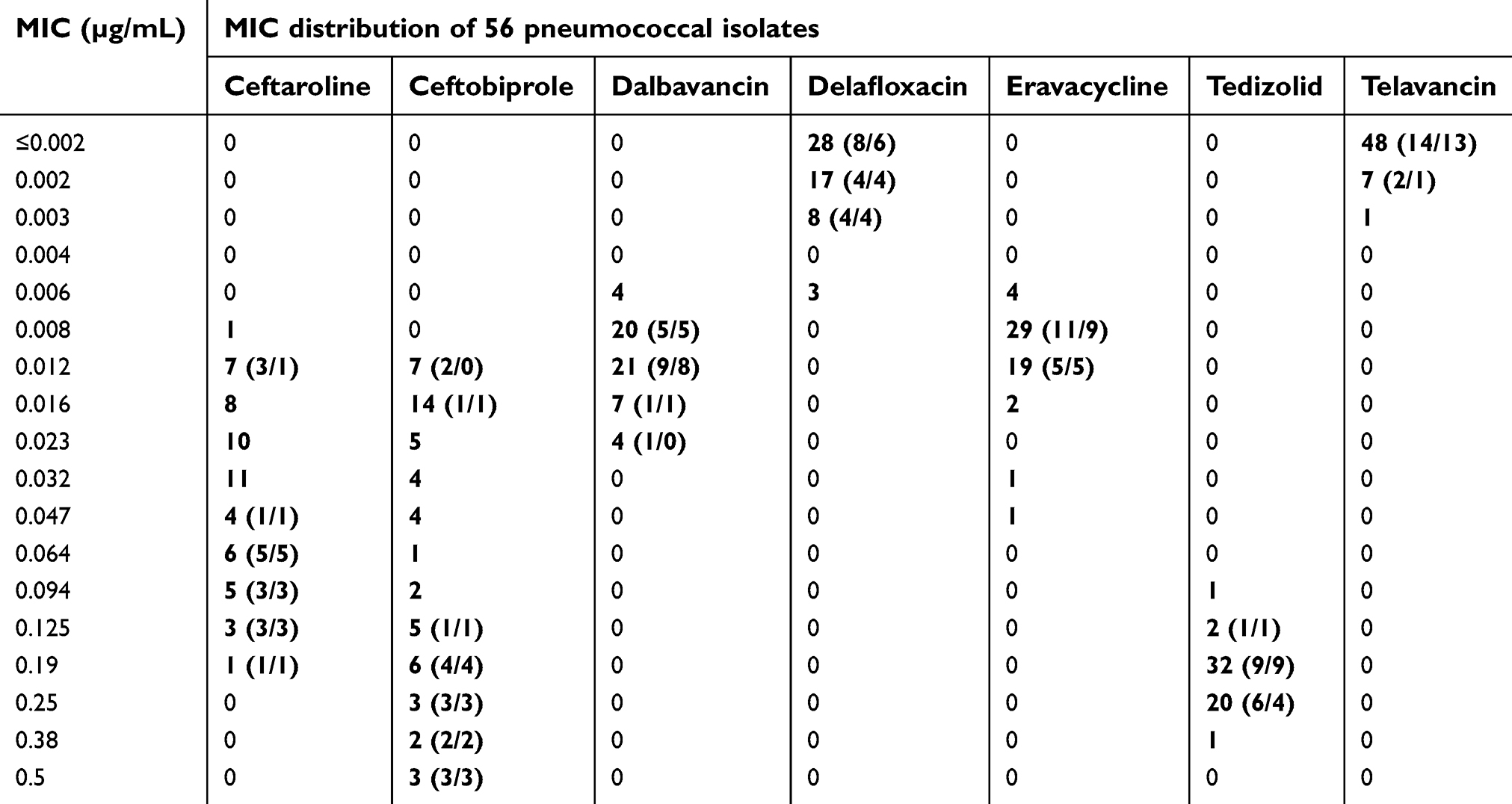 |
Table 2 Distribution of MIC values of different antimicrobial agents, determined with 56 penicillin non-susceptible S. pneumoniae isolates. Distribution of penicillin-resistant and cefotaxime non-susceptible isolates (n=16, penicillin MIC≥2 µg/mL and n=14 cefotaxime MIC>0.5 µg/mL and ≤2 µg/mL) in brackets. Antimicrobials are sorted in alphabetical order. |
High antimicrobial activity was observed for delafloxacin and telavancin. Both agents had a MIC50 below 0.002 µg/mL as well as a MIC90 of 0.003 µg/mL (delafloxacin) and 0.002 µg/mL (telavancin). Dalbavancin, too, showed a low MIC50 of 0.012 µg/mL and MIC90 of 0.016 µg/mL with a narrow distribution up to 0.023 µg/mL. Similarly, eravacycline inhibited 50% of strains at 0.008 µg/mL and 90% at 0.012 µg/mL. MIC values were distributed from 0.006 up to 0,047 µg/mL eravacycline.
Of all tested antimicrobials, tedizolid had the highest MIC50 and MIC90 values, achieving a growth inhibition at concentrations of 0.19 µg/mL for 50% and 0.25 µg/mL for 90% of the pneumococcal strains. The values were distributed within a range of 0.094 and 0.38 µg/mL.
Detailed MIC values for every test strain are provided in Table S2.
Discussion
This study was performed to evaluate 7 antimicrobials with activity against Gram-positive bacteria for their possible activities against PNSPs.
Delafloxacin had a high activity against all tested PNSP isolates and effected a microbial growth inhibition at low concentrations while showing high activity against penicillin-resistant strains. The determined MICs of ≤0.002 µg/mL up to 0.006 µg/mL were already shown to be bactericidal against PNSPs; furthermore, a maximum observed concentration, cmax, of roughly 7 µg/mL in plasma implies a possible in vivo activity of delafloxacin against PNSPs.11,13
In a similar way, eravacycline was observed to be potent at low MICs, regardless of the different levels of penicillin resistance of the strains. Eravacycline was effective in vitro in concentrations between 0.006 and 0.047 µg/mL. In vivo, eravacycline already showed bioavailability with cmax of 2.1 µg/mL in plasma and cmax of 0.7±0.3 µg/mL in epithelial lining fluid in the lung.14,15 It is therefore most likely that the agent would be an effective treatment for invasive or respiratory infections with PNSPs. However, eravacycline´s bacteriostatic mode of action has to be considered before therapy.
The efficiencies of the two bactericidal glycopeptides dalbavancin and telavancin against penicillin non-susceptible pneumococci were slightly different. While telavancin exhibited a very potent activity against all tested strains (all MICs ≤0.003 µg/mL), dalbavancin showed its effects at MICs between 0.006 and 0.023 µg/mL, that is at MICs at least twofold higher. Compared to the reachable serum cmax of 423 µg/mL for dalbavancin and 93.6 µg/mL for telavancin, both MIC ranges are promising for successful treatment of PNSP diseases.8,9
Compared to the other antimicrobials, the two cephalosporins ceftaroline and ceftobiprole showed a much wider range of MIC values. Considering that these two substances are the only agents (of the antimicrobials tested in this study) currently approved for treatment of pneumococcal disease, activity was rather low against strains with elevated penicillin MICs. The distribution of results furthermore showed a correlation between high penicillin and high cefotaxime MICs and high ceftaroline or ceftobiprole MICs. This might be explained by the shared resistance mechanism of S. pneumoniae against penicillin and cefotaxime due to an altered penicillin-binding protein 2× and a possible effect on ceftaroline and ceftobiprole susceptibility.16,17 The comparably high MICs for ceftaroline and ceftobiprole carry the risk of treatment failure despite the fact that all values were below the published susceptibility breakpoints.
The bacteriostatic antimicrobial tedizolid required comparatively higher concentrations than the other agents to inhibit bacterial growth. But in contrast to the cephalosporins, MIC values of tedizolid distributed in a narrow range, and no difference in the distribution of penicillin-resistant pneumococci was observed. Eventually, all MICs of tedizolid in the range of 0.094 to 0.38 µg/mL were below a reachable serum cmax of 3.0 µg/mL.10
In summary, the results of this study indicate a sufficient in vitro activity of newer antimicrobials against penicillin non-susceptible strains of Streptococcus pneumoniae. While high antimicrobial activity was observed in most agents, MICs of the two tested cephalosporins were close to the respective susceptibility breakpoints and advert to a connection between elevated penicillin and cefotaxime MICs.
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Pneumococcal conjugate vaccine for childhood immunization – WHO position paper. Wkly Epidemiol Rec. 2007;82(12):93–104.
2. Ardanuy C, Pallares R, Fenoll A, Lin J. Changes in antimicrobial resistance, serotypes and genotypes in Streptococcus pneumoniae over a 30-year period. Clin Microbiol Infect. 2010;16:402–410. doi:10.1111/j.1469-0691.2010.03182.x
3. Pallares R, Gudiol F, Liñares J, et al. Risk factors and response to antibiotic therapy in adults with bacteremic pneumonia caused by penicillin-resistant pneumococci. N Engl J Med. 1987;317:18–22. doi:10.1056/NEJM198707023170104
4. Riedel S, Beekmann SE, Heilmann KP, et al. Antimicrobial use in Europe and antimicrobial resistance in Streptococcus pneumoniae. Eur J Clin Microbiol Infect Dis. 2007;(26):485–490. doi:10.1007/s10096-007-0321-5
5. The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 8.1; 2018. Available from: http://Www.Eucast.Org. Accessed May 21, 2019.
6. European Centre for Disease Prevention and Control. Surveillance atlas of infectious diseases; 2017. Available from: https://ecdc.europa.eu/en/surveillance-atlas-infectious-diseases.
7. Zhanel GG, Baxter MR, Adam HJ, Sutcliffe J, Karlowsky JA. In vitro activity of eravacycline against 2213 Gram-negative and 2424 Gram-positive bacterial pathogens isolated in Canadian hospital laboratories : CANWARD surveillance study 2014 – 2015. Diagnostic Microbiol Infect Dis. 2018;91(1):55–62. doi:10.1016/j.diagmicrobio.2017.12.013
8. Durata Therapeutics Holding C.V. Full prescribing information DALVANCE® (dalbavancin) [package insert]. 2018;1–20.
9. Astellas Pharma US. Full prescribing information VIBATIV (telavancin) [package insert]. 2009.
10. Merck Sharp & Dohme Corp. Full Prescribing Information SIVEXTRO® (Tedizolid Phosphate) [package insert]. 2017;1–17
11. Melinta Therapeutics. Full prescribing information BAXDELATM (delafloxacin) [package insert]. 2017.
12. CLSI M100-ED28:2018 Performance Standards for Antimicrobial Susceptibility Testing.
13. Jorgensen SCJ, Mercuro NJ, Davis SL. Delafloxacin : place in therapy and review of microbiologic, clinical and pharmacologic properties. Infect Dis Ther. 2018;7(2):197–217. doi:10.1007/s40121-018-0198-x
14. Tetraphase Pharmaceuticals Inc. Full prescribing information XERAVA (eravacycline) [package insert]. 2018.
15. Connors KP, Housman ST, Pope JS, et al. Phase I, open-label, safety and pharmacokinetic study to assess bronchopulmonary disposition of intravenous eravacycline in healthy men and women. Antimicorbial Agents Chemother. 2014;58(4):2113–2118. doi:10.1128/AAC.02036-13
16. Grebe T, Hakenbeck R. Penicillin-binding proteins 2b and 2x of Streptococcus pneumoniae are primary resistance determinants for different classes of  -lactam antibiotics. Antimicorbial Agents Chemother. 1996;40(4):829–834. doi:10.1128/AAC.40.4.829
17. Mousavi SF, Pana M, Feizabadi M, et al. Diversity of mosaic pbp2x families in penicillin-resistant Streptococcus pneumoniae from Iran and Romania. Antimicorbial Agents Chemother. 2017;61(12):1–12.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.