")
Back to Journals » Advances in Medical Education and Practice » Volume 11
Impact of University Mergers on Admission of Medical Students in China
Authors Hou J, Xu M, Wang W, Kolars JC , Ke Y
Received 3 February 2020
Accepted for publication 30 April 2020
Published 19 May 2020 Volume 2020:11 Pages 351—358
DOI https://doi.org/10.2147/AMEP.S248210
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Jianlin Hou,1,* Maoyi Xu,2,* Weimin Wang,3 Joseph C Kolars,4 Yang Ke5
1Institute of Medical Education & National Center for Health Professions Education Development, Peking University, Beijing, People’s Republic of China; 2China Medical Tribune, Beijing, People’s Republic of China; 3Health Science Center, Peking University, Beijing, People’s Republic of China; 4University of Michigan Medical School, Ann Arbor, MI, USA; 5School of Oncology, Peking University, Beijing, People’s Republic of China
*These authors contributed equally to this work.
Correspondence: Yang Ke Email [email protected]
Objective: Mergers of health science faculties in China have resulted in two different admission pathways for medical students. A uniform-code model prioritizes admission to a specific institution with secondary assignment to major. A separate-code model prioritizes admission directly to a school within an institution. This study investigates the impact of these two admission pathways on medical student selection and on the satisfaction of students with their major.
Methods: Medical students at 16 medical schools across China completed a questionnaire survey. Descriptive calculation, chi-square tests, and probit models were used for analysing the data.
Results: A total of 3132 completed surveys were included in the analysis. Compared with the students admitted under the uniform-code pathway, a significantly larger proportion of the students admitted under the separate-code pathway had medicine as the first preferred major (89.6% vs 79.6%, p=0.000); compared with those students enrolled into medicine not as their first preferred major, a significantly larger proportion of students enrolled into medicine as their first preferred major were willing to study medicine if choosing again (80.1% vs 62.4%, p=0.000) or to recommend the major to other students (73.3% vs 65.2%, p=0.000). Probit models showed that medical students admitted under the separate-code admission pathway were more likely to choose medicine as their first preferred major at application (β=0.96, p=0.000); medical students admitted into medical school as their first preferred major were more likely to be willing to study medicine if choosing again (β=0.53, p=0.000) or to recommend the medical major to other students (β=0.18, p=0.010).
Conclusion: Separate-code admission is more likely to result in matriculants who choose medicine as their first preferred major and are more likely to be intrinsically interested in medicine than those applicants assigned to medicine from the uniform admission process.
Keywords: university merger, admission, selection, medical students, China
Background
The relationship of medical schools to universities in China has been changing. Since the 1950s, health sciences faculties (HSFs) including medicine, nursing, public health and dentistry have remained separate from other faculties within universities. Integration of HSFs into comprehensive universities started in the early 1990s. In 1998, the Ministry of Education (MOE) issued four principles to guide and encourage mergers: co-construction, adjustment, cooperation, and consolidation. Mergers were intended to promote inter-disciplinary communication and optimize allocation of educational resources. From 1990 to 2013, there were 76 mergers between HSFs and universities, involving 98 HSFs, with the peak in year 2000 when 20 mergers took place. Since 2007, mergers occurred less frequently and only two mergers took place in 2013. Mergers follow one of the two approaches: 1) HSFs merge with comprehensive universities or other educational institutions to form a new comprehensive university; 2) two or more HSFs merge to form a new HSF. When mergers resulted in new comprehensive universities, challenges regarding the integration of different administrative approaches of the resulting programs were common. For example, the mergers at Peking University and at Shanghai Jiao Tong University led to the establishment of health science centers (including medicine and other health sciences) with administrative practices that are relatively independent of the university. However, many other mergers led to an integration of management processes (referred to as a comprehensive university-running pattern).1–3 The two different administrative approaches after merger may have substantial differences regarding medical student selection.
Student selection is an important area in medical education, which impacts the supply of physicians, the provision of medical services by future physicians, and the quality of life of those selected.4 Selection factors vary widely between countries and may include prior academic performance and educational attainment, specialized aptitude tests, interviews, references, personal statements, and admission tests such as the Medical College Admissions Test (MCAT) in the United States, the Undergraduate Medicine and Health Sciences Admission Test (UMAT) in Australia and New Zealand, and the Health Professions Admission Test in Ireland (HPAT-Ireland).5–8
In China, the College Entrance Examination (CEE), a nation-wide examination managed by the MOE, is the primary admission determinant for high school students seeking entrance to medical education and other university programs. More than 90% of students are admitted through the CEE pathway which requires applicants to rank their preferred universities on their application form using the admission code of the university. Some universities utilize only one universal admission code for all schools within the institution. This is referred to as the uniform-code admission model. With this model, student admission is prioritized to their preferred university, followed by their preferred major as the second priority. Alternatively, some universities allocate different admission codes to different schools within the institution, which allows students to be admitted directly into the specific schools that they preferred. This is referred to as the separate-code admission model.9
For both admission models, students also need to rank-order their preferred majors using major codes and also indicate whether they are willing to be arranged into other majors that they have not ranked. Schools will rank-order applicants based on their CEE scores and admit those who have listed the program as their first preferred major as long as minimum score thresholds are satisfied. Students with CEE scores that do not result in placement into their first choice will then be placed into other majors if they indicated willingness in the application form to be arranged into other open programs. This policy of placement into majors was implemented with the resumption of the CEE in 197710. It is worth noting that in the Chinese culture, many students will prioritize a preferred university over a preferred major; these students will then comply with the assignment to a major other than their first choice, so as to avoid being left to the second round of selection by less preferred universities or not admitted by any university.11 For example, among 454 freshmen of a pharmaceutical university, 41.4% of students were not admitted into the major as their first choice.12
After the merger into comprehensive universities, most HSFs enrolled students using the uniform-code admission model. A few universities (eg, Peking University, Shanghai Jiao Tong University, Southeast University, and Fudan University) that kept substantive autonomy of health professional education regarding its management and organization utilized their own separate-code admission scheme and process.1,13,14
Mergers resulting in the adoption of the uniform-code model may have negative impacts on the admission of medical students. First, it may degrade the reputation of medical schools as individual institutions. Second, under the uniform-code admission pattern, the CEE score of medical applicants was ranked together with all the other applicants, resulting in greater competition. Studies have found that medical applicants admitted through this pathway had higher CEE scores. For example, the minimal threshold CEE score of applicants selected into Shanghai Medical University (before merger) had been lower than that of Shanghai Medical School of Fudan University (after merger). Third, though it seems that higher CEE scores indicate greater academic performance of students and higher admission scores of universities indicate better ranking and reputation among examinees, this resulted in some students seeking medicine to avoid certain universities with high admission score requirements.14
Universities using the uniform model may have fewer applicants with medicine as their first preferred major, resulting in more matriculants to the medical school who had prioritized other majors. Several studies have noted that students assigned to lower-ranked preferences for their major lacked interest and motivation in learning that may lead to mental health issues and poor academic performance relative to students who were admitted according to their first preferred major.12,15,16 For example, before the merger, about 90% of the matriculants at Shanghai Medical University listed this institution as their first choice. However, after the merger with Fudan University, this percentage dropped substantially. A study of 3rd-year health professional students in Fudan University showed that students admitted in line with their first choice accounted only for 29.6% of the total cohort; students assigned to health science from other majors accounted for 30.9%, of which 24.4% had no interest in health science. One option open to students is the opportunity to change their majors in the second semester of their freshman year. When the time came, the number of students who applied for major change was 4.8% (3/62) in those admitted in line with their first choice, but as high as 33.8% (24/71) in those assigned to health science programs despite other preferences.17 Similarly, before merging, all matriculants at Nanjing Railway Medical College were admitted according to their first choice for the program. However, in the first year after their merger with Southeast University, the uniform-code admission resulted in more than two thirds of the admitted students to health profession programs who were assigned despite their preferences for other majors (eg, finance, technology). Compared with previous years, the CEE scores of admitted students improved but the failing rate did not decrease and in fact, increased for some courses. Many of these health professional students were not interested in health sciences. Among students admitted in 2004, 32% applied to change their majors out of the health profession programs.18
An alternative approach of maintaining separate-code admission pattern could help health sciences faculties admit more students who are really aspiring to health sciences. When Southeast University adopted the independent admission for its health sciences majors for the first time in 2005, all the students were admitted according to their first choice. Although the CEE scores of health professional students were slightly lower than that of other majors in the university, not all examinees with higher scores were suitable for health sciences as their motivation for learning was directed towards other professional aspirations and interests.18
The impact of university mergers on the admission of health professional students has raised many concerns.1,13,14,17,19-21 However, most of the previous research on this topic was limited by selective sampling, small sample size, or more descriptive methodology with resulting limitations in generalizability. An approach using large-scale survey data and more sophisticated analysis is needed. To the best of our knowledge, there are no research reports on the impact of university mergers on medical student admissions.
The aim of this study is to explore the impact of admission models after university mergers on medical student selection and on students’ preference for medicine as a major using nation-wide data and inferential analysis methods. We hypothesize that: 1) The separate-code admission pathway results in a higher likelihood of medical schools matriculating students who prefer to study medicine than the uniform-code admission pathway; 2) medical students admitted into medicine as their first preferred major are more likely to be interested in the major and remain within the course of study.
Methods
Participants and Procedure
The survey was part of a situation analysis of China’s health professional education which was approved by the MOE. Full-time medical students in the second year of their curriculum at 16 medical schools across China were recruited in this study. Twelve medical schools were sampled from those with undergraduate medical programs, stratified by location, ownership (public or private), and whether or not they have been designated a Project 211 universities (ie, the 112 key universities receiving prioritized funding in a series of education reforms to address challenges for the 21st century beginning in 199522). In addition to the stratified sampling, another four top universities (also Project 211 universities) were added for convenience purposes as being typical or representative schools. At each of these medical schools, hard copies of questionnaire were distributed to medical undergraduate students and then submitted collectively.
Ethics and Consent to Participation
The study was submitted to and approved by Peking University Institutional Review Board. Informed consent was obtained from study participants.
Questionnaire
The tool used in this study is a self-administered questionnaire with 71 items of fixed-response/open-ended questions. It consisted of basic characteristics of the students and their family, learning experiences, along with assessment of medical education, financial status, and career preference upon graduation. The questionnaire was developed by Hou and select authors after reviewing relevant literature and consulting education experts in China.
Analysis
Participants’ responses were summarized using descriptive analysis, including the calculation of percentages, means, and standard deviations. Chi-square tests were used to compare those students enrolled into medicine as their first preferred major with those who were not and in relation to the participants’ admission type (Uniform-code admission pathway vs separate-code admission pathway), satisfaction with their major, willingness to study medicine if choosing again, willingness to recommend the major to other students. Next, probit regression was used to explore the determinants of the probability, respectively, for being enrolled into medicine as the 1st preferred major (Model 1), being willing to study medicine if choosing one more time (Model 2), being willing to recommend the major to other students (Model 3). The key independent variable entered into Model 1 was the admission type. The key independent variable for other two models was the major arrangement (admitted in line with the 1st preferred major or not). In each model, the effect of the key independent variable on the dependent variable was adjusted for covariates regarding the characteristics of the participants, their families, and their medical schools (Appendices 2–4).
Epi Data 3.1 was used to double enter the data. All analysis was conducted using Stata SE14.0. P value was set at 0.05 to indicate significant differences.
Results
Descriptive Statistics
A total of 4103 completed questionnaires were collected in the survey. Since factors like college preference and professional intention were involved, 3132 surveys completed by students who had not predetermined their career choice were analysed (Appendix 1). The mean age was 20 years (SD=1.2). Most of the participants were female (61.2%), of Han ethnicity (91.2%), from rural areas (52.8%), lived in a township or village before 15 years old (53.9%), had their high school education in counties (58.1%), and had parents who achieved a middle-school education level (46.8% for father, 39.4% for mother). Most were admitted into medical school in the second round (53.8%), under separate-code pathway (60.4%), and applied to medicine as their first preferred major (85.7%). A majority of the participants reported “Fair” (34.3%) or “Like” (48.3%) when assessing the satisfaction with their major, and were willing to study medicine if presented with the opportunity to choose again (77.6%), to recommend the major to other students (72.1%), and to be employed in the medical field when graduate (95.2%).
Chi-Square Tests
Table 1 demonstrates the results from chi-square tests. Compared with the students admitted into medical school through the uniform-code pathway, a significantly larger proportion of the students admitted into medical school through the separate-code pathway had medicine as the first preferred major (89.6% vs 79.6%, p=0.000). About half (48.9%) of the medical students enrolled in medicine as their first preferred major indicated that they “like” the major, while nearly half (44.7%) of those who were arranged into medicine choose “fair” when assessing the attractiveness of their major. Compared with students enrolled into medicine with other preferred majors, a significantly larger proportion of the students enrolled into medicine as their first preferred major were willing to study medicine if choosing again (80.1% vs 62.4%, p=0.000), to recommend the major to other students (73.3% vs 65.2%, p=0.000).
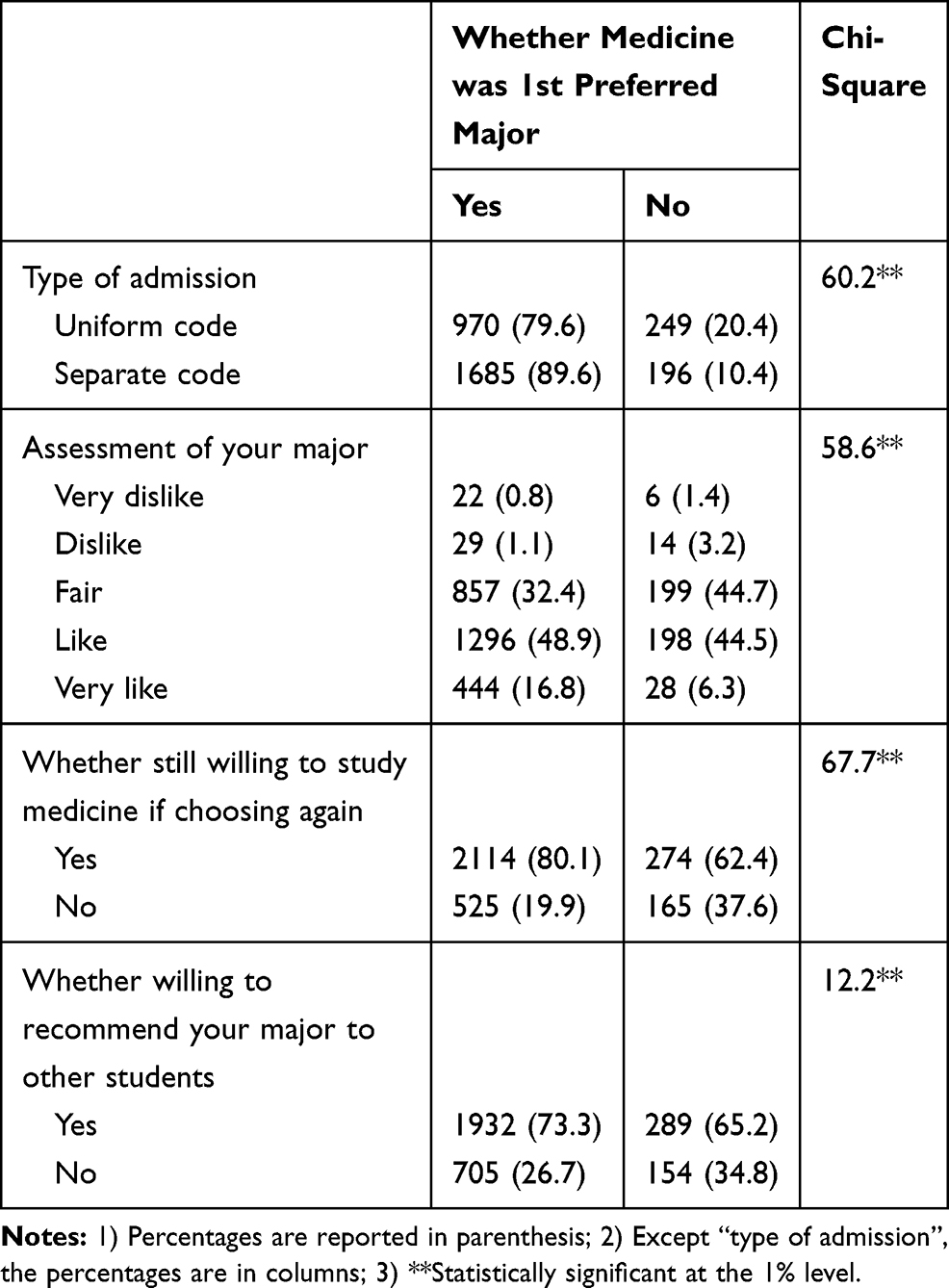 |
Table 1 Results of Chi-Square Tests |
Probit Models
Table 2 demonstrates the results from three probit models. Medical students admitted under the separate-code admission pattern were more likely to choose medicine as their first preferred major at application (β=0.96, p=0.000) (Model 1). Medical students admitted into medical school as their first preferred major were more likely to be willing to study medicine if choosing again (β=0.53, p=0.000) (Model 2) or to recommend the medical major to other students (β=0.18, p=0.010) (Model 3).
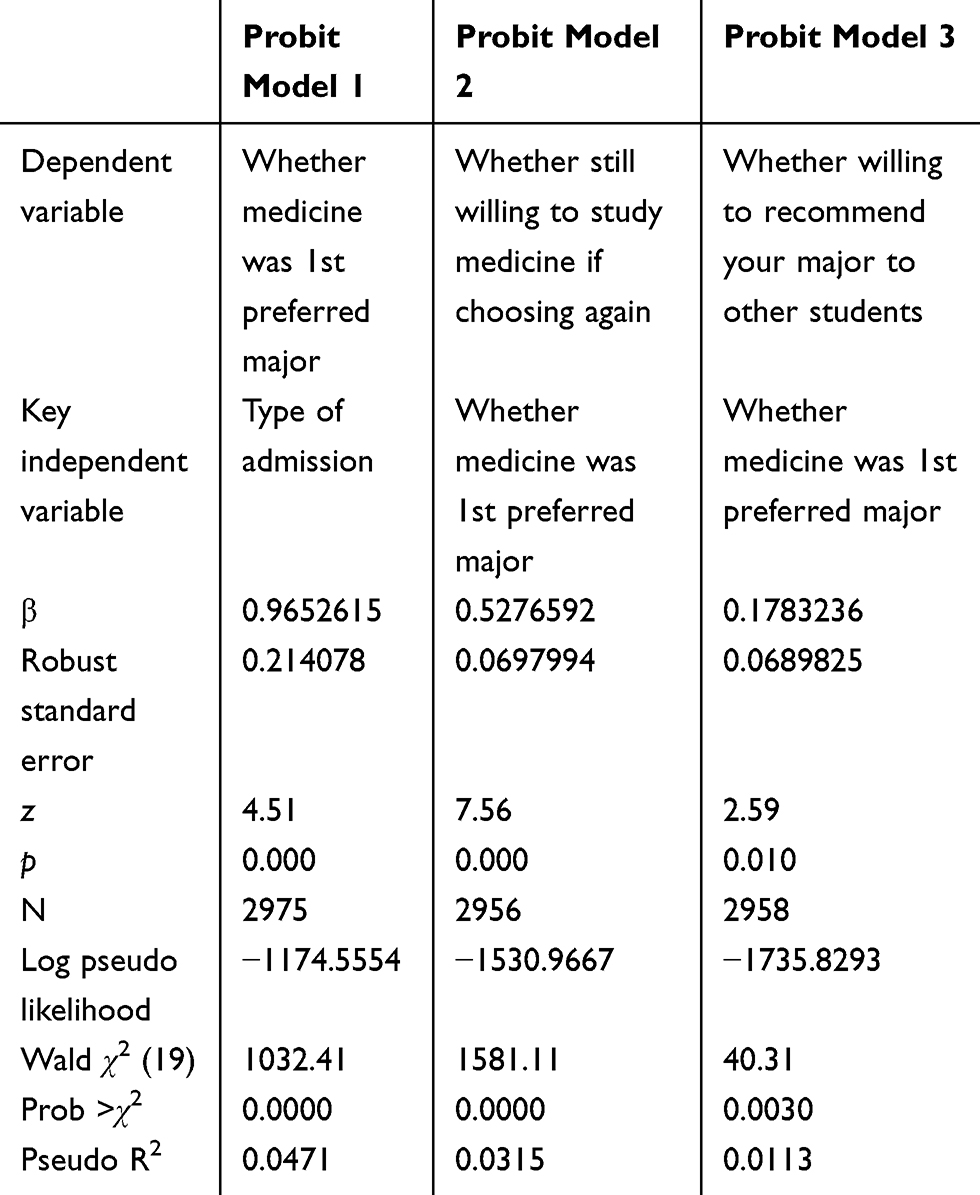 |
Table 2 Summary Results of Probit Model Estimations |
Discussion
In our study, we found that under the separate-code admission pathway, more medical students were admitted into medicine as their first preferred major, compared with those who were admitted under the uniform-code admission pathway. Also, medical students who were admitted into medicine as their first preferred major are more likely to be intrinsically interested in the major and to adhere to medicine.
Our results confirmed previous findings that uniform-code admission pathway may increase the proportion of students who were assigned into medicine despite preferences for other majors.1,13,14 By using a uniform-code approach, medical schools are actually offering places to those applicants who are not initially interested in studying medicine. In order to be accepted into a top or preferred university, these applicants may compromise their ability to choose a preferred major. In comparison, those applicants who are really interested in studying medicine may not apply because of the high admission score under the uniform-code admission pathway14. They may also be attracted to those majors which had much higher admission score than medical schools before the merger, so as not to “waste” their CEE score.
Our study results also contributes to previous research findings that applicants who were assigned into medicine despite preferences for other majors may lack interest and motivation in learning, with a higher tendency to drop out of medicine.20,21 Considering the large amount of investment needed for medical education, this is obviously a waste of educational resources. Also, previous research reported that after the uniform-code admission model was implemented, medical students did not demonstrated better academic performance despite having better CEE scores. In addition, many students seem to have anti-learning attitudes and mental health issues along with poor academic performance.18 This is not surprising as students who lack autonomy in directing their learning (ie, the choice of their major) may lack motivation in studying.
China’s medical schools may be missing applicants who have the potential to be excellent doctors because of an over reliance on the CEE scores. Under the uniform-code admission pathway, too much focus is put on the CEE score of applicants, by universities, by medical schools, and by applicants themselves. In many parts of the world with advanced health care systems, it is believed that more criteria should be used in selecting medical school applicants,4 including prior academic performance, cognitive aptitudes, and non-academic attributes.5,6 Furthermore, many developed countries recognized quite early that academic performance (ie, the intellect of medical applicants), should not be the only criteria for selection of medical applicants; the science of medicine must be combined with the humanistic attributes of caring. Service to patients is at the center of medical professionalism. Therefore, in addition to assessing the ability to learn complicated knowledge and skills, medical schools selection process should also include evaluation of applicants’ altruism, communication skills, and personality. These innovative reforms in medical school selection should also be made clear to the applicants and their families, so as to help applicants to make better informed decision and foster a self-selection before application.
The study results suggest that admission into medical schools at comprehensive university should change from uniform-code admission to separate-code admission in order to admit students who are intrinsically interested in medicine. Alternatively, while keeping the high admission score under the uniform-code admission pathway, universities should provide more opportunities for freshman and sophomore to change their majors at the early stages of training. This would allow those students who do not have sufficient CEE scores for the medical school at a top or preferred university to begin with other majors and then transfer into medicine if sufficiently qualified. Another strategy to consider would be to rely only on categorical admission into a broader category at a preferred university (eg, Health Sciences) with differentiation into a specific major (eg, Medicine) at this end of the first year. This would allow students to make a more informed decision and have more academic preparation before embarking on their preferred major.
Finally, it should be realized that medicine may not be regarded as an attractive major by many high school students in China because of “high input but low output”23 ie, in addition to longer duration of education and more stressful courses for medical students, working as a doctor in China suffers from low pay, demanding workload, and often unsatisfactory doctor–patient relationships.24–26 In the past few years, declines in the willingness to study medicine as well as the quality of admitted medical students have been reported.27,28 If these issues remain unaddressed, China’s medical schools are likely to be challenged by shortfalls in admissions with those who do matriculate not benefiting from more holistic admission criteria.
Our study has several limitations. First, although this is a nation-wide study with a sampling response of 4103 students from16 medical schools, only students who had not predetermined their career choice (n=3132, 76%) were included in the analysis. The exclusion of the other students might generate bias. Second, the process of conducting the survey among sampled schools might not be uniform and the return rates were not determined. Therefore, potential bias cannot be fully excluded. Third, though key confounding factors were adjusted in the probit models, there might still be residual confounding effects we have not considered. However, the highly significant coefficient found in our study is strong evidence of associations, which are less likely to be adjusted away by a few covariates. Fourth, there was no examination of effect modification or interaction between covariates. For example, it was possible that the effect of being admitted in medicine as the first preferred major (admission type) varies by sex, or Hukou (ie, the household registration system) and enrolment type may jointly affect a student’s willingness to continue their career in medicine. However, the study was not designed to address these points.
Conclusions
For medical schools, separate-code admission pathways are preferred over uniform-code admission pathways to maximize enrolment of applicants choosing medicine as their first preferred major. Students admitted under separate-code admission pathways are more likely to be intrinsically interested in medicine than those students who are assigned into medicine despite preferences for other majors. Therefore, admission into medical schools at comprehensive university should change from uniform-code admission to separate-code admission pathways. Alternatively, universities should employ broader categorical admission pathways and provide more opportunities for freshman and sophomore to change their majors at the early stage of training.
Abbreviations
HPAT, Health Professions Admission Test; HSF, Health sciences faculties; MCAT, Medical College Admissions Test; MOE, Ministry of Education; CEE, College Entrance Examination; MLE, Maximum likelihood estimation; SD, Standard deviation; UMAT, Undergraduate Medicine and Health Sciences Admission Test.
Ethics and Consent to Participation
The study was submitted to and approved by Peking University Institutional Review Board. Informed consent was obtained from study participants.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Dong S Whether or not should medical schools adopt the separate-code admission pattern?. China Education Daily; October 27, 2012. (in Chinese)
2. Ke Y. Thoughts on medical education practice after merged into the comprehensive university for five years. Med Educ. 2005:1–4. (in Chinese).
3. Ke Y. Review of university merger after ten years and recognition of the specialty of medical education. Chin J Med Educ. 2011;31(6):801–803. (in Chinese).
4. Yaghmaei M, Yazdani S, Ahmady S. Medical student selection and society: lessons we learned from sociological theories. Med J Islam Repub Iran. 2016;30:443.
5. O Sullivan DM, Moran J, Corcoran P, et al. Medical school selection criteria as predictors of medical student empathy: a cross-sectional study of medical students, Ireland. BMJ Open. 2017;7(7):e16076.
6. Sladek RM, Bond MJ, Frost LK, et al. Predicting success in medical school: a longitudinal study of common Australian student selection tools. BMC Med Educ. 2016;16:187. doi:10.1186/s12909-016-0692-3
7. Mcmanus IC, Iqbal S, Chandrarajan A, et al. Unhappiness and dissatisfaction in doctors cannot be predicted by selectors from medical school application forms: a prospective, longitudinal study. BMC Med Educ. 2005;5:38. doi:10.1186/1472-6920-5-38
8. Mcmanus IC, Dewberry C, Nicholson S, et al. Construct-level predictive validity of educational attainment and intellectual aptitude tests in medical student selection: meta-regression of six UK longitudinal studies. BMC Med. 2013;11:243. doi:10.1186/1741-7015-11-243
9. You J How is admission organized by undergraduate programs? Chinese Consumer News; July 14, 2004. (in Chinese)
10. Yu L. Major arrangement does not equal to losing your preferred major. J Coll Admission. 2008;6:24. (in Chinese).
11. Kong H. Principles determine the result—not overlooking separate-major admission principles. J Coll Admission. 2013;6:25–28. (in Chinese).
12. Ji X, Zhang F. Study on the motivation and adaption of students who were admitted via major arrangement. Pharm Sci Educ. 2011;2:59–61. (in Chinese).
13. Yu J, Sha W The autonomous admission policy of higher education will be adjusted. Nanning Daily; May 12, 2005. (in Chinese)
14. Tan J Fudan University Shanghai Medical School will separately admit students this year. Health News; June 21, 2013. (in Chinese)
15. You Y, Cao J, Zhao C. Analysis on the study situation of students who were admitted via major arrangement. Exam Wkly. 2012;90:162–163. (in Chinese).
16. Huang Y, Deng R, Zhu M, et al. Analysis on the learning adaption of nursing student who were admitted via major arrangement. J Gen Pract Nurs. 2013;1:1–2. (in Chinese).
17. Wang Q, Hu M, Huang J. Study on the sense of professional and adaption of campus after medical education institutions were merged into comprehensive universities. Chin Higher Med Educ. 2011;5:14–15. (in Chinese).
18. Xu C, Li T, Tong W. Analysis on the influence of university merger on the source of medical students and suggestions on responding measures. J Med Educ Explorat. 2006;5(6):571–573. (in Chinese).
19. Xu L. Economic analysis of university merging in China—take the merging of Fudan University and Shanghai Medical University as an example. China Higher Education Evaluation. 2003;1:18–22. (in Chinese).
20. Meng X, Tan J Many problems exist in the consolidation of higher education institutions. Health News; June 11, 2010. (in Chinese)
21. Gu M. Unpredictable changes in university merge. Chin Hosp Director. 2011;10:52–54. (in Chinese).
22. Yaisawarng S, Ng YC. The impact of higher education reform on research performance of Chinese universities. China Econ Rev. 2014;31:94–105. doi:10.1016/j.chieco.2014.08.006
23. Cao S, Tan Q, Li J Does good students not study medicine and medical schools trouble with admission shortfall? Nanfang Daily; August 14, 2015. (in Chinese)
24. Shan HP, Yang XH, Zhan XL, et al. Overwork is a silent killer of Chinese doctors: a review of Karoshi in China 2013–2015. Public Health. 2017;147:98–100. doi:10.1016/j.puhe.2017.02.014
25. Shen Y, Hao X, Guo T. Physician deaths from overwork should arouse greater attention in China. Int J Cardiol. 2018;256:23. doi:10.1016/j.ijcard.2017.06.116
26. He AJ. The doctor–patient relationship, defensive medicine and overprescription in Chinese public hospitals: evidence from a cross-sectional survey in Shenzhen city. Soc Sci Med. 2014;123:64–71. doi:10.1016/j.socscimed.2014.10.055
27. Jin R, Liu X, Zhang J, et al. Are medical undergraduate really unwilling to apply for clinic medicine speciality? Based on the quality of 5-year medical undergraduates. Chin J Health Policy. 2018;11(2):74–77. (in Chinese).
28. Chen B, Wang C. Analysis and thoughts on the quality of medical undergraduate admission in Beijing. China Health Hum Resour. 2015;6:84–88. (in Chinese).
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.