")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Impaired social cognition in anorexia nervosa patients
Authors Hamatani S , Tomotake M, Takeda T , Kameoka N, Kawabata M, Kubo H, Tada Y, Tomioka Y, Watanabe S, Ohmori T
Received 5 July 2016
Accepted for publication 30 August 2016
Published 5 October 2016 Volume 2016:12 Pages 2527—2531
DOI https://doi.org/10.2147/NDT.S116521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Taro Kishi
Sayo Hamatani,1 Masahito Tomotake,2 Tomoya Takeda,1 Naomi Kameoka,3 Masashi Kawabata,3 Hiroko Kubo,3 Yukio Tada,3 Yukiko Tomioka,4 Shinya Watanabe,4 Tetsuro Ohmori4
1Graduate School of Medical Sciences, Tokushima University, 2Department of Mental Health, Institute of Biomedical Sciences, Tokushima University Graduate School, 3Department of Psychiatry, Tokushima University Hospital, 4Department of Psychiatry, Institute of Biomedical Sciences, Tokushima University Graduate School, Tokushima, Japan
Background: The purpose of this study was to investigate the characteristics of social cognition in patients with anorexia nervosa (AN).
Methods: Eighteen female patients with AN (mean age =35.4±8.6 years) and 18 female healthy controls (HC) (mean age =32.8±9.4 years) participated in the study. Their social cognition was assessed with the Social Cognition Screening Questionnaire (SCSQ).
Results: The results showed that total score of the SCSQ and scores of theory of mind and metacognition were significantly lower in AN group than those in HC group. Moreover, significant differences in theory of mind, metacognition, and total score of the SCSQ remained when the effects of depression, anxiety, and starvation were eliminated statistically.
Conclusion: These results suggest that patients with AN may have difficulty inferring other people’s intention and also monitoring and evaluating their own cognitive activities. Therefore, these features may explain some aspects of the pathology of AN.
Keywords: anorexia nervosa, social cognition, theory of mind, metacognition
Introduction
Previous studies have revealed that some traits of autistic spectrum disorder (ASD) were often observed in anorexia nervosa (AN) patients and not a few AN patients were diagnosed as having ASD.1,2 Therefore, cognitive characteristics found in patients with ASD have been paid attention to in the research of AN. To date, set-shifting, central coherence, and social cognition of AN patients have been explored to discover the neurocognitive factors related to pathology of the disease.3–5
Holliday et al reported that difficulty of set-shifting in AN patients was not a consequence of starvation.6 Other studies also revealed that dysfunction of set-shifting was not due to the influence of other clinical factors such as psychiatric symptoms.7 Also, as for central coherence, it is reported that AN patients have weak central coherence that leads to their focus on local rather than global processing, particularly in visuospatial domain.8 Kanakam et al regarded poor ability of set-shifting and weak central coherence as the endophenotypes of eating disorders.4
On the other hand, research on social cognition including theory of mind (ToM) is still at initial stage and so far, divergent findings have been reported.9 Social cognition refers to the psychological processes that are related to perception, encoding, storage, retrieval, and regulation of information about other people and ourselves.10 ToM is the ability to understand the mental states of other people and oneself and use this information to predict their behavior.11 Harrison et al reported that AN patients had significantly lower score on the Reading the Mind in the Eyes12 and more difficulties in emotion regulation than healthy controls (HC).13 Later, they found in a study with a larger sample size that only restrictive AN patients had significantly lower score in Reading the Mind in the Eyes than HC.14 However, Tchanturia et al reported that AN patients showed worse performance not only in ToM task but also in control task, and did not bolster a specific link between ToM and AN.15 Oldershaw et al suggested that poor performance in ToM task in AN patients might be caused by starvation.5 Considering these results, characteristics of social cognition of AN patients are still unclear. Especially, it seems unclear whether poor performance in social cognition in AN patients is caused by depression and anxiety, which are the common symptoms in AN patients.13,14,16,17
Furthermore, researchers have begun to pay much attention to the metacognition of AN patients. Metacognition is the ability to evaluate the accuracy of one’s own judgments,18 and poor metacognition of AN patients has been reported.19,20 Nevertheless, as far as we know, there is no study to investigate if metacognition of AN patients is influenced by clinical symptoms such as depression, anxiety, and starvation.
The purpose of this study was to elucidate the characteristics of social cognition of AN patients.
Methods
Subjects
Clinical data were collected from the Department of Psychiatry, Tokushima University Hospital from 1 March 2015 to 31 March 2016. Subjects consisted of 18 female patients having a Diagnostic and Statistical Manual of Mental Disorders-521 diagnosis of AN and 18 HC matched for sex, age, and intellectual ability. Patients were excluded if they presented with any organic central nervous system disorder, epilepsy, mental retardation, severe somatic disorder, or substance dependence. Of 28 patients, 19 agreed to participate in the study. As one patient did not complete all the assessments, data from 18 patients were used for analysis.
As for HC, subjects were excluded if they had a history of any psychiatric illness or if their score of depression or anxiety was not within the range of mean ± 2 standard deviation (SD) or if their body mass index (BMI) was not within normal range (18.5–24.9).22 We recruited HC from university and the local community.
All subjects were native Japanese speakers and gave us written consent to participate in this study.
Measures
Subjects were examined by experienced clinical researchers using the following measures:
- Japanese Adult Reading Test (JART)
To estimate intellectual ability, we used the JART,23 that is, the Japanese version of the National Adult Reading Test.24 In the present study, 25-item short version of the JART was used. - Beck Depression Inventory-II (BDI-II)
The Japanese version of the BDI-II25,26 was used to assess severity of depression. The BDI-II consists of 21 self-report items and each item is measured on a 4-point scale. Higher score represents severe level of depression. - State–Trait Anxiety Inventory-Form JYZ (STAI-JYZ)
The STAI-JYZ,27 that is, the Japanese version of the STAI,28 was used to evaluate state and trait anxiety. It consists of 40 self-repot items and each item is rated on a 4-point scale. State anxiety reflects evoked anxiety to a temporary situation and trait anxiety involves a general tendency to perceive situations as threatening. Higher score indicates higher level of anxiety. - Social Cognition Screening Questionnaire (SCSQ)
The Japanese version of the SCSQ18,29 was used to assess social cognition. The SCSQ has five domains, which are verbal memory, schematic inference, ToM, metacognition, and hostility bias. The task comprises ten short vignettes. Tester reads aloud each vignette and the subject answers three questions for each vignette with “yes” or “no”. Then, in the last question for each vignette, the subject answers about their confidence level of the answers. Higher score represents better level in each domain, except for hostility bias. As for hostility bias, higher score means larger bias.
Statistical analysis
Data analysis was performed using the Predictive Analytics Software Statistics 18 software (2009; SPSS Japan Institute). The comparison of demographic and clinical variables and the scores of the SCSQ between the AN and HC groups was carried out using Mann–Whitney U-test, and r(Z/√N) was calculated to provide effect sizes, with an effect size of <0.1 defined as small, <0.3 as medium, and >0.5 as large.30 Then, in order to investigate whether there is still a significant difference in the scores of the SCSQ between the two groups when controlling for the effects of other clinical and demographic variables, analysis of covariance test was performed with the variables that showed significant differences in the preceding comparison as a covariate. Also, ηp2 (SS effect/[SS effect + SS error]) was calculated to provide effect sizes, with an effect size of <0.01 defined as small, <0.06 as medium, and >0.14 as large.
Ethical considerations
This study was approved by the Clinical Research Ethics Committee of Tokushima University Hospital.
Results
Demographic and clinical characteristics of the AN and HC groups are shown in Table 1. There was no significant difference in age and estimated intelligence quotient between the two groups. AN group presented a significantly lower BMI score (U=0.00, P<0.0001, r=−0.86) than HC group. Also, there were significant differences in BDI-II score (U=30.00, P<0.0001, r=−0.70), state anxiety score (U=51.50, P<0.0001, r=−0.58), and trait anxiety score (U=29.00, P<0.0001, r=−0.70) between the two groups.
 | Table 1 Demographic and clinical variables of the AN and HC groups |
Scores of the SCSQ in AN and HC groups are shown in Table 2. There were significant differences in ToM (U=85.50, P=0.012, r=−0.42), metacognition (U=94.00, P=0.023, r=−0.38), and total score of the SCSQ (U=67.50, P=0.003, r=−0.50) between the two groups. On the other hand, there was no significant difference in verbal memory, schematic inference, and hostility bias between them. Analysis of covariance with scores of the BDI-II, the STAI-JYZ, and BMI as a covariate showed significant differences in scores of ToM (F(1, 30)=6.60, P=0.015, ηp2=0.16), metacognition (F(1, 30)=5.62, P<0.024, ηp2=0.13), and the total (F(1, 30)=8.01, P=0.008, ηp2=0.17) between the two groups.
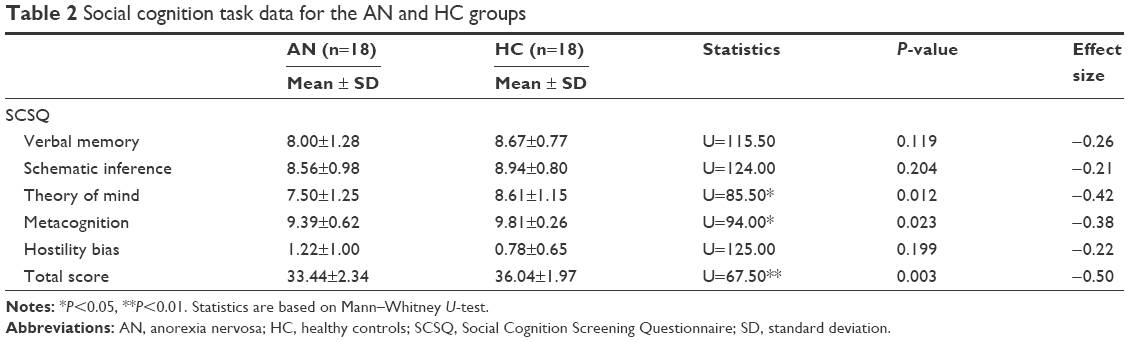 | Table 2 Social cognition task data for the AN and HC groups |
Discussion
As for ToM, although some previous studies reported poor performance in ToM task in AN patients,13,14 there are also studies reporting negative findings about it. For example, Tchanturia et al15 and Russell et al17 found that AN group showed worse performance in both control and ToM elements of Happé’s Task31 than HC group.
Tapajóz et al also reported that AN patients had poorer performance in both ToM and control tasks of the Faux Pas Test32 than HC.16 Moreover, Oldershaw et al reported that worse performance in ToM task might be a result of starvation.5 These studies suggest that general cognitive function of AN patients may be worsened by some clinical factors.15–17
Although it is well known that AN patients often suffer from depression, anxiety, or other symptoms due to starvation, whether these coexisting symptoms would influence their social cognition is still unclear. In the present study, the average BMI of AN patients was much lower than that reported in previous studies15–17 and the levels of depression and anxiety were much higher than HC. Nevertheless, ToM was still significant after eliminating the effects of depression, anxiety, and BMI statistically. Therefore, we could conclude that AN patients’ poor performance in ToM task is not a result of such symptoms, but a definite cognitive feature.
Our findings also show dysfunction of metacognition of AN patients. To date, the ability of metacognition of AN patients has been reported to be worse than HC.19,20,33,34 Moreover, Arbel et al reported that metacognition might be an important mediator between basic cognitive deficits and poor insight.35 However, little is known about whether coexisting clinical symptoms such as depression, anxiety, and starvation influence metacognition. In the present study, we found that poor ability of metacognition still existed after removing the effects of depression, anxiety, and BMI statistically. Since metacognition refers to one’s knowledge concerning one’s own cognitive processes or anything related to them,36 we could suggest that AN patients are not good at monitoring and evaluating their own cognitive activities. Olstad et al reported that metacognition explained 51% of the variance in eating disorder symptoms, with “need to control thoughts” being the most important factor.20 Konstantakopoulos et al37 and Steinglass et al38 explained that distortion of body image was the main aspect of lack of awareness of the illness. Similarly, the present results could contribute to the explanation of some symptoms such as poor insight into disease or distortion of body image.
Besides ToM and metacognition, there was no significant difference in other domains of the SCSQ between AN and HC groups in the present study. As for verbal memory, Tapajóz et al reported no significant difference between AN and HC groups in memory ability assessed with the Faux Pas Test.16 Oltra-Cucarella et al also reported no significant difference in short-term recall and delayed recall between AN and HC groups.39 Considering these findings, we could conclude that verbal memory of AN patients is not impaired. Also, as for schematic inference, since it refers to the ability to infer what is occurring in a specific situation from uncertain and ambiguous context information,18 our result suggests that AN patients have no deficit of the ability. As to hostility bias, Dapelo et al found that AN group had a tendency to recognize people’s expression as being angry in the facial emotion recognition task.40,41 On the other hand, no significant difference in hostility bias was found between AN and HC groups in the present study. From these findings, it seems possible that AN patients could correctly recognize hostility bias from sentence task, but not from nonlanguage task.
Limitations
The current study has some limitations. First, the participation rate was relatively low. Therefore, the results may not reflect the features of the entire population of AN patients. Second, the sample size was relatively small. Therefore, further study with larger sample size would be required to confirm our results.
Conclusion
In conclusion, in the present study, we found that AN patients had poor performance in ToM and metacognition tasks, and depression, anxiety, and starvation did not influence the results. Therefore, it is suggested that poor ability of the two areas of social cognition may be considered as factors related to the pathology of AN.
Acknowledgment
The authors would like to thank all subjects for participating in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Nilsson EW, Gillberg C, Gillberg IC, Råstam M. Ten-year follow-up of adolescent-onset anorexia nervosa: personality disorders. J Am Acad Child Adolesc Psychiatry. 1999;38(11):1389–1395. | ||
Okuhira Y. Investigation of autistic tendency in eating disorders: the follow-up survey using the autism-spectrum quotient (AQ). Jpn J Psychosom Med. 2008;48(5):339–348. Japanese. | ||
Tenconi E, Santonastaso P, Degortes D, et al. Set-shifting abilities, central coherence, and handedness in anorexia nervosa patients, their unaffected siblings and healthy controls: exploring putative endophenotypes. World J Biol Psychiatry. 2010;11(6):813–823. | ||
Kanakam N, Raoult C, Collier D, Treasure J. Set shifting and central coherence as neurocognitive endophenotypes in eating disorders: a preliminary investigation in twins. World J Biol Psychiatry. 2013;4(6):464–475. | ||
Oldershaw A, Hambrook D, Tchanturia K, Treasure J, Schmidt U. Emotional theory of mind and emotional awareness in recovered anorexia nervosa patients. Psychosom Med. 2010;72(1):73–79. | ||
Holliday J, Tchanturia K, Landau S, Collier D, Treasure J. Is impaired set-shifting an endophenotype of anorexia nervosa? Am J Psychiatry. 2005;162(12):2269–2275. | ||
Roberts ME, Tchanturia K, Treasure J. Exploring the neurocognitive signature of poor set-shifting in anorexia and bulimia nervosa. J Psychiatr Res. 2010;44(14):964–970. | ||
Lopez C, Tchanturia K, Stahl D, Booth R, Holliday J, Treasure J. An examination of the concept of central coherence in women with anorexia nervosa. Int J Eat Disord. 2008;41(2):143–152. | ||
Adenzato M, Todisco P, Ardito RB. Social cognition in anorexia nervosa: evidence of preserved theory of mind and impaired emotional functioning. PLoS One. 2012;7(8):1–8. | ||
Green MF, Horan WP, Lee J. Social cognition in schizophrenia. Nat Rev Neurosci. 2015;16(10):620–631. | ||
Premack D, Woodruff G. Does the chimpanzee have a theory of mind? Behav Brain Sci. 1978;4(4):515–526. | ||
Baron-Cohen S, Wheelwright S, Hill J, Raste Y, Plumb I. The ‘Reading the Mind in the Eyes’ test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J Child Psychol Psychiatry. 2001;42(2):241–251. | ||
Harrison A, Sullivan S, Tchanturia K, Treasure J. Emotion recognition and regulation in anorexia nervosa. Clin Psychol Psychother. 2009;16(4):348–356. | ||
Harrison A, Sullivan S, Tchanturia K, Treasure J. Emotional functioning in eating disorders: attentional bias, emotion recognition and emotion regulation. Psychol Med. 2010;40(11):1887–1897. | ||
Tchanturia K, Happé F, Godley J, Treasure J, Bara-Carril N, Schmidt U. ‘Theory of mind’ in anorexia nervosa. Eur Eat Disord Rev. 2004;12(6):361–366. | ||
Tapajóz Pde Sampaio F, Soneira S, Aulicino A, Martese G, Iturry M, Allegri RF. Theory of mind and central coherence in eating disorders: two sides of the same coin? Psychiatry Res. 2013;210(3):1116–1122. | ||
Russell TA, Schmidt U, Doherty L, Young V, Tchanturia K. Aspects of social cognition in anorexia nervosa: affective and cognitive theory of mind. Psychiatry Res. 2009;168(3):181–185. | ||
Kanie A, Hagiya K, Ashida S, et al. New instrument for measuring multiple domain of social cognition: construct validity of the social cognition screening questionnaire (Japanese version). Psychiatry Clin Neurosci. 2014;68(9):701–711. | ||
Davenport E, Rushford N, Soon S, McDermott C. Dysfunctional metacognition and drive for thinness in typical and atypical anorexia nervosa. Int J Eat Disord. 2015;3:24. | ||
Olstad S, Solem S, Hjemdal O, Hagen R. Metacognition in eating disorders: comparison of women with eating disorders, self-reported history of eating disorders or psychiatric problems, and healthy controls. Eat Behav. 2015;16:17–22. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013. | ||
World Health Organization Expert Committee on Physical Status: the Use and Interpretation of Anthropometry. Physical Status: the Use and Interpretation of Anthropometry, Report of a WHO Expert Committee. WHO Technical Report Series 854. Geneva: World Health Organization; 1995. | ||
Matsuoka K, Uno M, Kasai K, Koyama K, Kim Y. Estimation of premorbid IQ in individuals with Alzheimer’s disease using Japanese ideographic script (Kanji) compound words: Japanese version of National Adult Reading Test. Psychiatry Clin Neurosci. 2006;60(3):332–339. | ||
Nelson H, Willison J. National Adult Reading Test (NART). 2nd ed. Windsor, UK: NFER-Nelson; 1991. | ||
Beck AT, Steer RA, Ball R, Ranieri W. Comparison of beck depression inventories-IA and-II in psychiatric outpatients. J Pers Assess. 1996;67(3):588–597. | ||
Kojima M, Furukawa TA, Takahashi H, Kawai M, Nagaya T, Tokudome S. Cross-cultural validation of the beck depression inventory-II in Japan. Psychiatry Res. 2002;110(3):291–299. | ||
Hidano N, Fukuhara M, Iwawaki M, Soga S, Spielberger C. Manual for the State-Trait Anxiety Inventory-Form JYZ. Tokyo: Jitsumkyoiku-shuppan Co., Ltd; 2000. Japanese. | ||
Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory (Form Y). Palo Alto, CA: Consulting Psychologists Press; 1983. | ||
Roberts DL, Fiszdon J, Tek C. Initial validity of the social cognition screening questionnaire (SCSQ). Schizophr Bull. 2011;37(Suppl 1):280. | ||
Field A. Discovering Statistics Using SPSS. 2nd ed. London: SAGE Publications; 2005. | ||
Happé F, Brownell H, Winner E. Acquired ‘theory of mind’ impairments following stroke. Cognition. 1999;70(3):211–240. | ||
Baron-Cohen S, O’Riordan M, Stone V, Jones R, Plaisted K. Recognition of faux pas by normally developing children and children with Asperger syndrome or high functioning autism. J Autism Dev Disord. 1999;29(5):407–417. | ||
Cooper MJ, Grocutt E, Deepak K, Bailey E. Metacognition in anorexia nervosa, dieting and non-dieting controls: a preliminary investigation. Br J Clin Psychol. 2007;46(1):113–117. | ||
Woolrich RA, Cooper MJ, Turner HM. Metacognition in patients with anorexia nervosa, dieting and non-dieting women: a preliminary study. Eur Eat Disord Rev. 2008;16(1):11–20. | ||
Arbel R, Koren D, Klein E, Latzer Y. The neurocognitive basis of insight into illness in anorexia nervosa: a pilot metacognitive study. Psychiatry Res. 2013;209(13):604–610. | ||
Flavell JH. Metacognition and cognitive monitoring: a new area of psychological inquiry. Am Psychol. 1979;34(10):906–911. | ||
Konstantakopoulos G, Varsou G, Dikeos D, et al. Delusionality of body image beliefs in eating disorders. Psychiatry Res. 2012;30;200(2–3):482–488. | ||
Steinglass JE, Eisen JL, Attia E, Mayer L, Walsh BT. Is anorexia nervosa a delusional disorder? An assessment of eating beliefs in anorexia nervosa. J Psychiatr Pract. 2007;13(2):65–71. | ||
Oltra-Cucarella J, Espert R, Rojo L, Jacas C, Guillen V, Moreno S. Neuropsychological impairments in anorexia nervosa. a spanish sample pilot study. Appl Neuropsychol Adult. 2014;21(3):161–175. | ||
Dapelo MM, Surguladze S, Morris R, Tchanturia K. Emotion recognition in blended facial expressions in women with anorexia Nervosa. Eur Eat Disord Rev. 2016;24(1):34–42. | ||
Young AW, Perret DI, Calder AJ, Sprengelmeyer R, Ekman P. Facial Expressions of Emotions: Stimuli and Tests (FEEST). Bury St Edmunds: Thames Valley Test Company; 2002. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.