")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Impact of Single Combination Inhaler versus Multiple Inhalers to Deliver the Same Medications for Patients with Asthma or COPD: A Systematic Literature Review
Authors Zhang S, King D , Rosen VM, Ismaila AS
Received 17 October 2019
Accepted for publication 24 January 2020
Published 26 February 2020 Volume 2020:15 Pages 417—438
DOI https://doi.org/10.2147/COPD.S234823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Shiyuan Zhang,1 Denise King,2 Virginia M Rosen,3 Afisi S Ismaila1,4
1Value Evidence and Outcomes, GlaxoSmithKline plc, Collegeville, PA, USA; 2Value Evidence and Outcomes, GlaxoSmithKline plc, Brentford, UK; 3Optum Inc, Eden Prairie, MN, USA; 4Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada
Correspondence: Afisi S Ismaila
Value Evidence and Outcomes, GlaxoSmithKline plc., 1250 S. Collegeville Road, Collegeville, PA 19426-0989, USA
Tel +1 919 315 8229
Email [email protected]
Abstract: With increasing choice of medications and devices for asthma and chronic obstructive pulmonary disease (COPD) treatment, comparative evidence may inform treatment decisions. This systematic literature review assessed clinical and economic evidence for using a single combination inhaler versus multiple inhalers to deliver the same medication for patients with asthma or COPD. In 2016, Embase, PubMed and the Cochrane library were searched for publications reporting studies in asthma or COPD comparing a single-inhaler combination medicine with multiple inhalers delivering the same medication. Publications included English-language articles published since 1996 and congress abstracts since 2013. Clinical, economic and adherence endpoints were assessed. Of 2031 abstracts screened, 18 randomized controlled trials (RCTs) in asthma and four in COPD, nine retrospective and three prospective observational studies in asthma, and four observational studies in COPD were identified. Of these, five retrospective and one prospective study in asthma, and two retrospective studies in COPD reported greater adherence with a single inhaler than multiple inhalers. Nine observational studies reported significantly (n=7) or numerically (n=2) higher rates of adherence with single- versus multiple-inhaler therapy. Economic analyses from retrospective and prospective studies showed that use of single-inhaler therapies was associated with reduced healthcare resource use (n=6) and was cost-effective (n=5) compared with multiple-inhaler therapies. Findings in 18 asthma RCTs and one prospective study reporting lung function, and six RCTs reporting exacerbation rates, showed no significant differences between a single inhaler and multiple inhalers. This was in contrast to several observational studies reporting reductions in healthcare resource use or exacerbation events with single-inhaler treatment, compared with multiple inhalers. Retrospective and prospective studies showed that single-inhaler use was associated with decreased healthcare resource utilization and improved cost-effectiveness compared with multiple inhalers. Lung function and exacerbation rates were mostly comparable in the RCTs, possibly due to study design.
Keywords: health-related quality of life, cost-effectiveness, lung function, asthma exacerbations, COPD exacerbations
Background
Asthma and chronic obstructive pulmonary disease (COPD) are two of the most common chronic respiratory diseases, affecting approximately 334 million and 251 million people worldwide, respectively.1,2 Both place a considerable burden on communities, through loss of productivity from missed work and school days, and on healthcare systems. The total costs attributable to asthma in the United States for the year 2013 were estimated at $81.9 billion, with medical costs of $50.3 billion responsible for the greatest expense.3 The total costs attributable to COPD in the US were estimated to be $50 billion in 2010.4 Indirect costs vary by population and method of estimation; an annual mean range of $893–$2234 in indirect costs per person has been reported in one review of the literature.5 At an individual level, disease impacts on quality of life (QoL) are wide ranging: patients with asthma and COPD report inability to sleep, breathlessness, and limitations on physical activity and social life among their main concerns, as well as feelings of depression and stigmatization.6 However, asthma and COPD are manageable diseases, and the symptom burden and frequency of exacerbations can be reduced with appropriate treatment.
Patients with moderate-to-severe asthma or COPD usually require inhaled maintenance therapy; this often includes drugs with differing mechanisms of action, including long-acting β2-agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids (ICS).7,8 Nevertheless, despite the availability of effective treatments, suboptimal adherence, inhaler misuse, and poor inhalation technique are common in patients with asthma and COPD, and contribute substantially to treatment failure and to the economic burden of the disease.9,10 The importance of these factors is reflected in the Global Initiative for Chronic Obstructive Lung Disease 2019 report, which – in addition to considering efficacy and effectiveness – highlights the importance of considering the patient’s ability to use, understand, and afford (where relevant) an inhaler device when making treatment decisions for patients with COPD.11 The advent of single-inhaler combination therapies, which provide two – or, for COPD, up to three – treatments, has therefore been welcomed as a method by which we can simplify the management of asthma and COPD while increasing adherence to prescribed treatments, when compared with the use of multiple separate devices.12 While evidence of the advantages of single inhalers containing multiple drugs over single-inhaler monotherapy is widespread,13,14 less is known of comparisons between single inhalers and the equivalent combination taken using multiple inhalers. Because single-inhaler therapies offer the potential advantage of being easier for patients to use, other outcomes – including treatment adherence, cost-effectiveness, and health-related quality of life (HRQoL) – are also of particular interest when comparing them with the equivalent treatment via multiple inhalers.
Given the increasing number of available medications and inhaler devices available to treat asthma and COPD, and as simplified regimens become available, more evidence on clinical and economic outcomes and patient-reported outcomes (PROs) is needed to support optimal prescribing. Here, we present the results of a systematic literature review designed to identify and summarize the overall evidence for the comparative benefit of single versus multiple inhalers delivering the same drugs. Treatments for both asthma and COPD were included.
Methods
Published studies that compared any single combination inhaler device with multiple inhalers delivering the same medications (and doses) individually for the treatment of asthma or COPD were identified from the literature. Reported outcomes included clinical, economic (eg, healthcare resource utilization [HRU] and associated costs), humanistic burden, treatment adherence, inhalation technique, and critical errors.
PubMed/MEDLINE, Embase, and Cochrane library databases were searched on October 4, November 9, and November 10, 2016, respectively, using predefined search strategies. The initial search strategy was developed in the PubMed/MEDLINE database and the strategy was later translated for the Embase and Cochrane library database searches. Constructed search strings included Medical Subject Headings terms and free text terms. Terms for asthma and COPD were combined with terms relating to single and multiple inhalers and study designs. Studies that compared any single inhaler with multiple inhalers delivering the same medication individually were considered for inclusion. A list of studies that were excluded, and the rationale for exclusion, was recorded (Figures 1–4). Several measures were considered to be related to adherence, including medication usage (eg, self-reported in a patient diary), prescription and refill rates (number of prescriptions and refills over a period of time), medication possession ratio (MPR), treatment days, treatment interruptions (eg, break in prescription coverage), and residual treatment (residual doses of study medication in the inhalation device). While articles published in English during or after 1996, or congress abstracts during or after 2013, were included, reports that were letters to the editor, reviews or meta-analyses, protocols, or treatment guidelines were excluded.
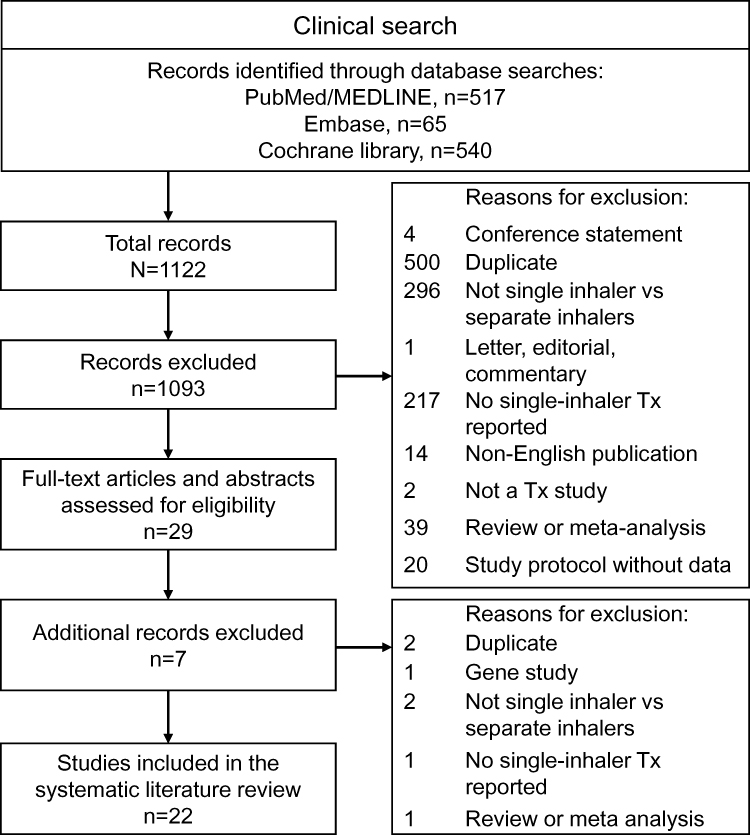 |
Figure 1 Screening selection of clinical studies. Abbreviation: Tx, treatment. |
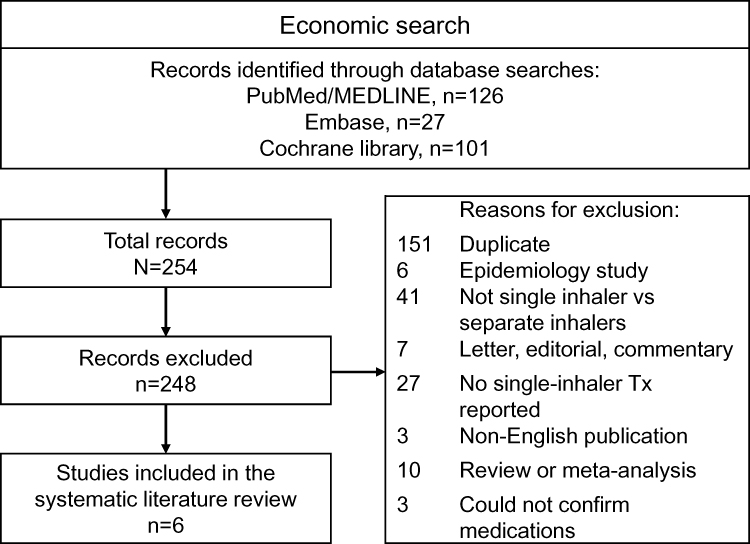 |
Figure 2 Screening selection of economic studies. Abbreviation: Tx, treatment. |
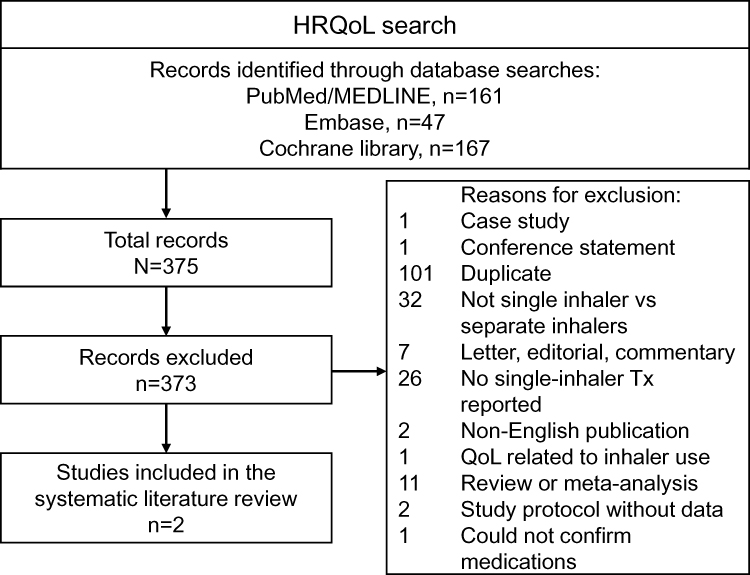 |
Figure 3 Screening selection of HRQoL studies. Abbreviations: HRQoL, health-related quality of life; QoL, quality of life; Tx, treatment. |
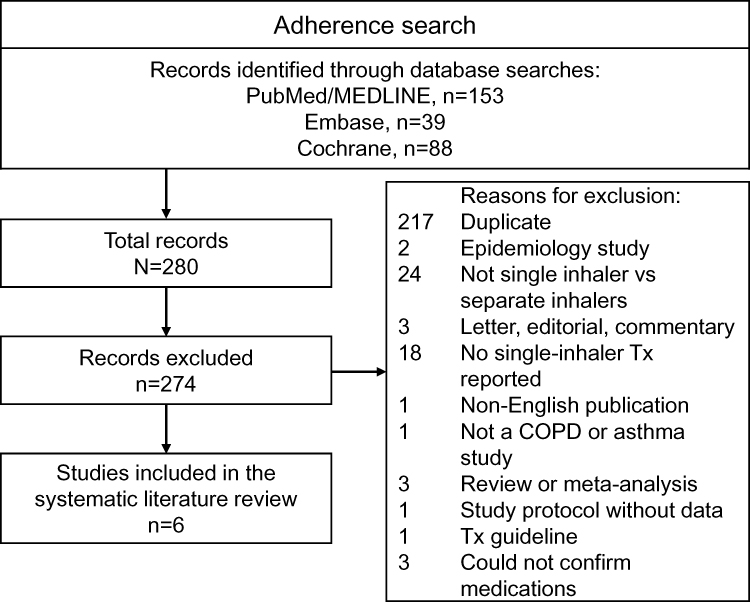 |
Figure 4 Screening selection of adherence studies. Abbreviations: COPD, chronic obstructive pulmonary disease; Tx, treatment. |
In addition to database searches, the bibliography sections of articles identified from the search were reviewed for possible additional published studies. For journal article abstracts and congress abstracts obtained from search results, a double screening and abstraction process was performed to reduce potential bias in study selection. Two reviewers independently assessed which studies met inclusion criteria, with any discrepancies resolved by a third reviewer. After determining the studies that met the inclusion criteria, a data abstraction and study quality assessment was performed by the three reviewers by the same method used for study selection. Published methodological checklists, including the Randomized Controlled Trial (RCT) checklist and Non-RCT clinical checklist from the National Institute for Health and Care Excellence (NICE) Guidelines Manual,15 were used in assessments of study quality, except for economic studies where the NICE Guidelines Manual Economic Checklist15 and the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist16 were used.
Results
Search Results and Screening
A total of 2031 records were retrieved from four searches, of which 38 studies were assessed by full text and met the inclusion criteria after screening (see Supplementary Table 1). These included 22 clinical studies (Figure 1) and three observational studies that reported clinical endpoints, six economic studies (Figure 2), two HRQoL studies (Figure 3), and six adherence studies (Figure 4). A total of 1093 clinical study records were excluded, the majority due to duplications (n=500), not relating to multiple-inhaler combinations versus single inhalers (n=296), or no single combination inhaler treatment reported (n=217).
Out of the 38 studies assessed, 12 asthma studies and four COPD studies reported on adherence outcomes, 11 asthma studies and eight COPD studies reported on HRU outcomes, three asthma studies and five COPD studies reported on cost and cost-effectiveness, 21 asthma studies and four COPD studies reported on symptoms and HRQoL, and 13 clinical studies in asthma and four clinical studies in COPD reported adverse events (AEs). The methodologies for these studies were assessed and met both NICE and CHEERS criteria.
Adherence Outcomes
Data on adherence (including compliance and persistence) were reported in non-randomized observational and RCTs in asthma (n=817–24 and n=4,25–28 respectively) and COPD (n=229,30 and n=2,31,32 respectively; Table 1). Adherence was assessed as medication usage (including self-reported),25–27,32 prescription/refill rates,17–19,21 MPR,18,20 treatment days,17,18 treatment persistence/interruptions,19,22–24,28–30 and residual treatment.31
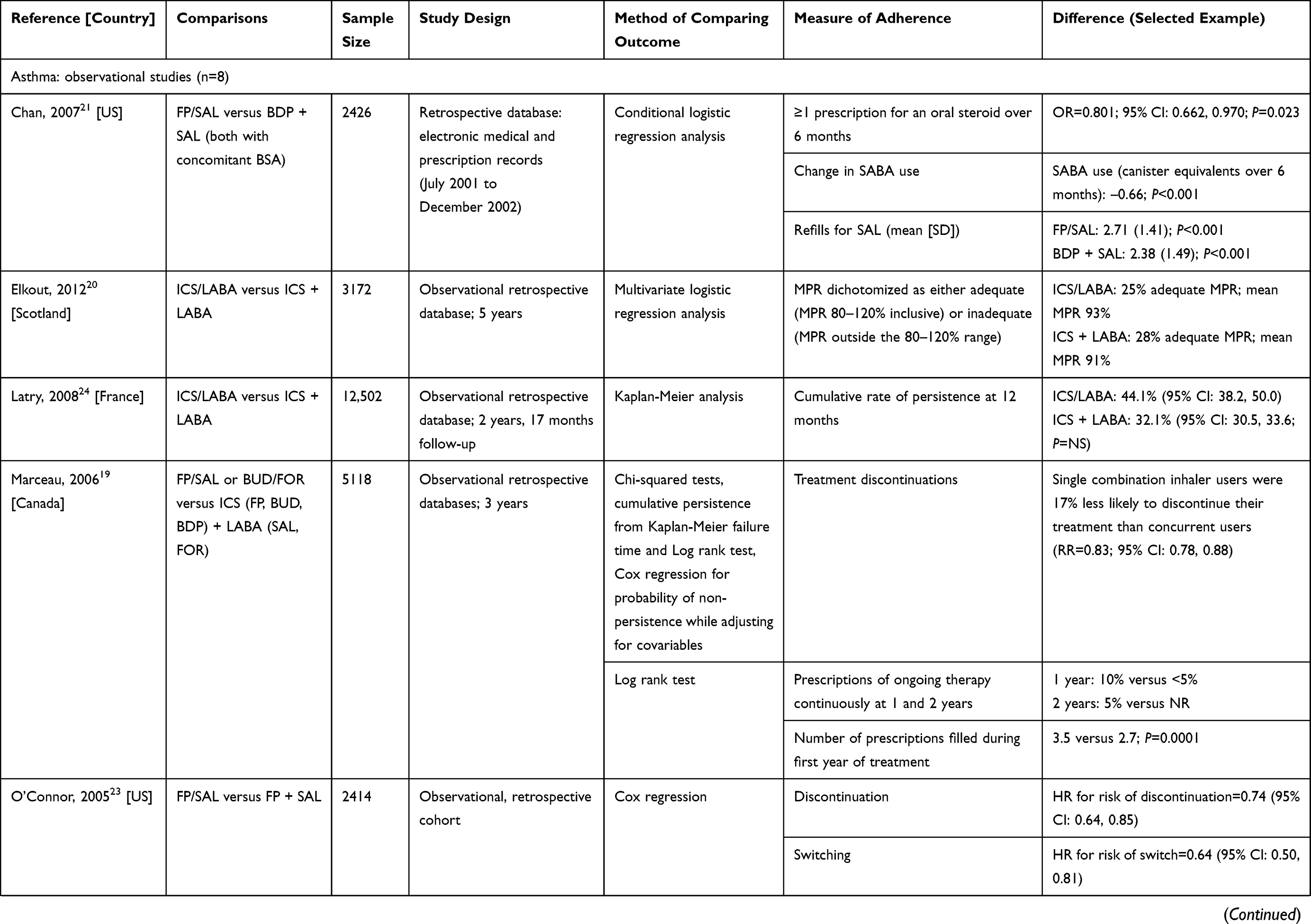 | 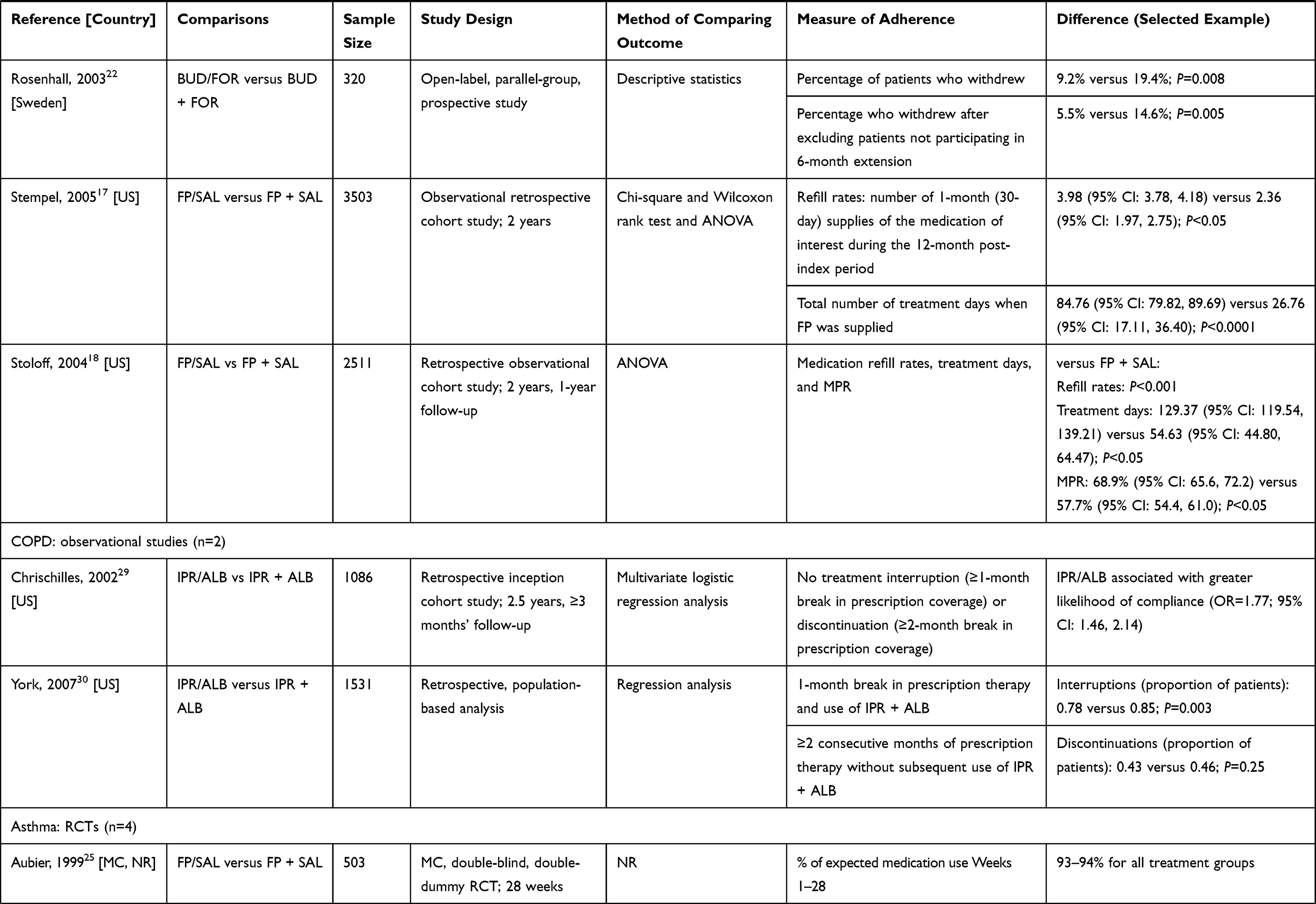 | 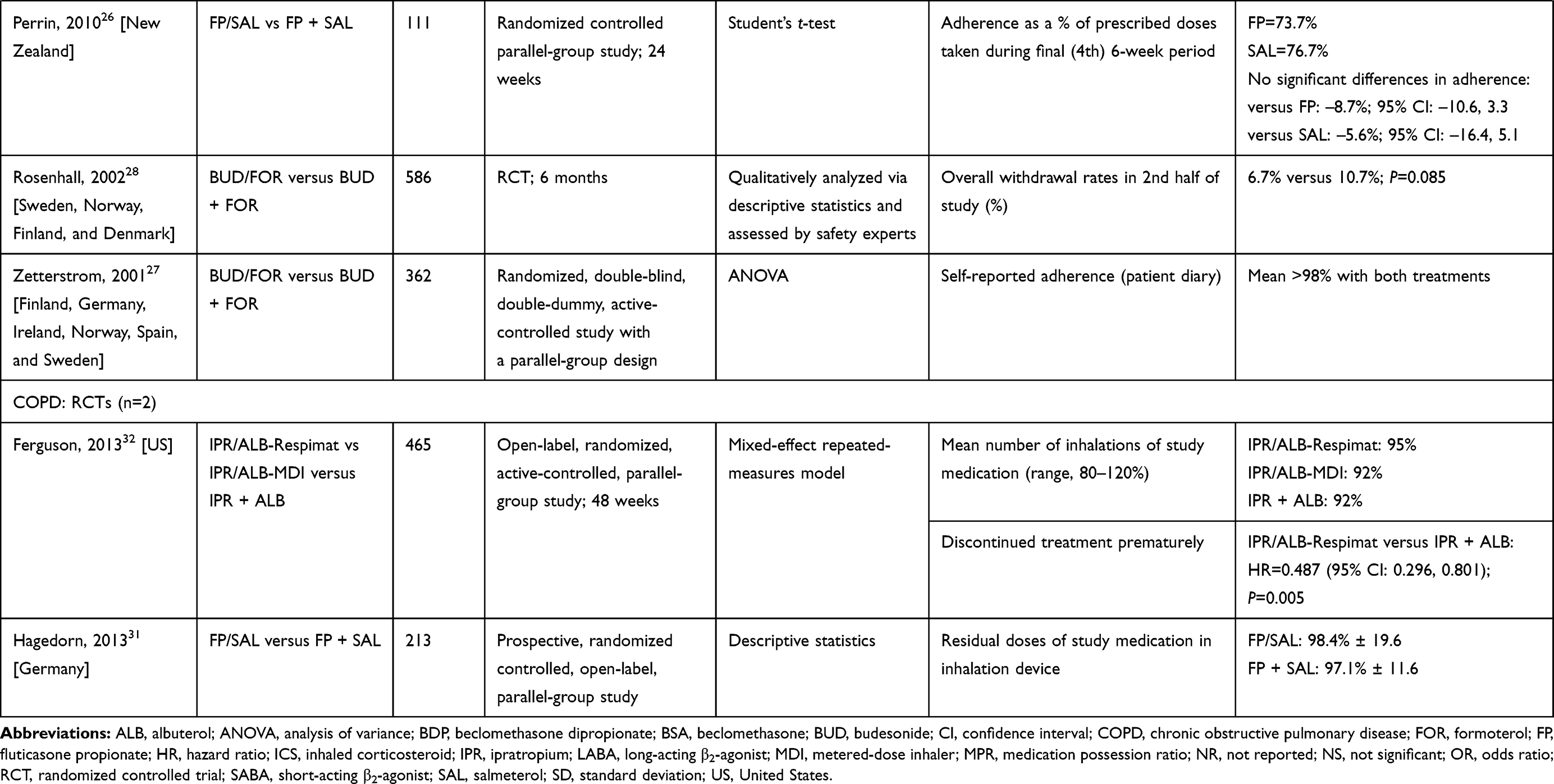 |
Table 1 Adherence Outcomes |
Evidence from Non-Randomized Observational Studies
Results from four retrospective studies in asthma (patient numbers ranging from 2426 to 5118) indicated that users of single inhalers filled significantly more prescriptions than users of multiple inhalers over time periods of 621 and 12 months17–19 (all P<0.05; Table 1). Using medical and pharmacy claims data from the Ingenix database collected between April 2001 and July 2001, prescriptions for single inhalers were significantly higher than the number of requests for ICS in the multiple-inhalers group (4.06 versus 2.35; P<0.001).18 In another US study based on administrative data from three commercial healthcare providers, the mean number of prescription fills for the single-inhaler (n=996) group (calculated as the number of 30-day supplies during the 12-month index period) was 3.98 versus 2.36 for the separate-inhaler group (fluticasone propionate [FP] + salmeterol [SAL], n=259; P<0.05).17 In a third US trial database study, the average refill rate over 6 months, for patients identified from the Kaiser Permanente Medical Care Program in California, was 2.71 versus 2.38 for patients receiving multiple inhaler components (FP/SAL versus beclomethasone dipropionate [BDP] + SAL, respectively, plus beclomethasone [BSA]) (P<0.001).21 Finally, using claims data between 1999 and 2002 of asthma patients in Quebec to create matched cohorts of patients newly treated with either concurrent ICS + LABA (n=2559) or combined ICS/LABA in a single inhaler (n=2559), combination users were found to fill an average of 0.9 more prescriptions per year than concurrent users (P=0.0001).19 No studies compared refill rates in patients with COPD.
Where evaluated in a non-randomized setting in asthma, treatment days (total number of days when the FP component of the regimen was supplied17 and number of days with both treatments supplied on that day18) were significantly higher for combined- versus separate-inhaler users (Table 1). Stempel et al17 (n=3503) found that the mean number of treatment days for FP/SAL was 84.76 versus 26.76 for FP + SAL (P<0.0001). In the study reported by Stoloff et al18 (n=2511), the mean treatment days for the single-inhaler cohort (129.37 days; 95% confidence interval [CI]: 119.54, 139.21) were significantly higher (P<0.05) than the mean treatment days of the FP + SAL cohort (54.63 days; 95% CI: 44.80, 64.47), over the 365-day post-index period. Additionally, two (of three) asthma studies (n=511819 and n=2414,23 respectively) found significant differences in treatment discontinuations, favoring single-inhaler users (Table 1). Across these studies, combination users were found to be 17% less likely to stop treatment over 12 months (adjusted hazard ratio [HR]=0.83; 95% CI: 0.78, 0.88)19 and have a lower risk of treatment discontinuation (HR=0.74; 95% CI: 0.64, 0.85) or switching (HR=0.64; 95% CI: 0.50, 0.81) than multiple-inhaler users.23 A third study (n=12,502) reported numerically higher rates of persistence in single-inhaler users compared with multiple-inhaler users (44.1% [95% CI: 38.2, 50.0] versus 32.1% [95% CI: 30.5, 33.6]; P=not significant [NS]).24
Similar findings were observed in COPD patients: in one study (n=1086), compliance (defined as not interrupting or discontinuing therapy during the follow-up period) was greater for single-inhaler users than patients taking the same regimen as separate inhalers (odds ratio [OR]=1.77; 95% CI: 1.46, 2.14),29 and another (n=1531) found significantly fewer interruptions for single-inhaler ipratropium bromide [IPR]/albuterol [ALB] versus IPR + ALB (0.78 versus 0.85; P=0.003; Table 1).30 The only conflicting evidence was reported in the same COPD study, which found no significant difference in treatment discontinuation rates between groups over 24 months.
A further observational study in asthma (n=320) looked at withdrawal rates in RCT extensions, and reported mixed findings. The study found that a greater percentage of patients using separate inhalers withdrew from budesonide [BUD] + formoterol [FOR] versus single-inhaler users (19.4% versus 9.2%; P=0.008), and the percentage who withdrew after excluding patients not participating in a 6-month extension was 14.6% versus 5.5%, respectively (P=0.005).22 Other measures of adherence included the MPR, which was reported in two studies (n=251118 and n=317220), one reporting significant improvements favoring single- versus multiple-inhaler users (68.9% [95% CI: 65.6, 72.2] versus 57.7% [95% CI: 54.4, 61.0]; P<0.05),18 and the other reporting similarly adequate levels (25% versus 28% adequate MPR).20
Evidence from Clinical Trials
Few RCTs reported measures of adherence (asthma, n=4; COPD, n=2), with three asthma studies (participant range, n=111 to n=586) testing for differences statistically26–28 and one providing descriptive results only (n=503),25 while neither COPD study (n=213 and n=465, respectively) tested for differences statistically (Table 1).31,32 Rates of adherence in clinical studies in asthma were, in general, high across all treatment groups (73.7% to >98%),25–27 with no significant difference found between the percentage of prescribed doses taken in the final 6-week period when tested in a single asthma study.26 In a study of 586 asthma patients, the overall rates of withdrawal were similar for multiple-inhaler and single-inhaler users (6.7% versus 10.7%; P=0.085).28 However, in one open-label RCT in COPD (n=465), patients in the IPR/ALB treatment group were less likely to stop treatment when compared to those receiving IPR + ALB (HR=0.487; 95% CI: 0.296, 0.801).32 This study utilized patient satisfaction with therapy as the primary endpoint, with IPR/ALB-Respimat reporting significantly higher scores with a modified Patient Satisfaction and Preference Questionnaire (PASAPQ) compared with IPR/ALB-metered-dose inhaler (MDI) and IPR + ALB at all visits starting with Week 3 (differences of 9.6 and 6.2, respectively; both P<0.001).32
Healthcare Resource Utilization
Data on HRU were reported in observational and RCTs in asthma (n=718–21,23,33,34 and n=4,27,35–37 respectively) and COPD (n=429,30,38,39 and n=4,31,32,40,41 respectively; Table 2).
 | 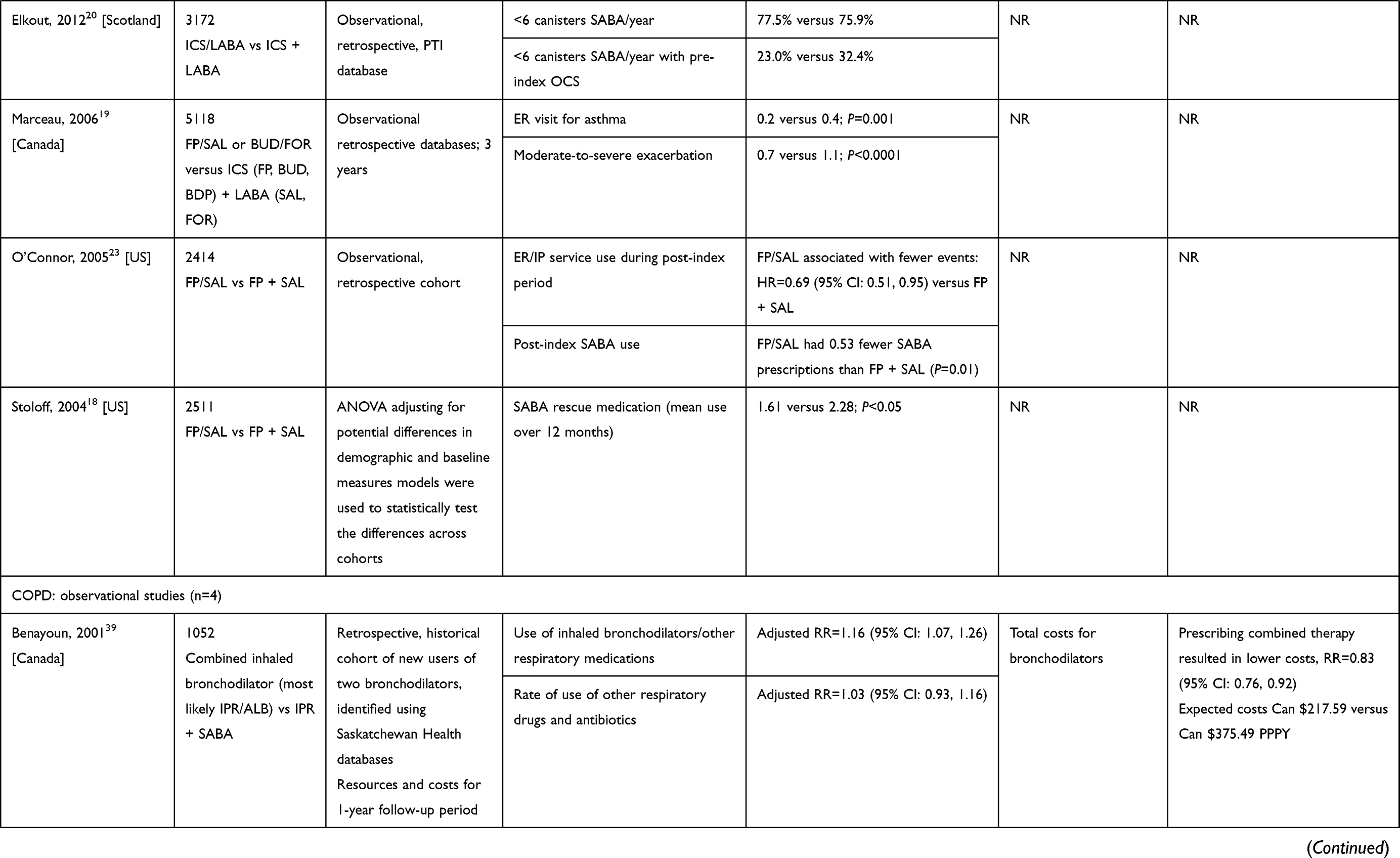 | 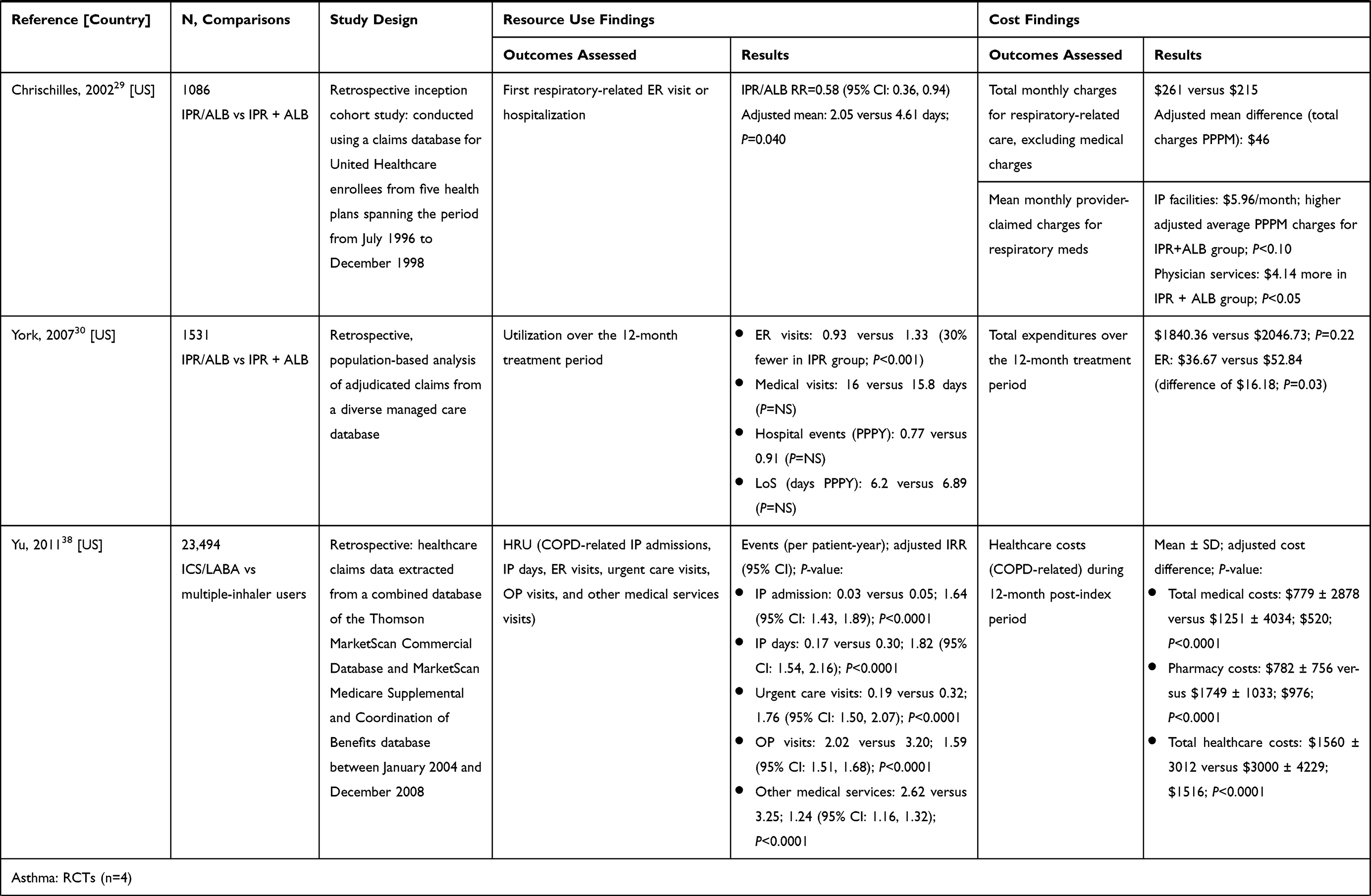 | 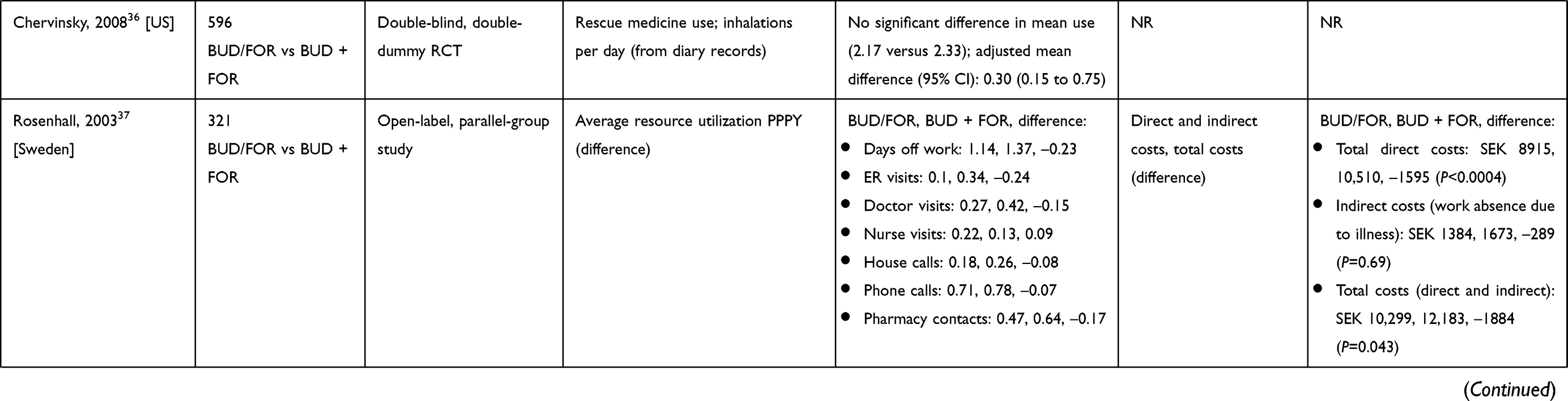 |
Table 2 Healthcare Resource Utilization and Costs |
Evidence from Non-Randomized Studies
Overall, evidence from six (of six) non-randomized (asthma, n=3; COPD, n=3) studies indicated that use of a single inhaler may be associated with a considerable reduction in emergency room (ER) visits and/or hospitalizations compared with equivalent therapies administered in separate inhalers (Table 2). In a study of asthma patients aged over 15 years in the US (n=2414), use of a single-inhaler combination (FP/SAL) was associated with an approximately 30% lower likelihood of having a hospitalization or ER event (OR=0.69; 95% CI: 0.51, 0.95) compared with multiple-inhaler components (FP + SAL), over a 12-month period.23 In a second study conducted in the US (n=2426), single-inhaler users (FP/SAL) experienced fewer acute respiratory exacerbations (AREs) than multiple-inhaler users (BDP + SAL); however, the difference did not reach statistical significance (OR=0.67; 95% CI: 0.44, 1.01; P=0.055).21 When considering only patients with an ARE in the previous 6 months, those who received the single inhaler in the post-index period had an approximately 47% lower likelihood of a subsequent ARE (OR=0.527; 95% CI: 0.291, 0.954; P=0.034).21 In a Canadian study (n=5118), rates of ER visits during treatment and moderate-to-severe asthma exacerbations 6 months after treatment cessation were significantly lower for single-inhaler users than their matched counterparts on multiple-inhaler therapy (0.7 versus 1.1 per patient per year [PPPY], P<0.0001; and 0.2 versus 0.4, P=0.001, respectively).19
In COPD, similar findings were observed. In one study (n=1086), the risk of ER use or hospitalization was significantly less (relative risk [RR]=0.58; 95% CI: 0.36, 0.94) for single-inhaler users of IPR/ALB compared with multiple-inhaler users.29 Additionally, of those with at least one hospitalization, the adjusted mean hospital length of stay (LoS) was lower for single- versus multiple-inhaler users (2.05 versus 4.61 days; P=0.040.) In a US study (n=23,494), Yu et al38 also found a significant difference in favor of single-inhaler users in relation to outpatient visits (2.02 versus 3.20; incidence rate ratio [IRR]=1.59 [95% CI: 1.51, 1.68]; P<0.0001), inpatient (IP) admissions (0.03 versus 0.05; IRR=1.64 [95% CI: 1.43, 1.89]; P<0.0001), urgent care visits (0.19 versus 0.32; IRR=1.76 [95% CI: 1.50, 2.07]; P<0.0001), and IP days (0.17 versus 0.30; IRR=1.82 [95% CI: 1.54, 2.16]; P<0.0001) over 12 months. Finally, in the study by York30 (n=1531), use of a single inhaler (IPR/ALB versus IPR + ALB) was associated with lower rates of ER visits (0.93 versus 1.33; P<0.001) and ER costs ($36.67 versus $52.84; P=0.03). In this study, however, there was no significant difference in hospital events PPPY, described as medical office visits, ER visits, and hospitalizations (0.77 versus 0.91; P=NS), or LoS. Regarding other medical services, Yu et al38 reported significantly higher use of other medical services (2.62 versus 3.25; IRR=1.24 [95% CI: 1.16, 1.32]; P<0.0001) and outpatient visits (2.02 versus 3.20; IRR=1.59 [95% CI: 1.51, 1.68]; P<0.0001) for multiple-inhaler users, whereas the York study30 showed no significant difference in medical visits (16 versus 15.8 days; P=NS).
In addition to lower rates of hospitalization and ER admission observed for single versus multiple inhalers, evidence was identified to suggest that single-inhaler use may be associated with a decrease in rescue medication usage over 6 and 12 months, compared with multiple inhalers. This was demonstrated by five (of seven) observational studies in asthma (including three US studies) where the rates of short-acting β2-agonists (SABA) use were consistently, and in most cases significantly, lower for single- versus multiple-inhaler users (Table 2). In one US study of individuals (n=2414) aged over 15 years, FP/SAL users had 0.53 fewer SABA prescriptions than FP + SAL users (P=0.01) over 12 months.23 Another US study (n=2426) found a greater reduction in SABA use with FP/SAL compared with BDP + SAL (–0.66 canister equivalents over 6 months; P<0.001).21 Finally, Stoloff et al18 found that the FP/SAL cohort had a significantly lower mean number of SABA claims dispensed in the 12-month post-index period compared with that in the FP + SAL cohort (1.61 versus 2.28; P<0.05). Similar findings were observed in a retrospective study in the United Kingdom.34 Prescription data for 10,454 asthmatic children using LABA and ICS either as a single inhaler or concurrently in separate inhalers were identified. The mean age during the study years (2002–2006) was between 8 and 10 years. In each year of the study, patients on concurrent therapy more often required at least one oral corticosteroid (OCS) course than did those on combination therapy (ORs, 2002=1.9; 2003=2.1; 2004=1.8; 2005=1.6). Additionally, patients using concurrent therapy more often required six or more SABA prescriptions annually than those using combination therapy (78% versus 68%, P<0.001; OR=1.7 for 2005–2006, P=0.005).34 Another observational study in asthma (n=5118) found that patients using single inhalers had less SABA use over the year versus multiple-inhaler users, but statistical differences were not assessed.19 None of the COPD non-randomized studies reported differences in SABA use between groups.
A US asthma study (n=2426) found a lower likelihood of filling an OCS prescription for FP/SAL compared with BDP + SAL (35.8% versus 38.0%; OR=0.801 [95% CI: 0.662, 0.970]; P=0.023).21 The authors also reported a higher usage of daily doses of ≥400 μg of ICS (32.0% versus 10.0%; P<0.001).
Evidence from Clinical Trials
Asthma RCTs that tested exacerbation-related endpoints statistically did not identify any differences between single and multiple inhalers (see Supplementary Table 1).19,35,42–45 Of the four RCTs in COPD patients, one, which compared IPR/ALB-metered-dose inhaler, IPR/ALB-Respimat, and IPR + ALB (n=465), found that the time to first exacerbation did not differ significantly between groups.32 Another study (n=213) found that single-inhaler FP/SAL was similar to the equivalent separate inhalers based on annual exacerbation rates.31
Regarding HRU and costs, among asthma studies, four clinical studies investigated HRU, specifically direct and indirect costs,35,37 and rescue medication use27,36 (Table 2). In two studies (n=1776 and n=321) it was found that direct costs were significantly lower (P<0.001) with single-inhaler treatment versus separate inhalers, although there were no statistically significant changes reported in HRU.35,37 No significant differences between single- or multiple-inhaler therapy were reported for rescue medication use in studies performed in the US (n=596) and in Europe (n=362).27,36
One prospective, open-label, COPD RCT (n=213) also reported HRU and described more days in hospital (21.9 ± 23.1 versus 18.1 ± 18.0) and the intensive care unit (2.2 ± 8.4 versus 1.0 ± 2.6), and higher percentage of patients hospitalized (23% versus 17%), with FP/SAL single-inhaler treatment compared with multiple inhalers.31 Three COPD RCTs (participant range, n=193 to n=1704) also reported small numerical differences in rescue medication use.32,40,41
Cost and Cost-Effectiveness
Data on cost and cost-effectiveness of single versus multiple inhalers were reported in observational studies and RCTs in asthma (n=1 and n=2, respectively) and COPD (n=4 and n=1, respectively). Costs reported include direct costs (drug and medical costs) as well as indirect costs (eg, ER costs).
Evidence from Non-Randomized Studies
One asthma study reported the cost-effectiveness of single- versus multiple-inhaler therapies via a retrospective health-economic evaluation,33 and four observational studies in COPD reported costs with a retrospective cohort design using various claims databases.29,30,38,39
Brüggenjürgen et al33 (2010) conducted a cost-minimization analysis of BDP/FOR versus BDP + FOR in separate inhalers (n=645) and found that the combination therapy showed reduced drug costs (€272 versus €353) and total medical costs (€525 versus €637), with an incremental cost-effectiveness ratio of –€9.77 per additional day free of asthma symptoms in favor of BDP/FOR, based on the percentage of patients hospitalized due to severe exacerbations. Two retrospective studies of IPR/ALB in COPD (n=1086 and n=1052) reported that single inhalers were associated with a lower mean drug cost when compared with multiple inhalers ($215 versus $261 and $217.59 versus $375.49, respectively).29,39 Statistically significant differences were found for ER costs (–$16.18; P=0.03) in favor of IPR/ALB versus IPR + ALB in a third study (n=1531).30 Lastly, in a COPD study comparing single-inhaler users of ICS/LABA versus multiple-inhaler users (n=23,494), the total medical costs ($779 ± $2878 versus $1251 ± $4034; adjusted cost difference $520; P<0.0001), total pharmacy costs ($782 ± $756 versus $1749 ± $1033; $976; P<0.0001), and total healthcare costs ($1560 ± $3012 versus $3000 ± $4229; $1516; P<0.0001) were all in favor of the single inhaler.38
Evidence from Clinical Trials
Two asthma clinical studies reported the cost and/or cost-effectiveness of single- versus multiple-inhaler therapies with a health-economic evaluation,35,37 and one COPD study reported cost and cost-effectiveness via a health-economic evaluation of a RCT.31
The two open-label asthma studies (n=1776 and n=321) conducted prospective health-economic analyses of BUD/FOR and BUD + FOR.35,37 Rosenhall et al37 (2003) reported that, when comparing single- to multiple-inhaler therapy, there was a statistically significant decrease in direct cost difference (Swedish Krona [SEK] –1595; P=0.0004) and total costs (SEK –1884; P=0.043), but not for indirect costs alone (SEK –289; P=0.69). Stallberg et al35 (2008) reported a statistically significant difference in total direct costs (SEK –796; P<0.001) for the single inhaler versus multiple inhalers. No difference was found for indirect costs (P=0.209) or total costs (P=0.855). Hagedorn et al31 (2013) reported COPD-related direct costs (n=213) and found that there was no difference between FP/SAL and FP + SAL (€831 versus €872, respectively).
Lung Function and Health-Related Quality of Life
Comparisons of symptoms and HRQoL in patients using single-inhaler versus multiple-inhaler therapy were reported in observational studies and randomized and real-world clinical trials in asthma (n=3, n=18, and n=1, respectively) and RCTs in COPD (n=4; see Supplementary Table 1). The Asthma Control Questionnaire (ACQ) or the Asthma Quality of Life Questionnaire (AQLQ) were used as evaluation tools in many of the included RCTs.25–28,36,37,42–49
Evidence from Non-Randomized Studies
Of the three prospective studies that looked at symptoms or HRQoL in asthma, two showed no differences between single versus multiple inhalers and one found significantly fewer symptoms.50
None of the retrospective observational studies in asthma and COPD comparing single- and multiple-inhaler therapy examined lung function. One prospective observational study in asthma (n=27) found that change from baseline in forced expiratory volume in 1 second (FEV1; mL) at 60 mins post-inhalation was significantly enhanced in those who used a single inhaler versus those using multiple inhalers (0.33 ± 0.23 versus 0.20 ± 0.16; P=0.02).50
Evidence from Clinical Trials
Of the 18 asthma and four COPD clinical studies that looked at different aspects of disease symptoms and HRQoL, including asthma symptom score, AQLQ, ACQ, and day- and night-time symptoms, only one double-blind RCT in asthma tested and found any statistically significant differences in a PRO endpoint, where the number of symptom-free days was statistically lower in patients treated with single-inhaler BDP/FOR compared with separate inhalers.44
For efficacy comparisons based on lung function, many of the asthma RCTs reported testing a non-inferiority hypothesis (n=3) or showing equivalence (n=5). In others, non-inferiority or equivalence margins were not defined (n=9), but results showed that the two treatment arms were comparable. Equivalence and non-inferiority were shown for FP/SAL,25,46,47,51 FP/FOR,42,43 BDP/FOR,44 and BDP/ALB,49 while comparable efficacy was shown for FP/SAL,26 BDP/FOR,52 IPR/SAL,50 FP/FOR,53 and BUD/FOR27,28,37,45,48,54 when comparing single-inhaler and equivalent multiple-inhaler therapies. Likewise, asthma RCTs that tested exacerbation-related endpoints statistically did not show any differences between single and multiple inhalers (see Supplementary Table 1).19,35,42–45 Of the four RCTs in COPD patients, one (n=1704) found that single-inhaler BUD/FOR provided significantly greater efficacy when compared with the equivalent separate inhalers for improving lung function at 6 months.41 The second (n=193) was designed to test a non-inferiority hypothesis and found that indacaterol [IND]/glycopyrronium [GLY] in a single inhaler was as effective as two separate inhalers at 4 weeks, based on a primary outcome of trough FEV1.40 The other two studies (n=213 and n=465) reported comparable efficacy for single- and multiple-inhaler FP/SAL and IPR/ALB,31,32 although no non-inferiority or equivalence hypotheses were tested.
Safety Results (All Studies)
Of the studies listed in Supplementary Table 1, 13 clinical studies in asthma25,27,28,35,37,42–49 and four clinical studies in COPD31,32,40,41 reported descriptive rates of AEs, but did not test for significance statistically between single and multiple inhalers.
Risk of Bias
Among the interventional studies, most of those that had a double-blind design were considered to be associated with the least risk of bias (selection, performance, attrition, and detection bias).25,27,40–42,44–49,51 Seven studies with an open-label design,28,31,32,37,43,52,54 and one double-blind study where the blinding method was not reported,26 were considered to be associated with a greater risk for bias. Most of the observational studies included within this systematic literature review were rated as having a greater risk of bias because of factors inherent in such analyses, such as non-random treatment assignment, potential for incomplete data, inability to determine disease severity from claims data, or possible imbalances in groups due to matching techniques used in database analyses.
Discussion
This systematic literature review focusing on single-inhaler therapy in the treatment of asthma and COPD sought to include a wide range of studies that compared single-inhaler dual therapies with multiple inhalers containing the same drugs. Studies identified in the literature included both observational and clinical interventional studies. In addition to clinical efficacy outcomes, patient adherence (including compliance and persistence) to therapy is of particular interest because of the potential for improvement if the single-inhaler therapy is easier for patients to use correctly. For the purpose of this review, several measures were considered relevant for the adherence outcome, such as medication usage (including self-reported), prescription/refill rates, MPR, treatment days, treatment interruptions, and residual treatment. The majority of studies tested for differences in adherence rates statistically, including log-rank, regression, analysis of variance (ANOVA), or multivariate modeling techniques – except in a single clinical study in asthma25 and two clinical studies in COPD,31,32 which presented descriptive results only. While adherence rates in retrospective observational studies in asthma and COPD were often statistically significantly17–19,21–23,30 or numerically29 better in patients using a single inhaler compared with those using multiple inhalers, rates were comparable in one case.20 Similarly, while adherence rates in RCTs in asthma and COPD were, as expected, generally high, particularly when compared with those reported in observational studies, discrepancies were apparent when differences were tested statistically, with either no difference26 or significance favoring single-inhaler therapy reported.28,32 This may be partly explained by the broad range of outcomes that was used to measure adherence in these studies, particularly as all six retrospective observational studies in asthma consistently reported enhanced rates with single-inhaler therapy when recording prescription/refill rates as the outcome measure. The lack of difference between single- and multiple-inhaler therapy seen in the majority of clinical studies may be explained by the fact that RCTs do not generally replicate treatment patterns occurring in a real-world setting, and that more frequent study visits are often required, providing opportunities to reinforce adherence and inhaler technique. In addition, although treatment adherence was investigated in many of the studies, none investigated inhaler technique or inhaler errors directly.
Due to the negative impact of asthma and COPD symptoms and associated reduction in HRQoL, they are often utilized as clinical trial endpoints. However, with the exception of symptom-free days in one asthma RCT,44 RCTs that measured symptom scores or HRQoL showed no differences between treatment with single- or multiple-inhaler therapy, either statistically27,28,37,40–43,47–49 or numerically.26,31
Economic and HRU analyses conducted in observational studies showed either statistically significant19,21,23,29,30,34,38 or numerical40 advantages for single-inhaler therapy, and savings were shown in HRU, including lower rates of ER visits and hospitalizations when compared with separate inhalers. The costs of asthma or COPD medication and other medical services were also lower with single inhalers compared with multiple inhalers,39 the majority statistically significantly so.23,35–37 Cost considerations such as these are expected to be increasingly important to healthcare systems as the prevalence of COPD and consequent demands on healthcare resources are predicted to reach a peak in the near future.55 Single-inhaler therapy was also associated with less use of rescue medication, which may be indicative of superior symptom control, as demonstrated in asthma.18,19,21,23,34,36
No differences were found for lung function or exacerbation outcomes in asthma or COPD RCTs, possibly because most of the studies were directed at establishing non-inferiority of the single-inhaler therapy. However, several observational studies in asthma and COPD that recorded healthcare events consistent with exacerbations, such as ER visits and hospitalization, reported statistically significantly greater reductions in these events with single-inhaler treatment compared with the use of equivalent multiple inhalers.19,29,38 Clinical RCTs in asthma and COPD that compared lung function with single inhalers with multiple inhalers met prespecified endpoints (peak expiratory flow or FEV1) for demonstrating either non-inferiority or equivalence. Safety results as described in the published RCTs did not show any apparent differences between the single-inhaler and multiple-inhaler treatments. Therefore, it can be concluded that for both asthma and COPD, single inhalers are at least comparable in efficacy to multiple devices and without any additional safety concerns.
This systematic review revealed some gaps in studies conducted with single inhalers. For example, RCTs in this study, as expected, tended to focus on demonstrating equivalence or non-inferiority, and, given the well-controlled trial setting and high compliance and adherence rates typically seen in RCTs,25–27 observed no difference in treatment effects when comparing the same drugs in a single device or multiple devices. Real-world evidence may provide a better guide to how single combined inhalers may result in better outcomes, due to factors such as simplicity and reduced number of inhalers, which is especially helpful for patients with multiple comorbidities and polypharmacy. Furthermore, no studies comparing single and multiple inhalers for inhalation technique and errors in use were identified for inclusion in this review. It must also be noted that the delivery devices used for single- and multiple-inhaler therapy were not identified for the purpose of this review. Another particularly noticeable gap in the literature was the lack of studies that focused on caregivers, which is especially relevant for patients with COPD and pediatric asthmatics. Additionally, as noted above, the lack of PROs in the claims data source limits the types of outcomes that can be feasibly evaluated and hinders the assessment of this important aspect of disease management. None of the retrospective observational studies reported HRQoL or symptom scores, as these studies relied mainly on administrative claims as the source of data, which rarely capture PRO endpoints. This highlights an area for future research, given the importance of analyzing patient-relevant real-world benefits of therapies. Another potential area for future research would be to include patient satisfaction as an outcome which, although out of scope for the current study, may provide further insight into the benefits of SITT. All literature reviews are limited by publication bias in the available literature, in that studies with significant findings are more likely to be reported. Coverage may be incomplete because articles covered in this review are all English language and the search was limited to journal articles published since 1996 and congress abstracts published since 2013. The last database search was carried out in 2016; therefore, it may be beneficial for a more recent systematic search of the literature to be performed to ensure that no relevant articles are omitted. Addressing all these gaps would provide a more complete view of real-world patient experience and/or behavior as applied to the comparison of single-inhaler and multiple-inhaler treatments.
As expected, this systematic review found that there are clear differences between RCTs and observational studies in terms of outcome measures and results, and that RCTs may not provide the best evidence, as they are often short term and restricted by a controlled environment. For example, the adherence rates in RCTs reported in this study are unlikely to reflect those observed in the real world. Substantial differences that favored single-inhaler therapy were noted in terms of direct and indirect costs (in analyses that included and excluded the cost of medications) and HRU, in large observational cohorts of around 5000 asthma patients21,23 and over 5 years in 23,494 patients with COPD in the US.38 Depending on the measure of adherence used, differences were observed, with rates based on prescription and refill rates favoring single-inhaler therapy, compared with rates based on MPRs and dispensed doses, which were generally comparable. Retrospective and prospective studies showed that using a single inhaler was associated with decreased HRU and improved cost-effectiveness compared with multiple inhalers. However, lung function with a single inhaler versus multiple inhalers was generally comparable. The lack of consistent results between observational and clinical studies was most likely due to differences in study design.
Conclusions
Retrospective and prospective studies showed that single-inhaler use was associated with decreased healthcare resource utilization and improved cost-effectiveness compared with multiple inhalers. Lung function and exacerbation rates were mostly comparable depending on study design and duration of follow-up. Several observational studies in asthma and COPD reported significantly greater reductions in events consistent with exacerbations with single-inhaler treatment. Overall, due to the lack of long-term data and the difficulty in comparing outcomes due to differences in outcome definitions and study designs, robust conclusions regarding the differences between single- and multiple-inhaler users cannot be made. Although substantial descriptive data allow us to make some general conclusions about the benefits of single-inhaler therapy, many lack the clarity provided by statistical comparisons. However, evidence from non-randomized studies was largely consistent, in terms of showing benefits for single-inhaler users compared with multiple-inhaler users receiving the same medication.
Abbreviations
ACQ, Asthma Control Questionnaire; AE, adverse event; ALB, albuterol; ANOVA, analysis of variance; AQLQ, Asthma Quality of Life Questionnaire; ARE, acute respiratory exacerbation; BDP, beclomethasone dipropionate; BSA, beclomethasone; BUD, budesonide; Can, Canadian; CE, cost-effectiveness; CHEERS, Consolidated Health Economic Evaluation Reporting Standards; CI, confidence interval; COPD, chronic obstructive pulmonary disease; ER, emergency room; FEV1, forced expiratory volume in 1 second; FOR, formoterol; FP, fluticasone propionate; GLY, glycopyrronium; HR, hazard ratio; HRU, healthcare resource utilization; HRQoL, health-related quality of life; ICER, incremental cost-effectiveness ratio; ICS, inhaled corticosteroid; ICU, intensive care unit; IND, indacaterol; IP, inpatient; IPR, ipratropium; IRR, incidence rate ratio; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; LoS, length of stay; LS, least-squares; M + R, maintenance and reliever; MC, multicenter; MDI, metered-dose inhaler; med, medication; MPR, medication possession ratio; NICE, National Institute for Health and Care Excellence; NR, not reported; NS, not significant; OCS, oral corticosteroid; OP, outpatient; OR, odds ratio; PASAPQ, Patient Satisfaction and Preference Questionnaire; PCP, primary care physician; PPPM, per patient per month; PPPY, per patient per year; PRO, patient-reported outcome; PTI, practice team information; QoL, quality of life; RCT, randomized controlled trial; RR, relative risk; SABA, short-acting β2-agonist; SAL, salmeterol; SD, standard deviation; SEK, Swedish Krona; Tx, treatment; UK, United Kingdom; US, United States.
Acknowledgment
The authors received editorial support (in the form of writing assistance, assembling tables and figures, collating author comments, grammatical editing, and referencing) from Tom Gallagher, PhD, and Bonnie Nicholson, PhD, of Gardiner-Caldwell Communications, Macclesfield, UK, which was funded by GlaxoSmithKline plc.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The database searches, literature evaluation, and writing assistance for the preparation of this systematic literature review were funded by GlaxoSmithKline plc. (study number HO-16-13836).
Disclosure
DK is a former GlaxoSmithKline plc. employee and is currently employed by Forest Systematic Reviews Ltd, contracted by GlaxoSmithKline plc; she was not paid for development of this publication. SZ and ASI are employees of, and hold shares in, GlaxoSmithKline plc.; ASI is also an unpaid part-time professor at McMaster University, Canada. VMR is an employee of Optum Inc., which was contracted by GlaxoSmithKline plc. to conduct the systematic literature review; she was not paid for development of this publication. The authors report no other conflicts of interest in this work.
References
1. Global Asthma Network. The global asthma report; 2014. Available from: http://www.globalasthmareport.org/2014/index.php.
2. World Health Organization. Chronic obstructive pulmonary disease (COPD) fact sheet; 2015. Available from: http://www.who.int/mediacentre/factsheets/fs315/en/.
3. Nurmagambetov T, Kuwahara R, Garbe P. The economic burden of asthma in the United States, 2008–2013. Ann Am Thorac Soc. 2018;15(3):348–356. doi:10.1513/AnnalsATS.201703-259OC
4. Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–245. doi:10.2147/CEOR.S34321
5. Patel JG, Nagar SP, Dalal AA. Indirect costs in chronic obstructive pulmonary disease: a review of the economic burden on employers and individuals in the United States. Int J Chron Obstruct Pulmon Dis. 2014;9:289–300. doi:10.2147/COPD.S57157
6. Svedsater H, Roberts J, Patel C, Macey J, Hilton E, Bradshaw L. Life impact and treatment preferences of individuals with asthma and chronic obstructive pulmonary disease: results from qualitative interviews and focus groups. Adv Ther. 2017;34(6):1466–1481. doi:10.1007/s12325-017-0557-0
7. US Dept of Health and Human Services National Heart, Lung and Blood Institute (NHLBI). Guidelines for the diagnosis and management of asthma. National Asthma Education and Prevention Program Expert Panel Report 3, Summary Report; October 2017. NIH Publication Number 08-5846.
8. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
9. Melani AS, Bonavia M, Cilenti V, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105(6):930–938. doi:10.1016/j.rmed.2011.01.005
10. Press VG, Arora VM, Shah LM, et al. Misuse of respiratory inhalers in hospitalized patients with asthma or COPD. J Gen Intern Med. 2011;26(6):635–642. doi:10.1007/s11606-010-1624-2
11. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2019. Available from: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf.
12. Cazzola M, Matera MG. Fixed-dose combination inhalers. Handb Exp Pharmacol. 2017;237:117–129.
13. Chantaphakul H, Ruxrungtham K. Fixed-dose combination of the inhaled corticosteroid and long-acting beta2-agonist therapy in adults with persistent asthma. Expert Opin Pharmacother. 2016;17(5):631–642. doi:10.1517/14656566.2016.1145659
14. Rodrigo GJ, Neffen H. A systematic review of the efficacy and safety of a fixed-dose combination of umeclidinium and vilanterol for the treatment of COPD. Chest. 2015;148(2):397–407. doi:10.1378/chest.15-0084
15. National Institute for Health and Care Excellence. Developing NICE guidelines: the manual [Appendix H]. London; 2015. Available from: https://www.nice.org.uk/process/pmg20/resources/appendix-h-pdf-2549710190.
16. Husereau D, Drummond M, Petrou S, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Value Health. 2013;16(2):e1–e5. doi:10.1016/j.jval.2013.02.010
17. Stempel DA, Stoloff SW, Carranza Rosenzweig JR, Stanford RH, Ryskina KL, Legorreta AP. Adherence to asthma controller medication regimens. Respir Med. 2005;99(10):1263–1267. doi:10.1016/j.rmed.2005.03.002
18. Stoloff SW, Stempel DA, Meyer J, Stanford RH, Carranza Rosenzweig JR. Improved refill persistence with fluticasone propionate and salmeterol in a single inhaler compared with other controller therapies. J Allergy Clin Immunol. 2004;113(2):245–251. doi:10.1016/j.jaci.2003.10.011
19. Marceau C, Lemiere C, Berbiche D, Perreault S, Blais L. Persistence, adherence, and effectiveness of combination therapy among adult patients with asthma. J Allergy Clin Immunol. 2006;118(3):574–581. doi:10.1016/j.jaci.2006.06.034
20. Elkout H, Helms PJ, Simpson CR, McLay JS. Adequate levels of adherence with controller medication is associated with increased use of rescue medication in asthmatic children. PLoS One. 2012;7(6):e39130. doi:10.1371/journal.pone.0039130
21. Chan J, Hui RL, Spence MM. Effects on resource utilization of adding salmeterol in combination or separately to inhaled corticosteroids. J Manag Care Pharm. 2007;13(1):21–27.
22. Rosenhall L, Borg S, Andersson F, Ericsson K. Budesonide/formoterol in a single inhaler (Symbicort) reduces healthcare costs compared with separate inhalers in the treatment of asthma over 12 months. Int J Clin Pract. 2003;57(8):662–667.
23. O’Connor RD, Rosenzweig JR, Stanford RH, et al. Asthma-related exacerbations, therapy switching, and therapy discontinuation: a comparison of 3 commonly used controller regimens. Ann Allergy Asthma Immunol. 2005;95(6):535–540. doi:10.1016/S1081-1206(10)61015-0
24. Latry P, Pinet M, Labat A, et al. Adherence to anti-inflammatory treatment for asthma in clinical practice in France. Clin Ther. 2008;30(Spec No):1058–1068. doi:10.1016/j.clinthera.2008.06.011
25. Aubier M, Pieters WR, Schlosser NJ, Steinmetz KO. Salmeterol/fluticasone propionate (50/500 microg) in combination in a Diskus inhaler (seretide) is effective and safe in the treatment of steroid-dependent asthma. Respir Med. 1999;93(12):876–884. doi:10.1016/S0954-6111(99)90053-7
26. Perrin K, Williams M, Wijesinghe M, James K, Weatherall M, Beasley R. Randomized controlled trial of adherence with single or combination inhaled corticosteroid/long-acting beta-agonist inhaler therapy in asthma. J Allergy Clin Immunol. 2010;126(3):505–510. doi:10.1016/j.jaci.2010.06.033
27. Zetterstrom O, Buhl R, Mellem H, et al. Improved asthma control with budesonide/formoterol in a single inhaler, compared with budesonide alone. Eur Respir J. 2001;18(2):262–268. doi:10.1183/09031936.01.00065801
28. Rosenhall L, Heinig JH, Lindqvist A, Leegaard J, Stahl E, Bergqvist PB. Budesonide/formoterol (Symbicort) is well tolerated and effective in patients with moderate persistent asthma. Int J Clin Pract. 2002;56(6):427–433.
29. Chrischilles E, Gilden D, Kubisiak J, Rubenstein L, Shah H. Delivery of ipratropium and albuterol combination therapy for chronic obstructive pulmonary disease: effectiveness of a two-in-one inhaler versus separate inhalers. Am J Manag Care. 2002;8(10):902–911.
30. York JM, Smeeding J, Brook RA, Hoehler F, Klein GL. Exploratory economic evaluation of patients with COPD on a combination product versus individual components (ipratropium bromide and albuterol). Adv Ther. 2007;24(4):757–771. doi:10.1007/BF02849969
31. Hagedorn C, Kassner F, Banik N, Ntampakas P, Fielder K. Influence of salmeterol/fluticasone via single versus separate inhalers on exacerbations in severe/very severe COPD. Respir Med. 2013;107(4):542–549. doi:10.1016/j.rmed.2012.12.020
32. Ferguson GT, Ghafouri M, Dai L, Dunn LJ. COPD patient satisfaction with ipratropium bromide/albuterol delivered via Respimat: a randomized, controlled study. Int J Chron Obstruct Pulmon Dis. 2013;8:139–150. doi:10.2147/COPD.S38577
33. Brüggenjürgen B, Ezzat N, Kardos P, Buhl R. Economic evaluation of BDP/formoterol fixed versus two single inhalers in asthma treatment. Allergy. 2010;65(9):1108–1115. doi:10.1111/j.1398-9995.2009.02317.x
34. Elkout H, McLay JS, Simpson CR, Helms PJ. A retrospective observational study comparing rescue medication use in children on combined versus separate long-acting beta-agonists and corticosteroids. Arch Dis Child. 2010;95(10):817–821. doi:10.1136/adc.2009.179069
35. Stallberg B, Ekstrom T, Neij F, et al. A real-life cost-effectiveness evaluation of budesonide/formoterol maintenance and reliever therapy in asthma. Respir Med. 2008;102(10):1360–1370. doi:10.1016/j.rmed.2008.06.017
36. Chervinsky P, Baker J, Bensch G, et al. Patient-reported outcomes in adults with moderate to severe asthma after use of budesonide and formoterol administered via 1 pressurized metered-dose inhaler. Ann Allergy Asthma Immunol. 2008;101(5):463–473. doi:10.1016/S1081-1206(10)60284-0
37. Rosenhall L, Elvstrand A, Tilling B, et al. One-year safety and efficacy of budesonide/formoterol in a single inhaler (Symbicort Turbuhaler) for the treatment of asthma. Respir Med. 2003;97(6):702–708. doi:10.1053/rmed.2003.1504
38. Yu AP, Guerin A, de Leon DP, et al. Clinical and economic outcomes of multiple versus single long-acting inhalers in COPD. Respir Med. 2011;105(12):1861–1871. doi:10.1016/j.rmed.2011.07.001
39. Benayoun S, Ernst P, Suissa S. The impact of combined inhaled bronchodilator therapy in the treatment of COPD. Chest. 2001;119(1):85–92. doi:10.1378/chest.119.1.85
40. Dahl R, Jadayel D, Alagappan VK, Chen H, Banerji D. Efficacy and safety of QVA149 compared to the concurrent administration of its monocomponents indacaterol and glycopyrronium: the BEACON study. Int J Chron Obstruct Pulmon Dis. 2013;8:501–508. doi:10.2147/COPD.S49615
41. Tashkin DP, Rennard SI, Martin P, et al. Efficacy and safety of budesonide and formoterol in one pressurized metered-dose inhaler in patients with moderate to very severe chronic obstructive pulmonary disease: results of a 6-month randomized clinical trial. Drugs. 2008;68(14):1975–2000. doi:10.2165/00003495-200868140-00004
42. Bodzenta-Lukaszyk A, Pulka G, Dymek A, et al. Efficacy and safety of fluticasone and formoterol in a single pressurized metered dose inhaler. Respir Med. 2011;105(5):674–682. doi:10.1016/j.rmed.2010.11.011
43. Bodzenta-Lukaszyk A, van Noord J, Schroder-Babo W, McAulay K, McIver T. Efficacy and safety profile of fluticasone/formoterol combination therapy compared to its individual components administered concurrently in asthma: a randomised controlled trial. Curr Med Res Opin. 2013;29(5):579–588. doi:10.1185/03007995.2013.772506
44. Huchon G, Magnussen H, Chuchalin A, Dymek L, Gonod FB, Bousquet J. Lung function and asthma control with beclomethasone and formoterol in a single inhaler. Respir Med. 2009;103(1):41–49. doi:10.1016/j.rmed.2008.09.002
45. Jenkins C, Kolarikova R, Kuna P, et al. Efficacy and safety of high-dose budesonide/formoterol (Symbicort) compared with budesonide administered either concomitantly with formoterol or alone in patients with persistent symptomatic asthma. Respirology. 2006;11(3):276–286. doi:10.1111/j.1440-1843.2006.00856.x
46. Van den Berg NJ, Ossip MS, Hederos CA, Anttila H, Ribeiro BL, Davies PI. Salmeterol/fluticasone propionate (50/100 microg) in combination in a Diskus inhaler (seretide) is effective and safe in children with asthma. Pediatr Pulmonol. 2000;30(2):97–105. doi:10.1002/1099-0496(200008)30:2<97::AID-PPUL4>3.0.CO;2-P
47. Chapman KR, Ringdal N, Backer V, Palmqvist M, Saarelainen S, Briggs M. Salmeterol and fluticasone propionate (50/250 microg) administered via combination Diskus inhaler: as effective as when given via separate Diskus inhalers. Can Respir J. 1999;6(1):45–51. doi:10.1155/1999/894803
48. Noonan M, Rosenwasser LJ, Martin P, O’Brien CD, O’Dowd L. Efficacy and safety of budesonide and formoterol in one pressurised metered-dose inhaler in adults and adolescents with moderate to severe asthma: a randomised clinical trial. Drugs. 2006;66(17):2235–2254. doi:10.2165/00003495-200666170-00006
49. Papi A, Canonica GW, Maestrelli P, et al. Rescue use of beclomethasone and albuterol in a single inhaler for mild asthma. N Engl J Med. 2007;356(20):2040–2052. doi:10.1056/NEJMoa063861
50. Mohan A, Guleria R, Das C, Sharma R. Comparison of the efficacy of inhaled ipratropium bromide and salbutamol sequentially and in fixed dose combination in patients with stable bronchial asthma. Chest. 2003;124(4):139S. doi:10.1378/chest.124.4_MeetingAbstracts.139S-a
51. Kawai M, Kempsford R, Pullerits T, et al. Comparison of the efficacy of salmeterol/fluticasone propionate combination in Japanese and Caucasian asthmatics. Respir Med. 2007;101(12):2488–2494. doi:10.1016/j.rmed.2007.07.001
52. Chawes BL, Piccinno A, Kreiner-Moller E, et al. Pharmacokinetic comparison of inhaled fixed combination vs. the free combination of beclomethasone and formoterol pMDIs in asthmatic children. Br J Clin Pharmacol. 2013;75(4):1081–1088. doi:10.1111/j.1365-2125.2012.04459.x
53. Hochhaus G, Kaiser K. Comparing the safety and efficacy of fluticasone/formoterol combination therapy in a single inhaler at low and medium doses, with fluticasone and formoterol concurrently or alone, in asthma patients. Allergy. 2011;66:585. doi:10.1111/j.1398-9995.2011.02683.x
54. Miller CJ, Senn S, Mezzanotte WS. Bronchodilation of formoterol administered with budesonide: device and formulation effects. Contemp Clin Trials. 2008;29(2):114–124. doi:10.1016/j.cct.2007.05.008
55. Simpson CR, Hippisley-Cox J, Sheikh A. Trends in the epidemiology of chronic obstructive pulmonary disease in England: a national study of 51 804 patients. Br J Gen Pract. 2010;60(576):277–284. doi:10.3399/bjgp10X514729
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.