")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Implementation of the National Health Insurance Scheme (NHIS) in Ghana: Lessons for South Africa and Low- and Middle-Income Countries
Authors Christmals CD, Aidam K
Received 11 January 2020
Accepted for publication 30 June 2020
Published 2 October 2020 Volume 2020:13 Pages 1879—1904
DOI https://doi.org/10.2147/RMHP.S245615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kent Rondeau
Christmal Dela Christmals,1 Kizito Aidam2
1Research on the Health Workforce for Equity and Quality, Centre for Health Policy, School of Public Health, University of Witwatersrand, Johannesburg, South Africa; 2Department of Bacteriology, Noguchi Memorial Institute for Medical Research, University of Ghana, Accra, Ghana
Correspondence: Christmal Dela Christmals
Research on the Health Workforce for Equity and Quality, Centre for Health Policy, School of Public Health, University of Witwatersrand, South Africa
Email [email protected]
Background: South Africa is having difficulties in rolling out the National Health Insurance(NHI) policy. There are ongoing arguments on whether the NHI will provide access to quality and equitable healthcare it is intended to and whether South Africa is ready to implement the policy. Many stakeholders believe the country needs more preparation if the policy will be successful. Ghana, on the other hand, has successfully implemented the National Health Insurance Scheme(NHIS) for over 15 years.
Objective: This paper sought to explore the implementation of the NHIS in Ghana and the lessons South Africa and other low- and middle-income countries can learn from such a process.
Methods: A scoping review was conducted using the Joanna Brigs Institute’s System for the Unified Management, Assessment and Review of Information (SUMARI) and Mendeley reference manager to manage the review process. Journal articles published on the NHIS in Ghana from January 2003 to December 2018 were searched from Science Direct, PubMed, Scopus, CINAHL, and Medline using the keywords: Ghana, Health, and Insurance.
Results: The implementation of the NHIS has provided access to healthcare for the Ghanaian population, especially to poor and vulnerable . Despite the successful implementation of the NHIS in Ghana, the scheme is challenged with poor coverage; poor quality of care; corruption and ineffective governance; poor stakeholder participation; lack of clarity on concepts in the policy; intense political influence; and poor financing.
Conclusion: The marked inequity in the South African health system makes the implementation of the NHI inevitable. The challenges experienced in the implementation of the NHIS in Ghana are not new to the South African healthcare system. South Africa must learn from the experiences of Ghana,a context that shares common socio-cultural and economic factors and disease burden,in order to successfully implement the NHI.
Keywords: national health insurance, universal health coverage, Ghana, South Africa, lower-middle income countries, sub-Saharan Africa
Introduction
National Health Insurance (NHI) is the lifeblood of Universal Health Coverage (UHC) globally, especially in sub-Saharan Africa.1,2 Many advanced nations have implemented various modifications of the Beveridge, Bismarck, or private health insurance models.3 In sub-Saharan African countries such as Ghana, Kenya, Nigeria, Tanzania, and Uganda, different forms of health insurance were observed. These health insurances are primarily community-based.4–6
In Ghana, the National Health Insurance Scheme (NHIS) was established in August 2003 to promote access to equitable and quality healthcare for all citizens, irrespective of the individual’s socio-economic features.7 The National Health Insurance Authority (NHIA) governs the scheme. The National Health Insurance Fund (NHIF), as stipulated in Act 650 of 2003, was set up to fund the healthcare of Ghanaians.7 The NHIF generates its cash inflow from five sources including 2.5% of the 17.5% Value-Added Tax (VAT), 2.5% of the 17.5% Social Security and National Insurance Trust (SSNIT) from formal sector employees, dividends of investments made by the NHIA, donations, and premiums paid by scheme subscribers.8,9 The scheme provides premium exemptions for the elderly (70 years and above), SSNIT pensioners, children below 18 years, pregnant women, and the beneficiaries of the Livelihood Empowerment Against Poverty (LEAP) – a pro-poor social intervention carried out by the central government.10 The insurance scheme covers 95% of the burden of diseases in Ghana.10 Services covered by the scheme include out-patient services, in-patient services, maternity care, eye care, and oral healthcare services.10
At the inception of the NHIS, the payment of healthcare providers was through itemized fee-for-service. However, in 2008, the Ghana Diagnostic Related Groupings (G-DRGs) for services and fee-for-service for medicines at all levels of service delivery was introduced in a reform. Under this system, the NHIS District/Municipal/Metropolitan offices engage the various NHIS certified health facilities on a contract basis. The health facilities then provide services for the NHIS subscribers and submit claims for services rendered to the NHIS District/Municipal/Metropolitan offices for reimbursement.11
Like any other policy, the implementation of the NHIS achieved some successes but had challenges. South Africa is having difficulties in rolling out the NHI policy. There are ongoing arguments on whether the NHI will produce the access, equity, and quality healthcare it is intended to, and whether South Africa is ready to implement the policy.12 Many stakeholders believe the country needs more preparation if the policy will be successful.13 Ghana, on the other hand, has successfully implemented the NHIS for over 15 years. South Africa and other countries with similar geography, disease burden, economic grouping, and sociocultural context could learn from the successes and the challenges of Ghana in developing National Health Insurance and Universal Health Coverage funding models for low- and middle-income countries.
Aim
This scoping review sought to explore the 15 years of implementation of the NHIS in Ghana and the lessons South Africa and other low- and middle-income countries can learn from such a process.
Design
A scoping review is either a pre-systematic review or a standalone review that seeks to map the breadth and depth of evidence in a field of study.14,15 This scoping review was conducted using the Joanna Brigs Institute’s (JBI) System for the Unified Management, Assessment, and Review of Information (SUMARI) and Mendeley reference manager to manage the review process.16 The scoping review method was chosen because it better synthesizes findings from both the positivist and the constructivist paradigms than other review methods.17 The JBI SUMARI provides a computerized framework for the reviewers to follow in conducting the review.
Search and Inclusion
Journal articles published on the NHIS in Ghana from January 2003 to December 2018 were searched from Science Direct, PubMed, Scopus, CINAHL, and Medline using the keywords; Ghana, Health, and Insurance. The search terms used were made broad so as to find approximately all studies on the National Health Insurance Scheme of Ghana over the 15 years. The PCC criteria, representing Population of interest (P), Concept (C), and the Context (C) guided the inclusion of studies in this review.
- The population of interest (P): represents all institutions and individuals involved in the implementation of the National Health Insurance Scheme in Ghana.
- The Concept (C): is the Implementation of the National Health Insurance Scheme.
- Context (C): represents the healthcare system of Ghana.
The review question, “how was the National Health Insurance Scheme implemented in Ghana” guided the scoping review. Studies were included if they were full journal articles published in English, written on the implementation of the National Health Insurance Scheme of Ghana from January 2003 to December 2018.
Critical Appraisal
The JBI evidence-based critical appraisal tools were used by three JBI trained reviewers to appraise the studies included in this study. . A minimum of two recommendations were necessary for inclusion. A study was included if it met 80% of the quality criteria set by the appraisal tool. All full-text articles appraised were included.
Data Collection
The second author extracted the findings from all studies included onto the SUMARI page for this review. The findings extracted onto the SUMARI were reviewed by the first author to ensure it was accurate. The finalized data extraction sheet is presented in a data matrix (Table 1).
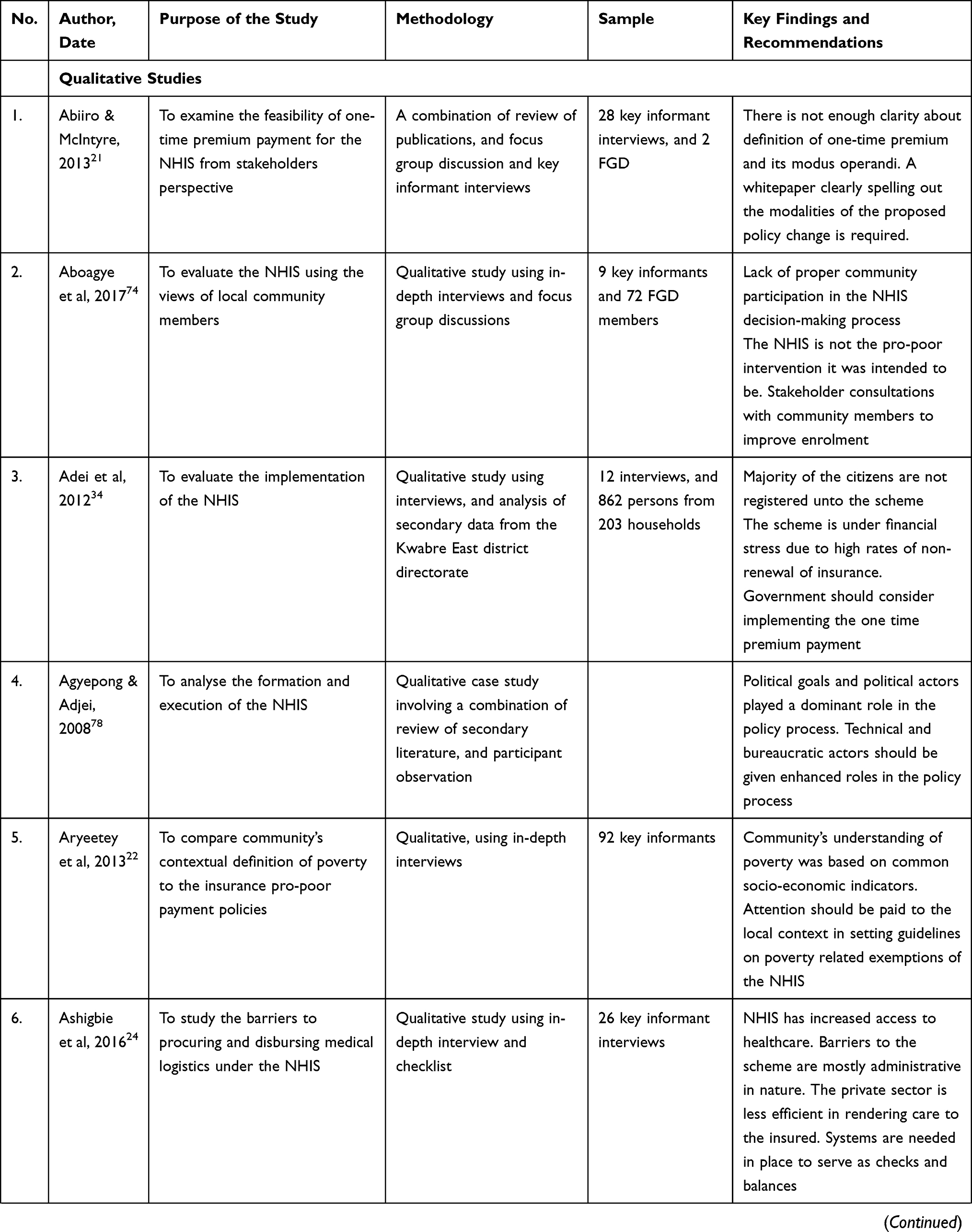 |  | 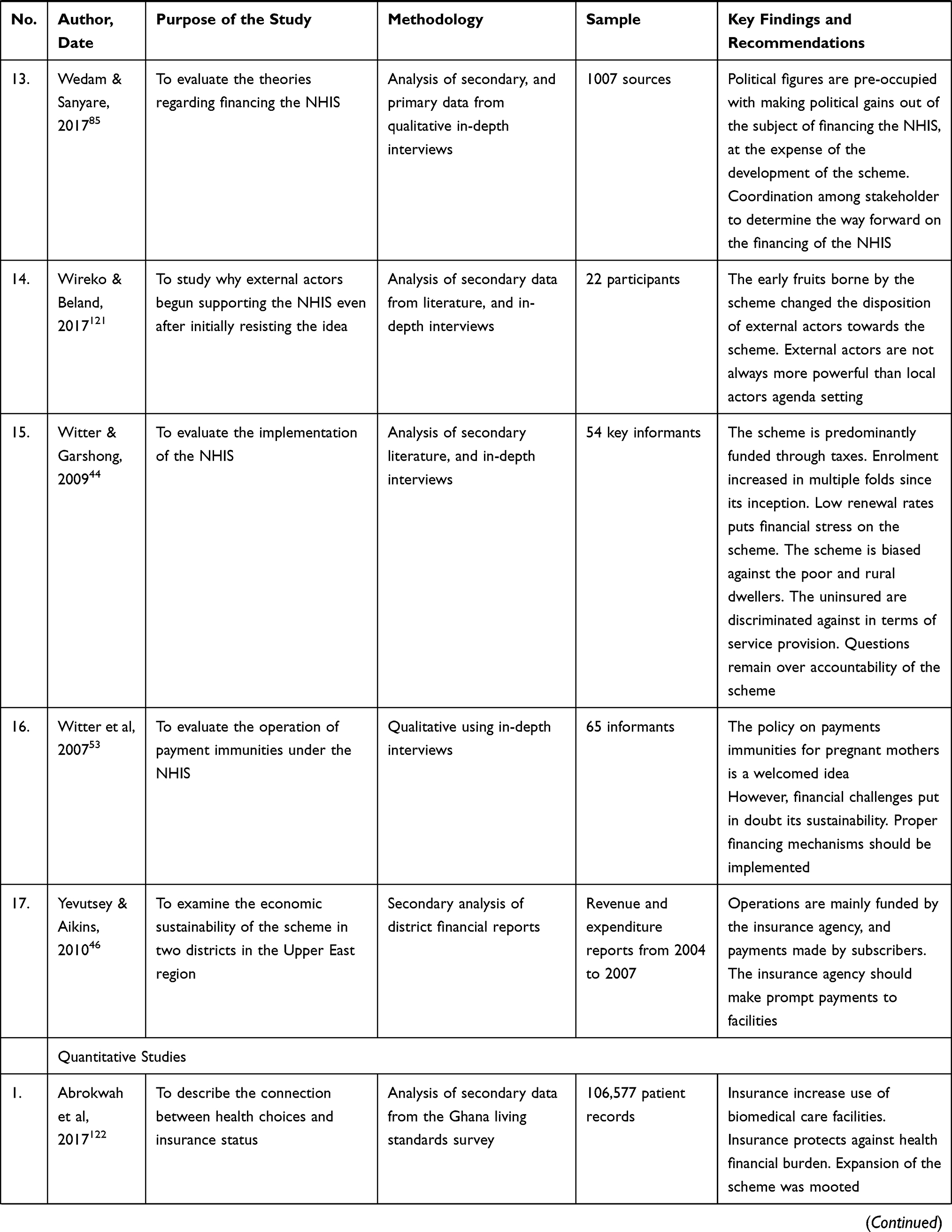 | 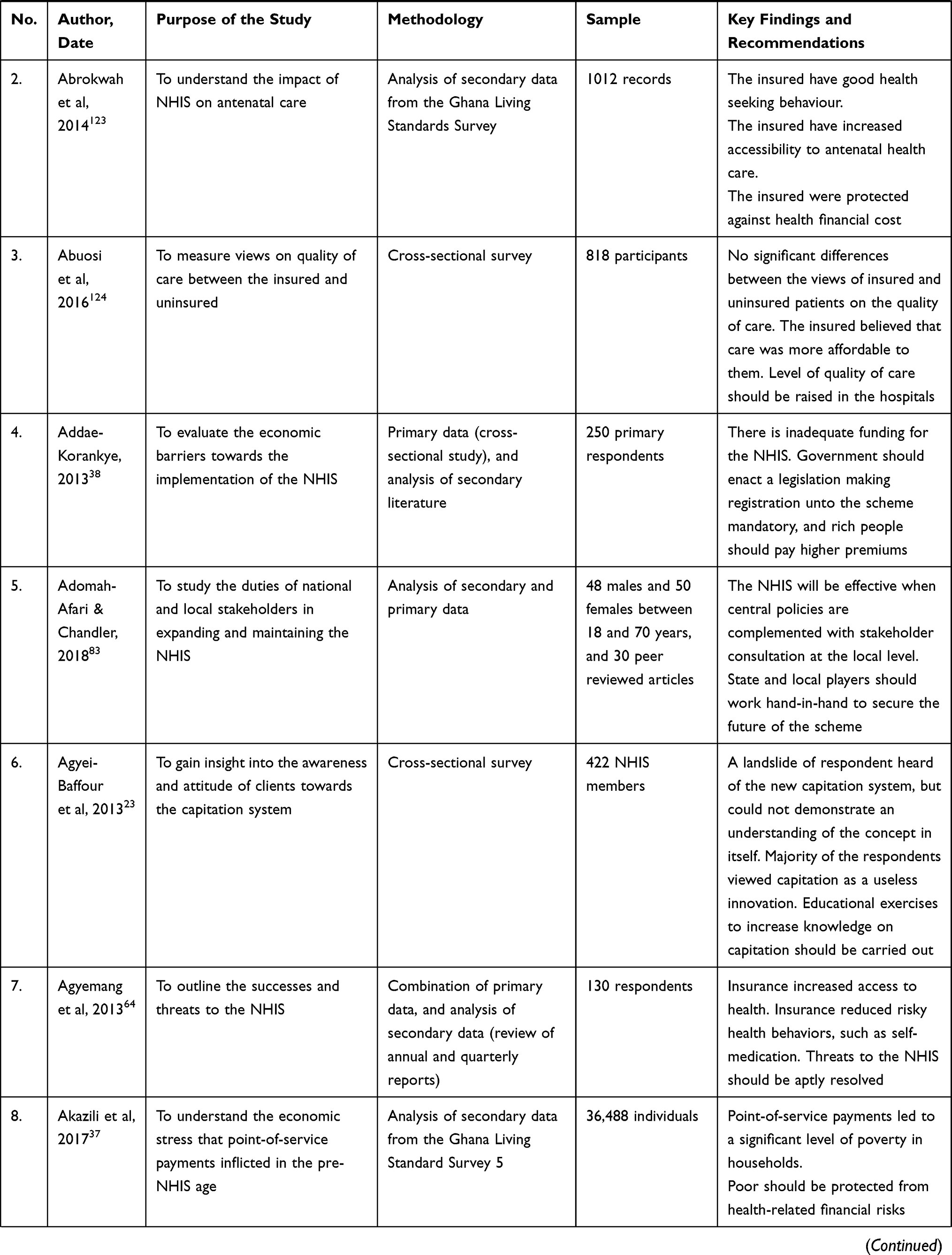 | 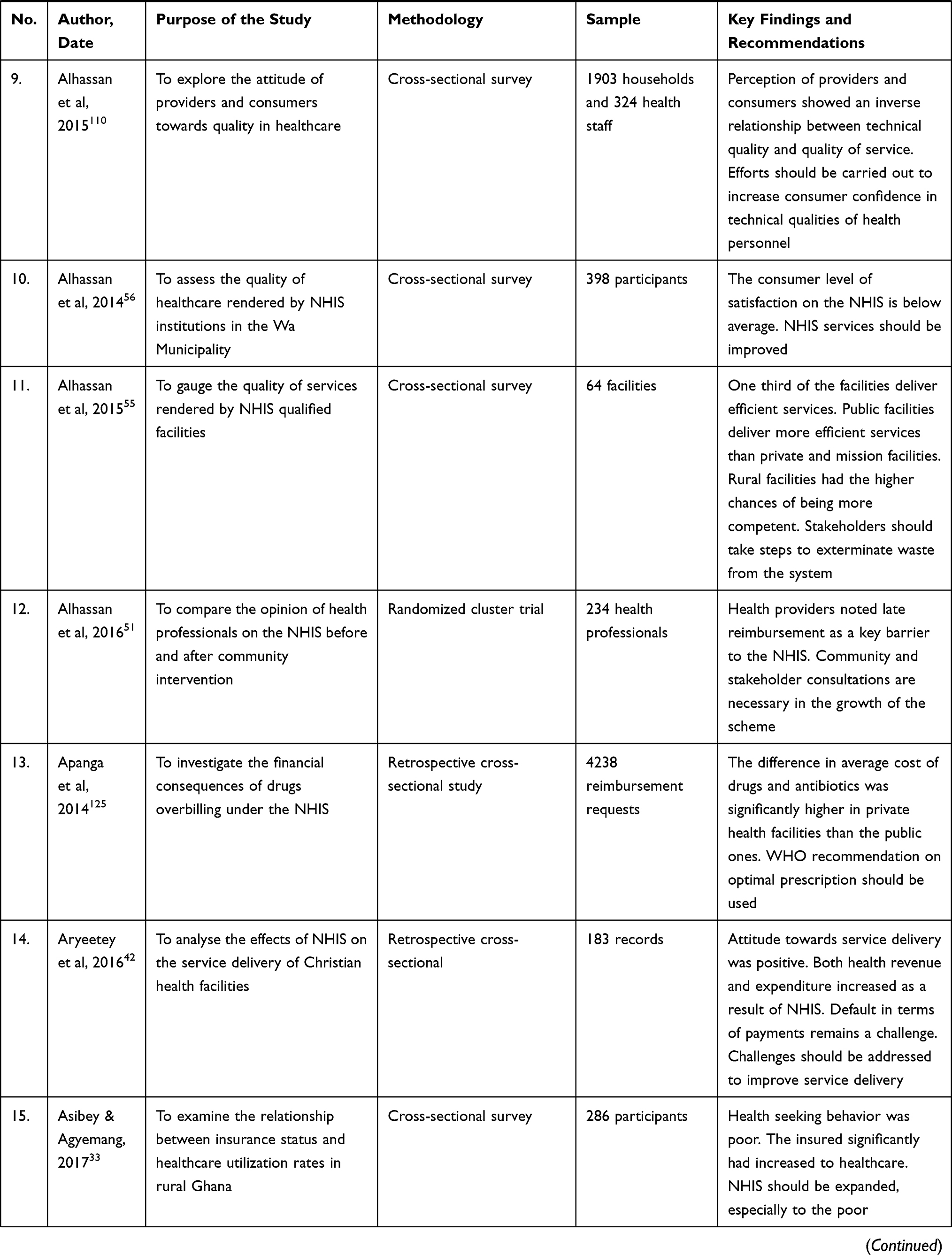 | 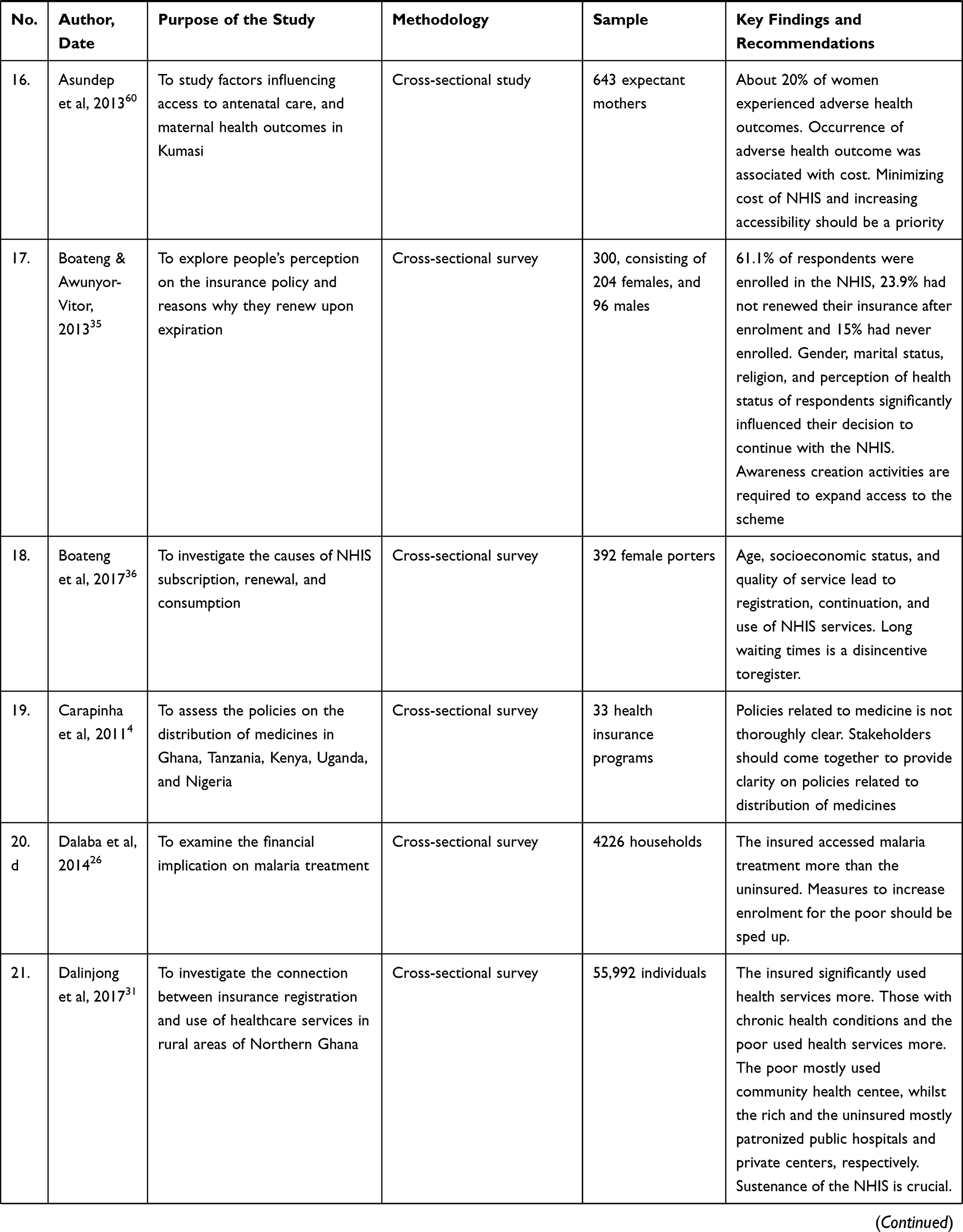 | 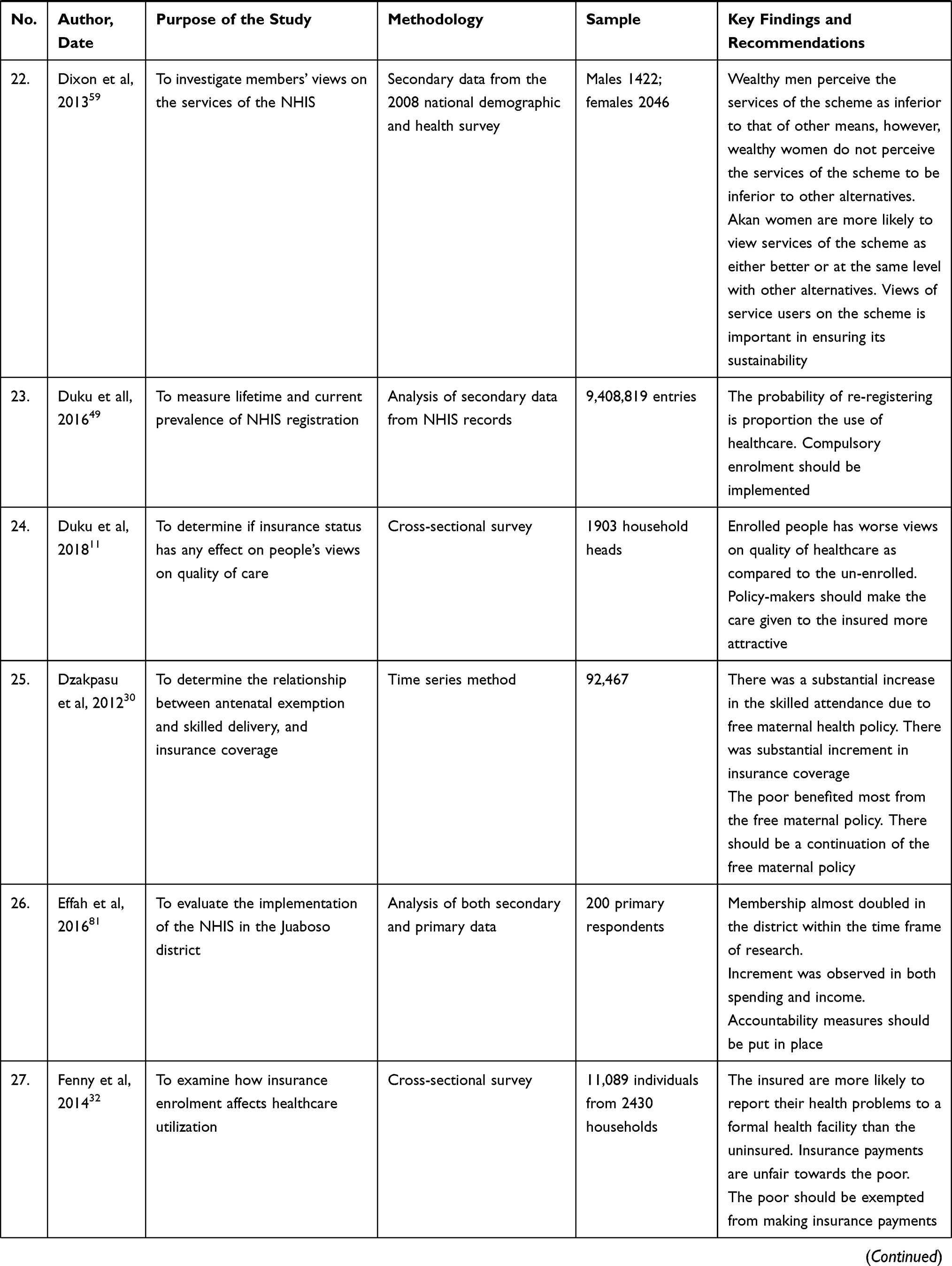 | 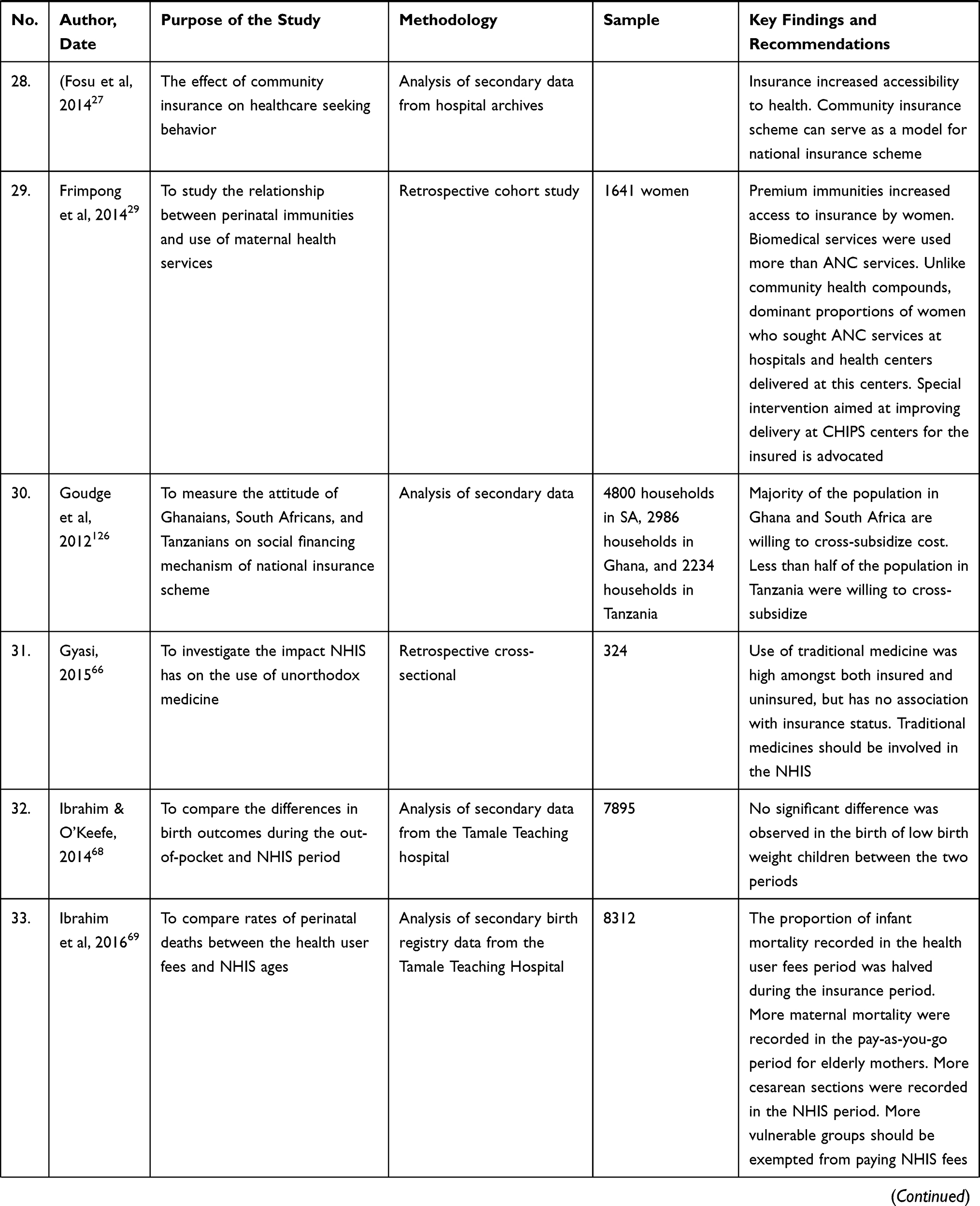 | 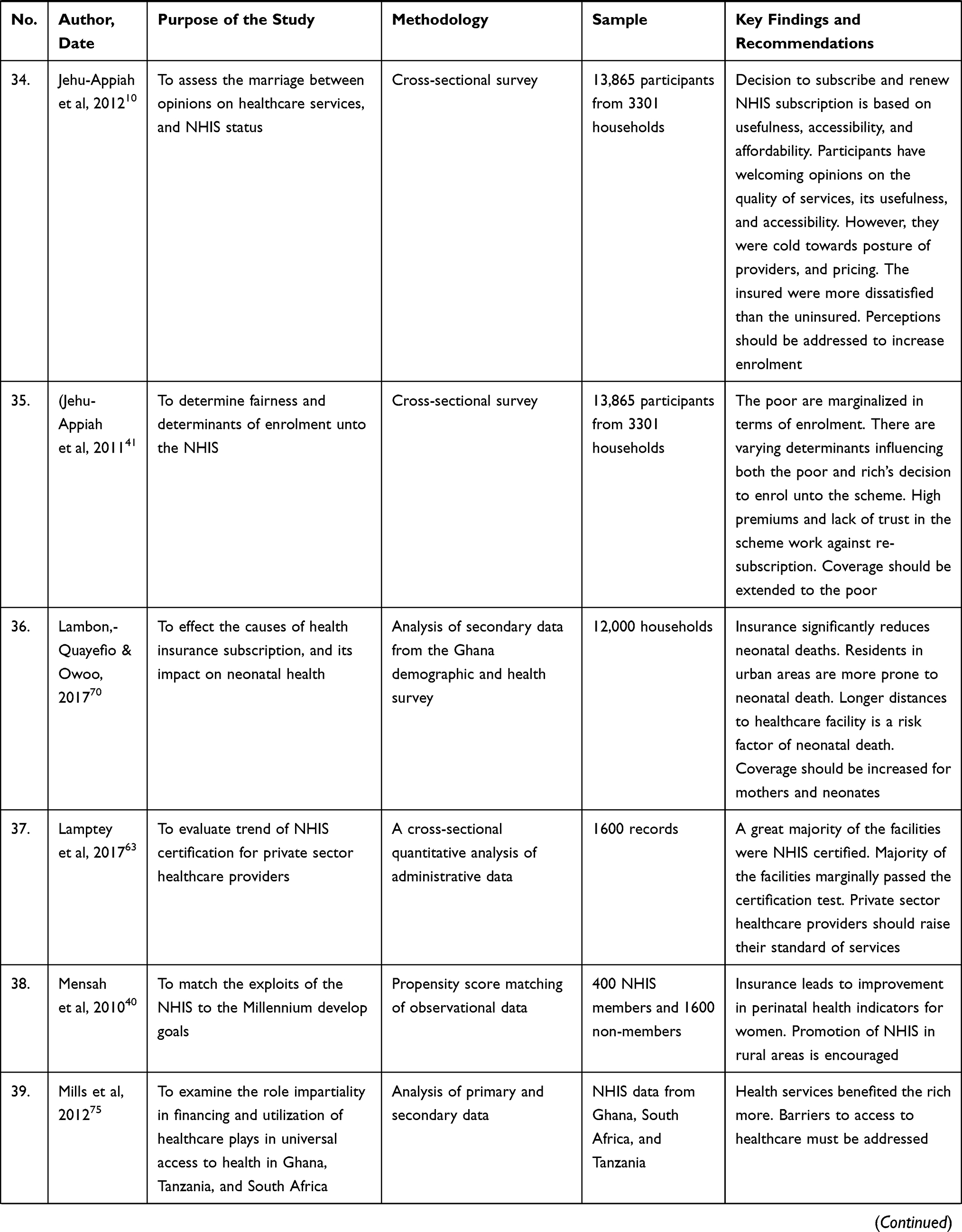 | 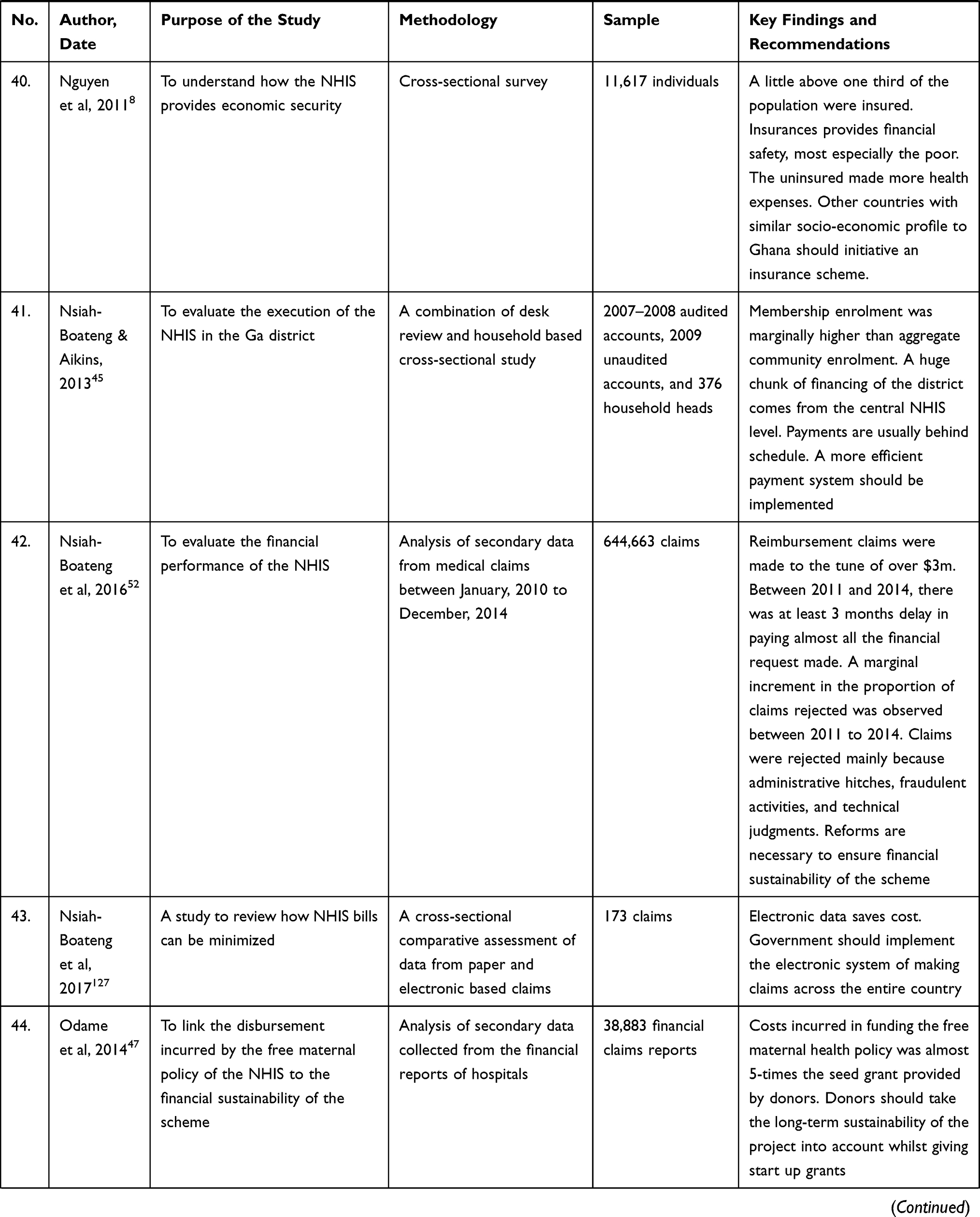 | 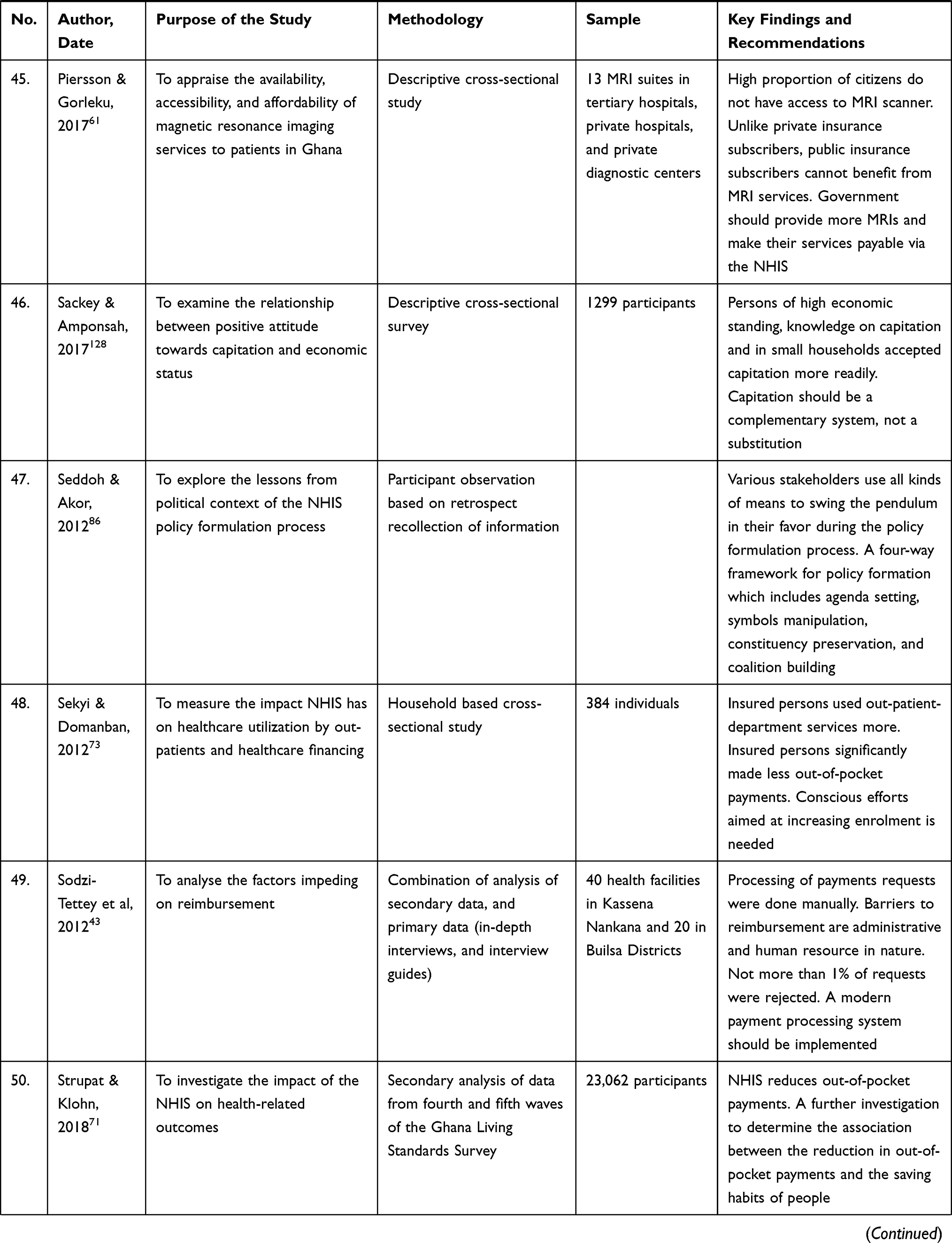 | 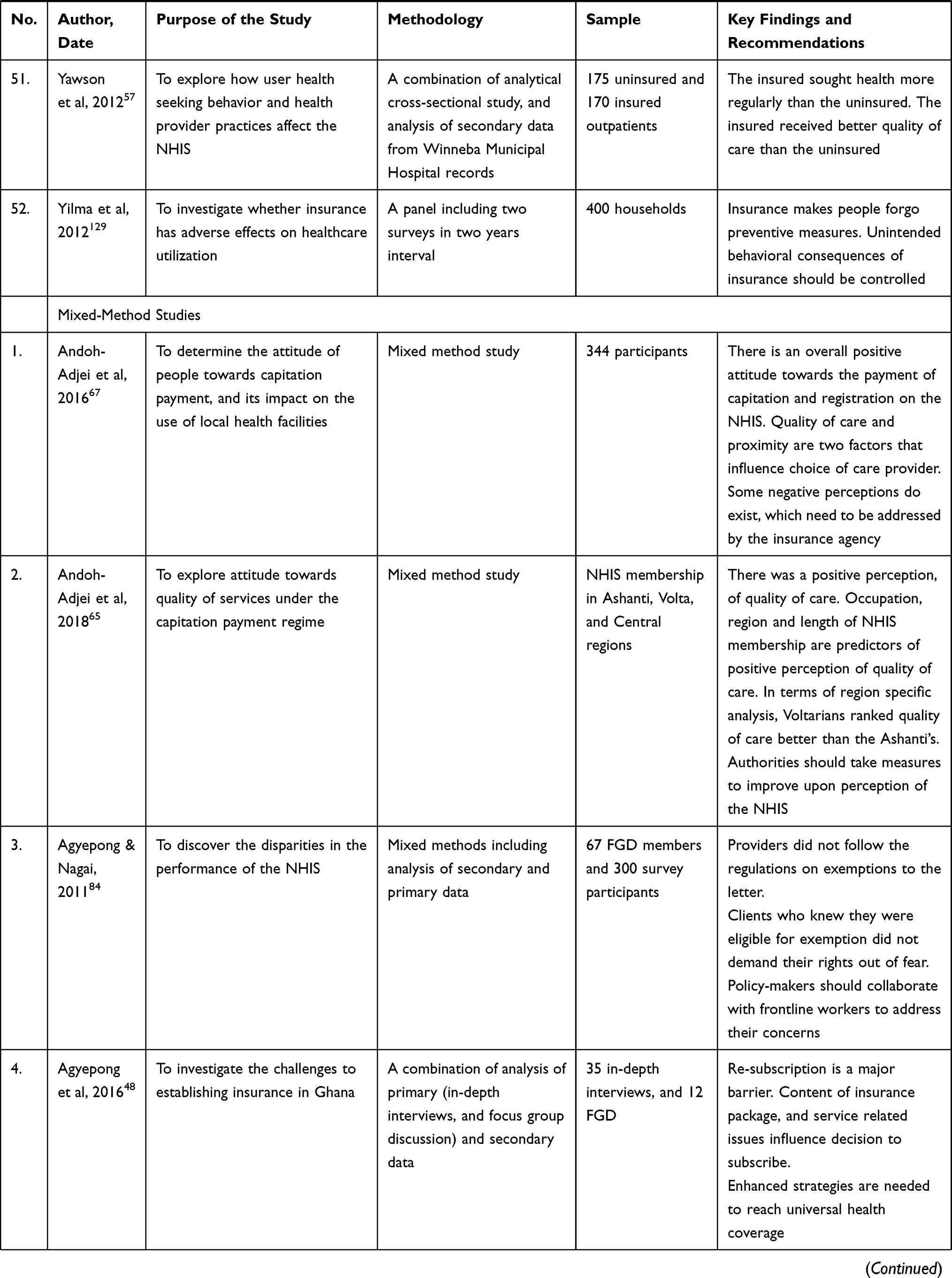 |  |
Table 1 Data Matrix |
Data Synthesis
Quantitative data were transformed through a qualitizing process then synthesized with the qualitative data using a convergent integrated approach.18,19 The assessment of the certainty of the evidence from the studies was not done due to the complexity of recommendations from studies included and the quantitative data transformation process. Also, this was a scoping review, and the reviewers did not seek to compare phenomena and make judgments, hence the exclusion of assessment of certainty. The review process and the results were reported according to the PRISMA Extension for Scoping Reviews (PRISMA-ScR) reporting checklist.20 The findings extracted on the data matrix were coded independently by the two reviewers, and the codes were compared and discussed for intercoder agreement. The codes were refined based on the intercoder agreement for final coding. Similar codes were combined into sub-themes and related sub-themes into themes, as presented in the Results section.
Results
Seventy-seven of the 418 studies found on the NHIS were included (Figure 1). Figure 2 shows the trend of publications from the year of inception until December 2018. There were no empirical studies published within the first 4 years (2003–2006) of the implementation stage. Studies increased from 2007 to 2012, decreased from 2012 to 2015, then recorded a sharp rise in 2016, which remained constant in 2017 and then sharply decreased in 2018. Generally, the trend line shows a steady increase in publications from the inception of the scheme in 2003 to December 2018. The findings from the studies included in the review were synthesized below.
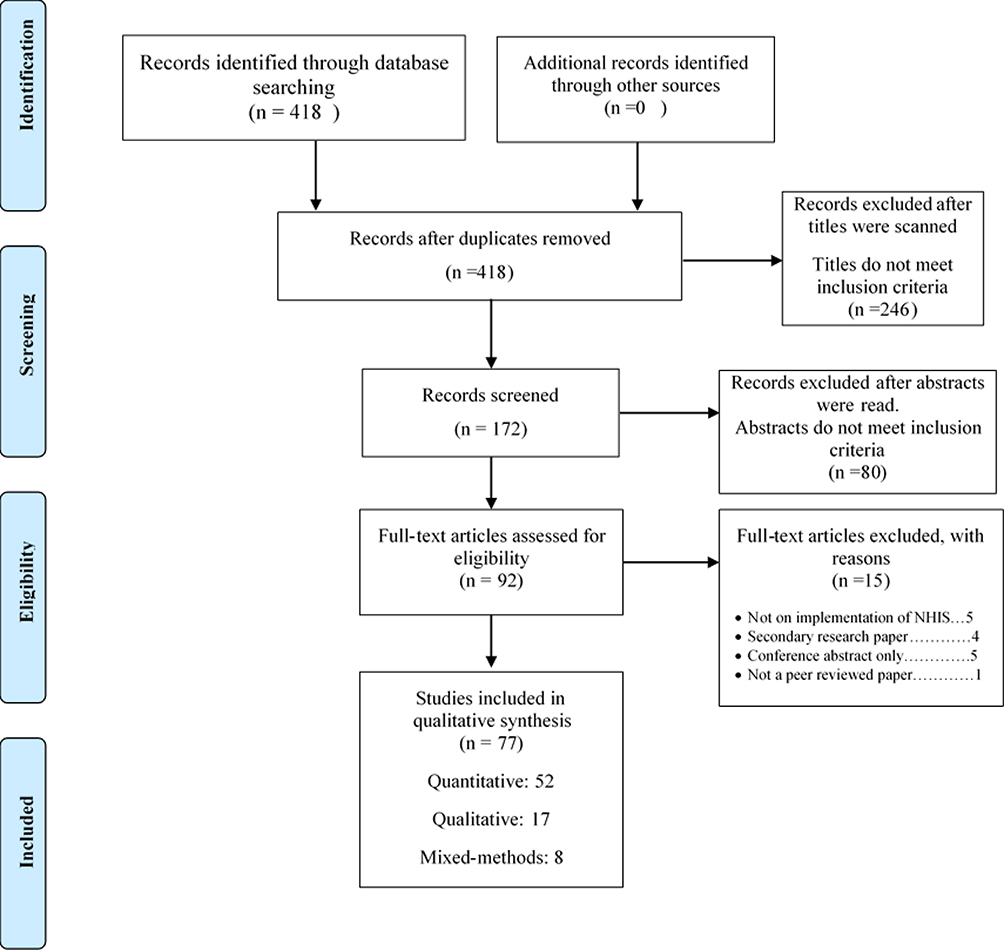 |
Figure 1 Search, appraisal, and inclusion of studies. |
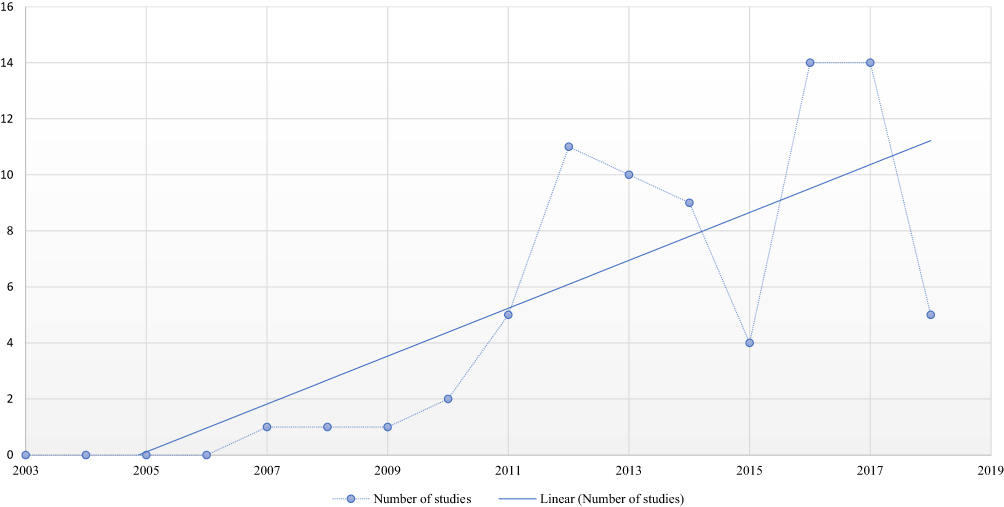 |
Figure 2 Yearly distribution of studies included in the review. |
Clarity of Policy
Social policy affects the total population. The National Health Insurance policy is written in English only. Even the academics are seeking clarification on the content of the policy.4,21 Aryeetey et al22 discovered that the users do not understand the concept of poverty as stated in the NHIS document. Also Agyei-Baffour et al23 found that some Ghanaians do not fully understand the premium payment concepts though they hear of them. Researchers are advocating for a white paper that clearly defines the major concepts, comprehensive stakeholder engagement, and public education on the NHIS policy document.4,21
Coverage
The NHIS has made care accessible and affordable in Ghana.24–28 Some groups of people such as the aged, children, and pregnant women are given immunity against premium payment.28,29 This helped in removing some socio-economic barriers to healthcare.29,30 In terms of healthcare-seeking behavior, people who are registered in the scheme use healthcare services more than those who are not insured.30–33
Though the NHIS increased access to healthcare, this access is far from universal, as it demands premium payment before one can access healthcare. Many studies8,–32,–34–36 reported varying proportions of the population who are not covered by the scheme; a World Bank study7 reported that only 40% of the Ghanaian population were enrolled in the scheme by 2013. The actual figures and percentage of the population covered by the scheme from 2005 to 2017 are presented in Figure 3.
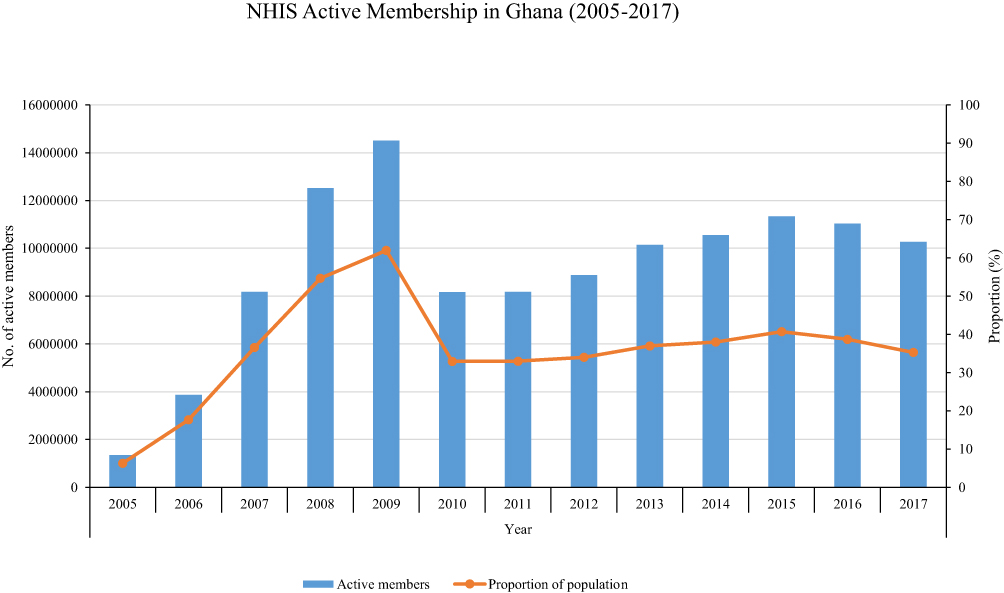 |
Figure 3 NHIS Active Membership from 2005 to 2017 (Source: National Health Insurance Authority118 119; Nsiah-Boateng & Aikins120 2018). |
Though the scheme covers the major disease burden of the country, other services are not under the scheme. Many citizens are not eligible to access care because they are not enrolled in the scheme due to financial problems. The scheme is expected to protect Ghanaians against the cost of healthcare but it rather excludes the very poor, thereby increasing the financial burden on the poor. Ghanaians should not use the international definition of poverty as exemption criteria for premium payment as many local context variables are unique to the concept of poverty in Ghana.22,32,37 Fenny et al32 also suggested that the poor should be exempted from making insurance payments. The financial barriers need to be eliminated if the scheme is to fulfil the Universal Health Coverage mandate.26,–37–39 Asundep et al30 believe that minimizing the premium and increasing access is essential. The free maternal, child, and aged care policy is laudable and should be continued. The more vulnerable groups should be exempted from paying the NHIS premium. This will ensure that coverage is extended to the poor.40,41
Financing
Both health revenue and expenditure increased because of NHIS.42 Enrolment in the scheme increased continually, though there was a high rate of non-renewal putting the scheme under high financial stress. This section describes the sources of funding, subscription, and renewal. In a study to enlist the challenges that the implementation of the NHIS has encountered, Sodzi-Tettey et al43 discovered that the scheme was threatened by organizational, financial, and administrative problems. The authors recommended, amongst other things, the adoption of a more modern payment system to salvage the future of the scheme.
Funding
The scheme is predominantly funded through taxes, specifically 2.5% of the 17.5% VAT, 2.5% of the 17.5% SSNIT from formal sector employees, dividends of investments made by the NHIA Council, donations, and premium payments.44–46 Addae-Korankye38 revealed that there is inadequate funding for the NHIS. Costs incurred in funding the free maternal health policy were almost 5-times the seed grant provided by donors.47
Enrolment and Resubscription
Enrolment and resubscription is a major barrier under the scheme.48 Enrolment in the scheme increased in multiple folds since its inception.44 Many studies8,32,34–36 reported varying proportions of enrolment. Boateng and Awunyor-Vitor35 discovered that out of the 61.1% of their respondents who were enrolled in the NHIS, 23.9% had not renewed their insurance after enrolment.35 High rate of non-renewal put the scheme under financial stress.34 Factors that influenced resubscription included age, economic status, usefulness, accessibility, affordability, and perception of the quality of service provided.36,41 Also, the probability of resubscription was proportional to having used the services in the previous year.49 Adei et al34 advised that the government should consider implementing the one-time premium payment.
Reimbursement of Providers
Default in paying service providers for the services provided for clients under the scheme negatively affected the implementation of the NHIS.42,50,51 Between 2011 and 2014, there was at least 4 months delay in paying almost all the financial claims made.52 This was as a result of poor funding, manual processing of claims, and mismanagement of scheme funds.43,53 To tackle the financial challenges surrounding the scheme, researchers45,53 advocated that proper financing mechanisms should be implemented.
Service Delivery
Quality, Attitudes of Providers, and User Satisfaction
Primary healthcare centers lacked adequate resources to discharge their services, thereby providing poor quality of preventative services under the scheme.50,54 User satisfaction with the services provided under the NHIS was below average. Only one-third of the facilities delivered efficient services, public facilities delivered more efficient services than private and mission facilities.55,56 Those insured under the scheme were more dissatisfied with service provided than the uninsured,10,11 in contrast to the findings of Yawson et al57 that the insured received a better quality of care than the uninsured. Dalinjong and Laar58 also reported that both insured and uninsured were satisfied with the quality of treatment they received.
The poor mostly used community health centers, whilst the rich and the uninsured mostly patronized public hospitals and private centers, respectively.31 Wealthy men perceived the services of the scheme as inferior to other mmodes, however, wealthy women did not perceive the services of the scheme to be inferior to other alternatives.59 Unlike community health compounds, dominant proportions of women who sought ANC services at hospitals and health centers delivered their babies at these facilities.29 Rural facilities had higher chances of being more competent than urban ones.55 Asundep et al 60 found that 20% of women accessing care through the scheme experienced adverse health outcomes.60 A high proportion of citizens did not have access to an MRI scanner.61 Also, long waiting time in the hospitals was a disincentive for people to subscribe to the scheme.36 Quality improvement measures should be instituted to improve the quality of services provided to the clients, especially in the private healthcare facilities.62,63
The access and financial protection provided by the scheme have improved health-seeking behaviors and reduced risky health behaviors such as self-medication among Ghanaians.64 Though some studies42,65 reported a positive attitude of providers towards service delivery, others10 reported poor attitudes of providers. Use of traditional medicine was high amongst both insured and uninsured but had no association with insurance status.66 Quality of care and proximity were two factors that influenced the choice of care provider.67
Outcomes
Those insured under the scheme believed that providers had poorer attitudes towards them than those who are not insured under the scheme.58 There was no statistically significant difference in the occurrence of low birth weight in before and after the implementation of the NHIS.68 However, the proportion of infant mortality recorded before the implementation of the scheme was halved during the insurance period; likewise, more maternal deaths were recorded in the previous system as compared to the NHIS regime.69 Also, a higher number of cesarean sections were conducted in the NHIS period than before.69 Lambon-Quayefio and Owoo70 observed that insurance significantly reduced neonatal death. Mensah et al40 also recorded that insurance leads to improvements in perinatal health indicators for women. Nguyen et al,8 Strupat and Klohn,71 and Aryeetey et al72 also found that the uninsured had more health expenses than the insured. Therefore, the insured sought to use health services more than the uninsured.57,58,73
Failures/Challenges
After 10 years of implementation (2003–2013) less than 40% of the population of Ghana had subscribed to the NHIS. National coverage or UHC is far from reach at this pace. National Health Insurance as portrayed by the government and the policy document is to protect the population against the negative consequences of the cost of healthcare. Though the NHIS was envisaged to be more preventive than curative it has lost its preventive nature and is currently more curative .24 The scheme is not as pro-poor as it has been envisaged.74 Mills et al stated that the policy favored the rich rather than the poor it was intended to, creating much more burden on the poor.75 Because, the rich and the poor pay the same amount to subscribe to the scheme but the rich access private fee-for-service healthcarewhen the NHI accredited facilities run out of medicines and other healthcare supplies.
Systemic corruption in sub-Saharan African institutions is a threat to the sustainability of the financial model in Ghana. Healthcare institutions issue false claims for reimbursement; some healthcare users admitted conniving with healthcare providers to defraud the scheme.25,76 Systems need to be put in place to keep the policy relevant to its purpose. As the health system develops and the health needs of the population change, a policy review will be necessary to make it effective.
Governance
This section covers system design, coalition building, transparency, oversight, and accountability.77 The sustainability of the NHIS in Ghana is of grave concern. It seems as though the implementation of the scheme was rushed.78 There was more emphasis on the roles of political actors than the technical insight provided by experts in the field of public health insurance policy.78 Whilst recognizing the crucial role that the political elite play in the formulation of public policy, Agyepong and Adjei78 cautioned that the overarching influence that the political class had on the program design and implementation could be a threat to the realization of its goals and objectives .
Financial Management
There are enough sources of funding for the scheme; corruption, mismanagement, lack of transparency in the funding, claims, and reimbursement issues should be checked by the leadership of the scheme. The government should implement the electronic claims, verification, and reimbursement system across the entire country to curb corruption and default in reimbursement of facilities.46,52 There is too much wastage in the NHIS, which should be dealt with by various stakeholders.55 Measures should be put in place to reach 100% subscription and resubscription status to raise more funds for the scheme.49 Also, the rich should be made to pay more to increase the funds for the scheme.38
System Design and Oversight
Political machinations and poor monitoring and evaluation hinder the smooth running of the scheme.54 Other challenges to the scheme are in the form of inadequate workforce and weak institutional arrangements and transparency.43,44,79 Administration at both central and local levels affect the decision of people to subscribe to the scheme and continue their subscription.80 The NHIS needs to be reviewed to ensure good leadership and governance, transparent and accountable institutional arrangement, and effectiveness and sustainability of the scheme.79,81,82
Community Participation
Lack of community participation is a common phenomenon in SSA. Many studies23,50,51,59,74,83 reported lack of community participation in the NHIS policy formulation and implementation. The policy resulted from a political campaign and the stakeholders knew only the intended political messages. They were not further educated on the consequences of registering or not as well as the details of the technical language that was contained in the policy document. Many people cannot demand services because they either do not understand or are afraid to ask questions about the package.84 People need to be empowered to demand services they are due. 84 Researchers recommended the need for stakeholder consultation in improving and sustaining the scheme.50,51,59,74,83
Competing Interest
Politicians attempted to make political gains out of the finances of the scheme at the expense of the development of the scheme.85 Because it was a political campaign promise, stakeholder consultation and input produced friction, as the politicians pushed to achieve their campaign promises, whether realistic or not. It is necessary for the politicians to know their boundaries and delegate the technocrats to superintend policies of such a magnitude.78 Other stakeholders of the scheme also tried to swing the policy in their favor using all means.86 Institutional arrangements among all stakeholder groups should be determined with terms of reference that will enhance the policy implementation. There is need for all stakeholders to clearly understand the content of the policy to avoid ambiguity and role conflicts.4,85
Discussion
From the results, Ghana has contributed much in efforts and funding to make the NHIS work but has struggled with issues of coverage, funding, stakeholder participation, and governance. Corruption and political interference are also seen as major threats to the sustenance of the scheme.
The proportion of the population enrolled in the NHIS from its inception has been less than 41%, apart from 2008 and 2009 where the scheme unexpectedly recorded 54.66% and 61.97%, respectively. This was attributed to the inability of the Scheme management to exclude the members who had not renewed their membership since the inception of the scheme. In 2008, the NHIS was at the center stage of the national election campaign, and politicians were seen enrolling people as part of the election campaign. This may also account for the higher figures in 2009 as elections were held in December 2008. Other reports cited indicated that the scheme had difficulty in reimbursing service providers coupled with administrative challenges, resulting in dissatisfaction of members who intentionally did not renew their membership. This resulted in a sharp decline in membership to 32.95% in 2010. The scheme recorded a slow increase in membership from 2010 to 2015; then took another downward stroke due to apathy among subscribers as a result of the delay in reimbursement of health service providers and charging of unapproved fees.87,88
Unlike Ghana, South Africa will not have issues with subscription, premium payment, and waivers for certain groups of people. The NHI bill provides for free healthcare for all South Africans.89 This allows healthcare to be completely accessible to all the population. Many stakeholders in South Africa are seeking clarification on the source of funding, modes of facility reimbursement, and the ability of the system to resist corruption.90–96 These critical questions need to be addressed to avoid system collapse. Various forms of inclusive sources of funding should be prioritized as well as efficient use of resources within the NHI in South Africa.91,96 The gross inequity in South Africa may be deepened if the system is not designed to address resource allocation and funding mechanisms.
The financial stress that the NHIS is subjected to is partly because 65% of the active members are exempted from paying premiums. This group is made up of mostly pregnant women, children under 18 years of age, the aged (70 years and above), and indigents. Though the exemption has led to increased access to quality healthcare by the exempted groupings, the burden of the care provided stresses the NHIS financially. Enough funding is made available from the various sources of funding, for example, the highest claims paid to health facilities was 81.1% of total income by the scheme. Poor governance and corruption as a result of poor stakeholder participation and political influence were cited as the major challenges threatening the financial sustainability of the scheme.43,4547,52,53
Even though the private sector caters for the health needs of 16% of the South Africans as opposed to the 84% that the public sector serves, private sector consumers account for 52% of the nation’s health sector budget, whilst the public sector accounts for a paltry 48%.97 The gross inequality created by the huge but less funded public sector and small but heavily funded private healthcare system is alarming and needs a system redesign. The National Health Insurance is a strategic political attempt to bridge the healthcare access and quality gap between the poor and the rich by the African National Congress.98 The entire NHI policy was expected to be rolled out in three phases within 14 years from 2012.99 After 7 years, stakeholders are concerned about the implementation of the NHI, especially in the areas of quality of the healthcare, corruption, mismanagement of funds, fear of overcrowding of private hospitals, poor attitudes of healthcare workers, and reimbursement mechanism.90,98,100–103
As seen in Ghana, both private and public healthcare sectors in South Africa have come under intense criticism regarding the quality of healthcare provided.104 Many believe that the current public health system needs a system clean-up and reorientation because of gross mismanagement, corruption, and poor quality of services provided.98 Though there is a general positive perception about the quality of healthcare provided in the private sector, 104 findings from a study conducted by the University of Cape Town revealed high malpractice within the private sector in South Africa.105 Though the NHI/UHC policies increase access to healthcare, it is necessary to look at the quality of care provided within the UHC, as poor quality of care tends to be costly in the long-term.106–108
In South Africa, the majority of the stakeholders believe that the policy-shift is inevitable. The fear, however, is the clarity in the roles of all stakeholders.109 General practitioners and specialists who practice or moonlight in the private sector, the private medical schemes, and the private hospital groups feel threatened and targeted by the policy. Stakeholders are calling for the NHI bill to clarify issues regarding the role of existing medical schemes, the NHI referral pathway, the benefit packages, and sources of funding.93,96
Policymakers should endeavor to involve frontline workers in addressing the concerns of the scheme.84 Communities should be encouraged through public education to expand the coverage of the scheme.35 Public awareness programs should be instituted to improve user knowledge and confidence in the scheme.110 Encouraging stakeholder participation in decision-making is widely recommended.91,109,111–113 Barker and Klopper112 reported that the community studied resisted taking power and decision-making roles in planning and delivering care. Participation in decision-making is the constitutional right of the communities in South Africa and must be respected by engaging them in critical decisions that affect their livelihood.114 Lastly, communities need to be empowered to demand accountability.
Many bright institutions have fallen because of poor and ineffective leadership in sub-Saharan Africa. Political influence in institutions that are expected to be autonomous is evident across the continent, especially when the government has a role in the appointment of the leadership and funding the institution. Corruption among healthcare leadership is a cancer that eats deep to the core of the healthcare sector in South Africa.95 Corruption is capable of making healthcare institutions resource-poor, ineffective, and produce poor quality health outcomes. Therefore, the South African healthcare system needs to be redesigned to curb corruption, especially when the NHI bill seeks to consolidate healthcare funds to be managed by boards that are accountable to a political authority, the Minister of Health.95,115
Many stakeholders also believe that the policy confers too much power on the Minister of Health to appoint and superintend committees; an ineffective or corrupt Minister of Health could destroy the well-intended healthcare system and funding mechanism. Opposition parties in parliament also believe that the NHI is a mechanism for the ruling party and its appointees to steal taxpayers’ money to enrich themselves. The Minister of Health, Dr Zweli Mkhize, however, said that the president recognizes the threat corruption poses to the insurance and has inaugurated health sector anti-corruption forum to check corruption within the NHI system.94 Good leadership and governance are essential to the implementation of NHI. Despite the imminent need for the implementation of the NHI in South Africa, the systems need to be redesigned to provide quality and resist corruption and mismanagement.98
Conclusion
The implementation of the NHIS in Ghana has provided access to healthcare for the underprivileged despite the numerous challenges. The scheme has successfully expanded care and protected the poor against the negative consequences of healthcare cost for a decade and a half. Nguyen et al8 recommended that other countries learn from the NHIS policy in Ghana, and implement a similar policy towards UHC. South Africa has a more robust economy and double the population of Ghana but has historical and sociocultural similarities with Ghana. Despite the huge capital ingestion into the healthcare sector, South African health indicators have not improved compared to countries that have similar or lesser capital inputs. This has been mainly attributed to the public–private, rich–poor, and rural–urban inequalities in healthcare delivery.116,117 The NHI policy is widely accepted as the means of eliminating inequalities in the healthcare system. Therefore, the success of NHI is imperative. Learning from a system that worked within the same region and building systems that overcome the mistakes, challenges, and roadblocks in the already implemented systems are essential.
Acknowledgment
We will like to acknowledge Professors Janet Gross and Laetitia Rispel for their support during the review process. We will also like to acknowledge Joanna Briggs Institute certified reviewers Dr Emmanuel Frimpong and Chenai Mlandu for their assistance in critical appraisal and inclusion of studies. Many thanks to the Centre for Health Professions Education, North-West University for their support during the manuscrip review phase.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There was no external funding for this study.
Disclosure
There were no conflicts of interest regarding this study.
References
1. Obermann K, Jowett M, Kwon S. The role of national health insurance for achieving UHC in the Philippines: a mixed methods analysis. Glob Health Action. 2018;11(1):1483638. doi:10.1080/16549716.2018.1483638
2. Fusheini A, Eyles J. Achieving universal health coverage in South Africa through a district health system approach: conflicting ideologies of health care provision. BMC Health Serv Res. 2016;16:558.
3. Cuadrado C, Crispi F, Libuy M, Marchildon G, Cid C. National Health Insurance: a conceptual framework from conflicting typologies. Health Policy (New York). 2019;123(7):621–629. doi:10.1016/j.healthpol.2019.05.013
4. Carapinha JL, Ross-degnan D, Tamer A, Wagner AK. Health insurance systems in five sub-Saharan African countries: medicine benefits and data for decision making. Health Policy (New York). 2011;99:193–202. doi:10.1016/j.healthpol.2010.11.009
5. Demissie B, Gutema Negeri K. Effect of community-based health insurance on utilization of outpatient health care services in Southern Ethiopia: a comparative cross-sectional study. Risk Manag Healthc Policy. 2020;13:141–153. doi:10.2147/RMHP.S215836
6. Basaza R. What are the emerging features of community health insurance schemes in east Africa? Risk Manag Healthc Policy. 2009;2:47. doi:10.2147/RMHP.S4347
7. Wang H, Otoo N, Dsane-Selby L. Ghana National Health Insurance Scheme: ImprovingFinancial Sustainability Based on Expenditure Review. Washington: World Bank Group; 2017.
8. Nguyen HTH, Rajkotia Y, Wang H. The financial protection effect of Ghana National Health Insurance Scheme: evidence from a study in two rural districts. Int J Equity Health. 2011;10:1–12. doi:10.1186/1475-9276-10-4
9. Badu E, Agyei-Baffour P, Ofori Acheampong I, Preprah Opoku M, Addai-Donkor K. Households sociodemographic profile as predictors of health insurance uptake and service utilization: a cross-sectional study in a municipality of Ghana. Adv Public Health. 2018;2018:1–13. doi:10.1155/2018/7814206
10. Jehu-Appiah C, Aryeetey G, Agyepong I, Spaan E, Baltussen R. Household perceptions and their implications for enrolment in the National Health Insurance Scheme in Ghana. Health Policy Plan. 2012;27:222–233. doi:10.1093/heapol/czr032
11. Duku SKO, Nketiah-amponsah E, Janssens W, et al. Perceptions of healthcare quality in Ghana: does health insurance status matter? PLoS One. 2018;13:1–18. doi:10.1371/journal.pone.0190911
12. Sithole HL. An overview of the National Health Insurance and its possible impact on eye healthcare services in South Africa. African Vis Eye Health. 2015;74:1–6.
13. Booysen F, Hongoro C. Perceptions of and support for national health insurance in South Africa’s public and private healthcare sectors. Pan Afr Med J. 2018;8688:1–9.
14. Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. doi:10.1186/1748-5908-5-69
15. Christmals CD, Armstrong SJ. The essence, opportunities and threats to advanced practice nursing in Sub-Saharan Africa: a scoping review. Heliyon. 2019;5(10):e02531. doi:10.1016/j.heliyon.2019.e02531
16. Mendeley. Free Reference Manager & Citation Generator - Mendeley. Elsevier; 2018:1.
17. Christmals CD, Gross J, Aziato L, Armstrong SJ. The state of nursing research in Ghana: an integrative literature review. SAGE Open Nurs. 2018;4:237796081878382. doi:10.1177/2377960818783820
18. Sandelowski M, Voils CI, Leeman J, Crandell JL. Mapping the mixed methods – mixed research synthesis Terrain. J Mix Methods Res. 2012;6:317–331. doi:10.1177/1558689811427913
19. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277–1288. doi:10.1177/1049732305276687
20. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467. doi:10.7326/M18-0850
21. Abiiro GA, McIntyre D. Universal financial protection through National Health Insurance: a stakeholder analysis of the proposed one-time premium payment policy in Ghana. Health Policy Plan. 2013;28:263–278. doi:10.1093/heapol/czs059
22. Aryeetey GC, Jehu-Appiah C, Kotoh AM, et al. Community concepts of poverty: an application to premium exemptions in Ghana’s National Health Insurance Scheme. Global Health. 2013;9:1–11. doi:10.1186/1744-8603-9-12
23. Agyei-Baffour P, Oppong R, Boateng D. Knowledge, perceptions and expectations of capitation payment system in a health insurance setting: a repeated survey of clients and health providers in Kumasi, Ghana. BMC Public Health. 2013;13:1–9. doi:10.1186/1471-2458-13-1220
24. Ashigbie PG, Azameti D, Wirtz VJ. Challenges of medicines management in the public and private sector under Ghana’s National Health Insurance Scheme - a qualitative study. J Pharm Policy Pract. 2016;9:1–10. doi:10.1186/s40545-016-0055-9
25. Barimah KB, Mensah J. Ghana’s national health insurance scheme: insights from members, administrators and health care providers. J Health Care Poor Underserved. 2013;24:1378–1390. doi:10.1353/hpu.2013.0144
26. Dalaba MA, Aborigo R, Akweongo P, et al. Does the National Health Insurance Scheme in Ghana reduce household cost of treating malaria in the Kassena-Nankana districts? Glob Health Action. 2014;7:7. doi:10.3402/gha.v7.23848
27. Fosu R, Opoku-asante K, Adu-Gyamfi K. Influence of community financing health insurance schemes on in-patient care in Ghana: the case of Nkoranza scheme. Dev Country Stud. 2014;4:53–64.
28. Hampshire KR, Porter G, Asiedu S, Tanle A, Abane A. Social science & medicine out of the reach of children? Young people ’ s health-seeking practices and agency in Africa’ s newly-emerging therapeutic landscapes. Soc Sci Med. 2011;73:702–710. doi:10.1016/j.socscimed.2011.06.035
29. Frimpong JA, Helleringer S, Awoonor-Williams JK, Aguilar T, Phillips JF, Yeji F. The complex association of health insurance and maternal health services in the context of a premium exemption for pregnant women: A case study in Northern Ghana. Health Policy Plan. 2014;29:1043–1053. doi:10.1093/heapol/czt086
30. Asundep NN, Carson AP, Archer C, et al. Determinants of access to antenatal care and birth outcomes in Kumasi, Ghana. J Epidemiol Glob Health. 2013;3(4):279–288.
31. Dalinjong PA, Welaga P, Akazili J, et al. The association between health insurance status and utilization of health services in rural Northern Ghana: evidence from the introduction of the National Health Insurance Scheme. J Health Popul Nutr. 2017;36:1–11.
32. Fenny AP, Enemark U, Asante FA, Hansen KS. Patient satisfaction with primary health care – a comparison between the insured and non-insured under the national health insurance policy in Ghana. Glob J Health Sci. 2014;6:9–21. doi:10.5539/gjhs.v6n4p9
33. Osei Asibey B, Agyemang S. Analysing the influence of health insurance status on peoples’ health seeking behaviour in Rural Ghana. J Trop Med. 2017;2017:7. doi:10.1155/2017/8486451
34. Adei D, Kwadwo VO, Diko SK. An assessment of the Kwabre district mutual health insurance scheme in Ghana. Curr Res J Soc Sci. 2012;4:372–382.
35. Boateng D, Awunyor-Vitor D. Health insurance in Ghana: evaluation of policy holders’ perceptions and factors influencing policy renewal in the Volta region. Int J Equity Health. 2013;12:1. doi:10.1186/1475-9276-12-50
36. Boateng S, Amoako P, Poku AA, Baabereyir A, Gyasi RM. Migrant female head porters ’ enrolment in and utilisation and renewal of the National Health Insurance Scheme in Kumasi, Ghana. J Public Health (Bangkok). 2017;25:625–634. doi:10.1007/s10389-017-0832-1
37. Akazili J, Ataguba JEO, Kanmiki EW, et al. Assessing the impoverishment effects of out-of-pocket healthcare payments prior to the uptake of the national health insurance scheme in Ghana. BMC Int Health Hum Rights. 2017;17:1–9. doi:10.1186/s12914-017-0121-7
38. Addae-Korankye A. Challenges of financing health care in Ghana: the case of National Health Insurance Scheme (NHIS). Int J Asian Soc Sci. 2013;3:511–522.
39. Dalinjong PA, Wang AY, Homer CSE. Has the free maternal health policy eliminated out of pocket payments for maternal health services? Views of women, health providers and insurance managers in Northern Ghana. PLoS One. 2018;13:1–20. doi:10.1371/journal.pone.0184830
40. Mensah J, Oppong JR, Schmidt CM. Ghana’s National Health Insurance Scheme in the context of the health MDGs: an empirical evaluation using propensity score matching. Health Econ. 2010;19:95–106. doi:10.1002/hec.1633
41. Jehu-Appiah C, Aryeetey G, Spaan E, et al. Equity aspects of the National Health Insurance Scheme in Ghana: who is enrolling, who is not and why? Soc Sci Med. 2011;72:157–165. doi:10.1016/j.socscimed.2010.10.025
42. Aryeetey GC, Nonvignon J, Amissah C, Buckle G, Aikins M. Migrating from user fees to social health insurance: exploring the prospects and challenges for hospital management. BMC Health Serv Res. 2016;12:1–9.
43. Sodzi-Tettey S, Aikins M, Awoonor-Williams J, Agyepong IA. Challenges in provider payment under the Ghana Na- Tional health insurance scheme: a case study of claims. Ghana Med J. 2012;46:189–200.
44. Witter S, Garshong B. Something old or something new? Social health insurance in Ghana. BMC Int Health Hum Rights. 2009;9:1–13. doi:10.1186/1472-698X-9-20
45. Nsiah-boateng E, Aikins M. Performance assessment of ga district mutual health insurance scheme, greater accra region, Ghana. Value Health Reg Issues. 2013;2:300–305. doi:10.1016/j.vhri.2013.06.005
46. Yevutsey SK, Aikins M. Financial viability of district mutual health insurance schemes of lawra and sissala East districts, upper west region, ghana. Ghana Med J. 2010;44:130–137. doi:10.4314/gmj.v44i4.68905
47. Odame EA, Akweongo P, Yankah B, Asenso-boadi F, Agyepong I. Sustainability of recurrent expenditure on public social welfare programmes: expenditure analysis of the free maternal care programme of the Ghana National Health Insurance Scheme. Health Policy Plan. 2014;29:271–279. doi:10.1093/heapol/czt013
48. Agyepong IA, Nana D, Abankwah Y, et al. Policy and implementation challenges and dilemmas of a lower middle income country. Natl Health Insur Scheme. 2016;16:1–14.
49. Duku SKO, Asenso-boadi F, Nketiah-amponsah E, Arhinful DK. Utilization of healthcare services and renewal of health insurance membership: evidence of adverse selection in Ghana. Health Econ Rev. 2016;6:1–12. doi:10.1186/s13561-016-0122-6
50. Awoonor-Williams JK, Tindana P, Dalinjong PA, Nartey H, Akazili J. Does the operations of the National Health Insurance Scheme (NHIS) in Ghana align with the goals of Primary Health Care? Perspectives of key stakeholders in northern Ghana. BMC Int Health Hum Rights. 2016;16:1–12. doi:10.1186/s12914-016-0096-9
51. Alhassan RK, Nketiah-amponsah E, Spieker N, Arhinful DK, De Wit TFR. Perspectives of frontline health workers on Ghana’ s National Health Insurance Scheme before and after community engagement interventions. BMC Health Serv Res. 2016;16:1–11. doi:10.1186/s12913-016-1438-y
52. Nsiah-boateng E, Aikins M, Asenso-boadi F. Value and service quality assessment of the national health insurance scheme in Ghana: evidence from Ashiedu Keteke District. Value Health Reg Issues. 2016;10C:7–13. doi:10.1016/j.vhri.2016.03.003
53. Witter S, Arhinful DK, Kusi A, Zakariah S. The experience of Ghana in implementing a user fee exemption policy to provide free delivery care. Reprod Health Matters. 2007;15:61–71. doi:10.1016/S0968-8080(07)30325-X
54. Fusheini A. The politico-economic challenges of Ghana’s National Health Insurance Scheme Implementation. Int J Health Policy Manag. 2016;5:543–552. doi:10.15171/ijhpm.2016.47
55. Alhassan RK, Nketiah-Amponsah E, Akazili J, Spieker N, Arhinful DK, Rinke de Wit TF. Efficiency of private and public primary health facilities accredited by the National Health Insurance Authority in Ghana. Cost Eff Resour Alloc. 2015;13:1–14. doi:10.1186/s12962-015-0050-z
56. Alhassan F, Moses K, Kukurah J-D, Sakara A. Service quality in national health insurance scheme healthcare: a case study of WA municipal national health insurance scheme in the upper west region of Ghana. Dev Country Stud. 2014;4:108–123.
57. Yawson AE, Biritwum RB, Nimo PK. Effects of consumer and provider moral hazard at a municipal hospital out-patient department on Ghana’s National Health Insurance Scheme. Ghana Med J. 2012;46:200–210.
58. Dalinjong PA, Laar AS. The national health insurance scheme: perceptions and experiences of health care providers and clients in two districts of Ghana. Health Econ Rev. 2012;2:1.
59. Dixon J, Tenkorang EY, Luginaah I. Ghana’s National Health Insurance Scheme: a national level investigation of members’ perceptions of service provision. BMC Int Health Hum Rights. 2013;13:1–10. doi:10.1186/1472-698X-13-35
60. Asundep NN, Carson AP, Archer C, et al. Determinants of access to antenatal care and birth outcomes in Kumasi, Ghana. J Epidemiol Glob Health. 2013;3:279–288. doi:10.1016/j.jegh.2013.09.004
61. Piersson AD, Gorleku PN. Radiography assessment of availability, accessibility, and affordability of magnetic resonance imaging services in Ghana. Radiography. 2017;23:e75–9. doi:10.1016/j.radi.2017.06.002
62. Ayimbillah Atinga R. Healthcare quality under the National Health Insurance Scheme in Ghana: perspectives from premium holders. Int J Qual Reliab Manag. 2012;29:144–161. doi:10.1108/02656711211199883
63. Lamptey AA, Nsiah-boateng E, Agyemang SA, Aikins M. National health insurance accreditation pattern among private healthcare providers in Ghana. Arch Public Health. 2017;75:1–7.
64. Agyemang KK, Adu-Gyamfi AB, Afrakoma M. Prospects and challenges of implementing a sustainable national health insurance scheme: the case of the Cape Coast Metropolis, Ghana. Dev Country Stud. 2013;3:140–149.
65. Andoh-Adjei FX, Van Der Wal R, Nsiah-Boateng E, Asante FA, Van Der Velden K, Spaan E. Does a provider payment method affect membership retention in a health insurance scheme? A mixed method study of Ghana’s capitation payment for primary care. BMC Health Serv Res. 2018;18:1–12. doi:10.1186/s12913-018-2859-6
66. Gyasi RM. Relationship between health insurance status and the pattern of traditional medicine utilisation in Ghana. Evidence-Based Complement Altern Med. 2015;2015:1–10. doi:10.1155/2015/717926
67. Andoh-Adjei FX, Cornelissen D, Asante FA, Spaan E, Van Der Velden K. Does capitation payment under national health insurance affect subscribers’ trust in their primary care provider? A cross-sectional survey of insurance subscribers in Ghana. BMC Health Serv Res. 2016;16:1–11. doi:10.1186/s12913-016-1622-0
68. Ibrahim A, O’Keefe A. Do infant birth outcomes vary among mothers with and without health insurance coverage in Sub-Saharan Africa? Findings from the National Health Insurance and Cash and Carry Eras in Ghana, West Africa. Int J Matern Child Health AIDS. 2014;2:200–208.
69. Ibrahim A, Maya ET, Donkor E, Agyepong IA, Adanu RM. Perinatal mortality among infants born during health user-fees (Cash & Carry) and the national health insurance scheme (NHIS) eras in Ghana: a cross-sectional study. BMC Pregnancy Childbirth. 2016;16:1–8. doi:10.1186/s12884-016-1179-2
70. Lambon-Quayefio M, Owoo NS. Determinants and the impact of the National Health Insurance on neonatal mortality in Ghana. Health Econ Rev. 2017;7:1–16. doi:10.1186/s13561-017-0169-z
71. Strupat C, Klohn F. Crowding out of solidarity? Public health insurance versus informal transfer networks in Ghana. World Dev. 2018;104:212–221. doi:10.1016/j.worlddev.2017.11.004
72. Aryeetey GC, Westeneng J, Spaan E, Jehu-Appiah C, Agyepong IA, Baltussen R. Can health insurance protect against out-of-pocket and catastrophic expenditures and also support poverty reduction? Evidence from Ghana’s National Health Insurance Scheme. Int J Equity Health. 2016;15:11. doi:10.1186/s12939-016-0401-1
73. Sekyi S, Domanban PB. The effects of health insurance on outpatient utilization and healthcare expenditure in Ghana. (Special Issue: arts and social science.). Int J Humanit Soc Sci. 2012;2:40–49.
74. Aboagye DC, South J, Khan HT. Evaluation of community perspectives on national health insurance policy to health service service delivery in Ghana. Illness Cris Loss. 2017:1–16.
75. Mills A, Ataguba JE, Akazili J, et al. Equity in fi nancing and use of health care in Ghana, South Africa, and Tanzania: implications for paths to universal coverage. Lancet. 2012;380:126–133. doi:10.1016/S0140-6736(12)60357-2
76. Debpuur C, Dalaba MA, Chatio S, Adjuik M, Akweongo P. An exploration of moral hazard behaviors under the national health insurance scheme in Northern Ghana: a qualitative study. BMC Health Serv Res. 2015;15(1):1–9. doi:10.1186/s12913-015-1133-4
77. Brinkerhoff DW, Bossert TJ. Health governance: principal-agent linkages and health system strengthening. Health Policy Plan. 2014;29:685–693. doi:10.1093/heapol/czs132
78. Agyepong IA, Adjei S. Public social policy development and implementation: a case study of the Ghana National Health Insurance scheme. Health Policy Plan. 2008;23:150–160. doi:10.1093/heapol/czn002
79. Fusheini A, Marnoch G, Gray AM, et al. Implementation Challenges of the National Health Insurance Scheme in Selected Districts in Ghana: evidence from the Field Implementation Challenges of the National Health Insurance Scheme in Selected Districts in Ghana: evidence from the Field. Int J Public Adm. 2017;40:416–426.
80. Fenny AP, Kusi A, Arhinful DK, Asante FA. Factors contributing to low uptake and renewal of health insurance: a qualitative study in Ghana. Glob Heal Res Policy. 2016;1:1–10.
81. Effah P, Appiah KO, Abor PA. Performance assessment of the Juaboso District Office of the National Health Insurance Authority. Value Health Reg Issues. 2016;10c:29–35. doi:10.1016/j.vhri.2016.06.002
82. Bandyopadhyay S, Kanji S, Wang L. The impact of rainfall and temperature variation on diarrheal prevalence in Sub-Saharan Africa. Appl Geogr. 2012;33:63–72. doi:10.1016/j.apgeog.2011.07.017
83. Adomah-afari A, Chandler JA. Social science & medicine the role of government and community in the scaling up and sustainability of mutual health organisations: an exploratory study in Ghana. Soc Sci Med. 2018;207:25–37. doi:10.1016/j.socscimed.2018.04.044
84. Agyepong AI, Nagai RA. We charge them; otherwise we cannot run the hospital ” front line workers, clients and health financing policy implementation gaps in Ghana. Health Policy (New York). 2011;99:226–233. doi:10.1016/j.healthpol.2010.09.018
85. Wedam EA, Sanyare FN. Health care financing and sustainability: A study of current conceptual dialectics in Ghana. World Dev Perspect. 2017;5:47–55. doi:10.1016/j.wdp.2017.03.003
86. Seddoh A, Akor SA. Policy initiation and political levers in health policy: lessons from Ghanas health insurance. BMC Public Health. 2012;12:1–11. doi:10.1186/1471-2458-12-S1-S10
87. National Health Insurance Authority. Holistic Assessment of 2017 Health Sector Programme of Work. Accra; 2018. Available from: https://www.moh.gov.gh/wp-content/uploads/2018/09/2017-Holistic-Assessment-Report_Final_09.08.2018.pdf.
88. Darko T How does government responsiveness come about? The politics of accountability in Ghana’s National Health Insurance Scheme. Brighton; 2016. Available from: https://www.researchgate.net/publication/319356476_How_does_government_responsiveness_come_about_The_politics_of_accountability_in_Ghana’s_National_Health_Insurance_Scheme.
89. Ataguba JE, McIntyre D. The incidence of health financing in South Africa: findings from a recent data set. Health Econ Policy Law. 2017:1–24.
90. Gwarube S. Urgent Clarity Needed from Treasury Regarding NHI Funding. Politicsweb; 2019:1.
91. Hofman KJ, McGee S, Chalkidou K, Tantivess S, Culyer AJ. National health insurance in South Africa: relevance of a national priority-setting agency. South Afr Med J. 2015;105:739–740. doi:10.7196/SAMJnew.8584
92. Fin24. Mediclinic Says More Clarity Needed on NHI Bill; 2019:1.
93. Phillip X. South Africa’s NHI Bill: Clarity Needed, and a Long Road Ahead | The Africa Report.com; 2019:1.
94. Mkhwanazi S. Mkhize Says Team to Fight Corruption in NHI | IOL News; 2019:1.
95. Rispel LC, de Jager P, Fonn S. Exploring corruption in the South African health sector. Health Policy Plan. 2016;31:239–249. doi:10.1093/heapol/czv047
96. Mametja S NHI BILL background: historical phases of healthcare financing dialogue in SA. In:
97. Mabuza LH, Ogunbanjo GA, Hlabyago KE, Mogotsi M. Awareness of health care practitioners about the National Health Insurance in Tshwane District, South Africa Abstract. Open Public Health J. 2018;11:93–103. doi:10.2174/1874944501811010093
98. Amado L, Christofides N, Pieters R, Rusch J. National Health Insurance: a lofty ideal in need of cautious, planned implementation Introduction to the winning entry of the 2012 University of the Witwatersrand ’ s Medical Protection Society Bioethics Competition. South Afr J Bioeth Law. 2012;5:1–15.
99. Oladimeji O, Alabi A, Adeniyi OV. Awareness, Knowledge and Perception of The National Health Insurance Scheme (NHIS) Among Health Professionals in Mthatha General Hospital, Eastern Cape, South Africa. Open Public Health J. 2017;10:187–194. doi:10.2174/1874944501710010187
100. Motsepe A, Radiography B, Radiography P, Wolvaardt JE, Webb EM. Rapid assessment of two primary health clinics: are we ready for National Health Insurance? South Afr J Public Health Incorp Strength Health Syst. 2020;4(1):22–26. doi:10.7196/SHS.2020.v4.i1.109
101. Tandwa L, Dhai A Public engagement in the development of the National Health Insurance: a study involving patients from a central hospital in South Africa; 2020. Available from: https://europepmc.org/article/ppr/ppr135484.
102. Tandwa L, Dhai A (NHI): knowledge, awareness and participation of patients from the Internal Medicine Department at Charlotte Maxeke Johannesburg Academic Hospital in the NHI …. 2019. Available from: https://europepmc.org/article/ppr/ppr148266.
103. Molokomme VK, Seekoe E, Goon DT. The Perception of Professional Nurses About the Introduction of the National Health Insurance (NHI) in a Private Hospital in Gauteng, South Africa. Open Public Health J. 2018;11:234–242. doi:10.2174/1874944501811010234
104. South African Lancet National Commission. Confronting the right to ethical and accountable quality healthcare in South Africa. Pretoria; 2019. Available from: http://rhap.org.za/wp-content/uploads/2019/01/SA-Lancet-Report-Synopsis-South-Africa_Confronting-the-Right-to-Ethical-Accountable-Healthcare.pdf.
105. Stellenberg E. Nursing failures fuel claims against private hospitals — stellenbosch study - Medical Brief. Med Br. 2018;1.
106. Kruk ME, Gage AD, Arsenault C, et al. The lancet global health commission high-quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob Health. 2018;6:1196–1252. doi:10.1016/S2214-109X(18)30386-3
107. WHO, OECD, World bank. Delivering quality health services: a global imperative for universal health coverage; 2018. Available from: http://documents.worldbank.org/curated/en/482771530290792652/pdf/127816-REVISED-quality-joint-publication-July2018-Complete-vignettes-ebook-L.pdf.
108. National Academies of Sciences Engineering and Medicine. Crossing the Global Quality Chasm: Improving Health Care Worldwide. Washington, DC: The National Academies Press; 2018. doi:10.17226/25152
109. South African Medical Device Industry Association. SAMED Commentary on the National Health Insurance Draft Policy Paper. 2011.
110. Alhassan RK, Duku SO, Janssens W, et al. Comparison of perceived and technical healthcare quality in primary health facilities: implications for a sustainable National Health Insurance Scheme in Ghana. PLoS One. 2015;10(10):1–20. doi:10.1371/journal.pone.0140109
111. Rifkin SB. Examining the links between community participation and health outcomes: a review of the literature. Health Policy Plan. 2014;29:ii98–106. doi:10.1093/heapol/czu076
112. Barker M, Klopper H. Community participation in primary health care projects of the Muldersdrift health and development programme. Curationis. 2007;30(2):36–47. doi:10.4102/curationis.v30i2.1070
113. Haldane V, Chuah FLH, Srivastava A, et al. Community participation in health services development, implementation, and evaluation: A systematic review of empowerment, health, community, and process outcomes. PLoS One. 2019;14:e0216112. doi:10.1371/journal.pone.0216112
114. Meier BM, Pardue C, London L. Implementing community participation through legislative reform: a study of the policy framework for community participation in the Western Cape province of South Africa. BMC Int Health Hum Rights. 2012;12:15. doi:10.1186/1472-698X-12-15
115. Rispel LC, Blaauw D, Ditlopo P, White J. Human resources for health and universal health coverage: progress, complexities and contestations. South Afr Health Rev. 2018;1:13–22.
116. von Fintel D, Richter L. Intergenerational transfer of health inequalities: exploration of mechanisms in the Birth to Twenty cohort in South Africa. BMJ Glob Health. 2019;4(5):e001828. doi:10.1136/bmjgh-2019-001828
117. McLaren ZM, Ardington C, Leibbrandt M. Distance decay and persistent health care disparities in South Africa. BMC Health Serv Res. 2014;14:1–9. doi:10.1186/s12913-014-0541-1
118. National Health Insurance Authority. National Health Insurance Authority Annual Report. Accra; 2009.
119. National Health Insurance Authority. National Health Insurance Authority 2013 Annual Report; 2009.
120. Nsiah-Boateng E, Aikins M. Trends and characteristics of enrolment in the National Health Insurance Scheme in Ghana: a quantitative analysis of longitudinal data. Glob Heal Res Policy. 2018;3:1–10.
121. Wireko I, Béland D. Transnational actors and health care reform: why international organizations initially opposed, and later supported, social health insurance in Ghana. Int J Soc Welf. 2017;26:405–415. doi:10.1111/ijsw.12257
122. Abrokwah SO, Callison K, Meyer DJ, Abrokwah SO, Callison K, Meyer DJ. Social health insurance and the use of formal and informal care in developing countries: evidence from Ghana’ s National Health Insurance Scheme. J Dev Stud. 2017;1–15.
123. Abrokwah SO, Moser CM, Norton EC. The effect of social health insurance on prenatal care: the case of Ghana. Int J Heal Care Financ. 2014;14:385–406. doi:10.1007/s10754-014-9155-8
124. Abuosi AA, Domfeh KA, Abor JY, Nketiah-Amponsah E. Health insurance and quality of care: comparing perceptions of quality between insured and uninsured patients in Ghana’s hospitals. Int J Equity Health. 2016;15:1–12. doi:10.1186/s12939-016-0365-1
125. Apanga S, Chirawurah D, Kudiabor C, Adda J, Adoesom JA. Cost implication of irrational drug prescription under the national health insurance scheme in rural Ghana. Value Health. 2014;17:A19. doi:10.1016/j.jval.2014.03.122
126. Goudge J, Akazili J, Ataguba J, et al. Social solidarity and willingness to tolerate risk- and income-related cross-subsidies within health insurance: experiences from Ghana, Tanzania and South Africa. Health Policy Plan. 2012;27:i55–63. doi:10.1093/heapol/czs008
127. Nsiah-Boateng E, Asenso-Boadi F, Dsane-Selby L, et al. Reducing medical claims cost to Ghana’s National Health Insurance scheme: a cross-sectional comparative assessment of the paper- and electronic-based claims reviews. BMC Health Serv Res. 2017;17:1–7. doi:10.1186/s12913-017-2054-1
128. Sackey FG, Amponsah PN. Willingness to accept capitation payment system under the Ghana National Health Insurance Policy: do income levels matter? Health Econ Rev. 2017;7:1–13. doi:10.1186/s13561-017-0175-1
129. Yilma Z, Van Kempen L, De Hoop T. A perverse ‘net’ effect? Health insurance and ex-ante moral hazard in Ghana. Soc Sci Med. 2012;75:138–147. doi:10.1016/j.socscimed.2012.02.035
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.