")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 8
Impact of Sarcopenia on Two-Year Mortality in Patients with HCV-Associated Hepatocellular Carcinoma After Radiofrequency Ablation
Authors Salman A , Salman M , Moustafa A , Shaaban HE , El-Mikkawy A, Labib S, Youssef A, Omar MG , Matter M, Elkassar H
Received 15 January 2021
Accepted for publication 25 March 2021
Published 29 April 2021 Volume 2021:8 Pages 313—320
DOI https://doi.org/10.2147/JHC.S300680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Ahmed Salman,1 Mohamed Salman,2 Ahmed Moustafa,3 Hossam El-Din Shaaban,4 Ahmed El-Mikkawy,5 Safa Labib,1 Ahmed Youssef,1 Mahmoud Gouda Omar,1 Mohamed Matter,6 Hesham Elkassar1
1Internal Medicine Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 2General Surgery Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 3Department of Endemic Medicine and Hepatology, Faculty of Medicine, Cairo University, Cairo, Egypt; 4Gastroenterology Department, National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt; 5Hepatology and Gastroenterology Department, Theodor Bilharz Research Institute, Cairo, Egypt; 6Radiodiagnosis Department, Faculty of Medicine, Alazhar University, Cairo, Egypt
Correspondence: Ahmed Salman
Internal Medicine Department, Faculty of Medicine, Cairo University, 110 L Hadayek Alahram, 11311, Cairo, Egypt
Tel +201000468664
Email [email protected]
Purpose: Radiofrequency ablation (RFA) appears effective for the treatment of hepatocellular carcinoma (HCC). Evaluation of prognostic factors is imperative for patient selection and improving treatment efficacy. This study aimed to assess sarcopenia as a predictor of the outcome of RFA in patients with HCC.
Methods: This prospective study included all patients with HCC on top of HCV-related cirrhosis who underwent RFA and followed up for a minimum of two years. CT scan was used to determine the skeletal muscle index at the psoas, erector spinae, quadratus lumborum, transversus abdominis, external and internal obliques, and rectus abdominis muscles. Cross-sectional areas were calculated to obtain a lumbar skeletal muscle index (L3-SMI).
Results: A total of 97 patients were enrolled in the study. The L3-SMI was 46.2± 12.1 cm2/m2. Older age was the only risk factor associated with sarcopenia (p = 0.001). The overall survival at two years for the whole group was 65.2%. Sarcopenia and MELD score were independent predictors of OS at two years with HR of 7.6 (95% CI: 3.1– 18.7) and 2.2 (95% CI: 1.0– 4.8), respectively. Recurrence-free survival was 84.1% at two years. Recurrence was not affected by all factors, including sarcopenia.
Conclusion: Sarcopenia is a surrogate predictor of overall survival at two years in HCC patients after RFA. Sarcopenia assessment might be an additional prognostic indicator with conventional biomarkers to optimize the selection criteria for receiving RFA for early-stage HCC.
Keywords: sarcopenia, mortality, hepatocellular carcinoma, radiofrequency ablation
Introduction
Worldwide, hepatocellular carcinoma (HCC) is the 7th most common cancer and the 3rd leading cause of cancer-related deaths with an obvious heterogeneous geographical distribution. In Egypt, HCC is the most common cancer in Egyptian males.1 Many surgical and non-surgical approaches are available for the treatment of HCC. Non-surgical therapy includes local tumor ablation, transarterial embolization, and radiotherapy.2 Radiofrequency ablation (RFA) appears to be a local curative treatment of small HCC lesions (< 3 cm in diameter).3 Existing literature reported promising long-term effectiveness of RFA treatment.4–6 However, the evaluation of prognostic factors is imperative for patient selection and improving treatment efficacy.
Sarcopenia is a progressive and generalized skeletal muscle disease characterized by accelerated loss of muscle mass and function.7 It has been associated with higher mortality among the general population8,9 and patients with cancer.8–10 Prevalence of sarcopenia varies widely from 1 to 29% among older people.11 Risk factors other than age include sex12 and inflammatory disease.13 Cancer patients are at risk of losing muscle mass due to anorexia, reduced physical activity, and aggressive treatment modalities.14,15 So far, sarcopenia’s effect on the outcome of RFA as a curative treatment of HCC is poorly investigated.16
This study aimed to assess the possible role of sarcopenia in predicting the outcome of radiofrequency ablation in patients with HCC.
Subjects and Methods
This prospective study included a consecutive sample of all patients with HCC who underwent RFA from August 2015 to April 2018. All patients were followed up for a minimum of two years after RFA. All patients gave informed consent for using their clinical, laboratory, and radiological data at the time of the first examination. The study protocol conformed to the Declaration of Helsinki (1975) and was approved by the local institutional review board. All organs were donated voluntarily with written informed consent, and that this was conducted in accordance with the Declaration of Istanbul.
In the current study, we recruited only patient with HCV-induced liver cirrhosis, and excluded patients with cirrhosis due to other etiologies, such as HBV, alcoholic liver diseases. The aim of this was to unify the studied population, as HCV-induced liver cirrhosis is the most prevalent cause of liver cirrhosis and HCC is Egypt.
Cirrhosis, diagnosed either by histology or clinically, was graded according to the Child-Turcotte-Pugh (CTP) classification and Model for End-stage Liver Disease (MELD) scores as liver impairment measures. HCC was diagnosed according to criteria of the American Association for the Study of Liver Disease17 and staged by abdominal contrast-enhanced dynamic CT scan or gadolinium-enhanced magnetic resonance imaging (MRI). Moreover, each patient underwent a chest X-ray/CT scan and bone scanning, as requested by the treating physicians.
Radiofrequency ablation was performed if the patient is a candidate for liver-directed procedures and meets the resectability criteria. These are liver-only disease and a single tumor < 4 cm in diameter with a CTP class A or B.
Initial data collection included age, sex, pre-treatment anthropometric features, laboratory findings including serum albumin, creatinine, international normality ratio (INR), complete blood picture, and alpha-fetoprotein (AFP), and dry weight body mass index (BMI). All data were obtained within two weeks before the RFA session. Follow-up ended after two years or upon patients’ death.
Image Analysis and Treatment Modality
CT scans were obtained routinely at baseline for tumor staging purposes within two weeks before initiating treatment and used to determine the skeletal muscle index (SMI). A transverse image at the level of L3 was chosen from each scan. Muscles at this level include psoas, erector spinae, quadratus lumborum, transversus abdominis, external and internal obliques, and the rectus abdominis.18 Obtained images were analyzed with SliceOmatic V 5.0 software (Tomovision, Montreal, Quebec, Canada), enabling specific tissue selection using previously determined Hounsfield units (HU). Skeletal muscle is selected and quantified by thresholds between –29 to +150 HU.19 These specific thresholds permit skeletal muscle assessment regardless of ascites in patients with cirrhosis, excluding muscular fat infiltration in the selected section. Two trained physicians checked all CT images. Cross-sectional areas were calculated and normalized for height as reported elsewhere20 to obtain a lumbar skeletal muscle index (L3-SMI).
The MRI imaging data were excluded to avoid methodological heterogeneity. L3-SMI was expressed in cm2/m2. L3-SMI was considered to indicate sarcopenia if ≤ 53 cm2/m2 in males with a BMI ≥ 25 or ≤ 43 cm2/m2 with a BMI < 25, and ≤ 41 cm2/m2 in women.21
Statistical Analysis
Statistical analysis was done using IBM© SPSS© Statistics version 23 (IBM© Corp., Armonk, NY, USA). Numerical data were expressed as mean and standard deviation or median and range as appropriate. Qualitative data were expressed as frequency and percentage. Chi-square test was used to examine the relation between qualitative variables. For quantitative data, comparison between two groups was made using independent sample t-test or Mann–Whitney test. Survival analysis was done using Kaplan-Meier method and comparison between two survival curves was done using Log rank test. Multivariate analysis was done using Cox proportional-hazards model for factors affecting survival on univariate analysis. Hazard ratio (HR) with it 95% confidence interval (CI) were used for hazard estimation. A p-value < 0.05 was considered significant.
Results
A total of 97 patients were enrolled in the study. Baseline and disease characteristics of the studied group are shown in Table 1, and laboratory findings in Table 2.
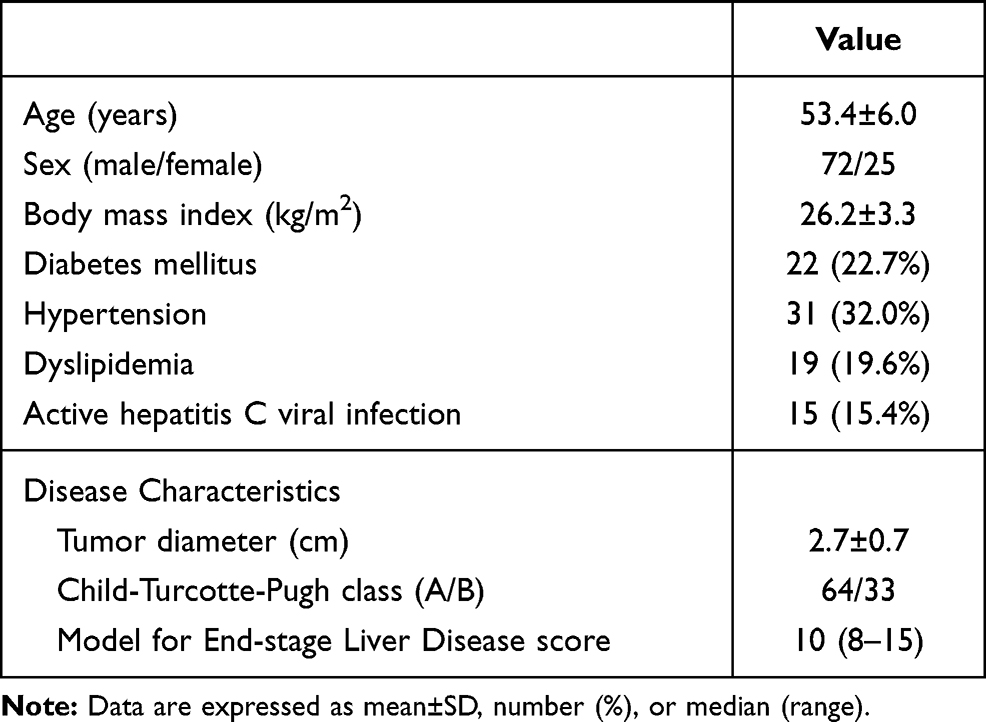 |
Table 1 Baseline and Clinical Characteristics of the Studied Group (n=97) |
 |
Table 2 Laboratory Results of the Studied Group (n=97) |
The L3-SMI of the whole studied group was 46.2±12.1 cm2/m2. Sarcopenia was diagnosed in 42 patients (43.3%). Table 3 shows a comparison between the Sarcopenia group (n=42) and those with normal muscle mass (Non-Sarcopenia group, n=55) regarding patients and disease factors. The only associated risk factor was older age in the sarcopenic group (p = 0.001).
 |
Table 3 Comparison Between Patients with and without Sarcopenia Regarding Possible Risk Factors |
During follow-up, 3 cases underwent transarterial chemoembolization, and 2 underwent transarterial radioembolization. Liver transplantation was done for 16 patients. At the end of follow-up, 33 patients died. Causes of death are shown in Table 4. The cumulative survival proportion at two years for the whole group (n=97) was 65.2%. Table 5 shows factors affecting overall survival. Sarcopenia was the only factor positively associated with worse survival at two-years (36.6% vs 85.5% for non-sarcopenic patients, p < 0.001). MELD score was near significance on univariate analysis (p = 0.053). On multivariate analysis, sarcopenia and MELD score were the only independent predictors of overall survival (Table 6). Sarcopenia carries a nearly 8-fold higher risk of death within 2 years. As a continuous variable, L3-SMI significantly affected overall survival in males, but not in females (Table 7). In males, higher SMI was associated with better survival with a HR of 0.95 (95% CI: 0.91–0.98).
 |
Table 4 Causes of Death in 33 Patients |
 |
Table 5 Factors Associated with Overall Survival at 2 Years in the Studied Group |
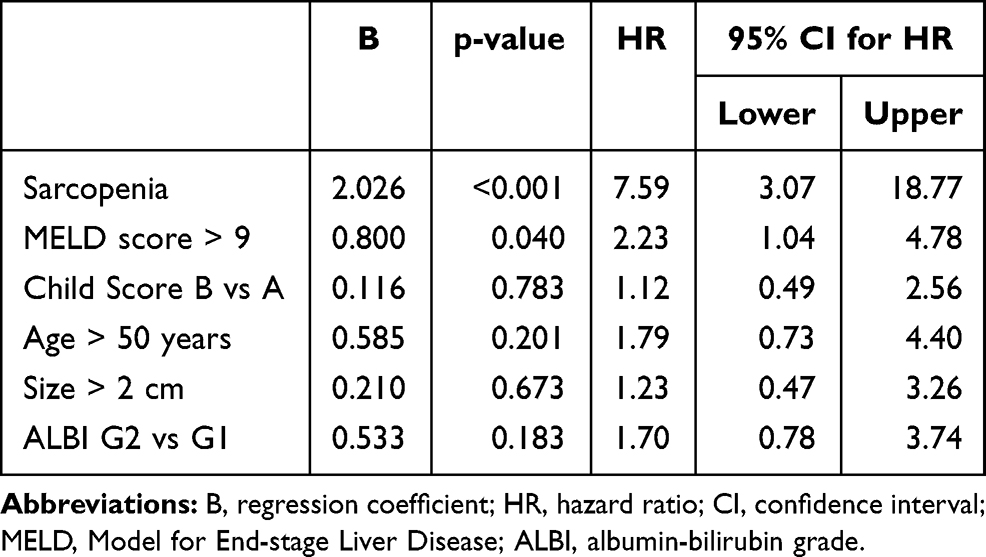 |
Table 6 Multivariate Cox Proportional Hazards Model for Factors Affecting Overall Survival |
 |
Table 7 Cox Proportional Hazards Model for Overall Survival and L3-SMI in Males and Females |
During follow up, 12 patients developed local recurrence. Recurrence-free survival was 84.1% at two years. Table 8 shows the factors associated with recurrence-free survival (RFS). RFS was not affected by all factors, including sarcopenia.
 |
Table 8 Factors Associated with Recurrence-Free Survival at Two Years in the Studied Group |
Discussion
The study demonstrated that sarcopenia was a common occurrence in patients with HCC treated by RFA, affecting 43.3% of them. Older age was the only factor associated with a higher frequency of sarcopenia. The overall survival of these patients at two years was 65.2% and recurrence-free survival was 84.1%. Sarcopenia was a surrogate predictor of overall survival at two years with a hazard ratio of 7.6 (95% CI: 3.1–18.8). On the other hand, there was no association between sarcopenia and disease recurrence in this series.
In Egypt, HCC is considered the most challenging health problem. According to recent statistical data, HCC is the most common cancer in Egyptian males.1 Many studies described a rising incidence of HCC, which could be attributed to better diagnostic and screening programs, increasing incidence of HCV and cirrhosis, and longer life expectancy of cirrhotic patients.22 Therefore, identifying patients with a high-mortality risk is an essential step to select the most satisfactory treatment for each patient according to his/her prognosis. Great efforts have been made in this respect that developed many prognostic staging systems. However, prognostic factors for HCC remain controversial. Assessment of general performance and nutritional and functional status of HCC patients can improve the predictive yield of existing staging systems.
A recent review found that many factors have been suggested to affect the survival of patients with HCC who underwent RFA. These prognostic factors include liver function as CTP class, high serum levels of AFP, and the presence of portosystemic collaterals.23 In the current study, we investigated the prognostic significance of sarcopenia in patients with early-stage HCC treated with RFA. All patients in the present study developed HCC on top of HCV-associated cirrhosis. This particular group is impressive because chronic liver diseases are considered a risk factor for sarcopenia.24 A recent systematic review of 13 studies including 3111 patients indicated a significant association between sarcopenia and all-cause mortality with a pooled adjusted hazard ratio of 1.95 (95% CI: 1.60–2.37).25 Comparable to the present study, most studies did not find an association between sarcopenia and HCC recurrence.25
Sarcopenia has gained increasing interest as a preoperative prognostic indicator in many cancer types.21,26,27 Previous studies identified sarcopenia as a predictor of poor survival of HCC patients undergoing liver resection.28–31 However, few studies investigated the impact of sarcopenia on the outcome of RFA. One study included patients subjected to RFA (n=29) or surgical resection (n=61). The authors reported impaired overall survival in sarcopenic patients with no difference between resection and RFA. The presence of sarcopenia did not affect recurrence.32 Another study said that low pre-treatment muscle mass was an independent predictor for survival. They evaluated muscle mass using the psoas muscle index (PMI, cm2/m2) on CT images.33 Yeh et al studied the prognostic role of pre-sarcopenia in patients treated with RFA. They defined pre-sarcopenia as psoas muscle area index < 4.24 and 2.50 cm2/m2 for males and females, respectively. The authors concluded that pre-sarcopenia is the prognostic factor of overall survival, but not of recurrence in early-stage HCC patients undergoing RFA.34
In the current study, 43.3% of the patients had sarcopenia. Previous studies have reported a widely variable frequency of sarcopenia in patients with HCC ranging from 12.4% to 66.3%.25 The only factor positively associated with sarcopenia was older age. However, the study sample was relatively younger than that reported in studies investigating the link between sarcopenia and RFA outcome. For example, 78% of patients in Yuri’s study33 were > 60 years, compared to only 9% in the current study. The mean age in Yeh’s study34 was 63.4 ± 10.1 years, while in the present study, it was 53.4±6.0 years. The younger age in the current study supports the concept that sarcopenia is an independent predictor of poor survival, even in younger patients. The young age also indicates the importance of chronic liver disease in the development of sarcopenia. It was reported to affect 30% to 70% of patients with cirrhosis.24
The pathogenesis of sarcopenia in cirrhosis is poorly explained, but suggested mechanisms have been proposed indicating an imbalance between muscle breakdown and formation. It is proposed to be affected by protein catabolism and hormonal and metabolic alteration leading to muscle depletion.24,35 These factors may predispose to poor survival in patients with HCC.36 Another mechanism may involve decreased insulin-like growth factor-1 (IGF-1), strongly associated with low muscle mass and strength.37 It has been reported that low plasma IGF-1 in HCC patients is associated with poor overall survival.38 Sarcopenia was also linked to the tumor necrosis factor-α system, which may enhance tumor migration and invasion in HCC.39
Many methods are available for the evaluation of skeletal muscle mass. These include dual-energy X-ray absorptiometry and bioelectrical impedance analysis. Currently, CT is considered the gold standard for sarcopenia evaluation owing to its accuracy and wide availability.40 Different CT methods are used to measure muscle mass. Like the present study, many investigators quantified sarcopenia by measuring muscle mass at the level of L3 vertebra on 2D planar sections of CT scans. This method has been recognized as the most accurate predictor of whole-body muscle mass41 and is accepted as a marker of sarcopenia and cachexia.42 Previous studies also showed a good correlation between total muscle area and psoas muscle area at the middle of the third lumbar vertebra level.43
In this series, the overall survival at two years was about 65.2%. This figure is a bit lower than some previous studies.44–46 This may be attributed to inclusion of post-HVC induced cirrhotic cases only in the current study. The most common causes of death were liver failure and sepsis (n=9, 27.3% for both), followed by metastases (21.2%)
There are some limitations to our study. First, we did not measure muscle strength or physical function in our patients. However, muscle mass loss is potentially associated with muscle strength decline. Studies are needed to incorporate muscle power or functional status, which would be as important as muscle mass for defining sarcopenia. Secondly, the follow-up period was relatively short and the sample size was quite small. HCV cirrhosis in many Egyptian patients is well known to be associated with a previous history of nosocomial HCV infection from parenteral mass treatment for schistosomiasis, a disease that is commonly associated with muscle wasting. Further studies should put this point into consideration in addition to the effect of treatment.
In conclusion, sarcopenia assessment might be an additional prognostic indicator with conventional biomarkers to optimize the selection criteria for receiving RFA for early-stage HCC. Future studies with a larger sample size and longer follow-up are vital to confirm the prognostic significance of sarcopenia in HCC patients receiving different treatment modalities.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi:10.3322/caac.21492
2. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68:723–750. doi:10.1002/hep.29913
3. Salati U, Barry A, Chou FY, Ma R, Liu DM. State of the ablation nation: a review of ablative therapies for cure in the treatment of hepatocellular carcinoma. Future Oncol. 2017;13:1437–1448. doi:10.2217/fon-2017-0061
4. Shiina S, Tateishi R, Arano T, et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am J Gastroenterol. 2012;107:
5. Kim Y, Lim HK, Rhim H, et al. Ten-year outcomes of percutaneous radiofrequency ablation as first-line therapy of early hepatocellular carcinoma: analysis of prognostic factors. J Hepatol. 2013;58:89–97. doi:10.1016/j.jhep.2012.09.020
6. Yang W, Yan K, Goldberg SN, et al. Ten-year survival of hepatocellular carcinoma patients undergoing radiofrequency ablation as a first-line treatment. World J Gastroenterol. 2016;22:2993–3005. doi:10.3748/wjg.v22.i10.2993
7. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet Elsevier. 2019;393:2636–2646. doi:10.1016/S0140-6736(19)31138-9
8. Otten L, Stobäus N, Franz K, et al. Impact of sarcopenia on 1-year mortality in older patients with cancer. Age Ageing Oxford Acad. 2019;48:413–418. doi:10.1093/ageing/afy212
9. Nakanishi R, Oki E, Sasaki S, et al. Sarcopenia is an independent predictor of complications after colorectal cancer surgery. Surg Today. 2018;48:151–157. doi:10.1007/s00595-017-1564-0
10. Zhang X-M, Dou Q-L, Zeng Y, Yang Y, Cheng ASK, Zhang -W-W. Sarcopenia as a predictor of mortality in women with breast cancer: a meta-analysis and systematic review. BMC Cancer. 2020;20:172. doi:10.1186/s12885-020-6645-6
11. Cruz-Jentoft AJ, Landi F, Schneider SM, et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing. 2014;43:748–759. doi:10.1093/ageing/afu115
12. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc. 2002;50:889–896. doi:10.1046/j.1532-5415.2002.50216.x
13. Argilés JM, Busquets S, Stemmler B, López-Soriano FJ. Cachexia and sarcopenia: mechanisms and potential targets for intervention. Curr Opin Pharmacol. 2015;22:100–106. doi:10.1016/j.coph.2015.04.003
14. Eriksson S, Nilsson JH, Strandberg Holka P, Eberhard J, Keussen I, Sturesson C. The impact of neoadjuvant chemotherapy on skeletal muscle depletion and preoperative sarcopenia in patients with resectable colorectal liver metastases. HPB (Oxford). 2017;19:331–337. doi:10.1016/j.hpb.2016.11.009
15. Farhangfar A, Makarewicz M, Ghosh S, et al. Nutrition impact symptoms in a population cohort of head and neck cancer patients: multivariate regression analysis of symptoms on oral intake, weight loss and survival. Oral Oncol. 2014;50:877–883. doi:10.1016/j.oraloncology.2014.06.009
16. Marasco G, Serenari M, Renzulli M, et al. Clinical impact of sarcopenia assessment in patients with hepatocellular carcinoma undergoing treatments. J Gastroenterol. 2020;55:927–943. doi:10.1007/s00535-020-01711-w
17. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–1022. doi:10.1002/hep.24199
18. Meza-Junco J, Montano-Loza AJ, Baracos VE, et al. Sarcopenia as a prognostic index of nutritional status in concurrent cirrhosis and hepatocellular carcinoma. J Clin Gastroenterol. 2013;47:861–870. doi:10.1097/MCG.0b013e318293a825
19. Mitsiopoulos N, Baumgartner RN, Heymsfield SB, Lyons W, Gallagher D, Ross R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J Appl Physiol. 1998;85:115–122. doi:10.1152/jappl.1998.85.1.115
20. Mourtzakis M, Prado CMM, Lieffers JR, Reiman T, McCargar LJ, Baracos VE. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab. 2008;33:997–1006. doi:10.1139/H08-075
21. Martin L, Birdsell L, Macdonald N, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol. 2013;31:1539–1547. doi:10.1200/JCO.2012.45.2722
22. Abd-Elsalam S, Elwan N, Soliman H, et al. Epidemiology of liver cancer in Nile delta over a decade: a single-center study. South Asian J Cancer. 2018;7:24–26. doi:10.4103/sajc.sajc_82_17
23. Canale M, Ulivi P, Foschi FG, et al. Clinical and circulating biomarkers of survival and recurrence after radiofrequency ablation in patients with hepatocellular carcinoma. Crit Rev Oncol Hematol. 2018;129:44–53. doi:10.1016/j.critrevonc.2018.06.017
24. Dasarathy S. Consilience in sarcopenia of cirrhosis. J Cachexia Sarcopenia Muscle. 2012;3:225–237. doi:10.1007/s13539-012-0069-3
25. Chang K-V, Chen J-D, Wu W-T, Huang K-C, Hsu C-T, Han D-S. Association between loss of skeletal muscle mass and mortality and tumor recurrence in hepatocellular carcinoma: a systematic review and meta-analysis. Liver Cancer. 2018;7:90–103. doi:10.1159/000484950
26. Prado CMM, Lieffers JR, McCargar LJ, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 2008;9:629–635. doi:10.1016/S1470-2045(08)70153-0
27. Thoresen L, Frykholm G, Lydersen S, et al. Nutritional status, cachexia and survival in patients with advanced colorectal carcinoma. Different assessment criteria for nutritional status provide unequal results. Clin Nutr. 2013;32:65–72. doi:10.1016/j.clnu.2012.05.009
28. Voron T, Tselikas L, Pietrasz D, et al. Sarcopenia impacts on short- and long-term results of hepatectomy for hepatocellular carcinoma. Ann Surg. 2015;261:1173–1183. doi:10.1097/SLA.0000000000000743
29. Harimoto N, Shirabe K, Yamashita Y-I, et al. Sarcopenia as a predictor of prognosis in patients following hepatectomy for hepatocellular carcinoma. Br J Surg. 2013;100:1523–1530. doi:10.1002/bjs.9258
30. Iritani S, Imai K, Takai K, et al. Skeletal muscle depletion is an independent prognostic factor for hepatocellular carcinoma. J Gastroenterol. 2015;50:323–332. doi:10.1007/s00535-014-0964-9
31. Itoh S, Shirabe K, Matsumoto Y, et al. Effect of body composition on outcomes after hepatic resection for hepatocellular carcinoma. Ann Surg Oncol. 2014;21:3063–3068. doi:10.1245/s10434-014-3686-6
32. Levolger S, Vledder MG, Van, Muslem R, et al. Sarcopenia impairs survival in patients with potentially curable hepatocellular carcinoma. J Surg Oncol. 2015;112:208–213. doi:10.1002/jso.23976
33. Yuri Y, Nishikawa H, Enomoto H, et al. Implication of psoas muscle index on survival for hepatocellular carcinoma undergoing radiofrequency ablation therapy. J Cancer. 2017;8:1507–1516. doi:10.7150/jca.19175
34. Yeh W-S, Chiang P-L, Kee K-M, et al. Pre-sarcopenia is the prognostic factor of overall survival in early-stage hepatoma patients undergoing radiofrequency ablation. Medicine. 2020;99:e20455. doi:10.1097/MD.0000000000020455.
35. Sinclair M, Gow PJ, Grossmann M, Angus PW. Review article: sarcopenia in cirrhosis–aetiology, implications and potential therapeutic interventions. Aliment Pharmacol Ther. 2016;43:765–777. doi:10.1111/apt.13549
36. Vitale G, Cesari M, Mari D. Aging of the endocrine system and its potential impact on sarcopenia. Eur J Intern Med. 2016;35:10–15. doi:10.1016/j.ejim.2016.07.017
37. Gielen E, O’Neill TW, Pye SR, et al. Endocrine determinants of incident sarcopenia in middle-aged and elderly European men. J Cachexia Sarcopenia Muscle. 2015;6:242–252. doi:10.1002/jcsm.12030
38. Elmashad N, Ibrahim WS, Mayah WW, et al. Predictive value of serum insulin-like growth factor-1 in hepatocellular carcinoma. Asian Pac J Cancer Prev. 2015;16:613–619. doi:10.7314/APJCP.2015.16.2.613
39. Sachdeva M, Chawla YK, Arora SK. Immunology of hepatocellular carcinoma. World J Hepatol. 2015;7:2080–2090. doi:10.4254/wjh.v7.i17.2080
40. Landi F, Calvani R, Cesari M, et al. Sarcopenia: an overview on current definitions, diagnosis and treatment. Curr Protein Pept Sci. 2018;19:633–638. doi:10.2174/1389203718666170607113459
41. Shen W, Punyanitya M, Wang Z, et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol (1985). 2004;97:2333–2338. doi:10.1152/japplphysiol.00744.2004
42. Golse N, Bucur PO, Ciacio O, et al. A new definition of sarcopenia in patients with cirrhosis undergoing liver transplantation. Liver Transpl. 2017;23:143–154. doi:10.1002/lt.24671
43. Hiraoka A, Aibiki T, Okudaira T, et al. Muscle atrophy as pre-sarcopenia in Japanese patients with chronic liver disease: computed tomography is useful for evaluation. J Gastroenterol. 2015;50:1206–1213. doi:10.1007/s00535-015-1068-x
44. Cabibbo G, Maida M, Genco C, et al. Survival of patients with hepatocellular carcinoma (HCC) treated by percutaneous radio-frequency ablation (RFA) is affected by complete radiological response. PLoS One. 2013;8:e70016. doi:10.1371/journal.pone.0070016
45. Kikuchi L, Menezes M, Chagas AL, et al. Percutaneous radiofrequency ablation for early hepatocellular carcinoma: risk factors for survival. World J Gastroenterol. 2014;20:1585–1593. doi:10.3748/wjg.v20.i6.1585
46. Waki K, Aikata H, Katamura Y, et al. Percutaneous radiofrequency ablation as first-line treatment for small hepatocellular carcinoma: results and prognostic factors on long-term follow up. J Gastroenterol Hepatol. 2010;25:597–604. doi:10.1111/j.1440-1746.2009.06125.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.