")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Implications from China patient safety incidents reporting system
Authors Gao XQ, Yan SP, Wu WQ, Zhang R, Lu YL, Xiao SY
Received 15 October 2018
Accepted for publication 10 January 2019
Published 8 February 2019 Volume 2019:15 Pages 259—267
DOI https://doi.org/10.2147/TCRM.S190117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Deyun Wang
Xinqiang Gao,1 Shipeng Yan,2 Wenqiong Wu,2 Rui Zhang,3 Yuliang Lu,4 Shuiyuan Xiao1
1Department of Social Medicine and Health Management, Xiangya School of Public Health, Central South University, Changsha, Hunan Province, China; 2Department of Cancer Prevention and Control, Hunan Cancer Hospital and The Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, Changsha, Hunan Province, China; 3Department of Health Policy and Management, School of Public Health, Peiking University, Peiking, China; 4Department of the Medical Affairs, Binzhou Medical University Hospital, Binzhou Medical University, Bingzhou, Shandong Province, China
Objective: We aimed to explain the operational mechanism of China National Patient Safety Incidents Reporting System, analyze patterns and trends of incidents reporting, and discuss the implication of the incidents reporting to improve hospital patient safety.
Design: A nationwide, registry-based, observational study design.
Data source: The database of China National Patient Safety Incidents Reporting System.
Outcome measures: Outcome measures of this study included the temporal, regional, and hospital distribution of the reports, as well as the incident type, location, parties, and possible reasons for frequently occurring incidents.
Results: During 2012–2017, 36,498 patient safety incidents were reported. By analyzing the time trends, we found that there was a significant upward trend on incidents reporting in China. The most common type of incidents was drug-related incidents, followed by nursing-related incidents and surgery-related incidents. The three most frequent locations of incident occurrence were Patient’s Room (65.4%), Ambulatory Care Unit (8.4%), and Intensive Care Unit (7.4%). The majority of the incidents involved nurses (40.7%), followed by physicians (29.5%) and medical technologist (13.6%). About 44.4% of the incidents were attributed to the junior staff (work experience ≤5 years). In addition, incidents triggered by the senior staff (work experience >5 years) were more often associated with severe patient harm.
Conclusion: To strengthen the incidents reporting system and generate useful evidence through learning from incidents reporting will be important to China’s success in improving the nation’s patient safety status.
Keywords: patient safety, NPSIRS, National Patient Safety Incidents Reporting System
Introduction
Patient safety is a serious global public health issue, affecting patients in all health care settings, whether in developed or developing countries.1 Estimates showed that ~42.7 million of patients worldwide endure disabling injuries or death annually, directly attributed to unsafe medical practices and medical errors. Globally, the cost associated with these unsafe medical practices and medical errors has been estimated at US$42 billion yearly, which amounts to almost 1% global expenditure on health.2,3
Patient safety in China has aroused great concern due to the immense scale of patient’s population. According to the newest statistics, the number of inpatients in China has reached 230 million yearly.4 Even assuming a minimum of 2% incidence rate,5 ~4.6 million inpatients will suffer from some degree of adverse events in each year. In addition to patients suffering, unsafe medical practices and medical errors also triggered serious social problems in China. A national survey showed that 63.7% of hospitals had experienced medical violence incidents, and most of these incidents were related with unsafe medical practices.6
Patient safety risks in health care process are inevitable, but considerable proportion of them can be prevented.7 Medical practices have proved that surveillance and learning from patient safety incidents can reduce the odds of making mistakes, and by doing so, improve patient safety. Given that, many countries have developed their reporting systems and have carried out a series of research works.8–10 In China, the National Patient Safety Incidents Reporting System (NPSIRS) was rolled out from early 2012. After a long run of the system, we accumulated some experiences and received abundant incidents data. In this study, we sought to explain the operational mechanism of the China NPSIRS, display the pattern and trend of incident reporting, and describe the characteristics of incidents by analyzing data extracted from the database.
Material and methods
Data source
The data used in this study are reported by NPSIRS staff as patient safety incidents from hospitals in China over the period from January 01, 2012 to December 31, 2017. The definition of a patient safety incident is “any unintended or unexpected incident that resulted in or could have resulted in harm to one or more patients”.11 Reporting incidents in NPSIRS is mandatory and non-confidential. Every medical personnel have a duty to report incidents that they observed or are involved in, of which most incidents are first notified to hospital internal reporting system and then sent in batch returns by the hospital risk manager to the national database. The basic working flowchart of NPSIRS is displayed in Figure S1. Each report contains structured categorical information about administrative data, time and location of occurrence, the parties and patient demographics, reporter’s assessment of severity of harm, and management measures after the incident. The report also contains unstructured free-text descriptions of the incident, potential contributory factors, and planned actions to prevent recurrence. The free-text descriptions, where the reporter is asked to describe, provide a rich body of qualitative data for identification of areas for improvement.
Study design and study setting
Based on the database of NPSIRS, we undertook an observational study design in this study. Aside from Taiwan, Hongkong, Macao, and Tibet, this database theoretically included all hospitals of the other 31 provincial administrative areas in China.
Classification of the incident and its contributing factors
The China NPSIRS only classified the extent of the harm but did not for the incident type. Given the need of improving patient safety, we empirically developed our own classification criteria to conduct a more detailed analysis of the incidents, containing those that are complicated in nature, which involve a series of events that culminate in, and contribute to, the incident. The thematic analysis was used for the qualitative aspects of this work. Each report was independently reviewed by a multidisciplinary team, and by inspecting the structured and unstructured information, a main reason for the incident was chosen and recorded as one of the following 12 incident types: surgery-related incidents, anesthesia incidents, laboratory-related incidents, medical procedure incidents, blood transfusion incidents, tube-related incidents, drug-related incidents, nursing-related incidents, medical device-related incidents, public accidents, unexpected incidents, and other incidents. The detailed specifications of incident type are shown in Table S1. After this thematic analysis, all the incidents were indexed and mapped onto the 12 categories and further collapsed into 6 domains according to their contributing factors.
The conceptual framework for the classification of incident type and contributing factor was built based on comprehensive literature review, expert consultation, as well as referencing the taxonomies from other reporting systems, such as Taiwan Patient Safety Reporting System and National Reporting and Learning System (NRLS).12,13 Before the formal work beginning, we hold a series of training sessions on the related criteria in order to achieve consensus. Moreover, we randomly choose partial data as a practice data set to test the investigator’s consistency in classifying the incidents. Only >75% agreement (kappa statistic) between investigators and an arbitrator was achieved; the investigators were eligible to code the study data.
Statistical analysis
We used descriptive statistical analysis to show the distribution pattern of incident reports and some characteristics of the incident itself. These involved the temporal, regional, and hospital distribution of the reports, as well as the incident type, location, parties, and possible reasons for frequently occurring incidents. All data collation and analysis in this study were performed using Microsoft Excel 2010 and SPSS 18.0 software.
Ethical statement
This study was approved by the institutional review board of the School of Public Health, Central South University (XYGW-2018-103).
Results
Distribution of incidents reporting
In the very beginning, the incidents reporting in China were based on paper-based form and procedure. This inefficient way directly makes medical organizations less willing to report incidents. During this stage, only a few hospitals established their internal reporting system and regularly reported incidents, resulting in great obstacle to the data utilization. In 2012, the web-based reporting system was developed by the former Ministry of Health of China through a central financing mechanism. Since then, the quantity and quality of the incidents reporting in China has dramatically increased. A total of 36,498 incidents were reported to the NPSIRS during the study period. Figure 1 clearly shows that the number of annual reports increased from 815 in 2012 to 8,088 in 2017. Regardless of the type of hospitals, there were obvious upward trends in their reports. Nevertheless, we found a significant hospital difference in the total number of incident reporting. Approximately 92.3% of the incidents were reported by secondary hospitals and tertiary hospitals. We also found obvious regional variations across China (Figure 2). About 40.3% (14,697/36,498) of incidents were reported by East China, while the number of incidents reported by Northeast and Northwest China each only accounted for about 6.5% of the total.
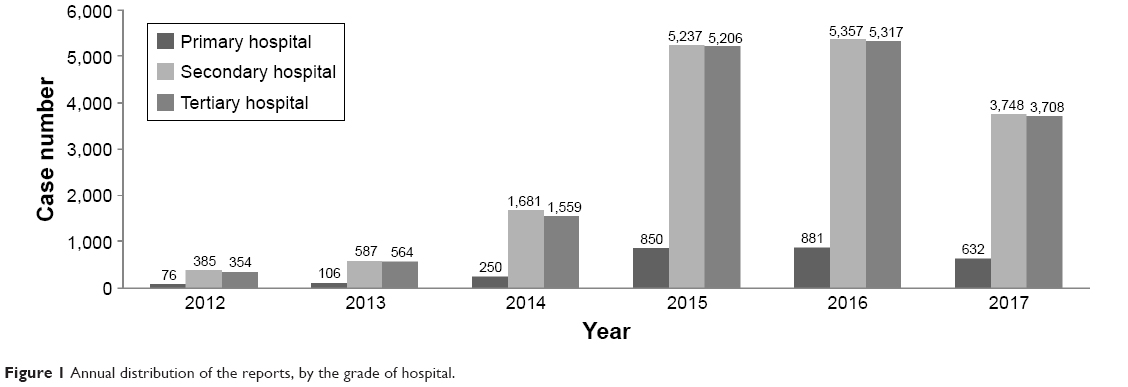 | Figure 1 Annual distribution of the reports, by the grade of hospital. |
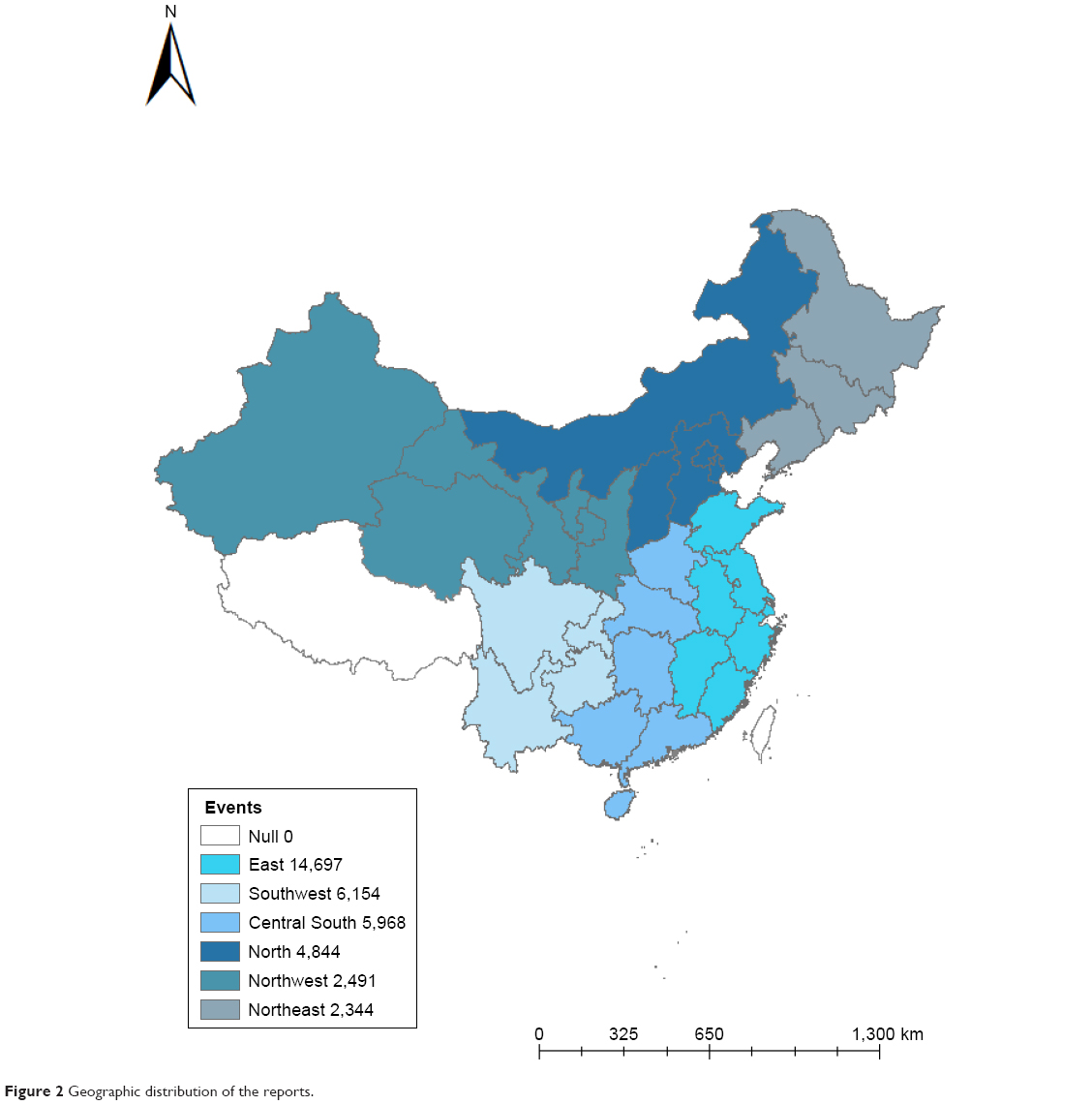 | Figure 2 Geographic distribution of the reports. |
Types of incidents and contributing factors
Analyzing the type of incidents showed that medication-related incidents were the most frequent type of incident (Table 1) and were chiefly caused by human factors and system failures (Table 2). Most of the patients enduring medication-related incident were receiving internal medicine treatment, with incidents owing to the mistakes in drug prescription, drug delivery, or drug administration. The next common frequent type was nursing-related incidents (ie, falling, decubitus, and self-injury), where most of them were caused by the poor standard of care and patient’s condition. It seems that patients with certain characteristics, such as older and critical patients, are more susceptible to this type of incident. Surgery-related incidents ranked the third most common type of incident, but about 21% of them resulted in severe injury and death. The main cause for this type of incident was the human factors, such as inexperienced operation and violation in standard operation procedure. In addition, the complexity of operative care itself also was the important contributor to this type of incident. Medical procedure incidents accounted for 10.7% of the total, and it tended to occur due to poor communication and unclear lines of authority among medical personnel. This type of incident is mainly caused by the systematic failure. Most tube-related incidents involved critical patients. These incidents were mainly caused by unplanned extubation trigerred by patient behavior, catheter-related infection, block, or accidental slide out.
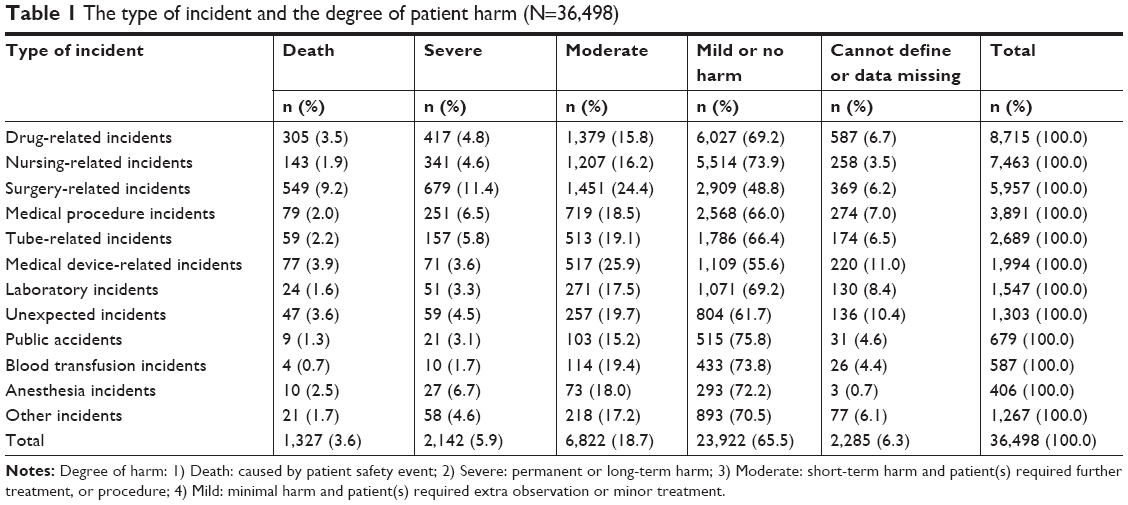 | Table 1 The type of incident and the degree of patient harm (N=36,498) |
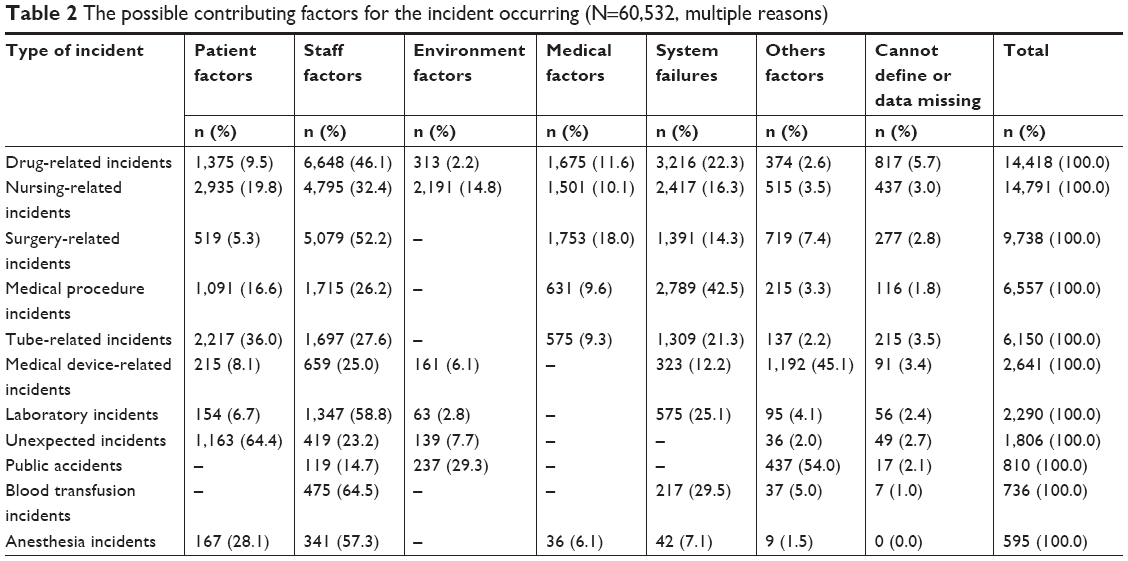 | Table 2 The possible contributing factors for the incident occurring (N=60,532, multiple reasons) |
Characteristics of the parties and site of incidents
A total of 28,192 reports provided the detailed information of the parties. Nurses were associated with the most incidents (40.7%, 11,474/28,192), followed by physicians (29.5%, 8,317/28,192), medical technologists (13.6%, 3,834/28,192), and pharmacists (5.1%, 1,438/28,192). The number of incidents attributed to multiple persons or others (ie, administrator or supporting staff) added up to 11.1% (3,129/28,192) of the total. Medical personnel who had been working for less than 5 years were responsible for 44.4 % (1,2517/28,192) of the incidents, those with 6–10 years of experience were responsible for 27.4% (7,713/28,192), and those with over 10 years were responsible for 24.5% (6,903/28,192). Seemingly, the severity of incidents has some sort of link with the work experience of medical staff. Medical staff with longer work experience were associated with a greater amount of deaths and severe incidents (Table 3). Overall, most incidents occurred in Patient’s Room (65.4%, 23,865/36,498), followed by Ambulatory Care Unit (8.4%, 3,049/36,498), and the Intensive Care Unit (7.4%, 2,718/36,498). The number of incidents that occurred in all other locations added up to 18.8% of the total. In different types of hospitals, the locations where the occurrence of incidents is frequent have a different distribution pattern. Except Patient’s Room and Ambulatory Care Unit, the most frequent locations in the secondary and tertiary hospitals are Intensive Care Unit and Operating Room, while in the primary hospitals they are Emergency Room and Auxiliary Examination Room. This disparity may be a reflection of different safety risks in different medical organizations.
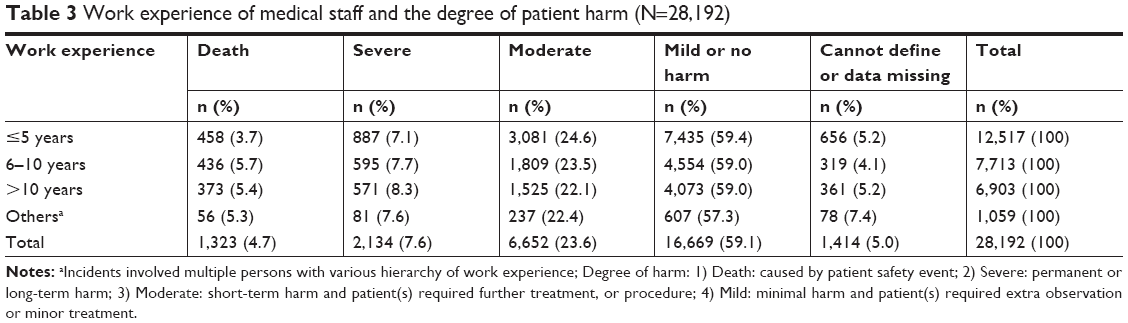 | Table 3 Work experience of medical staff and the degree of patient harm (N=28,192) |
Discussion
Although the number of incident reports has increased exponentially, the proportion of incidents that are reported remains too low, which may indicate that underreporting is common. In fact, this underreporting is not only a problem for NPSIRS; Barach and Small reported that incident reports may only account for 4%–50% of events that occur in the USA annually.14 Sari et al found that the routine reporting system in a larger hospital of UK only can identify 7% of incidents that resulted in patient harm.15 Many factors can hamper the reporting16–18 of which punitive safety culture is the main disincentive for China NPSIRS. Medical personnel who work in Chinese hospitals may suffer from a set of economic, administrative, or moral penalties if their mistake is found to have resulted in such incidents. Therefore, these staff fear to report patient safety incidents as they fear to be punished for that. During the first year of the launch of NPSIRS, only 815 incidents were reported from 137 medical organizations. We highly agree with the successful experience established by NRLS that cultivating a positive culture of patient safety in health care delivery is critical to improve incident reporting, and it is very gratifying to see that a series of major steps have been taken in China in recent years. These involved legislating to regularize and encourage reporting and building up a voluntary reporting system as a supplement to NPSIRS. Through its consistent efforts over the years, we have seen some positive changes in patient safety culture in China. In 2017, one large-scale investigation showed that the average “problematic responses” concerning patient safety climate in all dimensions were lower than those of previous studies,19 which indicates that there was an improving patient safety culture in China. Under this circumstance, we have also seen an obvious augment in both the number of reporting hospitals and incidents reported. Therefore, the key to improve the reporting of incidents is cultural change, which was also the viewpoint of Kingston et al.20
Our analysis indicated that the number of incident reporting has dramatic regional and hospital disparity. Most incidents are reported by larger hospitals and Chinese developed regions. These findings suggest that some socioeconomic factors are closely linked to incident reporting in China. Compared with undeveloped regions and primary hospitals, those developed regions and larger hospitals possess more manpower, material, and financial resources, enabling them to provide more effective support to their safety culture and reporting systems. Thus, further investigation of the nature of the regional and hospital differences and elimination of these differences are essential for China NPSIRS.
Similar to other studies,12,21,22 we found that the most frequent types of incidents were drug-related incidents and nursing-related incidents. Because only a few operations and procedures were involved, we tend to consider that both of these incidents were more likely to occur due to poor standard of care. Therefore, improvement of safety awareness and implementation of drug management and usage of standard audit procedures will contribute to prevent the occurrence of this type of incident. Surgery-related incidents are the third most common type in China. This is different from the results of other related studies.12,21 We suspect that this difference is mainly due to the variation in classification criteria. Nevertheless, considering surgery-related incidents are frequently associated with severe injury or death, we still believe that preventing this type of incident is one of the keys to improve patient safety. On analyzing the causes of these incidents, our findings showed that apart from human factors, system failures also play an important role for incident occurrence. This result strongly supports the viewpoint expressed by Thomas et al that many mistakes in health care are likely the result of poorly designed systems rather than negligent individual performance.23 Therefore, from this point of view, the reduction of patient safety incidents involving system failures in China will require an increased emphasis on the optimization of process design and the enforcement of standard procedures.
In our study, most incidents are associated with nurses, which may be a sign of reporter bias. Some studies indicated that nurses have a higher reporting willingness than others, often being the majority of the notifiers.20,24 Given a wide range of reporters may provide a different perspective on incidents, encouraging everyone, including patients and their families, to inform incidents should be a direction of efforts to China NPSIRS. In addition, other studies, as well as ours, have found that junior staff are responsible for most incidents.25,26 This finding may suggest that insufficient experience is one of the important predictors for incident occurrence. We also found that work experience has some sort of link with the severity of harm. Incidents triggered by senior staff are more likely to lead to severe harm. One plausible explanation is the fact that senior staff usually provide more complex and riskier care to severely ill patients. Future research on this phenomenon is suggested.
Strengths and limitations
Our study is the first systematic analysis of safety incident reports from China NPSIRS. Using comprehensive nationwide statistics and a set of mix methods, we have empirically developed taxonomy to characterize safety incident reports for the identification of the most common and frequent safety issues, as well as to understand the underlying clinical context reported by medical personnel. These findings will serve as a baseline for future assessment of the patient safety improving effort in China and will provide insights into the areas of greatest need for prioritization. However, there are some limitations in our study that should be taken into consideration. Because of the limitations of data quality, particularly the extent of underreporting, selective reporting, and incomplete reporting, our findings may not be a fully precise representation of actual incident characteristics at individual medical institutions. The authors suggest that carrying out more studies on the incident reports will be helpful to verify our findings.
Conclusion
Despite some limitations, our study provides some new insights related to China’s patient safety incidents. These results could be considered as a small but important step toward improving patient safety in China. Our findings suggested that the incident reporting in China has significant regional and hospital difference. The elimination of this difference is one of the major challenges for China NPSIRS. In addition, given the distribution of incidents in this study, efforts to improve medication safety, nursing care, and surgery are likely to play an important role in improving patient safety in Chinese hospitals. In the process, using some effective risk assessment methods, such as Root Cause Analysis, Swiss Cheese Model, and Prospective Failure Mode and Effects Analysis, to identify potential vulnerabilities in complex, high-risk processes are very necessary.
In conclusion, reporting patient safety incidents and learning from experience are the key steps to maintain and improve patient safety. Efforts to encourage reporting and learning will require some cultural change. We suggest that policymakers and health managers at all levels should dedicate to building an open, transparent, and supportive patient safety culture, especially in hospitals in underdeveloped areas, at lower levels, and with smaller sizes.
Acknowledgments
We wish to thank all the staff working on China NPSIRS.
Author contributions
SYX and XQG initially designed the survey. XQG wrote the first draft. XQG, SPY, WQW, RZ, and YLL provided data management and statistical expertise. All authors approved the final version of the study. All authors contributed to conception and design, data collection and analysis, drafting and critically revising the paper, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Patient Safety Assessment Manual Second Edition. Geneva: World Health Organization; 2016. | ||
World Health Organization. Medication without harm-global patient safety challenge on medication safety. Available from: http://www.who.int/patientsafety/medication-safety/medication-without-harm-brochure/en/. Accessed January 9, 2018. | ||
World Health Organization. 10 facts on patient safety, 2018. Available from: http://www.who.int/features/factfiles/patient_safety/en/. Accessed March 9, 2018. | ||
National Health and Family Planning Commission of the People’s Republic of China. The China Health and Family Planning Statistical Yearbook 2017. Beijing: Peking Union Medical College Publishing House; 2011 (in Chinese). | ||
Kalra J, Kalra N, Baniak N. Medical error, disclosure and patient safety: a global view of quality care. Clin Biochem. 2013;46(13–14):1161–1169. | ||
Xiaoli J, Hongzhu Z, Yue Z. Investigation on hospital violence during 2003 to 2012 in China. Chinese Hospital. 2014;18(3):1–3. | ||
Wilson RM, Michel P, Olsen S, et al. Patient safety in developing countries: retrospective estimation of scale and nature of harm to patients in hospital. BMJ. 2012;344:e832. | ||
Rutherford JS, Flin R, Irwin A. The non-technical skills used by anaesthetic technicians in critical incidents reported to the Australian incident monitoring system between 2002 and 2008. Anaesth Intensive Care. 2015;43(4):512–517. | ||
Cooper J, Edwards A, Williams H, et al. Nature of blame in patient safety incident reports: mixed methods analysis of a national database. Ann Fam Med. 2017;15(5):455–461. | ||
Soukavong M, Kim J, Park K, et al. Signal detection of adverse drug reaction of amoxicillin using the Korea Adverse Event Reporting System Database. J Korean Med Sci. 2016;31(9):1355–1361. | ||
National Health and Family Planning Commission of the People’s Republic of China. The notification on the regulations of medical quality and safety events reporting, 2011. Available from: http://www.nhfpc.gov.cn/yzygj/s3589/201101/16cbc063883440d1af15171bb73803d7.shtml. Accessed February 23, 2018. | ||
Lin CC, Shih CL, Liao HH, Wung CH. Learning from Taiwan patient-safety reporting system. Int J Med Inform. 2012;81(12):834–841. | ||
NRLS. Patient safety incident report form. Available from: https://report.nrls.nhs.uk/GP_eForm. Accessed June 1, 2018. | ||
Barach P, Small SD. Reporting and preventing medical mishaps: lessons from non-medical near miss reporting systems. BMJ. 2000;320(7237):759–763. | ||
Sari AB, Sheldon TA, Cracknell A, Turnbull A. Sensitivity of routine system for reporting patient safety incidents in an NHS Hospital: retrospective patient case note review. BMJ. 2007;334(7584):79. | ||
Smith KS, Harris KM, Potters L, et al. Physician attitudes and practices related to voluntary error and near-miss reporting. J Oncol Pract. 2014;10(5):e350–e357. | ||
Hewitt T, Chreim S, Forster A. Sociocultural factors influencing incident reporting among physicians and nurses: understanding frames underlying self- and peer-reporting practices. J Patient Saf. 2017;13(3):129–137. | ||
Howell AM, Burns EM, Bouras G, Donaldson LJ, Athanasiou T, Darzi A. Can patient safety incident reports be used to compare Hospital safety? Results from a quantitative analysis of the English National reporting and learning system data. PLoS One. 2015;10(12):e0144107. | ||
Zhou P, Li M, Wei X, Zhu H, Xue D. Patient safety climate in general public hospitals in China: a multiregion study. J Patient Saf. Epub 2017 Sep 29. | ||
Kingston MJ, Evans SM, Smith BJ, Berry JG. Attitudes of doctors and nurses towards incident reporting: a qualitative analysis. Med J Aust. 2004;181(1):36–39. | ||
Jämsä JO, Palojoki SH, Lehtonen L, Tapper AM. Differences between serious and nonserious patient safety incidents in the largest Hospital district in Finland. J Healthc Risk Manag. 2018;38(2):27–35. | ||
National patient safety Agency. Patient safety incident reports in the NHS: reporting and learning system quarterly data summary. Available from: http://www.nrls.npsa.nhs.uk/patient-safety-data/. Accessed May 30, 2018. | ||
Thomas EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care. 2000;38(3):261–271. | ||
Bagenal J, Sahnan K, Shantikumar S. Comparing the attitudes and knowledge toward incident reporting in junior physicians and nurses in a district general hospital. J Patient Saf. 2016;12(1):51–53. | ||
Davis P, Lay-Yee R, Briant R, Ali W, Scott A, Schug S. Adverse events in New Zealand public hospitals I: occurrence and impact. N Z Med J. 2002;115(1167):U271. | ||
Namiki J, Yamazaki M, Funabiki T, Hori S. Inaccuracy and misjudged factors of Glasgow Coma Scale scores when assessed by inexperienced physicians. Clin Neurol Neurosurg. 2011;113(5):393–398. |
Supplementary materials
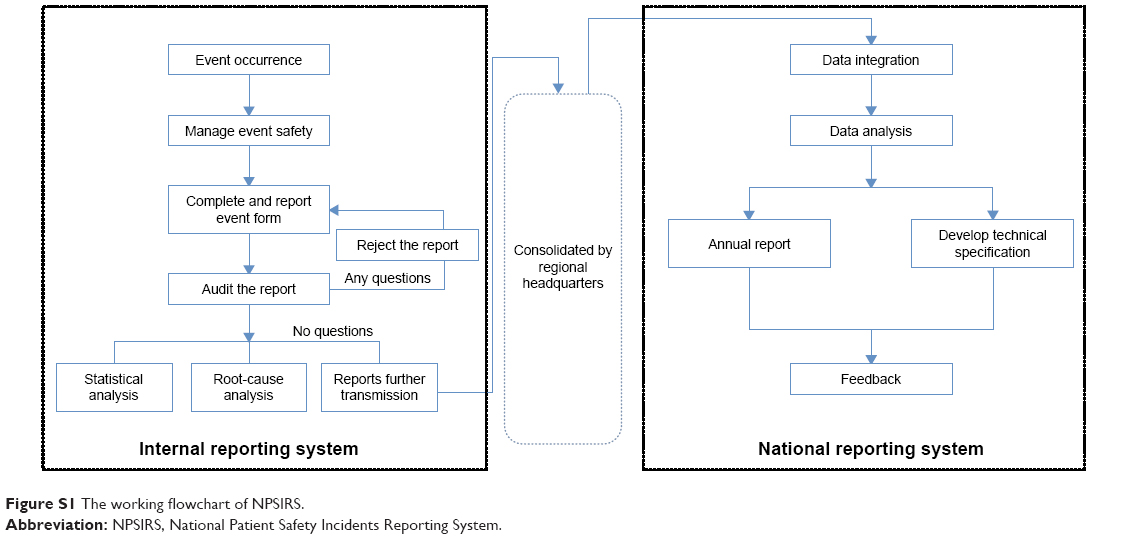 | Figure S1 The working flowchart of NPSIRS. |
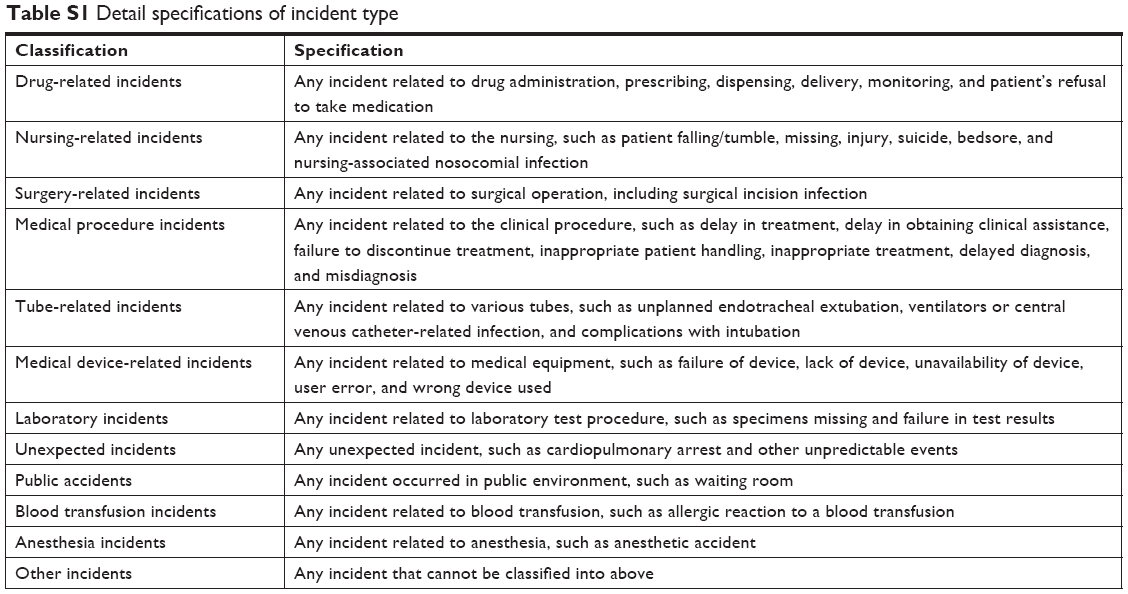 | Table S1 Detail specifications of incident type |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.