")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 7
Implementation of a collaborative care model for the treatment of depression and anxiety in a community health center: results from a qualitative case study
Authors Eghaneyan B, Sanchez K, Mitschke D
Received 29 June 2014
Accepted for publication 9 August 2014
Published 4 November 2014 Volume 2014:7 Pages 503—513
DOI https://doi.org/10.2147/JMDH.S69821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Brittany H Eghaneyan,1 Katherine Sanchez,2 Diane B Mitschke2
1Department of Psychiatry, UT Southwestern Medical Center, Dallas, TX, USA; 2School of Social Work, The University of Texas at Arlington, Arlington, TX, USA
Background: The collaborative care model is a systematic approach to the treatment of depression and anxiety in primary care settings that involves the integration of care managers and consultant psychiatrists, with primary care physician oversight, to more proactively manage mental disorders as chronic diseases, rather than treating acute symptoms. While collaborative care has been shown to be more effective than usual primary care in improving depression outcomes in a number of studies, less is known about the factors that support the translation of this evidence-based intervention to real-world program implementation. The purpose of this case study was to examine the implementation of a collaborative care model in a community based primary care clinic that primarily serves a low-income, uninsured Latino population, in order to better understand the interdisciplinary relationships and the specific elements that might facilitate broader implementation.
Methods: An embedded single-case study design was chosen in order to thoroughly examine the components of one of several programs within a single organization. The main unit of analysis was semi-structured interviews that were conducted with seven clinical and administrative staff members. A grounded theory approach was used to analyze the interviews. Line-by-line initial coding resulted in over 150 initial codes, which were clustered together to rebuild the data into preliminary categories and then divided into four final categories, or main themes.
Results: Four unique themes about how the implementation of a collaborative care model worked in this setting emerged from the interviews: organizational change, communication, processes and outcomes of the program, and barriers to implementation. Each main theme had a number of subthemes that provided a detailed description of the implementation process and how it was unique in this setting.
Conclusion: The results indicated that adequate training and preparation, acceptance and support from key personnel, communication barriers, tools for systematic follow-up and measurement, and organizational stability can significantly impact successful implementation. Further research is necessary to understand how organizational challenges may affect outcomes for patients.
Keywords: collaborative care, measurement based care, implementation, mental health, primary care
Background
Community health centers are continuing to grow as providers of mental health treatment services and can offer a number of benefits in treating mental disorders including “improved coordination and communication between behavioral and medical providers and reduced stigma for patients receiving treatment.”1 The collaborative care model was developed as a method to address mental health in primary care settings by managing mental disorders as a chronic disease rather than treating acute symptoms.2,3 While collaborative care has been shown to be more effective than usual primary care in improving depression outcomes in a number of studies, less is known about the factors that support the translation of intervention research to real-world program implementation.4,5
In an effort to design a new care system to treat patients with chronic illnesses, Wagner, Austin, and Von Korff developed the Chronic Care Model, composed of key practice elements to improve outcomes for chronically-ill patients: the use of plans and protocols, the reorganization of practice to meet patient needs, patient education based on the patient’s needs, an expert system to administer provider education and consultation, and supportive information systems to assist with outcome monitoring, care planning, reminders, and feedback.6 The Chronic Care Model applied to the treatment of mental disorders in primary care settings has become known as integrated health care or collaborative care.2,3 Collaborative care differs from traditional primary care in two essential ways: the use of care managers for proactive follow-up and systematic tracking of outcomes. Collaborative care is more than just co-locating primary care providers and mental health specialists – it is the collaboration of primary care providers and specialty mental health care providers to develop and adjust treatment plans based on the measurement of symptom-related outcomes.2
A recent meta-analysis of 32 studies by Thota et al found that a collaborative care model is effective for patients diagnosed with depression in improving depression symptoms, adherence to treatment, response to treatment, remission of symptoms, recovery from symptoms, quality of life, and satisfaction with care.7 Perhaps the most noted model of collaborative care, Project IMPACT (Improving Mood: Providing Access to Collaborative Treatment for Late-Life Depression), is described as a team of clinicians working together to treat depression using a stepped care treatment algorithm.8 This team includes the patient, the primary care physician, the depression clinical specialist, and a team psychiatrist. Adaptations of the IMPACT model have been effective in reducing depressive symptoms for low-income Latinos with diabetes, low-income patients with cancer, adolescents, and patients with comorbid major depression and/or dysthymia and diabetes mellitus.9–13
Primary care settings are the optimal locations for integration of behavioral and physical health care because they are often the first point of contact for health issues, making them the “gateway to identifying undiagnosed or untreated behavioral health conditions.”14 Evaluations of the IMPACT model have revealed the necessary components that made successful integration possible: a multidisciplinary team with a clearly-defined care manager at the center who is well-versed in depression treatment models and who engages patients using education and behavioral strategies, case presentations at regular team meetings, expert input by a consulting psychiatrist, the use of reliable tracking methods for follow-up, and regular feedback on patient outcomes communicated to team members using simple assessment tools.15
In this case study, we sought to examine implementation of a collaborative care model for the treatment of depression and anxiety in a Federally Qualified Health Center (FQHC) from the perspectives of clinical and administrative staff members. Additionally, we sought to identify perceived barriers to better understand how they may have affected the implementation process. Although research has shown that collaborative care models are superior to usual care in the treatment of depression for various populations,9–13 more research is needed to understand successful implementation of these models in specific settings. Furthermore, implementation research on collaborative health care models has primarily focused on the perspectives of clinical staff members across multiple settings,15 rather than a multi-disciplinary perspective from a single organization or setting.
Methods
Study design
An embedded single-case study design was chosen in order to thoroughly examine the components of one of several programs within a single organization. An advantage to the single-case study design is that it allows for researchers to observe and analyze phenomena that are otherwise inaccessible, in this case, the personal experiences of employees implementing a new program in the real-world setting of a community health center. The embedded variation of the single-case study design provided for a more detailed approach in examining the implementation of one of many programs in the community health center.16 Critical to the design of case studies is the use of multiple sources of data.17 The main unit of analysis for this study included interviews with staff members who were involved in the implementation of a new collaborative care program. In addition to the interviews, other units of analysis included direct observations, review of the grant application for the program, and review of reports and other clinic documents that describe the demographics of the population served, services offered, and other operational descriptions.
Setting
In August 2012, a University-Community partnership was formed between the University’s School of Social Work, a local community health center, and the local mental health authority to implement a measurement-based collaborative care program to treat depression and anxiety in an adult primary care setting. The community health center was the only FQHC in a large metropolitan area in Texas, providing health care services to underserved communities, including uninsured individuals and those with Medicare, Medicaid, and Children’s Health Insurance Program (CHIP). According to federal guidelines, the FQHC was governed by a nine-member board, the majority of whom (at least 51%) were patients of the clinic.
The community health center was located in the center of ten federally designated health professional shortage census tracts.18 In 2012, the community health center served 10,782 unduplicated patients for a total of 27,963 patient visits. Of those 10,782 patients, 81% were Hispanic and 69% of them were uninsured. At least 65% of the patients in 2012 lived below poverty level.
Program implementation
The two key elements of the program implementation included the creation of a collaborative care team and the use of measurement-based care.19 Members of the collaborative care team included the primary care providers, the care manager, a consulting psychiatrist, and the patients and their family members. Working together, these team members developed and executed treatment plans for patients who were enrolled in the program.
Measurement-based care required using the Patient Health Questionnaire (PHQ-9) and the Generalized Anxiety Disorder Assessment (GAD-7) to assess patient progress and guide treatment plans.20–22 These two measures were given to patients at every in-person or telephone session with the Care Manager. These measures were systematically documented by the Care Manager and communicated promptly to the collaborative care team using numbers and graphs.
The Care Manager was a Licensed Masters Social Worker (LMSW) who received specialized training in the collaborative care model. This key team member provided in-person clinical appointments and phone based care to review clinicians’ treatment plans, assure patient understanding of recommended treatment, address barriers to the proposed plan, and provide brief psychosocial interventions. The Care Manager also acted as a liaison between the consulting psychiatrist and the primary care providers, communicating the psychiatrist’s recommendations back to the primary care providers. One of the most important duties of the Care Manager was to maintain information on the measurement-based collaborative care received, including patient measures, and systematically document this information.
Participants
Participants for this case study were selected from the clinic staff because of their involvement in the implementation of the program. The inclusion of both clinical and administrative staff was deemed important in order to gain a broad understanding of the implementation of the program at the community health center. The study was approved by the University’s Institutional Review Board, and written informed consent was obtained prior to each interview.
Data collection
Data collection consisted of seven in-person interviews conducted using a semi-structured, interview guide with each participant. The interviews took place approximately 6 months after the start of the program and included 16 open-ended questions about the process of implementation. The first 15 questions of the interviews were constructed using the features of successful implementation of collaborative care identified by Oishi et al (Table 1).15 The final question asked the participant to describe any clinical or organizational barriers to the implementation of the program. The interviews were conducted by the researcher (BHE) and varied in length from 15 to 30 minutes. Each interview was audio recorded and transcribed verbatim.
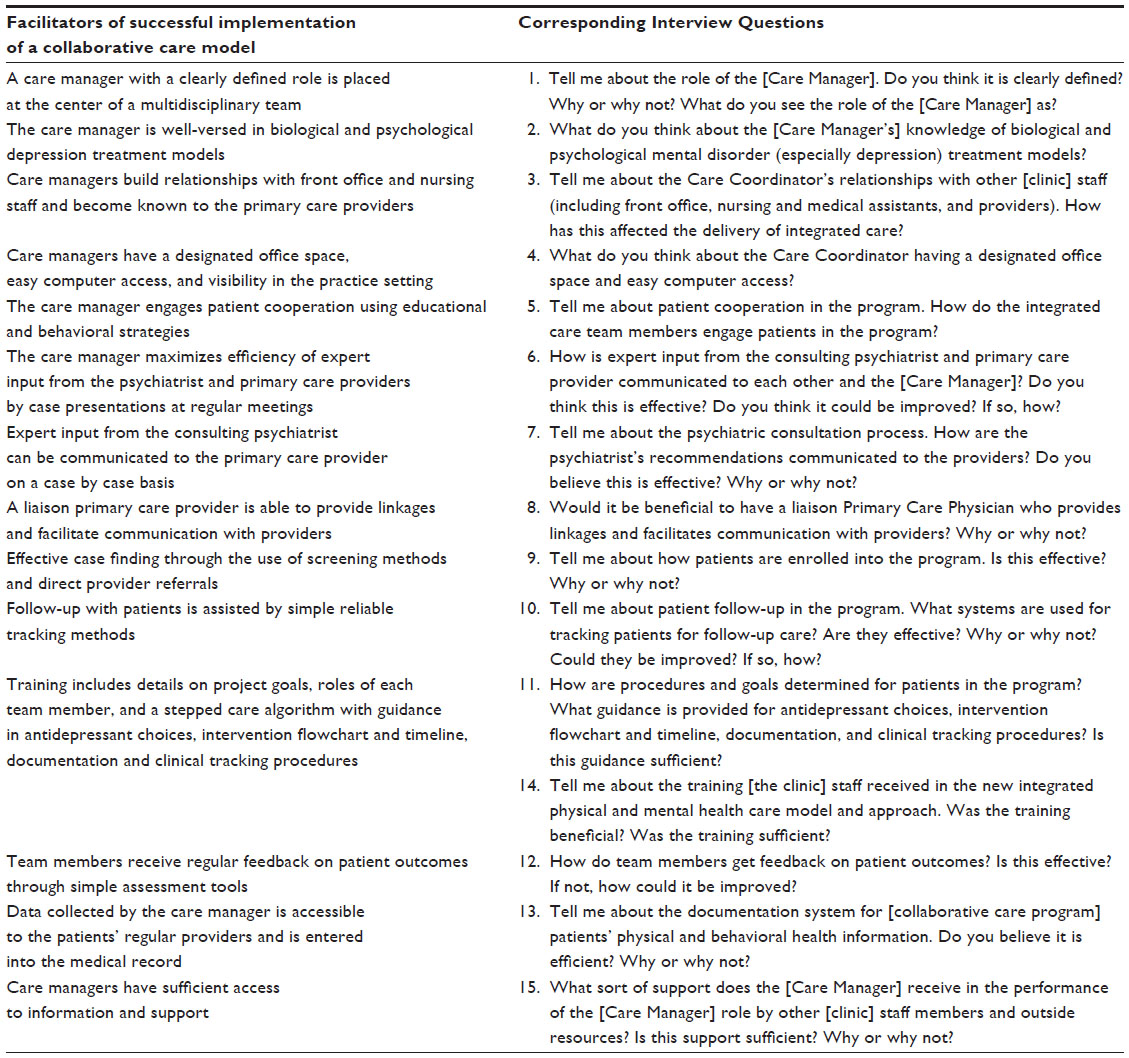 | Table 1 Features that facilitate implementation and corresponding interview questions |
Analysis
A grounded theory approach was used to analyze the qualitative interviews. While there are numerous approaches in analyzing qualitative data, grounded theory approach was chosen because it is best suited for developing an understanding of a central phenomenon based on the perceptions of participants of a process or interaction involving many individuals.17 The application of a grounded theory approach in this study allowed for emerging concepts to drive the process of revealing common themes, as well as divergent notions, from participants in order to gain an understanding of the implementation of a collaborative care model in this setting.
The first step in the interview analysis process was to perform a line-by-line initial coding, which allowed the researcher (BHE) to remain open in the analytics process and create codes that best fit the data.23 This initial coding process resulted in over 150 initial codes. Next, the researcher along with two secondary coders (KS, DM) compared the codes within and across interviews and clustered conceptually similar codes together to rebuild the data into preliminary categories. In the final steps of the analysis, the preliminary categories were divided into four final themes, which were agreed upon by the researcher and both secondary coders. Direct observations, review of the grant application for the program, and review of other clinic documents and reports were used as supplementary data to improve the understanding and context of the data gathered in the interviews.
Results
The participants in the study (N=7) included the Care Manager, three full-time primary care providers (including the Chief Medical Officer), the Nursing Director, the Project Manager, and the Chief Executive Officer. Four unique themes about how the implementation of a collaborative care model worked in this setting emerged from the interviews, with a number of subthemes (Table 2). What follows is a detailed description of the findings.
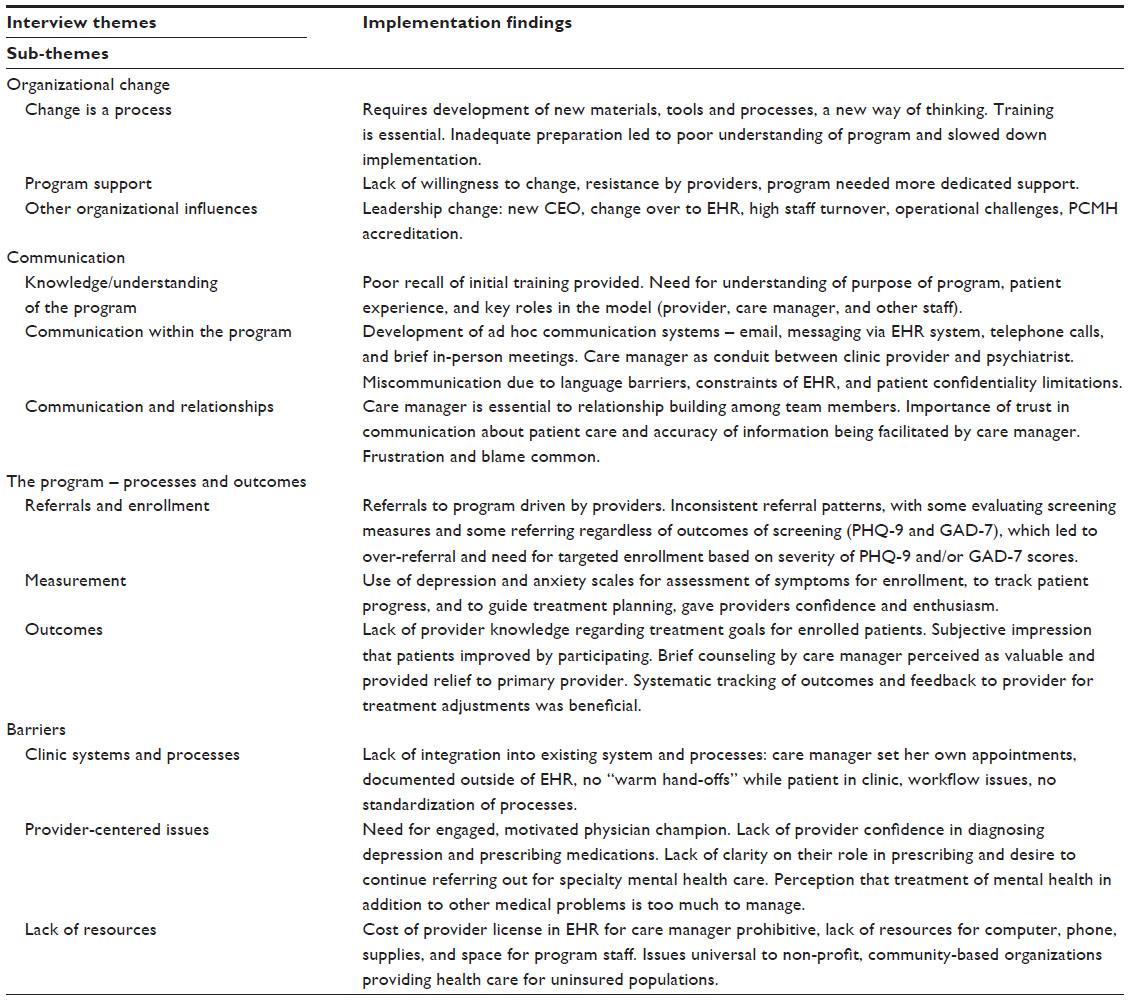 | Table 2 Qualitative findings of factors affecting implementation of a collaborative care model for the treatment of depression and anxiety |
Organizational change
Change is a process
The implementation of the program was a process that occurred in the context of many changes within the organization. It required the development of new materials and processes, as well as a new way of thinking about and approaching patient care. The necessary changes may have been more than the staff expected. One participant explained, “I think that the project is a lot bigger than we even imagined it was going to be.” The enormity of the change the program brought resulted in a lot of trial and error. Two administrative staff members discussed how clinic staff would test a process and see how it worked, then make necessary adjustments. One participant gave an example regarding the process of referring patients to the program:
I know when we first started with it, [the Care Manager] was pretty much getting referrals, pretty much like nonstop […] and then we identified that there was an additional item that needed to be addressed […] because it was getting too large. So I think the training at first wasn’t that great, but I think we obviously needed to have a plan and then try it out and then we saw that there needed to be changes and [the Care Manager] adapted that, and then she got more adequate referrals for the […] program. So I felt that it was a growing process.
Other staff members discussed the development of new materials necessary for the collaborative care team. The Care Manager and a student intern worked to create psychosocial assessments for the patients, a documentation and patient tracking system, as well as a patient progress report used to provide feedback to the providers and patients regarding the patients’ treatment. Along with the development of materials, staff members were also required to develop themselves in terms of the way they approached the treatment of depressed patients. One participant referred to the need of the staff members to adjust their “mindset” when it came to providing collaborative care.
Program support
Support for the program was necessary but not always evident. Several participants identified a lack of “staff willingness to change,” “resistance” by providers, and only a few staff members being “open to helping”. One participant hypothesized that the clinic staff may have felt this way because the addition of the program meant “a lot of new things for us to adapt to and be involved with”. While a few participants described the use of student interns and assistance from administrative staff members as forms of support the Care Manager was receiving, a majority of participants felt that the program needed more support than it had. When describing the importance of staff participation in making the program successful, one participant explained, “It’s ultimately the team effort that counts”.
Other organizational influences
During the implementation of the program, several other organizational changes were also occurring. One participant emphasized this point by saying, “There’s so many things happening in the clinic at the same time. It’s overwhelming to everybody.” These changes included a leadership transition with the hiring of a new Chief Executive Officer, the implementation of an electronic health record (EHR) system, high turnover in staff, and other “operational challenges”, as described by one administrative staff member. Additionally, three staff members referred to the Patient Centered Medical Home, an accreditation the organization was actively seeking at the time of program implementation.
Communication
Knowledge/understanding of the program
Communication about the program was critical for the staff members’ understanding/knowledge of the program. Initial communication was done through training before the implementation of the program. Some participants recalled that no training was given prior to implementation, while others acknowledged that they had a few meetings about the program, but believed the training was insufficient. One provider stated, “I think we have been told […] how to do the referral. That’s about it.” Staff members also expressed that they believed the training could have been improved:
[…] with a new program, this is what it’s about, this is what’s going to happen, this is what patients are going to experience, this is what the communication with the providers [will be]. It’s just, I don’t think that happened.
As a result of insufficient training, some of the participants described a lack of understanding about how the model worked, and more specifically, of the role of the Care Manager. One participant explained, “I’m not sure that everybody in [the clinic] clearly understands […] the Care [Manager] [position] itself and what it actually means.” Another participant expressed that when the Care Manager was first hired, staff members needed “more clarity on how things are going to flow”.
Once the program implementation began, staff members received guidance on procedures and goals from the Principal Investigator and Care Manager. Every participant agreed that the Care Manager had ample knowledge of biological and psychological depression treatment models. One participant described the Care Manager as “thorough” and “clear” when providing guidance to staff members and patients on depression scales. Other staff members highlighted the Care Manager’s knowledge of counseling, with some participants believing her knowledge was greater than the providers’. It was important for the Care Manager to communicate with providers and demonstrate her abilities so that she could “really put her role out there so that if she’s needed, she’s called upon,” or in other words, create awareness among the staff as to her role within the collaborative care team.
Communication within the program
The collaborative care team members used various forms of communication with each other. Emails, messaging via the EHR system, telephone calls, and in-person meetings were all ways in which communication about patients within the program was conducted. Staff members also noted that all communication about patients between the consulting psychiatrist and primary care providers happened through the Care Manager. One provider explained, “because of the time constraints that we as providers have, [the] Care [Manager] is the only one who is between the psychiatrist and the physicians here.” Some participants thought this was the most effective way of communicating given the circumstances, “Because the doctors don’t have time to actually set aside and talk to each other.”
Despite participants feeling that communication through the Care Manager was effective, all of the participants agreed that communication within the program could be improved overall. One participant believed there was a “huge gap” in communication between clinic staff. Other related issues included miscommunications between team members due to language barriers, issues with patient confidentiality, and constraints of the EHR system. Three participants felt that direct communication between the primary care providers and consulting psychiatrist would be beneficial. One of the providers explained:
That may be an opportunity, you know, where the Care [Manager] sets times […] designated times where they go over certain cases at the providers’ meetings and she brings cases and the psychiatrist is there. Let’s go quickly about this top three, or top four where we haven’t seen [improvement]. So I think that’s an area of improvement that I would suggest.
Communication and relationships
Communication between the collaborative care team members also played a critical role in relationship building. Several staff members commended the Care Manager on her ability to create relationships with clinic staff. One participant stated, “I think she’s been able to build a lot of relationships throughout all the different departments within the clinic.” One of the providers described her relationship with the Care Manager as a “really smooth, working relationship.” The importance of trust was brought up by another provider, who explained that since the clinic providers did not have direct communication with the consulting psychiatrist, they had to trust that the Care Manager was passing along accurate information from her.
Along with improvements in communication, some participants felt that relationships between collaborative care team members could also be strengthened. With regard to the Care Manager’s relationship with clinic staff, one administrative staff member stated, “I think they have respect for that role […] I think that there is still a need for improvement.” Two participants spoke of staff being frustrated with each other due to differences in “point of view” and staff being unable “to relate to and accept” information, with one participant describing situations in which “emotions run high” and staff members then blamed one another when things went wrong.
The program – processes and outcomes
Referrals and enrollment
As previously mentioned, it was the providers’ job to refer patients to the program. The PHQ-9 and GAD-7 were used to assess patients’ depression and anxiety levels and would guide the provider in making the decision as to whether or not to refer patients to the program. If the provider decided the patient needed more care, they would give the patient information on the program and encourage their participation. One provider explained this process:
So we screen them with the PHQ-9 or the GAD-7 […] and then depending on their score […] we go into detail with them about the program and how they may benefit […] After that discussion, if they say they want to participate, I then go ahead and write a referral in the computer system for the patient to be contacted by the […] program.
Some providers referred to the program, regardless of PHQ-9 or GAD-7 scores. One provider stated, “I just say okay, refer to [the program]. And I refer everything whether it’s mild, moderate, whatever the scores are. I just refer.” This approach led to over referring to the program and required the Care Manager to take a targeted approach to enrollment in the program by prioritizing patients based on the severity of their depression scores. One administrative staff member explained, “We have tons of referrals but that doesn’t mean that they’re all going to get enrolled […] what they’re doing is identifying those at higher levels of depression acuity […] You’re targeting the ones that need it the most.”
Measurement
All but one participant mentioned the use of scales to measure patients’ depression and/or anxiety levels in the program. The PHQ-9 and GAD-7 were not only used to assess patients for enrollment, but also to track patient progress throughout their participation in the program and guide treatment plans. The Care Manager developed a patient progress report to give feedback to providers using graphs of PHQ-9 and GAD-7 scores. One provider expressed her enthusiasm for the patient progress report by stating, “they do their PHQ-9s and they see how the scores are doing, which is a good thing […] That’s a measure, so it’s a good thing.” Another provider explained how measurement by the Care Manager was used to influence treatment plans:
She does the screening again and sees if their scores are improving, going up, and then tries to assess from them why that might be happening […] So I can go in there […] with a plan as to what we’re going to do from that point on, looking at those measures.
Outcomes
A majority of participants did not know what the goals were for patients who were enrolled in the program. Only two participants mentioned reductions in PHQ-9 and GAD-7 scores as a goal for patients, one of which said the goal was a 50% reduction, and the other who stated there was no stipulated goal. Despite not knowing what the goals were, most of the participants did feel the program was helpful to patients in decreasing their depression and anxiety. One provider stated, “I see an improvement in the patients that I send out to the […] program” and another provider agreed, “for most of the patients, I think it works out well.”
Providers also experienced benefits of having the program. All three of the provider participants expressed that the counseling provided to patients by the Care Manager was valuable. One provider shared:
I cannot do everything when I see a patient. Obviously, I will need more help […] If I spend more time, it’s a waste of resources and it’s a waste of finances. But a Care [Manager] can have a more targeted approach and that’s the whole purpose of her […] is that we reduce the amount of time that a physician can spend counseling or doing [things] that a Care [Manager] can do, or a person who is experienced in counseling can do.
The regular tracking of patients’ depression measures and feedback to the provider by the Care Manager in order to make treatment adjustments was also a benefit discussed by two of the providers. One provider stated, “That’s the reason why I send them out to the […] program. So they can be tracked appropriately and I can get a good report on what’s happening with their depression or anxiety.” Another provider shared, “That’s the beauty of the program. That’s the whole point. So that’s a great thing.”
Barriers to implementation
Clinic systems and processes
Several staff members referred to a lack of integration between the program and existing clinic systems and processes. The Care Manager had to make her own appointments, develop her own documentation system, and did not receive referrals for patients while they were still present in the clinic, a concept known as “warm hand-offs.” Other participants brought up workflow issues and the need for standardization in processes when discussing the implementation of the program.
Almost every participant mentioned the clinic’s EHR system, NextGen. Patient notes created by the Care Manager, as well as patients’ progress reports, were not integrated into the NextGen system. One participant believed the problems associated with NextGen stemmed from not having a NextGen “expert”, which prevented the Care Manager from accessing the mental health templates in the EHR. Most participants echoed the sentiment of one participant who stated, “The inability to fully integrate into a computer system has been a huge barrier.”
Provider-centered issues
Three participants brought up issues with the primary care providers when it came to integrating mental health into primary care at the clinic. One participant felt that providers “really weren’t interested in the mental health or integration” and another participant stated, “I think the need for engaged, motivated, champions around behavioral care […] in terms of our providers. I think that’s a barrier.” Other participants referred to the inhibition providers possessed in diagnosing mental disorders and prescribing medications. In describing the many issues surrounding the providers, one participant shared:
Physicians were barriers. Their thought process was different. The lack of education about the program, as well as […] anxiety and depression. The doctors here, although they prescribe medications, still lack some understanding of why we provide the medication and the fact that [the program] was here in the building to begin with. They still wanted to refer over to [the local mental health authority].
Another challenge concerning providers included the difficulty providers faced in managing their patients’ mental health. One provider explained, “Behavioral health is a difficult area in medicine to practice, especially in primary care, because we still got to manage all their other medical problems […]” Additionally, one participant questioned whether or not providers were using information gathered by the Care Manager during patient follow-ups to guide treatment plans.
Lack of resources
A lack of financial resources was brought up by nearly all of the participants and included the inability to purchase a provider license on the NextGen system for the Care Manager, the inability to purchase needed supplies such as computers and phones, and the inability to hire more staff to implement collaborative care and acquire space to place them. With regard to a lack of resources, one administrative staff member noted, “These are limitations that come with being an underfunded organization, being a community organization with huge financial challenges.”
Discussion
The current case study illustrates one example of implementation of a collaborative care program in the distinct context of an FQHC that serves a primarily low-income, Latino population. Review of the implementation process from the perspectives of clinical and administrative staff provided an in-depth, behind the scenes look at what can happen when an evidence-based model of depression care is implemented in a real-world primary care setting. Several key findings emerged from this study.
First, a lack of adequate preparation for the program was indicated by clinic staff members. Trainings that include defined procedures for interventions and explanations of how the programs will benefit their community, patients, and organizations are extremely helpful in implementing collaborative care in primary care settings.15,24 Clinic staff felt that they did not receive sufficient training prior to the implementation of the program, and as a result, many staff members did not have a full understanding of the purpose of the program and how it worked. Additionally, many tools and processes had to be developed after the start of implementation, which may have ultimately slowed down the implementation process. This potential loss of momentum in carrying out the program has been shown to negatively affect implementation outcomes in other programs.24
Support for the implementation of a new collaborative care program by staff members is critical to the program’s success. Efforts to improve depression care in primary care settings tend to face more challenges when they do not have acceptance and support, or “buy-in”, from all parties involved.25 More specifically, leadership support has been highlighted as an important factor in implementing changes in depression care treatment.24,25 While the clinic’s administrative staff was perceived as having a role in supporting the program, there was resistance from most of the other staff members, including primary care providers. Previous studies have found that buy-in from clinical providers was a stronger determinant in successful implementation of collaborative care models than leadership support.26
A lack of support for the program may have been influenced by the significant amount of change within the organization at the time of program implementation. Staff members seemed to be overwhelmed by the recent implementation of an EHR system, changes in leadership, high staff turnover, and the push for Patient Centered Medical Home accreditation. These findings confirm other research that has found it is more challenging to implement a collaborative care model in the face of management turnover, competing demands for clinician time, and competing quality improvement efforts.25,27
Communication and relationships between members of the collaborative care team proved to be very important aspects of the implementation process. Like other collaborative care models described,15 the program staff found various ways to communicate with each other including the use of email, phone calls, EHR system messaging, and brief in-person meetings. Despite their efforts, many felt that communication and relationships between staff could be improved. Suggested improvements included direct communication between primary care providers and the consulting psychiatrist, and confirmed previous research showing that structured, multidisciplinary team meetings were extremely helpful in creating treatment plans and facilitating program implementation.15,28 As emphasized by Oishi et al, weekly team meetings can serve as a powerful tool in promoting relationships among team members. The absence of team meetings coupled with the absence of a liaison primary care provider who functions to “facilitate communication with providers” may have hindered crucial communication and relationship building necessary for the successful implementation of the program.15
Along with the addition of the Care Manager, systematic tracking of patient outcomes is a core component of the collaborative care model.2,29 In this setting, while the importance of symptom measurement with the PHQ-9 and GAD-7 to guide clinical decision making, was emphasized by clinic staff, the use of stepped care treatment algorithms,8,30 was not. Furthermore, systematic tracking of patients is usually assisted by a web-based clinical information system (or patient registry), which has proved to be an invaluable tool in tracking outcomes and preventing patients from falling through the cracks.15,29 With the lack of such a tool, along with the many issues faced by the Care Manager in documentation in the EHR system, it is apparent that systematic patient follow-up and measurement was a huge challenge for this organization.
The value of clearly defined goals has been emphasized in the implementation of a collaborative care model.15 Many staff members at the clinic reported not knowing what the specific treatment goals were for patients (such as a defined decrease in PHQ-9 or GAD-7 scores) who were enrolled in the program, further emphasizing the need for more adequate training. However, even though they did not have a clear idea on goals for their patients, primary care providers generally felt that the program was helpful to patients in decreasing their depression and anxiety levels. This finding is consistent with other research that shows a majority of primary care physicians who implemented collaborative care felt that it improved clinical outcomes for depressed patients.31 Also consistent with previous findings was that clinic providers found it helpful that the Care Manager was able to regularly follow-up with and track patients, which helped facilitate treatment adjustments when needed.31
Finally, the unique organizational characteristics of community based clinics often present added barriers to the implementation of collaborative care,29 some of which were discussed in this study and included a limited amount of staff and space dedicated to the program and problems with using the EHR system. While such organizations often cite lack of reimbursement for services as financial barriers to collaborative care,32 the financial barriers reported by the clinic staff in the current study were different. The organization was struggling with financial challenges which included the ability to fund day-to-day operations, an issue which preceded the addition of the program. Concerns regarding reimbursement for program services may not have been a priority since the Care Manager’s position was partially funded by the University partnership and a majority of the clinic’s patients were uninsured. If the clinic seeks to establish long-term sustainability for the program, issues with reimbursement may become more of an interest.
Limitations
The present study has limitations with regard to generalizability. Because a single-system case study design was used, the findings from this study only reflect the perspectives of staff members who implemented a collaborative care model at one FQHC in Texas and may not be representative of collaborative care programs in other primary care settings. Additional limitations are related to the interview process used with participants in the study. The results of the interviews may reflect participant biases and not portray certain topics or themes accurately. Relationships with the researcher who was conducting the interviews could have also affected the results. Some participants may not have been as honest nor forthcoming with their opinions on the implementation of the program had they been interviewed by someone who had not been involved with the program or clinic.
Conclusion
Despite its limitations, this case study demonstrates that implementing a collaborative care model can be challenging for some organizations, especially for those that lack resources and support for staff members. Many things should be taken into consideration before implementing a new model to address mental health care in a primary care setting including adequate training and preparation, buy-in from key personnel, possible communication barriers, tools for systematic follow-up and measurement, and organizational stability. While this study highlighted several challenges that can be experienced during the implementation process, further research is needed to understand how these challenges affect health outcomes for patients.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
Druss BG, Bornemann T, Fry-Johnson YW, McCombs HG, Politzer RM, Rust G. Trends in Mental Health and Substance Abuse Services at the Nation’s Community Health Centers: 1998-2003. Am J Public Health. 2008;98(Suppl 9):S126–S131. | |
Thielke S, Vannoy S, Unützer J. Integrating mental health and primary care. Prim Care. 2007;34(3):571–592. | |
Unützer J, Schoenbaum M, Druss BG, Katon WJ. Transforming mental health care at the interface with general medicine: report for the presidents commission. Psychiatr Serv. 2006;57(1):37–47. | |
Gilbody S, Bower P, Fletcher J, Richards D, Sutton AJ. Collaborative Care for Depression. Arch Intern Med. 2006;166(21):2314–2321. | |
Unützer J, Powers D, Katon W, Langston C. From establishing an evidence-based practice to implementation in real-world settings: IMPACT as a case study. Psychiatr Clin North Am. 2005;28(4):1079–1092. | |
Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. 1996;74(4):511–544. | |
Thota AB, Sipe TA, Byard GJ, et al. Collaborative Care to Improve the Management of Depressive Disorders: A Community Guide Systematic Review and Meta-Analysis. Am J Prev Med. 2012;42(5):525–538. | |
Unützer J, Katon W, Williams JW Jr, et al. Improving primary care for depression in late life: the design of a multicenter randomized trial. Med Care. 2001;39(8):785–799. | |
Ell K, Xie B, Quon B, Quinn DI, Dwight-Johnson M, Lee PJ. Randomized controlled trial of collaborative care management of depression among low-income patients with cancer. J Clin Oncol. 2008;26(27):4488–4496. | |
Gilmer TP, Walker C, Johnson ED, Philis-Tsimikas A, Unützer J. Improving Treatment of Depression Among Latinos With Diabetes Using Project Dulce and IMPACT. Diabetes Care. 2008;31(7):1324–1326. | |
Katon WJ, Von Korff M, Lin EH, et al. The Pathways Study: A Randomized Trial of Collaborative Care in Patients With Diabetes and Depression. Arch Gen Psychiatry. 2004;61(10):1042–1049. | |
Richardson L, McCauley E, Katon W. Collaborative care for adolescent depression: a pilot study. Gen Hosp Psychiatry. 2009;31(1):36–45. | |
Unützer J, Katon W, Callahan CM, et al. Collaborative Care Management of Late-Life Depression in the Primary Care Setting: A Randomized Controlled Trial. JAMA. 2002;288(22):2836–2845. | |
Sanchez K, Chapa, T, Ybarra R, Martinez ON. Enhancing the delivery of health care: Eliminating health disparities through a culturally and linguistically centered integrated health care approach. Hogg Foundation for Mental Health; Jun 2012. | |
Oishi SM, Shoai R, Katon W, et al. Impacting Late Life Depression: Integrating a Depression Intervention into Primary Care. Psychiatric Q. 2003;74(1):75–89. | |
Yin RK. Case Study Research: Design and Methods. 3rd ed. SAGE Publications; 2003. | |
Creswell JW. Qualitative Inquiry and Research Design: Choosing Among Five Approaches. 3rd ed. SAGE Publications; 2012. | |
Find shortage areas: HPSA by state and county. 2013. Available from: http://hpsafind.hrsa.gov/HPSASearch.aspx. Accessed July 7, 2013. | |
Sanchez K, Trivedi MH. METRIHC: Measuring and Tracking Integrated Health Care. Arlington, TX: The University of Texas at Arlington; 2012:19. | |
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. | |
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. | |
Trivedi MH. Evaluating and monitoring treatment response in depression using measurement-based assessment and rating scales. J Clin Psychiatry. 2013;74(7):e14. | |
Charmaz K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis. Pine Forge Press; 2006. | |
Graff CA, Springer P, Bitar GW, Gee R, Arredondo R. A Purveyor Team’s Experience: Lessons Learned From Implementing a Behavioral Health Care Program in Primary Care Settings. Fam Syst Health. 2010;28(4):356–368. | |
Meredith LS, Mendel P, Pearson M, et al. Implementation and maintenance of quality improvement for treating depression in primary care. Psychiatr Serv. 2006;57(1):48–55. | |
Bauer AM, Azzone V, Goldman HH, et al. Implementation of collaborative depression management at community-based primary care clinics: an evaluation. Psychiatr Serv. 2011;62(9):1047–1053. | |
Nutting PA, Gallagher KM, Riley K, White S, Dietrich AJ, Dickinson WP. Implementing a Depression Improvement Intervention in Five Health Care Organizations: Experience from the RESPECT-Depression Trial. Adm Policy Ment Health. 2007;34(2):127–137. | |
Franx G, Oud M, de Lange J, Wensing M, Grol R. Implementing a stepped-care approach in primary care: results of a qualitative study. Implement Sci. 2012;7(1):8. | |
Fortney J, Enderle M, McDougall S, et al. Implementation outcomes of evidence-based quality improvement for depression in VA community based outpatient clinics. Implement Sci. 2012;7(1):30. | |
Trivedi MH, Fava M, Marangell LB, Osser DN, Shelton RC. Use of treatment algorithms for depression. J Clin Psychiatry. 2006; 67(9):1458–1465. | |
Levine S, Unützer J, Yip JY, et al. Physicians’ satisfaction with a collaborative disease management program for late-life depression in primary care. Gen Hosp Psychiatry. 2005;27(6):383–391. | |
Sanchez K, Thompson S, Alexander L. Current strategies and barriers in integrated health care: a survey of publicly funded providers in Texas. Gen Hosp Psychiatry. 2010;32(1):26–32. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.