")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 6
Improving medication management after a hospitalization with pharmacist home visits and electronic personal health records: an observational study
Authors Kogut S, Goldstein E, Charbonneau C, Jackson A, Patry G
Received 25 October 2013
Accepted for publication 29 November 2013
Published 17 January 2014 Volume 2014:6 Pages 1—6
DOI https://doi.org/10.2147/DHPS.S56574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Stephen Jon Kogut,1 Elaina Goldstein,1 Camille Charbonneau,1 Anita Jackson,1 Gail Patry2
1Department of Pharmacy Practice, College of Pharmacy, University of Rhode Island, Kingston, 2Healthcentric Advisors, Providence, RI, USA
Background: Substantial opportunity exists to improve medication management in the period following a hospital discharge. The objective of this study was to assess and improve medication management during care transitions through pharmacist home visits and the use of an electronic personal health record (ePHR) system.
Methods: Recently discharged patients aged 50 years or older and having a chronic medical condition were offered the opportunity to meet with a pharmacist in the home setting to review medication instructions and receive a demonstration of an ePHR system. Patients agreeable to using the ePHR system were offered pharmacist support with setting up the ePHR system, having emphasis on documenting and reviewing medication regimens. Medication-related problems identified by the pharmacist during the visit were categorized according to ePHR use and by other characteristics.
Results: Thirty recently discharged patients with chronic disease were visited by a pharmacist over a 6-month period. The percentage of medication-related problems identified by the pharmacist was greater among those patients who agreed to use the ePHR system, as compared with patients whose visit did not include use of the ePHR (75% versus 40%, respectively; P=0.06). Differing types of medication-related problems were identified, including therapy duplications, lack of use of clinically important therapies, and patient nonadherence.
Conclusion: For some patients, the home setting can be a suitable venue for medication review and education after discharge from hospital. Assisting patients with setting up the ePHR system may enhance pharmacists’ ability to identify and resolve medication-related problems that may lead to rehospitalization.
Keywords: medication reconciliation, care transition, electronic personal health record
Introduction
Patients who are recently discharged from hospital have an increased risk of experiencing an adverse drug event, and more than half of such adverse drug events may be preventable or ameliorable.1 In one study of the quality of medication instructions following a hospitalization, Coleman et al reported that 14% of recently discharged patients experienced a medication discrepancy, with an approximately equal proportion of discrepancies resulting from patient-related or health system-associated factors.2 In another study of medication discrepancies at discharge, Wong et al reported that over 40% of patients experienced at least one unintentional medication discrepancy. In this study, incompletely written prescriptions and omissions of medications were identified as the most common types of errors.3 Yet even when medication reconciliation is performed accurately during the discharge process, patients may misunderstand medication instructions, particularly when changes occur in complex medication regimens. For example, in one review of medication reconciliation at discharge, Ziaeian et al detected either a medication error or a lack of patient understanding about a medication change in approximately 80% of patients.4
Payers, providers, and policy-makers have directed increased attention and resources towards improving medication safety during care transitions. Current strategies include implementing robust medication reconciliation processes, and promoting other elements of good transitional care, such as enhancing teamwork and communication, and utilizing health information technologies. In 2012, the American Pharmacists Association and the American Society of Health-System Pharmacists jointly issued a white paper entitled “Improving Care Transitions: Optimizing Medication Reconciliation”.5 In this paper, these organizations describe an expansive vision for medication reconciliation, one that is “composed of multiple processes that together reduce medication errors, support safe medication use by patients, and encourage community-based providers and those practicing in hospitals and health systems to collaborate in organized medication reconciliation programs to promote overall continuity of patient care”.
Health information technologies can improve medication reconciliation functions.6,7 Patients can be empowered to assume management of their medication regimen through the use of an electronic personal health record system (ePHR). Using the ePHR, patients or authorized caregivers can maintain their medical information and medication list using a secure electronic application. Patients, pharmacists, and other care providers can utilize ePHR technology to promote greater patient self-efficacy in self-management of the medication regimen, and also to exchange and reconcile information among various information repositories.8 While these benefits are particularly apt during care transitions, research assessing the utility of ePHR systems to improve medication management is scant.9
Researchers from the University of Rhode Island College of Pharmacy piloted an intervention to improve medication management during care transitions. The project was one of several initiatives included in the Tech4Impact Program (Technologies for Improving Post-Acute Care Transitions), sponsored by the Center for Technology and Aging, a national leader in the use of patient-centered technologies for older adults.
Our intervention involved deploying pharmacists to visit the homes of recently discharged patients to review medication instructions and to offer patients free use of an ePHR system, with ongoing support in setting up and using the ePHR. We hypothesized that the pharmacist’s ability to identify medication-related problems would be greater among patients who used the ePHR system. To our knowledge, no study to date has coupled in-home pharmacist education with the use of an ePHR system to promote safe and effective medication management during care transitions. This report presents our findings in delivering this intervention during a 6-month period occurring between August 2011 and February 2012.
Materials and methods
This was a prospective nonrandomized pilot study in which recently hospitalized patients were offered the opportunity to meet with a pharmacist in their home within 14 days of their discharge from hospital to review medication instructions and to receive a demonstration of an ePHR system. Patients were informed that the pharmacist home visit would include a medication regimen review and help in setting up the ePHR system, if desired. Usual care consisted of medication reconciliation at discharge provided by hospital clinicians, but without subsequent home visits provided by pharmacists.
The ePHR utilized in this project was the ER-Card® system, developed by ER-Card LLC of West Warwick, Rhode Island. This product features online password-protected sharing of health record information via the Internet, or by USB drive provided by the consumer. The ER-Card system provides staff support for assisting with completing and updating the contents of the patient’s record. Medical conditions and medication information is self-reported by the patient, with pharmacists verifying medication lists with the patient’s pharmacy.
The study enrolled patients 50 years of age or older and having any of the following chronic conditions: cardiovascular disease and related conditions (eg, atrial fibrillation), respiratory illness (eg, chronic obstructive pulmonary disease/asthma), and/or diabetes mellitus. As our focus was on medication self-management among community-dwelling patients, we did not recruit patients with dementia or patients who were transitioning from the hospital to a long-term care facility. The pharmacist home visit was offered to patients who were participating in an associated care transitions initiative conducted by the Rhode Island Quality Improvement Organization (Healthcentric Advisors) in cooperation with Rhode Island’s Aging and Disability Resource Center. Patients were also recruited via referral from Rhode Island Medicaid nurse case managers. A third pathway for patient recruitment was on-site solicitation of patients at Kent Hospital in Warwick, Rhode Island, which served as the predominant patient recruitment source.
Patients agreeable to the pharmacist home visit completed an informed consent process explaining the activities that the pharmacist would be providing during the home visit. Patients were informed that that they were not required to utilize the ePHR system to receive the pharmacist home visit, and that if they decided to utilize the ePHR system, their information could be shared with other health care providers only if they provided permission. Those patients deciding to utilize the ePHR system completed an authorization form routinely required by the ePHR vendor for compliance with the Health Insurance Portability and Accountability Act. The ePHR was offered to patients at no cost, and patients were allowed to discontinue their use of the ePHR at any time. The study was approved by the Institutional Review Board on Human Subjects at the University of Rhode Island and Kent Hospital.
For patients consenting to participate in the study, a home visit was scheduled by the study pharmacist for a suggested period of 2 hours. When a medication-related problem was identified during the medication review, the pharmacist discussed the concern with the patient, and encouraged the patient to contact the prescriber or pharmacy when appropriate. The pharmacist demonstrated the ePHR program using a laptop computer, and if the patient was agreeable to trying the ePHR system, the pharmacist supported the patient in entering their medical information and medication list into the ePHR system. During the home visit the pharmacist completed a data collection form that captured information describing the medication-related problems identified and other data relevant to the study.
We categorized study participants according to the referral source and by the primary diagnosis associated with the recent hospitalization. Age was categorized as 50–64 years or 65 years or older. We categorized the types of medication-related problems identified during the home visit as involving therapy duplication, interactions, medication cost, or incorrect use or underuse of a medication (eg, poor adherence). We compared the frequency of medication-related problems identified between users and nonusers of the ePHR system, overall and according to patient age and sex. We also documented medication discrepancies using the tool developed by Dr Eric A Coleman’s Care Transitions Program®,10 which categorizes events as patient-related or health-system related. Our results are presented here as descriptive statistics, with the chi-square test used to determine the statistical significance of differences in observed rates of medication-related problems between users and nonusers of the ePHR. Fisher’s exact test was used where any cell size was less than five observations.
We attempted to contact patients no earlier than 30 days following the home visit to enquire about their satisfaction with the pharmacist visit, to determine if patients continued to utilize the ePHR system, and to ascertain if patients had been rehospitalized in the period following the home visit.
Results
Approximately 300 patients were identified as eligible for our program and were approached by study recruiters. While 59 of these eligible patients initially agreed to participate in the study, we were unable to schedule a home visit with 29 patients, because some did not return our subsequent telephone calls to schedule the home visit, while other patients changed their mind about participating, transitioned to a long-term care setting or died. The study pharmacists completed home visits for a total of 30 patients, with 20 of these patients agreeing to utilize the ePHR system. Among the 30 patients visited, 16 (53%) were male and 23 (77%) were 65 years of age or older. The majority of patients had been hospitalized due to a cardiovascular-related illness (n=24), while six patients were hospitalized for an exacerbation of their respiratory illness or diabetes (see Table 1).
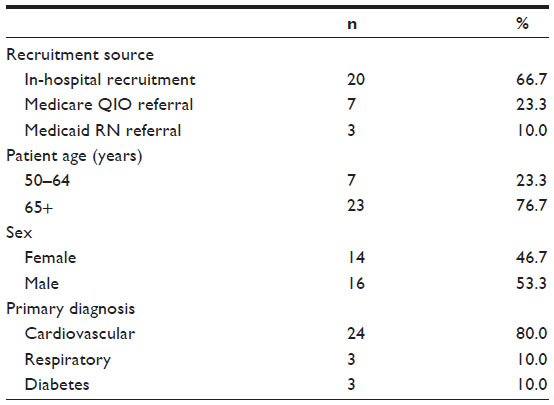 | Table 1 Characteristics of patients with chronic disease completing a pharmacist home visit following a hospitalization (n=30) |
At each patient home visit, the pharmacist performed a medication regimen review and documented medication-related problems that were identified. Table 2 presents the range of problems discovered, which are categorized as cost-related, involving therapeutic duplication, drug interaction, underuse (lack of use) of a clinically important therapy, or having incorrect or unclear instructions for medication use. Several patients discontinued a clinically important medication due to cost, while other patients did not appear to be utilizing indicated therapies (eg, lack of aspirin use following a myocardial infarction, with no apparent contraindication to aspirin therapy). Instances of therapeutic duplication included concomitant use of two proton pump inhibitors, use of two different albuterol inhaler products, and use of multiple products containing acetaminophen.
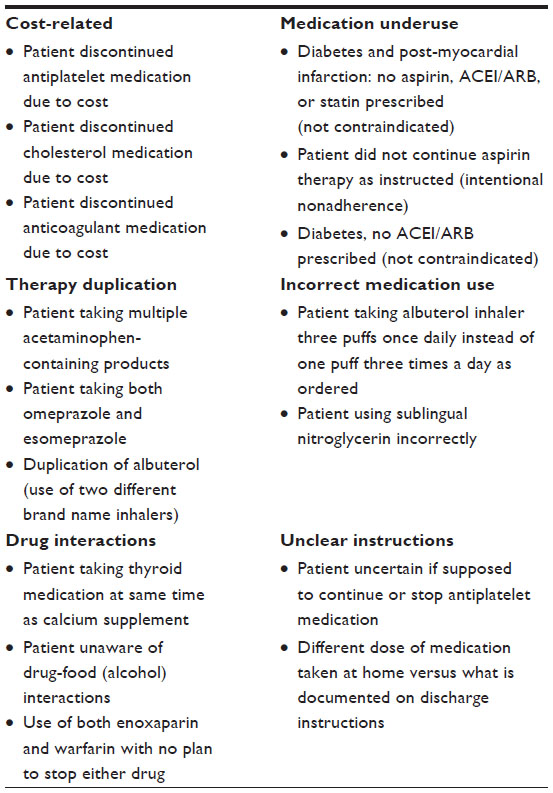 | Table 2 Examples of medication-related problems identified during pharmacist home visits following hospital discharge |
The percentage of medication-related problems detected by the pharmacist was higher among those patients agreeing to use the ePHR system (15/20, 75%), as compared with patients who did not use the ePHR (4/10, 40%). Medication-related problems were also identified more frequently among patients who were younger than 65 years of age, as compared with older patients (71% versus 61%, respectively), and were identified more frequently among males as compared with females (69% versus 57%, respectively). Medication-related problems were identified among approximately 60% of patients who were recently hospitalized for a cardiovascular-related condition, and among 67% of patients who were recently hospitalized for a respiratory illness. Despite large proportional differences across several of these cross-tabulations, statistically significant differences were not observed, reflecting the small sample size in this pilot study (Table 3).
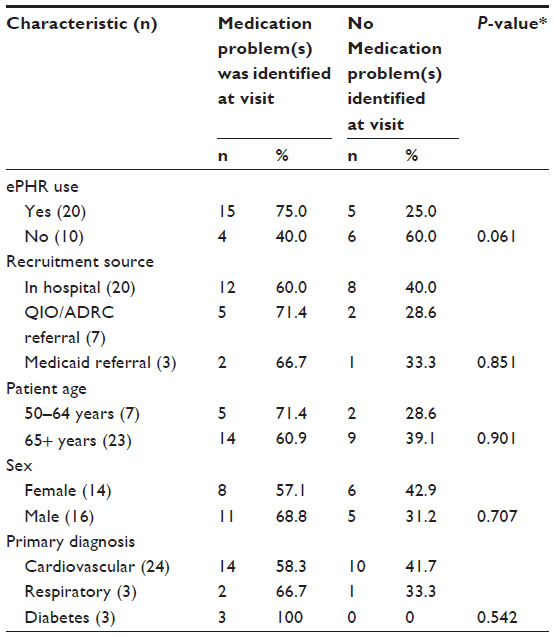 | Table 3 Frequency of medication-related problems identified during home visit following discharge: results stratified by ePHR use, recruitment source, and other patient characteristics |
Table 4 presents the frequencies and types of medication discrepancies identified during the home visit using the Care Transitions Program® Medication Discrepancies Tool for Multiple Events.10 Discrepancies were detected among 16 of the 30 patients we visited (53%): six of the discrepancies were categorized as relating to patient-associated factors, while ten of the discrepancies were considered to have resulted from system-related factors. The most frequently observed discrepancy was “conflicting information from different informational sources”, as documented in five of the 30 home visits that were completed.
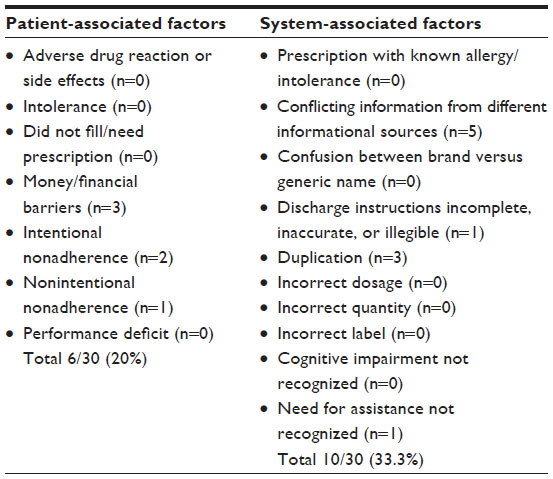 | Table 4 Medication discrepancies identified during pharmacist home visits following a hospital discharge (n=30)* |
We succeeded in following up with 19 of the 30 patients whom we visited. Of these 19 patients, three had been rehospitalized within 30 days (3/19, 16%). Patients who were surveyed at follow-up expressed a high level of satisfaction with the pharmacist home visit, with all patients responding affirmatively to our follow-up survey question: “Do you think that the pharmacist home visit was helpful in reviewing your medications and addressing your questions?” Seven patients reported that they had used the ePHR to share information with care providers during their post-discharge medical visits.
Discussion
In this pilot program, pharmacists conducting home visits frequently identified medication-related problems among recently discharged patients. At least three of the 30 patients had discontinued an important medication therapy due to high cost. In these instances, the pharmacist instructed the patient to contact her/his health care provider to discuss treatment options, which might include switching to an affordable alternative therapy (eg, changing to a generic cholesterol-lowering medication). Additionally, several patients reported errors related to their medication regimen that occurred during their transitioning into or out of hospital, with 16 such discrepancy events documented using the Medication Discrepancy Tool®.
Among the 30 patients who were visited by the pharmacist, 20 agreed to use the ePHR technology, and seven patients reported that they had used the ePHR to share information with their care providers during follow-up visits or rehospitalizations. While these results indicate that the ePHR system can be effectively used by patients during care transitions, our sample size was too small to draw any firm conclusions regarding the characteristics of patents who are more likely to effectively utilize an ePHR to manage their medication regimen.
This intervention was challenging to operationalize. Foremost, patient recruitment was difficult, because many of the patients whom we encountered were not agreeable to meeting with the pharmacist in their home. Patient perceptions regarding the role of the pharmacist in the health system may have posed a barrier to our work, as pharmacists do not commonly enter the patient’s home to provide medication counseling services. The lack of awareness among patients of the potential benefits of an ePHR system also posed a barrier to recruitment. We provided an explanation of the ePHR system and its potential benefits during recruitment, and as an element of the informed consent process. However, it was challenging to effectively explain the potential utility of the ePHR during our brief recruitment encounters, especially considering that our population of focus included hospitalized or recently hospitalized patients who were often severely ill. Additionally, approximately half of the patients who consented to participate in the study subsequently changed their mind about completing the home visit, or did not return telephone calls when the scheduler contacted them.
Our study had several limitations that should be considered in interpreting our findings. Most importantly, it should be recognized that this was a pilot study involving a small number of patients. Larger scale application of the model is warranted before any strong conclusions can be made about the benefits of ePHR systems to aid medication management during care transitions. The small sample size also limited our ability to determine a difference in effectiveness of the intervention according to the characteristics of the patients studied. Additionally, the nonrandomized design may have resulted in selection bias, whereby participating patients may have generally been more accepting of the role of pharmacists and of information technology. Another limitation of our study pertains to the role of the pharmacist in our model, which did not include direct intervention with the patient’s pharmacy or prescribers to pursue each medication-related problem identified to its resolution. We believe that establishing more formalized communications with health care team members would be an important step towards ensuring that the visiting pharmacist’s observations and recommendations are best incorporated into clinical decision-making. Finally, we were unable to follow up with 11 of the 30 patients to determine their satisfaction with the intervention, or if they continued to use the ePHR system.
Conclusion
Our findings from this pilot study suggest that pharmacist home visits following a hospitalization can aid in identifying medication-related problems. The frequency and clinical significance of the problems identified suggests a need for increased involvement of pharmacists during care transitions. The ability to identify such problems may be enhanced when pharmacists work together with patients to review and enter the discharge medication list into an ePHR system.
Acknowledgments
This work was funded by a grant from the Center for Technology and Aging, which sponsored the Tech4Impact program (Technologies for Improving Post-Acute Care Transitions) to advance the use of technologies that improve care transitions and reduce avoidable hospitalizations. Funding was also provided through a Rhode Island State Legislative grant to support application of the ePHR program (ER-Card) in promoting care quality among Rhode Island seniors. The authors are grateful for the review and instructive comments provided by Kevin M Ryan, University of Rhode Island, and by David Lindeman and Valerie Steinmetz from the Center for Technology and Aging.
Disclosure
The researchers did not receive funding from any pharmaceutical manufacturer in relation to this work. The authors report no other conflicts of interest in this work.
References
Forster AJ, Murff HJ, Petersen JF, Gandi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167. | |
Coleman EA, Smith JD, Raha D, Min SJ. Post-hospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005;165(16):1842–1847. | |
Wong JD, Bajcar JM, Wong GG, et al. Medication reconciliation at hospital discharge: evaluating discrepancies. Ann Pharmacother. 2008;42(10):1373–1379. | |
Ziaeian B, Araujo KL, Van Ness PH, Horwitz LI. Medication reconciliation accuracy and patient understanding of intended medication changes on hospital discharge. J Gen Intern Med. 2012;27(11):1513–1520. | |
American Pharmacists Association, American Society of Health-System Pharmacists. Improving care transitions: optimizing medication reconciliation. J Am Pharm Assoc (2003). 2012;52(4):e43–e52. | |
Kramer JS, Hopkins PJ, Rosendale JC, et al. Implementation of an electronic system for medication reconciliation. Am J Health Syst Pharm. 2007;64(4):404–422. | |
Agrawal A, Wu WY. Reducing medication errors and improving systems reliability using an electronic medication reconciliation system. Jt Comm J Qual Patient Saf. 2009;35(2):106–114. | |
Tang PC, Ash JS, Bates DW, Overhage JM, Sands DZ. Personal health records: definitions, benefits, and strategies for overcoming barriers to adoption. J Am Med Inform Assoc. 2006;13(2):121–126. | |
Kaelber DC, Jha AK, Johnston D, Middleton B, Bates DW. A research agenda for personal health records (PHRs). J Am Med Inform Assoc. 2008;15(6):729–736. | |
Smith JD, Coleman EA, Min SJ. A new tool for identifying discrepancies in postacute medications for community-dwelling older adults. Am J Geriatr Pharmacother. 2004;2(2):141–147. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.