")
Back to Journals » Patient Related Outcome Measures » Volume 11
Impact of Stigma on People Living with Chronic Hepatitis B
Authors Smith-Palmer J , Cerri K, Sbarigia U, Chan EKH, Pollock RF , Valentine WJ, Bonroy K
Received 12 August 2019
Accepted for publication 14 February 2020
Published 9 March 2020 Volume 2020:11 Pages 95—107
DOI https://doi.org/10.2147/PROM.S226936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Jayne Smith-Palmer,1 Karin Cerri,2 Urbano Sbarigia,2 Eric KH Chan,3 Richard F Pollock,1 William J Valentine,1 Kristien Bonroy2
1Ossian Health Economics and Communications, Basel, Switzerland; 2Janssen Pharmaceutica NV, Beerse, Belgium; 3Janssen Global Services, LLC, Raritan, NJ, USA
Correspondence: Jayne Smith-Palmer
Ossian Health Economics and Communications GmbH, Bäumleingasse 20, Basel 4051, Switzerland
Tel +41 61 271 6214
Email [email protected]
Background: People with chronic infectious diseases such as hepatitis B can face stigma, which can influence everyday life as well as willingness to engage with medical professionals or disclose disease status. A systematic literature review was performed to characterize the level and type of stigma experienced by people infected with hepatitis B virus (HBV) as well as to identify instruments used to measure it.
Methods: A literature review was performed using the PubMed, Embase and Cochrane Library databases to identify studies describing HBV-related stigma. For inclusion, articles were required to be published in full-text form, in English and report quantitative or qualitative data on HBV-related stigma that could be extracted.
Results: A total of 23 (17 quantitative and 6 qualitative) articles examined HBV-related stigma. The scope of the review was global but nearly all identified studies were conducted in countries in the WHO Southeast Asia or Western Pacific regions or within immigrant communities in North America. Several quantitative studies utilized tools specifically designed to assess aspects of stigma. Qualitative studies were primarily conducted via patient interviews. Internalized and social stigma were common among people living with chronic HBV . Some people also perceived structural/institutional stigma, with up to 20% believing that they may be denied healthcare and up to 30% stating they may experience workplace discrimination due to HBV.
Conclusion: HBV-related stigma is common, particularly in some countries in Southeast Asia and the Western Pacific region and among Asian immigrant communities, but is poorly characterized in non-Asian populations. Initiatives are needed to document and combat stigma (particularly in settings/jurisdictions where it is poorly described) as well as its clinical and socioeconomic consequences.
Keywords: hepatitis B, stigma, discrimination
Background
In many countries, people living with infectious bloodborne viruses such as hepatitis B virus (HBV), hepatitis C virus and human immunodeficiency virus (HIV) frequently face stigma and discrimination. Stigma associated with HIV has been well characterized, where it is a key barrier in terms of seeking both testing and treatment.1 However, despite a much higher global prevalence,2,3 stigma associated with HBV is less well characterized, which may be partly attributable to a lack of political prioritization around HBV compared with the substantial public health and political initiatives focused on HIV.4
Stigma has previously been defined as
a social process, experienced or anticipated, characterized by exclusion, rejection, blame or devaluation that results from experience, perception or reasonable anticipation of an adverse social judgement about a person or group.5
And Scambler et al further add that this judgment is “medically unwarranted.” Stigma can be further categorized as social (also known as public or enacted) stigma, internalized (self/felt) stigma and structural (institutional) stigma. In the context of HBV, an example of social stigma, which involves the endorsement of negative preconceptions or stereotypes by social groups, would be the assumption that a person living with HBV also injects drugs. Similarly, internalized stigma refers to stigma felt by people on an individual level and includes the anticipation of social rejection or negative stereotyping due to living with a bloodborne virus such as HBV. Structural stigma, which exists at a system wide or policy level, has not been documented in North America and Western Europe. However, structural stigma related to HBV has been reported in China. Here, it was only in 2007 that anti-discrimination legislation was introduced to prevent the denial or termination of employment on the basis of a positive HBV test and testing for HBV prior to employment or entrance to university was not banned until 2010.6–8
The stigma directed towards people living with HBV emanates from multiple origins. These include preconceptions that a person may use drugs or may be sexually promiscuous as well as an irrational fear of contagion, often fueled by a lack of knowledge and understanding of transmission routes for HBV. In HIV the phenomenon of “intersectional” stigma has been reported. Intersectional or “layered” stigma refers to stigma due to “synergistic, mutually constitutive relationship between social identities and structural inequities”9,10 and can occur on an internal, social or structural level. In the context of HIV, and HBV, groups that already face discrimination or stigma such as people who inject drugs (PWID) or commercial sex workers are further marginalized by the association with higher prevalence rates of HIV and HBV. In Europe and North America, the main transmission routes for both HIV and HBV are horizontal, meaning that in these settings, a large proportion of incident cases of HBV occur in high-risk groups such as MSM or PWID, where HBV may be transmitted from person to person through high-risk sexual practices or the sharing of drug-related paraphernalia, respectively. In contrast, vertical transmission of HBV from mother-to-infant was a major transmission route in many Asian settings for prevalent cases. However, the incidence of vertical transmission in many countries, particularly in Southeast Asia and the Western Pacific region has declined substantially since the 1980s owing to the introduction of vaccination programs. For example, in Taiwan, which was the first country to introduce universal vaccination in 1984, the prevalence of HBsAg declined from 9.8% in 1984 to 1.3% in 1994.11 Indeed, as of 2013 infant vaccination programs were in place in 183 out of 192 United Nations member states.12 This suggests that for HBV, intersectional stigma may be more relevant for North American and European people living with HBV that for those living with HBV in some Asian settings.
The implications of stigma related to living with infectious bloodborne viruses such as HBV, both on a social and clinical level, are manifold.13–16 Even prior to diagnosis the existence of stigma around a disease may result in those who suspect they may have been exposed to the risk of infection through horizontal routes delaying or avoiding seeking testing.13–16 This in turn may result in a lack of monitoring and clinical management and potentially a delay in treatment for those people that may require treatment to prevent the progression of their disease. From a public health perspective, a lack of awareness in terms of being infected with a bloodborne virus may potentiate the onward transmission of the infectious agent.
To more fully characterize HBV-related stigma a systematic literature review was conducted to identify articles on the subject and to provide a synopsis of the literature published to date as well as to identify instruments used to quantify HBV-related stigma.
Methods
Literature searches were performed using the PubMed, Embase and Cochrane Library databases. Search strategies were designed using high-level Medical Subject Headings (MeSH) terms supplemented with free text terms (full details of the search strings used are provided in the Supplementary Materials). All searches were performed on 7 November 2016. No time limits were applied to the searches but searches were limited to articles published in English. For inclusion, publications were required to be full-text publications (conference abstracts were excluded owing to the limited amount of data available and the potential for duplication with full-text articles). Limits were also applied to publication type such that publications that were letters, commentaries, editorials, narrative reviews, or case studies were also excluded. For inclusion, studies were required to either quantitatively or qualitatively examine stigma in HBV. Articles not in, or specifically related to, people living with HBV or not related to stigma (or where stigma was only mentioned in passing and was not a focus of the research) were excluded. Articles in mixed populations of people living with HBV or HCV where data for the HBV subset could not be isolated were excluded owing to the potential for different levels of stigma in HBV compared with HCV.
First-round screening of titles and abstracts was performed independently by two reviewers using Sourcerer literature screening software (Covalence Research Ltd, London, UK).17 Any discrepancies following first-round screening were resolved by discussion. Second- round screening of full-text articles and data extraction was then performed.
Results
Literature Search Results
Searches of the PubMed, Embase and Cochrane Library databases yielded a total of 1498 hits and after removal of duplicates, a total of 1077 unique articles remained. A total of 991 articles were excluded during first-round screening, and a further 63 articles were excluded during second-round screening, leaving 23 articles for inclusion in the review (Figure 1).
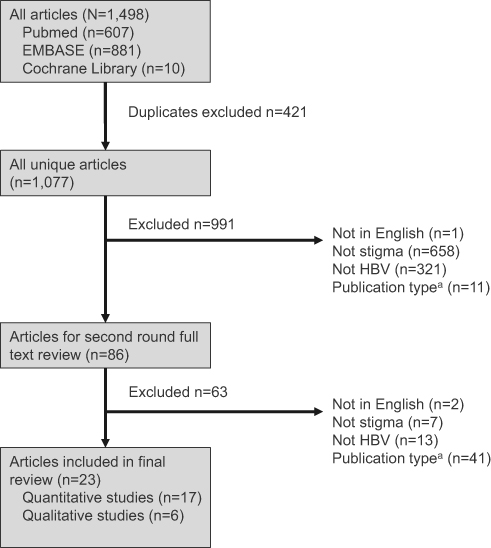 |
Figure 1 Summary of literature review process. Notes: aPublication type refers to articles that were excluded on the basis of being published in abstract from only, as well as case studies, commentaries, editorials, letters and narrative reviews. |
A total of 17 articles quantitatively examined HBV-related stigma.18–34 and a further six articles provided a qualitative assessment of stigma, typically through either semi-structured interviews or focus group discussions.35–40 The quantitative studies included a total of 15 studies conducted in people living with HBV or in the general population about people living with HBV and two studies that were conducted exclusively in healthcare providers. Seven of these studies assessed stigma exclusively in people living with HBV,18,22,23,27–29,31 two of which also conducted separate analyses in people without HBV,23,31 and the remainder were conducted in general population samples.
Quantitative Assessment of HBV-Related Stigma
Analysis of the literature showed that, to date, the majority of studies assessing HBV-related stigma have been conducted either in countries in the WHO Southeast Asia or Western Pacific regions (in particular, China, Taiwan, Malaysia and Vietnam) or within North America in respondents self-identifying as Asian American, including respondents born in the US and respondents born in China, South Korea, Japan, Vietnam and Cambodia. In terms of methodology, most included studies used custom-built surveys, and frequently stigma was assessed in parallel with HBV-related knowledge. In terms of custom-built surveys, several were based on previously published instruments used to assess HIV-related stigma (Table 1). For example, Cotler et al (2012)20 constructed the HBV Stigma Instrument, which was developed utilizing previously published surveys of stigma in HIV41,42 and was subsequently used in two other studies identified in the current review.21,23 A further two studies, both conducted in China, used the same five questions to assess HBV-related stigma in rural adults or rural migrants to a major Chinese city.24,32 These questions related to the extent that a person was willing to interact, or let their children interact with someone living with chronic HBV. However, there is currently very limited evidence to support the psychometric properties (eg reliability and validity) of identified stigma instruments.
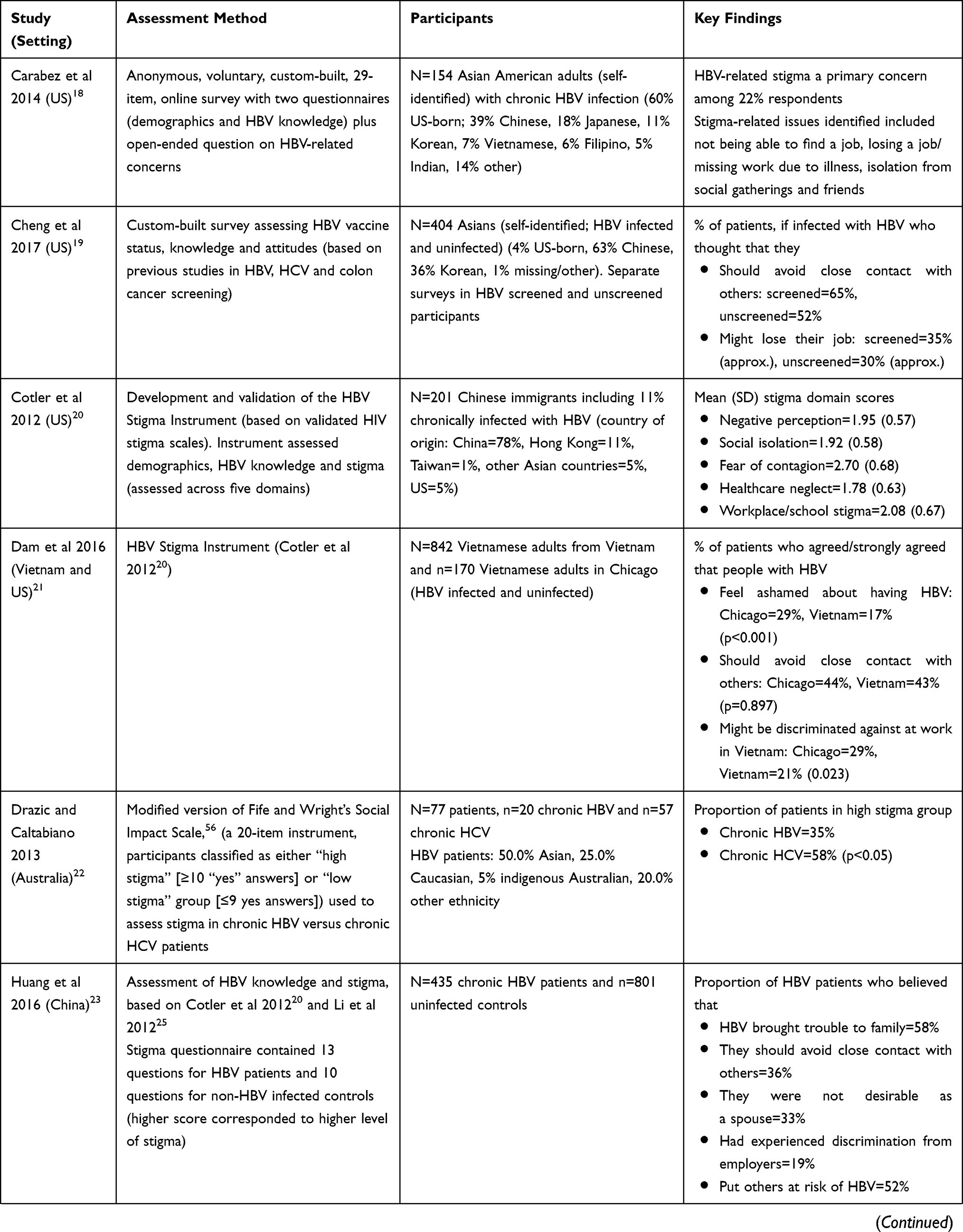 | 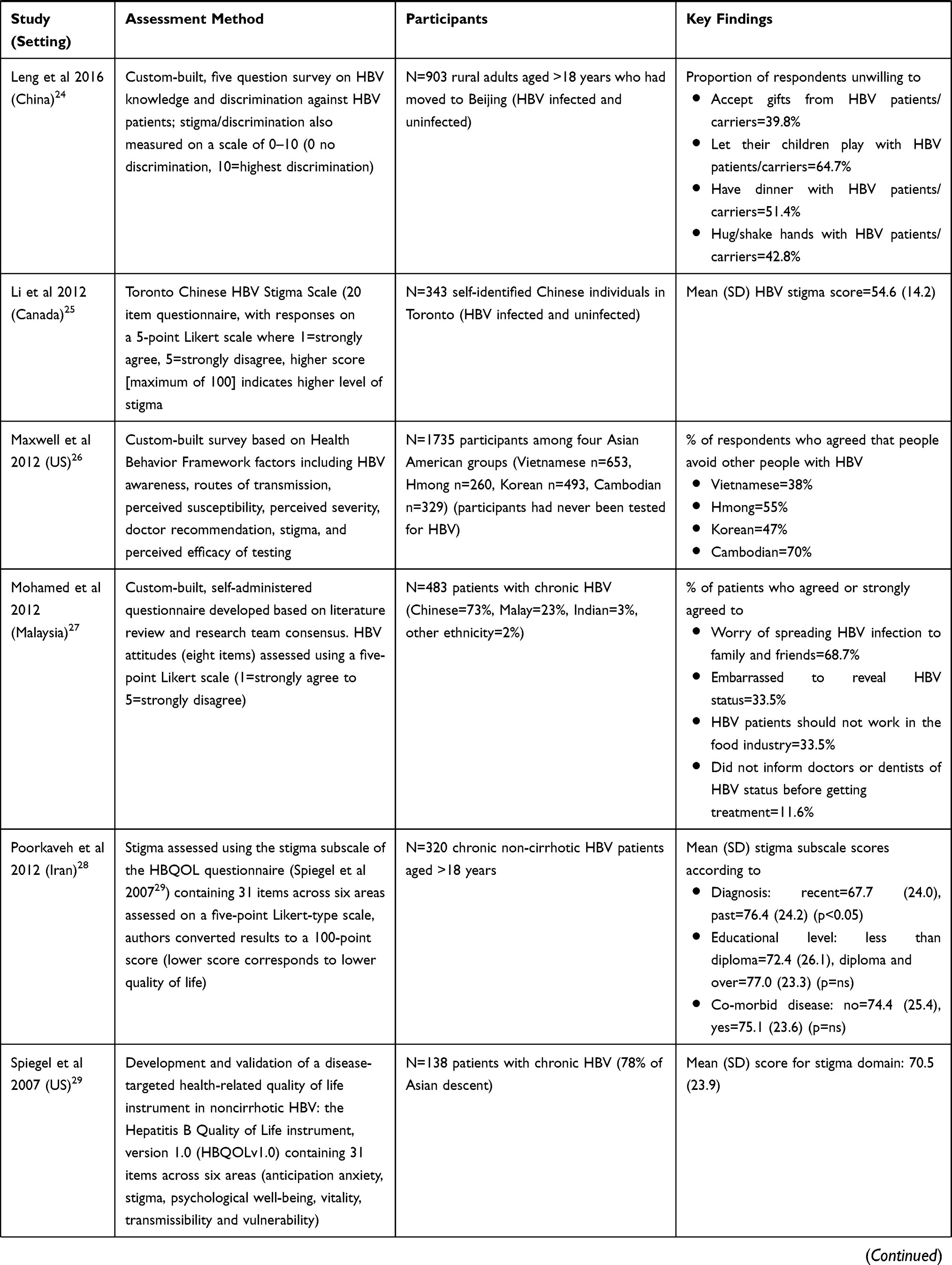 | 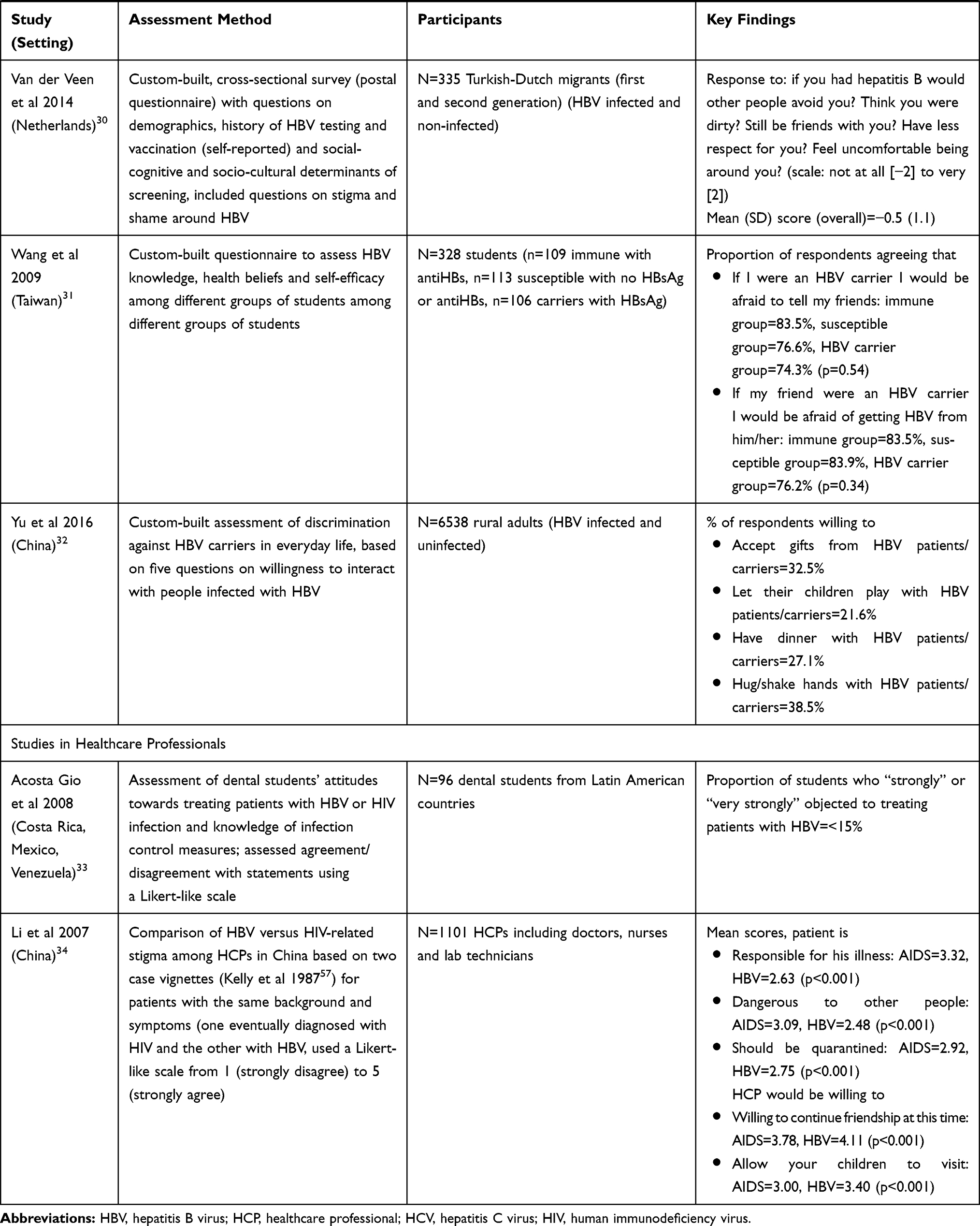 |
Table 1 Summary of Included Quantitative Studies |
Stigma was consistently evident across studies conducted in people living with chronic HBV, with several studies showing that people often felt either embarrassed or ashamed, or that their HBV brought shame to their families (Table 1).20,21,23,27 For example, in Chinese or Vietnamese populations, or Chinese/Vietnamese immigrants to the US between 34% and 58% of the respondents believed that living with chronic HBV would bring trouble to their family.
Another consistent theme both from individuals living with chronic HBV or those without HBV was the feeling that people with HBV should avoid close contact (such as kissing or hugging) with others (Table 1).19–21,23,24,27,32 For example, in one study primarily in Chinese immigrants to the US, 62% of the respondents thought that they should avoid close contact with others.20 Similarly, in a study of 404 individuals who self-identified as Asian Americans (in which 63% identified as Chinese and 36% as Korean and 94% were born outside the US), 65% of the respondents who had not been screened and 52% of the respondents who had been screened for HBV stated that if infected they would avoid close contact with others,19 and in a study in rural Chinese adults, only 39% would be willing to hug or shake hands with someone with HBV.32 A key driver of avoidance of close contact was fear of contagion, often driven by lack of knowledge. For example, 69% of a sample of Malaysian people living with HBV were worried about the possibility of transmitting HBV to others,27 whilst in Vietnam, 55% of a general population sample erroneously believed that HBV could be transmitted through sharing cutlery with someone living with HBV.21
In terms of institutional stigma, one study showed that this was believed to be more common in China than in the US. In a study population consisting primarily of Chinese immigrants to the US, 8% of the respondents believed that they might be denied healthcare in the US, but 12% believed they might be denied healthcare in China.20 Similarly, 21% of Vietnamese immigrants living in the US believed that having HBV might result in being refused healthcare in Vietnam.21 In terms of institutional stigma from employers, in one study from China 15% of people living with HBV felt that they had been denied employment opportunities owing to their HBV status.23 Additionally, in a custom-built survey administered to self-identified Asian-Americans (of which 94% of the respondents were born outside the US and in terms of ethnicity 67% were Chinese, 31% Korean and 2% other/missing data), Cheng et al reported that 30–35% of the respondents believed that they would be at risk of losing their job if they were infected with HBV.19
Stigma directed towards people living with HBV was also consistently evident in studies conducted in general population samples where only a minority of respondents were living with chronic HBV.19,20,23–26,30,32 Some of the most extreme examples of stigma were reported in two studies among rural adults or rural immigrants to a major city in China, both of which assessed stigma using the same series of five questions.24,32 In these two studies, 43% and 50% of the respondents, respectively, were unwilling to hug or shake hands with someone with HBV, 51% and 57% were unwilling to have dinner with someone with HBV and 78% and 82% of the respondents were unwilling to let their son/daughter marry someone with HBV.
Qualitative Studies
A total of six studies provided a qualitative assessment of patient or healthcare provider attitudes towards people living with HBV, including aspects of stigma and discrimination (Table 2).35–40 Two of the qualitative studies were conducted in people living with HBV in Malaysia and Iran.36,37 In Malaysia, people frequently reported feeling anxious and/or distressed following initial diagnosis, which was attributed to a combination or lack of knowledge, stigma around HBV, and physicians’ emphasizing HBV-related complications. Respondents also noted that one of the consequences of stigma was an unwillingness to disclose their disease status beyond their immediate family members.36 Similarly, in Iran, Valizadeh et al noted three main recurring themes in interviews with people living with HBV. These were a grief reaction following diagnosis, an inferiority complex and emotional challenges, which included worry, fear of stigma and deprivation, fear of being treated like an HIV patient and fear of losing employment or marriage opportunities.37
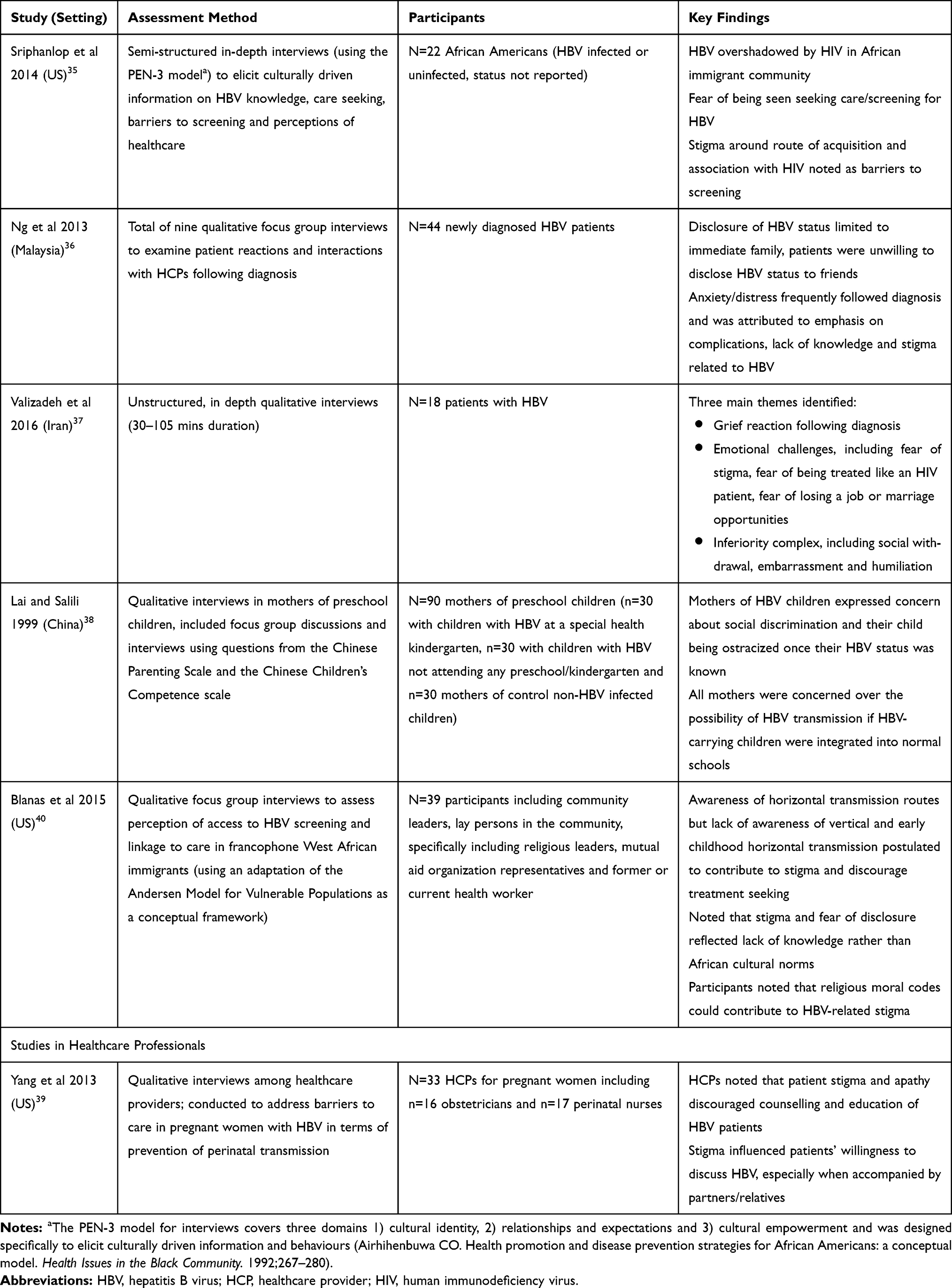 |
Table 2 Summary of Qualitative Studies Examining HBV-Related Stigma |
Of the remaining four qualitative studies, three were conducted in the US35,39,40 and one was conducted in China.38 Several consistent themes were noted in the US-based studies including the existence of HBV-related stigma and its negative impact on seeking testing as well as the relationship between stigma and lack of disease-related knowledge. Additionally, in one US study, conducted in African Americans in New York City, the authors noted that among immigrant communities, HBV is often overshadowed by HIV and often not considered to be as common and/or as serious as HIV.35
The qualitative study from China compared attitudes and concerns among mothers of children living with chronic HBV with those of mothers of children without HBV. At the time at which the study was conducted, children with HBV were frequently precluded from enrolment in normal preschools/kindergartens in China. The primary concerns among mothers of children living with HBV were the fear of social discrimination and their child becoming ostracized if their HBV status became known. All mothers noted concern relating to the possibility of HBV transmission if children with HBV were integrated into mainstream schools.38
Stigma from Healthcare Professionals
Two quantitative studies33,34 and one qualitative study39 identified in the review examined HBV-related stigma and discrimination specifically among healthcare professionals (HCPs). The first quantitative study examined knowledge and discriminatory attitudes towards people living with HBV among dental students in three Latin American countries (Costa Rica, Mexico and Venezuela). Here, fewer than approximately 15% of the dental students stated that they “strongly” or “very strongly” objected to treating people with HBV.33 Additionally, analysis of HBV knowledge revealed that only 26–43% dental students (depending on country) were aware that the risk of HBV transmission was higher than that for HIV.33 The second quantitative study was conducted among HCPs in Yunnan province in China, including doctors, nurses and lab technicians, and used a 14-item questionnaire based on case vignettes to investigate and compare attitudes towards people living with HBV versus those living with HBV.34 Overall, healthcare professionals believed that people living with chronic HBV should be treated with sympathy and understanding (mean score of 4.22 for the statement “deserves sympathy and understanding” where 1=strongly disagree and 5=strongly agree). However, when asked whether a person living with HBV should be considered as “dangerous to other people” the mean score was 2.48 (for people living with HIV the corresponding score was 3.09; p<0.001). Overall, HCPs exhibited a higher level of stigma towards people living with HIV than those living with HBV, with the authors reporting a significant difference in terms of HCP’s willingness to interact socially with people with HBV compared with those with HIV.34 The authors suggest that, despite the higher infectivity of HBV relative to HIV, the higher level of HIV-related stigma may be driven by the perception of HIV being more life-threatening relative to HBV and a layered stigma effect for people living with HIV, wherein HIV was more strongly associated with other stigmatized behaviours including the use of injectable drugs and commercial sex work. Additionally, the authors also reported that both prejudicial attitudes and willingness to interact socially were significantly linked to medical education level.
Additionally, one qualitative study was conducted in HCPs caring for pregnant women in the US and examined barriers to care in terms of preventing perinatal transmission of HBV.39 The authors noted that stigma and apathy discourage education and counselling among people living with HBV and that stigma also had a negative influence on peoples willingness to discuss HBV, particularly when accompanied by partners or relatives.39
Discussion
Overall findings of the review suggest that HBV-related stigma is best characterized in China, as well as in particular immigrant communities but that studies in North American, European and African HBV populations as well as comparative studies across different ethnic groups are lacking. This geographical bias is in line with the higher prevalence of HBV in Asia compared with North America and Europe. The WHO estimate that worldwide, 60% of people infected with HBV are resident in either Southeast Asia or the Western Pacific Region.43 However, it should be noted that within both the WHO Southeast Asia and Western Pacific region the prevalence of HBsAg-positive individuals varies considerably between different countries (eg Schweitzer et al [2015] report HBsAg prevalence rates ranging from <1% for Nepal and Malaysia, but over 5% in several countries including Thailand, China and Vietnam44). Consequently, even though on a regional level, the global burden of disease lies largely within Southeast Asia and the Western Pacific the clinical burden and social implications of HBV infection vary considerably for different countries within these regions.
Only one study from Europe was identified in the current review and this study assessed attitudes towards HBV in Turkish immigrants to the Netherlands. Although, even within Southeast Asia and the Western Pacific region, HBV-related stigma and the extent to which this influences the everyday lives of people living with HBV is not well studied, although to date, stigma around HBV is best characterized in the Chinese setting. Evidence from published literature suggests that HBV-related stigma is both particularly pronounced and deeply entrenched within Chinese society, especially amongst those in rural areas and/or with lower socioeconomic status.24,32
Several studies included in the review sought to establish the underlying causes of stigma directed toward HBV. Although vertical transmission was a key transmission route for a large proportion of the prevalent population, it has been suggested that in China, a substantial proportion of HBV-related stigma may be attributable to a legacy of fear, misconception and poor understanding of HBV transmission routes following a major outbreak of hepatitis A in Shanghai in 1988.6,7 The seriousness of the hepatitis A outbreak, combined with a lack of knowledge of viral hepatitis, in particular around routes of transmission may have provided the basis for much of the structural, as well as social and internalized stigma that has been reported in China. The basis for structural stigma in particular was further perpetuated by legislation that permitted employers and universities to screen applicants for HBV and reject them on the basis of a positive HBV test result.7 Pre-employment HBV screening was officially banned in 2010 but, despite several high profile lawsuits, is still widespread.6 Employers or educational establishments can also effectively work around such legislation by asking applicants to sign a voluntary agreement for an HBV test, or by testing the liver function of applicants.45,46
Other key underlying reasons for stigma included fear of infection, as well as negative assumptions and stereotyping around the sources of infection, with HBV transmission in adults often being perceived as being associated with the use of injectable drugs, sexual promiscuity or homosexuality. Further, research in HIV suggests that already marginalized populations such as PWIDs experience a higher level of stigma if infected with HIV owing to an “intersectional” or “layered” stigma effect47; however, studies examining whether this is also the case with HBV are lacking. Fear of infection was consistently noted as a key concern, both among people living with chronic HBV and among the general population. In particular, the fear of infecting close family was consistently noted as a major issue among those living with chronic HBV.18–20,23,27 Allied to this, a general unwillingness to engage in close physical contact, such as kissing or hugging, people living with HBV was also noted,21,23,24,32 which was often partly attributed to a lack of knowledge around routes of transmission. For example, in one study conducted in Beijing, 58% of the respondents thought that people with HBV should not be allowed to work in restaurants, which is likely related to the fact that 73% of the respondents believed that HBV could be spread by sharing food or utensils.23 However, the relationship between HBV knowledge and stigma appears to be both complex and inconsistent, with some investigators noting that in order to fully elucidate the relationship between HBV knowledge and stigma it may be important to delineate between total HBV knowledge and know specifically relating to transmission routes.20,23 Notably, two studies noted a stronger association between stigma and knowledge of transmission routes than to overall knowledge.20,23
Two studies examined the influence of vaccination on HBV-related stigma.24,32 In one study in rural Chinese adults, vaccination was associated with lower levels of stigma, which the authors postulated was due to “a stronger sense of security” owing to being protected against HBV infection.32 In contrast, another study from China reported that a severe level of HBV-related stigma was more common among vaccinated compared with unvaccinated individuals (52% versus 44%), which the authors hypothesized was due to vaccinated individuals being more knowledgeable about the potential clinical consequences of chronic HBV.24 On a related note, one hypothetical issue that has not been examined in published literature to date is whether stigma, particularly that emanating from fear of contagion, would be influenced by the availability of curative treatments. A key difference between HBV and HIV and hepatitis C is the availability of curative treatments. Replication of HIV and HBV can be suppressed, but as yet, neither HBV or HIV can be eradicated, whereas in contrast, HCV is now curable for almost all people with chronic HCV.48 A recent study in men who have sex with men (MSM) who were living with HIV and resident in China reported that many men believed that if a cure was available for HIV it would reduce the stigma around HIV. In this study, respondents were reported to experience layered stigma owing to negative attitudes towards both MSM and HIV and that a cure for HIV would only combat stigma related to HIV and not MSM.49 However, data relating to whether the availability of a curative treatment would influence HBV-related stigma are currently lacking.
Another area where a paucity of data was noted was related to patient perceptions of HCPs who were living with chronic HBV. A small number of studies examined the perception of treating patients with chronic HBV by HCPs33,34 but despite the higher risk for iatrogenic transmission of HBV compared with HIV the issue of disclosure and attitudes towards HCPs living with chronic HBV remains poorly characterized. The rate of HBV transmission from an HCP with HBV to a patient is 240–2400 per million procedures compared with 2.4–24 per million procedures for an HCP with HIV50 and in the US, up to 1994, a total of 375 people are reported to have acquired HBV from HCPs.51 Disclosure practices among HCPs in particular are subject to considerable debate around ethics and privacy.50 US guidelines state that every case should be considered on an individual basis.51 However, it has been documented that in some settings, such as Canada, medical students living with chronic HBV are encouraged to specialize in areas such as psychiatry with minimal exposure-prone procedures.52
One theme that has been consistently noted among immigrant communities, both for HBV and HIV, is that the close-knit nature of such communities and the fear of being recognized at a clinic or hospital by other people or even HCPs from within that community often served as a barrier to testing and treatment-seeking.35,53 For HBV, the clinical implications of delaying or avoiding testing or treatment-seeking include the potential for onward transmission for people who remain undiagnosed and the potential for the disease progression in those who do not seek treatment. In settings such as North America for example, where horizontal transmission of bloodborne viruses is more common, this barrier is further compounded by a broader overarching stigma directed towards infections that can be transmitted sexually.54 Indeed, Lichtenstein (2003) noted that in the southern US there is often a perception that people with a sexually transmitted infection (STI) have acquired it through “immoral sexual acts”, and also that “the role of gossip in perpetuating STI-related stigma cannot be overstated”.54 Recently, public health initiatives such as the San Francisco Hep B Free Campaign, which began in 2007 and was specifically targeted at Asian Americans, have sought to reposition HBV from a taboo subject to a preventable and treatable condition.55
A limitation of the current review is that owing to the heterogeneity of different studies included and the inherent difficulty in characterizing and quantifying stigma no formal assessment of study quality was performed. However, overall the instruments/questionnaires used to assess stigma appeared to be well suited to purpose and were typically performed using validated questionnaires or used previously validated questionnaires as a framework for custom-built questionnaires. Additionally, most studies used relatively large sample groups, with only two quantitative studies utilizing sample groups of under 100 respondents.22,33 A further limitation was that the review was limited to articles published in English, and therefore does not capture any articles characterizing stigma published in non-English language journals.
Conclusions
In summary, the findings of the current review show that HBV-related stigma is common in several Asian countries, particularly China, and within immigrant communities from China, South Korea, and Vietnam in North America, but has not been extensively documented in European, North American, African or other populations. Moreover, it may not be possible to generalize the findings from settings such as China to other countries or regions owing to the substantial social and cultural differences that exist, as well as the fact that in regions such as Europe and North America, HBV is primarily transmitted through horizontal routes, whereas vertical transmission from mother to infant is key transmission route in countries such as China. HBV-related stigma can negatively influence many aspects of everyday life for people living with HBV and key causes of stigma include misconceptions around routes of transmission and fear of infection. Further, in many countries there remains an unmet need for public health and awareness initiatives aimed at overcoming HBV-related stigma and the barrier it presents to accessing testing and treatment.
Abbreviations
HBeAg, hepatitis B envelope antigen; HBV, hepatitis B virus; HCP, healthcare professional; HCV, hepatitis C virus; HIV, human immunodeficiency virus; IDU, intravenous drug user; MeSH, medical subject heading; MSM, men who have sex with men; STI, sexually transmitted infection; WHO, World Health Organization.
Acknowledgments
The abstract of this paper and summary findings were presented at the European Association for the Study of the Liver (EASL) International Liver Congress in April 2018. The abstract for the poster was published in the Journal of Hepatology 2018; 68 (Suppl 1) pS185.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by funding from Janssen Pharmaceutica NV.
Disclosure
KB, KC, US and EC are current employees of Janssen, which provided funding for this manuscript. JSP, WV and RP are current or former employees of Ossian Health Economics and Communications, which has received consulting fees from Janssen Pharmaceutica NV.
References
1. Mahajan AP, Sayles JN, Patel VA, et al. Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. AIDS. 2008;22 Suppl 2:S67–S79. doi:10.1097/01.aids.0000327438.13291.62
2. Polaris Observatory Collaborators. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol. 2018;3(6):383–403. doi:10.1016/S2468-1253(18)30056-6
3. World Health Organization. HIV/AIDS fact sheet. Available from: http://www.who.int/news-room/fact-sheets/detail/hiv-aids.
4. World Hepatitis Alliance. Viral hepatitis kills more people than HIV, malaria or tuberculosis. Available from: http://www.worldhepatitisalliance.org/news/sep-2017/viral-hepatitis-kills-more-people-hiv-malaria-or-tuberculosis.
5. Scambler G. Health-related stigma. Sociol Health Illn. 2009;31:441–455. doi:10.1111/shil.2009.31.issue-3
6. Liu K. Hepatitis B infection in China: the stigma behind the stigmata. Liver Int. 2016;36:1582–1584. doi:10.1111/liv.2016.36.issue-11
7. Understanding and challenging employment discrimination against people living with HBV in China. Beijing: Yirenping Centre; 2010. Available from: http://www.clb.org.hk/sites/default/files/archive/en/share/File/research_reports/HBV_report_final.pdf.
8. China Daily. Discrimination in the job market common: survey. Liu Weifeng for China Daily; 2007. Available from: http://www.chinadaily.com.cn/china/2007-06/14/content_893811.htm.
9. Rice WS, Logie CH, Napoles TM, et al. Perceptions of intersectional stigma among diverse women living with HIV in the United States. Soc Sci Med. 2018;208:9–17. doi:10.1016/j.socscimed.2018.05.001
10. Logie CH, James L, Tharao W, Loutfy MR. HIV, gender, race, sexual orientation, and sex work: a qualitative study of intersectional stigma experienced by HIV-positive women in Ontario, Canada. PLoS Med. 2011;8(11):e1001124.
11. Chen HL, Chang MH, Ni YH, et al. Seroepidemiology of hepatitis B virus infection in children: ten years of mass vaccination in Taiwan. JAMA. 1996;276(11):906–908. doi:10.1001/jama.1996.03540110060032
12. Lok AS, Hepatitis B. 50 years after the discovery of Australia antigen. J Viral Hepat. 2016;23(1):5–14. doi:10.1111/jvh.12444
13. World Hepatitis Alliance. Holding Governments Accountable. Available from: http://www.worldhepatitisalliance.org/sites/default/files/resources/documents/holding_governments_accountable_-_civil_society_survey_report.pdf.
14. World Health Organization. Global health sector strategy on viral hepatitis 2016–2012. Available from: http://apps.who.int/iris/bitstream/handle/10665/246177/WHO-HIV-2016.06-eng.pdf;jsessionid=16A028EBC622CBF5B5E3903DD6365BFC?sequence=1.
15. World Health Organization. Global hepatitis report; 2017. Available from: http://apps.who.int/iris/bitstream/handle/10665/255016/9789241565455-eng.pdf?sequence=1.
16. Wallace J, Pitts M, Chaojie GL, et al. Needs assessment of people with viral hepatitis – China. July 2015. Available from: https://www.latrobe.edu.au/__data/assets/pdf_file/0006/649302/China-Needs-Assessment-English.pdf.
17. Covalence Research Ltd. Sourcerer. London, UK; 2018. Available from: https://sourcerer.pro/.
18. Carabez RM, Swanner JA, Yoo GJ, Ho M. Knowledge and fears among Asian Americans chronically infected with hepatitis B. J Cancer Educ. 2014;29:522–528. doi:10.1007/s13187-013-0585-7
19. Cheng S, Li E, Lok AS. Predictors and barriers to hepatitis B screening in a midwest suburban Asian population. J Community Health. 2017;42:533–543. doi:10.1007/s10900-016-0285-4
20. Cotler SJ, Cotler S, Xie H, Luc BJ, Layden TJ, Wong SS. Characterizing hepatitis B stigma in Chinese immigrants. J Viral Hepat. 2012;19:147–152. doi:10.1111/j.1365-2893.2011.01462.x
21. Dam L, Cheng A, Tran P, et al. Hepatitis B stigma and knowledge among vietnamese in Ho Chi Minh City and Chicago. Can J Gastroenterol Hepatol. 2016;2016:1910292. doi:10.1155/2016/1910292
22. Drazic YN, Caltabiano ML. Chronic hepatitis B and C: exploring perceived stigma, disease information, and health-related quality of life. Nurs Health Sci. 2013;15:172–178. doi:10.1111/nhs.2013.15.issue-2
23. Huang J, Guan ML, Balch J, et al. Survey of hepatitis B knowledge and stigma among chronically infected patients and uninfected persons in Beijing, China. Liver Int. 2016;36:1595–1603. doi:10.1111/liv.2016.36.issue-11
24. Leng A, Li Y, Wangen KR, Nicholas S, Maitland E, Wang J. Hepatitis B discrimination in everyday life by rural migrant workers in Beijing. Hum Vaccin Immunother. 2016;12:1164–1171. doi:10.1080/21645515.2015.1131883
25. Li D, Tang T, Patterson M, Ho M, Heathcote J, Shah H. The impact of hepatitis B knowledge and stigma on screening in Canadian Chinese persons. Can J Gastroenterol. 2012;26:597–602. doi:10.1155/2012/705094
26. Maxwell AE, Stewart SL, Glenn BA, et al. Theoretically informed correlates of hepatitis B knowledge among four Asian groups: the health behavior framework. Asian Pac J Cancer Prev. 2012;13:1687–1692. doi:10.7314/APJCP.2012.13.4.1687
27. Mohamed R, Ng CJ, Tong WT, Abidin SZ, Wong LP, Low WY. Knowledge, attitudes and practices among people with chronic hepatitis B attending a hepatology clinic in Malaysia: a cross sectional study. BMC Public Health. 2012;12:601. doi:10.1186/1471-2458-12-601
28. Poorkaveh A, Modabbernia A, Ashrafi M, et al. Validity, reliability and factor structure of hepatitis B quality of life questionnaire version 1.0: findings in a large sample of 320 patients. Arch Iran Med. 2012;15:290–297. doi:10.12155/AIM.009
29. Spiegel BM, Bolus R, Han S, et al. Development and validation of a disease-targeted quality of life instrument in chronic hepatitis B: the hepatitis B quality of life instrument, version 1.0. Hepatology. 2007;46:113–121. doi:10.1002/hep.21692
30. van der Veen YJ, van Empelen P, Looman CW, Richardus JH. Social-cognitive and socio-cultural predictors of hepatitis B virus-screening in Turkish migrants, the Netherlands. J Immigr Minor Health. 2014;16:811–821. doi:10.1007/s10903-013-9872-y
31. Wang WL, Wang CJ, Tseng HF. Comparing knowledge, health beliefs, and self-efficacy toward hepatitis B prevention among university students with different hepatitis B virus infectious statuses. J Nurs Res. 2009;17:10–19. doi:10.1097/JNR.0b013e3181999ca3
32. Yu L, Wang J, Zhu D, Leng A, Wangen KR. Hepatitis B-related knowledge and vaccination in association with discrimination against Hepatitis B in rural China. Hum Vaccin Immunother. 2016;12:70–76. doi:10.1080/21645515.2015.1069932
33. Acosta-Gío AE, Borges-Yáñez SA, Flores M, et al. Infection control attitudes and perceptions among dental students in Latin America: implications for dental education. Int Dent J. 2008;58:187–193. doi:10.1111/j.1875-595X.2008.tb00347.x
34. Li L, Wu Z, Zhao Y, Lin C, Detels R, Wu S. Using case vignettes to measure HIV-related stigma among health professionals in China. Int J Epidemiol. 2007;36:178–184. doi:10.1093/ije/dyl256
35. Sriphanlop P, Jandorf L, Kairouz C, Thelemaque L, Shankar H, Perumalswami P. Factors related to hepatitis B screening among Africans in New York City. Am J Health Behav. 2014;38:745–754. doi:10.5993/AJHB.38.5.12
36. Ng CJ, Low WY, Wong LP, Sudin MR, Mohamed R. Uncovering the experiences and needs of patients with chronic hepatitis B infection at diagnosis: a qualitative study. Asia Pac J Public Health. 2013;25:32–40. doi:10.1177/1010539511413258
37. Valizadeh L, Zamanzadeh V, Negarandeh R, Zamani F, Hamidia A, Zabihi A. Psychological reactions among patients with chronic hepatitis B: a qualitative study. J Caring Sci. 2016;5:57–66. doi:10.15171/jcs.2016.006
38. Lai AC, Salili F. Parental attitudes toward their parenting styles and children’s competence in families whose children are hepatitis B virus (HBV) carriers in Guangzhou China. J Comp Fam Stud. 1999;30:281–295. doi:10.3138/jcfs.30.2.281
39. Yang EJ, Cheung CM, So SK, Chang ET, Chao SD. Education and counseling of pregnant patients with chronic hepatitis B: perspectives from obstetricians and perinatal nurses in Santa Clara County, California. Asian Pac J Cancer Prev. 2013;14:1707–1713. doi:10.7314/APJCP.2013.14.3.1707
40. Blanas DA, Nichols K, Bekele M, et al. Adapting the Andersen model to a francophone West African immigrant population: hepatitis B screening and linkage to care in New York City. J Community Health. 2015;40:175–184. doi:10.1007/s10900-014-9916-9
41. Holzemer WL, Uys LR, Chirwa ML, et al. Validation of the HIV/AIDS Stigma Instrument - PLWA (HASI-P). AIDS Care. 2007;19:1002–1012. doi:10.1080/09540120701245999
42. Kalichman SC, Simbayi LC, Jooste S, et al. Development of a brief scale to measure AIDS-related stigma in South Africa. AIDS Behav. 2005;9:135–143. doi:10.1007/s10461-005-3895-x
43. World Health Organization. 2017. Available from: http://www.who.int/hepatitis/en/.
44. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet. 2015;386(10003):1546–1555. doi:10.1016/S0140-6736(15)61412-X
45. Yang T, Wu MC. Discrimination against hepatitis B carriers in China. Lancet. 2011;378(9796):1059. doi:10.1016/S0140-6736(11)61460-8
46. Wallace J, Pitts M, Liu C, et al. More than a virus: a qualitative study of the social implications of hepatitis B infection in China. Int J Equity Health. 2017;16(1):137. doi:10.1186/s12939-017-0637-4
47. Morris JL, Lippman SA, Philip S, Bernstein K, Neilands TB, Lightfoot M. Sexually transmitted infection related stigma and shame among African American male youth: implications for testing practices, partner notification, and treatment. AIDS Patient Care STDS. 2014;28:499–506. doi:10.1089/apc.2013.0316
48. Bartenschlager R, Baumert TF, Bukh J, et al. Critical challenges and emerging opportunities in hepatitis C virus research in an era of potent antiviral therapy: considerations for scientists and funding agencies. Virus Res. 2018;248:53–62. doi:10.1016/j.virusres.2018.02.016
49. Wu F, Zhang A, Babbitt A, et al. Overcoming HIV stigma? A qualitative analysis of HIV cure research and stigma among men who have sex with men living with HIV. Arch Sex Behav. 2017. doi:10.1007/s10508-017-1062-x
50. Barrigar DL, Flagel DC, Upshur RE. Hepatitis B virus infected physicians and disclosure of transmission risks to patients: a critical analysis. BMC Med Ethics. 2001;2:E4. doi:10.1186/1472-6939-2-4
51. Henderson DK, Dembry L, Fishman NO, et al; Society for Healthcare Epidemiology of America. SHEA guideline for management of healthcare workers who are infected with hepatitis B virus, hepatitis C virus, and/or human immunodeficiency virus. Infect Control Hosp Epidemiol. 2010;31:203–232. doi:10.1086/650298
52. Colistro R. Hepatitis B and medical students. CMAJ. 2000;163:259–260.
53. Russ LW, Meyer AC, Takahashi LM, et al. Examining barriers to care: provider and client perspectives on the stigmatization of HIV-positive Asian Americans with and without viral hepatitis co-infection. AIDS Care. 2012;24:1302–1307. doi:10.1080/09540121.2012.658756
54. Lichtenstein B. Stigma as a barrier to treatment of sexually transmitted infection in the American deep south: issues of race, gender and poverty. Soc Sci Med. 2003;57:2435–2445. doi:10.1016/j.socscimed.2003.08.002
55. Yoo GJ, Fang T, Zola J, Dariotis WM. Destigmatizing hepatitis B in the Asian American community: lessons learned from the San Francisco Hep B Free Campaign. J Cancer Educ. 2012;27:138–144. doi:10.1007/s13187-011-0252-9
56. Fife B, Wright E. The dimensionality of stigma: a comparison of its impact on the self of persons with HIV/AIDS and cancer. J Health Soc Behav. 2000;41:50–67. doi:10.2307/2676360
57. Kelly JA, St Lawrence JS, Smith S, Hood HV, Cook DJ. Stigmatization of AIDS patients by physicians. Am J Public Health. 1987;77:789–791. doi:10.2105/AJPH.77.7.789
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.