")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 12
Impact of Sugammadex Versus Neostigmine/Glycopyrrolate on Perioperative Efficiency
Authors Deyhim N, Beck A, Balk J, Liebl MG
Received 29 June 2019
Accepted for publication 26 September 2019
Published 31 January 2020 Volume 2020:12 Pages 69—79
DOI https://doi.org/10.2147/CEOR.S221308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Dean Smith
Niaz Deyhim,1,2 Amanda Beck,1 Jonathan Balk,1 Michael G Liebl3
1Department of Pharmacy Services, Houston Methodist Hospital, Houston, TX, USA; 2Department of Pharmacy Practice, University of Houston College of Pharmacy, Houston, TX, USA; 3Department of Pharmacy Services, Houston Methodist System, Houston, TX, USA
Correspondence: Amanda Beck
Department of Pharmacy Services, Houston Methodist Hospital, 6565 Fannin Street, DB1-09, Houston, TX 77030, USA
Tel +1 713 363 7342 Fax +1 713 4411225
Email [email protected]
Purpose: Neuromuscular blockade in the operating room necessitates the utilization of reversal agents to accelerate postoperative recovery and sustain operating room patient throughput. Cholinesterase inhibitors represent the historical standard of care for neuromuscular blockade reversal within anesthesia practice. Sugammadex, a synthetic gamma-cyclodextrin, was introduced to the market with evidence of more rapid and predictable reversal of neuromuscular blockade compared to alternative agents. Higher medication acquisition costs have limited more extensive use of sugammadex compared to that of neostigmine/glycopyrrolate. The purpose of this study was to examine the impact of sugammadex versus neostigmine/glycopyrrolate on perioperative efficiency to validate medication acquisition cost value.
Methods: A retrospective investigation was performed of patients with a surgical procedure at Houston Methodist Hospital from July 31, 2017 through August 1, 2018. The primary endpoint was time from reversal medication administration to operating room exit. Patient-specific doses were assessed to calculate average medication acquisition costs. The economic benefits of sugammadex were measured through review of average operating room and postanesthesia care unit costs per minute.
Results: There were a total of 640 surgical cases at Houston Methodist Hospital eligible for inclusion into the research study. The time from medication administration to operating room exit was significantly faster for sugammadex compared to neostigmine/glycopyrrolate (P< 0.001) upon univariate analysis. However, when measured with linear regression, the difference in operating room exit time between sugammadex and neostigmine/glycopyrrolate was no longer statistically significant (P=0.122). Medication acquisition cost review highlighted a difference of $178.20, favoring use of neostigmine/glycopyrrolate.
Conclusion: The utilization of sugammadex does not correlate to consequential time saved in the operating room or extrapolation to workflow capacity for increased surgical case volume. Consideration of the medication acquisition cost promotes more restrictive use of sugammadex to indications with clinical relevance.
Keywords: reversal, neuromuscular blockade, anesthesia, pharmacoeconomics
Introduction
Neuromuscular blockade necessitates the utilization of reversal agents in the operating room to accelerate postoperative recovery and sustain operating room patient throughput. Cholinesterase inhibitors represent the historical standard of care for neuromuscular blockade reversal within anesthesia practice.1 Sugammadex, a synthetic gamma-cyclodextrin, was introduced to the market with evidence of more rapid and predictable reversal of neuromuscular blockade compared to alternatives, such as neostigmine/glycopyrrolate.1,2 Its novel mechanism of action is mediated through the formation of water-soluble complexes at a one-to-one ratio with steroidal neuromuscular blocking agents.1,2 In addition to clinical efficacy, decreased incidence of postoperative residual curarization and reduced adverse sequelae, purported benefits of the medication, correspond to an improved patient safety profile with decreased treatment costs.1,2
Higher medication acquisition costs limit more extensive use of sugammadex compared to that of neostigmine/glycopyrrolate.2 However, the enhanced onset of neuromuscular blockade reversal may reduce comprehensive costs through the reduction of patient encounter time in the operating room (OR).1,2 To demonstrate the cost-effectiveness of sugammadex, the prompt recovery of muscle strength must be converted to a reduction of recovery time within clinical practice to permit increased staff productivity.2,3 Consideration of these components extrapolate to an optimized surgical workflow system with the capability to incorporate additional revenue-generating procedures within the OR schedule.4
A 2017 Cochrane systematic review indicated that sugammadex was 10.22 min (6.6 times) and 45.78 min (16.8 times) faster than neostigmine in reversing moderate and deep induced paralysis, respectively.5 Within a 2015 randomized control trial, the time between reversal agent administration and OR exit was observed to be shorter for sugammadex versus neostigmine/glycopyrrolate (19.9 vs. 24.1 min; P=0.020).3 Anesthetic theater time decreased from 143.5 ± 85.8 to 120 ± 71.2 min (P=0.01) with removal of sugammadex availability restrictions.6 Time within the postanesthesia care unit (PACU) remained consistently unchanged, however.6
Economic assessments theorized that reduction in OR recovery time may correlate with increased cost-efficacy.1,2,7,8 Shortened recovery time exhibited an inverse relationship with the minimum value of each minute of “saved” recovery time, increasing sugammadex cost-effectiveness.1,2 A 2010 systematic review estimated OR and PACU cost valuation of £4.44 per minute and £0.33 per minute for time saved, respectively.2 Sokolovic et al. demonstrated that a 13-min decrease in OR turnover time increased OR occupancy by 1 hr per day.1,9 Reduced mean OR turnover time between 10 and 19 min may reduce staffing costs by 2.5–4.0%.1,10 Shortened recovery duration by 5 to 10 min may permit up to 2.4% additional operations per planning period.1
Prior supposition of the fiscal benefits of sugammadex in relation to shortened OR occupancy and reduced recovery time is established through prospective trials. Limited research is available to examine the reliability of these results in practical settings without measures for experimental control.7 Further analysis is necessary to measure the pragmatic outcomes associated with sugammadex for extrapolation to multi-center cost-savings initiatives.
Hence, a retrospective review of sugammadex and neostigmine/glycopyrrolate utilization in real-world scenarios was conducted. This cost-effectiveness analysis assessed impact of sugammadex on OR and PACU occupancy as compared to neostigmine/glycopyrrolate. Results will be used in an effort to impact OR revenue and pharmacy department medication costs throughout the Houston Methodist system.
Materials and Methods
Trial Design
This study was approved as a quality improvement initiative by the Houston Methodist Research Institute Institutional Review Board. Therefore, patient consent to obtain data from the electronic medical record (EMR) system, Epic (Verona, Wisconsin), was not required. Patient data confidentiality was maintained and in compliance with the Declaration of Helsinki.
The Houston Methodist system comprises an academic medical center in the Texas Medical Center, Houston Methodist Hospital (HMH), and seven community hospitals. Sugammadex received approval for addition to the Houston Methodist formulary in March 2016. Restrictions to the medication were limited to anesthesiology service lines and intent to use within the OR. Neostigmine/glycopyrrolate previously served as the standard of care for reversal of neuromuscular paralysis.
The time period of this retrospective research study was from July 31, 2017 to August 1, 2018. Data were obtained from Epic (Verona, Wisconsin) with assistance of the Houston Methodist System Quality Operations and Analytics Department.
Patients admitted to HMH with a performed surgical procedure were included within the review. Exclusion criteria consisted of the following: neurosurgical or cardiac catheterization procedure, reversal agent administration within the PACU, extubation prior to reversal agent administration or procedure completion, sugammadex reversal of cisatracurium or succinylcholine, non-recorded pre-PACU/postreversal agent train-of-four, zero-minute time difference from procedure start or completion to reversal agent administration, missing endpoint documentation, and reversal with both sugammadex and neostigmine/glycopyrrolate.
OR and PACU Workflow
The ORs at HMH are scheduled to an allotted surgical case capacity of eight hours per workday. Houston Methodist contracts anesthesia service for operation at hospitals throughout the system. A surgical case consists of a surgical technologist, an OR nurse, and a “floater” nurse to facilitate operations between two rooms, in addition to the anesthesia team. Technicians are scheduled with accordance to planned and prospective OR activity. On-call teams are available for emergent surgical cases and 24-hour accountability.
Following procedure completion, patients are transferred from the OR to the PACU with an allocation of two patients per PACU nurse; however, this coverage may vary dependent upon the acuity of the patient. If a patient originates from the intensive care unit or remains intubated upon arrival, then a one-to-one patient per nurse ratio is maintained to facilitate a high level of patient care.
All patients within the PACU will be evaluated by a registered nurse and discharged following an order from the anesthesiologist and/or physician. Vital signs will be measured no less than every 15 min until discharge criteria are met, then at appropriate intervals while still in the PACU. The modified Aldrete scoring system, measured upon admission to the PACU, at 30 min, at 1 hr, and at discharge, is used to facilitate patient discharge from the PACU, which occurs when a minimum Aldrete score of 9 out of 10 is achieved. Additional considerations include a maintained patent airway without support for 30 min, peripheral capillary oxygen saturation (SPO2) greater than or equal to 94%, neurological status relative to baseline mental status, and pain level management.
Study Endpoints
The primary endpoint was the time from neuromuscular blocker reversal agent administration to the time of OR exit.
Secondary endpoints were related to surgical efficiency and consisted of time from procedure completion to OR exit, time from reversal agent administration to extubation, time from procedure completion to extubation, time from reversal agent administration to PACU entry, time from reversal agent administration to anesthesia end, and PACU duration. Procedure completion refers to incision close time.
Exploratory endpoints were post-surgical length of stay and time of reversal agent administration with correlation to pre- and post-procedure completion.
Safety Assessments
Complications related to postoperative residual curarization (PORC) include pneumonia, oxygen desaturation, and re-intubation for airway protection, which are associated with increased post-surgical length of stay and financial costs. Pneumonia was defined as diagnosis within 96 hr of procedure completion. Incidences of re-intubation and SPO2 of less than 90% were measured within the timeframe of reversal agent administration to PACU exit.
Postoperative nausea and vomiting (PONV), which correlate to prolonged PACU time and increased medication costs, were measured by documentation of antiemetic administration within the PACU.
Cost Evaluation Methods
Pharmacoeconomic analysis entailed a review of medication acquisition costs and reversal agent impact on perioperative efficiency.
The average wholesale price of sugammadex and neostigmine/glycopyrrolate was obtained from the Houston Methodist wholesale pharmaceutical distributor. Sugammadex is available for purchase as a 100 milligram (mg)/1 milliliter (mL) single-dose 2-mL or 5-mL vial, whereas neostigmine is accessible as a 0.5 mg/1 mL and 1 mg/mL multiple-dose 10-mL vial. Glycopyrrolate is available as a 0.2 mg/1 mL single-dose 1-mL or 2-mL vial. The per-unit price for a vial was compared with the average medication dose, which was obtained from division of the total administered dose by patient weight. Total pharmaceutical cost was calculated through multiplication of each medication cost by the number of utilized vials.
The economic benefits of sugammadex were assessed through review of average OR and PACU costs per minute at HMH within the research study timeframe. The estimated OR cost was derived from the labor cost, which included a surgical technologist, an OR nurse, and a “floater” nurse. The estimated PACU cost was calculated from the labor cost, which consisted of salary for the nursing staff. The time differences between the two reversal agents were multiplied by the OR and PACU per minute labor costs to evaluate for a financial impact from reversal agent selection.
Statistical Analyses
A sample size minimum of 257 patients per treatment group was required to have 80% power at a 0.05 significance level to detect a clinically meaningful 23-min difference in the time from neuromuscular blocker reversal agent administration to the time of OR exit between the groups. The Shapiro–Wilk normality test dictated nonparametric analysis of continuous data with the Wilcoxon rank-sum test or Mann–Whitney U-test. The chi-squared test or Fisher’s exact test was utilized for the analysis of categorical variables, as appropriate. Multiple linear regression with medication and service line assessed variable correlation with predictive endpoint effect. Research data are presented as median with associated interquartile range, unless otherwise indicated.
Statistical analyses and tests were conducted with Stata/SE (version 15.1, College Station, Texas).
Results
From July 31, 2017 to August 1, 2018, there were 640 surgical cases at HMH eligible for inclusion in the research study.
Baseline Characteristics
The ratio of sugammadex to neostigmine/glycopyrrolate use was one-to-one. Patients were similar in baseline characteristics relative to age, gender, and weight (Table 1). Neuromuscular blockade induction with rocuronium and vecuronium occurred in 97.97% and 1.25% of surgical cases, respectively. The administration of sugammadex for reversal of succinylcholine was excluded from review; however, succinylcholine was present 0.78% of the time as the primary neuromuscular blocking agent within the neostigmine/glycopyrrolate cohort.
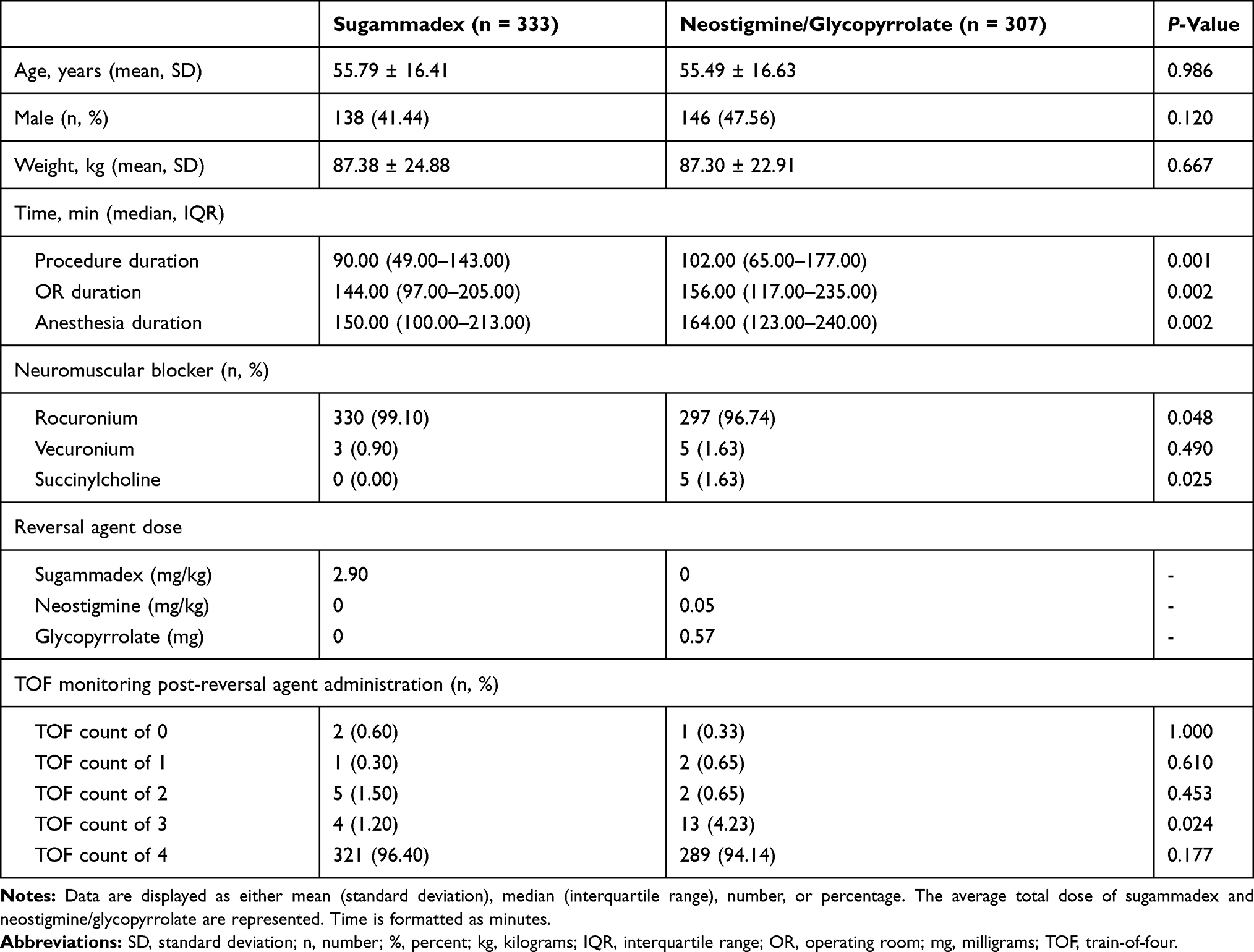 |
Table 1 Baseline Characteristics |
The average initial dose of sugammadex was 2.90 mg/kg, representing appropriate reversal of moderate to deep rocuronium- or vecuronium-induced blockade per the package labeling. The average dose of neostigmine administered was 0.05 mg/kg, corresponding to an appropriate midrange dose selection based on package insert recommendations.
The last recorded peripheral nerve stimulator reading, or train-of-four, prior to PACU entry and following sugammadex and neostigmine/glycopyrrolate administration was 4 in 96.40% and 94.14% of patients, respectively.
Procedural duration and anesthesia period differed in statistical significance between the two reversal agent cohorts, as seen in Table 1.
Research Endpoints
The time from medication administration to exit from the OR was significantly shorter for sugammadex compared to neostigmine/glycopyrrolate (23.00 vs. 27.00 min, respectively; P<0.001), as indicated in Table 2. Neostigmine/glycopyrrolate was associated with a median OR duration of 156.00 min, which was marginally longer when compared to the median OR duration of 144.00 min in the sugammadex cohort (P=0.002). Multiple linear regression exhibited predictive outcome of the reversal agent to the primary endpoint (P=0.035; r2 = 0.039) and to OR duration (P=0.042; r2=0.007) through control of service line factor.
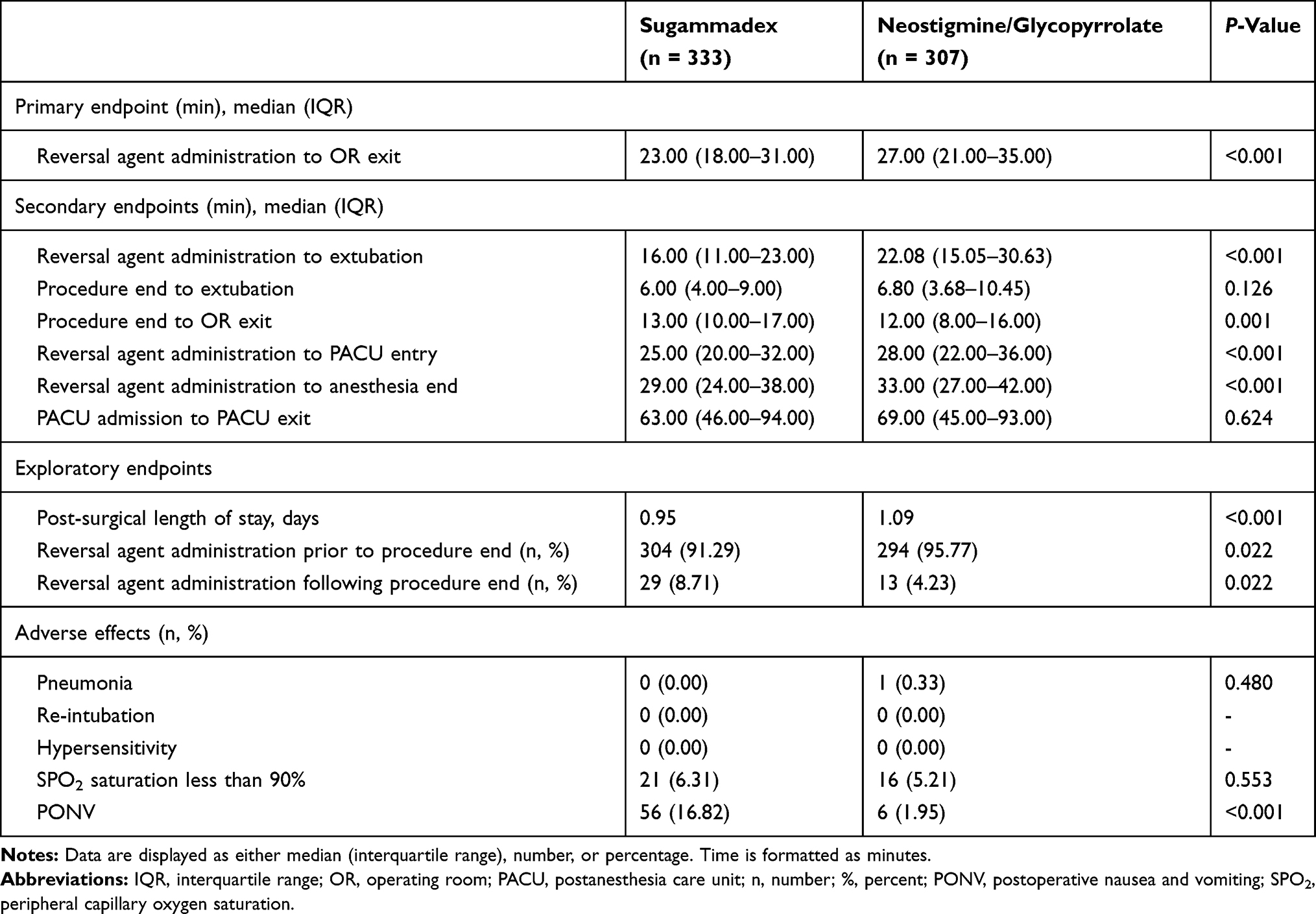 |
Table 2 Research Outcomes |
The time to extubation showed benefit through neuromuscular paralysis reversal with sugammadex (P<0.001). Linear regression identified correlation between the primary endpoint and time to extubation (P<0.001; r2 = 0.941). The time from reversal agent administration to anesthesia end time was also statistically significant (P<0.001), but did not represent the completion of anesthesia prior to OR exit. Temporal outcome associated with PACU duration was no different between the groups, with a median 6-min difference (P=0.624).
Examination of post-surgical length of stay revealed a median inpatient duration of 0.95 days and 1.09 days (P<0.001) in patients administered sugammadex and neostigmine/glycopyrrolate, respectively.
Timeframe review of reversal agent administration with connection to procedure completion resulted in a statistically significant outcome (Table 2). Sugammadex was administered prior to procedure completion in 91.29% of surgical cases compared to neostigmine/glycopyrrolate, which was administered prior to procedure completion in 95.77% of surgical cases (P=0.022). The median time from medication administration to procedure completion was 9.00 min within the sugammadex cohort and 14.00 min within the neostigmine/glycopyrrolate cohort.
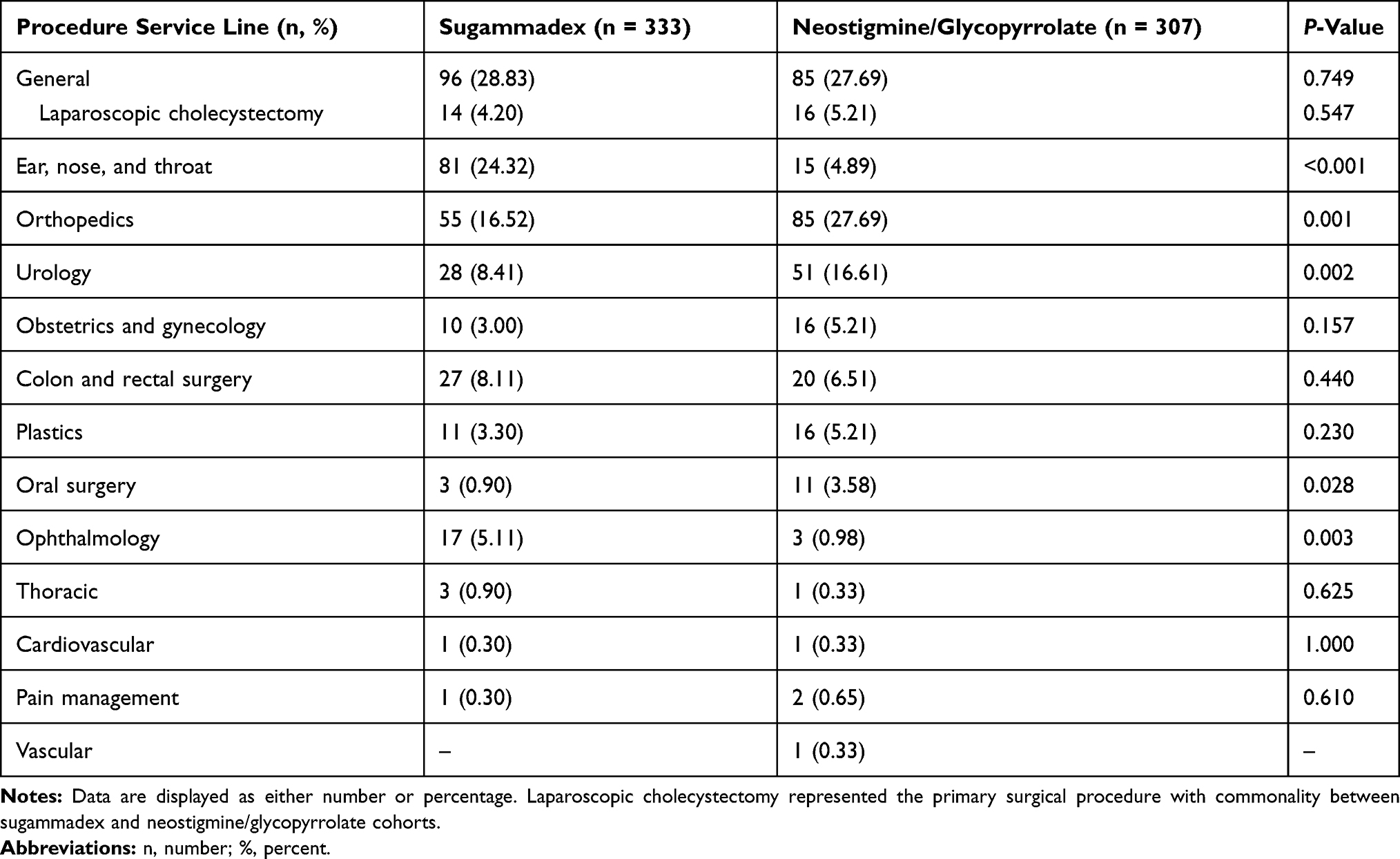 |
Table 3 Houston Methodist Hospital Procedure Service Line Distribution |
Adverse Events
Postoperative adverse events were analyzed through initial incidence of reversal agent hypersensitivity, pneumonia, re-intubation, SPO2 less than 90%, and PONV (Table 2). Ninety-eight patients (15.31%) within the review exhibited an event related to either a medication-related adverse effect or PORC. Sugammadex was associated with 77 events (77.00%) compared to neostigmine/glycopyrrolate, which was associated with 23 events (23.00%).
PONV represented 56 (72.73%) of the adverse events within patients that were administered sugammadex, whereas the event occurrence was six (26.09%) within the neostigmine/glycopyrrolate cohort (P<0.001). These events were identified through initial treatment with an antiemetic medication in the PACU.
Peripheral capillary oxygen desaturation occurred with similar incidence rates following reversal with sugammadex and neostigmine/glycopyrrolate (P=0.553). Diagnosis of pneumonia resulted in one patient (0.16%) present in the neostigmine/glycopyrrolate cohort (P=0.480) compared to zero patients in the sugammadex cohort. No re-intubation events were identified in either group, suggesting adequate neuromuscular blockade reversal.
Hypersensitivity to either sugammadex or neostigmine/glycopyrrolate was not evident through review of patient allergy information.
Surgical Service Lines
Nineteen surgical service lines were represented by the data (Table 3). Procedural cases were primarily within the general service line, which exhibited an incidence of 28.83% within sugammadex and neostigmine/glycopyrrolate cohorts (P=0.748). The remainder of surgical cases were further divided between service lines at volumes with variable statistical significance. Of note, the ear, nose, and throat (ENT) service line exhibited high correlation to the selection of sugammadex as the neuromuscular paralysis reversal agent (P<0.001; r2=0.074).
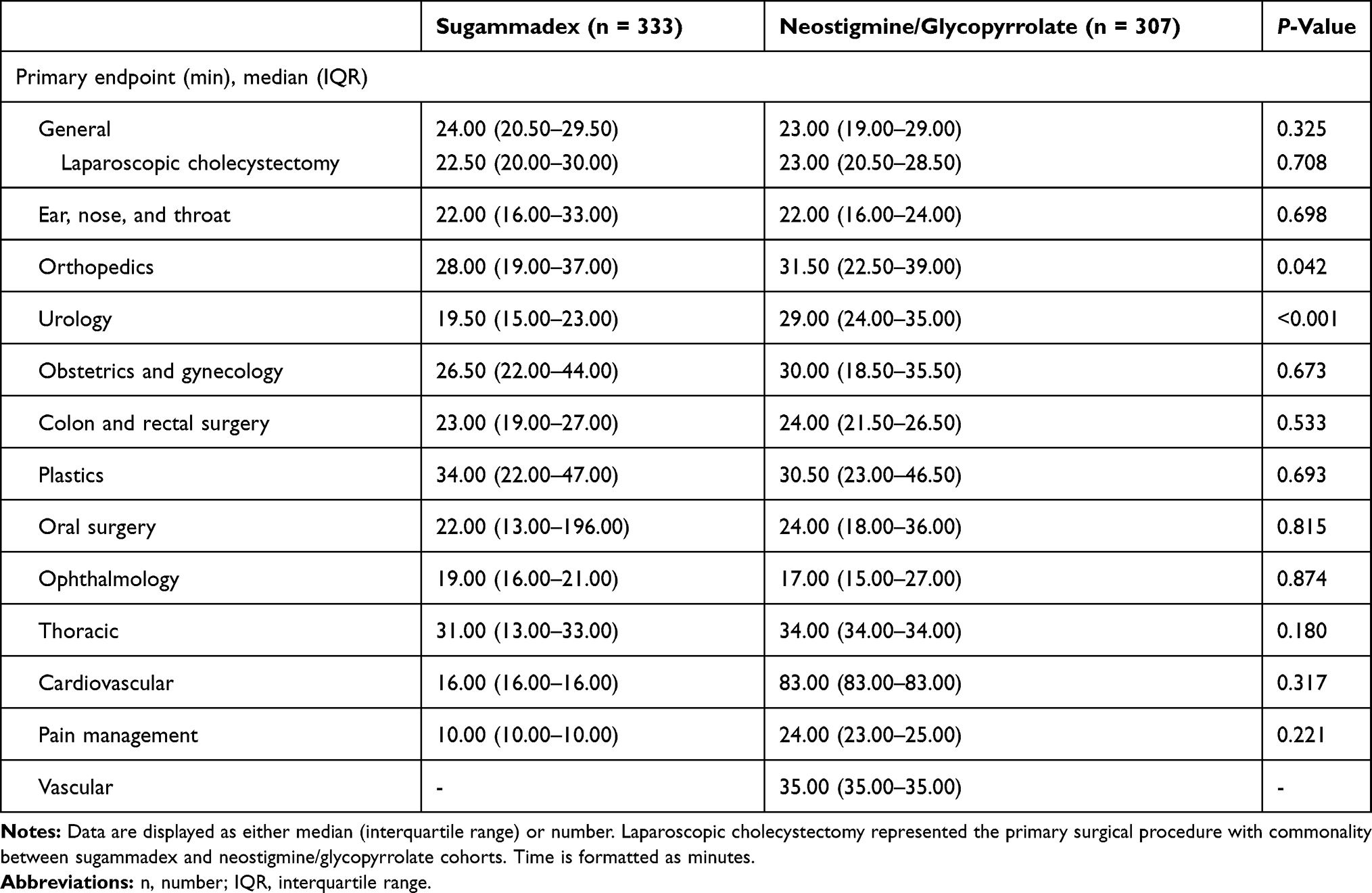 |
Table 4 Houston Methodist Hospital Procedure Service Line by Primary Endpoint |
Neuromuscular paralysis reversal with sugammadex exhibited temporal benefit within the orthopedics and urology service lines at median values of 29.00 min (P=0.042) and 19.50 min (P<0.001), respectively (Table 4). Other service lines were without statistical difference to the level of the primary endpoint.
The most common surgical procedure, with similar frequency between both sugammadex and neostigmine/glycopyrrolate cohorts, was laparoscopic cholecystectomy. The procedure consisted of 4.69% of the surgical case volume and resided within the general service line. Further examination of laparoscopic cholecystectomy procedures indicated a primary endpoint median difference of 0.50 min and the absence of statistical significance (P=0.708).
Cost-Effectiveness Analysis
Patient-specific doses of sugammadex and neostigmine/glycopyrrolate were assessed to calculate medication acquisition costs. Estimated costs were in reference to medication formulations available for purchase from the Houston Methodist wholesaler.
Based on average wholesale unit price, the average medication dose cost for neuromuscular paralysis reversal with sugammadex was $223.85 and $186.18 with utilization of 5-mL single-dose vials and 2-mL single-dose vials, respectively (Table 5). Analysis demonstrated reversal costs associated with neostigmine/glycopyrrolate to differ between vial concentration and volume. The lowest average neostigmine/glycopyrrolate cost was observed through combination of neostigmine 5 mg/10 mL multiple-dose 10-mL vials and glycopyrrolate 0.2 mg/1 mL single-dose 1-mL vials. Medication acquisition cost review highlighted an average maximum difference of $178.20 through selection of reversal agent.
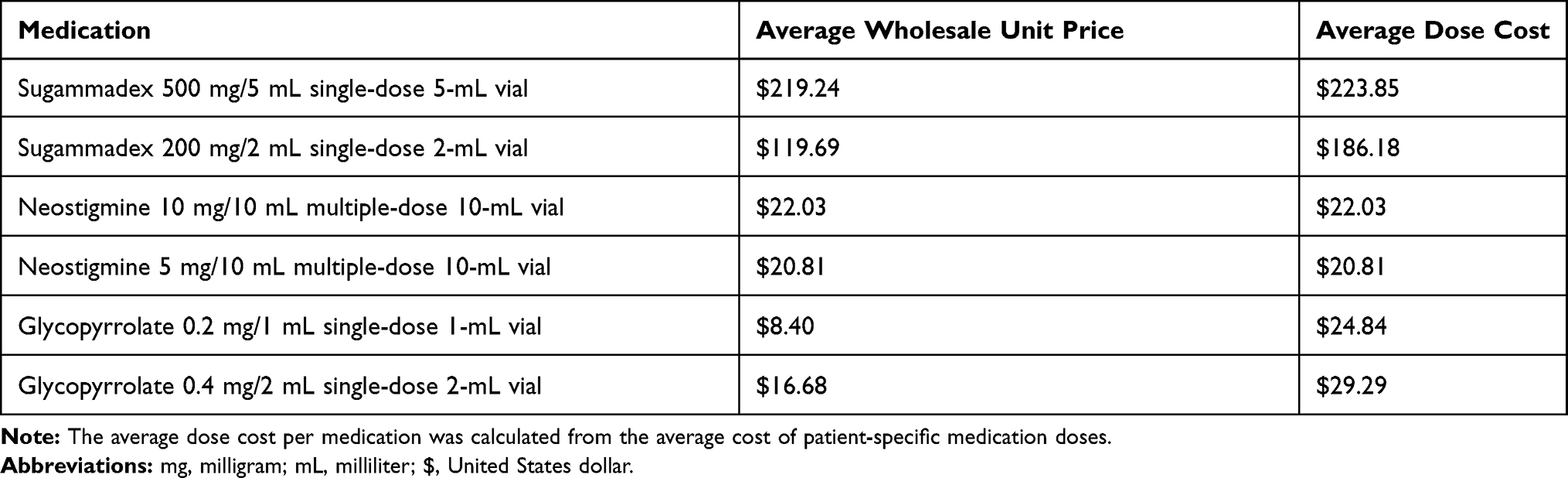 |
Table 5 Average Medication Wholesale Price Information with Average Dose Cost |
The average OR cost at HMH is $4.50 per minute, whereas the average PACU cost is $2.00 per minute. Based on the primary endpoint median difference, sugammadex use may result in a per-case OR cost savings of $18.00. Furthermore, shortened PACU time, estimated by a median 6 min difference, may result in a per-case PACU cost savings of $12.00. Selection of sugammadex versus neostigmine/glycopyrrolate may correlate to a total per case OR and PACU cost savings of $30.00.
Discussion
The cost-effectiveness of sugammadex is established upon two concepts, as presented through review by Chambers et al.8,11 The first concept associates a reduction in patient recovery time through the utilization of sugammadex as compared with neostigmine/glycopyrrolate, whereas the second relates the pertinence of time savings application to corresponding productivity benefits. Nonetheless, ambiguity persists with regards to productive activities that may be incorporated within surgical workflow processes, which is contingent upon the proportion of time consistently saved through selection of sugammadex. To accommodate an increased daily volume of surgical cases, average time savings within a workday would have to be in excess of the average surgical case duration per institution service line and procedure type. De Robertis et al. conducted a research study with bariatric surgical procedures and demonstrated average OR occupancy time savings of 23.3 min through administration of sugammadex.4 Extensive calculations were supplied by Zaouter et al. to support the integration of additional surgical cases into the OR schedule.11 However, Ledowski et al. concluded no differences with anesthesia duration, OR occupancy time, and PACU time attributable to sugammadex when equated to the standard of care.12 Further investigation was warranted to assess research outcomes within an academic medical center.
Houston Methodist contracts anesthesia service with a fixed expense established upon overall room occupancy and without connection to service duration. The organization structure is unique compared to healthcare institutions that may directly employ anesthesia staff and allocate costs to the operational budget. HMH OR and PACU costs are variable and contingent upon cost for nursing staff compensation. Expenses for anesthesia service, medical equipment, and surgical materials are fixed and not attributed to the selection of reversal agent. Furthermore, HMH OR and PACU staff would not have work shifts of variable duration dependent upon time saved from a surgical case. The reduction in OR turnover time would be beneficial, if correlated to prevention of surgical case postponement or increased capacity for surgical case volume.
The minimal time saved through administration of sugammadex rather than neostigmine/glycopyrrolate was determined to be insignificant for application to incorporate additional surgical procedures into the OR schedule and validate pharmacy department medication costs. The results were contrary to extant literature with evidence to support the economic impact of sugammadex to a healthcare system.4,11 Explanation may be attributable to pre-optimized OR and anesthesia service workflow systems. Research outcomes at HMH demonstrate more consistent administration of neostigmine prior to procedure completion compared to sugammadex, indicating a correct anticipation of the pharmacokinetics and pharmacodynamics of neostigmine’s onset of action. Statistically significant results with regards to reduced OR duration may be of interest, but the endpoint was predisposed to confounding by factors unrelated to the medication, as demonstrated through linear regression.
Analyses of reversal agent administration timeframe to extubation and to OR exit confirmed evidence that rapid recovery from neuromuscular blockade facilitated extubation and permitted patient transfer to the PACU. The time from reversal agent administration to extubation was particularly similar to results from a randomized, parallel-group trial.3 However, occupancy time within the PACU was without meaningful difference between sugammadex and neostigmine/glycopyrrolate, consistent with prior evaluations of the two reversal agents.3,6,12 Healthcare institution workflow processes may impede the relevance of rapid OR exit to increased surgical case volume subsequent to patient oversaturation within the PACU. Patients with enhanced time to neuromuscular blockade recovery should theoretically be more apt for transfer from the PACU to the acute care floor, and while the post-surgical LOS was noticeably shorter with sugammadex, the results were clinically significant and may be contingent upon variable patient characteristics, a multitude of service lines, and inpatient versus outpatient status.
Observed reduction in anesthesia time through administration of sugammadex supplemented to literature of improved time to recovery from general anesthesia. Jones et al. revealed that more patients were awake and oriented prior to PACU transfer and following tracheal extubation secondary to administration of sugammadex rather than neostigmine/glycopyrrolate.1,13 The findings were supported by Khuenl-Brady et al. through analysis of pre-transfer clinical recovery indicators, as 60.4% of patients in the sugammadex cohort were awake and oriented compared to 57.8% of patients in the neostigmine/glycopyrrolate cohort.1,14 The overall results corresponded with the afferentiation theory, which postulates muscle activity to generate afferent input to brain arousal foci.1,15,16 However, the concept of reversal-agent–induced stimulation was potentially invalidated, albeit singular sugammadex analysis.16 At defined time periods following the administration of sugammadex, Illman et al. evaluated bispectral index, state entropy, and response entropy.16 The indices were not found to exhibit time-dependent changes with correlation to anesthesia depth.16 Further evaluation may be warranted to conclude a comparative impact of neuromuscular blockade reversal to anesthesia depth and recovery.
The scope of clinical practice assessment in this study was increased through the inclusion of all surgical service lines. Service line comparison to the level of the primary endpoint provided context to potential variation that may be inherently attributed to the procedure type. Results indicate the local, preferential selection of sugammadex for reversal of neuromuscular blockade within the ENT service line (P<0.001), which is consistent with rationale provided by current literature. ENT surgical cases require a deep level of neuromuscular blockade to enable manipulation of the airway within a comparatively shortened procedure timeframe.17,18 Traditional agents for neuromuscular blockade reversal, acetylcholinesterase inhibitors, are limited in ability to reverse profound block, particularly with volatile anesthetics that reinforce effects of the neuromuscular blocking agent.18,19 The rapid recovery of neuromuscular paralysis is favorable in procedures that require intraoperative facial nerve monitoring, such as parotid surgery.19 Deep neuromuscular blockade with rocuronium may also be required for thoracic and abdominal surgeries, which further advocates the advantage of sugammadex compared to neostigmine/glycopyrrolate in select procedure types.18 The evidence for deep neuromuscular blockade in laparoscopic procedures, to improve intraoperative working conditions or enhance patient outcomes, has been varied and without sufficient objective data to support reversal with sugammadex.17,20
The clinical benefits of sugammadex have had extensive endorsement since the medication’s initial entry to the pharmaceutical market. Paton et al. conducted a systematic review of randomized controlled trials to evaluate the recovery time impact of sugammadex as compared to neostigmine/glycopyrrolate.2 Sugammadex promoted recovery from moderate and profound rocuronium-induced neuromuscular blockade in 2.02 and 3.90 min, respectively, which is markedly less than the recovery time with neostigmine/glycopyrrolate in 25.39 and 70.69 min, respectively.2 The adverse effects of neostigmine/glycopyrrolate, which include circulatory complications and PORC, were expected to be avoided through administration of sugammadex.8,21 Further confirmation was provided through research studies of the pharmacological action of sugammadex for rapid, complete, and safe reversal of neuromuscular paralysis in high-risk patient populations.7,22–24 However, the economic benefits of sugammadex for reversal of routine neuromuscular blockade have not been as evident.2
The results of this quality improvement initiative highlight the importance of periodic evaluations for medications approved by a pharmacy and therapeutics committee to a multi-hospital health-system formulary.25 Formulary management is integral to the minimization of medication costs and control of prescribing patterns to ensure appropriate medication utilization.26 Sugammadex was approved in March 2016 to the Houston Methodist formulary with restriction only to anesthesia service for use within perioperative settings. The clinical benefits of sugammadex are evident, but its administration for routine neuromuscular blockade reversal reveals an inopportune representation of its reported advantages compared to neostigmine/glycopyrrolate. Rapid recovery from neuromuscular paralysis may not contribute to perioperative efficiency, but it can prove beneficial in select patient populations with consideration to disease states and comorbid conditions.
The research study was predisposed to limitations attributed to study design and retrospective data availability. Endpoints developed with consideration of time may be inherently subject to documentation bias, which correlates to the time of event occurrence versus EMR documentation. Instances where train-of-four (TOF) measurements were not recorded may explain documentation of the final TOF measurement as equal to zero. Surgical case factors that may impact the endpoints, such as need to evaluate an exsanguinated dressing, initial inadequate reversal dose, delayed emergence from anesthetic, and PACU nurse availability, are not expected to differ secondary to the selection of neuromuscular blockade reversal agent, but present as unable to be delineated through retrospective review. Similarly, external, non-controllable factors that may affect PACU duration without regard to reversal agent selection include incomplete pain management, bed availability, transfer service availability, and pending diagnostic studies or laboratory results. Furthermore, certified registered nurse anesthetists, who administer neuromuscular blockade reversal agents, may prefer a specific medication, dependent upon patient characteristics, procedure type, or personal bias. The inclusion of all surgical service lines into analysis demonstrates potential to confound results, but reversal agent clinical outcomes are not expected to differ upon procedure type. In addition, assessment of initial neuromuscular blockade depth was not incorporated into study design. The time to recovery from deep neuromuscular blockade, although not specifically evaluated, was established to be superior with sugammadex, as concluded in prior research studies.5
Conclusion
While sugammadex is associated with more rapid reversal of neuromuscular paralysis, its utilization does not correlate to meaningful time saved in the OR, as postulated by prior analyses, or extrapolation to workflow capacity for increased surgical case volume. The time from reversal agent administration to OR exit is pragmatically comparable with that of neostigmine/glycopyrrolate and without operational effect. When considering the lack of safety differences identified between sugammadex and neostigmine regimens and the inability of the patient care progression process to capitalize on the reduced time to reversal of neuromuscular paralysis, the higher sugammadex acquisition costs do not appear to be value-added. A more targeted use of sugammadex in patients with deep neuromuscular blockade or patients with requirement of emergency reversal may be prudent.
Acknowledgments
Data acquisition was facilitated by Yung Tran, Applications Analyst in the Houston Methodist System Quality Operations and Analytics Department. Statistical analysis support was provided by David Putney, PharmD, MPH, BCPS.
Author Contributions
All of the authors contributed to the research design, data analysis, and drafting or revising of the article. The authors provided final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors have declared no potential conflicts of interest. Funding was not received for this research study.
References
1. Carron M, Zarantonello F, Lazzarotto N, Tellaroli P, Ori C. Role of sugammadex in accelerating postoperative discharge: a meta-analysis. J Clin Anesth. 2017;39:38–44. doi:10.1016/j.jclinane.2017.03.004
2. Paton F, Paulden M, Chambers D, et al. Sugammadex compared with neostigmine/glycopyrrolate for routine reversal of neuromuscular block: a systematic review and economic evaluation. Br J Anaesth. 2010;105(5):558–567. doi:10.1093/bja/aeq269
3. Brueckmann B, Sasaki N, Grobara P, et al. Effects of sugammadex on incidence of postoperative residual neuromuscular blockade: a randomized, controlled study. Br J Anaesth. 2015;115(5):743–751. doi:10.1093/bja/aev104
4. De Robertis E, Zito Marinosci G, Marco Romano G, et al. The use of sugammadex for bariatric surgery: analysis of recovery time from neuromuscular blockade and possible economic impact. Clinicoecon Outcomes Res. 2016;8:317–322. doi:10.2147/CEOR.S109951
5. Hristovska A, Duch P, Allingstrup M, Afshari A. Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev. 2017;8(8):CD012763.
6. Watts R, London J, van Wijk R, Lui Y. The influence of unrestricted use of sugammadex on clinical anaesthetic practice in a tertiary teaching hospital. Anaesth Intensive Care. 2012;40(2):333–339. doi:10.1177/0310057X1204000218
7. Carron M, Baratto F, Zarantonello F, Ori C. Sugammadex for reversal of neuromuscular blockade: a retrospective analysis of clinical outcomes and cost-effectiveness in a single center. Clinicoecon Outcomes Res. 2016;8:43–52. doi:10.2147/CEOR.S100921
8. Chambers D, Paulden M, Paton F, et al. Sugammadex for the reversal of muscle relaxation in general anaesthesia: a systematic review and economic assessment. Health Technol Assess (Rockv). 2010;14(39):1–211.
9. Sokolovic E, Biro P, Wyss P, et al. Impact of the reduction of anaesthesia turnover time on operating room efficiency. Eur J Anaesthesiol. 2002;19(8):560. doi:10.1097/00003643-200208000-00003
10. Dexter F, Abouleish A, Epstein R, Whitten C, Lubarsky D. Use of operating room information system data to predict the impact of reducing turnover times on staffing costs. Anesth Analg. 2003;97(4):1119–1126. doi:10.1213/01.ANE.0000082520.68800.79
11. Zaouter C, Mion S, Palomba A, Hemmerling T. A short update on sugammadex with a special focus on economic assessment of its use in North America. J Anesth Clin Res. 2017;8(7):740. doi:10.4172/2155-6148
12. Ledowski T, Hillyard S, Kozman A, et al. Unrestricted access to sugammadex: impact on neuromuscular blocking agent choice, reversal practice and associated healthcare costs. Anaesth Intensive Care. 2012;40(2):340–343. doi:10.1177/0310057X1204000219
13. Jones R, Caldwell J, Brull S, Soto R. Reversal of profound rocuronium-induced blockade with sugammadex. Anesthesiology. 2008;109(5):816–824. doi:10.1097/ALN.0b013e31818a3fee
14. Khuenl-Brady K, Wattwil M, Vanacker B, Lora-Tamayo J, Rietbergen H, Álvarez-Gómez J. Sugammadex provides faster reversal of vecuronium-induced neuromuscular blockade compared with neostigmine: a multicenter, randomized, controlled trial. Anesth Analg. 2010;110(1):64–73. doi:10.1213/ane.0b013e3181ac53c3
15. Chazot T, Dumont G, Le Guen M, Hausser-Hauw C, Liu N, Fischler M. Sugammadex administration results in arousal from intravenous anaesthesia: a clinical and electroencephalographic observation. Br J Anaesth. 2011;106(6):914–916. doi:10.1093/bja/aer142
16. Illman H, Antila H, Olkkola K. Reversal of neuromuscular blockade by sugammadex does not affect EEG derived indices of depth of anesthesia. J Clin Monit Comput. 2010;24(5):371–376. doi:10.1007/s10877-010-9257-x
17. Copp M, Barrett T. Sugammadex: role in current anaesthetic practice and its safety benefits for patients. World J Anesthesiol. 2015;4(3):66. doi:10.5313/wja.v4.i3.66
18. Lemmens HJ, El-Orbany MI, Berry J, Morte JB
19. Bensghir M, Elkoundi A, Ahtil R, Meziane M, Haimeur C. Use of sugammadex in parotid surgery: a case report. J Med Case Rep. 2016;10(1):187. doi:10.1186/s13256-016-0972-x
20. Kopman A, Naguib M. Laparoscopic surgery and muscle relaxants. Anesth Analg. 2015;120(1):51–58. doi:10.1213/ANE.0000000000000471
21. Ünal DY, Baran İ, Mutlu M, Ural G, Akkaya T, Özlü O. Comparison of sugammadex versus neostigmine costs and respiratory complications in patients with obstructive sleep apnoea. Turk J Anaesthesiol Reanim. 2015;43(6):387–395. doi:10.5152/TJAR.2015.35682
22. Amao R, Zornow M, Cowan R, Cheng D, Morte J, Allard M. Use of sugammadex in patients with a history of pulmonary disease. J Clin Anesth. 2012;24(4):289–297. doi:10.1016/j.jclinane.2011.09.006
23. Dahl V, Pendeville P, Hollmann M, Heier T, Abels E, Blobner M. Safety and efficacy of sugammadex for the reversal of rocuronium-induced neuromuscular blockade in cardiac patients undergoing noncardiac surgery. Eur J Anaesthesiol. 2009;26(10):874–884. doi:10.1097/EJA.0b013e32832c605b
24. McDonagh D, Benedict P, Kovac A, et al. Efficacy, safety, and pharmacokinetics of sugammadex for the reversal of rocuronium-induced neuromuscular blockade in elderly patients. Anesthesiology. 2011;114(2):318–329. doi:10.1097/ALN.0b013e3182065c36
25. Leonard M, Thyagarajan R, Wilson A, Sekeres M. Strategies for success in creating an effective multihospital health-system pharmacy and therapeutics committee. Am J Health Sys Pharm. 2018;75(7):451–455. doi:10.2146/ajhp170531
26. Abramowitz P. Controlling financial variables—changing prescribing patterns. Am J Health Sys Pharm. 1984;41(3):503–515. doi:10.1093/ajhp/41.3.503
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.