")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Impact of the Coronavirus Disease 2019 Pandemic on an Emergency Department Service: Experience at the Largest Tertiary Center in Taiwan
Authors Tsai LH , Chien CY , Chen CB, Chaou CH , Ng CJ , Lo MY, Seak CK, Seak JCY, Goh ZNL , Seak CJ
Received 18 July 2020
Accepted for publication 4 February 2021
Published 22 February 2021 Volume 2021:14 Pages 771—777
DOI https://doi.org/10.2147/RMHP.S272234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Li-Heng Tsai,1,2 Cheng-Yu Chien,1– 3 Chen-Bin Chen,1,2,4 Chung-Hsien Chaou,1,2 Chip-Jin Ng,1,2 Mei-Yi Lo,5 Chen-Ken Seak,6 Joanna Chen-Yeen Seak,6 Zhong Ning Leonard Goh,6 Chen-June Seak1,2,4,7
1Department of Emergency Medicine, Lin-Kou Medical Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 2College of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Department of Emergency Medicine, Ton-Yen General Hospital, Zhubei, Taiwan; 4Department of Emergency Medicine, New Taipei Municipal Tucheng Hospital, New Taipei City, Taiwan; 5Department of Nursing, Lin-Kou Medical Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 6Sarawak General Hospital, Kuching, Sarawak, Malaysia; 7Center for Quality Management, New Taipei Municipal Tucheng Hospital, New Taipei City, Taiwan
Correspondence: Chen-June Seak
Department of Emergency Medicine, Lin-Kou Medical Center, Chang Gung Memorial Hospital, No. 5, Fusing St., Guei-Shan Township, Taoyuan County 333, Taiwan
Tel +886-3-3281200 ext. 5235
Fax +886-3-3287715
Email [email protected]
Purpose: Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2) is an emerging contagious pathogen that has caused community and nosocomial infections in many countries. This study aimed to evaluate the impact of Coronavirus disease 2019 (COVID-19) on emergency services of the largest medical center in Taiwan by comparing emergency department (ED) usage, turnover, and admission rates before the COVID-19 outbreak with those during the outbreak.
Materials and Methods: A retrospective cohort study was conducted in the ED of the largest tertiary medical center in Taiwan. Trends of adult, non-trauma patients who visited the ED during February–April 2019 were compared with those during February–April 2020. The number of visits, their dispositions, crowding parameters, and turnover rates were analyzed. The primary outcome was the change in ED attendance between the two periods. The secondary outcomes were changes in hospital admission rates, crowding parameters, and turnover rates.
Results: During the outbreak, there were decreased non-trauma ED visits by 33.45% (p < 0.001) and proportion of Taiwan Triage and Acuity Scale (TTAS) 3 patients (p=0.02), with increased admission rates by 4.7% (p < 0.001). Crowding parameters and turnover rate showed significant improvements.
Conclusion: Comparison of periods before and during the COVID-19 outbreak showed an obvious decline in adult, non-trauma ED visits. The reduction in TTAS 3 patient visits and the increased hospital admission rates provide references for future public-health policy-making to optimise emergency medical resource allocations globally.
Keywords: emergency department, Coronavirus disease 2019, Taiwan Triage and Acuity Scale, Stratification to Prevent Overcrowding Taskforce, SPOT
Introduction
In recent decades, emergency department (ED) overcrowding and overuse has become a major healthcare problem in many countries. In Taiwan, the total number of ED visits per year increased from 10.2 million in 1997 (approximately 46.9 visits per 100 persons) to 11.8 million in 2018 (approximately 50.1 visits per 100 persons).1 Coronavirus disease 2019 (COVID-19) was first detected in late 2019, and the World Health Organization stated that there were 3,090,445 cases worldwide by April 30, 2020.2 Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2) is a new, emerging virus that is thought to be transmissible through respiratory droplets and direct contact,3 and community and nosocomial infections have been reported in many countries. ED staff, as frontline healthcare workers, have a high possibility of exposure to this contagious virus.
The first COVID-19 case in Taiwan was confirmed on January 21, 2020,4 and the first episode of nosocomial infection (involving eight people, including nursing staff, the hospitalized patient, the patient’s family members, and healthcare workers) was reported on February 28, 2020.1 Following this incident, the Ministry of Health and Welfare (MOHW) of Taiwan implemented several measures to inhibit the spread of the virus, including banning the entry of foreigners into the country and suggesting that the public avoid unnecessary hospital visits, maintain social distancing of more than one meter, use surgical masks in public areas, and frequently wash their hands; these recommendations were promoted through television, radio broadcasts, and the Internet.5 Taiwan Linkou Chang Gung Memorial Hospital (LCGMH), one of the largest hospitals in the world, immediately made its ED available to help manage the virus response during the outbreak period.6
This study aimed to evaluate the impact of COVID-19 on emergency services by comparing the usage, turnover, and admission rates of an ED before the COVID-19 outbreak with the equivalent data during the outbreak. Such an investigation could help to differentiate actual ED demand from non-essential ED demand, which could, in turn, inform quality-improvement policies.
Materials and Methods
Study Design and Setting
We conducted a retrospective cohort study through reviewing electronic medical charts from LCGMH. LCGMH, the largest tertiary care hospital located in northern Taiwan, has a capacity of 3406 beds; its ED contains 190 beds and two negative-pressure isolation rooms, and receives approximately 150,000 visits annually.6,7
Participant Selection
We analyzed data for visits to the medical center’s ED before (February–April 2019; hereafter ‘T1ʹ) and during (February–April 2020; hereafter ‘T2ʹ) the COVID-19 outbreak. Adult, non-trauma ED patients aged over 18 years were selected for the research (Figure 1). Trauma patients were excluded as, based on our experiences during the 2003 SARS pandemic, emergency services for trauma were not expected to be disrupted by the outbreak.
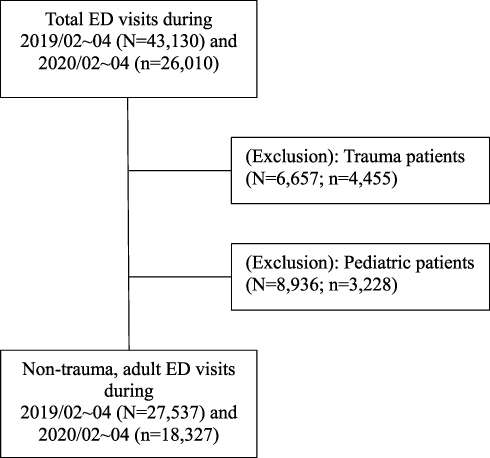 |
Figure 1 Study algorithm. |
Taiwan Triage and Acuity Scale (TTAS)
The TTAS levels8–10 are defined as follows – level 1: patient requiring immediate treatment, level 2: patient requiring treatment within 10 minutes, level 3: patient requiring management within 30 minutes, level 4: patient requiring management within one hour, level 5: patient requiring management within two hours. The full criteria for triaging can be found in Table 1. In general, TTAS levels 1–3 are categorized as emergency conditions.
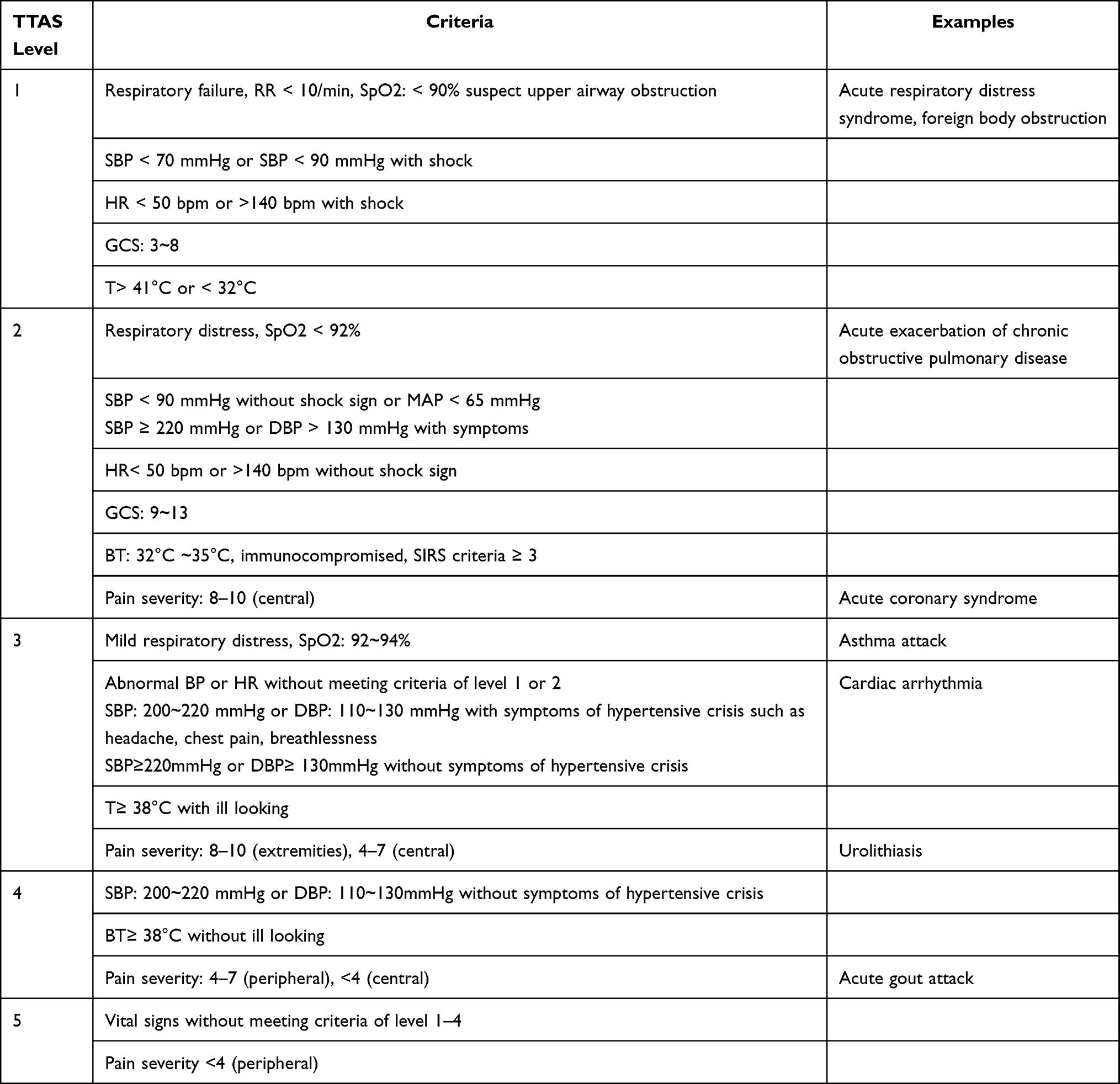 |
Table 1 Taiwan Triage and Acuity Scale (TTAS) |
Data Collection
A blinded, trained study assistant reviewed the de-identified computer-based registry records and conducted data extraction using a standard reporting template that contained clear definitions and codes. Data were collected from electronic charts, medical records, and nurses’ records, in particular each patient’s age and sex, primary reason for visiting the ED, ED diagnosis, time of visit, level of triage (according to TTAS), vital signs, and disposition. The number of ED patients awaiting general ward or intensive care unit (ICU) admission, the number of patients who stayed in the ED (at the scene or in an observation room), and the average waiting time for admission was also determined.
Patients who stayed at the scene (PSAS) were defined as patients whose disposition remained unresolved two hours after registration; meanwhile, patients who were placed in an observation room had a clear disposition: awaiting admission.
Outcome Measures
The primary outcome of this study was the difference between T1 and T2 regarding the composition of ED visits. The secondary outcomes included the differences between T1 and T2 regarding the hospital admission rates and variations in crowding and turnover parameters.
Statistical Analysis
Categorical data were reported as numerical values with percentages, and were compared across groups using chi-square tests. Meanwhile, continuous variables with normal distributions were reported as means and standard deviations, and were compared using Student’s t-test. Statistical analyses were performed using SPSS Statistics for Windows, Version 20.0 IBM Corp. P-values of less than 0.05 were considered to indicate statistical significance.
Ethical Approval
This study was approved by the Chang Gung Medical Foundation’s Hospital Ethics Committee on Human Research (IRB: 202000941B1). The study protocol was reviewed, and the study was exempted from the requirement of obtaining informed consent.
Results
Compared to T1, LCGMH saw a significant decrease in adult non-trauma ED visits (p<0.001) and unaccompanied ED visits (p<0.001) with a significant increase in number of patients brought in by emergency medical services (p<0.001) in T2. The number of patients triaged as TTAS 3 decreased significantly (p=0.02) during the pandemic, with a concurrent significant rise in TTAS 4 cases (p=0.03). Parameters of disease severity, in terms of cardiac arrests and use of mechanical ventilators, showed no significant difference between the two study periods (Table 2).
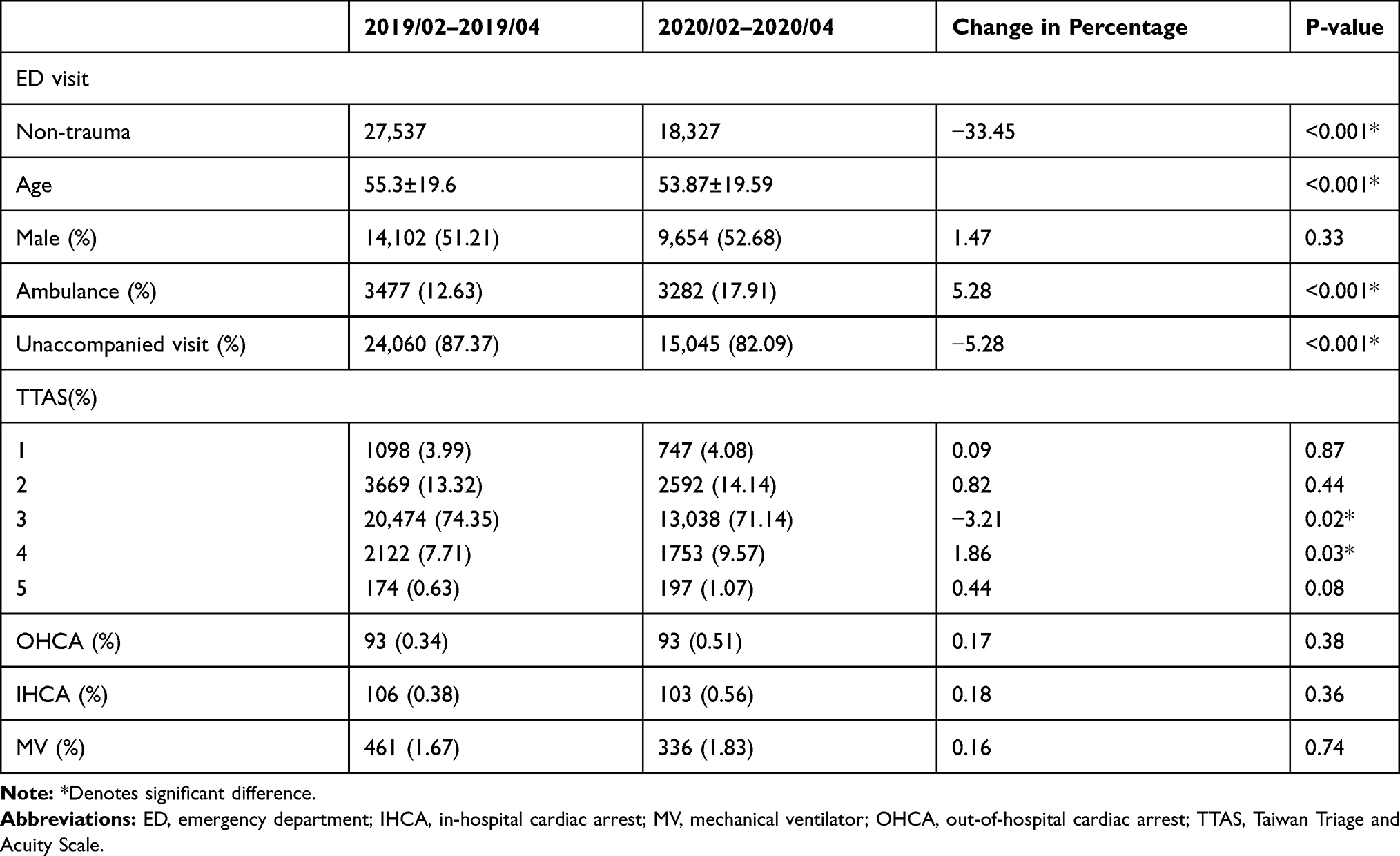 |
Table 2 Characteristics of the Adult, Non-Trauma ED Patients |
Regarding admission rates, T2 saw a significant rise in overall hospital admissions (p<0.001) with similar proportions of ward and ICU admissions, despite a significant and dramatic fall in ED visits by approximately a third (p<0.001). At the same time, the proportion of patients discharged from the ED significantly decreased in T2 (p<0.001) (Table 3).
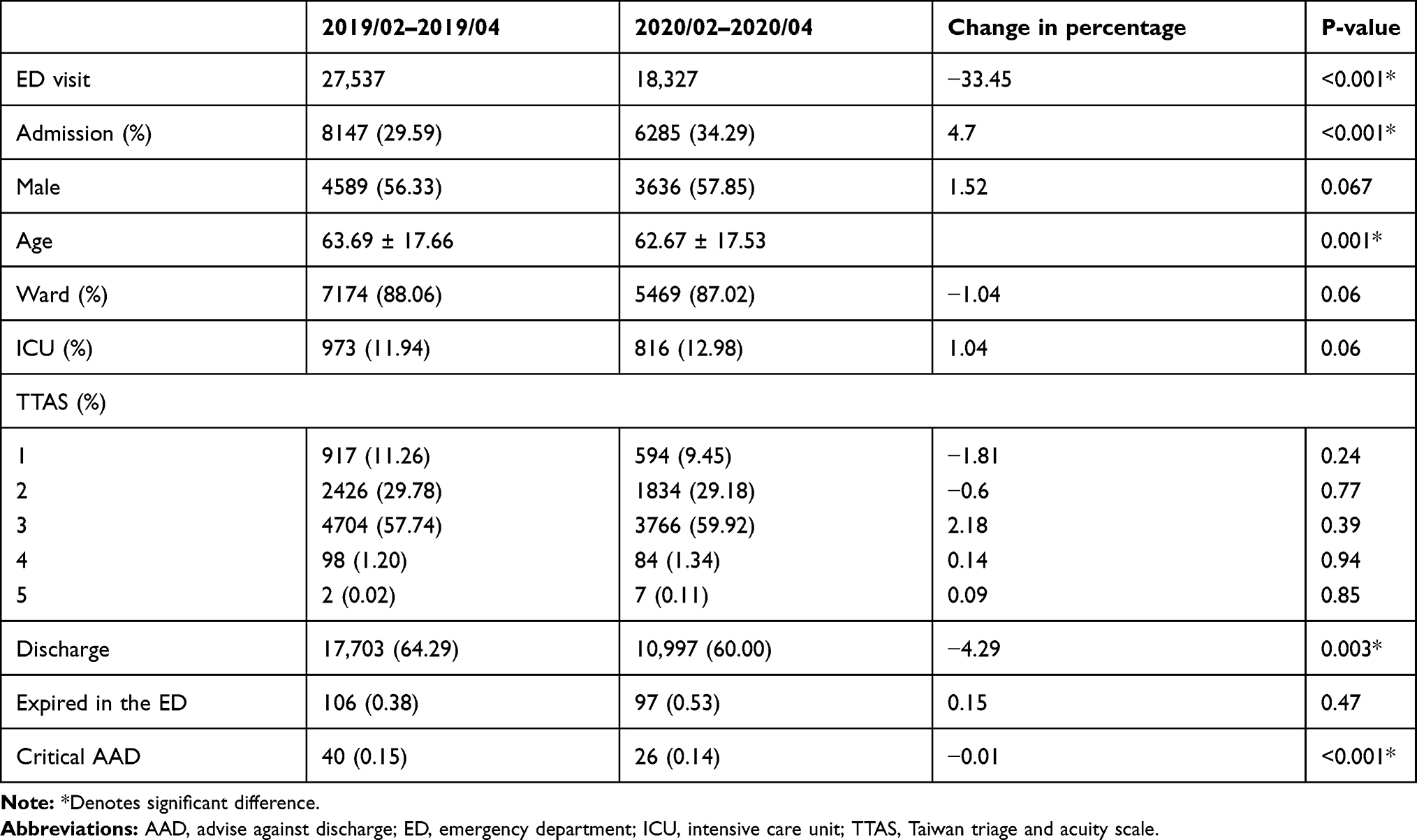 |
Table 3 Comparison of Admission Rate Among Adult, Non-Trauma ED Patients |
The number of PSAS was significantly lower during this period (p<0.001), as was the number of patients in observation rooms (p<0.001) and who stayed in the ED for >48 hours (p<0.001). Average waiting time for ward admission was significantly shorter during the outbreak (p<0.001) but average time to ICU admission was significantly longer (p<0.001) (Table 4).
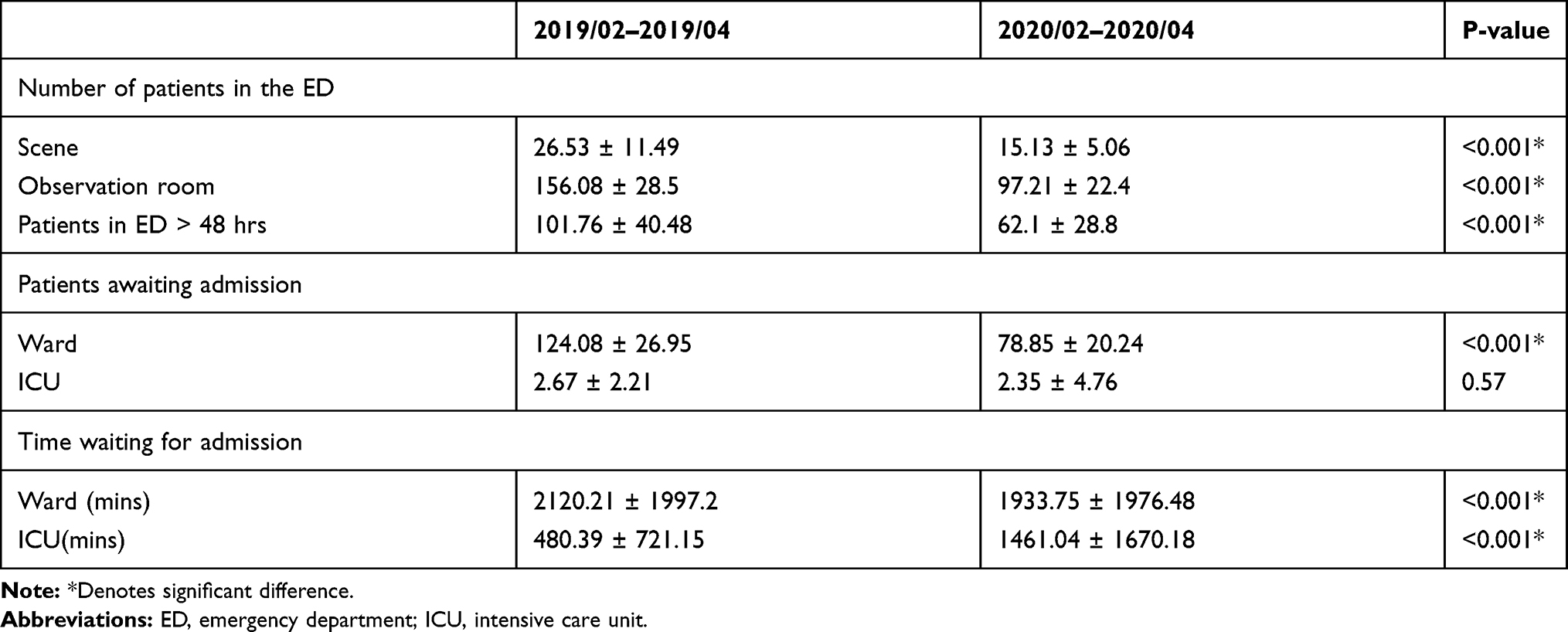 |
Table 4 Crowding Parameters and Turnover Rates for the ED |
Discussion
This study showed that, during the COVID-19 outbreak, there was a clear reduction in daily ED visits (33.45%) when compared to the pre-epidemic period (Table 2). We attribute this decline in ED visits solely to the impact of the COVID-19 pandemic and corresponding containment measures by the Taiwanese MOHW, with no other obvious confounding systemic changes in our healthcare setting during this period. This trend resembles that which was observed during the 2003 SARS outbreak,11 as well as the initial trends in other countries such as Italy during this current COVID-19 pandemic.12
Furthermore, a significant 5.28% reduction in patients visiting EDs unaccompanied was noted. These results show that the public-health policies that were implemented in Taiwan, which were informed by previous SARS experience, successfully reduced the number of unnecessary ED visits.13 In other words, a combination of public-health-policy promotion and people’s fear of visiting hospitals during the COVID-19 outbreak effectively reduced ED visits, thereby giving front-line ED staff more flexibility and capacity to respond to unpredictable situations and to screen uncertain cases.14 Nevertheless, those patients who indeed were more ill and required urgent medical attention presented themselves to the ED all the same, as evidenced by similar proportions of TTAS 1 and 2 patients across both periods.
The TTAS levels used in Taiwan are based on the patient’s chief complaint, vital signs, consciousness level, pain scale, and prehospital oxygen-dependent status, all of which indicate the urgency level.9 During T2, the decline in adult, non-trauma ED visits was mainly related to TTAS 3 patients (representing 3.21% of the decline in the total number of patients); the number of TTAS 3 patients reduced significantly by 7436 (36.32%) between T1 and T2. This suggests that during the pandemic, these patients chose to stay at home or seek alternatives, such as taking over-the-counter medications and visiting other local hospitals, before visiting the ED of a tertiary medical center. Despite that, there was no significant reduction in the visits of patients with TTAS 1 and 2 (18.22%) indicating sicker patients who indeed required emergency services still came to ED and admitted (38.63%). The percentage of TTAS 4 and 5 ED patients increased during the pandemic; a possible explanation for this result is that many patients with mild symptoms of upper respiratory infections feared that they had contracted COVID-19 and visited EDs to undergo screening.
The admission rates increased during T2 from 29.59% to 34.29%. This demonstrates that many of the ED visits during T2 were from patients with a higher need for inpatient care. The percentage of admissions accounted for by TTAS 1–3 patients was similar – 98.78% in T1 vs 98.55% in T2, suggesting that the association between TTAS level and likelihood of admission to hospital remained almost the same between the two periods. The percentage of patients discharged from the ED in T1 was higher (64.29% in T1; 60% in T2, p = 0.003), which may be due to a higher percentage of patients with non-critical illness visiting the ED during this earlier period.
Comparison of the crowding parameters15 in T1 and T2 showed that the total number of PSAS, those admitted to observation rooms, and patients who stayed in the ED over 48 hours all decreased significantly in T2 (Table 4). This may reflect patients’ and families’ fear of staying in the hospital, and resulted in more ward vacancies and a higher turnover rate.16 This is evidenced by the decrease in the number of patients awaiting admission and in the average time to admission. Previous studies have shown that crowding in ED environments can contribute to poor outcomes for ED patients.17 Improvement in crowding parameters and turnover rate during T2 allowed emergency staff to provide better patient care and optimise patient flow.
The decline in ED visits during the COVID-19 outbreak afforded an opportunity to monitor and evaluate the actual level of demand for emergency care in a tertiary medical center in Taiwan. Public-health policy, which advocates referral and a hierarchy of medical care, has long explored means of optimising emergency medical resource allocation in Taiwan; however, positive outcomes have remained elusive.18 Taiwan’s medical environment has changed in recent years, and now emphasises maximising tertiary care hospital development while gradually reducing the focus on community and local hospitals. This situation contributed to the phenomenon of patients immediately visiting medical centers with relatively minor or chronic illnesses. During the COVID-19 outbreak, the obvious decline in the amount of total adult, non-trauma ED visits, of which the majority were TTAS 3, could provide a profile for evaluating the actual demand for emergency medical resources, and could influence future policy-making regarding national health insurance payments.
Limitations
This study should be interpreted in the context of the following limitations.
First, the study was conducted at a single medical center in northern Taiwan within a limited time period, which may restrict the generalisability of our findings. More validation studies conducted in different regions and ED settings would be of interest. Second, no analysis of survival outcomes was conducted. Although the decline in adult, non-trauma ED visits was obvious, further studies investigating ED usage and efficiency could provide additional interesting results.
Conclusions
Comparison of periods before and during the COVID-19 outbreak showed a drastic decline in adult, non-trauma ED visits. The findings regarding the relative urgency of the ED visits (TTAS > 3) and the admission rates during this period could help inform future public-health policy-making to optimise emergency medical resource allocations worldwide.
Abbreviations
ED, emergency department; COVID-19, coronavirus disease 2019; SARS, severe acute respiratory syndrome; MOHW, Ministry of Health and Welfare; LCGMH, Linkou Chang Gung Memorial Hospital; TTAS, Taiwan Triage and Acuity Scale; ICU, intensive care unit; PSAS, patients who stayed at the scene.
Acknowledgments
We would like to thank the investigators of SPOT (Stratification to Prevent Overcrowding Taskforce) from Department of Emergency Medicine, Lin-Kou Medical Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan, Department of Emergency Medicine, New Taipei Municipal Tucheng Hospital, New Taipei City, Taiwan and Sarawak General Hospital, Kuching, Sarawak, Malaysia for their assistance in investigation. SPOT includes the following members: Feng-Lin Wang, Yi-Ling Chan, Chih-Huang Li, Hsien-Yi Chen, Chih-Chuan Lin, Kuang-Yu Niu, Chiao-Hsuan Hsieh, Yu-Shao Chou, Tzu-Heng Cheng, Chun-Wei Wu, Chia-Hau Chang, Chien-Lin Chen, Su-Ann Yong and Johan Seak.
Funding
This study was supported by the Ministry of Science and Technology of Taiwan [MOST 109-2314-B-182A-102-] and Chang Gung Memorial Hospital in Taiwan [CORPG3H0231, CORPG3H0191, CPRPG3D0012, and CMRPG3J1721] awarded to Chen-June Seak. The funder had no role in design of the study and collection, analysis, interpretation of data, and in writing the manuscript.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Ministry of Health and Welfare, Taiwan. Availabe from: https://dep.mohw.gov.tw/DOS/lp-1931-113.html.
2. World health organization (WHO) Coronavirus disease 2019 (COVID-19) situation report −101. Availabe from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200430-sitrep-101-covid-19.pdf?sfvrsn=2ba4e093_2.
3. Bi Q, Wu Y, Mei S, et al. Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: a retrospective cohort study. Lancet Infect Dis. 2020;20:911–919. doi:10.1016/S1473-3099(20)30287-5
4. Cheng SC, Chang YC, Fan Chiang YL, et al. First case of coronavirus disease 2019 (COVID-19) pneumonia in Taiwan. J Formos Med Assoc. 2020;119(3):747–751. doi:10.1016/j.jfma.2020.02.007
5. Wang CJ, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analytics, new technology, and proactive testing. JAMA. 2020;323:1341–1342. doi:10.1001/jama.2020.3151
6. Seak CJ, Liu YT, Ng CJ. Rapid responses in the emergency department of Linkou Chang Gung Memorial Hospital, Taiwan effectively prevents spread of COVID-19 among healthcare workers of emergency department during outbreak: lessons learnt from SARS. Biomed J. 2020;43(4):388–391. doi:10.1016/j.bj.2020.06.002
7. Tsai LH, Huang CH, Su YC, et al. Comparison of prehospital triage and five-level triage system at the emergency department. Emerg Med J. 2017;34(11):720–725. doi:10.1136/emermed-2015-205304
8. Lin YK, Niu KY, Seak CJ, Weng YM, Wang JH, Lai PF. Comparison between simple triage and rapid treatment and Taiwan Triage and Acuity Scale for the emergency department triage of victims following an earthquake-related mass casualty incident: a retrospective cohort study. World J Emerg Surg. 2020;15(1):20. doi:10.1186/s13017-020-00296-2
9. Ng CJ, Yen ZS, Tsai JC, et al. Validation of the Taiwan triage and acuity scale: a new computerised five-level triage system. Emerg Med J. 2011;28(12):1026–1031. doi:10.1136/emj.2010.094185
10. Ng CJ, Chien CY, Seak JC, et al. Validation of the five-tier Taiwan Triage and Acuity Scale for prehospital use by emergency medical technicians. Emerg Med J. 2019;36(8):472–478. doi:10.1136/emermed-2018-207509
11. Chen WK, Cheng YC, Chung YT, Lin CC. The impact of the SARS outbreak on an urban emergency department in Taiwan. Med Care. 2005;43(2):168–172. doi:10.1097/00005650-200502000-00010
12. Comelli I, Scioscioli F, Cervellin G. Impact of the COVID-19 epidemic on census, organization and activity of a large urban emergency department. Acta Biomed. 2020;91(2):45–49. doi:10.23750/abm.v91i2.9565
13. Huang HH, Yen DH, Kao WF, Wang LM, Huang CI, Lee CH. Declining emergency department visits and costs during the severe acute respiratory syndrome (SARS) outbreak. J Formos Med Assoc. 2006;105(1):31–37. doi:10.1016/S0929-6646(09)60106-6
14. Chen WK, Wu HD, Lin CC, Cheng YC. Emergency department response to SARS, Taiwan. Emerg Infect Dis. 2005;11(7):1067–1073. doi:10.3201/eid1107.040917
15. Stang AS, Crotts J, Johnson DW, Hartling L, Guttmann A. Crowding measures associated with the quality of emergency department care: a systematic review. Acad Emerg Med. 2015;22(6):643–656. doi:10.1111/acem.12682
16. Chang AM, Lin A, Fu R, McConnell KJ, Sun B. Associations of emergency department length of stay with publicly reported quality-of-care measures. Acad Emerg Med. 2017;24(2):246–250. doi:10.1111/acem.13102
17. Sun BC, Hsia RY, Weiss RE, et al. Effect of emergency department crowding on outcomes of admitted patients. Ann Emerg Med. 2013;61(6):605–611.e6. doi:10.1016/j.annemergmed.2012.10.026
18. Yan YH, Kung CM, Yeh HM. The impacts of the hierarchical medical system on national health insurance on the resident’s health seeking behavior in Taiwan: a case study on the policy to reduce hospital visits. Int J Environ Res Public Health. 2019;16(17):3167. doi:10.3390/ijerph16173167
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.