")
Back to Journals » Journal of Asthma and Allergy » Volume 15
Impact of the COVID-19 Pandemic on Incidence of Asthma Exacerbations and Hospitalizations in US Subspecialist-Treated Patients with Severe Asthma: Results from the CHRONICLE Study
Authors Moore WC , Ledford DK, Carstens DD, Ambrose CS
Received 23 February 2022
Accepted for publication 8 August 2022
Published 31 August 2022 Volume 2022:15 Pages 1195—1203
DOI https://doi.org/10.2147/JAA.S363217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Wendy C Moore,1 Dennis K Ledford,2 Donna D Carstens,3 Christopher S Ambrose4
1Wake Forest School of Medicine Department of Internal Medicine, Section on Pulmonary, Critical Care, Allergy and Immunologic Diseases, Winston-Salem, NC, USA; 2Morsani College of Medicine, University of South Florida, and James A. Haley Veterans’ Hospital, Tampa, FL, USA; 3BioPharmaceuticals Medical, AstraZeneca, Wilmington, DE, USA; 4BioPharmaceuticals Medical, AstraZeneca, Gaithersburg, MD, USA
Correspondence: Wendy C Moore, Wake Forest School of Medicine Department of Internal Medicine, Section on Pulmonary, Critical Care, Allergy and Immunologic Diseases, Medical Center Boulevard, Winston-Salem, NC, 27157, USA, Tel +1 336-716-7765, Fax +1 336-716-7277, Email [email protected]
Purpose: Patients with severe asthma (SA) are at an increased risk of asthma-related hospitalizations and exacerbations. Despite concerns that COVID-19 circulation would increase exacerbations of SA, anecdotal reports suggest that social distancing and exposure avoidance may have led to reduced exacerbations.
Patients and methods: CHRONICLE is an ongoing noninterventional observational study of 3100 subspecialist-treated patients with SA. Eligible adults (≥ 18 years of age) have (1) current use of monoclonal antibody (ie, biologic) therapy for SA, (2) use of maintenance systemic corticosteroids (mSCS) or other systemic immunosuppressants for ≥ 50% of the prior 12 months for SA, or (3) persistently uncontrolled asthma while treated with high-dosage inhaled corticosteroids with additional controllers. For enrolled patients, electronic medical records were reviewed to record all exacerbations and asthma-related hospitalizations. Descriptive analyses were conducted of the monthly incidence of exacerbations, exacerbation-related visits to the emergency department (ED), and asthma hospitalizations from July 2018 through July 2021.
Results: Exacerbations, exacerbation-related ED visits, and hospitalizations decreased since April 2020. Exacerbations in 2020 were 20% to 52% lower in April through August relative to the same months in 2019. Exacerbations remained lower than the prior year through May 2021. Similar results were observed by United States (US) census region, with an earlier decrease in exacerbation rates in the western US versus other regions. Across all months, exacerbation rates were lower among biologic recipients.
Conclusion: In a clinical cohort of subspecialist-treated patients with SA, there was a meaningful reduction in exacerbations, exacerbation-related ED visits, and asthma hospitalizations following COVID-19–related stay-at-home orders and social distancing recommendations. Reasons for these reductions are likely multifactorial, including reduced viral infections due to less social contact and altered patient behavior.
Keywords: management/control, healthcare resource use
Introduction
An estimated 5% to 10% of individuals with asthma have severe disease, which typically requires subspecialist care.1,2 Patients with severe asthma (SA) are at an increased risk of experiencing exacerbations.3 Environmental exposures including allergens, air pollution, viruses, bacteria, and stress are often driving factors in the onset of exacerbations.3 Further, exacerbations often lead to increased rates of adverse outcomes including increased costs of care, hospitalizations, and mortality.3 An estimated 12% of patients in the United States (US) with SA will require an asthma-related hospitalization at least once within a 12-month time frame.4
Despite concerns that asthma could be a risk factor for severe COVID-19 disease and that COVID-19 might increase the disease burden of asthma, reports suggest that asthma was not a significant risk factor for severe COVID-19 and that COVID-19–related recommendations for social distancing and exposure avoidance may have reduced the incidence of asthma exacerbations in both adults and children.5–8 Patients with SA generally have regular physician visits to monitor their disease control and may have experienced restricted access to healthcare as a result of distancing efforts during the pandemic.9 The impact of the COVID-19 pandemic on the longitudinal incidence of exacerbations and hospitalizations in adults with SA in the US has not been well-described. The ongoing observational CHRONICLE study of US subspecialist-treated patients with confirmed SA was initiated in 2018 and thus has provided a unique opportunity to evaluate this question based on ongoing, consistent, longitudinal data collection before and during the COVID-19 pandemic.
Methods
Study Participants
The design of the ongoing CHRONICLE study (ClinicalTrials.gov identifier: NCT03373045) has been described in detail previously.4 The definition for SA is in accordance with the European Respiratory Society (ERS)/American Thoracic Society (ATS) guidelines. Patients are adults (≥ 18 years of age) currently receiving care from subspecialist physicians at a participating site. In addition, to align with the patient population in the International Severe Asthma Registry, patients are required to meet ≥ 1 of the following criteria: (1) current use of Food and Drug Administration (FDA)-approved monoclonal antibody therapy for SA, (2) use of maintenance systemic corticosteroids (mSCS) or other systemic immunosuppressants for ≥ 50% of the prior 12 months for SA, or (3) persistently uncontrolled asthma (per ERS/ATS guidelines) while treated with high-dosage inhaled corticosteroids with additional controllers. Per protocol, sites approach all eligible patients for enrollment in CHRONICLE.
Data Collection
Exacerbations and asthma-related hospitalizations are ascertained by review of the electronic medical record, beginning 12 months before patient enrollment, with updates every 6 months after enrollment. An asthma exacerbation is defined as an event requiring hospitalization or requiring treatment with ≥ 3 days of oral corticosteroids or ≥ 1 corticosteroid injection.
Statistical Analysis
Data were analyzed for patients who were enrolled in the study between February 2018 and November 2021. Monthly incidence rates of asthma exacerbations, exacerbation-related visits to the emergency department (ED), and asthma hospitalizations were calculated from July 2018 through the last month with a sufficient sample based on data reported (July 2021).
Rates of exacerbations, exacerbation-related ED visits, and asthma hospitalizations were analyzed for all enrolled patients. Monthly exacerbation rates were calculated by US Census region and by treatment category (those receiving biologics, mSCS, or treatment without biologic or mSCS use), based on each patient’s treatment during each month. For treatment-category–specific rates, moving 3-month averages were calculated due to small sample sizes and imprecision in the monthly rates. Results were reported descriptively with no formal statistical testing.
Approximate dates of initiation and termination of COVID-19 stay-at-home orders for each state were obtained from a report by the US Centers for Disease Control and Prevention (CDC).10
Results
There were 3100 patients enrolled in CHRONICLE between February 2018 and November 2021. The mean age of enrolled patients was 54 years. Most patients were female (69%) and identified as White race (74%; Table 1). Over one-half of patients received care from a pulmonologist (53%), and 57% had commercial health insurance. The study sites for CHRONICLE are distributed throughout the US, and 46% of patients reported suburban residence. The number of sites per state/territory is shown in Figure 1.
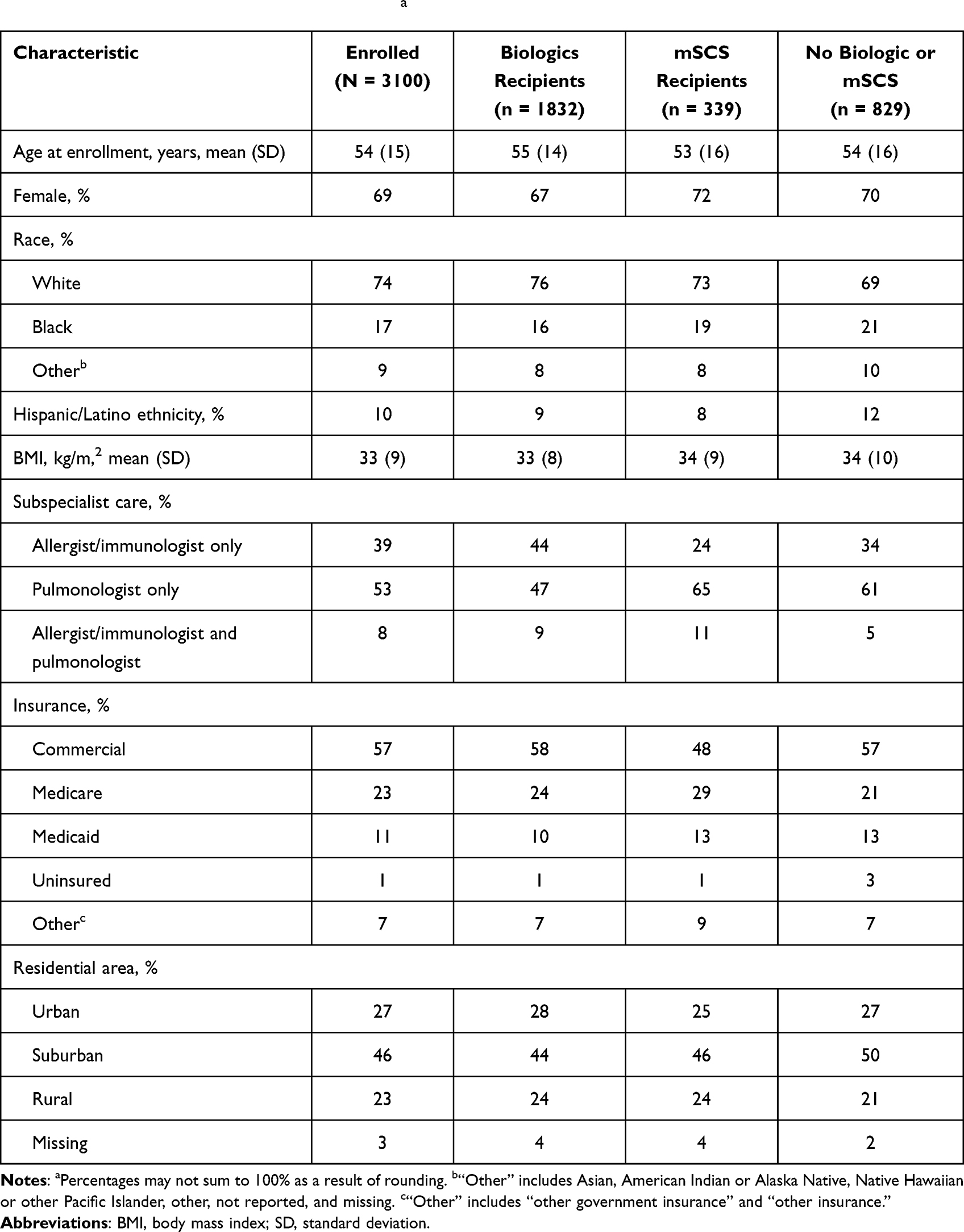 |
Table 1 Patient Characteristics at Enrollmenta |
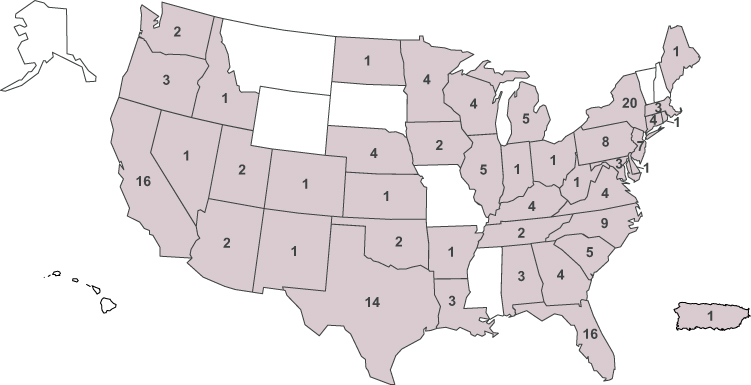 |
Figure 1 Distribution of CHRONICLE sites across the United States. |
The overall rate of subspecialist-reported asthma exacerbations by month from July 2018 through July 2021 is shown in Figure 2. Following initiation of stay-at-home orders, school and business closures, and masking and social distancing requirements, asthma exacerbations decreased in April 2020. Asthma exacerbations were lower than the prior year through May 2021. Relative to the same months in 2019, exacerbations in 2020 were 20% to 52% lower in April through August.
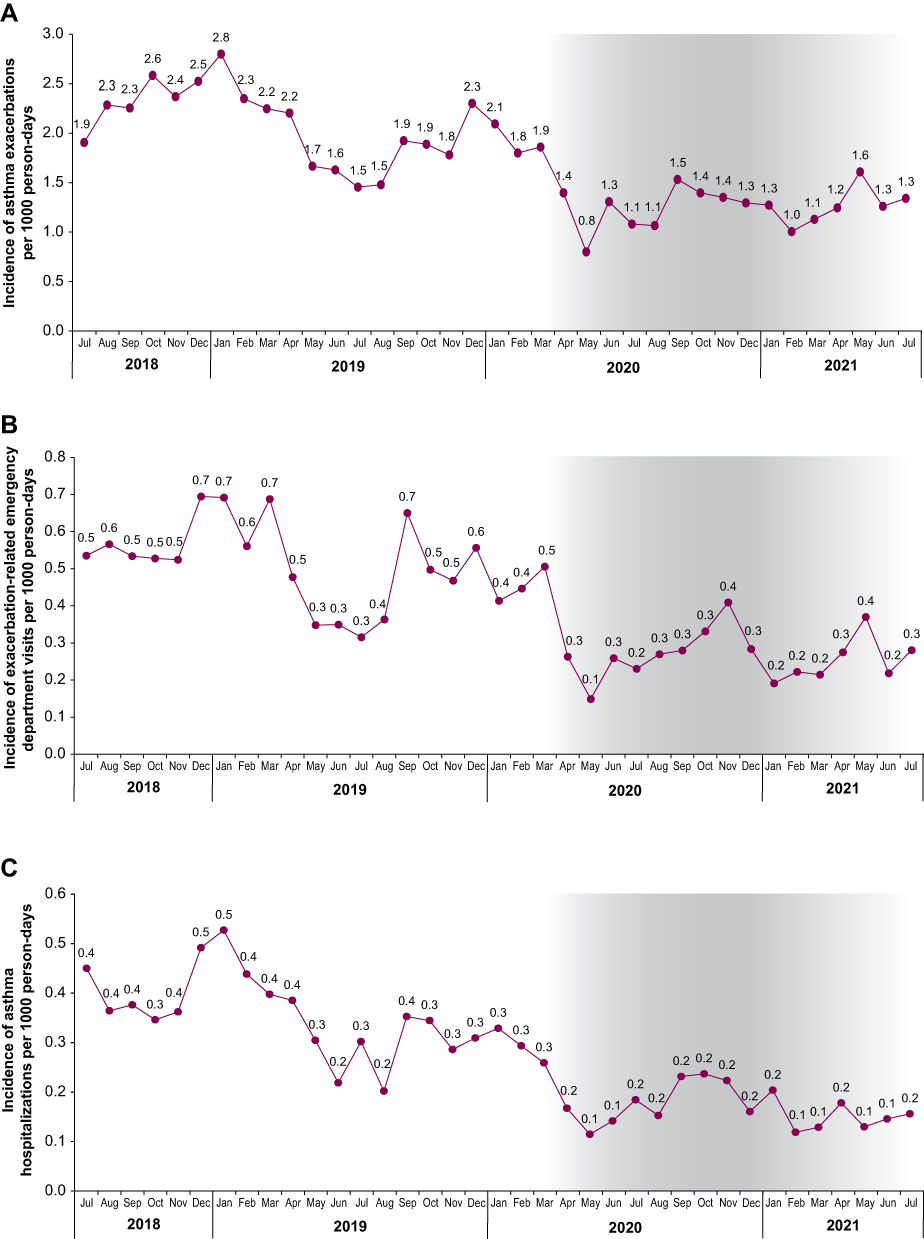 |
Figure 2 Overall rates of (A) asthma exacerbations, (B) exacerbation-related emergency department visits, and (C) asthma hospitalizations by month from July 2018 through July 2021. (A–C) Gray bands represent the implementation of state-level COVID-19 restrictions. |
Overall rates of exacerbation-related ED visits and hospitalizations decreased concurrently with asthma exacerbations in April 2020 (Figure 2). Exacerbation-related ED visits were lower than the prior year through May 2021, whereas asthma hospitalizations were lower than the prior year through April 2021. Relative to the same months in 2019, exacerbation-related ED visits were 26% to 57% lower in April through August in 2020. Similar results were observed by US Census region, with an initial decrease in the exacerbation rate in April in the western US and May in other regions. Relative to the same months in 2019, asthma hospitalizations in 2020 were 25% to 62% lower in April through August 2020.
At enrollment, 66% of patients were receiving biologics, 12% were receiving mSCS, and 30% were not receiving biologics or mSCS. A small percentage of patients (7%) received both biologics and mSCS. Analysis of exacerbation rates by treatment category revealed a similar decrease in exacerbation rates across all treatment groups (Figure 3). The exacerbation rate was lowest for biologic recipients across all months observed. The proportion of patients who were receiving biologics increased from 56.9% in quarter 3 of 2018 to 68.3% in quarter 2 of 2021 (Figure 4).
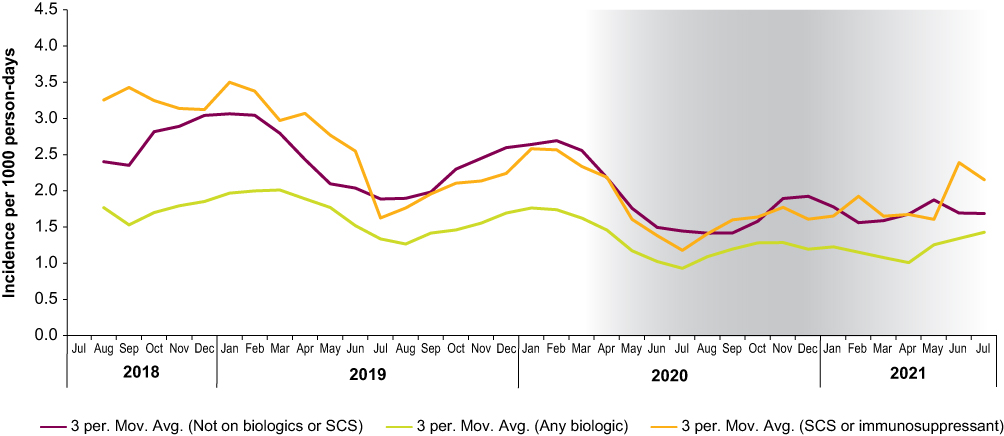 |
Figure 3 Monthly exacerbation rates by treatment category: 3-month moving averages. Gray bands represent the implementation of COVID-19 restrictions. Biologic use and SCS use were not mutually exclusive. Abbreviations: 3 per. Mov. Avg., moving 3-month averages; SCS, systemic corticosteroids. |
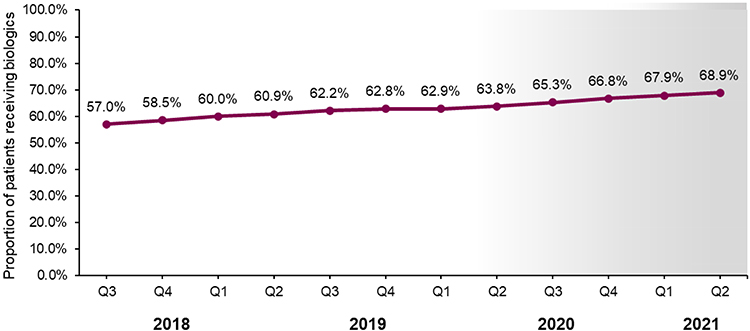 |
Figure 4 Proportion of patients receiving treatment with biologics from 2018 through 2020. The gray band represents the implementation of COVID-19 restrictions. Abbreviation: Q, quarter. |
Discussion
In this real-world study of US patients with SA, decreases in exacerbations, exacerbation-related ED visits, and asthma hospitalizations were observed following the implementation of COVID-19 stay-at-home orders and other societal disruptions in 2020 compared with the previous year. After stay-at-home orders were lifted, rates of asthma-related hospitalizations and exacerbations remained below prior-year rates through the middle of 2021, consistent with continued behavioral changes among patients and communities. Across all months observed, exacerbation rates were lower among recipients of biologics compared with recipients of mSCS and those not receiving biologics or mSCS. Results were also similar across geographical regions. An earlier onset in the western US most likely reflected the earlier stay-at-home order in California, where most of the study sites in the western US are located.
The decrease in exacerbations has implications for ongoing clinical studies of SA. With reduced exacerbation incidence, fewer patients will meet the definition of uncontrolled disease based on exacerbation frequency, which could negatively affect recruitment into ongoing studies of uncontrolled SA. Additionally, non-randomized observational studies of SA will need to account for COVID-19–related reductions in exacerbations.
The effects of stay-at-home orders, social distancing, and mask use resulting from the COVID-19 pandemic very likely reduced exposure to respiratory viruses as well as air pollutants.3,11,12 Sustained reductions in influenza virus, respiratory syncytial virus, parainfluenza viruses, and common human coronaviruses were specifically demonstrated in the US between March 2020 and Spring 2021.13 Decreased exposure to environmental factors known to drive adverse asthma outcomes are known to reduce rates of exacerbations and hospitalizations in patients with SA.3 In addition, decreased rates of exacerbations and hospitalizations could also be related to changes to clinic and hospital policies during the COVID-19 pandemic that reduced healthcare accessibility, potentially leading to reduced healthcare utilization for milder exacerbations.9
The ongoing and longitudinal nature of CHRONICLE has offered unique insights into trends in exacerbations temporally related to the COVID-19 pandemic.14 Exacerbation rates can decrease following enrollment in interventional observational trials, such as the Severe Asthma Research Program (SARP), due to increased patient engagement, education, and monitoring arising from study visits.14,15 In contrast, CHRONICLE is an observational study that does not require clinic visits or face-to-face patient contact beyond the initial enrollment visit, which itself generally occurs as part of routine care.14 Data collection in CHRONICLE is performed through medical record extraction by sites with no patient or physician interaction.14 In addition, patient care is not impacted or altered by study participation.14 This methodological strength of CHRONICLE suggests that findings of reduced exacerbations were primarily due to the COVID-19 pandemic, and not due to changes in patient care as a result of study participation.
Other studies have observed similar reductions in asthma exacerbations and hospitalizations.3,5,16–24 In the US, data from the PREPARE pragmatic trial of inhaled corticosteroid therapy in African American/Black and Hispanic/Latinx adult patients with moderate to severe asthma corroborate the reduction in exacerbations observed in real-world data sources.18 The relative reduction in exacerbations, as measured by the Asthma Exacerbations Questionnaire, was 41% in quarter 1 to quarter 2 of 2020 compared with the previous year.18 Similarly, several studies have observed decreases in pediatric exacerbations, hospitalizations, and ED visits among US children with asthma of any severity following the implementation of stay-at-home orders, compared with prior years.20,21,23,24 Another US report observed 76% fewer ED visits for children with asthma following stay-at-home orders, and a drop in subsequent asthma-related hospital admissions from 31% to 22%.17 Reduced exacerbation rates have also been reported in Japan, the United Kingdom, and the Netherlands following the implementation of COVID-19 stay-at-home orders in those countries compared with prior-year rates.5,16,19,25
Although several previous studies have investigated the impact of the real-world COVID-19 pandemic on adults with asthma,22,26,27 this analysis of CHRONICLE is the first to describe the effect of the COVID-19 pandemic on adults with subspecialist-confirmed SA in the US. Early in the pandemic, the CDC identified patients with moderate to severe asthma as a high-risk group that may experience greater morbidity from COVID-19, and thus encouraged avoiding asthma triggers, using prescribed asthma medications, and following a personalized asthma action plan.28,29 Relatedly, there is some evidence that the reductions in asthma exacerbations observed during the pandemic may also have been partially driven by increased disease awareness and medication adherence.30–32 An analysis of controller inhaler usage among patients with asthma or chronic obstructive pulmonary disease (COPD) found a 14.5% increase in medication adherence from the beginning of January 2020 to the end of March 2020.31 Patients with asthma may have thought they had a higher risk of contracting severe COVID-19 disease, which could contribute to positive changes in medication adherence.30 Further research is warranted to explore the effect of medication adherence on asthma exacerbations among patients with SA in the context of the global COVID-19 pandemic.
CHRONICLE’s limitations have been previously described, including differences in standard of care policies across study sites, missing medical record data, and patient recall bias. In addition, the site selection procedure was not random, thus the generalizability of the study results is unknown.14 CHRONICLE is limited to US adults with SA receiving subspecialist care and may not be generalizable to the broader SA population in the US or globally.14 Additional variables, including patient stress resulting from COVID-19, variation in biologic treatment administration, and general improvement in year-on-year asthma care may have also impacted exacerbation rates. This analysis was limited to descriptive statistics of observed associations.
Conclusion
In this real-world cohort of subspecialist-confirmed patients with SA, there was a reduction in exacerbations and asthma hospitalizations following US COVID-19–related stay-at-home orders and social distancing recommendations. Asthma exacerbations and hospitalizations increased to near baseline levels in the middle of 2021. These observations confirm a reduction in asthma exacerbation-related events among US adults with subspecialist-treated SA following COVID-19–related societal changes, as has been observed with US adults and children with less severe asthma and individuals with asthma in other countries. Reasons for these declines are likely multifactorial, including reduced viral infections due to less social contact, altered patient behavior, and possibly reduced healthcare utilization for asthma.
Abbreviations
ATS, American Thoracic Society; CDC, Centers for Disease Control and Prevention; COPD, chronic obstructive pulmonary disease; ED, emergency department; ERS, European Respiratory Society; FDA, Food and Drug Administration; mSCS, maintenance systemic corticosteroids; SA, severe asthma; SARP, Severe Asthma Research Program: US, United States.
Data Sharing Statement
CHRONICLE is an ongoing study; individual de-identified participant data cannot be shared until the study concludes. The full study protocol is available upon request of the corresponding author. Individuals who were or were not involved in the study may submit publication proposals to the study’s Publication Steering Committee by contacting the corresponding author.
Ethics Approval and Consent to Participate
The CHRONICLE study protocol received central institutional review board (Advarra, Columbia, MD) approval on November 3, 2017. Patients completed written informed consent. The CHRONICLE study is being performed according to ethical principles consistent with the Declaration of Helsinki, International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) Good Clinical Practices, Good Pharmacoepidemiology Practices, the Health Insurance Portability and Accountability Act (HIPAA), and applicable legislation for observational studies.
Acknowledgments
Medical writing services were provided by Karen Kurtyka, MPH, and Casey Demko, MS, of Oxford PharmaGenesis Inc., Newtown, PA, USA, in accordance with Good Publication Practice (GPP3) and funded by AstraZeneca, Gaithersburg, MD, USA. Portions of this manuscript were presented at the American Thoracic Society 117th International Conference, May 14–19, 2021.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported and funded by AstraZeneca.
Disclosure
Wendy C. Moore has participated in advisory boards conducted by AstraZeneca, Genentech, GlaxoSmithKline, Regeneron, and Sanofi. Dennis K. Ledford has been a consultant for AstraZeneca and GlaxoSmithKline and received speaker honoraria from ALK, AstraZeneca, Boehringer Ingelheim, Genentech/Roche, GlaxoSmithKline, Novartis, and Sanofi/Regeneron. Donna D. Carstens and Christopher S. Ambrose are employees and shareholders of AstraZeneca. The authors report no other conflicts of interest in this work.
References
1. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. doi:10.1183/09031936.00202013
2. Global Initiative for Asthma. Global strategy for asthma management and prevention; 2017. Available from: https://ginasthma.org/wp-content/uploads/2019/04/GINA-Severe-asthma-Pocket-Guide-v2.0-wms-1.pdf.
3. Denlinger LC, Heymann P, Lutter R, Gern JE. Exacerbation-prone asthma. J Allergy Clin Immunol Pract. 2020;8(2):474–482. doi:10.1016/j.jaip.2019.11.009
4. Trevor J, Lugogo N, Carr W, et al. Severe asthma exacerbations in the United States: incidence, characteristics, predictors, and effects of biologic treatments. Ann Allergy Asthma Immunol. 2021;127(5):579–587.e571. doi:10.1016/j.anai.2021.07.010
5. Abe K, Miyawaki A, Nakamura M, Ninomiya H, Kobayashi Y. Trends in hospitalizations for asthma during the COVID-19 outbreak in Japan. J Allergy Clin Immunol Pract. 2021;9(1):494–496.e491. doi:10.1016/j.jaip.2020.09.060
6. Patrucco F, Benfante A, Villa E, Principe S, Scichilone N, Solidoro P. Severe asthma and COVID-19: lessons from the first wave. J Asthma. 2022;59(2):239–242. doi:10.1080/02770903.2020.1861622
7. Skevaki C, Karsonova A, Karaulov A, Xie M, Renz H. Asthma-associated risk for COVID-19 development. J Allergy Clin Immunol. 2020;146(6):1295–1301. doi:10.1016/j.jaci.2020.09.017
8. Terry PD, Heidel RE, Dhand R. Asthma in adult patients with COVID-19. Prevalence and risk of severe disease. Am J Respir Crit Care Med. 2021;203(7):893–905. doi:10.1164/rccm.202008-3266OC
9. Eguiluz-Gracia I, van den Berge M, Boccabella C, et al. Real-life impact of COVID-19 pandemic lockdown on the management of pediatric and adult asthma: a survey by the EAACI Asthma Section. Allergy. 2021;76(9):2776–2784. doi:10.1111/all.14831
10. Moreland A, Herlihy C, Tynan MA, et al. Timing of state and territorial COVID-19 stay-at-home orders and changes in population movement—United States, March 1–May 31, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(35):1198. doi:10.15585/mmwr.mm6935a2
11. Gallo O, Bruno C, Orlando P, Locatello LG. The impact of lockdown on allergic rhinitis: what is good and what is bad? Laryngoscope Investig Otolaryngol. 2020;5(5):807–808. doi:10.1002/lio2.459
12. Partridge E, McCleery E, Cheema R, et al. Evaluation of seasonal respiratory virus activity before and after the statewide COVID-19 shelter-in-place order in northern California. JAMA Netw Open. 2021;4(1):e2035281. doi:10.1001/jamanetworkopen.2020.35281
13. Olsen SJ, Winn AK, Budd AP, et al. Changes in influenza and other respiratory virus activity during the COVID-19 pandemic — United States, 2020–2021. MMWR Morb Mortal Wkly Rep. 2021;70(29):1013–1019. doi:10.15585/mmwr.mm7029a1
14. Ambrose CS, Chipps BE, Moore WC, et al. The CHRONICLE study of US adults with subspecialist-treated severe asthma: objectives, design, and initial results. Pragmat Obs Res. 2020;11:77–90. doi:10.2147/POR.S251120
15. Denlinger LC, Phillips BR, Sorkness RL, et al. Responsiveness to parenteral corticosteroids and lung function trajectory in adults with moderate-to-severe asthma. Am J Respir Crit Care Med. 2021;203(7):841–852. doi:10.1164/rccm.202002-0454OC
16. de Boer G, Braunstahl G-J, Hendriks R, Tramper-Stranders G. Asthma exacerbation prevalence during the COVID-19 lockdown in a moderate-severe asthma cohort. BMJ Open Resp Res. 2021;8(1):e000758. doi:10.1136/bmjresp-2020-000758
17. Kenyon CC, Hill DA, Henrickson SE, Bryant-Stephens TC, Zorc JJ. Initial effects of the COVID-19 pandemic on pediatric asthma emergency department utilization. J Allergy Clin Immunol Pract. 2020;8(8):2774–2776.e2771. doi:10.1016/j.jaip.2020.05.045
18. Salciccioli JD, She L, Tulchinsky A, Rockhold F, Cardet JC, Israel E. Effect of COVID-19 on asthma exacerbation. J Allergy Clin Immunol Pract. 2021;9(7):2896–2899.e2891. doi:10.1016/j.jaip.2021.04.038
19. Shah SA, Quint JK, Nwaru BI, Sheikh A. Impact of COVID-19 national lockdown on asthma exacerbations: interrupted time-series analysis of English primary care data. Thorax. 2021;76(9):860–866. doi:10.1136/thoraxjnl-2020-216512
20. Sheehan WJ, Patel SJ, Margolis RHF, et al. Pediatric asthma exacerbations during the COVID-19 pandemic: absence of the typical fall seasonal spike in Washington, DC. J Allergy Clin Immunol Pract. 2021;9(5):2073–2076. doi:10.1016/j.jaip.2021.02.008
21. Guijon OL, Morphew T, Ehwerhemuepha L, Galant SP. Evaluating the impact of coronavirus disease 2019 on asthma morbidity: a comprehensive analysis of potential influencing factors. Ann Allergy Asthma Immunol. 2021;127(1):91–99. doi:10.1016/j.anai.2021.03.018
22. Ho KS, Howell D, Rogers L, Narasimhan B, Verma H, Steiger D. The relationship between asthma, eosinophilia, and outcomes in coronavirus disease 2019 infection. Ann Allergy Asthma Immunol. 2021;127(1):42–48. doi:10.1016/j.anai.2021.02.021
23. Hurst JH, Zhao C, Fitzpatrick NS, Goldstein BA, Lang JE. Reduced pediatric urgent asthma utilization and exacerbations during the COVID-19 pandemic. Pediatr Pulmonol. 2021;56(10):3166–3173. doi:10.1002/ppul.25578
24. Ulrich L, Macias C, George A, Bai S, Allen E. Unexpected decline in pediatric asthma morbidity during the coronavirus pandemic. Pediatr Pulmonol. 2021;56(7):1951–1956. doi:10.1002/ppul.25406
25. Davies GA, Alsallakh MA, Sivakumaran S, et al. Impact of COVID-19 lockdown on emergency asthma admissions and deaths: national interrupted time series analyses for Scotland and Wales. Thorax. 2021;76(9):867–873. doi:10.1136/thoraxjnl-2020-216380
26. Cao L, Lee S, Krings JG, et al. Asthma in patients with suspected and diagnosed coronavirus disease 2019. Ann Allergy Asthma Immunol. 2021;126(5):535–541.e532. doi:10.1016/j.anai.2021.02.020
27. Robinson LB, Wang L, Fu X, et al. COVID-19 severity in asthma patients: a multi-center matched cohort study. J Asthma. 2021;59(3):1–14.
28. Bouazza B, Hadj-Said D, Pescatore KA, Chahed R. Are patients with asthma and chronic obstructive pulmonary disease preferred targets of COVID-19? Tuberc Respir Dis. 2021;84(1):22–34. doi:10.4046/trd.2020.0101
29. Centers for Disease Control and Prevention. CDC updates, expands list of people at risk of severe COVID-19 illness [Press release]. Atlanta, GA, USA: Centers for Disease Control and Prevention; 2020 [June 25]. Available from: https://www.cdc.gov/media/releases/2020/p0625-update-expands-covid-19.html.
30. Arora N, Lowe D, Sarsour N, et al. Asthma care during COVID-19: differences in attitudes and expectations between physicians and patients. J of Asthma. 2021;59(5):1–7.
31. Kaye L, Theye B, Smeenk I, Gondalia R, Barrett MA, Stempel DA. Changes in medication adherence among patients with asthma and COPD during the COVID-19 pandemic. J Allergy Clin Immunol Pract. 2020;8(7):2384–2385.
32. Dhruve H, d’Ancona G, Holmes S, Dhariwal J, Nanzer AM, Jackson DJ. Prescribing patterns and treatment adherence in patients with asthma during the COVID-19 pandemic. J Allergy Clin Immunol Pract. 2021;10(1):100–107.e2. doi:10.1016/j.jaip.2021.09.032
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.