")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Improving Newborn Health in Countries Exposed to Political Violence: An Assessment of the Availability, Accessibility, and Distribution of Neonatal Health Services at Palestinian Hospitals
Authors Massad S , Tucktuck M , Dar Khawaja R, Dalloul H, Abu Saman K , Salman R, Kafri R , Khammash H
Received 2 July 2020
Accepted for publication 18 August 2020
Published 13 November 2020 Volume 2020:13 Pages 1551—1562
DOI https://doi.org/10.2147/JMDH.S270484
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Salwa Massad,1 Marina Tucktuck,2 Ranin Dar Khawaja,3,4 Hadil Dalloul,1 Khalid Abu Saman,1 Rand Salman,1 Rawan Kafri,1 Hatem Khammash5,6
1Research Unit, Palestinian National Institute of Public Health, Ramallah, Palestine; 2School of Medicine, St. George’s University, Grenada, West Indies; 3Epidemiology and Public Health, Swiss Tropical and Public Health Institute (Swiss THP), Basel, Switzerland; 4Faculty of Medicine, University of Basel, Basel, Switzerland; 5Neonatology Department, Makassed Hospital, Jerusalem, Palestine; 6Pediatric Department, Al-Quds University, Jerusalem, Palestine
Correspondence: Salwa Massad
Research Unit, Palestinian National Institute of Public Health, Ministry of Health Building, 1st Floor, Qadora Street, Ramallah, Palestine
Tel +970 2 296 6842/7
Fax +970 2 296 6852
Email [email protected]
Introduction: Geopolitical segregation of Palestine has left a fragile healthcare system with an unequal distribution of services. Data from the Gaza Strip reflect an increase in infant mortality that coincided with a significant increase in neonatal mortality (12.0 to 20.3 per 1000 live births).
Objective: A baseline study was carried out to evaluate available resources in neonatal units throughout Palestine.
Study Design: A cross-sectional, hospital-based study was conducted in 2017 using the World Health Organization’s “Hospital care for mothers and newborn babies: quality assessment and improvement tool.” Data on the main indicators were updated in 2018.
Results: There were 38 neonatal units in Palestine: 27 in the West Bank, 3 in East Jerusalem, and 8 in the Gaza Strip. There was an uneven geographic distribution of incubators in relation to population and births that was more marked in the Gaza Strip; 79% of the neonatal units and 75% of the incubators were in the West Bank. While almost all hospitals with neonatal units accepted very and extremely low birth weight and admitted out-born neonatal cases, there was a shortage in the availability of incubators with humidifiers, high-frequency oscillatory ventilation, mechanical ventilators with humidifiers and isolation wards. There was also a considerable shortage in neonatologists, neonatal nurses, and pediatric subspecialties.
Conclusion: Almost all the neonatal units accepted extremely low birth weight neonatal cases despite not being ready to receive these newborns due to considerable shortages in human resources, equipment, drugs, and essential blood tests, as well as frequent disruptions in the availability of based amenities. Together, these factors contribute to the burden of providing quality care to newborns, which is further exacerbated by the lack of referral guidelines and challenges to timely referrals resulting from Israeli measures. Ultimately, this contributes to suboptimal care for neonates and negatively impacts future health outcomes.
Keywords: neonatal services, Palestine, assessment, hospitals
Introduction
The neonatal period spans the first 28 days of a newborn’s life. It is considered an integral indicator of future child survival and well-being, 1,2 as well as sustainable social and economic development at the broader level.3 Globally, the neonatal mortality rate, defined as the probability of dying in the first 28 days of life, was 18 deaths per 1,000 live births in 2017. This included approximately 2.5 million newborns who died within the first month, with the highest percentage dying in the first week. Specifically, 36% died on the day they were born, and three-quarters died during the first week of life.3
Between 2000 and 2017, the neonatal mortality rate decreased by 41%. This decline was less than the reduction in the mortality rate among children aged 1–4 years old (reported as 60%).3 Despite the decrease in the neonatal mortality rate, there are two main problems with this trend: the rate of decline is slower than in any other reported period,2 and the reduction in the neonatal mortality rate has not been equal among different countries.2 Specifically, between 1990 and 2017, there was a 47% reported decline in the neonatal mortality rate in developing countries as compared to a 58% decline in developed countries.
Given the global burden of preventable neonatal deaths, neonatal health has become a priority under the United Nations Sustainable Development Goals (SDGs). SDG 3.2 urges all countries to reduce neonatal mortality to 12 neonatal deaths per 1,000 live births by 2030 (target 3.2.2). 2 Evidence indicates that a lack of accelerated action towards neonatal health will result in the death of 28 million newborns between 2018 and 2030.3 It is therefore imperative to identify, understand, and address the causes of neonatal death, especially in low- and middle-income countries.1 It is equally essential to identify and overcome barriers to effective case management to improve neonatal and child survival rates and formulate appropriate policies on child health and well-being.1
As it currently stands, the burden of neonatal mortality is unequally distributed across regions: it is most pronounced in low- and middle-income countries.4,5 where 99% of the neonatal deaths occur.6 Many factors contribute to this trend in neonatal morbidity and mortality. The first factor, which has been termed the 3-delays model, outlines three “delays” that impact pregnancy-related mortality and constitute major challenges to improving child survival rates. The 3-delays include a delay in recognizing a problem and seeking healthcare (low utilization of services); a delay in reaching the health facility; and a delay in receiving appropriate care at the health facility. A second factor is the migration of the health workforce from low-income to high-income countries, creating a disproportionate gap in the availability of health professionals. This gap is further exacerbated by a third factor, which is the lack of sufficient supplies, equipment, and resources to provide basic care to neonates and respond to projected needs, such as neonatal resuscitation. Other factors include a lack of prevention strategies that correspond to neonatal health needs; weaknesses in existing health systems in terms of equitable access to services; and inadequate knowledge, skill, and experience of healthcare workers to respond appropriately to neonatal health ailments.6
As a developing middle-income country, Palestine mirrors some of the same challenges faced globally in neonatal health. However, it is challenging to examine trends in neonatal mortality in the country because of the incompleteness of the national death registry.7 The neonatal mortality rate in Palestine in 2017 (11.3 deaths per 1000 live births) is underreported. According to the Palestinian Central Bureau of Statistics, the death registry was only 60.2% complete in 2013, primarily due to the underreporting of infant deaths, for which completeness in the death registry was estimated to be 25.6%.8 As a result, in 2013, while the reported infant mortality rate was 5.66 deaths per 1000 infants, the estimated mortality rate was 18.11 deaths per 1000 infants.8 Based on a 2015 United Nations Relief and Works Agency (UNRWA) study in the Gaza Strip (GS), where 67% of the population are refugees and are served by UNRWA, between 2008 and 2013, infant mortality increased from 20.2 per 1000 live births to 22.4 per 1000 live births. This change reflected a significant increase in the neonatal mortality rate (from 12.0 to 20.3 per 1000 live births, p = 0.01). The main causes of death were preterm birth, congenital anomalies, and infections.9
Significant challenges exist regarding the scaling up of service delivery and the enhancement of quality, integration, and continuity of neonatal care. Healthcare delivery in Palestine faces inequality resulting from disparities in the availability of healthcare services, which is due in part to the geopolitical segregation imposed by the presence of multiple checkpoints and the separation wall, as well as the inadequate distribution of services.10 The legislative and physical division of Palestine, in terms of both the separation of the GS from the West Bank (WB) and the fragmentation of the occupied WB, present major difficulties for the cohesiveness of the health system and access to staff, ambulances, patients, and patients’ relatives.11,12 East Jerusalem (EJ), has been isolated from the remainder of the WB and is under full control of Israel. For Palestinians living in the WB and GS, EJ is largely inaccessible. The GS has been under an illegal Israeli blockade for over 12 years. As such, the healthcare system in Gaza is comprised of captive clients who are entirely dependent on Israel, international bodies, and the aid industry for goods and services, with no means of independent development.13 In addition, the fragmented health sector with multiple actors often challenges effective alignment with the overall national health development agenda.14
This is the first study to assess neonatal services in Palestine that will be used as a baseline to inform policy with the goal of improving neonatal services as one of the strategies to reduce infant and neonatal mortality. It aims to assess the availability, distribution, and accessibility of neonatal health services in Palestinian hospitals.
Materials and Methods
Study Design and Setting
A cross-sectional, quantitative study was conducted at Palestinian hospitals from June to August 2016, and the main indicators were updated in August 2018. The study covered all Palestinian governmental, non-governmental, UNRWA, and private sector hospitals in the WB (including EJ) and GS that offer neonatal health services. The study survey was based on the international standardized tool: “Hospital care for mothers and new-born babies: quality assessment and improvement tool,” developed by the WHO and first published in 2009.15 The tool was used in many regions, including Africa, Europe, and the Middle East to evaluate the quality of care in hospitals, identify areas of improvement, and develop future action plans.6 The tool was adapted for the current study following consultations with experts in neonatal and pediatric care working in Palestine.
The fieldwork consisted of a preparatory phase and a data collection phase. During the first phase, a workshop was conducted with key health service providers, including heads of hospitals and heads of neonatal units or their representatives. During the workshop, the goal of the study and its importance as a baseline study at the national and hospital levels were presented, along with the risks and benefits of participating in the study. The data collection tool was introduced and feedback from the participating hospitals was considered in refining it. All hospitals from the workshop agreed to participate in the study, and informed oral consent was obtained after explaining the study objectives and measures to protect confidentiality, and giving them the right to decline from participating in the study. Each hospital assigned a focal point to coordinate with key persons in each hospital to collect the information in the study tool, as outlined below:
- A focal point from the administrative office to collect data on neonatal admission load, specific neonatal and delivery statistics, and neonatal medical admission causes in 2015
- Head nurse of the neonatal unit to examine availability and number of neonatal staff, specifically their shifts, credentials, and training, and the continuous availability of amenities (electricity, back-up power supply, diesel/gas, running water, hot water, heating and air-conditioning)
- Head physician of the neonatal unit to collect information on availability of beds, equipment, and supplies for hospitals and neonatal units, protocols and guidelines in delivery and neonatal departments, availability of basic and support facilities (isolation wards, facilities for mothers to breastfeed newborns, and facilities for breast milk expression)
- Pharmacist to examine the availability of drugs and total parenteral nutrition (TPN) for very sick neonates
- Lab supervisor in each hospital to collect information on available laboratory tests
The study was complied with the Declaration of Helsinki. To protect confidentiality, hospital identifiers were excluded from data analysis. Following the data collection phase, all personal identifiers of the interviewed health service providers who provided information for different sections of the tool were destroyed. There was no risk of breach of confidentiality for individual hospitals as data pertaining to each hospital was only included in the individual reports, which were sent to each hospital separately. The data presented in this paper include aggregated data from all the participating hospitals. The study proposal and the verbal informed consent process was approved by the Ministry of Health Ethical Review Committee in January 2016.
Outcome Measures
The main outcome measures of the study were:
- Number of deliveries, neonatal admissions, and referrals in 2016 (collected from registries available at the hospitals)
- Availability of
- Facilities: NICU unit, emergency department, isolation ward, facility for out-born admission
- Services: in-born admission, out-born admission, very low birth weight admission, extremely low birth weight admission
- Human resources
- Equipment and supplies
- Drugs and nutrition essential for neonatal care
- Laboratory tests essential for neonatal care
- Protocols and guidelines
- Distribution of neonatal health services by
- Geographic area (north, central, south of WB, EJ, and north, central, south of GS)
- Region (WB, EJ, and GS)
- Sector (governmental and non-governmental)
- Accessibility of neonatal health services by
- Geographic area (north, central, south of WB, EJ, and north, central, south of GS)
- Sector (governmental and non-governmental)
- Hospital level: An additional outcome measure was to identify a hospital levelling score for each neonatal unit in accordance with a regionalized care grading system for neonatal health services (basic neonatal care vs specialty neonatal care vs sub-specialty neonatal intensive care) (Table 1). The scoring was based on the “American Academy of Pediatrics, Guidelines for Perinatal Care, Seventh Edition,” and adapted to the Palestinian context.16 This score was used to assess neonatal unit readiness and its capability to accept referrals or its need to refer its neonates to another neonatal unit to ensure optimum neonatal care.
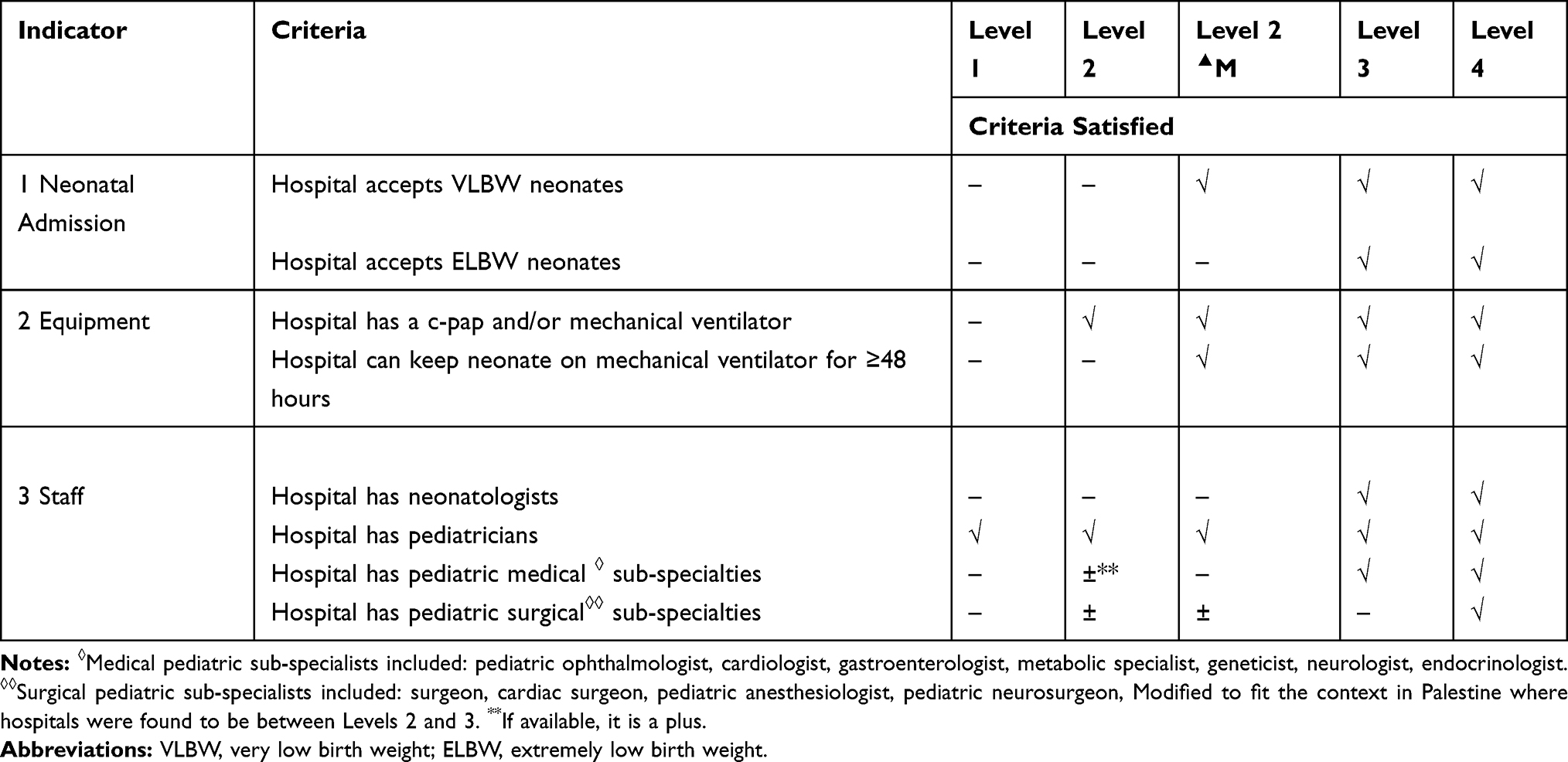 |
Table 1 Levelling Indicators and Criteria of Neonatal Units for Referral Program Guidelines, 2018 |
Statistical Analysis
Analyses were conducted at the hospital and neonatal unit levels. For descriptive categorical outcome measures, proportions (%) of the total number of neonatal units and of all hospitals, where appropriate, were computed. For categorical outcome measures, data were presented as proportions (%). For descriptive continuous outcome measures, data were presented in terms of absolute numbers or sums, where appropriate. Each outcome measure was stratified by region (WB excluding EJ, EJ, and GS), geographic area (north, central, and south of the WB, EJ, and north, central, and south of the GS), and sector (government or non-governmental). Descriptive data were presented to map the current situation of neonatal services in Palestine. The Statistical Package for the Social Sciences (SPSS) software, version 23 was used for data analysis.
Results
General Characteristics of Palestinian Hospitals Offering Neonatal Services
In Palestine, there were 60 delivery hospitals and 38 hospitals with neonatal health units. Around 60% (22/38) of hospitals with neonatal units were non-governmental. The south of the WB had fewer hospitals with neonatal units; almost half of the hospitals with neonatal units (14/30) were in the north of the WB. In the GS, only one hospital with a neonatal unit was located in the north, while the other seven hospitals with neonatal units were distributed in the middle and southern areas (see Figure 1).
 |
Figure 1 Availability of delivery units, neonatal units, and number of incubators in Palestine by region and geographic area, 2017. |
Burden of Maternal and Neonatal Healthcare
Large Number of Deliveries and Neonatal Admissions
Based on the registries available at the hospitals, the number of deliveries (normal and C-section) in Palestine for 2016 was reported to be 127,504 (66,696 deliveries in the WB, excluding EJ, 7424 in EJ, and 53,384 in the GS). This included a total of 29,160 (23%) C-section deliveries (16,703 (25%) in the WB, 1680 (23%) in EJ, and 10,777 (20%) in the GS). In addition, the neonatal admission load was reported to be 16,415 neonates (7880 in the WB excluding EJ, 1887 in EJ, and 6648 in the GS). The registers did not include indicators on whether admitted neonates were born within the hospital or referred from outside.
Neonatal Medical Admission Causes
The top causes of neonatal medical admission across the WB, including EJ, and the GS were transient tachypnea of the new-born (TTN), hyaline membrane disease (HMD), neonatal hyperbilirubinemia, neonatal sepsis, and prematurity. EJ hospitals also included congenital anomalies and metabolic diseases; however, these causes were not observed in hospitals in the WB and GS.
Readiness of Hospitals for the Provision of Neonatal Health Services
Facility Infrastructure
The study data indicated that 32/38 (22 in the WB (excluding EJ), 3 in EJ, and 7 in the GS) hospitals with neonatal units had an isolation facility/infectious cases ward. In addition, 18/38 (11 in the WB (excluding EJ), 2 in EJ, and 5 in the GS) hospitals with neonatal units had emergency department/beds for neonates, while only 9/38 (6 in the WB (excluding EJ), 0 in EJ, and 3 in the GS) hospitals with neonatal units had a ward/room for out-born neonatal admission.
Support Services
Almost all hospitals with neonatal units accepted both very low birth weight (VLBW, <1500 g) and extremely low birth weight (ELBW, <1000 g) neonatal cases: 25/27 neonatal units in the WB, and all neonatal units in EJ and the GS. Additionally, almost all hospitals with neonatal units admitted in-born neonatal cases: 26/27 in the WB (excluding EJ), 3/3 in EJ, and 6/8 in the GS. Furthermore, most of the hospitals with neonatal units admitted out-born neonatal cases: 25/27 in the WB (excluding EJ), 1/3 in EJ, and 8/8 in the GS.
Equipment
The study data indicated that there was a shortage in the availability of high-frequency oscillatory ventilation (HFOV) across hospitals in Palestine. Also, several hospitals in the WB and GS did not have mechanical ventilators with humidifiers (see Table 2).
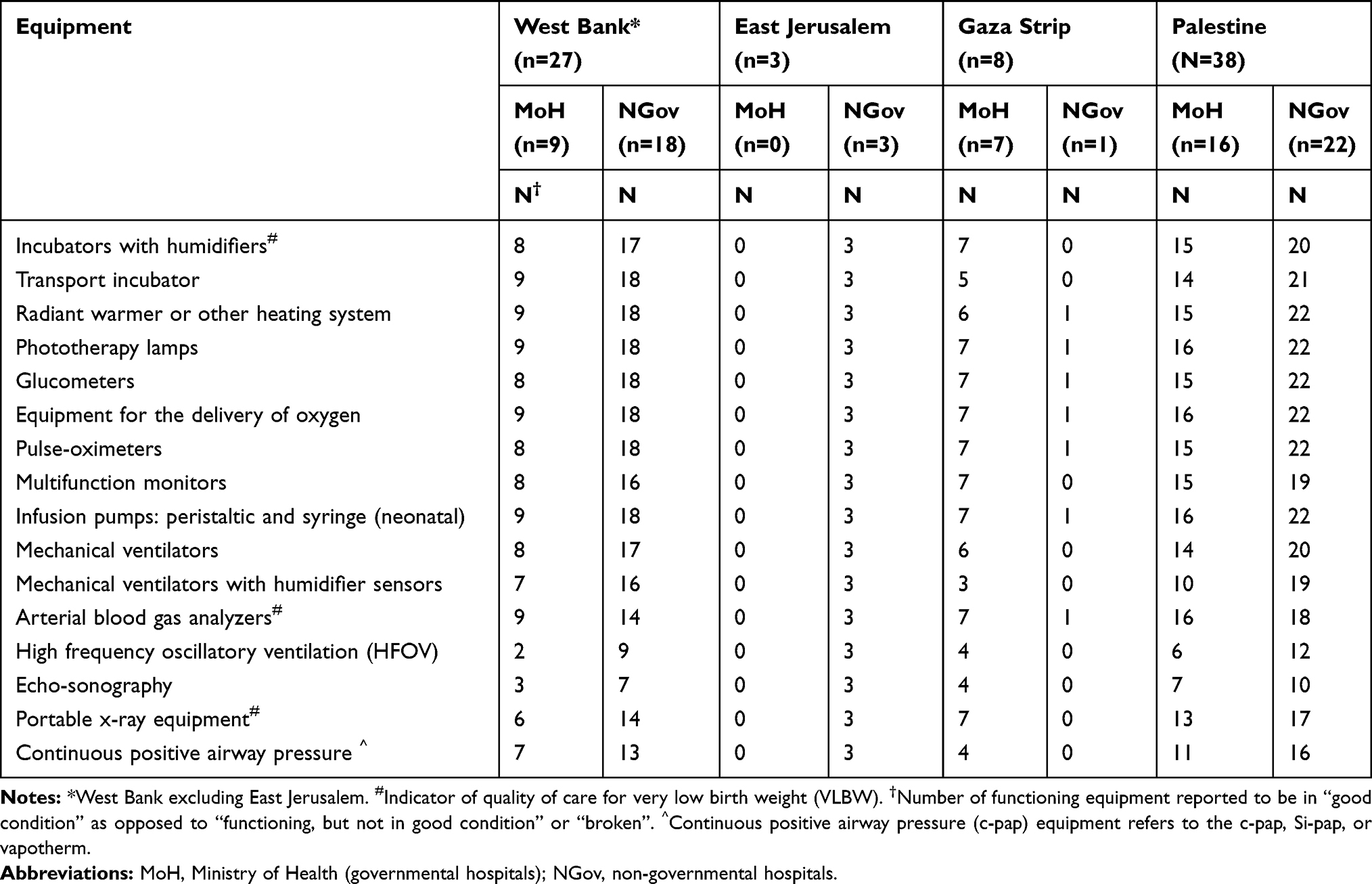 |
Table 2 Number of Neonatal Hospitals (N) with Available Functioning Equipment to Support Neonatal Health Stratified by Region (West Bank, East Jerusalem, Gaza Strip) and Sector (Ministry of Health, Non-Governmental Hospital) (N=38), 2018 |
As shown in Figure 2, there was an uneven geographical distribution of incubators in relation to population and births that was more marked in the GS; 79% of the neonatal units and 75.1% of the incubators were located in the WB.
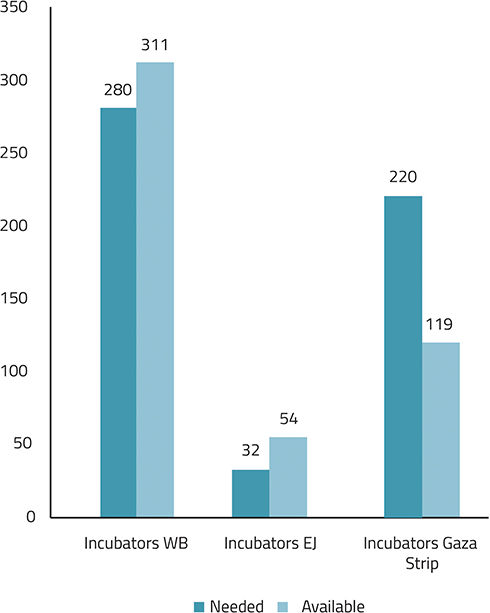 |
Figure 2 Number of neonatal beds needed and available by region, 2018. |
Human Resources
The total number of neonatologists reported in Palestine was 11, covering 15 full time/part-time posts: 6 in EJ, 4 in the WB, and 1 in the GS. Regarding the availability of pediatricians, there was a total of only 38 pediatricians who work in the eight neonatal intensive care units (NICUs) in the GS, while there were 85 pediatricians in the WB (excluding EJ), and 12 in EJ. There was a dearth in the availability of pediatric sub-specialists across all geographic areas in Palestine, especially in the GS and Ministry of Health (MoH, governmental) hospitals. In the GS, none of the hospitals with neonatal units had a pediatric orthopedic specialist, pediatric endocrinologist, pediatric nephrologist, pediatric metabolic specialist, pediatric pulmonologist, gastroenterologist, pediatric anesthesiologist, pediatric ophthalmologist, or pediatric cardiac surgeon.
Regarding the availability of specialized nurses, only 13.5% (86/637) of nurses working in neonatal units in Palestine were specialized neonatal nurses. Of the 86 neonatal nurses available in Palestine, 55 were in the WB and 31 were in EJ hospitals. There were no neonatal nurses in the GS. Only 21% of the nurses in the MoH units in the WB were specialized neonatal nurses qualified to work in neonatal units (see Table 3).
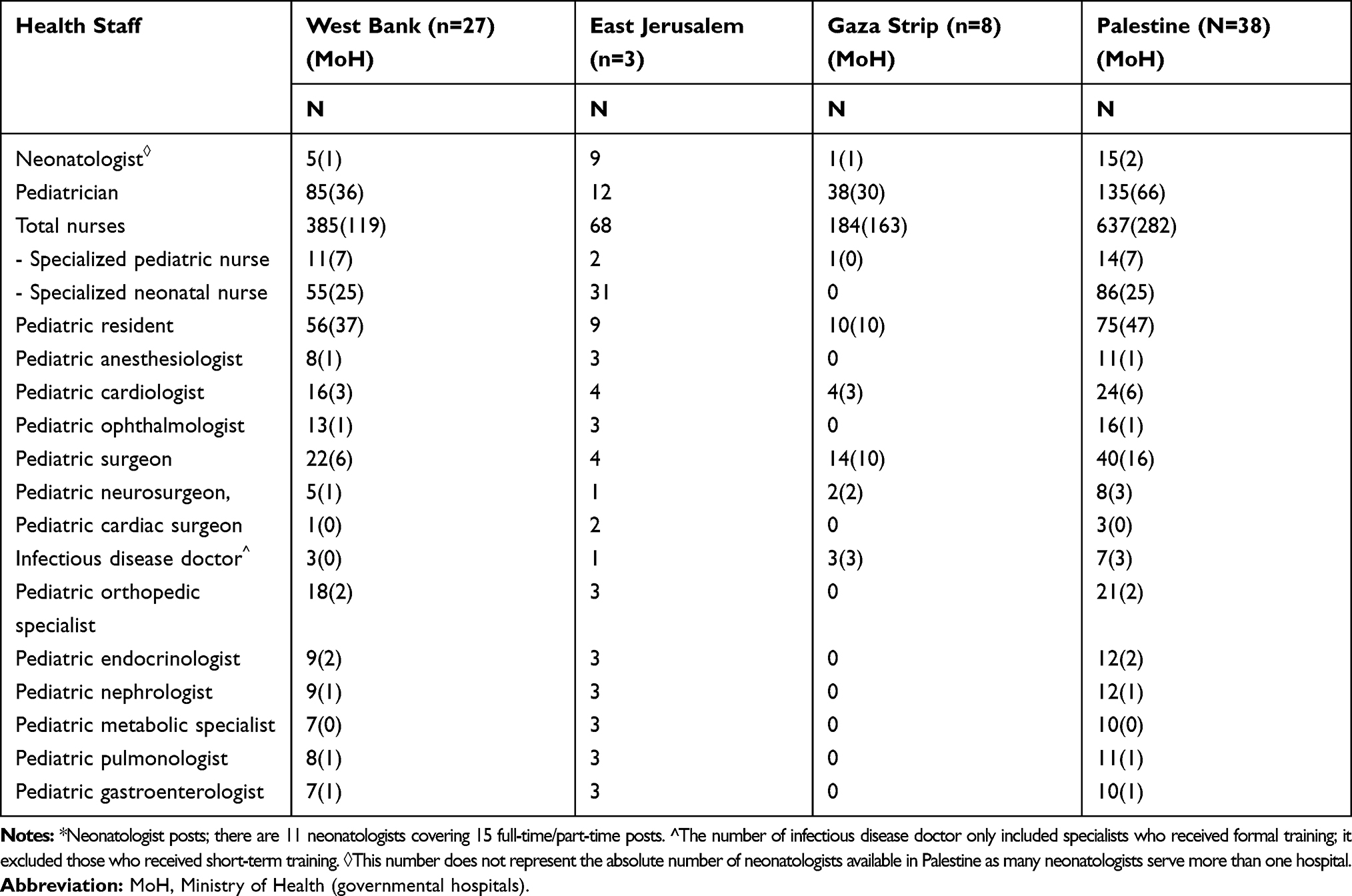 |
Table 3 Total Number (N) of Neonatal Staff per Neonatal Unit (Full Time/Part Time/Upon Request) by Region (West Bank, East Jerusalem, Gaza Strip) (N=38), 2018 |
Regarding the availability of neonatologists, pediatricians, and nurses for neonatal care, it was reported that 23/27 hospitals in the WB, 2/3 hospitals in EJ, and 6/8 hospitals in the GS had neonatologists/pediatricians on duty in the delivery ward and in other units at the hospital during their assigned shift in the neonatal unit. Also, 7/27 hospitals in the WB and 2/8 hospitals in the GS had nurses who were on duty in the delivery ward in the hospital during their assigned shift in the neonatal unit. Additionally, 9/27 hospitals in the WB and 1/8 hospitals in the GS had nurses who were available to other units at the hospital during their shifts in the neonatal unit.
Competency Assessment of Staff at the Neonatal Units
None of the neonatologists in the WB or GS had taken the neonatal resuscitation program (NRP). Almost one-fourth of nurses in the WB and EJ and only one out of the 174 nurses in the GS took the training. In EJ, half of the neonatologists and all pediatricians took NRP training. Pediatric advanced life support training was received by 22% of the neonatologists and 71% of the pediatricians in EJ, but none of the staff in the GS. A small number of nurses completed breastfeeding training in Palestine. Most of the training lasted for short periods of time ranging from a few days to several months.
Drugs
Neonatal units were assessed for the availability of essential antibiotics including ampicillin, ceftriaxone/cefotaxime, cloxacillin, and gentamicin. These essential antibiotics were not completely available in nine neonatal units in the WB and five neonatal units in the GS. Regarding the availability of infusion drugs (glucose 5%, glucose 10%, glucose 50%, glucose with sodium chloride, potassium chloride, sodium chloride 0.9% isotonic, and sodium bicarbonate), one hospital in the WB reported that it does not have all infusion drugs and none of the hospitals in the GS reported having all infusion drugs.
The study indicated that there was a shortage in acyclovir, amphotericin B, fluconazole, and vancomycin in all hospitals in Palestine. Only 9/27 hospitals in the WB, 2/3 hospitals in EJ, and 2/8 hospitals in the GS reported having all the drugs. In reference to the availability of caffeine citrate and surfactant, 11/27 hospitals in the WB and 7/8 hospitals in the GS reported that they did not have one or both of the essential medications.
Nutrition, Breastfeeding Facilities, and Materials
It was reported that not all of the hospitals with neonatal units in Palestine have facilities that were effectively designed to promote breastfeeding. Only 69% of governmental hospitals had a facility for expressing breast milk, versus 64% of non-governmental hospitals. There was also a shortage in the availability of parenteral nutrition, which is critical for very low and extremely low birth weight cases. A shortage of Total Parenteral Nutrition (TPN) elements was most pronounced in WB hospitals, but there was a shortage of vitamins and minerals for TPN across all geographic areas, except for EJ. TPN was only available in 29/38 neonatal units in Palestine.
Laboratory Tests
Essential blood tests, including blood glucose, hemoglobin, full blood count, blood gas analysis, blood bilirubin, renal function tests, and electrolytes, should be available in all neonatal units. In our study, only 22/27 hospitals in the WB and 7/8 hospitals in the GS had all essential blood tests. The study indicated that all blood bank tests, including Coomb’s test, blood grouping and cross-matching, rhesus antibodies, major blood groups and rhesus typing, and blood cross-matching were available in 24/27 hospitals in the WB, 2/3 hospitals in EJ, and 8/8 hospitals in the GS.
All hospitals in Palestine had all septic workup tests, including bacteriology (culture), urine culture, blood culture, cerebrospinal fluid culture, and urine analysis.
Protocols
Almost all hospitals that provide neonatal services in EJ have protocols. GS hospitals lacked protocols on the use and maintenance of equipment. The most common protocol sources were international, followed by local or hospital-based protocols, and national or MoH protocols. Of the protocols that followed international standards, the main sources were the American Academy of Pediatrics (AAP), the Harriet Lane Handbook, and the Nelson Textbook of Pediatrics.
Amenities
The results of the study indicated that basic amenities, including electricity, back-up power supply, running water, heating, and air-conditioning, were consistently available in only 19 of the 38 neonatal facilities in Palestine.
Levelling of Neonatal Units
Based on the study findings, the distribution of the hospital levelling score of the neonatal units was as shown in Figure 3. There was only one level 4 neonatal unit, located in EJ. In the GS, there was only two level 3 units, located in the middle area.
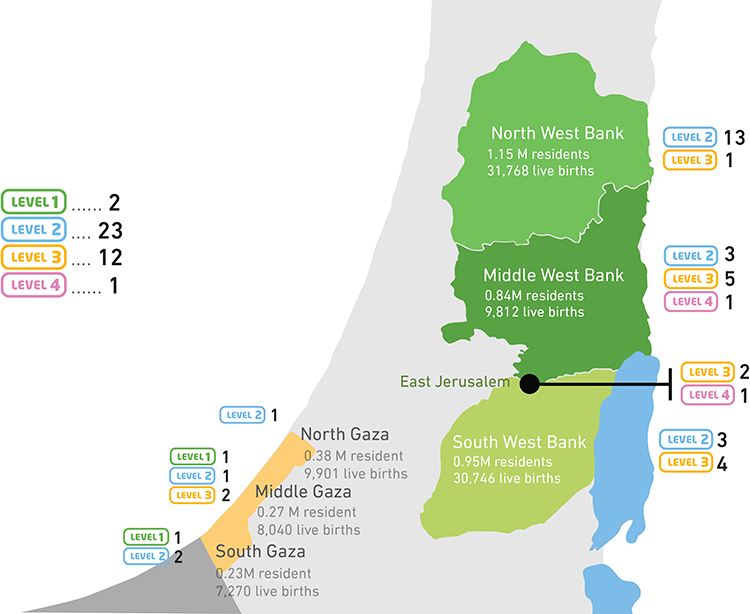 |
Figure 3 Geographic distribution of specialized neonatal services by proposed levelling system, 2018. |
Discussion
Our study found a shortage of resources, unequal distribution of neonatal services, and barriers to accessing neonatal services in Palestine. Together, these findings contribute to the burden of providing quality care to newborns, which is further exacerbated by the lack of referral guidelines to level 3 and level 4 hospitals. These factors compound the existing challenges posed by Israeli checkpoints and the separation wall in referring newborns in a timely manner. Ultimately, this contributes to suboptimal care to neonates and positive future health outcomes.
Availability of Facilities and Resources
While almost all neonatal units in both the WB and GS admit ELBW infants, many are not prepared to receive very sick and VLBW newborns due to the considerable shortage of neonatologists, neonatal nurses, pediatric subspecialty practitioners, equipment, drugs, and essential blood tests, especially in the GS. This category of infants requires at least level 3 NICU care with appropriate staff and resources, which must be considered when making referrals, even before birth in cases of antenatal diagnosis. Additionally, not all NICU units had portable incubators. To improve survival and health outcomes for referred cases, neonates need to be transported from the delivery room to wards, from the ward to other services within the hospital, and between hospitals using a transport incubator and with the support of a dedicated team capable of implementing life support for babies.
Additionally, most of the hospitals with neonatal units admit out-born neonatal cases despite not having a ward/room for out-born neonatal admission or isolation wards. Because the isolation of cases is the main infection prevention measure among newborns,17–19 the absence of isolation wards is a contributing factor for healthcare-associated infections.20 Furthermore, not all hospitals have TPN to support the nutrition of very sick newborns. If the preterm infant meets the criteria to receive TPN, then it should be administered immediately, ideally within 6 hours of birth.21
Regarding the availability of equipment, based on the American Academy Guidelines and the number of beds available, only the GS has a shortage of beds with only around half of the beds needed based on live births. This is reflected in the quality of care in neonatal units in Gaza and may affect the morbidity and mortality of neonates, especially tiny and sick ones. The low number of beds also results in overcrowding, with some units experiencing more than 150% occupancy. In addition, not all units have mechanical ventilators with humidification. Inappropriate humidification can lead to mucosal injury, desquamation of cells, excessive pulmonary secretion, and reduced vital capacity.14 These units may face difficulties caring for sick newborns and tiny babies who require prolonged ventilation. A blood gas analyzer and portable X-ray machine are also essential components for the management and monitoring of very sick newborns requiring mechanical ventilation.
Based on the study findings, basic amenities were consistently available in half the neonatal facilities in Palestine. However, basic amenities must be available at all times in neonatal units for ventilation, feeding, and care for sick and premature newborns. A lack of basic amenities exacerbates the shortage of neonatal beds, as an NICU bed cannot function and may put neonates at risk of morbidity and mortality. As a result, the remaining 19 facilities should be disregarded as providers of NICU, although this may also accentuate the lack of neonatal beds in Palestine.
Accessibility to Neonatal Services
Study findings indicate that there is an uneven distribution of neonatal units among different geographical areas in both the WB and GS. This has serious implications for access to care due to geopolitical segregation and the siege on the GS.22
In addition, most delivery and neonatal services are outside of the MoH. This significantly impacts the cost for neonatal care and emphasizes the need for referral guidelines. For example, in 2016, there were 1793 referrals for neonatal services outside the governmental sector at an estimated cost of 10 million USD.23
Distribution of Neonatal Health Services at Palestinian Hospitals
Neonatal services are not adequately geographically distributed to match the population and birth rate. Most neonatal services are outside the GS, and most neonatal units in Gaza are level 1 and 2. In addition to shortages in specialized services and equipment in Gaza, the ongoing siege has severely increased the barriers to accessing timely and quality neonatal care.
The only level 4 hospital is located in EJ, and is largely inaccessible to patients from the WB and GS who require a permit from the Israeli authorities to enter, which is not guaranteed. Additionally, in the WB, neonatal services are mostly in the north and middle WB, which contributes to the shortage of beds in the south and delays accessing neonatal care due to checkpoints.
Limitations
The study had several limitations. First, credentials of the neonatologists were not assessed. Second, the study only examined the availability of resources, not actual quality of care. However, this study is unique in several respects, including that it is the first assessment of neonatal health services in Palestine. In addition, the results of the study could potentially reflect similar challenges in other low-income countries where resources are scarce and political challenges hinder the delivery of quality health services. Likewise, outcomes and initiatives resulting from the study can provide examples of methods to address these challenges in similar contexts. For example, the study resulted in the creation of a leveled system of neonatal units in Palestine and was used as a guideline for decision makers to identify resources available in the country and build the neonatal-perinatal referral protocol accordingly. The protocol will ensure the provision of standard care for newborns and is the first step towards the regionalization of perinatal and neonatal healthcare in Palestine. The ultimate goal is the creation of a Palestinian neonatal network to optimize outcomes, provide the best possible care for patients, and ensure high standards that will significantly aid in decreasing the burden on the healthcare system.
Conclusion
To ensure quality care, neonatal units with different assigned levels of service should have the required number of specialists, adequate equipment, supporting facilities, and guidelines for the referral of pregnant women and newborns. Our study found that there is a shortage in the availability of key components of neonatal care (such as incubators) as well as barriers to access to neonatal services. This was coupled with an unequal distribution of neonatal services across the WB, GS, and EJ, hindering the optimal delivery of care to neonates. This is vital for the GS in particular because of the ongoing siege and the challenge of referring patients outside the region. Due to the siege on the GS, separation of EJ from the WB, fragmentation of the WB by many checkpoints and road barriers, limited resources, and the high costs of referrals outside the MoH, as well as the need for timely management of high-risk pregnancies and very sick newborns, there is an urgent need to strengthen neonatal health services in Palestine. In order to have effective and high-quality neonatal services in place, interventions should target four primary issues:
- Due to the geopolitical segregation in Palestine, as well as the study findings that almost all the neonatal units accept extremely low birth weight neonatal cases and outborn cases, it is vital to upgrade all hospitals that provide neonatal services, ensuring they have adequate resources and can provide the appropriate services.
- Standards of care must be implemented in all governmental and non-governmental neonatal care units as part of licensing services and referrals. Currently, the presence of neonatologists and neonatal specialized nurses is not required for the licensing of neonatal units. In addition, MoH hospitals, military services hospitals, and UNRWA hospitals do not require a license to operate.
- Based on study findings that around 60% (22/38) of hospitals with neonatal units are non-governmental, in addition to the challenges to timely referral posed by Israel, it is vital to improve regionalization and build an effective referral system. Study findings on resource availability indicate that certain hospitals should or should not accept certain cases of neonates. There is also a need to develop a referral system for pregnant women and neonates based on the proposed levelling of neonatal units.
- As there is only one level 4 hospital in Palestine, and only 12 out of the 38 units are level 3 units, and given that almost all accept outborn neonates, there is a need to develop an effective transport system. Ambulances are poorly equipped to transport patients, and there is currently no dedicated neonatal transport service.
Abbreviations
WHO, World Health Organization; WB, West Bank; GS, Gaza Strip; EJ, East Jerusalem; UNRWA, United Nations Relief and Works Agency for Palestine Refugees; NGO, non-governmental organization; MoH, Ministry of Health; SPSS, Statistical Package for the Social Sciences; NICU, neonatal intensive care unit; VLBW, very low birth weight; ELBW, extremely low birth weight; AAP, American Academy of Pediatrics; SDG, sustainable development goal; TTN, transient tachypnea of the newborn; HMD, hyaline membrane disease; TPN, total parenteral nutrition; HFOV, high-frequency oscillatory ventilation; NRP, neonatal resuscitation program.
Statement of Ethics
Approval to conduct the study was granted in January 2016 from the Palestinian Minister of Health. All hospitals consented to participation in the study.
Funding
We did not receive any external funding. Study costs were covered by the Palestinian National Institute of Public Health, Ramallah, Palestine.
Disclosure
The authors have no conflicts of interest to declare.
References
1. UNICEF, World Health Organization, World Bank Group, United Nations. Levels and Trends in Child Mortality Report 2015; 2015. Available from: https://www.un.org/en/development/desa/population/publications/mortality/child-mortality-report-2015.asp.
2. World Health Organization. World Health Statistics 2016: Monitoring Health for the SDGs, Sustainable Development Goals; 2016. Available from: https://www.who.int/gho/publications/world_health_statistics/2016/en/.
3. UNICEF, World Health Organization, World Bank Group, United Nations. Levels and Trends in Child Mortality, Report 2018, Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation; 2018. Available from: https://www.unicef.org/media/47626/file/UN-IGME-Child-Mortality-Report-2018.pdf.
4. Darmstadt GL, Bhutta ZA, Cousens S, Adam T, Walker N. Bernis L de. Evidence-based, cost-effective interventions: how many newborn babies can we save? The Lancet. 2005;365(9463):977–988. doi:10.1016/S0140-6736(05)71088-6
5. Cooper P. The challenge of reducing neonatal mortality in low-and middle-income countries. Pediatrics. 2014;133(1):4–6. doi:10.1542/peds.2013-2579
6. St Clair N, Batra M, Kuzminski J, Lee A, O’Callahan C. Global challenges, efforts, and controversies in neonatal care. Clin Perinatol. 2014;41(4):749–772.
7. Massad S, Dalloul H, Ramlawi A, Rayyan I, Salman R, Johansson L. Accuracy of mortality statistics in Palestine: a retrospective cohort study. BMJ Open. 2018;9:4.
8. Palestinian Central Bureau of Statistics. Assessment of Birth and Mortality Data in the West Bank 2011–2012; 2013.
9. van den Berg MM, Madi H, Khader A, et al. Increasing neonatal mortality among palestine refugees in the Gaza Strip. PLoS One. 2015;10:8. doi:10.1371/journal.pone.0135092
10. Abu-Zaine M, Moatti J-P, Ventelou B. Measuring and decomposing socioeconomic inequality in healthcare delivery: a microsimulation approach with application to the Palestinian conflict-affected fragile setting. Soc Sci Med. 2011;72(2):133–141. doi:10.1016/j.socscimed.2010.10.018
11. World Health Assembly. Health Conditions in the Occupied Palestinian Territory, Including East Jerusalem, and in the Occupied Syrian Golan; 2010. Available from: https://apps.who.int/iris/handle/10665/2399.
12. Prime Minister Office. Sustainable Development Goals: Palestinian national voluntary review on the implementation of the 2030 agenda.; 2018. Available from: https://sustainabledevelopment.un.org/content/documents/20024VNR2018PalestineNEWYORK.pdf.
13. Smith R. The effects of the Israeli siege on health provision in the Gaza Strip: a qualitative and theoretical analysis. Lancet. 2018;391.
14. World Health Organization, World Bank. Improving Health System Financing and Service Provision for Universal Health Coverage in Palestine: Addressing the Challenges for a Sustainable and Equitable Health System Development; 2016.
15. World Health Organization. Hospital Care for Mothers and Newborn Babies: quality Assessment and Improvement Tool; 2014. Available from: https://www.euro.who.int/__data/assets/pdf_file/0004/244831/Hospital-care-for-mothers-and-newborn-babies-quality-assessment-and-improvement-tool.pdf?ua=1.
16. American Academy of Pediatrics. Guidelines for Perinatal Care.
17. Jena D, Tripathy R, Pradhan S, Sethi G. Assessment of socio-clinical profile of neonates admitted in sick neonatal care unit of tertiary care hospital: Odisha. Int J Res Med Sci. 2017;5(9):4077–4081. doi:10.18203/2320-6012.ijrms20173986
18. Som M, Nayak C, Padhi B, Ashwani N. Patterns of morbidity among newborns admitted in SNCUs of Odisha, India. Int J Heal Sci Res. 2018;8(9):10–19.
19. Serbesa M, Iffa M. Diagnose at admission and factors associated with management outcome of neonate in Ayder Referral Hospital, Northern Ethiopia: institutional based cross-sectional record review study. J Pediatr Neonatal Care. 2019.
20. Bahl L, Sharma R, Sharma J. Etiology of neonatal jaundice at Shimla. Indian Pediatr. 1994;31(10):1275–1278.
21. Paridhi G, Nilesh D, Sumit A, Vinit W. Study of aetiology of neonatal jaundice at tertiary care centre in Maharastra. SJAMS ISSN. Sch J Appl Med Sci. 2015.
22. OCHA. Over 700 road obstacles control Palestinian movement within the West Bank Jerusalem. 2018. Available from: https://www.ochaopt.org/content/over-700-road-obstacles-control-palestinian-movement-within-west-bank#:~:text=Bulletin%7CSeptember2018-,Over700roadobstaclescontrolPalestinianmovementwithintheWest,insomecasespedestrian%2Cmovement.
23. Ministry of Health. Ministry of Health Annual Report 2017; 2017. http://site.moh.ps/index/Books/BookType/2/Language/ar.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.