")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Improving the Quality of Emergency Intrahospital Transport for Critically Ill Patients by Using Toyota Production System Methods
Authors Lu KK, Zhang MM, Zhu YL, Ye C, Li M
Received 28 January 2022
Accepted for publication 20 April 2022
Published 17 May 2022 Volume 2022:15 Pages 1111—1120
DOI https://doi.org/10.2147/JMDH.S360261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ke-Ke Lu,1 Miao-Miao Zhang,1 Yue-Li Zhu,2 Chen Ye,1 Min Li3
1Emergency Department, Hangzhou Linping Hospital of Integrated Traditional Chinese and Western Medicine, Hangzhou, Zhejiang Province, People’s Republic of China; 2Department of Nursing, Hangzhou Linping Hospital of Integrated Traditional Chinese and Western Medicine, Hangzhou, Zhejiang Province, People’s Republic of China; 3Department of Infectious Diseases, Hangzhou Linping Hospital of Integrated Traditional Chinese and Western Medicine, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Yue-Li Zhu, Department of Nursing, Hangzhou Linping Hospital of Integrated Traditional Chinese and Western Medicine, Hangzhou, Zhejiang Province, People’s Republic of China, Email [email protected]
Objective: To explore the effects of the Toyota Production System (TPS) for improving the quality of emergency intrahospital transport for critically ill patients in management.
Methods: Between April and June 2021, 68 critically ill patients were transported to corresponding wards, while 63 critically ill patients were transported to corresponding wards between July and September 2021. The pre-TPS and post-TPS management groups each included 30 cases based on their propensity score. The TPS management tool was combined with the PDCA method for analysing the current situation as well as determining the target for improvement, calculating the value and process efficiencies, and modifying and evaluating relevant processes. At last, the changes in transport time, receiving department, patient satisfaction, and adverse event rate of critically ill patients after TPS management were analysed.
Results: The total intrahospital transport time of critically ill patients decreased from 39 minutes (median) before the implementation of TPS management to 27 minutes (median) after TPS management, and the difference was statistically significant (P< 0.05). Process efficiency and value efficiency both increased from 33.33% and 38.46% before TPS management to 42.86% and 40.74% after TPS management, respectively. Likewise, the satisfaction of receiving departments and patients increased from 73.33% and 76.67% before TPS management to 96.67% and 96.67% after TPS management (P< 0.001). Finally, the adverse event rate decreased as a result of TPS management from 13.33% to 3.33% (P> 0.05).
Conclusion: TPS management may significantly shorten the intrahospital transport time for critically ill patients, reduce the occurrence of adverse events in emergency care, advance patient satisfaction, and improve the overall quality and safety of emergency care.
Keywords: Toyota Production System, TPS, critically ill patients, transportation of patients, patient satisfaction, emergency care
Introduction
As the first stage for the diagnosis and treatment of acute or critically ill patients, emergency departments are critical for rescuing patients and maintaining vital signs while facilitating subsequent specialised treatment. When the patients’ conditions meet relevant requirements for transport, they should be admitted to the corresponding specialised departments for further specific treatment as soon as possible. Therefore, for critically ill patients, high-quality intrahospital transport is critical for timely diagnosis and treatment as well as mortality reduction.1,2 Acute or critically ill patients face complex emergencies which often need advanced life support; and for them, intrahospital transport is a difficult process.3,4 Therefore, to guarantee the timeliness and safety of intrahospital transport for these patients, it is urgent to standardise and optimise the intrahospital transport process. In light of this, the emergency department should have the ability to provide high-quality and rapid intrahospital transport services to affected patients. For this to occur, it is necessary to specifically analyse every link in the intrahospital transport process for critically ill patients, to continuously optimise the clinical service process, reduce relevant costs, and improve the satisfaction of doctors and patients. The Toyota Production System (TPS), also known as the Lean Production System (LPS), is an advanced mode for production organisation and management created by Toyota Motor Corporation, Japan, aims to eliminate waste and reduce costs through the improvement of activities based on the Just-In-Time (JIM) methodology and automation. It is an effective tool for improving process efficiency with the core concept of waste elimination and continuous improvement.5,6 With a unique meaning in TPS theory, waste may be simply explained in terms of the medical field as all behaviours that are not helpful to patients or conducive to their diagnosis and treatment or recovery. TPS was first applied to the management of manufacturing processes and then gradually introduced to other industries. In medicine, it has been applied to the management of health care sub-domains like surgery and cardiovascular disease treatment.7,8
At present, the application of TPS in intrahospital transport for critically ill patients is still at a nascent stage and relevant systematic specifications have yet to be formed.9 Improving the quality of intrahospital transport for patients through TPS may reduce unnecessary waiting time for patients, lay a solid foundation for definite diagnosis as well as timely and efficient treatment, and reduce the risk associated with transport and potential disability of patients. For various departments, it may optimise transport and handover processes, overcome difficulties in critical links, standardise the transport process itself, and reduce adverse events in emergency care, thereby promoting its overall quality and safety. For hospitals, it may improve work efficiency and the quality of medical services, as well as build doctor-patient trust. In doing this, TPS can also speed up the turnover of beds, improve the economic benefit to hospitals, and assist them in maintaining a good reputation with their patients. In this study, TPS was integrated into all links of intrahospital transport for critically ill patients to shorten the time, improve the quality, and guarantee the safety of intrahospital transport for critically ill patients, thus achieving doctor-patient satisfaction and effective escorting for patient safety and satisfaction in their medical treatment, as reported below.
Subjects and Methods
Subjects
In June 2021, our department completed improvement work concerning advancing the quality of intrahospital transport for critically ill patients via the implementation of TPS. Between April and June 2021, 68 critically ill patients were transported to corresponding wards, while 63 critically ill patients were transported to corresponding wards between July and September 2021. The pre-TPS management group included 30 cases based on their propensity score, including 17 males with an average age of 55 years (range: 47 ~ 89 years) and 13 females with an average age of 56 years (range: 47 ~ 90 years). After the introduction of TPS management, 30 critically ill patients who experienced emergency intrahospital transport, served as the post-TPS management group. This group included 15 males with an average age of 56 years (range: 48 ~ 88 years) and 15 females with an average age of 55 years (range: 48 ~ 89 years). Typically, the term ‘critically ill patients’ refer to those patients with conditions that are urgent and life-threatening, for which medical attention should be given as soon as possible; otherwise, life may be at risk, serious impairment of vital organ functions may occur, or vitals may become unstable and deteriorate. For specific criteria, please refer to the “Standards and Guidelines for Diagnosis and Treatment of Critically Ill Patients requiring Emergency Treatment” (Document No. 32, 2013, issued by the National Health Office).10
Study Flowchart
Figure 1 presents the TPS implementation process for improving the quality of emergency intrahospital transport for critically ill patients.
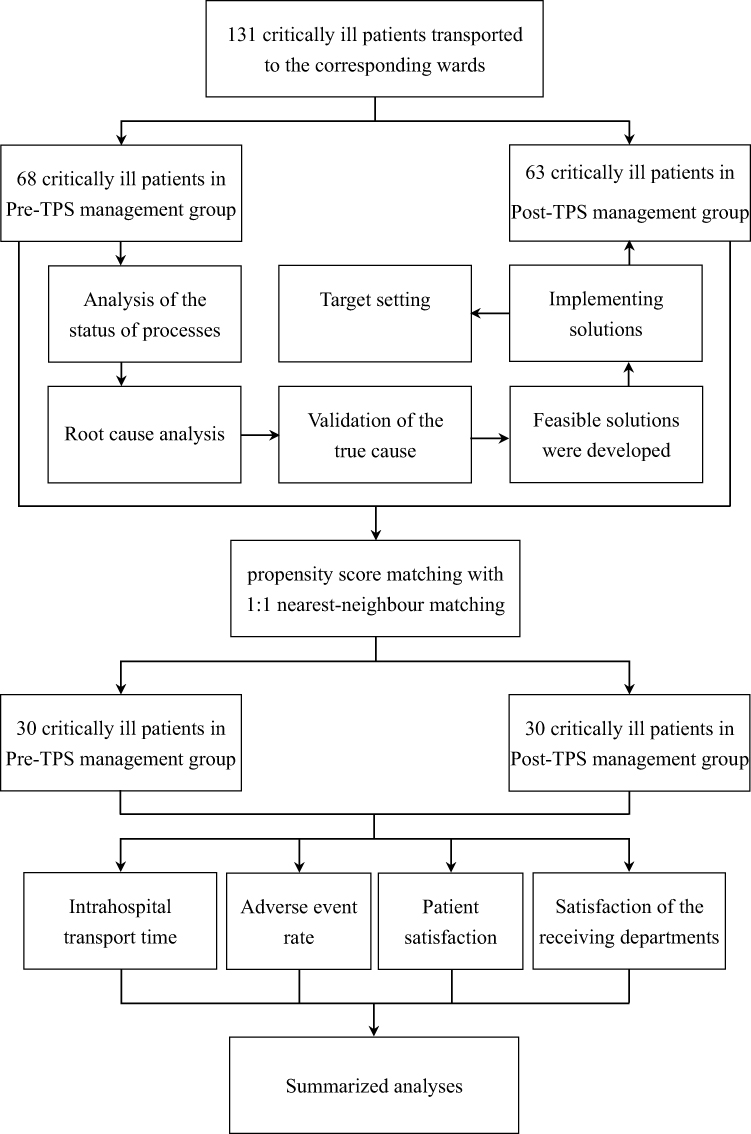 |
Figure 1 Process of using TPS to improve the quality of emergency intrahospital transport for critically ill patients. |
Methods
Problem Analysis and Topic Determination
The TPS improvement team consisted of emergency nurses, hospital logisticians, and the nursing department. All of the medical staff involved were certified to work in the emergency department and had more than 3 years experience working there. Besides, there was no turnover of emergency medical staff before and after the implementation of TPS management, for the intrahospital transport process of critically ill patients. At first, the Likert rating scale was used to investigate the satisfaction of the family members of critically ill patients, identify any problems that existed in the intrahospital transport of critically ill patients, and collect relevant suggestions. After discussions, the team reached a consensus that it is necessary to improve the quality of intrahospital transport for critically ill patients. Sudden changes of condition for critically ill patients during intrahospital transport are rare in our hospital, so any improvement should focus on shortening intrahospital transport time for them.
Assessment of the Current Situation
First, the flow chart of emergency intrahospital transport procedures for critically ill patients was plotted, then each process was classified and defined according to direct value, indirect value, and no value. Next, the time spent on the process was calculated and the summary was created. For a specific analysis of the processes, see Table 1.
 |
Table 1 Intrahospital Transport Time for Critically Ill Patients Before and After TPS Management |
Analysis of the Process Status
In the analysis of the status of TPS processes, each step was classified according to different values and calculated for value efficiency and process efficiency with the following formulas: Process efficiency = valuable steps/total steps ×100%; Value efficiency = valuable time/total process time ×100%, as shown in Table 2.
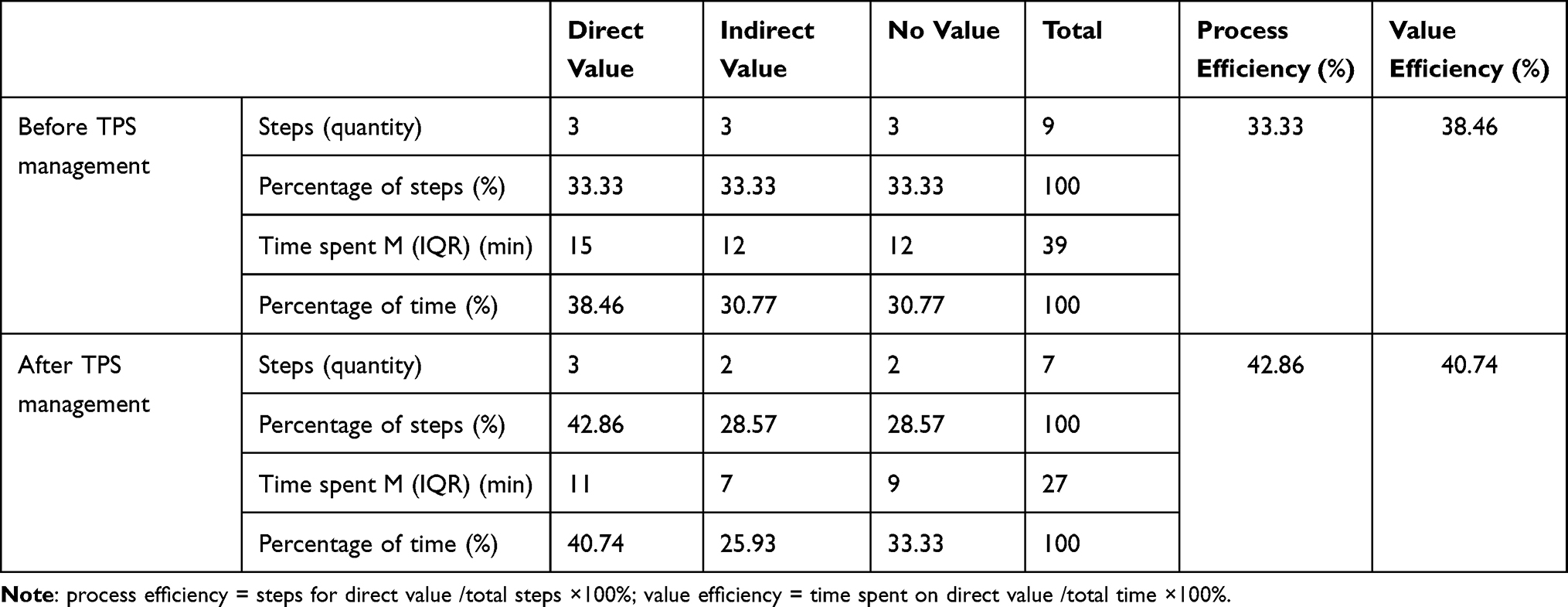 |
Table 2 Situation of Transport Process for Critically Ill Patients Before and After TPS Management |
Target Setting
Intrahospital transport time for critically ill patients was shortened as a means of guaranteeing their safety during intrahospital transport. Considering that there was no specific provision for this in the “Evaluation Criteria for General Hospitals of Zhejiang Province” (2019 edition)11 or relevant authoritative guidelines, the target of this study is set as follows: The intrahospital transport time after the introduction of TPS management is less than before TPS management and the difference is statistically significant. In the calculation, the “standard intrahospital transport time” for a critically ill patient is defined as the time from when the doctor issues the medical advice for admission to the time when the target department has received the patient.
Root Cause Analysis
An analysis of the pre-TPS intrahospital transport data of 68 critically ill patients found that the intrahospital transport time for critically ill patients was 39 minutes (median), which left a great deal of room for improvement. The time spent on ward preparation - 11 minutes (median) -was the longest, followed by waiting for an elevator at 5 minutes (median), and transport time at 6 minutes (median).The project members, clinicians, and staff of relevant departments were summoned for multiple rounds of brainstorming and a method based on the fishbone diagram was used to identify the relevant causes from five aspects: staffing, equipment, method, environment, and material. Subsequently, a 5Whys analysis12 was used to find the root causes of the problem. At last, five root causes were identified as follows: long waiting times for elevators, delayed arrival of hospital nursing workers, long times spent on admission procedures, inadequate preparation of relevant materials, and unreasonable transport routes.
Determination of Solutions
Feasible solutions were developed based on the five root causes according to the actual conditions of the hospital.
(1) Reasonable arrangement of elevators for transport: Through communicating with the relevant departments, the surgical elevators were taken as the preferred elevators for transport, with others reserved for backup. The relevant elevator operators were notified to wait by the phone while transport and logistics supervisors were contacted to prioritise the transport of emergency patients and strengthen the training of elevator managers, thus reducing the elevator waiting times. (2) Scientific arrangement of transport workers: Logistics companies were contacted to arrange the schedules of experienced workers in the emergency department responsible for transport and other relevant work, as well as reasonably organise the transportation workers so that they were on duty at any given time even if they were responsible for other work. At the same time, contingency plans were arranged. It was determined that every worker should be made to pass relevant tests before employment and that there should be regular training for improving the quality of transport. (3) Optimisation of admissions procedures: The emergency room cashiers were tapped as supplements for admissions procedures related to critically ill patients, and the admissions agents and green channels were opened for critically ill patients with administrative difficulties. The test and CT report sheets were pre-printed for the emergency patients to save time and information technology was used to simplify the materials required for admission. (4) Standardisation of workflow: The transport instruments and medical equipment in the clinical departments were managed based on the McKinsey 7S Model, and transport ECG monitoring was replaced with a specialised ECG monitoring transport module. Before transport, the receiving department was to be notified by phone of the handover patient’s condition, and relevant items were to be prepared. The transport system was revised to become more authoritative and practical after standardisation. The training and teaching work for new employees was strengthened to improve their professional skills. (5) Opening of transport channels: The connecting corridor on the second floor was opened as the emergency passageway for transport. After negotiating with the logistics company, routine hospital access patrol was strengthened so that the transport access is never blocked.
Observational Indexes
The transport time for acute or critically ill patients = time spent on completion of emergency hospitalization handover-time spent on the issuance of medical advice for admission by the relevant doctor; process efficiency = steps for direct value /total steps ×100%; value efficiency = time spent on direct value /total time ×100%; patient satisfaction = number of satisfied patients/total number of patients under investigation ×100% based on the follow-up results; satisfaction of the receiving departments = number of patients satisfied with the receiving department/total number of patients under investigation ×100%, based on an overall evaluation on the receipt. Adverse events are defined as accidents that lead to the suspension of transport and necessary emergency treatment of patients, eg, dropping of the ECG monitoring module, slippage or blockage of the infusion tube, insufficient oxygen supply, or accidental extubation during transport.
Statistical Analysis
SPSS26.0 software was used for data processing and the Shapiro-wilk normality test was used for analysing the distribution of data. For normal distributions,  ±s was adopted, while non-normally distributed data were represented by M (IQR).Besides, for inter-group comparisons of normal distribution, the t-test was used. The rank-sum test was used for an inter-group comparison based on non-normal distributions and the chi-square test or Fisher’s exact probability method was used for the rate comparison. The propensity score matching (PSM) method was used for balancing the effects of the two sets of covariables on intrahospital transport, thereby eliminating selection bias caused by confounding factors. Additionally, a logistic regression analysis was used to calculate the propensity score. The 1:1 nearest neighbour matching method was adopted, with calliper= 0.05 as the matching tolerance. If P<0. 05, there was statistical significance.
±s was adopted, while non-normally distributed data were represented by M (IQR).Besides, for inter-group comparisons of normal distribution, the t-test was used. The rank-sum test was used for an inter-group comparison based on non-normal distributions and the chi-square test or Fisher’s exact probability method was used for the rate comparison. The propensity score matching (PSM) method was used for balancing the effects of the two sets of covariables on intrahospital transport, thereby eliminating selection bias caused by confounding factors. Additionally, a logistic regression analysis was used to calculate the propensity score. The 1:1 nearest neighbour matching method was adopted, with calliper= 0.05 as the matching tolerance. If P<0. 05, there was statistical significance.
Results
Comparison of Transport Time for Critically Ill Patients Before and After TPS Management
The Shapiro-wilk normality test was used to analyse the time spent on each process as well as the total time used for critically ill patients. The results showed that all of the data were of non-normal distribution and could not be converted to normal distribution. The Mann Whitney U-test was used for inter-group comparison. There was no difference (P > 0.05) for the time spent on issuing medical advice by relevant doctors, review by nurses, informing the patients of relevant conditions and risks and signing, and severity evaluation. The time spent on the remaining steps and the total time for all processes was significantly reduced (P < 0.05).Due to process improvements, a comparison for before and after the implementation of TPS management could not be performed for two of the steps, ie, ward preparations and waiting for nursing staff. (Table 1).
Analysis of the Current Transport Process Situation for Critically Ill Patients Based on TPS Management
Two steps, ward preparation and waiting for nursing staff, were removed after TPS management. Based on an accurate calculation with the formulas of process and value efficiency, process efficiency increased by 9.53%, from 33.33% before TPS management to 42.86% after TPS management, and value efficiency increased by 2.28%, from 38.46% before TPS management to 40.74% after TPS management (Table 2).
Propensity Score Matching Results Before and After TPS Management
The PSM method was used to analyse the covariables of the two groups before and after TPS management was implemented. It was performed according to the effects of different characteristics on intrahospital transport in critically ill patients. Results showed that before matching there were significant differences in transport grade, gender, age, and history of malignancy between the two groups, but not for hypertension and diabetes history. However, after matching, the levels were very similar for all characteristic variables between the two groups of critically ill patients. Besides, the differences in characteristics between the samples were reduced significantly, indicating a good matching effect (Table 3).
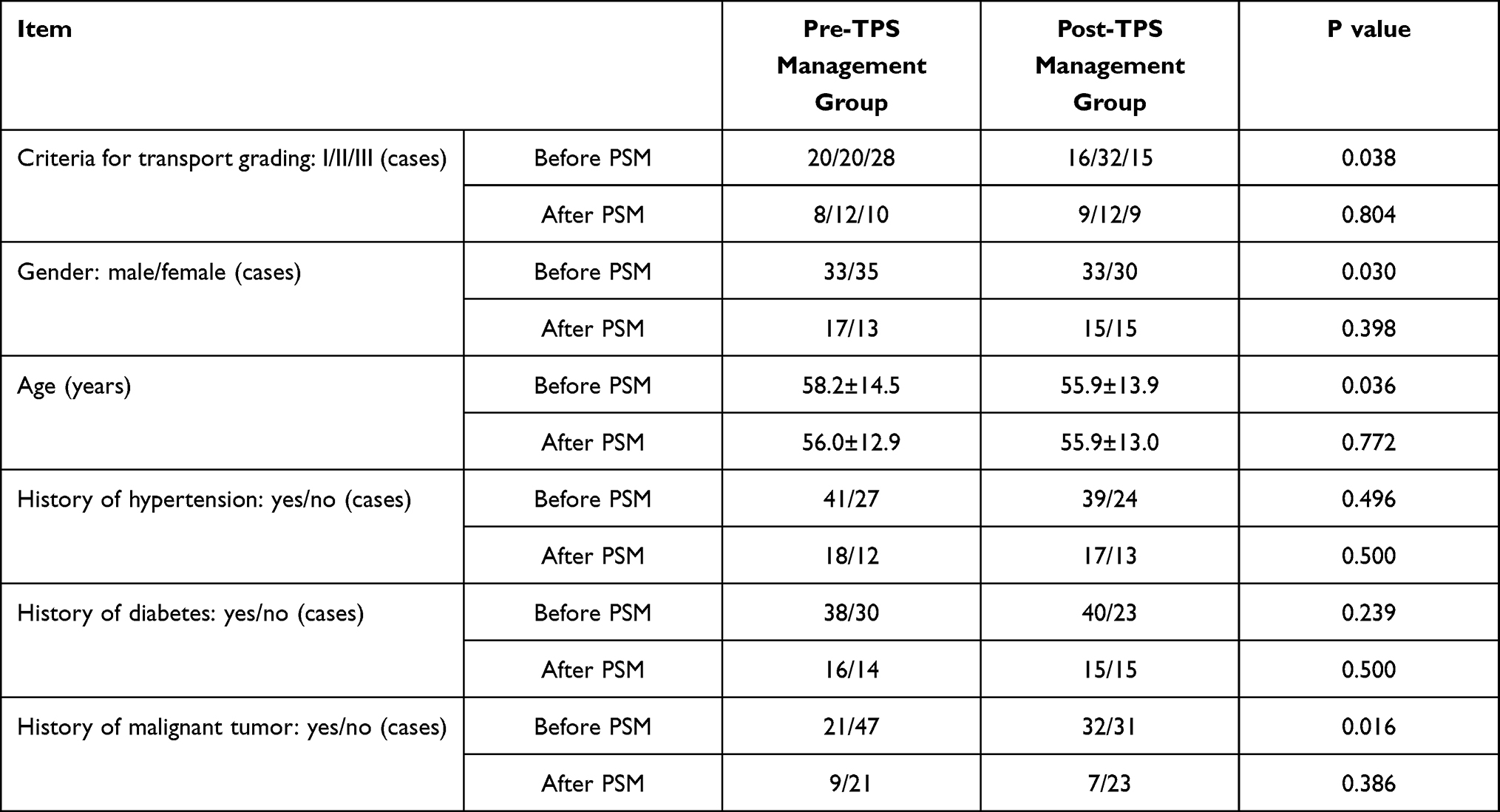 |
Table 3 Comparison Between Groups Before and After PSM Balancing |
Evaluation of the Overall Effect of TPS Management on the Transport of Critically Ill Patients.
The intrahospital transport time for critically ill patients after TPS management was 27 minutes (median), which was significantly shorter than the previous median time of 39 minutes, and the difference was statistically significant (P <0.05). The adverse event rate decreased from 13.33%, pre-TPS to 3.33%, post-TPS (P>0.05), but the difference was not statistically significant. The satisfaction rate of receiving departments and patients increased by 23.34% and 20.00%, respectively, from 73.33% and 76.67% before TPS management to 96.67% and 96.67% after TPS management. Moreover, these differences all had statistical significance (P<0.05) (Table 4). A comprehensive evaluation showed that TPS management not only achieved the expected goals but also brought added value such as high satisfaction rates and a low occurrence of complications (Figures 2 and 3).
 |
Table 4 Comparison of Satisfaction of Receiving Departments and Patients Before and After TPS Management |
 |
Figure 2 Intrahospital transport time and adverse event rate for critically ill patients during intrahospital transport before and after TPS management. Note: (A) Intrahospital transport time; (B) adverse event rate. |
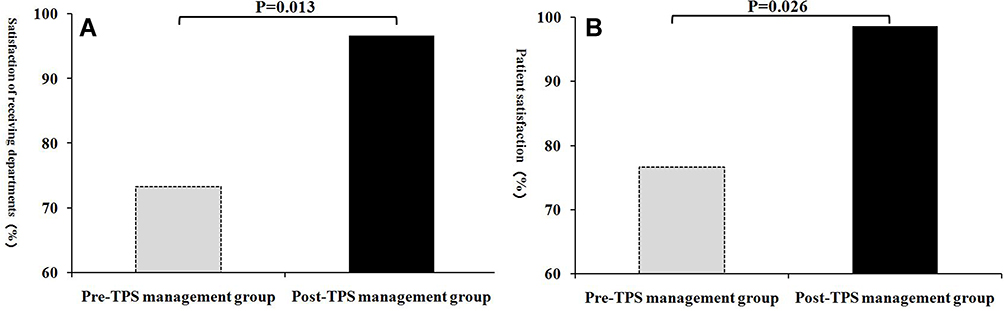 |
Figure 3 Satisfaction concerning emergency intrahospital transport for critically ill patients before and after TPS management. Note: (A) Satisfaction of receiving departments; (B) patient satisfaction. |
Discussion
In various industries, TPS management may be used for the improvement of quality and reduction of inefficiencies and costs. In a health system, TPS is believed to improve the quality of care by focusing attention on individual patients.13 TPS is a continuous quality improvement process based on data, and whether these relevant data can be objectively collected and scientifically analysed or not is the primary factor for the successful completion of relevant projects.14 Therefore, for this topic, detailed original data for intrahospital transport of 68 critically ill patients between April and June 2021 were collected for an in-depth analysis of each step, and the overall process, according to the workflow. As a result, six steps, including handling admission procedures, looking for nursing staff, and waiting for elevators, were found to pose issues. Time spent looking for nursing staff and ward preparation were both removed because these two steps may be taken as routine work, while the other four steps could be further optimised to derive a new process that was similar to the practices of Raab SS.15 Detailed process analysis is a key to reflecting the core idea of TPS (eliminating or reducing waste without value, shortening working hours and improving product quality), as well as the basis for quality improvement, which is related to the success of the entire project. For steps to be improved, a systematic analysis integrating continuous quality management tools (quality control circle, fishbone chart and 5Whys method) found five root causes, for which feasible solutions were subsequently developed. At last, four key indexes (transport time, patient satisfaction, satisfaction of receiving departments and adverse event rate) of intrahospital transport quality for critically ill patients were calculated. Based on scientific evaluation, TPS may significantly improve the quality of emergency intrahospital transport for critically ill patients.
The “Consensus on Intrahospital Transport for Critically Ill Patients”, released by the Chinese Association of Emergency Medicine, recommends a standardised transport classification scheme,16 but the time for guidance is not provided. Thus far, relevant international literature has not been retrieved; therefore, the target for this study is set as follows: the difference in intrahospital transport time before and after TPS management is statistically significant (the intrahospital transport time after TPS management is less than before TPS management was implemented). GeLF17 used the Healthcare Failure Mode and Effect Analysis (HFMEA) to improve intrahospital transport for critically ill patients. According to the results, the transport time was 46.82±7.32 minutes before improvement, and 22.63±3.48 minutes after improvement. In addition, Wang X J et al18 reduced the intrahospital transport time for critically ill patients from 7.61±1.34 minutes to 6.39±1.35 minutes by modifying the transport support. This study has shown that, through TPS management, the intrahospital transport time for critically ill patients may be shortened significantly (transport time P50 before TPS management:39 minutes, reduced to 27 minutes after TPS management). This result was similar to the results of GeLF17 and Wang X J18 et al, but there was a difference in the degree of improvement, which may be caused by inconsistencies in measuring the beginning and end of the transport time, as well as differences in transport time distribution, the actual situation of hospitals, and the use of management tools. These studies shortened the transport time for critically ill patients by merely a single measure, while this study comprehensively used a variety of means for whole-process optimisation. Therefore, the results of this study are superior to the others.
TPS management not only significantly shortened the intrahospital transport time for critically ill patients but also enhanced the patient satisfaction rate from 76.67% to 96.67%, which was generally consistent with the reports of GeLF. The improvement in patient satisfaction was an indirect indication that the overall level of intrahospital transport service and patient safety was improved. However, considering that the patients were not medical professionals, and, thus, could not be evaluated in terms of transport for critically ill patients, this study added an evaluation for receiving departments regarding the patient transport process. This was to fill in the pre-existing gaps in professional evaluation. This study showed that the satisfaction rate of receiving departments after TPS management increased by 23.34% (73.33% before TPS management vs 96.67% after TPS management), and the adverse event rate decreased from 13.33% before TPS management to 3.33% after TPS management, indicating a downward trend. However, there was no statistical significance in the differences, which may be related to the small sample size. Despite this, it may still provide evidence for the improvement of intrahospital transport quality for critically ill patients. Therefore, TPS management may improve the intrahospital transport service for critically ill patients while significantly advancing the transport quality. In this study, two satisfaction ratings and one adverse event rating were used for the evaluation of quality regarding intrahospital transport for critically ill patients, which was superior to the evaluation of Fu S et al19 based on simple patient satisfaction. The limitations of this study are as follows: First, the sample size is small and the effectiveness of TPS should be evaluated using a larger sample size. Second, the effect of each corrective action should be analysed and evaluated for determining their effectiveness, which is the next step of this study.
Conclusion
To sum up, we integrated the TPS method into the entire process of intrahospital transport for critically ill patients, allowing everyone from ordinary nursing staff to relevant departments to be involved in continuous improvement. This allows for constant discovery, analysis and problem solving while encouraging the concept of continuous improvement to permeate into the consciousness of every employee. By standardising and sustaining transport for critically ill patients, the intrahospital transport time for critically ill patients may be shortened greatly and the quality of transport may be improved significantly. Furthermore, a good reputation may be established for relevant hospitals in a way that promotes their overall development. In addition, for this project, the realisation of short-term goals is not the end of our improvement activities; that is, there should be continuous improvements of new processes featuring increasing rationalism and advanced work efficiency, thereby truly improving the quality of transport for critically ill patients and reducing the waste of medical resources.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Hangzhou Linping Hospital of Integrated Traditional Chinese and Western Medicine (No.202203182057000084848).This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Yang Z, Song K, Lin H, Li C, Ding N. Factors Associated with Emergency Department Length of Stay in Critically Ill Patients: a Single-Center Retrospective Study. Med Sci Monit. 2021;27:e931286. doi:10.12659/MSM.931286
2. Mathews KS, Durst MS, Vargas-Torres C, Olson AD, Mazumdar M, Richardson LD. Effect of Emergency Department and ICU Occupancy on Admission Decisions and Outcomes for Critically Ill Patients. Crit Care Med. 2018;46(5):720–727. doi:10.1097/CCM.0000000000002993
3. Mantha Y, Harada R, Hieda M. Management of Common Cardiovascular Emergencies in Critically Ill Patients. Heart Fail Clin. 2020;16(2):153–166. doi:10.1016/j.hfc.2019.11.001
4. Kisorio LC, Langley GC. Critically ill patients’ experiences of nursing care in the intensive care unit. Nurs Crit Care. 2019;24(6):392–398. doi:10.1111/nicc.12409
5. Radhakrishnan NS, Singh H, Southwick FS. Teaching novice clinicians how to reduce diagnostic waste and errors by applying the Toyota Production System. Diagnosis. 2019;6(2):179–185. doi:10.1515/dx-2018-0081
6. Liston DE, Richards MJ, Karl HW. Adapting the Toyota production model to teach systems-based practice to anesthesiology fellows. J Clin Anesth. 2017;38:87–88. doi:10.1016/j.jclinane
7. Harolds JA. Quality and Safety in Healthcare, Part LXXXIX: principles of the Toyota Production System. Clin Nucl Med. 2021. doi:10.1097/RLU.0000000000003761
8. Leming-Lee T, Polancich S, Pilon B. The Application of the Toyota Production System LEAN 5S Methodology in the Operating Room Setting. Nurs Clin North Am. 2019;54(1):53–79. doi:10.1016/j.cnur.2018.10.008
9. Williams P, Karuppiah S, Greentree K, Darvall J. A checklist for intrahospital transport of critically ill patients improves compliance with transportation safety guidelines. Aust Crit Care. 2020;33(1):20–24. doi:10.1016/j.aucc.2019.02.004
10. Circular of the General Office of the National Health and Family Planning Commission on issuance of “Standards and Guidelines for Diagnosis and Treatment of Critically Ill Patients requiring Emergency Treatment”. Bulletin of the National Health and Family Planning Commission of the People’s Republic of China. 2013;11:29
11. Health Commission of Zhejiang Province. The “Evaluation Criteria for General Hospitals of Zhejiang Province”. Health Commission of Zhejiang Province. 6. 2019.
12. Cai R, Fei Y, Li X, Xu L, Wu CL, Wu N. Research on the Effect of 5Why-Based Nursing Intervention in Blood Purification Nursing. J Healthc Eng. 2021;2021:6535238. doi:10.1155/2021/6535238
13. Cress P, Fiala T. Adapting the Toyota Production System in Plastic Surgery Practices to Improve Practice Management and the User Experience (UX). Aesthet Surg J. 2022;sjac001. doi:10.1093/asj/sjac001
14. Breen LM, Trepp R, Gavin N. Lean Process Improvement in the Emergency Department. Emerg Med Clin North Am. 2020;38(3):633–646. doi:10.1016/j.emc.2020.05.001
15. Raab SS, Andrew-Jaja C, Condel JL, Dabbs DJ. Improving Papanicolaou test quality and reducing medical errors by using Toyota production system methods. Am J Obstet Gynecol. 2006;194(1):57–64. doi:10.1016/j.ajog.2005.06.069
16. Jian G, Xiaoxue H, Jun X. The “Consensus on Intrahospital Transport for Critically ill patients Ill Patients” – standardised scheme for graded transport[J]. Chin J Em Med. 2017;5:512–516.
17. Lingfang G. Application effect of HFMEA mode in intrahospital transport for critically ill patients ill patients. Int J Nursing. 2020;1:19–2521.
18. Xianjiang W, Jie H, Dongmei Y, Yunchao S. Application of folding transport support in intrahospital transport for critically ill patients [J]. Chin Critical Care Em Med. 2020;9:1125–1127.
19. Fu S, Wu XG, Zhang L, Wu LF, Luo ZM, Hu QL. Service Quality Improvement of Outpatient Blood Collection by Lean Management. Patient Prefer Adherence. 2021;1:37–1543. doi:10.2147/PPAS320163
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.