")
Back to Journals » Clinical Ophthalmology » Volume 9
Implementation of a vision-screening program in rural northeastern United States
Authors Tsui E, Siedlecki A, Deng J, Pollard M, Cha S, Pepin S, Salcone E
Received 26 June 2015
Accepted for publication 6 August 2015
Published 7 October 2015 Volume 2015:9 Pages 1883—1887
DOI https://doi.org/10.2147/OPTH.S90321
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Edmund Tsui,1,2 Andrew N Siedlecki,3 Jie Deng,3 Margaret C Pollard,3 Sandolsam Cha,3 Susan M Pepin,4 Erin M Salcone4
1Department of Surgery, Dartmouth–Hitchcock Medical Center, Lebanon, NH, 2Department of Ophthalmology, New York University School of Medicine, New York, NY, 3Geisel School of Medicine at Dartmouth, Hanover, NH, 4Section of Ophthalmology, Dartmouth–Hitchcock Medical Center, Lebanon, NH, USA
Background: Rural populations comprise almost 20% of the US population and face unique barriers in receiving health care. We describe the implementation of a medical student-run free vision-screening clinic as a strategy to overcome barriers in accessing eye care in New Hampshire and Vermont.
Methods: Medical students were trained by an ophthalmologist to administer screening eye examinations. Patients from New Hampshire and Vermont were enrolled through a free community clinic. Screening included a questionnaire, distance and near visual acuity, extraocular movements, confrontational visual fields, and Amsler grid. Patients who met predetermined screening criteria were referred to an ophthalmologist or optometrist for further evaluation. Data including patient demographics, appointment attendance, level of education, and diagnoses were recorded and analyzed.
Results: Of 103 patients (mean age of 45.5±12.3 years, 63% female), 74/103 (72%) were referred for further evaluation, and 66/74 (89%) attended their referral appointments. Abnormal ophthalmologic examination findings were observed in 58/66 (88%) patients who attended their referral appointment. Uncorrected refractive error was the most common primary diagnosis in 38% of referred patients. Other diagnoses included glaucoma suspect (21%), retinal diseases (8%), amblyopia (8%), cataract (6%), others (6%), and normal examination (12%). Of the 8/74 (11%) referred patients who did not attend their appointments, reasons included patient cancellation of appointment, work conflicts, or forgetfulness. Patients traveled a mean distance of 16.6 miles (range: 0–50 miles) to attend screening examinations. Mean time for patients’ last effort to seek eye care was 7.1 years (range: 1–54 years).
Conclusion: This study underscores the high prevalence of unmet eye care needs in a rural population. Furthermore, it demonstrates that using community health centers as a patient base for screening can yield a high referral attendance rate for this at-risk population and facilitate entrance into the eye care system in a rural setting.
Keywords: vision screening, rural health, uninsured
Introduction
Blindness defined as best-corrected visual acuity of ≤20/200 in the better-seeing eye, or low vision defined as best-corrected visual acuity of <20/40 in the better-seeing eye, affects approximately 3% of adult American population over 40 years of age and is a determinant in overall physical impairment.1 It has far-reaching consequences that contribute to a major economic burden totaling 139 billion dollars annually.2 The majority of visual impairment in the USA is attributed to eye diseases for which treatment or prevention already exist.1 Although the utility of vision screening for the general public remains inconclusive, vision screening has been proved to be effective in at-risk patients, such as diabetic and pediatric populations.3,4
Rural populations comprise almost 20% of the US population5 and face unique barriers in receiving health care. Barriers include long travel distance, limited provider availability, and lower incomes compared to those of urban populations.6,7 Being compounded with poor rankings on health indicators, rural communities face heightened challenges in achieving good health.8,9 Furthermore, studies have demonstrated that individuals in rural areas have significantly less insurance coverage for eye care, decreased access to eye care, and low utilization of eye care services.6,7 According to the US 2010 Census, Vermont (VT) and New Hampshire (NH) have the second (61.1%) and eleventh (39.7%) highest proportion of residents in rural areas, respectively.5 The utility of vision screening has been evaluated in underserved populations in urban settings,10–12 but to the best of our knowledge there are no investigations detailing general adult vision screening in underserved and uninsured rural communities in the USA. We hypothesize that there is a high prevalence of unmet eye care needs among the northeastern rural population and that a free vision-screening clinic for these patients can address these gaps in vision health.
Methods
This study was approved by the Committee for the Protection of Human Subjects at Dartmouth College. Vision screening entailed monthly sessions at the Good Neighbor Health Clinic (White River Junction, VT, USA), a free clinic providing primary medical and dental care to uninsured and underinsured VT and NH residents whose household incomes are <250% of the federal poverty level. Screening was performed by volunteer 2nd-year Dartmouth medical students from October 2011 to February 2014. In addition to standard physical examination instruction in the preclinical medical curriculum, volunteer students received 3-hour didactic training by a board-certified ophthalmologist to discuss in further detail and practice the following evaluations: distance visual acuity using a 10 ft Snellen chart, near visual acuity using a 14-inch acuity card, extraocular motility testing, confrontation visual fields, and Amsler grid with each eye tested separately. This was followed by observation, evaluation, and critique by a board-certified ophthalmologist in the practical administration of learned skills. The previously mentioned examination approaches were utilized to screen patients. Our sample consisted of patients of the Good Neighbor Health Clinic, and patients were recruited via flyers distributed at the clinic and word of mouth from clinic providers. Written consent was obtained at the screening visit. Patients were asked questions (Table 1) adapted from previously published questionnaires.10,11 Basic demographics and time since last eye examination were recorded. Average distance traveled to clinic was calculated using patients’ home zip code and the screening clinic zip code.
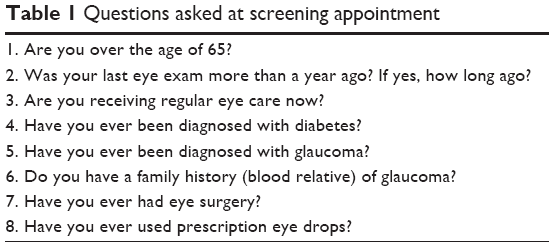 | Table 1 Questions asked at screening appointment |
Similar to previous studies,10,11 patients were referred for further assessment if any one of the following criteria was met: 1) two or more positive answers on the questionnaire; 2) <20/30 distance acuity despite pinhole, or <20/40 near acuity; 3) any distortions, blind spots, or irregularities with Amsler grid testing; 4) any abnormality of extraocular movements in the cardinal positions of gaze; and 5) any visual field defect on confrontation visual field testing. Following scheduling of a referral appointment to a local volunteer eye care provider, patients received a letter and a phone call reminder 1 week prior to their appointments. Vouchers were provided by the community clinic for up to $50 for eyeglasses if patients were diagnosed with refractive error. Initial ophthalmologic assessment was managed through local volunteer optometrists or ophthalmologists, and all initial assessments were documented and analyzed. Patients who did not attend their referral appointments were contacted via telephone to document the reason for missed appointment. Patients who required further ophthalmologic evaluation after initial evaluation by an eye care provider were referred to the Dartmouth–Hitchcock Medical Center and received assistance on entering the Dartmouth-Hitchcock Medical Center health care network.
Results
A total of 103 patients were screened and patient demographic data are presented in Table 2. Median age of participants was 48 years (range: 17–67 years). Of all patients, 74/103 (72%) were referred for further evaluation, and 66/74 (89%) attended their referral appointments. Abnormal ophthalmologic examination findings were observed in 58/66 (88%) patients who attended their initial referral appointment. The most common ophthalmic abnormalities found on examination included refractive error, glaucoma suspicion, retinal diseases (consisting of choroidal nevus, early age-related macular degeneration, history of retinal tear, and history of retinal scar [two patients]), amblyopia, and cataract (Table 3). Nine patients had a documented history of diabetes, but with no evidence of retinopathy. Three of 58 patients required referral to the Dartmouth–Hitchcock Medical Center for further assessment of the following: neurology evaluation for nyctalopia, cataract surgery evaluation, and glaucoma management. A total of 8/74 (11%) referred patients did not attend their appointments. The most common reason given for not attending the scheduled appointment was conflicting engagements in 3/8 (38%) patients. Other reasons included forgotten appointment and illness (Table 3). Patients traveled an average of 16.6 miles (range: 0–50 miles) to attend screening examinations. Average time for patients’ last effort to seek eye care was 7.1 years (range: 1–54 years). In our sample, 81/103 (78.6%) resided in NH and 22/103 (21.4%) resided in VT.
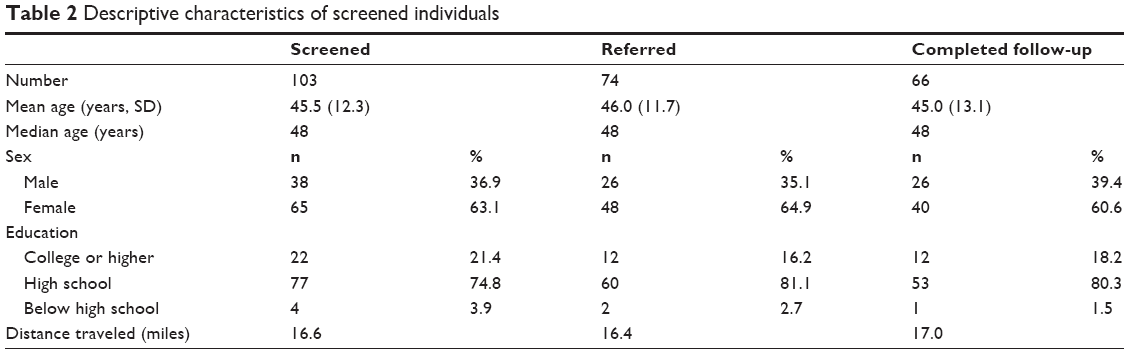 | Table 2 Descriptive characteristics of screened individuals |
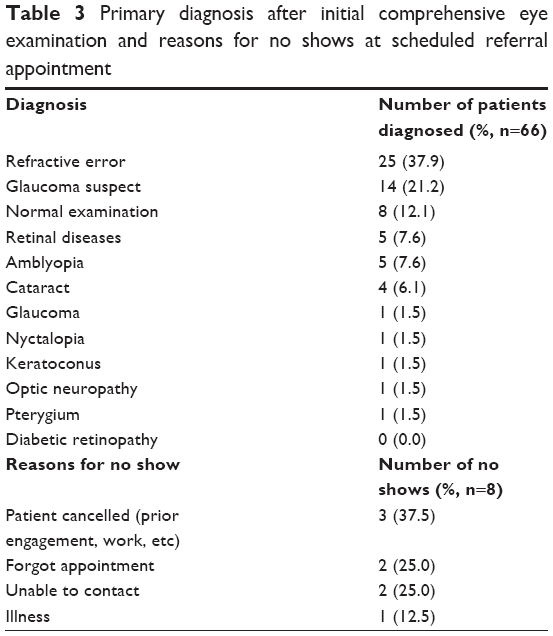 | Table 3 Primary diagnosis after initial comprehensive eye examination and reasons for no shows at scheduled referral appointment |
Discussion
Disparity of health care delivery continues to be a prevalent issue in the USA and vision health is not an exception. Connecting vision care to patients who need it the most remains a priority in reducing the morbidity and economic burden associated with low vision. By screening established patients at the Good Neighbor Health Clinic, a free clinic serving NH and VT residents, our initiative aimed to identify at-need patients and connect them with the appropriate care. Here, we presented data describing the implementation of a vision-screening clinic for the uninsured and underserved population in rural NH and VT.
Almost three-quarters of screened patients required follow-up care, demonstrating the prevalence of unmet eye care in this population. This referral rate is comparable to that of other screening initiatives with similar referral criteria.11 Notably, our referral appointment attendance rate of 89% was dramatically higher than that of other reported initiatives, including 41% in a Baltimore screening program,10 39% in a Rhode Island screening program,11 and 47% estimated in an Ohio screening program.12
In the present study, uncorrected refractive error was the most common primary diagnosis in 37.8% of referred patients. This is consistent with other studies demonstrating that the uncorrected refractive error accounted for the largest proportion of visual impairment.10,12 Importantly, a study of medical claims in the USA showed that refractive error was the largest contributor of direct medical costs in the middle-aged population.13 Moreover, those who require visual aid the most may be least likely to be able to afford the costs.6,7 Therefore, the present study underscores not only the importance of a cost-effective, efficient vision-screening program for high-risk individuals, but also the critical need for initiatives that will help bridge barriers and financial gaps to provide further care.
Applying incentives similar to those used in other programs, such as eye examinations at no out-of-pocket cost and discounted cost for eyeglasses, helped mitigate known barriers to eye care. The majority of our patients (96/103, 93%) lived outside of the clinic zip code, thus requiring transportation to their screening clinic appointment. Despite not offering transportation or having an extensive network of public transportation, the majority of patients attended their follow-up appointment. Screening and referring patients who were already established in the free clinic system and have demonstrated a history of motivation for their own health care may have led to a high referral attendance compared to that of other screening programs set up outside of an established free clinic system.10 We also attribute our high attendance rate to the reminder letter and phone call that was performed 1 week prior to the scheduled appointment. Furthermore, if referral criteria were met, the patient was scheduled and provided with a referral appointment date at the time of screening. We believe that immediately scheduling an appointment likely contributed to the higher referral attendance rate compared to programs in which patients were contacted at a later date to schedule an appointment. This method also eliminates the inability to contact the patient after the initial screening appointment because, in similar vision-screening programs, “No appointment given” was the top barrier to referral appointment attendance.10,11
The main limitation of our study is the small sample size, as a result of lower populations in rural areas compared to urban areas,14 and we recognize that our findings may not be readily generalizable to the larger population. In addition, hosting vision screening only in a single health clinic population further narrowed the scope of our study sample. However, screening this subpopulation of motivated patients may have led to higher attendance of appointments. Vision screenings and data collection are currently ongoing at this site with the aim to obtain long-term follow-up data for patients as well as increase the sample size.15 While limitations may exist for using laypersons for screening examinations instead of professionals, community vision screening by trained medical students has the benefit of increasing the number of potential screeners and further expanding the students’ medical experiences.
Conclusion
The current study highlights the high prevalence of unmet eye care needs in a rural population, but furthermore demonstrates that using medical students and community health centers as a patient base to screen can yield a high referral attendance rate for this at-risk population.
Acknowledgments
The authors thank the Albert Schweitzer Fellowship and the Good Neighbor Health Clinic for assistance in establishing the program. The authors also thank the volunteers (eye care providers and medical students) for their continued participation in the program. This work was presented in part at the Association for Research in Vision and Ophthalmology Annual Meeting in Denver, CO, USA, in May 2015 and in part at the New England Ophthalmological Society Meeting in Boston, MA, USA, in June 2015.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Congdon N, O’Colmain B, Klaver CCW, et al. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol. 2004;122(4):477–485. | ||
Wittenborn JS, Rein DB. Cost of Vision Problems: The Economic Burden of Vision Loss and Eye Disorders in the United States. Chicago, IL: University of Chicago; 2013. Available from: http://www.preventblindness.org/sites/default/files/national/documents/Economic%20Burden%20of%20Vision%20Final%20Report_130611.pdf. Accessed November 8, 2014. | ||
Zimmer-Galler IE, Kimura AE, Gupta S. Diabetic retinopathy screening and the use of telemedicine. Curr Opin Ophthalmol. 2015;26(3):167–172. | ||
Donahue SP, Baker JD, Scott WE, et al. Lions Clubs International Foundation Core Four Photoscreening: results from 17 programs and 400,000 preschool children. J AAPOS. 2006;10(1):44–48. | ||
United States of America Census. United States 2010 Census Urban and Rural Classification and Urban Area Criteria. Suitland, MD: U.S. Census Bureau; 2014. Available from: https://www.census.gov/geo/reference/ua/urban-rural-2010.html. Accessed November 8, 2014. | ||
Zhang X, Saaddine JB, Lee PP, et al. Eye care in the United States: do we deliver to high-risk people who can benefit most from it? Arch Ophthalmol. 2007;125(3):411–418. | ||
Elam AR, Lee PP. High-risk populations for vision loss and eye care underutilization: a review of the literature and ideas on moving forward. Surv Ophthalmol. 2013;58(4):348–358. | ||
Hartley D. Rural health disparities, population health, and rural culture. Am J Public Health. 2004;94(10):1675–1678. | ||
Morgan A. A national call to action: CDC’s 2001 Urban and Rural Health Chartbook. J Rural Health. 2002;18(3):382–383. | ||
Quigley HA, Park CK, Tracey PA, Pollack IP. Community screening for eye disease by laypersons: the Hoffberger program. Am J Ophthalmol. 2002;133(3):386–392. | ||
Cheung NC, Greenberg PB, Anderson KL, Feller ER. Effectiveness of a medical student-organized community vision screening initiative. Med Health R I. 2010;93(8):239, 242, 243. | ||
Friedman DS, Cassard SD, Williams SK, Baldonado K, O’Brien RW, Gower EW. Outcomes of a vision screening program for underserved populations in the United States. Ophthalmic Epidemiol. 2013;20(4):201–211. doi:10.3109/09286586.2013.789533. | ||
Rein DB, Zhang P, Wirth KE, et al. The economic burden of major adult visual disorders in the United States. Arch Ophthalmol. 2006;124(12):1754–1760. | ||
United States of America Census. State and County QuickFacts. Suitland, MD: U.S. Census Bureau; 2014. Available from: http://quickfacts.census.gov/qfd/index.html. Accessed November 8, 2014. | ||
Byrd JM, Longmire MR, Syme NP, Murray-Krezan C, Rose L. A pilot study on providing ophthalmic training to medical students while initiating a sustainable eye care effort for the underserved. JAMA Ophthalmol. 2014;132(3):304–309. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.