")
Back to Journals » Journal of Pain Research » Volume 12
Impact of water therapy on pain management in patients with fibromyalgia: current perspectives
Authors Zamunér AR, Andrade CP , Arca EA , Avila MA
Received 15 August 2018
Accepted for publication 20 May 2019
Published 3 July 2019 Volume 2019:12 Pages 1971—2007
DOI https://doi.org/10.2147/JPR.S161494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Erica Wegrzyn
Antonio Roberto Zamunér,1 Carolina Pieroni Andrade,2 Eduardo Aguilar Arca,3 Mariana Arias Avila4
1Departamento de Kinesiología, Universidad Católica del Maule, Talca, Maule, Chile; 2Secretaria de Saúde do Município de Guareí, Guareí, São Paulo, Brasil; 3Departamento de Fisioterapia, Universidade do Sagrado Coração, Bauru, São Paulo, Brasil; 4Departamento de Fisioterapia e Programa de Pós-Graduação em Fisioterapia, Universidade Federal de São Carlos, São Carlos, São Paulo, Brasil
Abstract: Exercise-related interventions have been recommended as one of the main components in the management of fibromyalgia syndrome (FMS). Water therapy, which combines water’s physical properties and exercise benefits, has proven effective in improving the clinical symptoms of FMS, especially pain, considered the hallmark of this syndrome. However, to our knowledge, the mechanisms underlying water therapy effects on pain are still scarcely explored in the literature. Therefore, this narrative review aimed to present the current perspectives on water therapy and the physiological basis for the mechanisms supporting its use for pain management in patients with FMS. Furthermore, the effects of water therapy on the musculoskeletal, neuromuscular, cardiovascular, respiratory, and neuroendocrine systems and inflammation are also addressed. Taking into account the aspects reviewed herein, water therapy is recommended as a nonpharmacologic therapeutic approach in the management of FMS patients, improving pain, fatigue, and quality of life. Future studies should focus on clarifying whether mechanisms and long-lasting effects are superior to other types of nonpharmacological interventions, as well as the economic and societal impacts that this intervention may present.
Keywords: hydrotherapy, exercise, pain management, chronic pain, physical therapy, aquatic therapy
Introduction
Fibromyalgia syndrome (FMS) is a chronic syndrome characterized by widespread musculoskeletal pain, chronic fatigue, and nonrestorative sleep, among other symptoms.1,2 It can be considered a clinical and pathological heterogeneous syndrome, thus requiring individualized and patient-tailored treatment.3 FMS is one of the most common conditions seen in the general population and outpatient rheumatology practice.1
The burden of FMS is substantial and comparable to some other chronic disease such as osteoarthritis, rheumatoid arthritis, diabetes, and hypertension.4–6 FMS patients incur direct costs approximately equal to rheumatoid arthritis patients, but visit more emergency physicians, physicians, and physical therapists than rheumatoid arthritis patients.7 Several studies have evaluated the economic burden of FMS, including direct and indirect costs of the disease.6,8–15 These costs include the large number of medical consultations and medication, and the health system and societal expenses of disability from work, accounting for more than three-quarters of total FMS-related costs.16 Hence, a cost-effective treatment, or at least one that helps decrease the economic and societal burden, is more than welcome.17
Recent recommendations for the management of FMS have suggested the use of pharmacological and nonpharmacological interventions,18 with exercise being recognized as one of the most important components of FMS treatment.19–22 Moreover, aerobic and strengthening exercises were the only therapeutic approach with a “strong for” recommendation by the European League Against Rheumatism,18 due to its positive effects on pain, physical function, and well-being, along with its availability, relatively low cost, and low risk.23–26
Among different types and modalities of exercises for FMS, water therapy can be considered one of the most known and doctor-recommended interventions, as it combines water physical properties and exercise benefits.22,27 Indeed, several studies have investigated the effects of water therapy as a strategy in the management of FMS, reporting improvements in well-being, fitness, and symptoms, especially pain.28–32 However, to our knowledge, mechanisms underlying the water therapy effects on pain are still scarce. Therefore, the aim of this narrative review is to present the current perspectives of water therapy and the physiological basis for the mechanisms supporting its use for pain management in patients with FMS.
Clinical implication of water physics
Aquatic exercise describes an environment for structured activity rather than a type of exercise, as water's physical properties and the physiological effects of immersion turn this environment into a unique one.33 According to the Chartered Society of Physiotherapists, water therapy or aquatic exercise refers to the use of water properties to design a therapy program aimed at improving function.27,34 Indeed, there is evidence27 that aquatic exercise is able to reduce the burden of musculoskeletal illnesses, which rely, basically, on the therapeutic effects achieved by the summation of physiological effects of immersion and principles of hydrodynamic exercises.35 The four most important water physics principles are buoyancy, resistance (drag forces), hydrostatic pressure, and thermal conduction. Definitions of the water physics principles, their properties, and implications for clinical use are summarized in Table 1.27,27,31,35–47
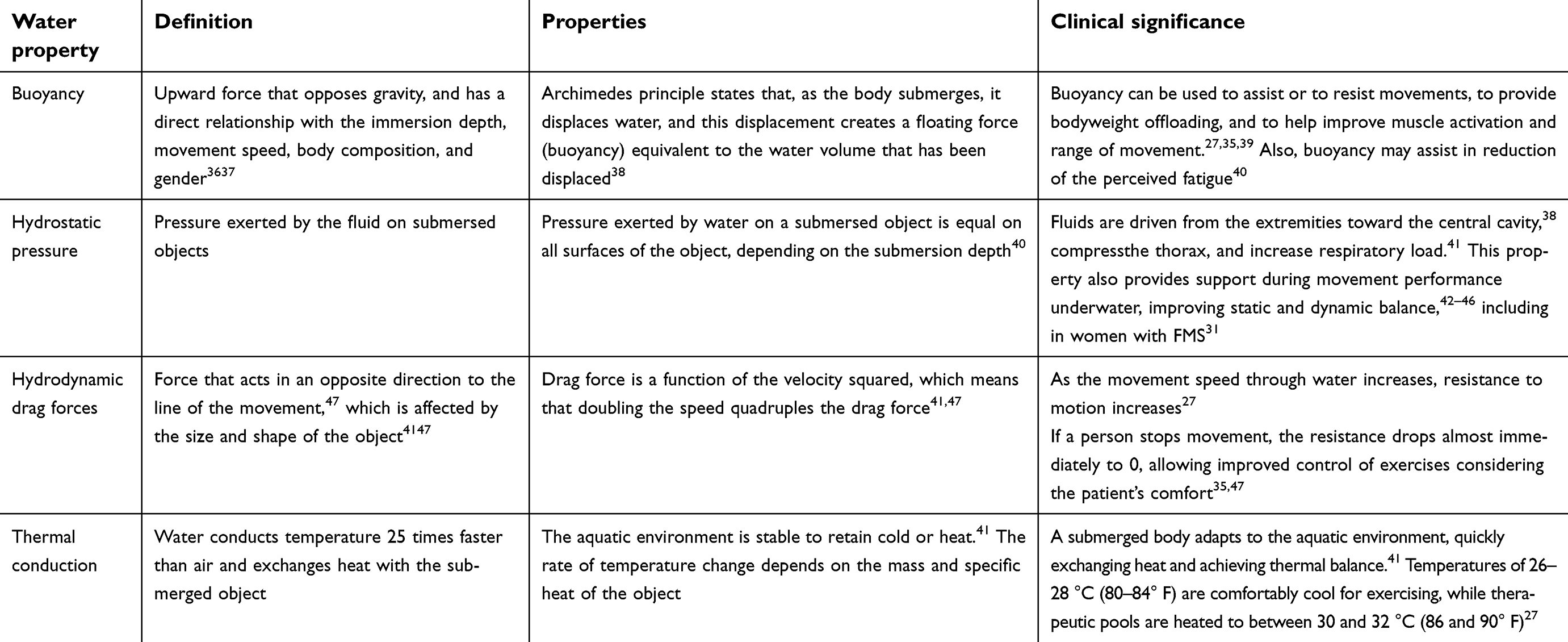 |
Table 1 Summary of water physics principles |
Water therapy physiological effects and its relationship with pain
Several studies have reported beneficial effects of aquatic therapy on several conditions,33,39,48–50 among which stands FMS.27,28,32,51,52 Indeed, guidelines for the management of FMS18 have recommended water therapy mainly due to its analgesic effects and improvement in quality of life.27,28,32,51,52
Although this narrative review does not intend to perform a systematic review on the theme, Table 2 summarizes the clinical trials assessing the effects of hydrotherapy on FMS symptoms, especially pain. We carried out a search of the following databases: MEDLINE/PubMed, Scopus, Web of Science, SciELO, CINAHL, LILACS, ScienceDirect, and Springer. The following keywords were used: “aquatic exercise”, “aquatic training”, “balneotherapy”, “fibromyalgia”, “fibromyalgia syndrome”, “fibromyalgic patients”, “hydrotherapy”, and “pool-based exercises”. Two authors independently extracted data from all of the trials and all discrepancies or disagreements were resolved by consensus.
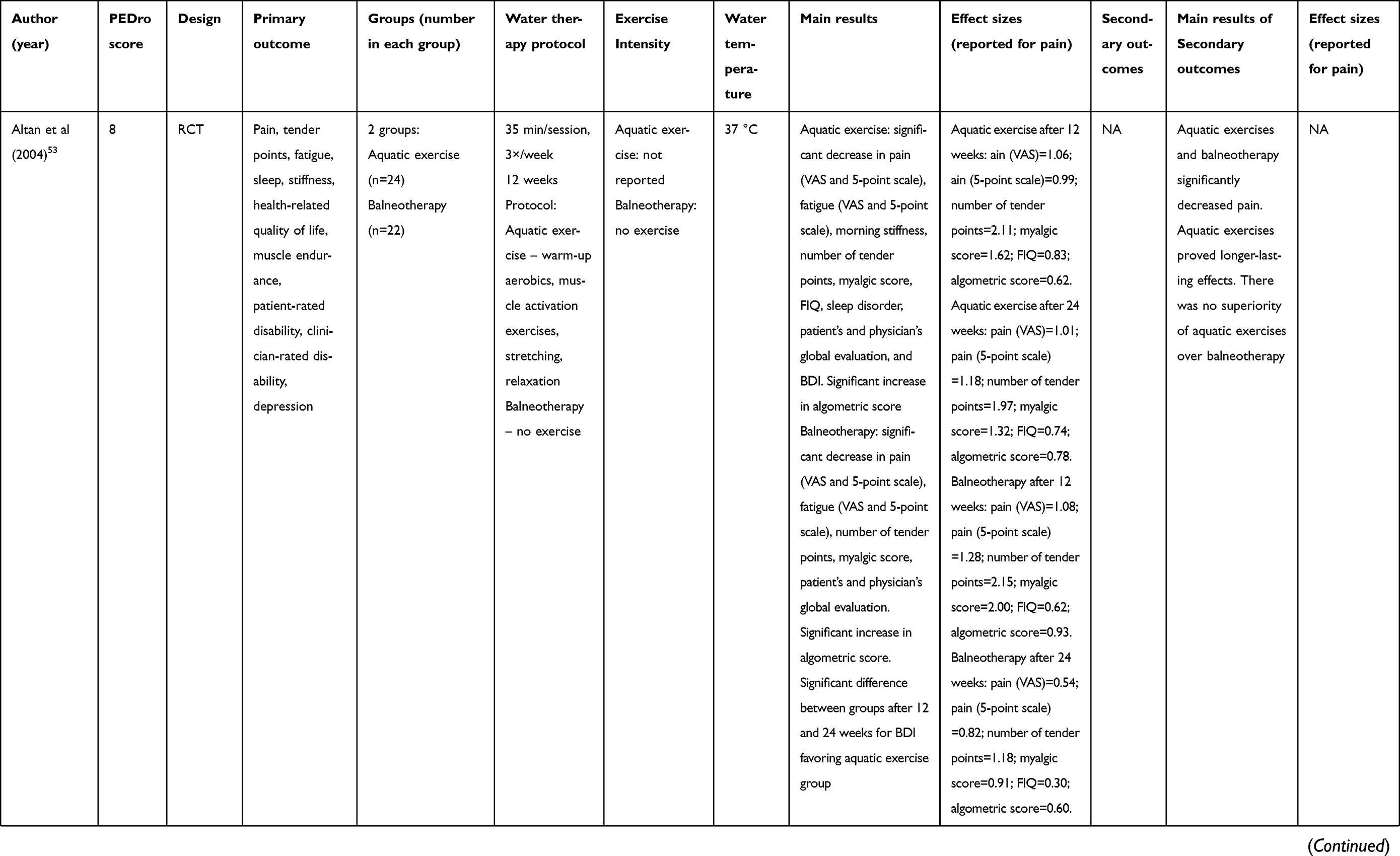 | 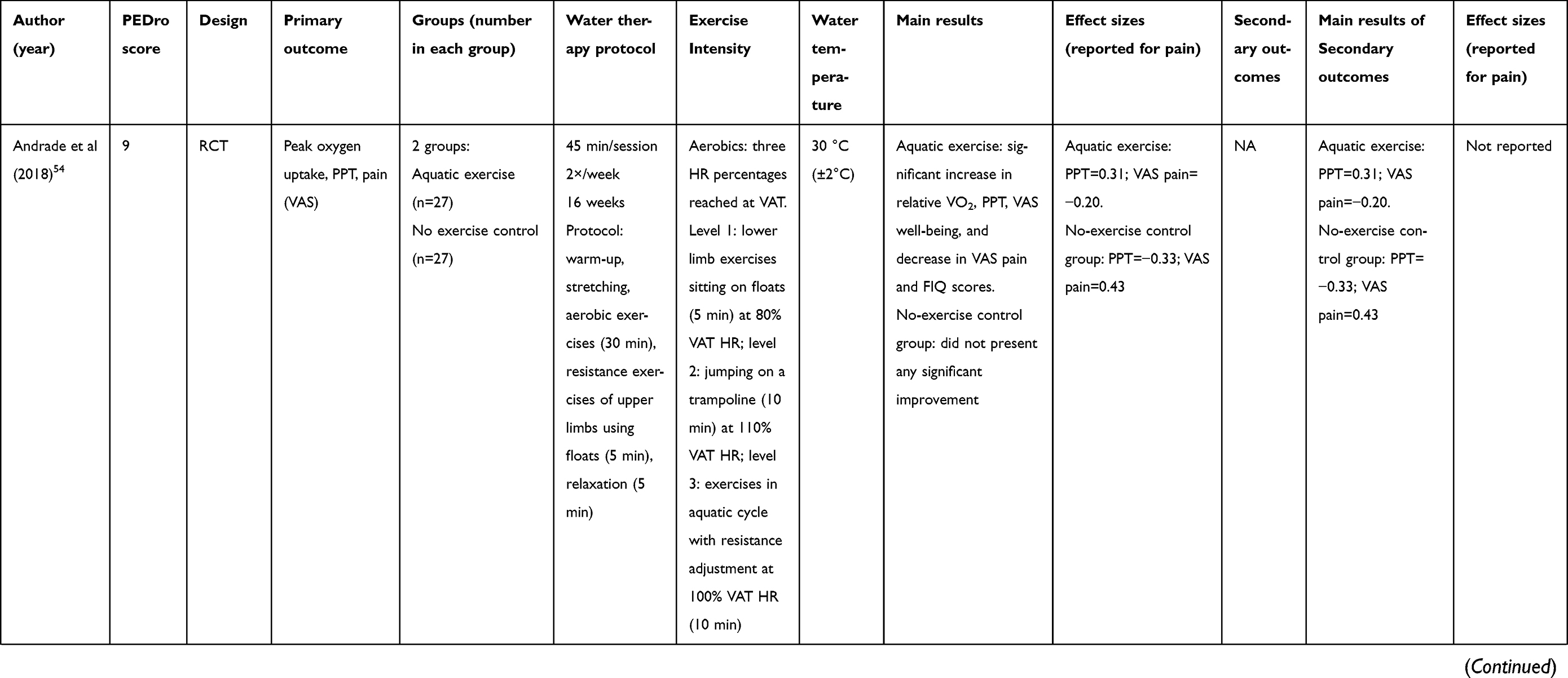 | 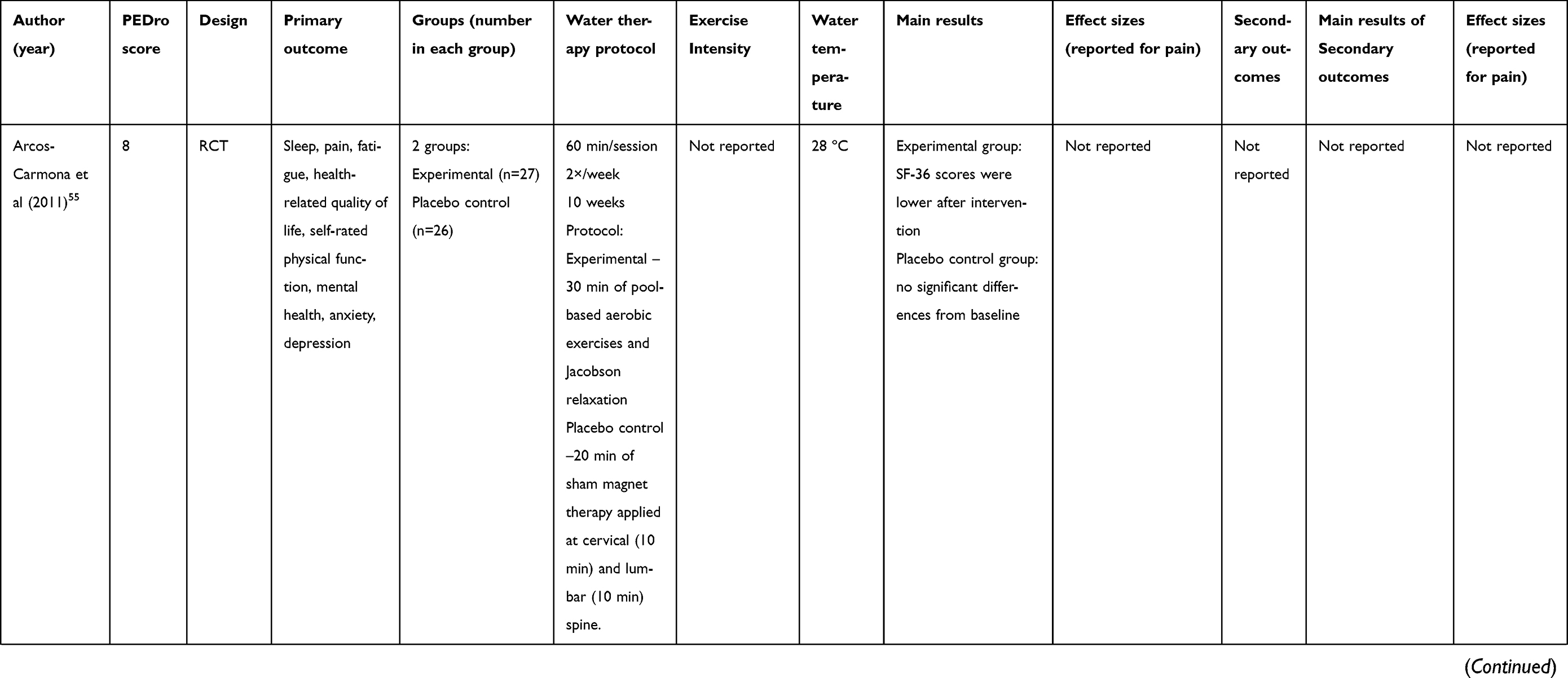 | 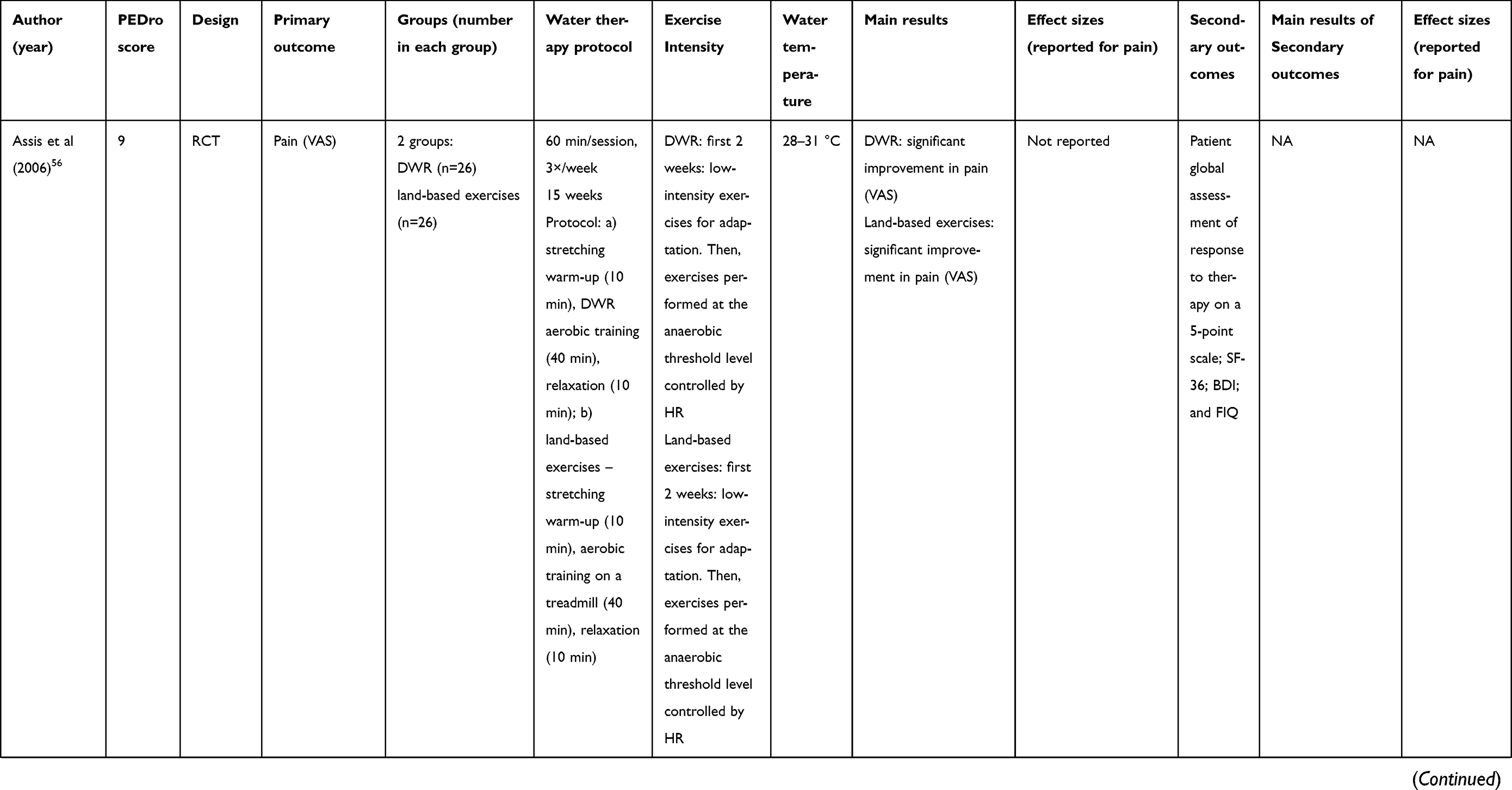 | 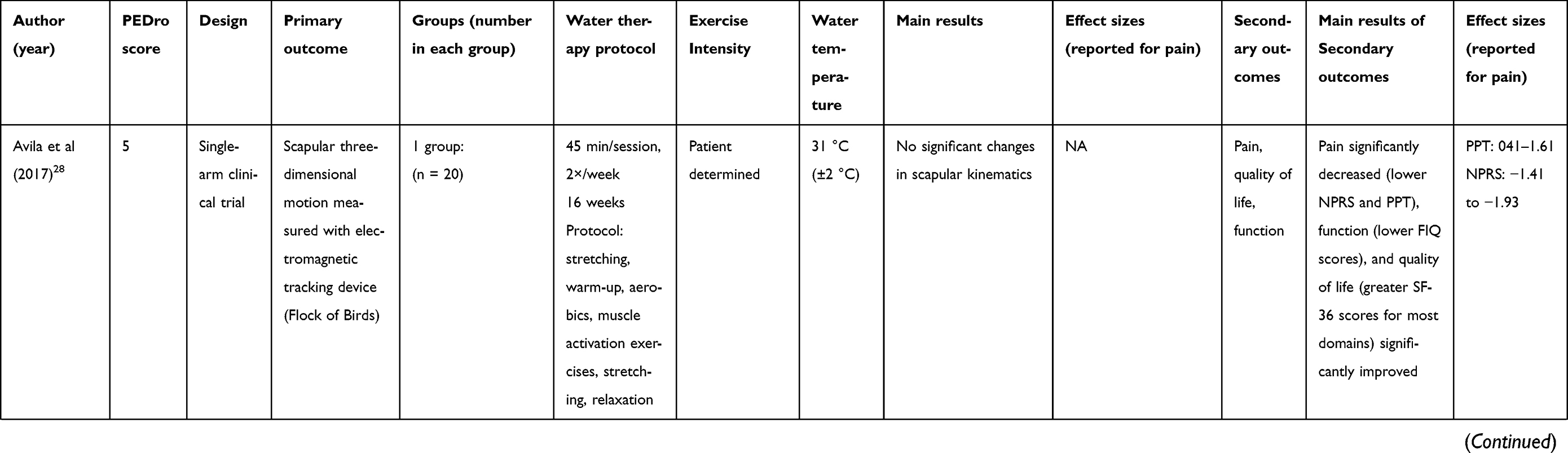 | 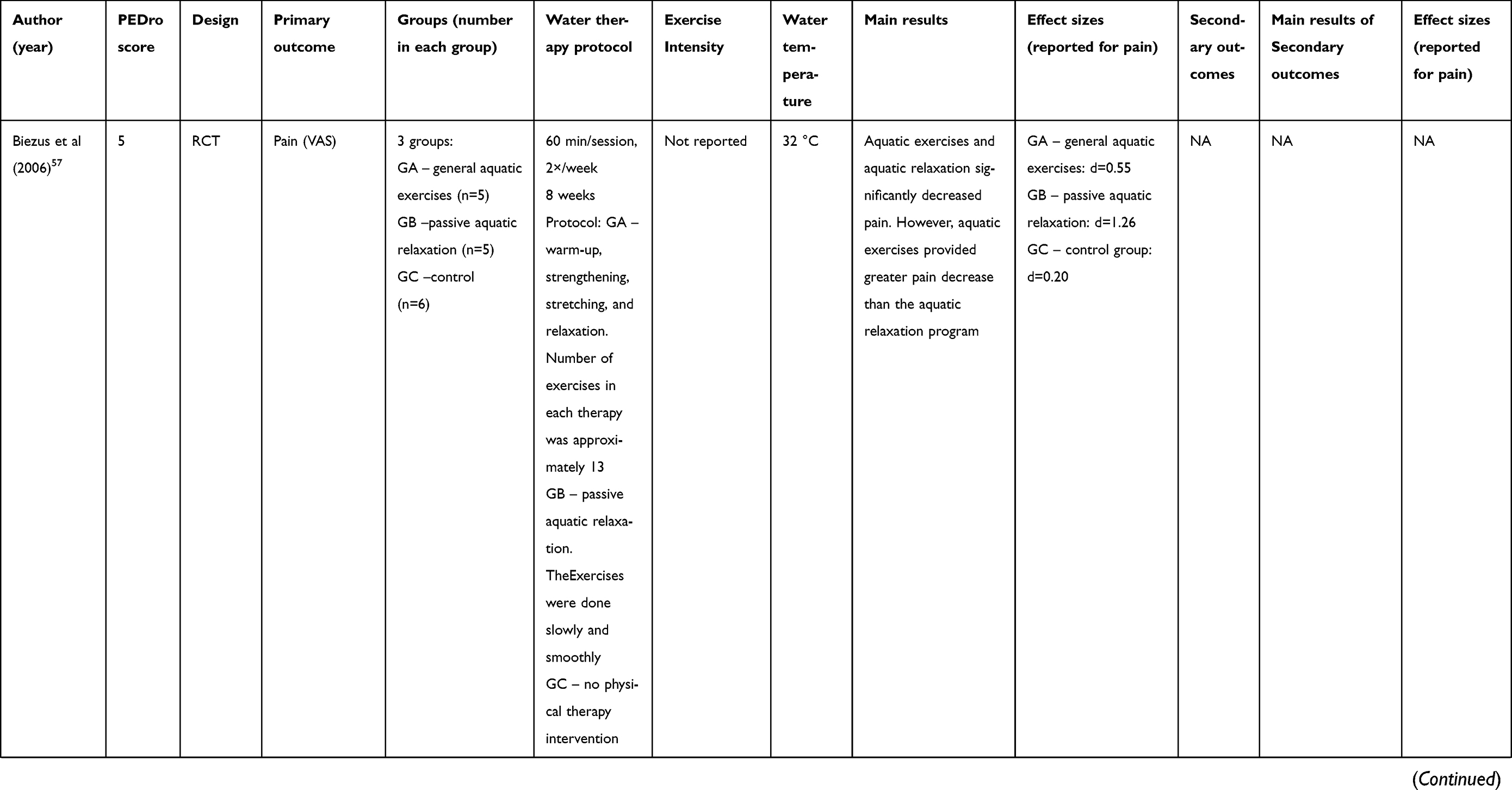 | 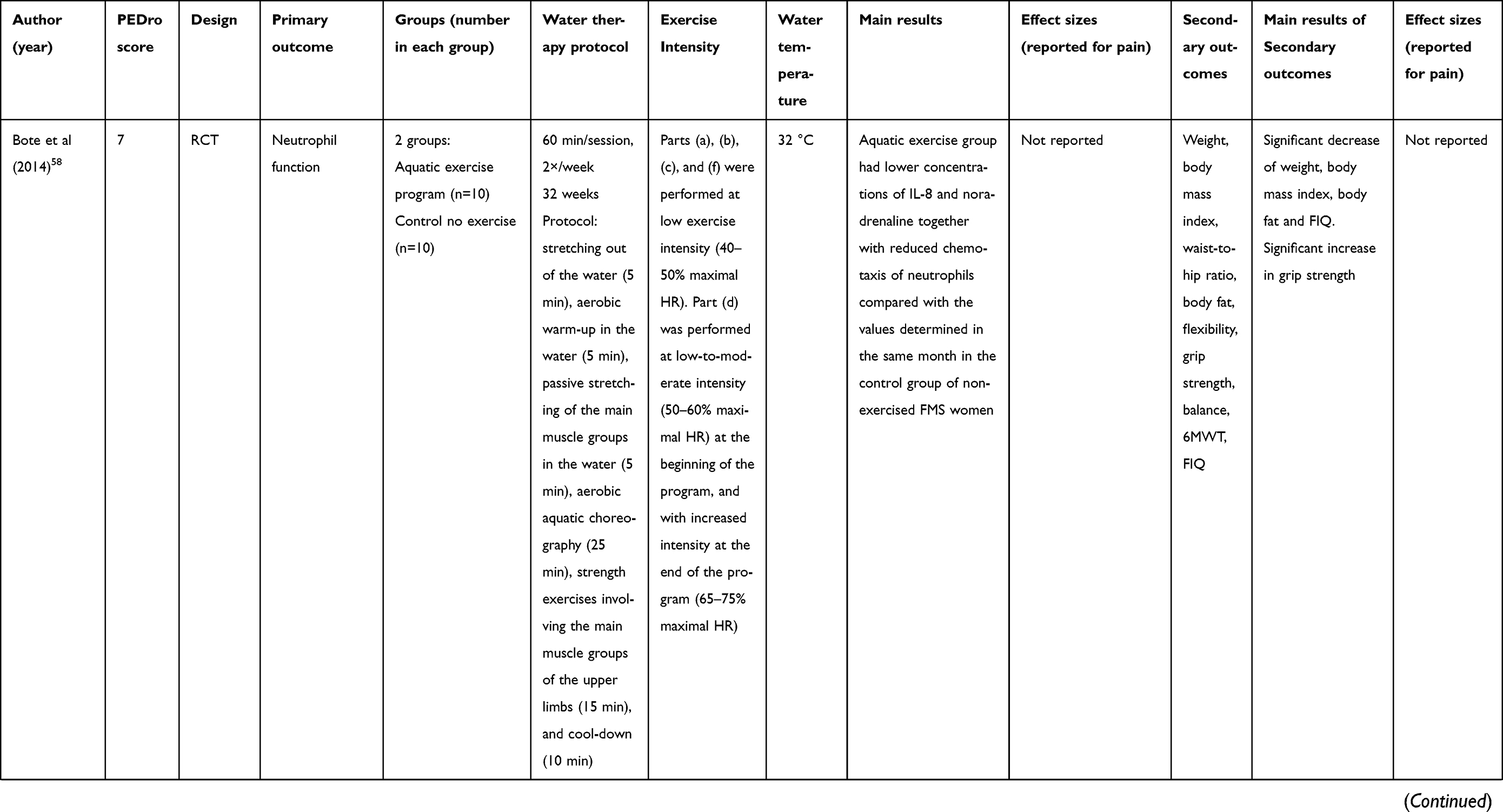 | 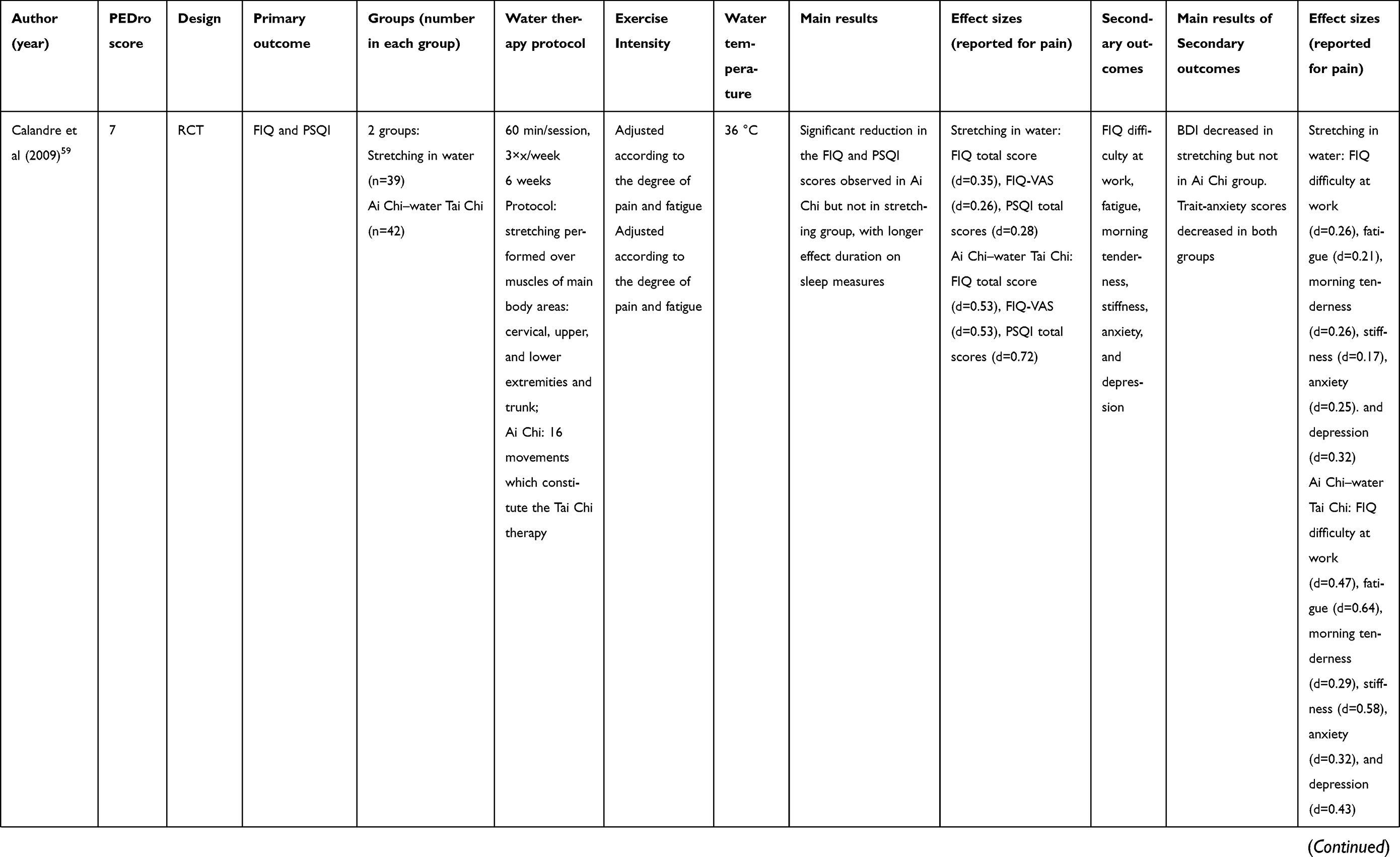 | 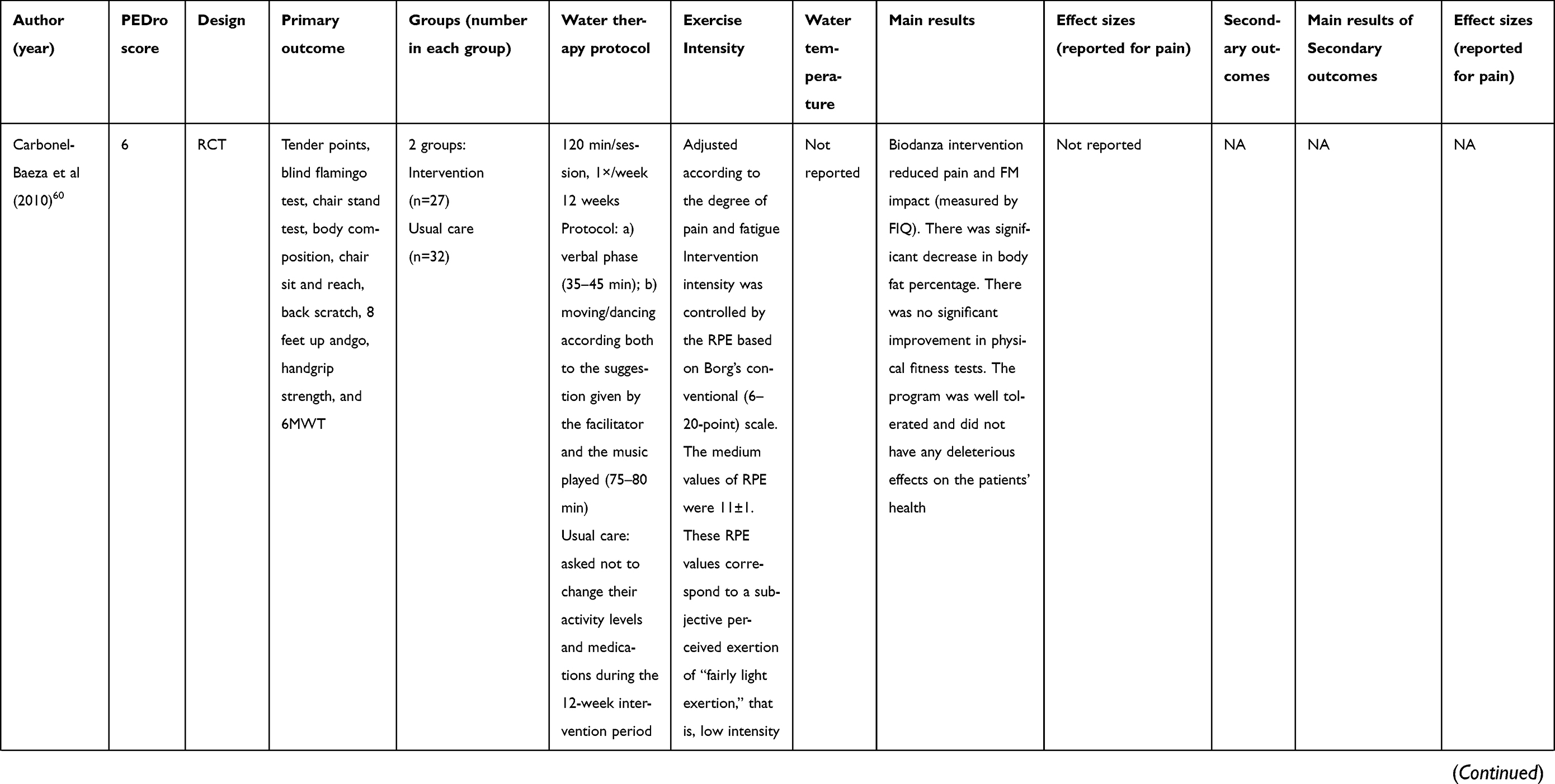 | 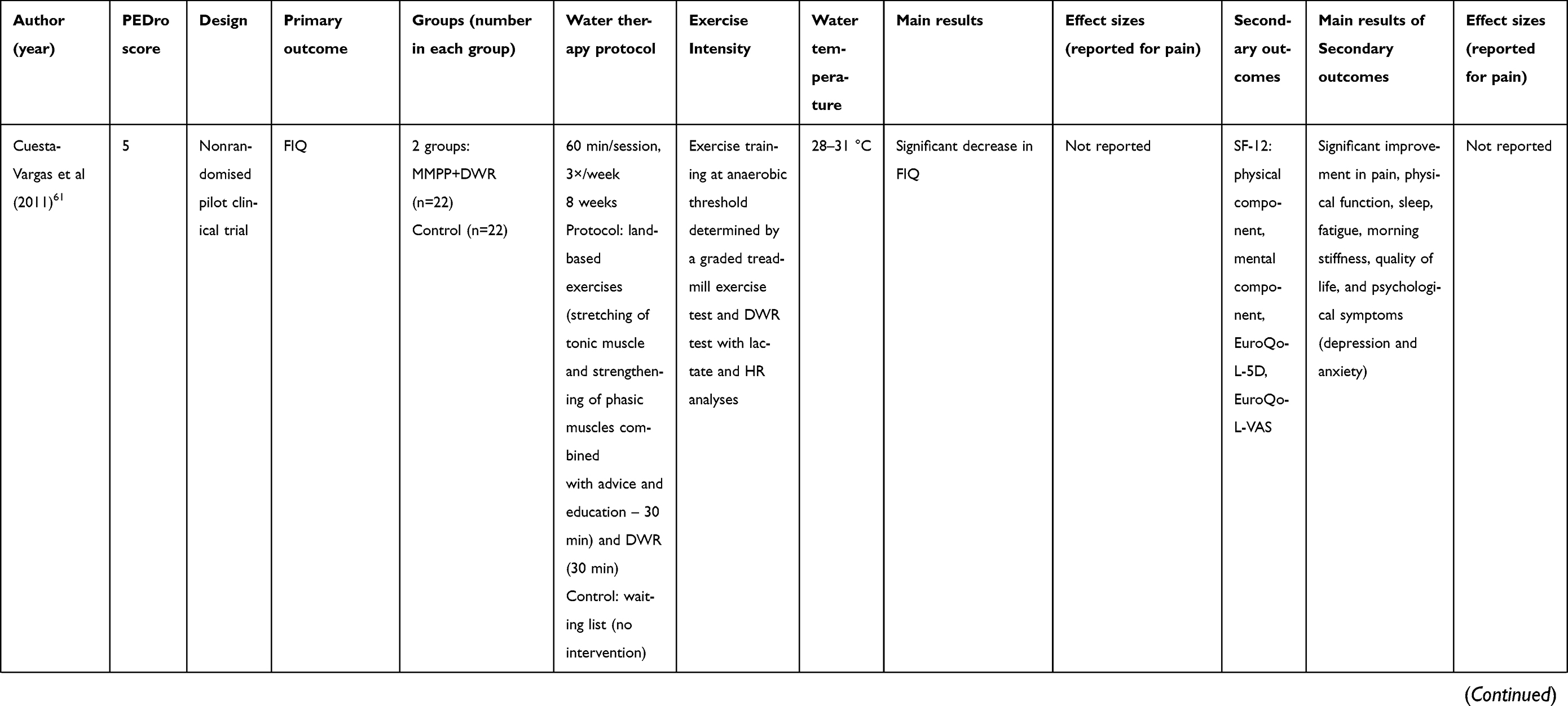 | 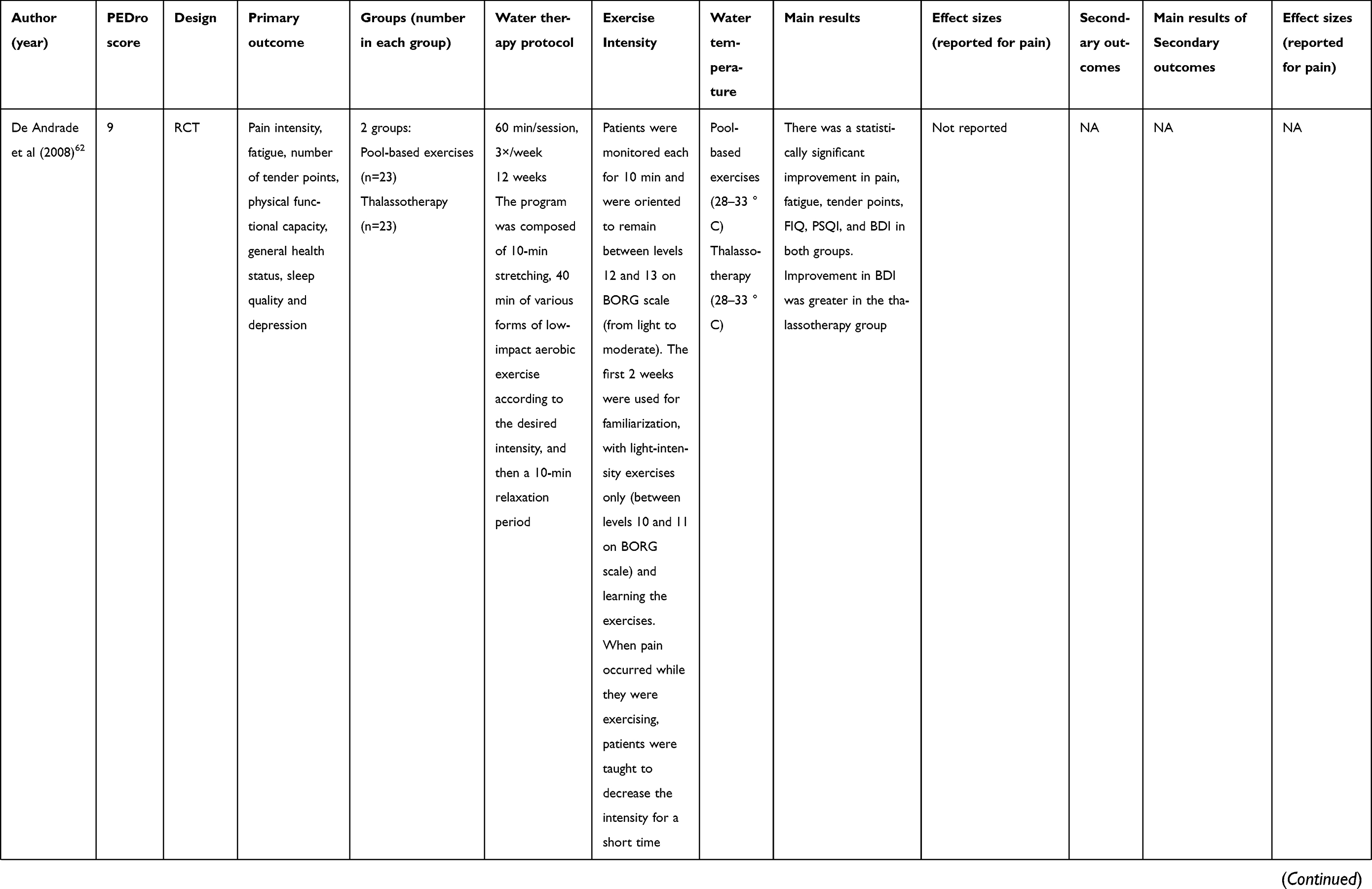 | 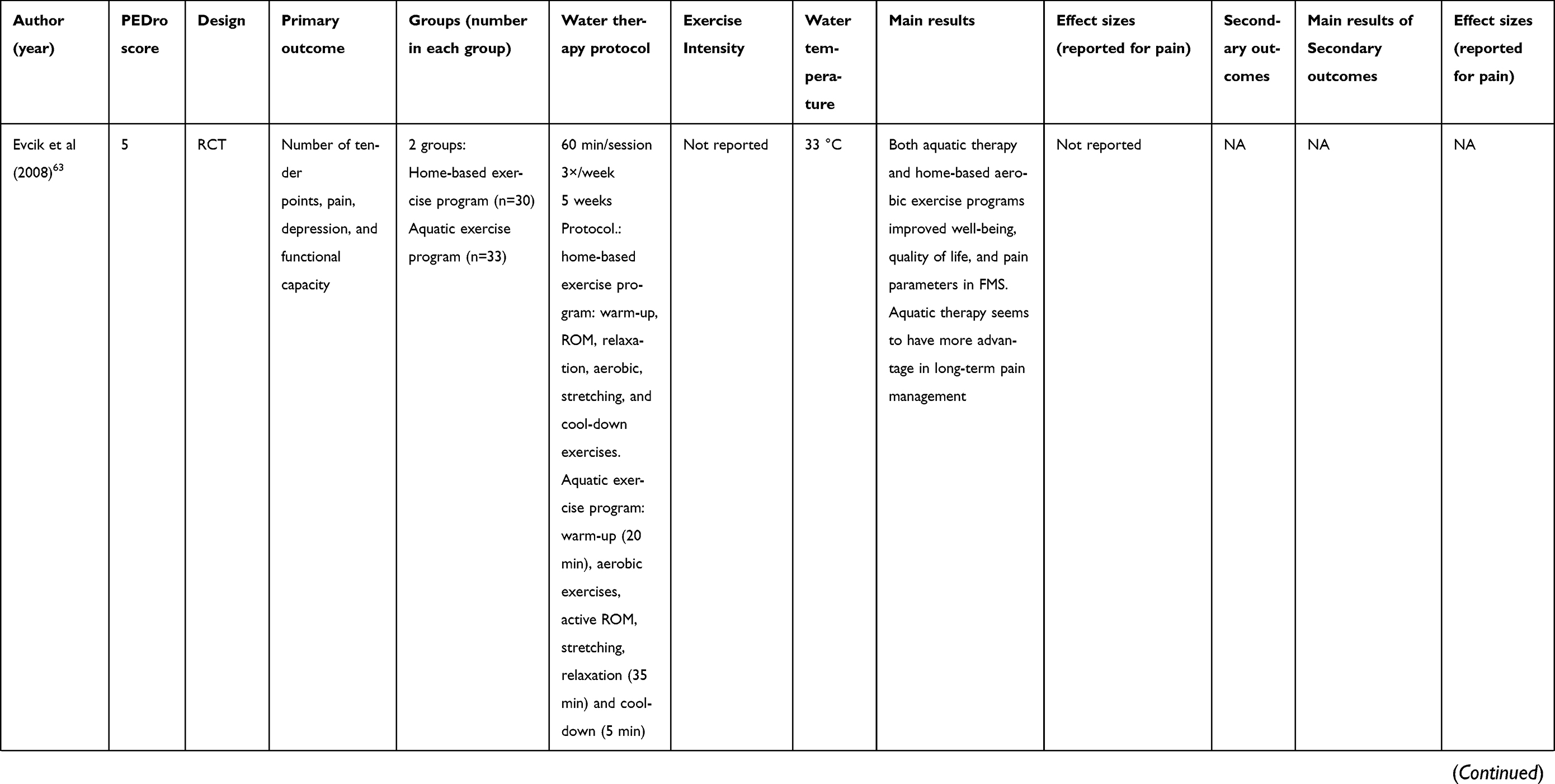 | 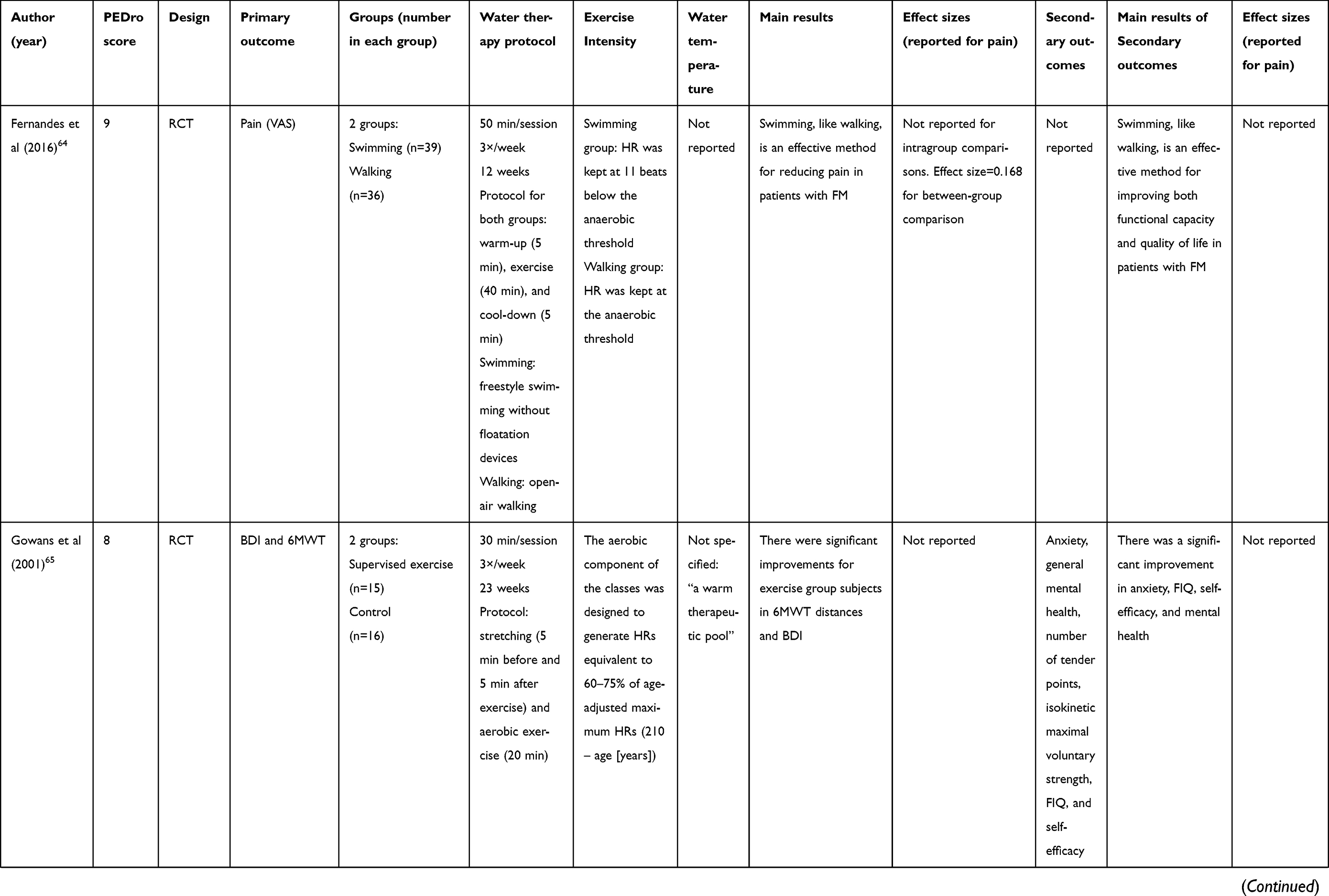 | 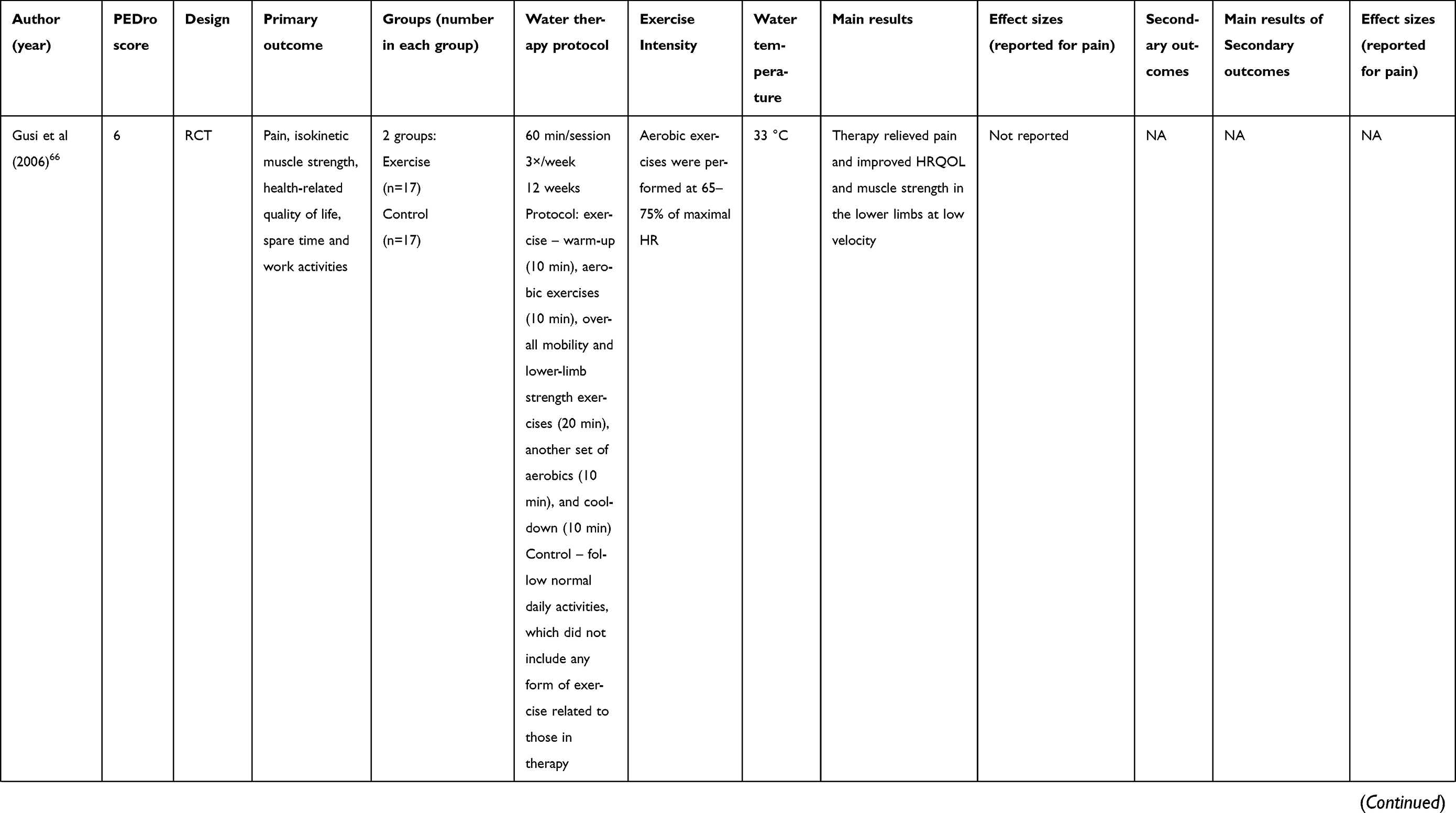 | 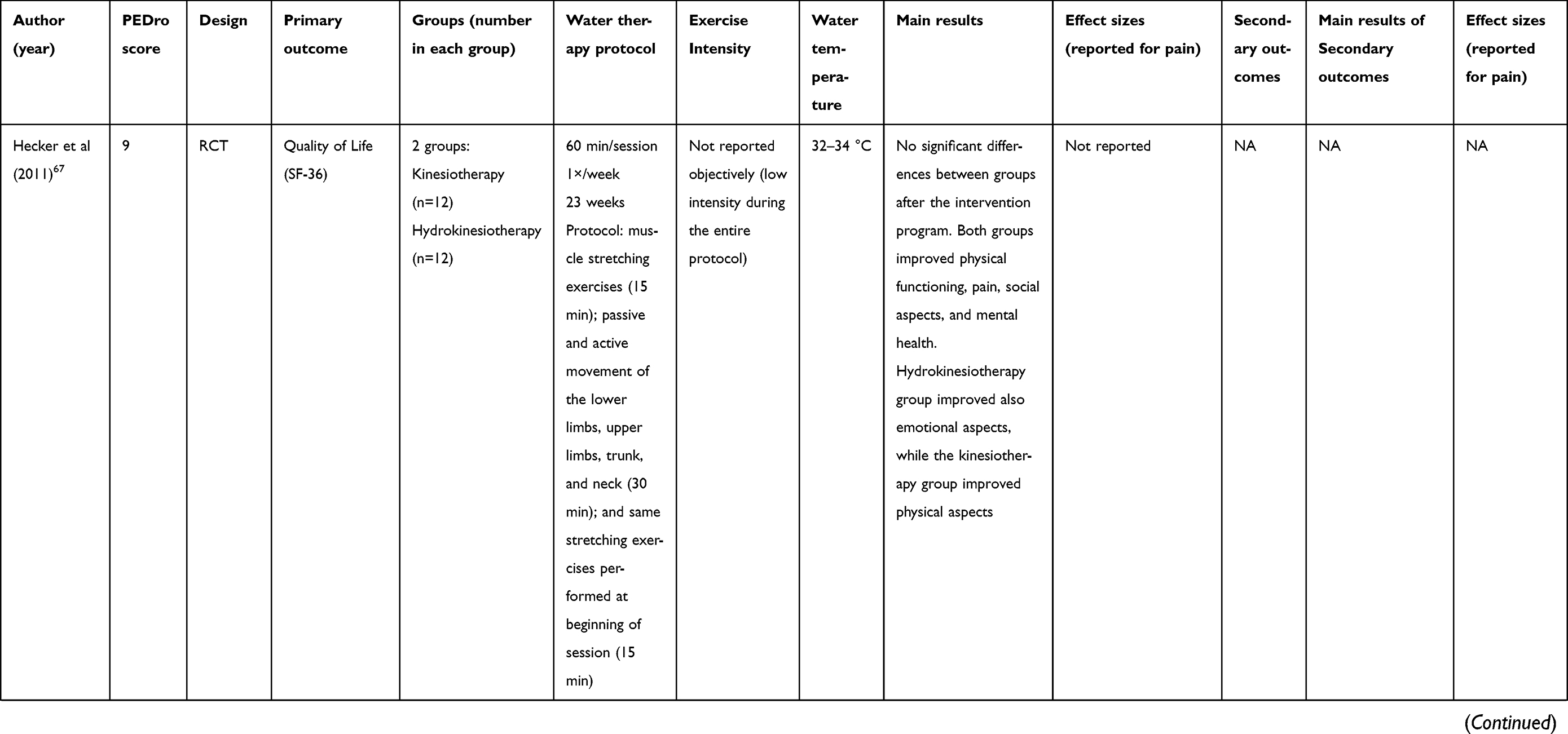 | 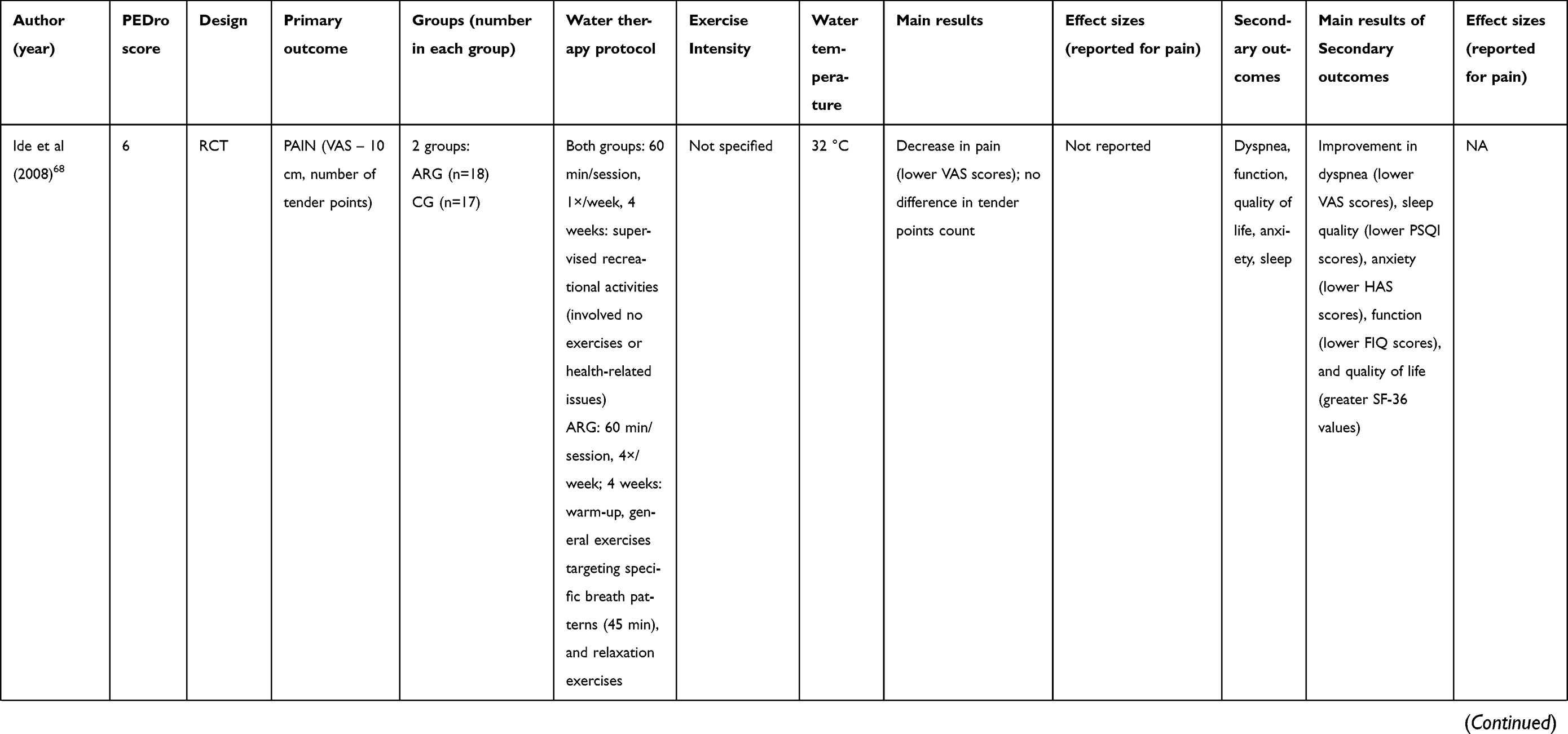 | 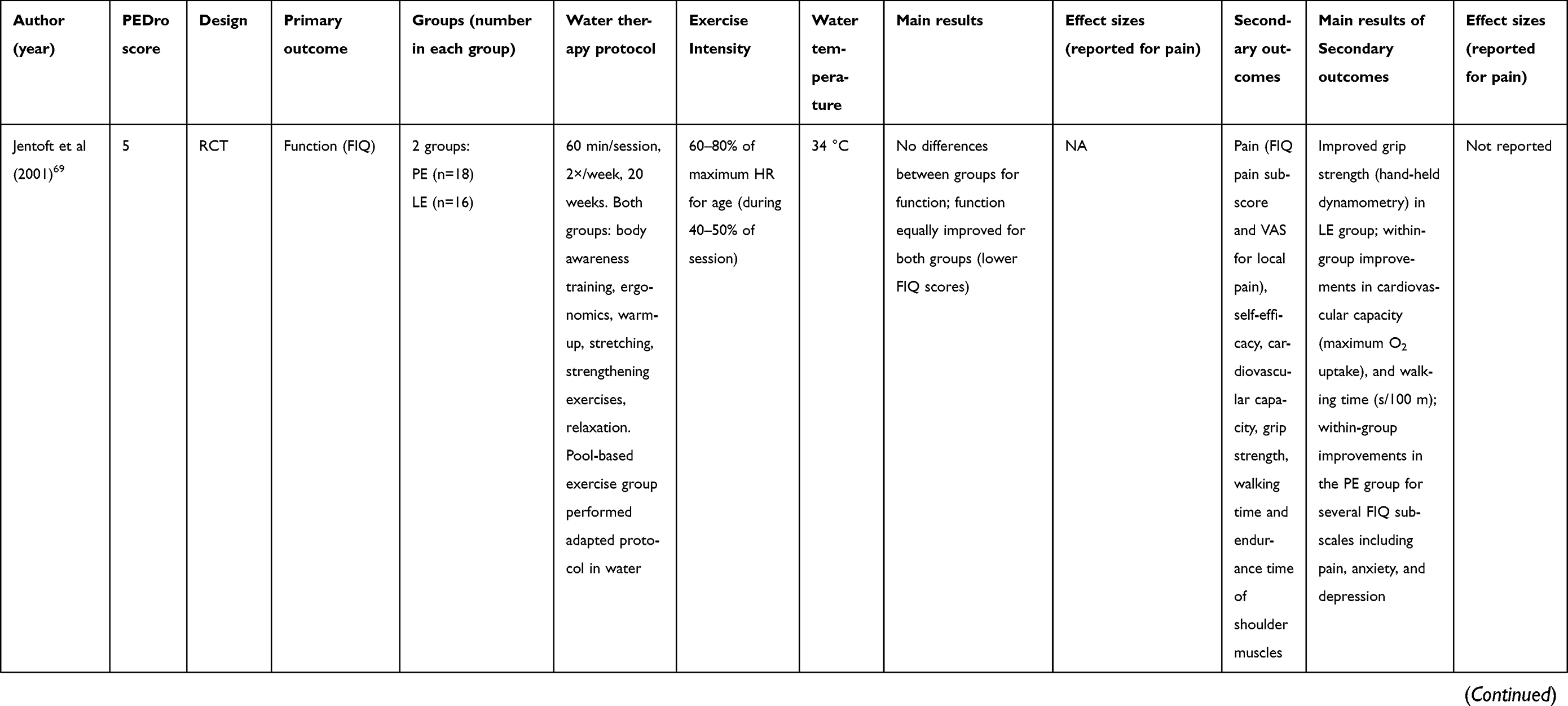 | 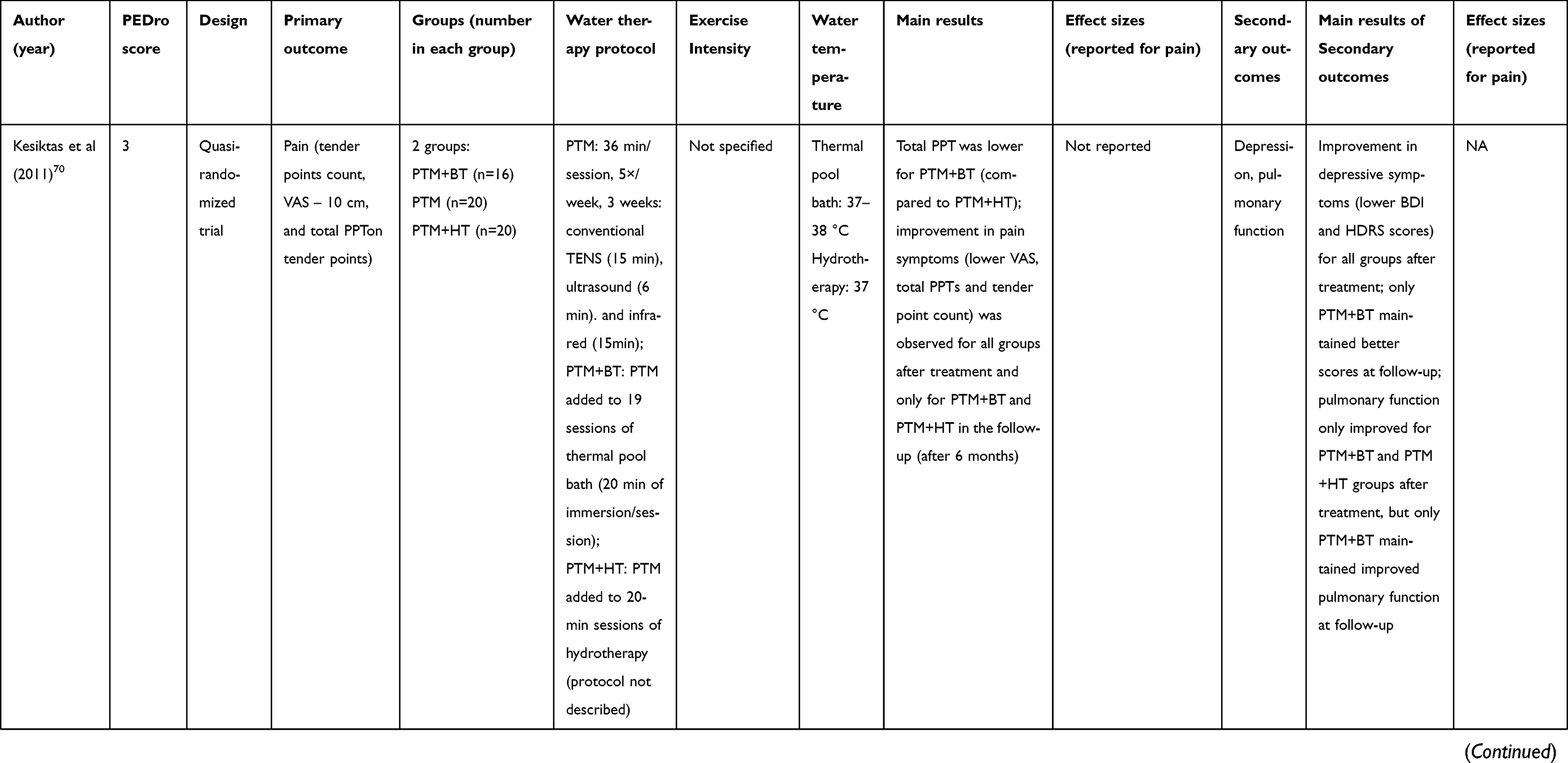 | 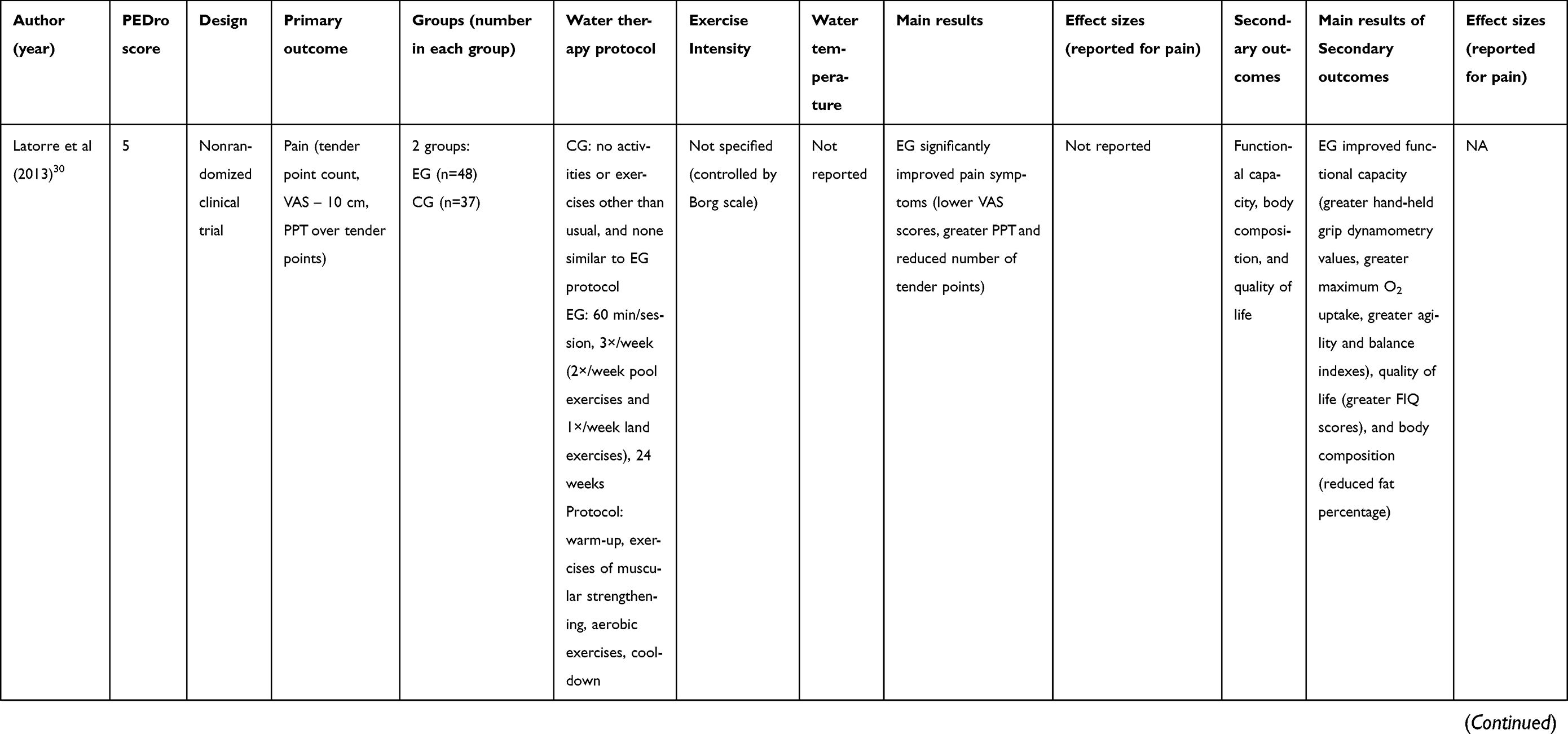 | 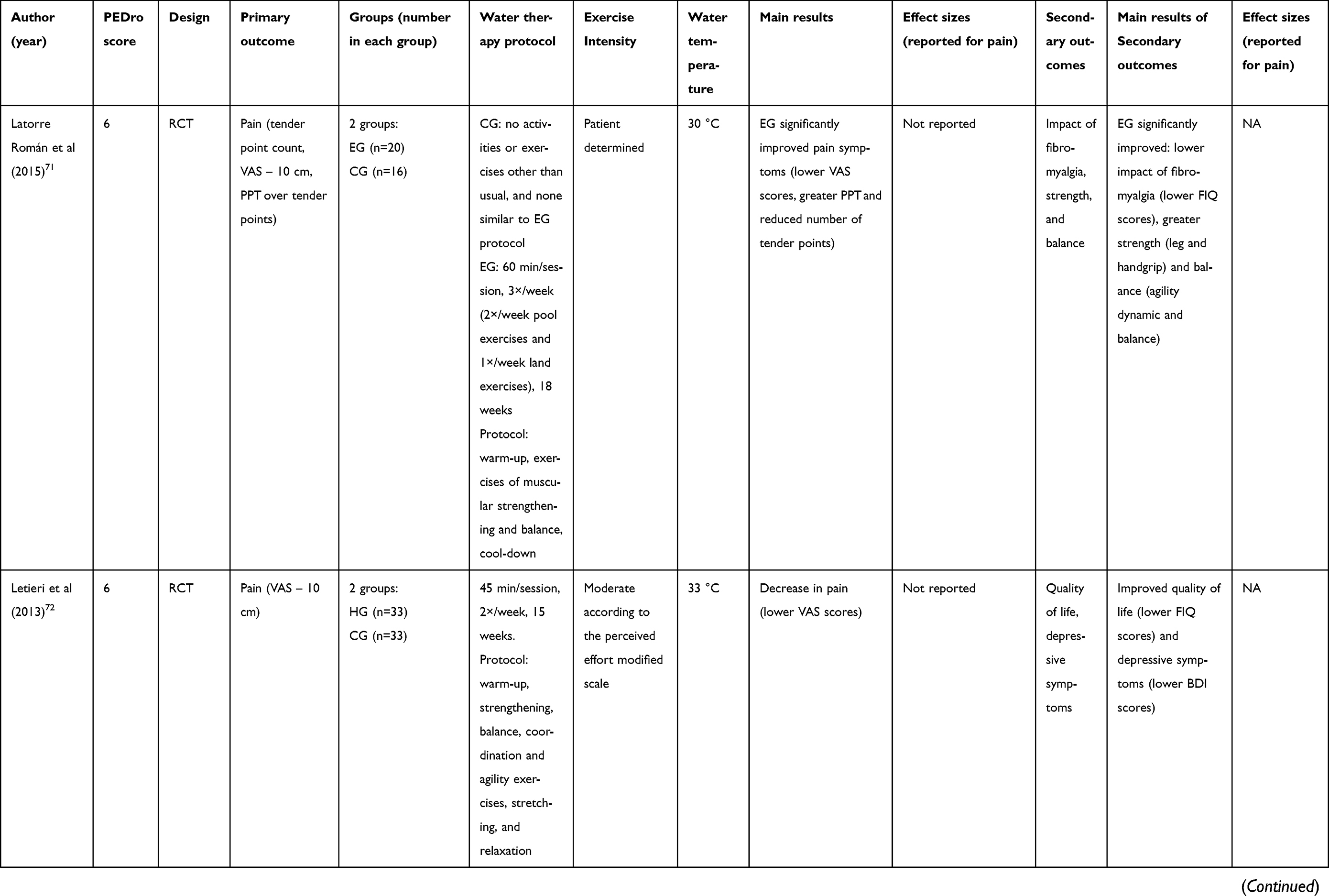 | 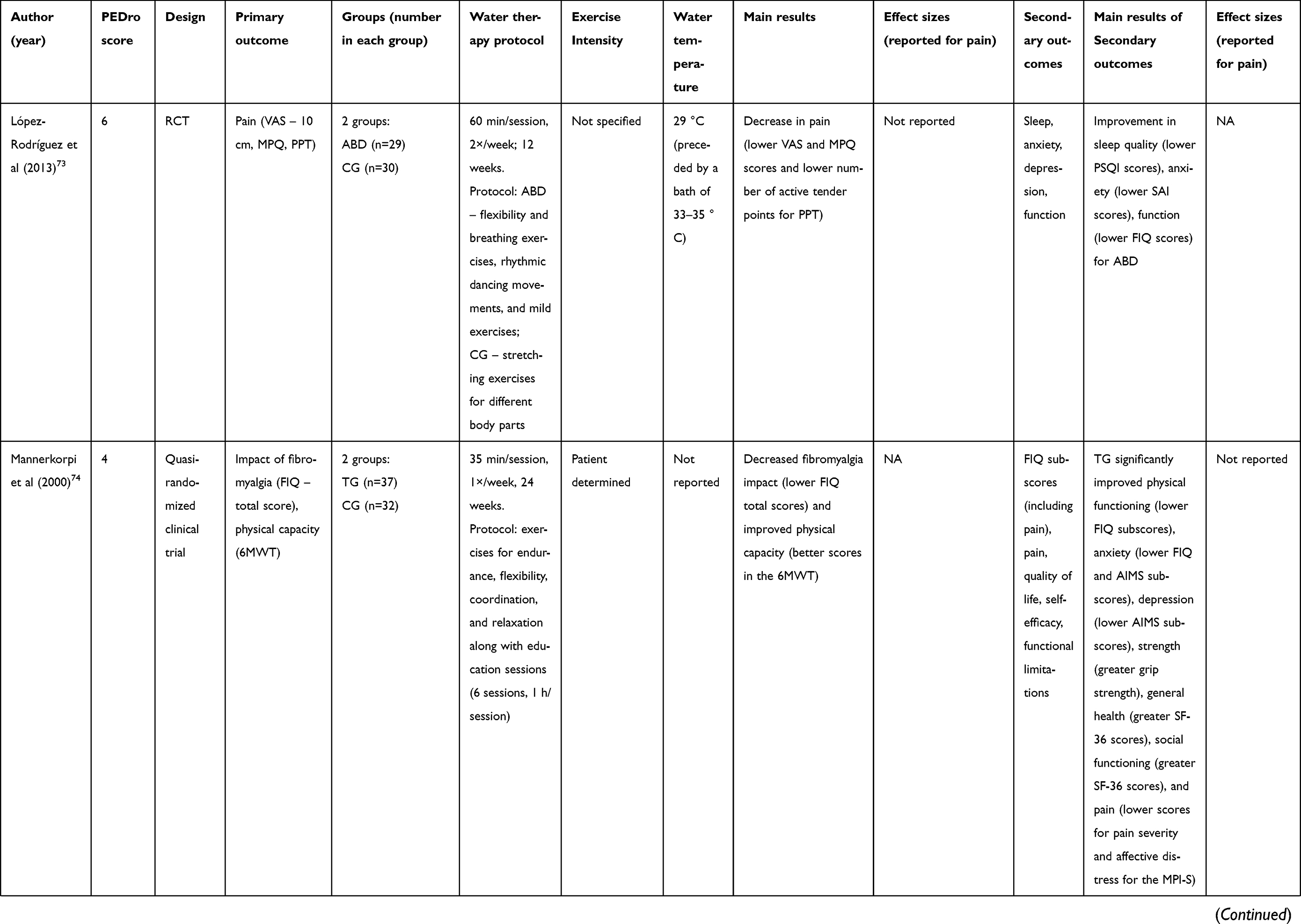 | 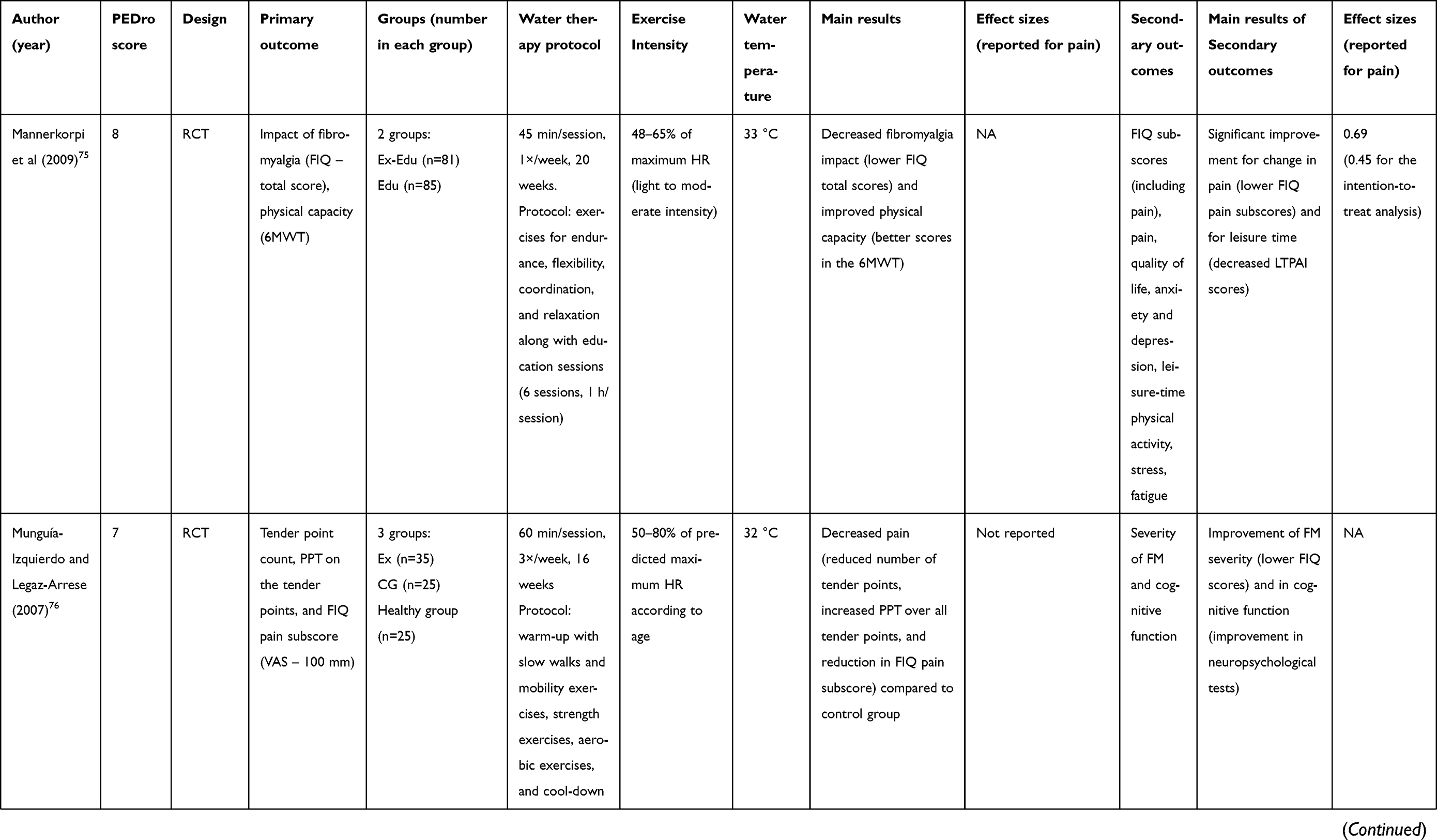 | 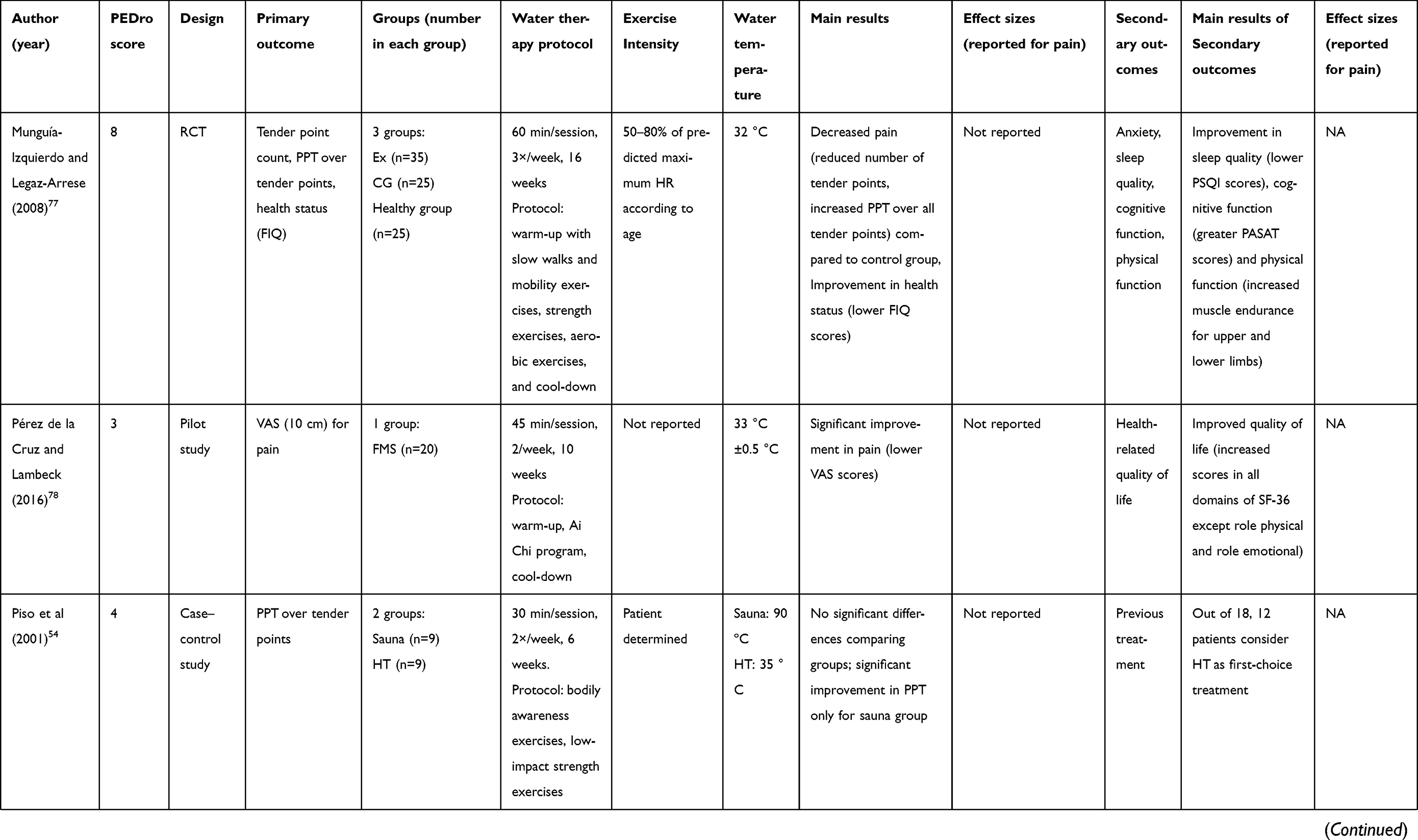 | 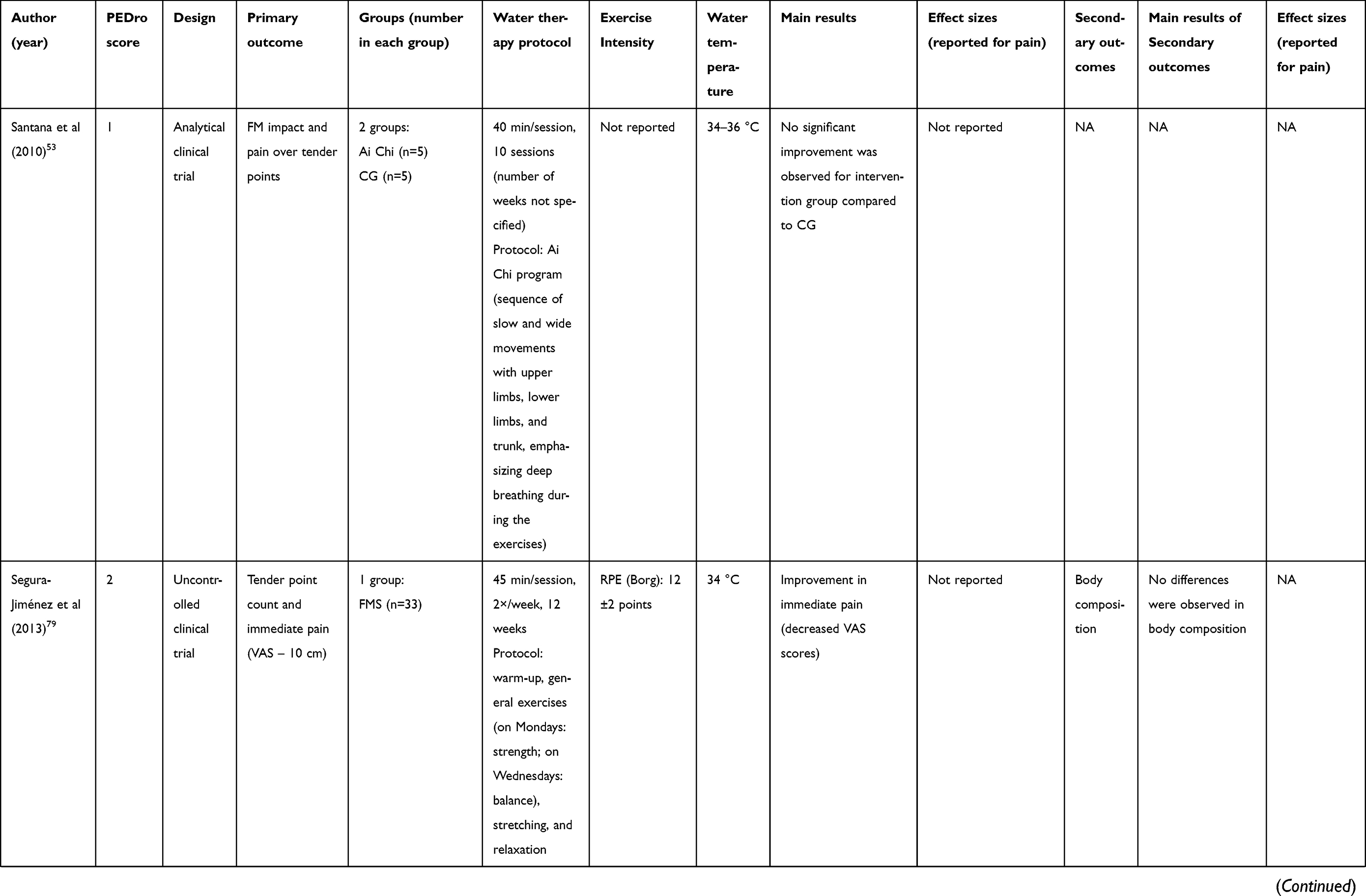 | 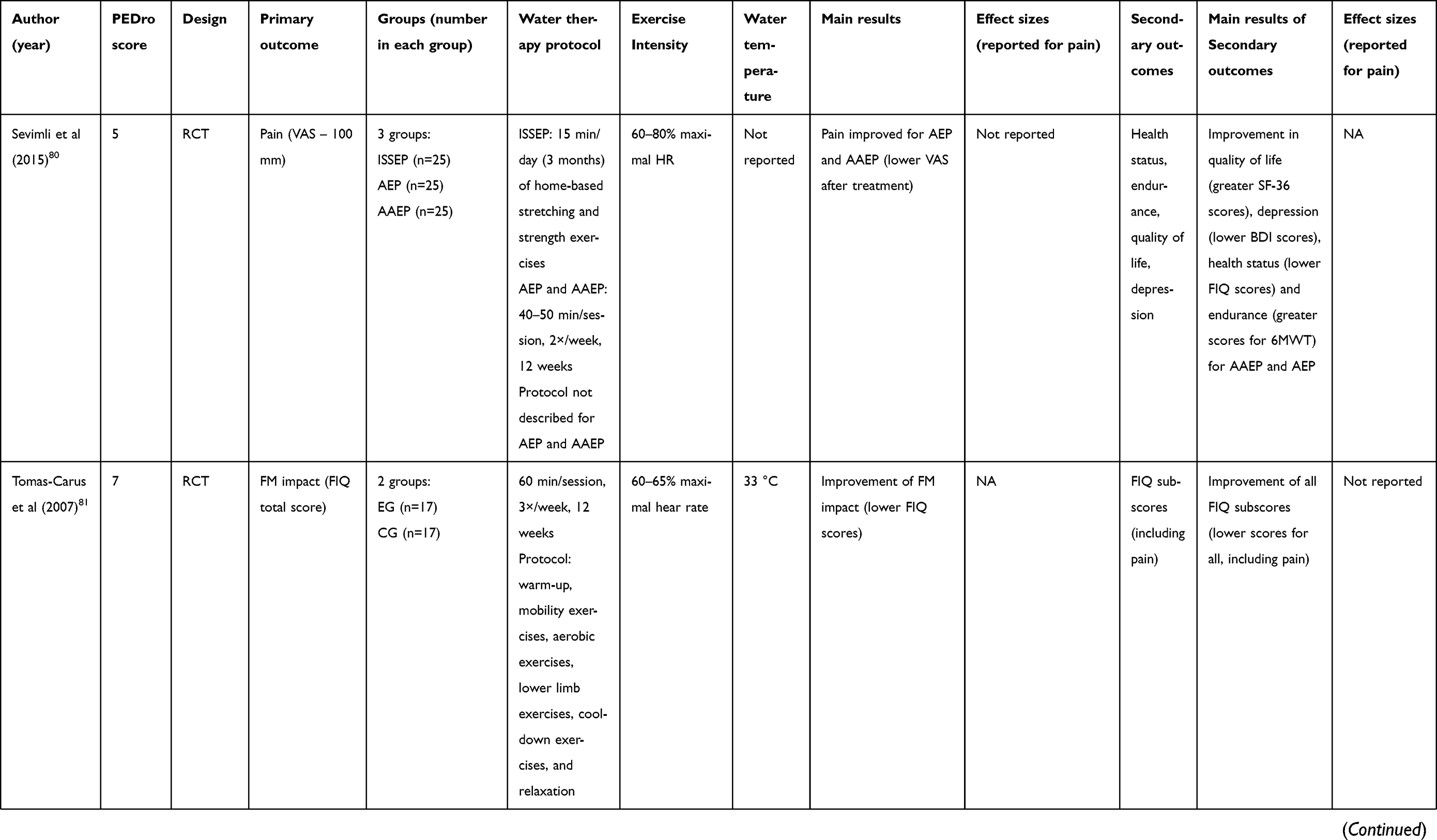 |
Table 2 Summary of studies using water therapy for FMS treatment |
Randomized clinical trials, nonrandomized clinical trials, and crossover design studies assessing the effects of any aquatic intervention on pain in FMS patients were considered eligible for inclusion. The methodological quality of the studies was analyzed using the PEDro scale.
Thirty-five studies were included. Methodological quality varied between 1 and 9 according to the PEDro scale. Water temperature ranged between 28 and 37/38 ºC, and 7 studies did not report. Regarding the effectiveness of water therapy, only 2 studies reported no significant improvement compared to the baseline condition. However, one of these studies was composed of only 10 participants (5 in the Ai Chi group and 5 in a control group; PEDro score=1)83 and the other comprised 18 participants (9 in the sauna group and 9 in the hydrotherapy group; PEDro score=4).84 Thus, 94% of the included studies showed improvement in pain besides ameliorating other symptoms. In the following sections, we will discuss the possible mechanisms underlying the aquatic exercise effects.11,28,30,31,83–82
Musculoskeletal and neuromuscular systems and the association with pain
The main symptom reported by FMS patients is pain.1,2,85,86 Pain is a dynamic and complex phenomenon that is the final result of several factors. The association between nociceptive activity and pain perception depends on several intrinsic and extrinsic influences. For the same nociceptive stimulus, pain perception and related brain activity will greatly differ between subjects. In the case of chronic rheumatic diseases that do not regress spontaneously, such as FMS, functional and structural central nervous system changes cause a generalized reduction in the pain threshold that is not limited to the anatomical structures involved, thus leading to the hyperalgesia and allodynia in many, if not all, body regions.21 FMS is associated with changes in the central nervous system that affect sensory information processing, amplifying peripheral input and/or generating pain perception in the absence of a noxious stimulus.21 People with FMS are reported to present hyperactivity of the hypothalamic–pituitary–adrenal axis,86,87 and this may be linked to the initiation or worsening of FMS symptoms. Moreover, dopamine dysfunctions have been linked to the pathophysiology of FMS, which are associated with hyperalgesia and deficient pain inhibition.59
Accordingly, exercise has been one of the most recommended nonpharmacological interventions for FMS.19,20 It has been shown that exercise is able to influence gene expression and structural complexity in the limbic structures that regulate the hypothalamic–pituitary–adrenal axis21 and can improve conditioned pain modulation due to increased endogenous opioids, stimulation of brain structures involved in the inhibitory descending pathways that regulate painful response.88 Geytenbeek89 has examined over 500 articles that were available on the theme and has concluded, after examining randomized controlled trials, case–control studies, and cohort studies, that high to moderate quality evidence supports the use of hydrotherapy for pain, function, joint mobility strength, and balance. Moreover, exercise seems to be the most effective component of a hydrotherapy program for FMS.89,90
Hence, exercising in an aquatic environment is advantageous. The pain-relieving effect of water-based exercises is suggested to be due to the joint effect of exercise, warm water, and buoyancy on thermal receptors and mechanoreceptors.33 Sensory-motor hyperstimulation exerted by the hydrostatic pressure, viscosity, and water temperature increases the triggers of thermal receptors and mechanoreceptors while blocking nociceptors.48,91 The viscosity of the water provides an environment with three-dimensional resistance, which facilitates proprioceptive feedback through functional patterns of movement and increases the synchronization of the motor units due to slowed movement.92 Also, immersion in warm water helps to increase blood flow and oxygen supply, improving nutrition and removal of catabolites, and thereby reducing signal molecules, such as IL-8 and noradrenaline,58 responsible for activation of nociceptors.93 In addition, regular exercise has been shown to improve overall health, as shown in other chronic conditions.27 This prominent effect on pain could be previously observed in several studies.27,28,31,32,53
It is noteworthy to mention that patients with FMS present abnormalities regarding pain modulation, including central sensitization and other pathophysiological mechanisms, such as the accumulation of cytotoxic substances in the extracellular space (glutamate, lactate, bradykinin, prostaglandins, etc.) generated by muscle activity, which exert algogenic effects by sensitizing and exciting nociceptors.94,95 Glutamate is a major cortical excitatory neurotransmitter that acts in pain neurotransmission. Increased levels of insular glutamate have been reported to be present in FMS. In addition, the concentration of this molecule is correlated with pain report. Enhanced glutamatergic neurotransmission resulting from higher concentrations of glutamate within the posterior insula may play a role in the pathophysiology of FMS and other central pain augmentation syndromes.96 Moreover, the sympathetic nervous system, which is already in a condition of hyperactivity (see section “Cardiovascular and respiratory systems and the association with pain”), under the action of bradykinin stimulates the release of noradrenaline and prostaglandins that further potentiate sympathetic hyperactivity and sensitize the nociceptors.
Therefore, another mechanism explaining the pain improvement may rely on the combination of hydrostatic pressure and temperature on nerve endings, which would lead to competing stimuli that would diminish the peripheral nociceptive input.97 Aquatic therapy also leads to muscle relaxation,98 which would in turn lead to less pain. Buoyancy decreases compressive weight-bearing stresses on joints and allows functional exercise with lessened gravitational load, making the movements easier, and even facilitating the improvement of both strength and range of motion.39,99 Furthermore, drag forces can be used as a resource to assist movements or to impose resistance favoring muscle strengthening.33 Nonetheless, quantifying the resistance training intensity and planning a progressive overload program in aquatic environments is challenging due to several factors (eg, speed of movements, range of motion, shape and size of floats, etc.). Therefore, it is still not clear whether aquatic exercises can really induce strength gains, since controversial results have been reported.33
Regarding chronic fatigue, another core feature of FMS, its perception may be reduced after water therapy due to the buoyancy effects.40 Buoyancy helps reduce the musculoskeletal system’s gravitational forces due to gravitational muscle relaxation and energy conservation, which seems to reduce perceived fatigue. Water immersion may also reduce neuromuscular responses or trigger inhibitory mechanisms, with an overall reduction in neural transmissions, which would impact not only on the perceived fatigue but also on the nociceptive input, reducing pain perception.
Cardiovascular and respiratory systems and the association with pain
FMS patients present cardiorespiratory dysfunction characterized by reduced respiratory muscle endurance, inspiratory muscle strength, and thoracic mobility.100 Moreover, cardiovascular autonomic control and baroreflex sensitivity have been also shown to be altered in this population.32,101,102 In addition, although it is not possible to identify a causal relationship, several studies have shown that these cardiorespiratory abnormalities are related to the pain in these subjects. Forti et al100 showed that inspiratory muscle strength is associated with the number of active tender points. In addition, Zamunér et al103 found that FMS show reduced respiratory sinus arrhythmia magnitude as compared to healthy women. Also, the indices obtained during the deep breathing test, a vagal maneuver, had an important association with pain in FMS. In another study, Zamunér et al104 also showed that sympathetic activity, as assessed by muscle sympathetic nerve activity, was related to pain in this population.
Several studies have described the interaction between autonomic and nociceptive pathways occurring at multiple levels,105–107 with the nucleus tractus solitarius playing an important role. The nucleus tractus solitarius, located in the brainstem, receives visceral information through the primary afferents of the vagus nerve and receives the spinal pathways involved in pain processing, functioning as an interface between the autonomic and sensory systems.107,108 Therefore, improving cardiovascular and respiratory outcomes in FMS patients should be considered one of the aims in the management of FMS.
It is well established that aerobic exercise improves cardiorespiratory function in patients with FMS.19,109 In addition, an aquatic environment can allow higher-intensity exercises to be undertaken, with lower cardiovascular stress than is possible on land.19,110 In this sense, some studies have assessed the effects of water therapy on the cardiorespiratory system. Zamunér et al32 found that a 16-week aquatic therapy program proved to be effective in ameliorating symptoms, aerobic functional capacity, and cardiac autonomic control in FMS patients. Surprisingly, improvements in cardiac autonomic control were related to the improvements in pain and the impact of FMS on quality of life, thus suggesting an important role of autonomic control mediating symptoms. Regarding the improvement of functional aerobic capacity, aquatic therapy has also been proven to be effective.32,51,80 However, studies have shown no association between cardiorespiratory fitness improvements and FMS symptom improvements.32,51,111–113
In summary, cardiorespiratory function and cardiac autonomic control should be routinely monitored in the management of FMS patients since they seem to be related to the symptoms; and water therapy might be seen as a strategic method to improve these outcomes in this population. However, improving cardiorespiratory fitness should not be the main goal in the therapy, but instead a tailored approach directed to the key FMS symptoms (pain, sleep disorders, fatigue, depression, disability) with exercise assignment that does not exacerbate post-exercise pain should take place.114,115
Neuroendocrine system and inflammation
Growing interest has been shown in the study of the benefits of aquatic therapy on the neuroendocrine system116–118 and inflammation. However, little is known about these in FMS patients. This is of interest since neurohormonal abnormalities have been reported in this population, such as low levels of serotonin,119 hypothalamic–pituitary–adrenal axis dysfunction,120–122 and low levels of growth hormone, which is associated with poor sleep quality.123,124 Moreover, although there are no specific biomarkers for FMS, some studies have suggested the involvement of inflammatory disorders on its etiology.125,126 Those disorders involve cytokines, proteins responsible for mediating the inflammatory reaction in the immune system.127 Studies have shown that FMS patients have increased levels of serum IL-8,128 IL-6, IL-10, and IL-1β.129 Ortega et al130 found that FMS patients present a higher circulation concentration of C-reactive protein and that their monocytes release more IL-1β, tumor necrosis factor alpha, IL-6, and IL-10 than those from an age-matched healthy control group. Additionally, FMS patients present a greater concentration of IL-8 in cerebrovascular fluid.131,132 IL-8 release is stimulated by substance P secretion and promotes sympathetic pain,133 and thus is considered an inflammatory marker of FMS,62 which is indicative of underlying low-grade systemic inflammation. There is evidence showing the participation of chemokines (signaling molecules present in inflammatory and immune responses) in FMS, with higher concentrations of inflammatory chemokines (TARC/CCL17, MIG/CXCL9, MDC/CCL22, I-TAC/CXCL11, and eotaxin/CCL11).134
Aquatic therapy has been shown to reduce plasma levels of norepinephrine,135–137 epinephrine,135,138 β-endorphin, and cortisol139 in healthy men. In this context, we may suggest that aquatic therapy may contribute to a reduction of stress, improvement of sleep quality, and reduction of pain sensitivity.26,137 Regarding FMS patients, to our knowledge, no studies have assessed the effects of aquatic therapy on the neuroendocrine system. However, Bote et al140 found that a single session of moderate cycling improved the inflammatory and stress status of FMS patients. Moreover, their results also suggest that the neuroendocrine mechanism seems to be an exercise-induced decrease in the stress response of these patients, since they observed a reduction in the systemic concentration of cortisol, noradrenaline, and extracellular heatshock protein 72. In agreement with these findings, Ortega et al130 studied the effects of an aquatic fitness program performed for 8 months twice a week. After the program, monocytes from FMS patients presented similar spontaneous release of IL-1β and IL-6 to that of healthy controls and a reduction in C-reactive protein, showing that aquatic exercise might exert anti-inflammatory effects.
Current perspectives
A considerable amount of evidence27 has shown that water therapy improves pain, fatigue, and quality of life. However, current recommendations for the management of fibromyalgia elaborated by the European League Against Rheumatism18 suggest a “weak for” recommendation, implying that most therapists would, although a substantial minority would not, recommend water therapy for FMS patients. This recommendation underlies the small amount of evidence suggesting superiority of water therapy over land-based therapies.141
Therefore, future studies should focus on the possible mechanisms explaining the beneficial effects of water therapy in order to elucidate whether they are similar or not to the mechanisms leading to the improvement of symptoms and quality of life promoted by land-based exercises. Moreover, studies should also compare the detraining effects or long-lasting effects promoted by water therapy and land-based exercises since these have been addressed only by a few studies and the results are controversial. A recent study54 showed that 16 weeks of aquatic exercise therapy was effective in improving aerobic capacity and symptomatology such as pain, quality of life, and fatigue in FMS patients. However, after 16 weeks of detraining, all variables returned to near baseline. Thus, elucidating whether this is comparable to land-based exercises would assist FMS patients and therapists on the proper therapeutic approach recommendation and selection.
Another noteworthy point to be mentioned regards the FMS patient’s adherence to treatment and engagement with aftercare tasks in the long term.86 Coupled with the fact that pharmacological interventions seem to be ineffective, as they seldom induce minimally important clinical differences in pain after 3 months of therapy,142,143 this makes the development of treatments that benefit patients over their lifetime extremely challenging. Hence, a multidisciplinary approach and educational strategies may be helpful additions to physical treatment, in this case, water therapy; these strategies show the importance of continuing with treatment, that the disease may vary in intensity over the time, and, more importantly, that they have to take responsibility for their healthcare and habits that influence on FMS symptoms, giving them tools to help with daily FMS management. Water therapy, in this context, comes as an alternative that makes movement easier and may increase compliance with the treatment.
Another topic to be discussed is the cost-effectiveness of water therapy for FMS. One previous study11 has shown that adding water therapy to the usual care for FMS patients is cost-effective for both healthcare and societal costs. The authors also concluded that the characteristics of facilities (distance from patients’ homes and the number of patients who can participate per session) are major determinants that have to be considered before a health manager decides to invest in such a program. Therefore, this point should be addressed in future studies that aim to elucidate whether the cost-effectiveness differs among other kinds of interventions. Studies involving cost-effectiveness may also be helpful in guiding the development of public policies for the healthcare of FMS patients, and, as such, are much needed.
The present study has some limitations, as it is not a systematic review. As such, performance of a metaanalysis was not possible. As a narrative review, the scope of the present study was to highlight and discuss the possible mechanisms involved in the improvement of pain for FMS patients who undergo water therapy. Nonetheless, this discussion is still difficult as the protocols described vary in duration, session length, and techniques used into the swimming pool, as well as the outcomes chosen; also, several outcomes are not sufficiently described.
Conclusion
Water therapy may be recommended as a nonpharmacologic therapeutic approach for the management of FMS patients, improving pain, fatigue, and quality of life; these therapeutic effects are achieved by the physiological changes caused by in-water exercising. However, future studies should be conducted in order to clarify the action mechanisms and whether long-lasting effects are superior to other types of intervention, especially land-based exercises.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Wolfe F, Clauw DJ, Fitzcharles M-A, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319–329. doi:10.1016/j.semarthrit.2016.08.012
2. Sluka KA, Clauw DJ. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience. 2016;338:114–129. doi:10.1016/j.neuroscience.2016.06.006
3. Häuser W, Perrot S, Clauw DJ, Fitzcharles M-A. Unravelling fibromyalgia—steps toward individualized management. J Pain. 2018;19(2):125–134. doi:10.1016/j.jpain.2017.08.009
4. Doron Y, Peleg R, Peleg A, Neumann L, Buskila D. The clinical and economic burden of fibromyalgia compared with diabetes mellitus and hypertension among Bedouin women in the Negev. Fam Pract. 2004;21(4):415–419. doi:10.1093/fampra/cmh411
5. Ghavidel-Parsa B, Bidari A, Amir Maafi A, Ghalebaghi B. The iceberg nature of fibromyalgia burden: the clinical and economic aspects. Korean J Pain. 2015;28(3):169–176. doi:10.3344/kjp.2015.28.3.169
6. White LA, Birnbaum HG, Kaltenboeck A, Tang J, Mallett D, Robinson RL. Employees with fibromyalgia: medical comorbidity, healthcare costs, and work loss. J Occup Environl Med. 2008;50(1):13–24. doi:10.1097/JOM.0b013e31815cff4b
7. Silverman S, Dukes EM, Johnston SS, Brandenburg NA, Sadosky A, Huse DM. The economic burden of fibromyalgia: comparative analysis with rheumatoid arthritis. Curr Med Res Opin. 2009;25(4):829–840. doi:10.1185/03007990902728456
8. Berger A, Dukes E, Martin S, Edelsberg J, Oster G. Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int J Clin Pract. 2007;61(9):1498–1508.
9. Annemans L, Le Lay K, Taïeb C. Societal and patient burden of fibromyalgia syndrome. PharmacoEconomics. 2009;27(7):547–559.
10. Boonen A, van Den Heuvel R, van Tubergen A, et al. Large differences in cost of illness and wellbeing between patients with fibromyalgia, chronic low back pain, or ankylosing spondylitis. Ann Rheum Dis. 2005;64(3):396–402. doi:10.1136/ard.2003.019711
11. Gusi N, Tomas-Carus P. Cost-utility of an 8-month aquatic training for women with fibromyalgia: a randomized controlled trial. Arthritis Res Ther. 2008;10(1):R24. doi:10.1186/ar2377
12. Perrot S, Winkelmann A, Dukes E, et al. Characteristics of patients with fibromyalgia in France and Germany. Int J Clin Pract. 2010;64(8):1100–1108. doi:10.1111/j.1742-1241.2010.02418.x
13. Skaer TL. Fibromyalgia: disease synopsis, medication cost effectiveness and economic burden. PharmacoEconomics. 2014;32(5):457–466. doi:10.1007/s40273-014-0137-y
14. Wagner J-S, Chandran A, DiBonaventura M, Cappelleri JC. The costs associated with sleep symptoms among patients with fibromyalgia. Expert Rev Pharmacoecon Outcomes Res. 2013;13(1):131–139. doi:10.1586/erp.12.82
15. Annemans L, Wessely S, Spaepen E, et al. Health economic consequences related to the diagnosis of fibromyalgia syndrome. Arthritis Rheumatol. 2008;58(3):895–902. doi:10.1002/art.23265
16. Chandran A, Schaefer C, Ryan K, Baik R, McNett M, Zlateva G. The comparative economic burden of mild, moderate, and severe fibromyalgia: results from a retrospective chart review and cross-sectional survey of working-age U.S. adults. J Manag Care Pharm. 2012;18(6):415–426. doi:10.18553/jmcp.2012.18.6.415
17. Brown TM, Garg S, Chandran AB, McNett M, Silverman SL, Hadker N. The impact of ‘best-practice’ patient care in fibromyalgia on practice economics. J Eval Clin Pract. 2012;18(4):793–798. doi:10.1111/j.1365-2753.2011.01678.x
18. Macfarlane GJ, Kronisch C, Dean LE, et al. EULAR revised recommendations for the management of fibromyalgia. Ann Rheum Dis. 2017;76(2):318–328. doi:10.1136/annrheumdis-2016-209724
19. Bidonde J, Busch AJ, Schachter CL, et al. Aerobic exercise training for adults with fibromyalgia. Cochrane Database Syst Rev. 2017;6:CD012700.
20. Busch AJ, Webber SC, Brachaniec M, et al. Exercise Therapy for Fibromyalgia. Curr Pain Headache Rep. 2011;15(5):358–367. doi:10.1007/s11916-011-0214-2
21. Eller-Smith OC, Nicol AL, Christianson JA. Potential mechanisms underlying centralized pain and emerging therapeutic interventions. Front Cell Neurosci. 2018;12. doi:10.3389/fncel.2018.00035
22. Lauche R, Cramer H, Hauser W, Dobos G, Langhorst J. A systematic overview of reviews for complementary and alternative therapies in the treatment of the fibromyalgia syndrome. Evid Based Complement Alternat Med. 2015;2015:610615. doi:10.1155/2015/610615
23. Ambrose KR, Golightly YM. Physical exercise as non-pharmacological treatment of chronic pain: why and when. Best Pract Res Clin Rheumatol. 2015;29(1):120–130. doi:10.1016/j.berh.2015.04.022
24. Demir-Göçmen D, Altan L, Korkmaz N, Arabaci R. Effect of supervised exercise program including balance exercises on the balance status and clinical signs in patients with fibromyalgia. Rheumatol Int. 2013;33(3):743–750. doi:10.1007/s00296-012-2444-y
25. Geneen LJ, Moore RA, Clarke C, Martin D, Colvin LA, Smith BH. Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2017;4:CD011279. doi:10.1002/14651858.CD011279.pub3
26. Thomas EN, Blotman F. Aerobic exercise in fibromyalgia: a practical review. Rheumatol Int. 2010;30(9):1143–1150. doi:10.1007/s00296-010-1369-6
27. Bidonde J, Busch AJ, Webber SC, et al. Aquatic exercise training for fibromyalgia. Cochrane Database Syst Rev. 2014;(10):CD011336. doi:10.1002/14651858.CD011336
28. Avila MA, Camargo PR, Ribeiro IL, Alburquerque-Sendin F, Zamuner AR, Salvini TF. Effects of a 16-week hydrotherapy program on three-dimensional scapular motion and pain of women with fibromyalgia: a single-arm study. Clin Biomech. 2017;49:145–154. doi:10.1016/j.clinbiomech.2017.09.012
29. Carbonell-Baeza A, Aparicio VA, Chillón P, Femia P, Delgado-Fernandez M, Ruiz JR. Effectiveness of multidisciplinary therapy on symptomatology and quality of life in women with fibromyalgia. Clin Exp Rheumatol. 2012;29(6 Suppl 69):S97–S103.
30. Latorre PÁ, Santos MA, Heredia-Jiménez JM, et al. Effect of a 24-week physical training programme (in water and on land) on pain, functional capacity, body composition and quality of life in women with fibromyalgia. Clin Exp Rheumatol. 2013;31(6 Suppl 79):S72–S80.
31. Trevisan DC, Avila MA, Driusso P, Gramani-Say K, Araujo-Moreira FM, Parizotto NA. Effects of hydrotherapy on postural control of women with fibromyalgia syndrome: a single arm study. Myopain. 2015;23(3–4):125–133. doi:10.1080/24708593.2017.1300205
32. Zamunér AR, Andrade CP, Forti M, et al. Effects of a hydrotherapy programme on symbolic and complexity dynamics of heart rate variability and aerobic capacity in fibromyalgia patients. Clin Exp Rheumatol. 2015;33(1 Suppl 88):S73–S81.
33. Heywood S, McClelland J, Mentiplay B, Geigle P, Rahmann A, Clark R. Effectiveness of aquatic exercise in improving lower limb strength in musculoskeletal conditions: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2017;98(1):173–186. doi:10.1016/j.apmr.2016.08.472
34. Charter of Physiotherapists. The definition of aquatic physiotherapy. Aqualines. 2009;21(2):6.
35. Becker BE. Aquatic therapy: scientific foundations and clinical rehabilitation applications. PM&R. 2009;1(9):859–872. doi:10.1016/j.pmrj.2009.05.017
36. Haupenthal A, Fontana H, Ruschel C, Dos Santos DP, Roesler H. Ground reaction forces in shallow water running are affected by immersion level, running speed and gender. J Sci Med Sport. 2013;16(4):348–352. doi:10.1016/j.jsams.2012.08.006
37. Roesler H, Haupenthal A, Schütz GR, de Souza PV. Dynamometric analysis of the maximum force applied in aquatic human gait at 1.3 m of immersion. Gait Posture. 2006;24(4):412–417. doi:10.1016/j.gaitpost.2005.09.014
38. Torres-Ronda L, Schelling I Del Alcázar X. The properties of water and their applications for training. J Hum Kinet. 2014;44(1):237–248. doi:10.2478/hukin-2014-0129
39. Barker AL, Talevski J, Morello RT, Brand CA, Rahmann AE, Urquhart DM. Effectiveness of aquatic exercise for musculoskeletal conditions: a meta-analysis. Arch Phys Med Rehabil. 2014;95(9):1776–1786. doi:10.1016/j.apmr.2014.04.005
40. Wilcock IM, Cronin JB, Hing WA. Physiological response to water immersion: a method for sport recovery? Sports Med. 2006;36(9):747–765. doi:10.2165/00007256-200636090-00003
41. Ayme K, Gavarry O, Rossi P, Desruelle A-V, Regnard J, Boussuges A. Effect of head-out water immersion on vascular function in healthy subjects. Appl Physiol Nutr Metab. 2014;39(4):425–431. doi:10.1139/apnm-2013-0153
42. Aveiro MC, Avila MA, Pereira-Baldon VS, et al. Water- versus land-based treatment for postural control in postmenopausal osteoporotic women: a randomized, controlled trial. Climacteric. 2017;20(5):427–435. doi:10.1080/13697137.2017.1325460
43. Avelar NCP, Bastone AC, Alcântara MA, Gomes WF. Effectiveness of aquatic and non-aquatic lower limb muscle endurance training in the static and dynamic balance of elderly people. Braz J Phys Ther. 2010;14(3):229–236.
44. Furnari A, Calabrò RS, Gervasi G, et al. Is hydrokinesitherapy effective on gait and balance in patients with stroke? A clinical and baropodometric investigation. Brain Inj. 2014;28(8):1109–1114. doi:10.3109/02699052.2014.910700
45. Volpe D, Giantin MG, Maestri R, Frazzitta G. Comparing the effects of hydrotherapy and land-based therapy on balance in patients with Parkinson’s disease: a randomized controlled pilot study. Clin Rehabil. 2014;28(12):1210–1217. doi:10.1177/0269215514536060
46. Zhu Z, Cui L, Yin M, et al. Hydrotherapy vs. conventional land-based exercise for improving walking and balance after stroke: a randomized controlled trial. Clin Rehabil. 2016;30(6):587–593. doi:10.1177/0269215515593392
47. Pöyhönen T, Keskinen KL, Hautala A, Mälkiä E. Determination of hydrodynamic drag forces and drag coefficients on human leg/foot model during knee exercise. Clin Biomech (Bristol, Avon). 2000;15(4):256–260.
48. Bender T, Karagulle Z, Balint GP, Gutenbrunner C, Balint PV, Sukenik S. Hydrotherapy, balneotherapy, and spa treatment in pain management. Rheumatol Int. 2005;25(3):220–224. doi:10.1007/s00296-004-0487-4
49. Batterham SI, Heywood S, Keating JL. Systematic review and meta-analysis comparing land and aquatic exercise for people with hip or knee arthritis on function, mobility and other health outcomes. BMC Musculoskelet Disord. 2011;12:123. doi:10.1186/1471-2474-12-181
50. Gibson AJ, Shields N. Effects of aquatic therapy and land-based therapy versus land-based therapy alone on range of motion, edema, and function after hip or knee replacement: a systematic review and meta-analysis. Physiother Can. 2015;67(2):133–141. doi:10.3138/ptc.2014-01
51. Andrade CP, Zamuner AR, Forti M, Franca TF, Tamburus NY, Silva E. Oxygen uptake and body composition after aquatic physical training in women with fibromyalgia: a randomized controlled trial. Eur J Phys Rehabil Med. 2017;53(5):751–758. doi:10.23736/S1973-9087.17.04543-9
52. Rivas Neira S, Pasqual Marques A, Pegito Perez I, Fernandez Cervantes R, Vivas Costa J. Effectiveness of aquatic therapy vs land-based therapy for balance and pain in women with fibromyalgia: a study protocol for a randomised controlled trial. BMC Musculoskelet Disord. 2017;18(1):22. doi:10.1186/s12891-017-1624-z
53. Altan L, Bingol U, Aykac M, Koc Z, Yurtkuran M. Investigation of the effects of pool-based exercise on fibromyalgia syndrome. Rheumatol Int. 2004;24(5):272–277. doi:10.1007/s00296-003-0371-7
54. Andrade CP, Zamuner AR, Forti M, Tamburus NY, Silva E. Effects of aquatic training and detraining on women with fibromyalgia: controlled randomized clinical trial. Eur J Phys Rehabil Med. 2019;55(1):79–88. doi:10.23736/S1973-9087.18.05041-4
55. Arcos-Carmona IM, Castro-Sanchez AM, Mataran-Penarrocha GA, Gutierrez-Rubio AB, Ramos-Gonzalez E, Moreno-Lorenzo C. [Effects of aerobic exercise program and relaxation techniques on anxiety, quality of sleep, depression, and quality of life in patients with fibromyalgia: a randomized controlled trial]. Med Clin. 2011;137(9):398–401. doi:10.1016/j.medcli.2010.09.045
56. Assis MR, Silva LE, Alves AM, et al. A randomized controlled trial of deep water running: clinical effectiveness of aquatic exercise to treat fibromyalgia. Arthritis Rheum. 2006;55(1):57–65. doi:10.1002/art.21693
57. Biezus J, Ide MR, Tanaka C, Caromano FA, Rodrigues JRAL. Aquatic exercises for the pain of individuals with fibromyalgia. Rev Bras Cienc Farm. 2006;10(3):246.
58. Bote ME, Garcia JJ, Hinchado MD, Ortega E. An exploratory study of the effect of regular aquatic exercise on the function of neutrophils from women with fibromyalgia: role of IL-8 and noradrenaline. Brain Behav Immun. 2014;39:107–112. doi:10.1016/j.bbi.2013.11.009
59. Calandre EP, Rodriguez-Claro ML, Rico-Villademoros F, Vilchez JS, Hidalgo J, Delgado-Rodriguez A. Effects of pool-based exercise in fibromyalgia symptomatology and sleep quality: a prospective randomised comparison between stretching and Ai Chi. Clin Exp Rheumatol. 2009;27(5 Suppl 56):S21–S28.
60. Carbonell-Baeza A, Aparicio VA, Martins-Pereira CM, et al. Efficacy of Biodanza for treating women with fibromyalgia. J Altern Complement Med. 2010;16(11):1191–1200. doi:10.1089/acm.2010.0039
61. Cuesta-Vargas AI, Adams N. A pragmatic community-based intervention of multimodal physiotherapy plus deep water running (DWR) for fibromyalgia syndrome: a pilot study. Clin Rheumatol. 2011;30(11):1455–1462. doi:10.1007/s10067-011-1825-z
62. de Andrade SC, de Carvalho RF, Soares AS, de Abreu Freitas RP, de Medeiros Guerra LM, Vilar MJ. Thalassotherapy for fibromyalgia: a randomized controlled trial comparing aquatic exercises in sea water and water pool. Rheumatol Int. 2008;29(2):147–152. doi:10.1007/s00296-008-0644-2
63. Evcik D, Yigit I, Pusak H, Kavuncu V. Effectiveness of aquatic therapy in the treatment of fibromyalgia syndrome: a randomized controlled open study. Rheumatol Int. 2008;28(9):885–890. doi:10.1007/s00296-008-0538-3
64. Fernandes G, Jennings F, Nery Cabral MV, Pirozzi Buosi AL, Natour J. Swimming improves pain and functional capacity of patients with fibromyalgia: a randomized controlled trial. Arch Phys Med Rehabil. 2016;97(8):1269–1275.
65. Gowans SE, deHueck A, Voss S, Silaj A, Abbey SE, Reynolds WJ. Effect of a randomized, controlled trial of exercise on mood and physical function in individuals with fibromyalgia. Arthritis Rheum. 2001;45(6):519–529.
66. Gusi N, Tomas-Carus P, Häkkinen A, Häkkinen K, Ortega-Alonso A. Exercise in waist-high warm water decreases pain and improves health-related quality of Life and strength in the lower extremities in women with fibromyalgia. Arthritis Rheum. 2006;55(1):66–73. doi: 10.1002/art.21718
67. Hecker CD, Melo C, Tomazoni S, Martins RÁBL, Leal Junior ECP. Análise dos efeitos da cinesioterapia e da hidrocinesioterapia sobre a qualidade de vida de pacientes com fibromialgia: um ensaio clínico randomizado. Fisioter Mov. 2011;24:57–64. doi:10.1590/S0103-51502011000100007
68. Ide MR, Laurindo IMM, Rodrigues-Júnior AL, Tanaka C. Effect of aquatic respiratory exercise-based program in patients with fibromyalgia. Int J Rheum Dis. 2008;11(2):131–140. doi:10.1111/j.1756-185X.2008.00348.x
69. Jentoft ES, Kvalvik AG, Mengshoel AM. Effects of pool-based and land-based aerobic exercise on women with fibromyalgia/chronic widespread muscle pain. Arthritis Rheum. 2001;45(1):42–47. doi:10.1002/1529-0131(200102)45:1<42::AID-ANR82>3.0.CO;2-A
70. Kesiktas N, Karagulle Z, Erdogan N, Yazicioglu K, Yilmaz H, Paker N. The efficacy of balneotherapy and physical modalities on the pulmonary system of patients with fibromyalgia. J Back Musculoskelet Rehabil. 2011;24(1):57–65.
71. Latorre Roman PA, Santos ECMA, Garcia-Pinillos F. Effects of functional training on pain, leg strength, and balance in women with fibromyalgia. Mod Rheumatol. 2015;25(6):943–947.
72. Letieri RV, Furtado GE, Letieri M, et al. Dor, qualidade de vida, autopercepção de saúde e depressão de pacientes com fibromialgia, tratados com hidrocinesioterapia. Rev Bras Reumatol. 2013;53:494–500.
73. Lopez-Rodriguez MM, Fernandez-Martinez M, Mataran-Penarrocha GA, Rodriguez-Ferrer ME, Granados Gamez G, Aguilar Ferrandiz E. [Effectiveness of aquatic biodance on sleep quality, anxiety and other symptoms in patients with fibromyalgia]. Med Clin. 2013;141(11):471–478.
74. Mannerkorpi K, Nyberg B, Ahlmen M, Ekdahl C. Pool exercise combined with an education program for patients with fibromyalgia syndrome. A prospective, randomized study. J Rheumatol. 2000;27(10):2473–2481.
75. Mannerkorpi K, Nordeman L, Ericsson A, Arndorw M; Group GAUS. Pool exercise for patients with fibromyalgia or chronic widespread pain: a randomized controlled trial and subgroup analyses. J Rehabil Med. 2009;41(9):751–760.
76. Munguia-Izquierdo D, Legaz-Arrese A. Exercise in warm water decreases pain and improves cognitive function in middle-aged women with fibromyalgia. Clin Exp Rheumatol. 2007;25(6):823–830.
77. Munguia-Izquierdo D, Legaz-Arrese A. Assessment of the effects of aquatic therapy on global symptomatology in patients with fibromyalgia syndrome: a randomized controlled trial. Arch Phys Med Rehabil. 2008;89(12):2250–2257.
78. Perez de la Cruz S, Lambeck J. A new approach to the improvement of quality of life in fibromyalgia: a pilot study on the effects of an aquatic Ai Chi program. Int J Rheum Dis. 2018;21(8):1525–1532. doi:10.1111/1756-185X.12930.
79. Segura-Jimenez V, Carbonell-Baeza A, Aparicio VA, et al. A warm water pool-based exercise program decreases immediate pain in female fibromyalgia patients: uncontrolled clinical trial. Int J Sports Med. 2013;34(7):600–605.
80. Sevimli D, Kozanoglu E, Guzel R, Doganay A. The effects of aquatic, isometric strength-stretching and aerobic exercise on physical and psychological parameters of female patients with fibromyalgia syndrome. J Phys Ther Sci. 2015;27(6):1781–1786.
81. Tomas-Carus P, Hakkinen A, Gusi N, Leal A, Hakkinen K, Ortega-Alonso A. Aquatic training and detraining on fitness and quality of life in fibromyalgia. Med Sci Sports Exerc. 2007;39(7):1044–1050.
82. Tomas-Carus P, Gusi N, Hakkinen A, Hakkinen K, Raimundo A, Ortega-Alonso A. Improvements of muscle strength predicted benefits in HRQOL and postural balance in women with fibromyalgia: an 8-month randomized controlled trial. Rheumatology. 2009;48(9):1147–1151.
83. Santana JS, Almeida AP, Brandao PM. [The effect of Ai Chi method in fibromyalgic patients]. Cien Saude Colet. 2010;15(Suppl 1):1433–1438. doi:10.1590/S1413-81232010000700054
84. Piso U, Küther G, Gutenbrunner C, Gehrke A. Analgetische Wirkungen der Sauna bei der Fibromyalgie. Phys Med Rehab Kuror. 2001;11(03):94–99. doi:10.1055/s-2001-14438
85. Clauw DJ. Fibromyalgia. JAMA. 2014;311(15):1547–1547.
86. Hauser W, Ablin J, Fitzcharles MA, et al. Fibromyalgia. Nat Rev Dis Primers. 2015;1:15022.
87. Wingenfeld K, Heim C, Schmidt I, Wagner D, Meinlschmidt G, Hellhammer DH. HPA axis reactivity and lymphocyte glucocorticoid sensitivity in fibromyalgia syndrome and chronic pelvic pain. Psychosom Med. 2008;70(1):65–72.
88. Naugle KM, Riley JL. Self-reported physical activity predicts pain inhibitory and facilitatory function. Med Sci Sports Exerc. 2014;46(3):622–629.
89. Geytenbeek J. Evidence for effective hydrotherapy. Physiotherapy. 2002;88(9):514–529.
90. Perraton L, Machotka Z, Kumar S. Components of effective randomized controlled trials of hydrotherapy programs for fibromyalgia syndrome: A systematic review. J Pain Res. 2009;2:165–173.
91. Mooventhan A, Nivethitha L. Scientific evidence-based effects of hydrotherapy on various systems of the body. N Am J Med Sci. 2014;6(5):199–209.
92. Brody LT, Hall CM. Impaired muscle performance. In:
93. Hall J, Swinkels A, Briddon J, McCabe CS. Does aquatic exercise relieve pain in adults with neurologic or musculoskeletal disease? A systematic review and meta-analysis of randomized controlled trials. Arch Phys Med Rehabil. 2008;89(5):873–883.
94. Coutaux A, Adam F, Willer JC, Le Bars D. Hyperalgesia and allodynia: peripheral mechanisms. Joint Bone Spine. 2005;72(5):359–371.
95. Mense S. Algesic agents exciting muscle nociceptors. Exp Brain Res. 2009;196(1):89–100.
96. Harris RE, Sundgren PC, Craig AD, et al. Elevated insular glutamate in fibromyalgia is associated with experimental pain. Arthritis Rheum. 2009;60(10):3146–3152.
97. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979.
98. Kjellgren A, Sundequist U, Norlander T, Archer T. Effects of flotation-REST on muscle tension pain. Pain Res Manag. 2001;6(4):181–189.
99. Pöyhönen T, Sipilä S, Keskinen KL, Hautala A, Savolainen J, Mälkiä E. Effects of aquatic resistance training on neuromuscular performance in healthy women. Med Sci Sports Exerc. 2002;34(12):2103–2109.
100. Forti M, Zamuner AR, Andrade CP, Silva E. Lung function, respiratory muscle strength, and thoracoabdominal mobility in women with fibromyalgia syndrome. Respir Care. 2016;61(10):1384–1390.
101. Furlan R, Colombo S, Perego F, et al. Abnormalities of cardiovascular neural control and reduced orthostatic tolerance in patients with primary fibromyalgia. J Rheumatol. 2005;32(9):1787–1793.
102. Reyes Del Paso GA, Garrido S, Pulgar A, Duschek S. Autonomic cardiovascular control and responses to experimental pain stimulation in fibromyalgia syndrome. J Psychosom Res. 2011;70(2):125–134. doi:10.1016/j.jpsychores.2010.09.012
103. Zamunér AR, Forti M, Andrade CP, Avila MA, Da Silva E. Respiratory sinus arrhythmia and its association with pain in women with fibromyalgia syndrome. Pain Pract. 2016;16(6):704–711. doi:10.1111/papr.12321
104. Zamunér AR, Barbic F, Dipaola F, et al. Relationship between sympathetic activity and pain intensity in fibromyalgia. Clin Exp Rheumatol. 2015;33(1 Suppl 88):S53–S57.
105. Bou-Holaigah I, Calkins H, Flynn JA, et al. Provocation of hypotension and pain during upright tilt table testing in adults with fibromyalgia. Clin Exp Rheumatol. 1997;15(3):239–246.
106. Aicher SA, Randich A. Antinociception and cardiovascular responses produced by electrical stimulation in the nucleus tractus solitarius, nucleus reticularis ventralis, and the caudal medulla. Pain. 1990;42(1):103–119.
107. Bruehl S, Chung OY. Interactions between the cardiovascular and pain regulatory systems: an updated review of mechanisms and possible alterations in chronic pain. Neurosci Biobehav Rev. 2004;28(4):395–414. doi:10.1016/j.neubiorev.2004.06.004
108. Bruehl S, Chung OY, Jirjis JN, Biridepalli S. Prevalence of clinical hypertension in patients with chronic pain compared to nonpain general medical patients. Clin J Pain. 2005;21(2):147–153.
109. Andrade A, Vilarino GT, Serafim TT, Junior AAP, de Souza CA, Sieczkowska SM. Modulation of autonomic function by physical exercise in patients with fibromyalgia syndrome: A systematic review. PM&R. 2019. doi:10.1002/pmrj.12158
110. Hall J, Grant J, Blake D, Taylor G, Garbutt G. Cardiorespiratory responses to aquatic treadmill walking in patients with rheumatoid arthritis. Physiother Res Int. 2004;9(2):59–73.
111. Valim V, Oliveira L, Suda A, et al. Aerobic fitness effects in fibromyalgia. J Rheumatol. 2003;30(5):1060–1069.
112. Langhorst J, Musial F, Klose P, Hauser W. Efficacy of hydrotherapy in fibromyalgia syndrome–a meta-analysis of randomized controlled clinical trials. Rheumatology. 2009;48(9):1155–1159. doi:10.1093/rheumatology/kep182
113. McVeigh JG, McGaughey H, Hall M, Kane P. The effectiveness of hydrotherapy in the management of fibromyalgia syndrome: a systematic review. Rheumatol Int. 2008;29(2):119–130. doi:10.1007/s00296-008-0674-9
114. Cazzola M, Atzeni F, Salaffi F, Stisi S, Cassisi G, Sarzi-Puttini P. Which kind of exercise is best in fibromyalgia therapeutic programmes? A practical review. Clin Exp Rheumatol. 2010;28(6 Suppl 63):S117–S124.
115. Hauser W, Arnold B, Eich W, et al. Management of fibromyalgia syndrome–an interdisciplinary evidence-based guideline. German Med Sci. 2008;6:Doc14.
116. Arca EA, Martinelli B, Martin LC, Waisberg CB, Franco RJ. Aquatic exercise is as effective as dry land training to blood pressure reduction in postmenopausal hypertensive women. Physiother Res Int. 2014;19(2):93–98. doi:10.1002/pri.1565
117. Asa C, Maria S, Katharina SS, Bert A. Aquatic exercise is effective in improving exercise performance in patients with heart failure and type 2 diabetes mellitus. Evid Based Complement Alternat Med. 2012;2012:349209. doi:10.1155/2012/349209
118. Benfield RD, Hortobagyi T, Tanner CJ, Swanson M, Heitkemper MM, Newton ER. The effects of hydrotherapy on anxiety, pain, neuroendocrine responses, and contraction dynamics during labor. Biol Res Nurs. 2010;12(1):28–36. doi:10.1177/1099800410361535
119. Tander B, Gunes S, Boke O, et al. Polymorphisms of the serotonin-2A receptor and catechol-O-methyltransferase genes: a study on fibromyalgia susceptibility. Rheumatol Int. 2008;28(7):685–691. doi:10.1007/s00296-008-0525-8
120. Crofford LJ. The hypothalamic-pituitary-adrenal stress axis in fibromyalgia and chronic fatigue syndrome. Z Rheumatol. 1998;57(Suppl 2):67–71.
121. Crofford LJ. Neuroendocrine abnormalities in fibromyalgia and related disorders. Am J Med Sci. 1998;315(6):359–366.
122. Griep EN, Boersma JW, de Kloet ER. Altered reactivity of the hypothalamic-pituitary-adrenal axis in the primary fibromyalgia syndrome. J Rheumatol. 1993;20(3):469–474.
123. Cuatrecasas G, Riudavets C, Guell MA, Nadal A. Growth hormone as concomitant treatment in severe fibromyalgia associated with low IGF-1 serum levels. A pilot study. BMC Musculoskelet Disord. 2007;8:119. doi:10.1186/1471-2474-8-119
124. Jones KD, Deodhar P, Lorentzen A, Bennett RM, Deodhar AA. Growth hormone perturbations in fibromyalgia: a review. Semin Arthritis Rheum. 2007;36(6):357–379. doi:10.1016/j.semarthrit.2006.09.006
125. Omoigui S. The biochemical origin of pain: the origin of all pain is inflammation and the inflammatory response. Part 2 of 3 - inflammatory profile of pain syndromes. Med Hypotheses. 2007;69(6):1169–1178. doi:10.1016/j.mehy.2007.06.033
126. van West D, Maes M. Neuroendocrine and immune aspects of fibromyalgia. BioDrugs. 2001;15(8):521–531. doi:10.2165/00063030-200115080-00004
127. Totsch SK, Sorge RE. Immune system involvement in specific pain conditions. Mol Pain. 2017;13:1744806917724559. doi:10.1177/1744806917724559
128. Wang H, Buchner M, Moser MT, Daniel V, Schiltenwolf M. The role of IL-8 in patients with fibromyalgia: a prospective longitudinal study of 6 months. Clin J Pain. 2009;25(1):1–4. doi:10.1097/AJP.0b013e31817e13a3
129. Imamura M, Targino RA, Hsing WT, et al. Concentration of cytokines in patients with osteoarthritis of the knee and fibromyalgia. Clin Interv Aging. 2014;9:939–944. doi:10.2147/CIA.S60330
130. Ortega E, Bote ME, Giraldo E, Garcia JJ. Aquatic exercise improves the monocyte pro- and anti-inflammatory cytokine production balance in fibromyalgia patients. Scand J Med Sci Sports. 2012;22(1):104–112. doi:10.1111/j.1600-0838.2010.01132.x
131. Kadetoff D, Lampa J, Westman M, Andersson M, Kosek E. Evidence of central inflammation in fibromyalgia — increased cerebrospinal fluid interleukin-8 levels. J Neuroimmunol. 2012;242(1–2):33–38. doi:10.1016/j.jneuroim.2011.10.013
132. Kosek E, Altawil R, Kadetoff D, et al. Evidence of different mediators of central inflammation in dysfunctional and inflammatory pain — interleukin-8 in fibromyalgia and interleukin-1 β in rheumatoid arthritis. J Neuroimmunol. 2015;280:49–55. doi:10.1016/j.jneuroim.2015.02.002
133. Ortega E, Garcia JJ, Bote ME, et al. Exercise in fibromyalgia and related inflammatory disorders: known effects and unknown chances. Exerc Immunol Rev. 2009;15:42–65.
134. Garcia JJ, Cidoncha A, Bote ME, Hinchado MD, Ortega E. Altered profile of chemokines in fibromyalgia patients. Ann Clin Biochem. 2014;51(Pt 5):576–581. doi:10.1177/0004563213506413
135. Grossman E, Goldstein DS, Hoffman A, Wacks IR, Epstein M. Effects of water immersion on sympathoadrenal and dopa-dopamine systems in humans. Am J Physiol. 1992;262(6 Pt 2):R993–R999. doi:10.1152/ajpregu.1992.262.6.R993
136. Johansen LB, Pump B, Warberg J, Christensen NJ, Norsk P. Preventing hemodilution abolishes natriuresis of water immersion in humans. Am J Physiol. 1998;275(3 Pt 2):R879–888. doi:10.1152/ajpregu.1998.275.3.R879
137. Semiz EA, Hizmetli S, Semiz M, et al. Serum cortisol and dehydroepiandrosterone-sulfate levels after balneotherapy and physical therapy in patients with fibromyalgia. Saudi Med J. 2016;37(5):544–550. doi:10.15537/smj.2016.5.15032
138. Connelly TP, Sheldahl LM, Tristani FE, et al. Effect of increased central blood volume with water immersion on plasma catecholamines during exercise. J Appl Physiol. 1990;69(2):651–656. doi:10.1152/jappl.1990.69.2.651
139. Sramek P, Simeckova M, Jansky L, Savlikova J, Vybiral S. Human physiological responses to immersion into water of different temperatures. Eur J Appl Physiol. 2000;81(5):436–442. doi:10.1007/s004210050065
140. Bote ME, Garcia JJ, Hinchado MD, Ortega E. Fibromyalgia: anti-inflammatory and stress responses after acute moderate exercise. PLoS One. 2013;8(9):e74524. doi:10.1371/journal.pone.0074524
141. Naumann J, Sadaghiani C. Therapeutic benefit of balneotherapy and hydrotherapy in the management of fibromyalgia syndrome: a qualitative systematic review and meta-analysis of randomized controlled trials. Arthritis Res Ther. 2014;16(4):R141. doi:10.1186/ar4603
142. Hauser W, Urrutia G, Tort S, Uceyler N, Walitt B. Serotonin and noradrenaline reuptake inhibitors (SNRIs) for fibromyalgia syndrome. Cochrane Database Syst Rev. 2013;(1):CD010292. doi:10.1002/14651858.CD010292
143. Hauser W, Wolfe F, Tolle T, Uceyler N, Sommer C. The role of antidepressants in the management of fibromyalgia syndrome: a systematic review and meta-analysis. CNS Drugs. 2012;26(4):297–307. doi:10.2165/11598970-000000000-00000
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.