")
Back to Journals » Patient Preference and Adherence » Volume 16
Impact of Routines and Rituals on Burden of Treatment, Patient Training, Cognitive Load, and Anxiety in Self-Injected Biologic Therapy
Authors Coyne M, Rinaldi A , Brigham K, Hawthorne J , Katsaros D, Perich M, Carrara N, Pericaud F, Franzese C, Jones G
Received 26 May 2022
Accepted for publication 15 September 2022
Published 19 September 2022 Volume 2022:16 Pages 2593—2607
DOI https://doi.org/10.2147/PPA.S375037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Marty Coyne,1,2 Amy Rinaldi,1 Katherine Brigham,1 James Hawthorne,1,2 Dimos Katsaros,1,2 Morgan Perich,2 Nicholas Carrara,1 Flore Pericaud,3 Chris Franzese,1,2 Graham Jones4
1Matchstick, Boonton, NJ, USA; 2University of Rhode Island School of Pharmacy, Kingston, RI, USA; 3Technical Research and Development, Novartis Pharmaceuticals, Basel, Switzerland; 4Technical Research and Development, Novartis Pharmaceuticals, East Hanover, NJ, USA
Correspondence: Graham Jones, Technical Research and Development, Novartis Pharmaceuticals, East Hanover, NJ, USA, Email [email protected]
Background: Self-injection of biologics is a mainstay of chronic disease treatment, yet the process of self-injection often causes persistent apprehension and anxiety, distinct from needle phobia. While literature alludes to the role that routines and rituals play in self-injection, there is no comprehensive study on the routines and rituals self-injectors employ, nor of the process by which they are discovered and ingrained.
Methods: We conducted a mixed-method, observational pilot ethnography study of 27 patients with plaque psoriasis, psoriatic arthritis, or ankylosing spondylitis with and without prior biologic self-injection experience. Patients submitted self-made videos, photos, and projective exercises of an actual biologic self-injection and completed validated instruments to assess burden of treatment. Videos and photos containing routine and ritual elements were thematically categorized based on functional and emotional benefit, and analyzed for differences based on current biologic, dosing frequency, time on current biologic, and burden of treatment measures.
Results: During patients’ initial at-home injections, training gaps became apparent, leading to a process of experimentation aimed at reducing pain/anxiety, increasing confidence, and building a consistent injection process. Routines were present in 27/27 (100%) patients and anchored the time, place, and process for injection, and incorporated approved use steps for the injection device. Ritual elements served as emotional coping strategies for patients and were present in 21/27 (77.8%) of patients.
Conclusion: Our findings suggest that providing patients device training using adult learning principles, teaching routines and rituals concurrently, and providing at-home opportunities for practice with a device trainer may be useful strategies to reduce anxiety, avoid unnecessary experimentation, and improve adherence to injection therapy. While further studies are needed to generalize our findings, we posit that routine and ritual elements can be incorporated into existing patient-clinician interactions or novel digital interventions through mobile medical applications, smart training devices, and connected injection ecosystems.
Keywords: training, drug delivery device, combination product, patient support, routines, rituals, burden of treatment, chronic disease, injection trainer, mixed methods research
Introduction and Background
Treatment Burden for Self-Injection
Biologics, specifically monoclonal antibodies (mAbs) or fusion proteins, are often used for the management of more severe forms of several chronic diseases, including inflammatory bowel disease (IBD), rheumatoid arthritis (RA), plaque psoriasis (PsO), psoriatic arthritis (PsA), multiple sclerosis, chronic or episodic migraine, and asthma.1–7
The overall burden of treatment (BoT) associated with chronic disease management is commonly conceptualized as the “workload” of being a patient, and may require extensive time, attention, cognitive energy, and effort.8,9 To counterbalance this workload, patients must have adequate capacity, which comprises their abilities and resources, such as their mental/physical functioning, socioeconomic and psychological resources, literacy, language, and social support.10 Many patients may lack the capacity to neutralize the workload, and thus struggle to manage health-care demands.
Currently, approved biologics are administered parenterally. To reduce the BoT associated with administration of biologics, many therapies are supplied as subcutaneous injections, thereby allowing administration at home by patients or caregivers rather than intravenously in a clinical setting.11–13 Despite the advantages, convenience, and focus on usability testing, at-home administration undeniably places a significant burden of responsibility onto patients.
Contributing Factors to Emotional Gaps in Self-Injection
Although many (if not all) self-administered biologics have an FDA label requirement for patient training on use steps, not all patients routinely receive training.14,15 Training may omit emotional support for patients, as providers may not prioritize these aspects.14 Consequentially, otherwise physically capable patients may never start or prematurely discontinue self-injection therapies.16–19 Numerous authors speak to the emotional aspects of self-injection and resulting apprehensions, including concerns about incorrect technique, fear of side effects, lack of self-confidence, stigma of illness and social embarrassment, frustration with illness and treatment, and anxiety from needles.19–23
Notably, this apprehension is distinct from clinically significant needle fear, which is present in 7–11% of the general population.24–26 Needle phobia is a well-studied barrier to self-administration and is diagnosed through the Diagnostic and Statistical Manual (DSM) of Mental Disorders–IV criteria.26–29 However, there is no such DSM diagnosis for generalized apprehension or anxiety related to self-injection in the absence of clinically significant needle phobia.
Role of Routines and Rituals in Self-Injection
As a response to treatment burden and emotional distress, patients may utilize techniques to decrease the impact of treatment on their overall well-being. The development of two such techniques, routines and rituals, has been specifically observed in the case of self-injection.14,23
While previous authors have discussed routines and rituals, the two techniques are not consistently defined and sometimes not even differentiated.14,30–32 Prior to establishing the role of routine and rituals, clear definitions of both these techniques are needed. Based on previous literature and subject expertise, we define a routine as a sequentially repetitive manner of completing a specified task, that is anchored on a time, place, and/or process. Unlike routines, we define ritual activities as being extremely personalized, grounded in emotion, and entirely independent of the core steps for the device. Rituals primarily address thoughts, emotions, and mindset related to self-injection.
Routines can effectively help patients perform health-care tasks with little conscious thought, and thus remove much of the cognitive load during task completion.30 One such example is using the act of brushing teeth in the morning as a prompt to take a morning dose of a medication.33 On the other hand, rituals are comprised of tangible, enduring meaning; they may not be readily interpreted by outsiders or those unfamiliar with the ritual.34 For example, a patient may dim the lights prior to injection therapy or use the same chair at the same time for every injection.14
While the mechanism is not entirely clear, existing research outside self-administration suggests rituals can significantly improve cognitive performance possibly via the regulation of anxiety, and that the adoption of novel rituals by ritual-naïve individuals can elicit an immediate positive cognitive response.32,34 Routines and rituals feature prominently in professional athletics, and literature around swimming performance suggests correlations exist between anxiety and deteriorated performance.35–38
Previous authors also describe that patient-developed injection routines and rituals may play important roles in reducing the treatment burden for those taking biologics, and suggest that knowledge and emotional gaps encourage their development.14,23 In an ethnography study of patients’ self-injecting experience, researchers discovered that: 1) some patients engage in routinized, ritual-like behavior to reduce injection anxiety; 2) ritual development was largely beneficial and patients who participated in rituals reported more confidence during self-injection; 3) patients preferred to perform injections under consistent circumstances (ie, in the same place, at the same time, using the same methodology); and 4) some patients inadvertently habitualized incorrect behavior, due to gaps in instruction.14
While prior studies introduce the concepts of routines and rituals, directed research of these behaviors as they relate to self-injection is currently limited. Such research could serve to identify patients who may benefit from routine and ritual elements, teach these elements systematically as part of initiation, and improve patient experience with self-injection. To test these hypotheses, we conducted a pilot study to specifically explore routines, rituals, and how they may vary across common attributes of self-injected biologics.
Materials and Methods
Participant Eligibility
Eligible participants were ≥18 years of age, had a formal diagnosis of PsO, PsA, or ankylosing spondylitis (AS), and were currently using a pre-filled syringe or autoinjector for self-administration of adalimumab, abatacept, certolizumab pegol, etanercept, golimumab, guselkumab, or secukinumab. Patients previously naïve to biologics and those with prior biologic experience were eligible to participate. Patients whose current injection was their first ever injection were considered biologic naïve (BxN), and patients who had been on previous injections prior to their current injection were considered biologic experienced (BxE). Patients were not eligible to participate if they did not have reliable internet connection, computer, and smartphone, they or an immediate family member worked for a pharmaceutical company or a market research firm, or they were going to start to take their injection beyond four weeks from the start of the study. Patients currently on ustekinumab were excluded due to the drugs’ wide dosing frequency, and thus a logistical inability for patients to fit recruitment timelines.
Research Methods
This was a non-interventional ethnographic study designed to observe current patient practices, experiences, and behavior related to self-injection. Patients completed an informed consent document outlining the observational nature of the study, the requirements for participation, and the steps taken to protect their privacy. Data were collected through closed-form surveys and passive observation using a remote ethnography approach with patient-made videos, photos, and projective exercises. All responses were recorded in such a manner that the identities of the participants could not be readily ascertained. Patients completed Self-injection Assessment Questionnaire (SIAQ),39 Treatment Burden Questionnaire (TBQ),9 and Patient Acceptable Symptom State (PASS)40,41 assessments online prior to beginning study activities. Patients were asked to complete all study activities in their usual home environment, on their normal injection day, and where they normally self-inject to improve fidelity of data collected and avoid potential influence on the topics being explored. Participants were not specifically instructed to capture rituals or routines at the study outset in order to allow these behaviors to manifest and be observed naturally. Each participant completed approximately 4–5 hours of activity over four days (see Table 1). All study procedures were conducted in accordance with the 1964 Declaration of Helsinki and its subsequent revisions.
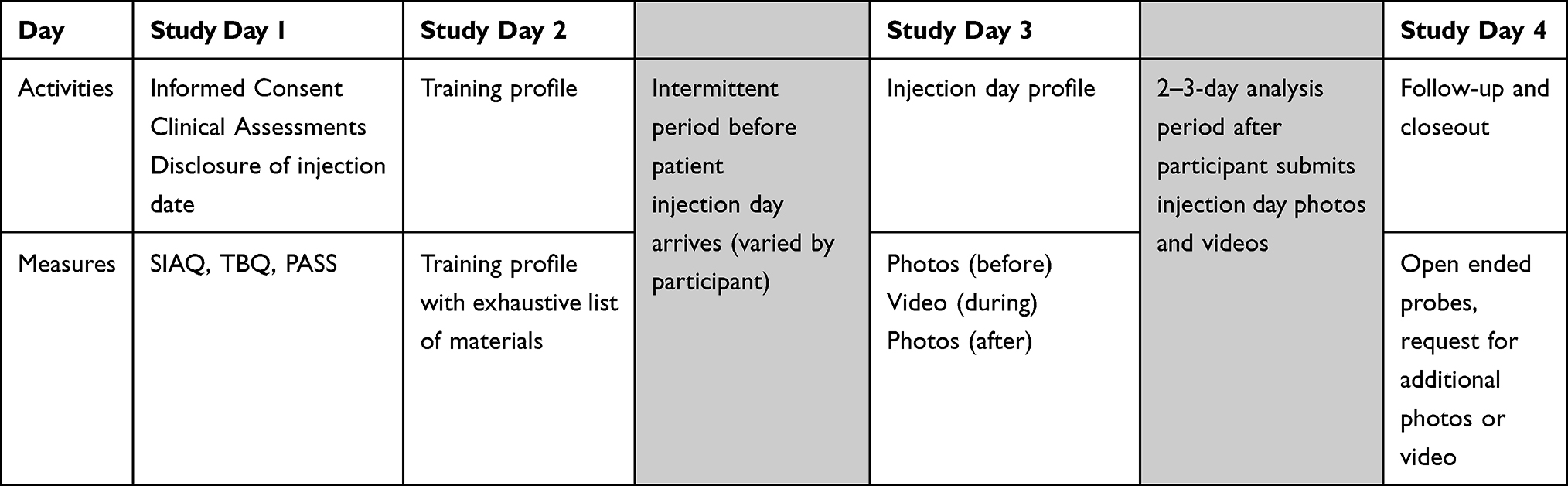 |
Table 1 Study Overview |
Study Day 1: Patients completed informed consent and then were quantitatively assessed for burden of treatment using SIAQ and TBQ/PASS, all of which have been used as outcome measures in prior published injection-related studies. These measures were used by the moderators to provide additional context for individual participants during follow-on study activities, and for post hoc analysis.
Study Day 2: Patients completed a training workmat where they profiled different training activities based on stage of therapy. Training activities for the workmat were developed by the authors’ secondary research and analysis of the components of US-based patient support programs that are publicly available from each pharmaceutical manufacturer of the biologics within the study eligibility criteria. These were supplemented with a complete list of potential in-clinic training methods and tools.
Patients were presented with a series of training elements which were classified into tell, which included verbal instruction from an HCP or patient support program coach, show, including HCP demonstration using a training device or HCP-performed injection of actual biologic, and try/do, where patients either practiced with a trainer device or conducted their first injection under HCP supervision (Table 2).
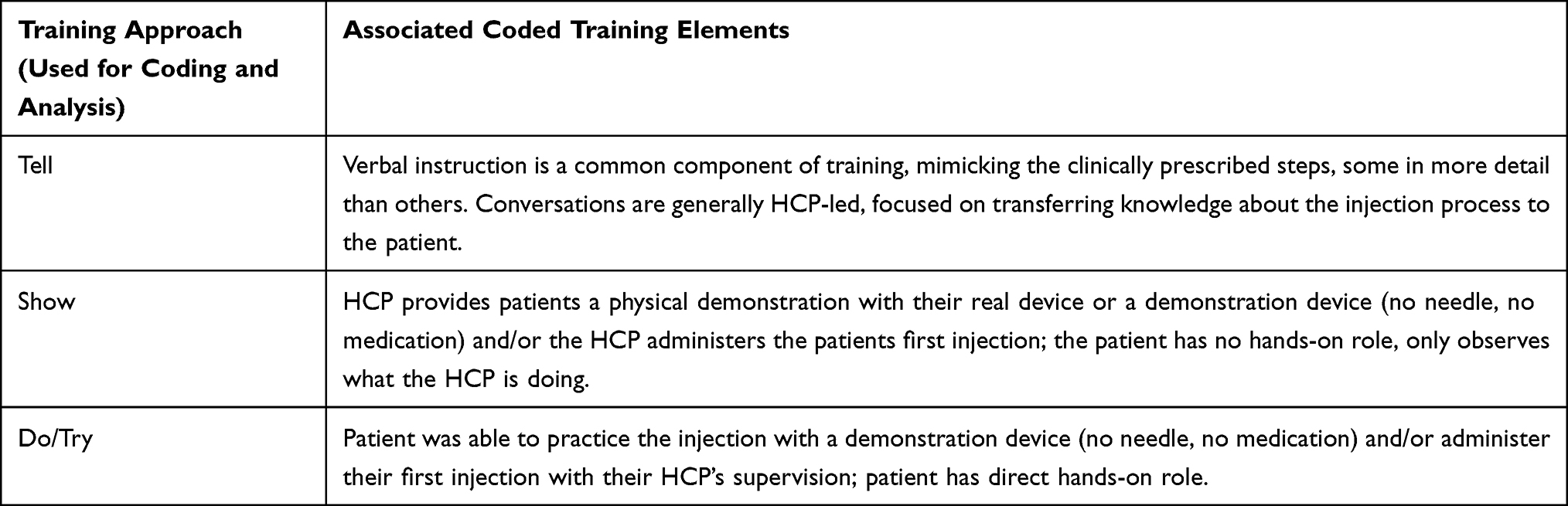 |
Table 2 Training Elements |
Study Day 3: On each patient’s actual injection day, participants were asked to document activities before their injection using photos, during the injection with a passive recording, and after the injection with photos.
Study Day 4: Patients participated in a follow-up session for moderators to clarify observed points in workmats, photos, and videos, using an adaptive approach tailored to each participant. If a sequence of specific observed elements for a given participant was unclear, moderators asked participants to clarify the sequence they performed elements before, during, or after injection as applicable.
Data Collection
Videos, photos, and open-ended submissions were collected, transcribed, and coded by the moderator (AR) and a research assistant (KB). Initial coding was executed as participants completed each activity to develop an opening codebook, followed by an iterative process of reviewing and refining coding sequences to develop mutually exclusive themes by two additional researchers (CF, MC). Observed elements were recorded and coded based on whether the observed step was an instructional step (as determined by the current version of the package insert approved in the US for each biologic), core routine step, personalized routine step, or ritual. Core routines go beyond the minimum viable instructions, weaving in distinct steps that increase organization, predictability, and pain management. Personalized routines also introduce personalized details not captured in the IFU but still accomplish the same task (eg, holding the injector in a hand or back pocket to speed up warm up, ensuring privacy during injection, and use of makeshift sharps disposals). Rituals go beyond routines, adding personalized non-obvious activities that result in emotional benefit. The coding of the study followed an adaptive approach where the study moderator could follow up with tailored questions for patients based off earlier submissions.
Through the review and coding process, each participant’s injection day was reduced to a sequential series of steps, each coded as instructional step, routine, or ritual. Day 4 activities were used to understand context and meaning behind routine and ritual elements observed in Day 3 activities. As qualitative routine and ritual data accumulated for each participant, researchers continuously monitored for code saturation (the point at which no additional routines or rituals were identified) and meaning saturation (the point at which issues were fully understood and no further dimensions or nuances of issues could be discerned). Researchers evaluated for saturation by taking into consideration the five dimensions suggested by Malterud et al: study aim, sample specificity, use of established theory, quality of dialogue, and analysis strategy.42 Given our narrow study scope, specific participant sample, and robust study design, once themes were repeatedly observed without the birth of new ideas, data saturation was determined and collection was halted.43
Throughout the study, an iterative process of reviewing and refining coding sequences was conducted to develop mutually exclusive themes, similar to what has been described by Baggot et al.44 Thus, data collection and analysis occurred concurrently. Qualitative data were analyzed to identify thematic groups within the entire participant group as well as the biologic-experienced (BxE) and biologic-naïve (BxN) subgroups. Routines and rituals were clustered separately based on functional (routine) and emotional (ritual) benefit.
Data Analysis
Statistical analyses were exploratory and of a descriptive nature. Quantitative analysis was used to identify differences in adoption of routines and rituals based on current biologic, dosing frequency, time on current biologic, and burden of treatment measures. Analysis was performed on the full dataset using R.45 Quantitative assessment variables were compared between sub-groups using Kruskal–Wallis tests, with Wilcoxon tests being used in the case of a binary variable due to the non-normal nature of the sub-groups. When appropriate, post-hoc multiple comparisons were calculated using a Dunn Test. All analyses used a two-sided Type I error of α = 0.05. Quantitative variables were also compared against one another using Pearson correlations. When comparing two qualitative variables, Pearson’s chi squared test was used, and standard residuals were calculated post-hoc.
Results
Twenty-nine participants were successfully recruited into the study. Devices utilized by the participants on video were positively confirmed against reported self-injection medication and device provided by the participant during recruiting. Two participants were excluded from analysis for falsely reporting self-injection device. Of those, one participant was not observed to use the device expected from recruiting, and the other participant actively concealed his or her device during injection day. One patient was excluded from data analysis specifically in the injection training activity shown in Figure 1 due to being enrolled in a clinical trial at the time of initiation, but not at the time of the study. Participant demographics are presented in Tables 3 and 4.
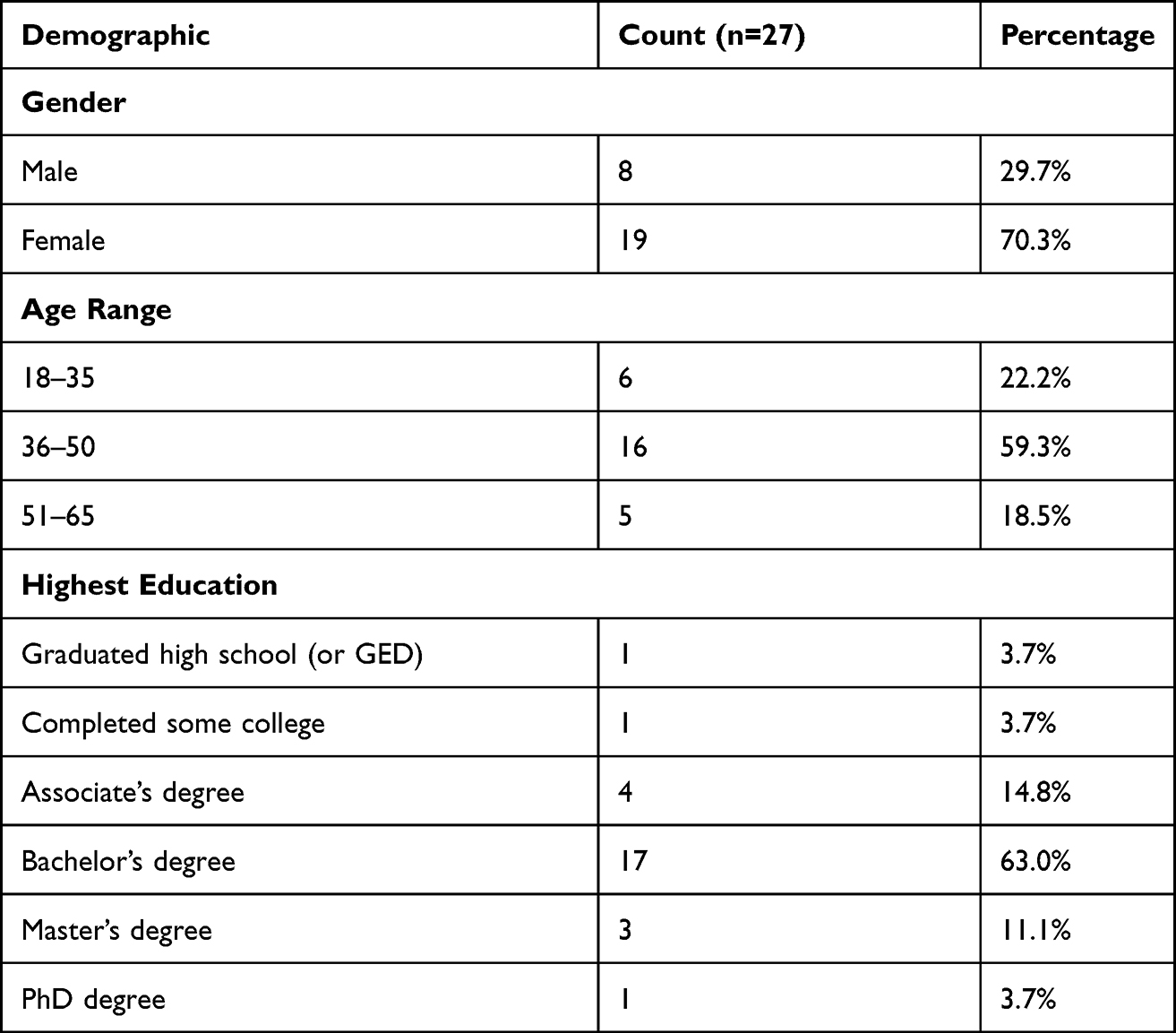 |
Table 3 Participant Demographics |
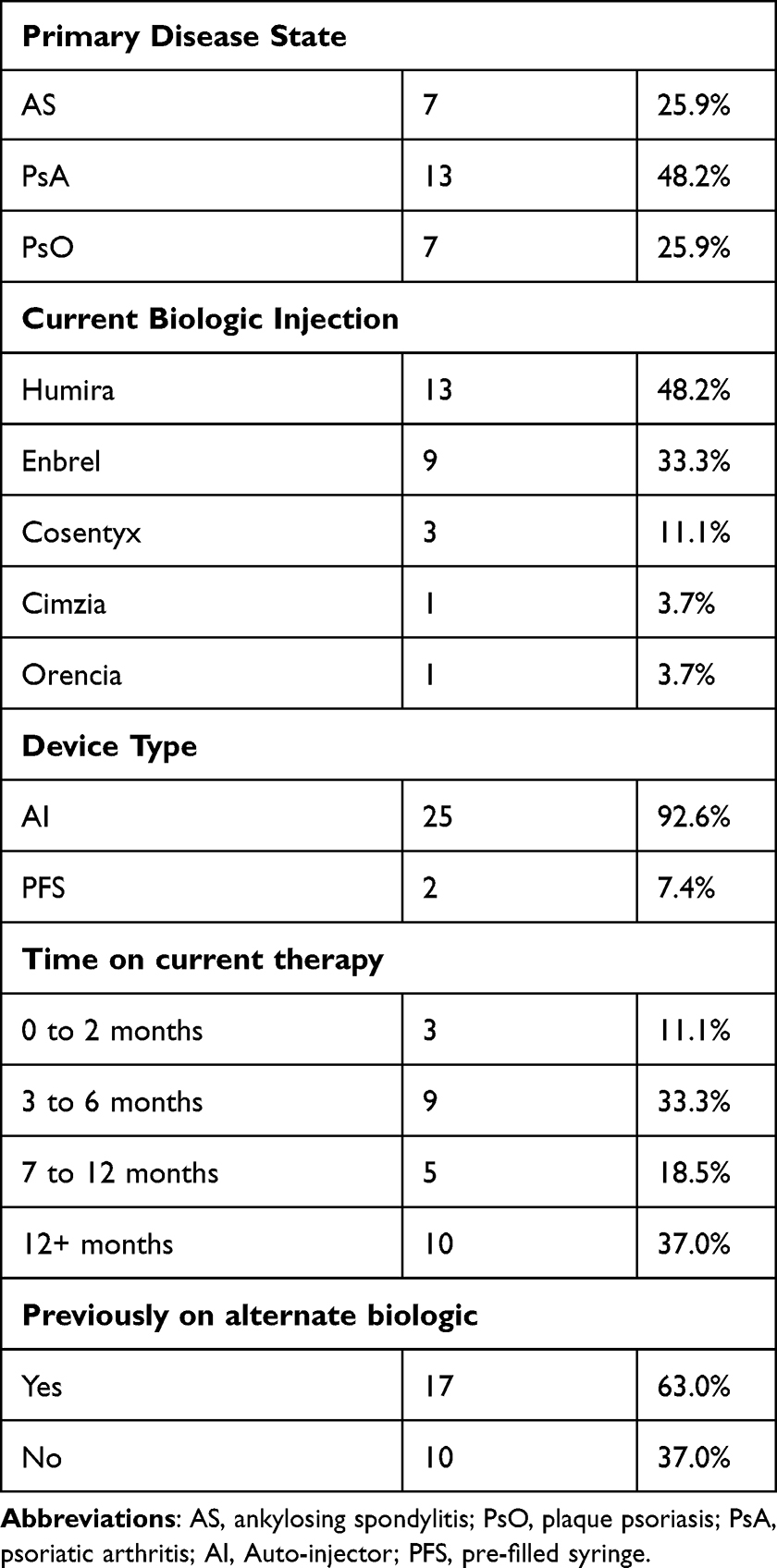 |
Table 4 Relevant Patient Medical Information |
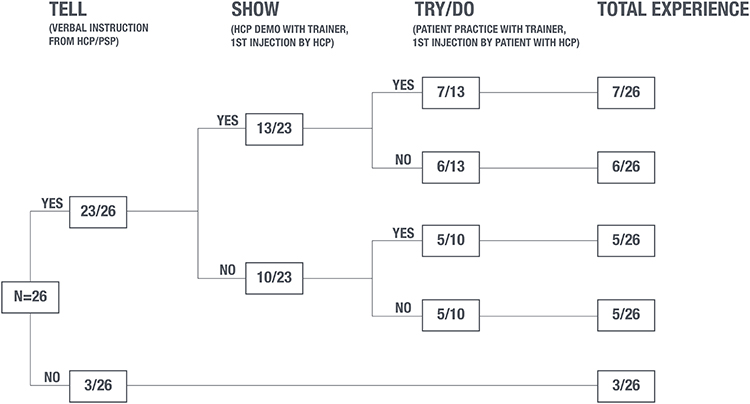 |
Figure 1 Training methods experienced by study participants. |
Injection Training
We found that patients had wide variability in training experiences. Analysis of training methods reported by study participants is summarized in Figure 1. One patient was excluded from data analysis specifically in the activity shown in Figure 1 because they were enrolled in a clinical trial at the time of initiation, but not at the time of the study.
Most participants (23/26, 88.5%) received injection training in some capacity. However, the depth of training varied between those participants who did receive training. Only 7 (27%) participants received all three of: verbal instruction, a visual demonstration, and a first injection observed by an HCP. Some participants (3/26, 11.5%) received no training at all; these participants were all previously biologic-naïve. The remaining participants were taught using various permutations of these methods, including verbal instruction only without demonstration (5/26), verbal instruction followed by demonstration (6/26), and observed first injection (6/26) (Figure 1). Participant quotes describing their training experience are shown in Table 5.
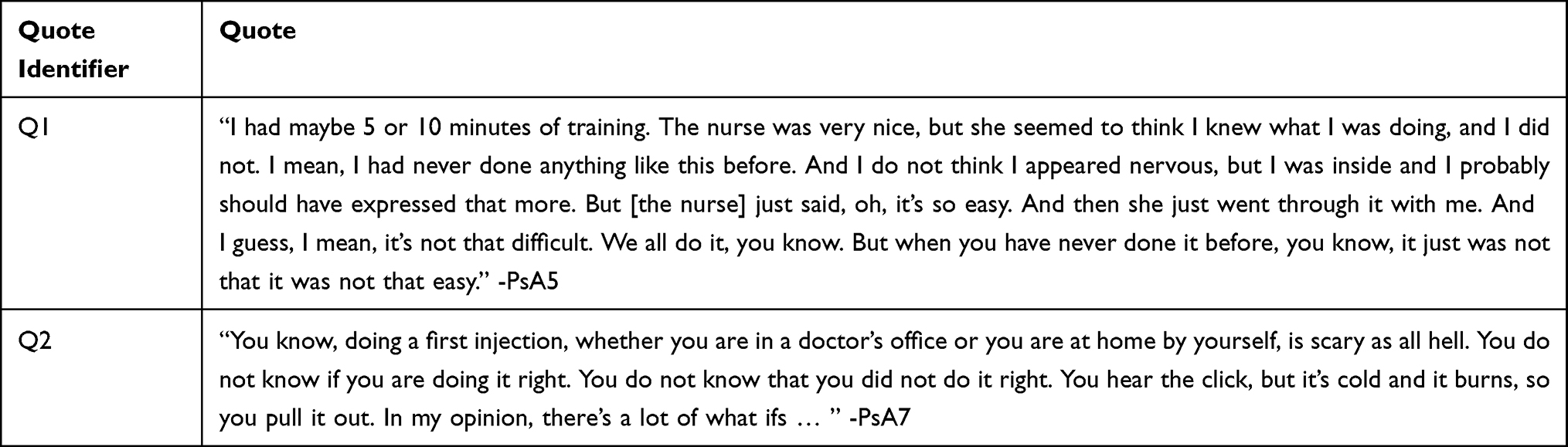 |
Table 5 Participant Statements Regarding Their Training Experiences |
Patients who experienced mixed-method training, with verbal instruction, demonstration, and first injection observed by the HCP had lower SIAQ anxiety compared to patients who did not receive all three methods, although this difference did not reach statistical significance (p = 0.07). Pairwise comparisons between individual training methods did not yield statistically significant differences in SIAQ anxiety.
Routines & Rituals
Based on the themes identified, a generalized flow was developed to explain the emergence of routine and ritual behaviors observed (Figure 2). Through accumulated experiences, patients self-identified behaviors that did or did not work in efforts to create their own routines and rituals. Observed routine and ritual elements are shown in Table 6. Regardless of how training takes place, when both biologic-naïve and experienced patients began injecting at home, knowledge gaps became apparent, and the emotional pressure was higher compared to the HCP office (Table 5, Q1 & Q2).
 |
Table 6 Routine & Ritual Elements |
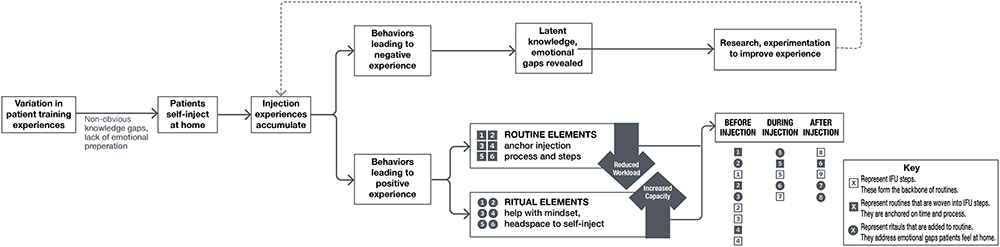 |
Figure 2 Patient discovery process for routines and rituals, workload is the intersection between managing a chronic illness along with all the other tasks of daily living. Workload encompasses the demands on patient time, energy, and attention. Capacity is an individual’s emotional, cognitive, and physical ability to handle their workload. |
Patients described a process of research on how to use their device, where they sought to close knowledge and information gaps. Patients reported that they most often consulted information from YouTube (15/27, 55.6%), manufacturer websites (12/27, 44.4%), or general internet searches (12/27, 44.4%).
Routine elements were present across all participants. Irrespective of injection device used (autoinjector or syringe) and biologic used, core routine steps were interwoven with the biologic and device instructional steps, serving to reduce cognitive load, increase organization, reduce probability of forgetting steps or mis-ordering them, and managing pain. Routines were featured prominently throughout the injection process, with participants demonstrating these elements before (15/27; 55.6%), during (15/27; 55.6%), and after (10/27; 37.0%) injection.
Many participants (19/27; 70.4%) personalized core routine steps. Similar to generalized routine elements, personalized routine elements served to not only correctly perform the physical injection, but also introduce personalized details not captured in the IFU, such as holding the injector in a back pocket to speed up the warming period. Examples of observed routines are presented in Table 6.
Ritual elements were found to be extremely personalized between patients. Before the injection, patients aim to establish their ideal mindset, grounding themselves mentally, causing a distraction, alleviating anxiety, and taking proactive steps for their own health. During the injection, patients build up courage for the moment of injection and comfort themselves with surrounding sounds and physical objects. After the injection, patients allot time for relaxation, reward themselves, abstain from physical activity, and reflect on the experience. Examples of observed rituals are in Table 6.
Many participants (18/27; 66.7%) self-described their injection day as having elements of both routine and ritual; 9 study participants reported their injections were solely routine. Upon video review, 3 of those 9 were found to have latent ritual elements despite patients’ self-characterization to the contrary. These participants expressed that the ritual elements felt natural, non-obvious, and “second nature”; however, their responses clearly indicated an emotional benefit provided. Overall, 21 participants (77.8%) had routines and rituals, while 6 participants (22.2%) had routines only. Participant quotes describing the self-perceptions, roles, and impact of devices on routines and rituals are shown in Table 7.
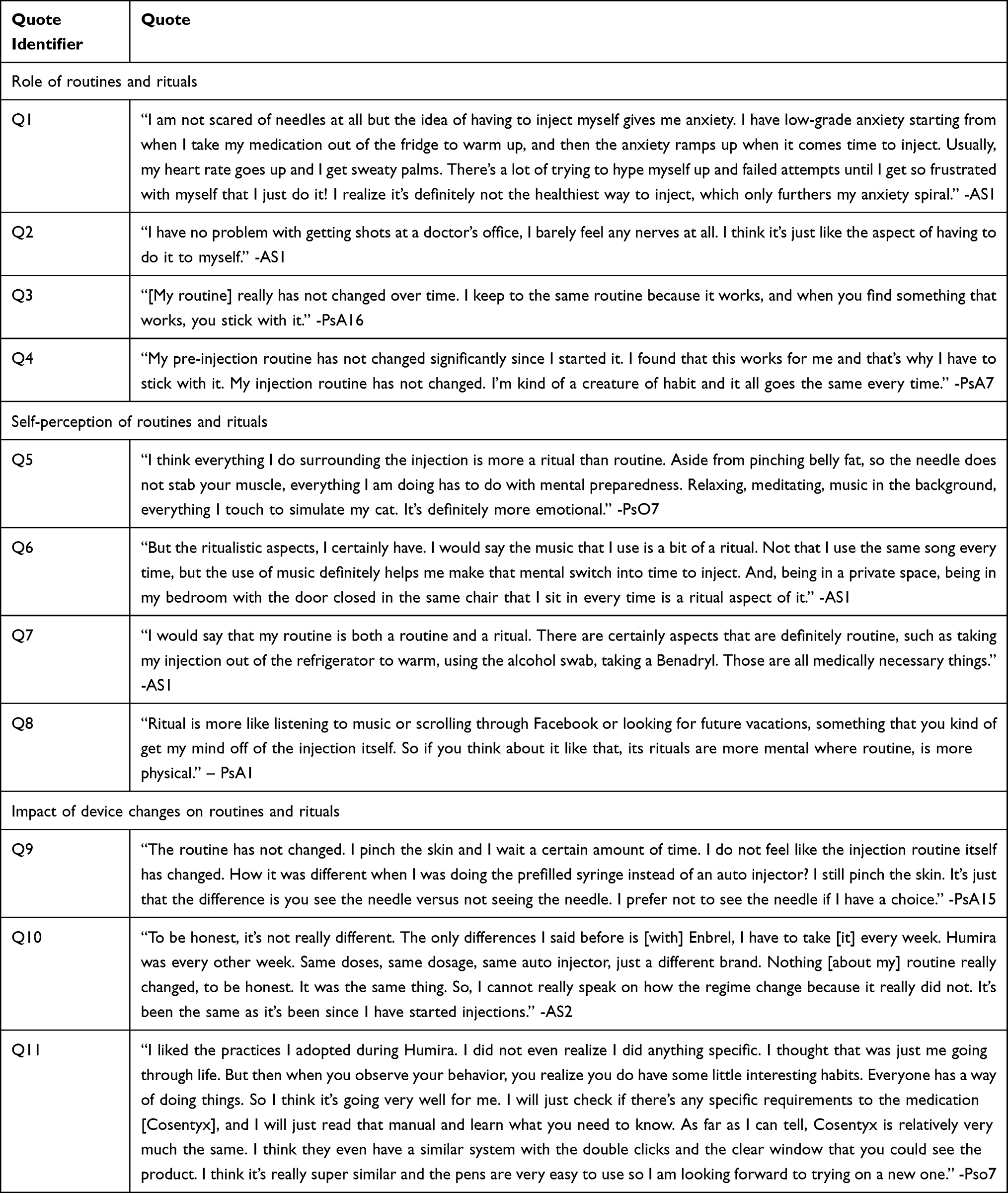 |
Table 7 Participant Statements Regarding Their Routine and Ritual Elements |
Among patients with ritual elements, quantity varied widely from 1 to 7 (mean: 2.95 median: 3; mode: 1). Longer injection rituals were somewhat associated with higher burden of treatment scores, as measured by TBQ (r2=0.32), higher self-injection anxiety as measured by SIAQ (r2 = 0.45), and lower self-confidence as measured by SIAQ (r2 = 0.57). Reflecting after the injection was the most prevalent ritual in patients with high injection anxiety. Anxiety, as measured by SIAQ, decreased with increasing time on current biologic, as did the number of ritual elements.
Those who saw their injection process as containing both routine and ritual elements most often noted steps involving the injector itself, organization, consistency as the core routine; activities addressing mindset and emotions were noted as ritualistic in nature (eg, Table 7; Q5). Those who considered their injection process a routine devoid of any ritualistic elements attributed it to lack of emotional needs, displaying no purposeful planning and the task-oriented mindset injection process elements are simply steps to follow.
No participants received instruction on routines or rituals from their HCP or others. Instead, they were found completely by a process of discovery and experimentation. Ritual elements were influenced by strategies that are already management strategies outside of self-injection (such as prayer, meditation, or journaling), or inspired by experienced patients’ stories on social outlets, often projecting tips and tricks addressing self-injection challenges. Once established, these routines and rituals rarely changed, and became integrated into a patient’s injection process (eg, Table 7; Q3).
Discussion
We found that all patients had routines, which anchored time, place, and injection process, and were woven into the approved use steps for the actual injection device. Given the relatively uniform use steps among injection devices, we found constancy in routine elements. Ritual elements were present in a subset of participants, particularly those with higher BoT measures, and served as emotional coping strategies.
Routine and ritual elements evolved through experimentation and subsequent habitualization. Experimentation was aimed at reducing pain/anxiety, increasing confidence, and building a consistent injection process. Patients retained elements that led to a positive perceived experience and discarded those that did not. Patients viewed their routines and rituals as highly personalized, reflecting their experimentation and discovery process. Neither routines nor rituals were taught and were always self-discovered by patients.
Both routine and ritual elements can play roles in alleviating burden associated with performing self-injection. Routines focus more on the process and can effectively reduce cognitive burden associated with health-care tasks, thus decrease overall workload associated with their care. Rituals strengthen a patient’s mental state, and thus increases a patient’s intrinsic capacity to manage the workload required. Rituals and routines can simultaneously decrease workload and capacity, and thus effectively decrease overall treatment burden.
Self-Injection Training & Training Variations
We found patients do not uniformly receive self-injection training despite FDA labeling requirements that training take place. Approximately one-third of patients in our study were either untrained or received only verbal instruction; the three patients who received no training whatsoever were all biologic-naïve and therefore injecting biologics for the first time. Of note, the study took place prior to the ongoing COVID-19 pandemic. Training gaps may be even more eminent in current practice, as many office visits have shifted to remote settings.
When training was not adequate, many patients sought accessible information sources to provide them with more guidance. YouTube was the most common source of information, with over half our participants reporting searching YouTube videos for guidance. While some videos may be helpful, YouTube videos are not typically regulated for accuracy, thus this practice may result in inaccurate information being relayed and could potentially increase the risk for developing improper technique.46 Both HCPs and the pharmaceutical industry should place a greater emphasis on guiding patients towards authentic and accurate resources to supplement training.
Regardless of training content and method, training gaps were commonplace in our study and became apparent only once patients inject themselves at home, as foreshadowed by Schiff and colleagues.14 Patients in our study distinguished between the HCP office setting (if trained there) and the home. Whereas they found the office to be controlled and calm, they described being surprised by the feelings of apprehension once home alone to self-inject for the first few times. This supports the notion that even simple devices, carefully engineered and tested extensively for usability, may frequently prove difficult given the backdrop of emotion and apprehension that leads to uncertainty, lack of recall about what was taught, missed or misperformed steps, and negative initial experiences. Similar findings on the relationship between anxiety and performance have been reported across domains outside healthcare.37,38
Role of Routines and Rituals
Rituals are most often developed in response to situations which illicit strong negative emotions such as anxiety, stress, trauma, or uncertainty.34 While there are many theorized psychosocial processes through which rituals can decrease negative emotions, overall, they allow a sense of regained control over the situation or circumstance.31,34 Rituals can create stronger patient mindsets, increasing patient capacity to cope with treatment burden.
The use of rituals to decrease anxiety and increase performance is not a novel concept, as humans have utilized these techniques extensively. Outside of injections, the utilization of rituals has been shown to decrease anxiety and improve performance during high anxiety tasks such as public singing and math tests.32 Rituals within self-injection appear to be used by patients to counter injection anxiety (eg, Table 7; Q8), as our study found that patients with higher anxiety utilized longer rituals.
On the other hand, routines act to reduce cognitive burden as they require little to no conscious thought to perform.30,47 Some routine elements utilize cues, such as putting on a seatbelt after entering a car or washing hands after using the bathroom. By transferring the cognitive load required to consciously remember when and how to do tasks to these external cues, dependence on conscious attention and memory requirements are reduced.48 Thus, routines can help alleviate treatment burden by decreasing overall patient workload.
While self-injecting may present a very different use case compared to the above examples, routines and rituals are still used to combat similar negative emotions and cognitive burden. Negative emotions such as injection anxiety, injection phobias, and lack of confidence have been identified to be both prevalent and a barrier to long-term adherence in populations who self-inject.20,29,49 Considering rituals are developed when negative emotions are present, it is no surprise to observe these themes in our study. Further, since injection processes can be complicated and contribute to these negative emotions, it is natural for patients to routinize injection steps to facilitate task completion.
Routines and Rituals as Distinct Behaviors
Although some authors use the term rituals to describe routine and ritual elements somewhat interchangeably, there are important distinctions between these concepts. In the case of self-injection, routine elements serve to organize the process and environment in efforts to decrease patient workload and are centered around the physical device and instructed steps (eg, Table 7; Q7). Our study found that routine elements were largely similar across disease states and drug therapies. Routine elements are anchored on device use steps and given the similarities in injection device use steps overall, it is perhaps unsurprising that routine elements were similar across all patients (eg, Table 7; Q11). In contrast, rituals are grounded in emotion, and serve to strengthen patient’s mental state, thus increasing patients’ intrinsic capacity to manage workload required.
The observation that routines and rituals were present in both biologic-naïve and biologic-experienced patients may point to an enduring psychological benefit that translates to reduced injection anxiety and increased injection performance. Although the sample size was small, our study suggests patients with higher treatment burden, greater injection anxiety, and lower injection confidence had longer ritual elements. Further studies with larger sample sizes are needed to establish a clear relationship between rituals and patient emotions.
Routine & Ritual Discovery by Experimentation
No patients in our study were taught their routines or rituals by their HCP, thereby forcing them to create these practices on their own. As patients accumulated experiences with their therapies, they learned what worked or did not work for them. This is consistent with other studies, which show the evolution of these elements through discovery and experiment, not by teaching.14,50 Through trial and error, patients may figure out specifically “what works” for them in managing their health-care responsibilities.50
We found that the development of routines and rituals followed a consistent process that is independent of prior experience with biologics, demonstrating that common training gaps early in initiation may lead to experimentation, adoption of elements that create positive experiences, and rejection of elements that create negative ones.
Previous Findings on Routines and Rituals in Healthcare
While this study specifically looks at rituals and routines in injection therapies, previous literature establishes the use of these practices across several routes of administration and disease states. Our findings on the value of routines and rituals are consistent with previously published literature on patients with injection therapies, oral therapies, as well as ophthalmics. One study found that among pediatric patients taking injectable medications for asthma, children that were part of families with better medication taking routines had better medication adherence.51 In contrast, a study exploring similar parameters determined that children with parents who practice fewer home routines had lower quality of life scores and higher asthma morbidity outcomes compared to their more routinized counterparts.52 Similar findings have been observed in patients taking oral therapies for HIV, as two studies examining variables associated with medication adherence found that integration of HIV medication routines into daily lives was an indicator of increased adherence success.53,54 Further, routines are commonly used to support patient adherence to ophthalmic medications. In glaucoma, patients often must administer lifelong eye drops, in some cases multiple times a day. One qualitative study found that taking eye drops became second nature when patients followed strict routines to incorporate their medication into their daily lives. When patients deviated from routines; however, the risk of missing a dose of eye drops seemed to increase.55
Utilizing Digital Platforms to Promote Routines & Rituals
Our observations suggest that routines and rituals, if taught early during initiation, may be a useful approach to avoid unnecessary experimentation by patients and build confidence and capability to self-inject more quickly. Digital ecosystems can potentially help to facilitate this process by personalizing content to “meet patients where they are.” Digital platforms can share common routines and rituals that may be used by other patients, which could speed up the exploration process and help patients establish these processes early on.
Further, through digital ecosystems, there may be a reduced reliance on HCP access, skills, materials, and unreliable online resources. While this study specifically looked at patients, future studies should look at the HCP perception of routines and rituals, and potential benefits routines and rituals on HCP’s as it relates to their workload and patient interactions.
Limitations
The positive findings of this study must be considered in the context of its limitations. Our convenience sample was intended to capture a range of dosing frequencies to explore how routines and rituals varied based on dosing frequency, but was not designed to be a representative, proportional sample based on prescriptions for new biologic starts in PsO, PsA, or AS.
Training characterization activities were completed by retrospective participant self-reporting and not by longitudinal ethnography. While most patients (63%) were on therapy ≤12 months, a portion of patients relied on prior recollection of an initial experience that occurred months earlier, which could be associated with negative bias or false memory.14 Nonetheless, we did not observe qualitative differences in self-reported use of training between the “recent” and “less recent” groups. These are potentially confounding factors that are not included in our data collection or analysis but could play a role in the differences observed. Ideally, these studies would be conducted in a more controlled setting where patient and HCP training interactions could be characterized dyadically to eliminate possibility of confounding effects; however, this is practically difficult. Future studies may consider prospective designs with larger sample size that allow for sub-group analysis to be properly powered.
We did not enroll an evenly matched sample of patients on prefilled syringes and autoinjectors. Autoinjectors comprise the majority of delivery devices for self-injected biologics in the US market, reflected in our convenience sample. However, as a result, our study did not have sufficient numbers of patients using prefilled syringes to compare differences between these two groups. Future studies may recruit balanced autoinjector and syringe populations where these differences may be of interest.
Our study was not powered a priori to detect differences in training, routines, or rituals. Effect size estimates were unavailable, as the literature in this area is sparse, and one purpose of our pilot study was to estimate effect sizes to inform larger-scale studies and statistically designed sampling plans.
Conclusion
This study identifies the specific routine and ritual elements self-injection patients employ, and the mechanism by which these elements are discovered and become ingrained. We observed that routines and rituals may play distinct roles in decreasing workload and increasing capacity among patients who self-inject biologics for chronic disease. Together, these elements may decrease the treatment burden experienced by patients. In this pilot study, we found that routines were present in all study participants, while rituals were present in some individuals, mainly those with higher underlying workload, lower underlying capacity, or shorter time on current biologic therapy. We found that routines and rituals were distinct, providing additional information to inform future research. Ritual elements, in particular, appear to be useful tools for patients who need additional emotional support, suffer from higher relative burden of treatment, or view their own treatment burden as unacceptable.
These findings suggest immediate improvements for clinical practice around biologic self-injection initiation focused on training consistency and teaching routines and rituals at initiation, as well as informing larger scale, longitudinal studies with a broader patient population. In addition to physical interventions, digital ecosystems can provide suggestions and specific guidance for patients as they develop their routines and rituals. Our study findings map closely to the existing literature, and together with other authors’ reports, offer actionable opportunities to improve the self-injection initiation experience for patients. Overall, our finding suggests that routines and rituals may have broad applicability across chronic disease states treated with self-injected biologics. Additional studies may be needed to further confirm this hypothesis and generalize our findings to other chronic disease states as whole.
Ethics and Consent Statements
All procedures followed in this study were in accordance with the 1964 Declaration of Helsinki and its subsequent revisions. Informed consent was obtained from all patients included in the survey. This article describes a non-interventional survey, and so does not involve any new studies of human or animal subjects performed by any of the authors.
Acknowledgments
The authors acknowledge Ale Linares Martinez for her contributions towards design of the graphical figures in this manuscript. The authors would also like to acknowledge the candor and enthusiasm of the study participants in sharing the personal aspects of their injection, routines, and rituals with the research team.
Author Contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship, take responsibility for integrity of the work, and have given final approval to the version to be published. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
MC, CF, KB, AR, JH, DK, NC are employees of Matchstick, who received consulting fees and research support from Novartis Pharmaceuticals. In addition, MC, CF, KB, AR, JH, and DK report pending patent to Novartis for portions of content patent described in paper. GJ and FP are employees of Novartis Pharmaceuticals. Dr Graham Jones has a patent PAT059185US pending to Novartis Pharmaceuticals. MP has no disclosures. The authors report no other conflicts of interest in this work.
References
1. Cohen LB, Nanau RM, Delzor F, Neuman MG. Biologic therapies in inflammatory bowel disease. Transl Res. 2014;163(6):533–556. doi:10.1016/j.trsl.2014.01.002
2. Sharma PK, Hota D, Pandhi P. Biologics in rheumatoid arthritis. J Assoc Physicians India. 2004;52:231–236.
3. Rich SJ, Bello-Quintero CE. Advancements in the treatment of psoriasis: role of biologic agents. J Manag Care Pharm. 2004;10(4):318–325. doi:10.18553/jmcp.2004.10.4.318
4. Mease PJ. Biologic therapy for psoriatic arthritis. Rheum Dis Clin N Am. 2015;41(4):723–738. doi:10.1016/j.rdc.2015.07.010
5. Buc M. New biological agents in the treatment of multiple sclerosis. Bratislava Medical J. 2018;119(04):191–197. doi:10.4149/bll_2018_035
6. Cohen JM, Ning X, Kessler Y, et al. Immunogenicity of biologic therapies for migraine: a review of current evidence. J Headache Pain. 2021;22(1):3. doi:10.1186/s10194-020-01211-5
7. McGregor MC, Krings JG, Nair P, Castro M. Role of biologics in asthma. Am J Resp Crit Care. 2018;199(4):433–445. doi:10.1164/rccm.201810-1944ci
8. May C. The hard work of being ill. Chronic Illn. 2006;2(3):161–162. doi:10.1177/17423953060020030701
9. Tran VT, Harrington M, Montori VM, Barnes C, Wicks P, Ravaud P. Adaptation and validation of the Treatment Burden Questionnaire (TBQ) in English using an internet platform. Bmc Med. 2014;12(1):109. doi:10.1186/1741-7015-12-109
10. Shippee ND, Shah ND, May CR, Mair FS, Montori VM. Cumulative complexity: a functional, patient-centered model of patient complexity can improve research and practice. J Clin Epidemiol. 2012;65(10):1041–1051. doi:10.1016/j.jclinepi.2012.05.005
11. Gelhorn HL, Balantac Z, Ambrose CS, Chung YN, Stone B. Patient and physician preferences for attributes of biologic medications for severe asthma. Patient Prefer Adher. 2019;13:1253–1268. doi:10.2147/ppa.s198953
12. Abolhassani H, Sadaghiani MS, Aghamohammadi A, Ochs HD, Rezaei N. Home-based subcutaneous immunoglobulin versus hospital-based intravenous immunoglobulin in treatment of primary antibody deficiencies: systematic review and meta analysis. J Clin Immunol. 2012;32(6):1180–1192. doi:10.1007/s10875-012-9720-1
13. Pivot X, Gligorov J, Müller V, et al. Patients’ preferences for subcutaneous trastuzumab versus conventional intravenous infusion for the adjuvant treatment of HER2-positive early breast cancer: final analysis of 488 patients in the international, randomized, two-cohort PrefHer study. Ann Oncol. 2014;25(10):1979–1987. doi:10.1093/annonc/mdu364
14. Schiff M, Saunderson S, Mountian I, Hartley P. Chronic disease and self-injection: ethnographic investigations into the patient experience during treatment. Rheumatology Ther. 2017;4(2):445–463. doi:10.1007/s40744-017-0080-4
15. Lang VA, Nalan D. Combination product patient training: how are patients trained and who conducts the training? Des Medical Devices Conf. 2018;V001T09A003–V001T09A003. doi:10.1115/dmd2018-6956
16. Tallman K, Janisse T, Frankel RM, Sung SH, Krupat E, Hsu JT. Communication practices of physicians with high patient-satisfaction ratings. Perm J. 2007;11(1):19–29. doi:10.7812/tpp/06-106
17. Cox D, Stone J. Managing self–injection difficulties in patients with relapsing–remitting multiple sclerosis. J Neurosci Nurs. 2006;38(3):167–171. doi:10.1097/01376517-200606000-00005
18. Mohr DC, Cox D, Epstein L, Boudewyn A. Teaching patients to self-inject: pilot study of a treatment for injection anxiety and phobia in multiple sclerosis patients prescribed injectable medications. J Behav Ther Exp Psy. 2002;33(1):39–47. doi:10.1016/s0005-7916(02)00011-3
19. Bemt BJF, van den Gettings L, Domańska B, Bruggraber R, Mountian I, Kristensen LE. A portfolio of biologic self-injection devices in rheumatology: how patient involvement in device design can improve treatment experience. Drug Deliv. 2019;26(1):384–392. doi:10.1080/10717544.2019.1587043
20. Zimmer PA, Braun LT, Fraser R, Hecht L, Kelliher F. Promoting success in self-injection: listening to patients. Medsurg Nurs. 2015;24:279–282.
21. Brod M, Rousculp M, Cameron A. Understanding compliance issues for daily self-injectable treatment in ambulatory care settings. Patient Prefer Adherence. 2008;2008(2):129–136.
22. Ridgeway JL, Egginton JS, Tiedje K, et al. Factors that lessen the burden of treatment in complex patients with chronic conditions: a qualitative study. Patient Prefer Adher. 2014;8:339–351. doi:10.2147/ppa.s58014
23. Rosbach M, Andersen JS. Patient-experienced burden of treatment in patients with multimorbidity – a systematic review of qualitative data. PLoS One. 2017;12(6):e0179916. doi:10.1371/journal.pone.0179916
24. Bienvenu OJ, Eaton WW. The epidemiology of blood-injection-injury phobia. Psychol Med. 1998;28(5):1129–1136. doi:10.1017/s0033291798007144
25. Cox D, Mohr DC. Managing difficulties with adherence to injectable medications due to blood, injection, and injury phobia and self-injection anxiety. Am J Drug Deliv. 2003;1(3):215–221. doi:10.2165/00137696-200301030-00005
26. Taddio A, Ipp M, Thivakaran S, et al. Survey of the prevalence of immunization non-compliance due to needle fears in children and adults. Vaccine. 2012;30(32):4807–4812. doi:10.1016/j.vaccine.2012.05.011
27. Zambanini A, Newson RB, Maisey M, Feher MD. Injection related anxiety in insulin-treated diabetes. Diabetes Res Clin Pr. 1999;46(3):239–246. doi:10.1016/s0168-8227(99)00099-6
28. Turner AP, Williams RM, Sloan AP, Haselkorn JK. Injection anxiety remains a long-term barrier to medication adherence in multiple sclerosis. Rehabil Psychol. 2009;54(1):116–121. doi:10.1037/a0014460
29. Wright S, Yelland M, Heathcote K, Ng SK, Wright G. Fear of needles–nature and prevalence in general practice. Aust Fam Physician. 2009;38(3):172–176.
30. Arlinghaus KR, Johnston CA. The importance of creating habits and routine. Am J Lifestyle Med. 2019;13(2):142–144. doi:10.1177/1559827618818044
31. Hobson NM, Schroeder J, Risen JL, Xygalatas D, Inzlicht M. The psychology of rituals: an integrative review and process-based framework. Pers Soc Psychol Rev. 2018;22(3):260–284. doi:10.1177/1088868317734944
32. Brooks AW, Schroeder J, Risen JL, et al. Don’t stop believing: rituals improve performance by decreasing anxiety. Organ Behav Hum Dec. 2016;137:71–85. doi:10.1016/j.obhdp.2016.07.004
33. Ahmed M, Wheeler C, Franklin BD, Begum R, Garfield S. Resilience of medication adherence practices in response to life changes: learning from qualitative data obtained during the COVID-19 pandemic. Healthc. 2021;9(8):1048. doi:10.3390/healthcare9081048
34. Lang M, Krátký J, Shaver JH, Jerotijević D, Xygalatas D. Effects of anxiety on spontaneous ritualized behavior. Curr Biol. 2015;25(14):1892–1897. doi:10.1016/j.cub.2015.05.049
35. Basiaga-Pasternak J. Pre-performance rituals and anxiety among young Polish and Ukrainian football players. Baltic J Heal Phys Activity. 2019;69–76. doi:10.29359/bjhpa.11.4.08
36. Jnr JEH, Schack T. Integrating pre-game rituals and pre-performance routines in a culture-specific context: implications for sport psychology consultancy. Int J Sport Exerc Psychol. 2017;17(1):1–14. doi:10.1080/1612197x.2017.1292301
37. Burton D. Do anxious swimmers swim slower? Reexamining the elusive anxiety-performance relationship.pdf. J Sports Exercise Psychol. 1988;10:45–61. doi:10.1123/jsep.10.1.45
38. Humara M. The relationship between anxiety and performance- a cognitive-behavioral perspective.pdf. Athletic Insight. 1999;1:1–4.
39. Keininger D, Coteur G. Assessment of self-injection experience in patients with rheumatoid arthritis: psychometric validation of the Self-Injection Assessment Questionnaire (SIAQ). Health Qual Life Out. 2011;9(1):2. doi:10.1186/1477-7525-9-2
40. Tran VT, Montori VM, Eton DT, Baruch D, Falissard B, Ravaud P. Development and description of measurement properties of an instrument to assess treatment burden among patients with multiple chronic conditions. Bmc Med. 2012;10(1):68. doi:10.1186/1741-7015-10-68
41. Tran VT, Montori VM, Ravaud P. Is my patient overwhelmed? Mayo Clin Proc. 2020;95(3):504–512. doi:10.1016/j.mayocp.2019.09.004
42. Malterud K, Siersma VD, Guassora AD. sample size in qualitative interview studies. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
43. Sandelowski M, Leeman J. Writing usable qualitative health research findings. Qual Health Res. 2012;22(10):1404–1413. doi:10.1177/1049732312450368
44. Baggott C, Chan A, Hurford S, et al. Patient preferences for asthma management: a qualitative study. BMJ Open. 2020;10(8):e037491. doi:10.1136/bmjopen-2020-037491
45. Team RC. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; 2020.
46. Rittberg R, Dissanayake T, Katz SJ. A qualitative analysis of methotrexate self-injection education videos on YouTube. Clin Rheumatol. 2016;35(5):1329–1333. doi:10.1007/s10067-015-2910-5
47. Fiese BH, Tomcho TJ, Douglas M, Josephs K, Poltrock S, Baker TA. Review of 50 years of research on naturally occurring family routines and rituals: cause for celebration? J Fam Psychol. 2002;16(4):381–390. doi:10.1037/0893-3200.16.4.381
48. Gardner B, Lally P, Wardle J. Making health habitual: the psychology of ‘habit-formation’ and general practice. Br J Gen Pract. 2012;62(605):664–666. doi:10.3399/bjgp12x659466
49. Mohr DC, Boudewyn AC, Likosky W, Levine E, Goodkin DE. Injectable medication for the treatment of multiple sclerosis: the influence of self-efficacy expectations and infection anxiety on adherence and ability to self-inject. Ann Behav Med. 2001;23(2):125–132. doi:10.1207/s15324796abm2302_7
50. Grossoehme DH, Filigno SS, Bishop M. Parent routines for managing cystic fibrosis in children. J Clin Psychol Med S. 2014;21(2):125–135. doi:10.1007/s10880-014-9396-1
51. Fiese BH, Wamboldt FS, Anbar RD. Family asthma management routines: connections to medical adherence and quality of life. J Pediatrics. 2005;146(2):171–176. doi:10.1016/j.jpeds.2004.08.083
52. Peterson‐Sweeney K. The relationship of household routines to morbidity outcomes in childhood asthma. J Spec Pediatr Nurs. 2009;14(1):59–69. doi:10.1111/j.1744-6155.2008.00175.x
53. Ryan GW, Wagner GJ. Pill taking ‘routinization’: a critical factor to understanding episodic medication adherence. Aids Care. 2003;15(6):795–806. doi:10.1080/09540120310001618649
54. Gifford AL, Bormann JE, Shively MJ, Wright BC, Richman DD, Bozzette SA. Impact of medical and nonmedical factors on physician decision making for HIV/AIDS antiretroviral treatment. J Acquir Immune Defic Syndr. 2000;23(5):396–404. doi:10.1097/00126334-200004150-00005
55. Frech S, Guthoff RF, Gamael A, et al. Patterns and facilitators for the promotion of glaucoma medication adherence—a qualitative study. Healthc. 2021;9(4):426. doi:10.3390/healthcare9040426
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.