")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Impact of Research Training on Newly Graduated Health Professionals’ Motivation to Undertake Research
Authors D’Arrietta LM , Vangaveti VN, Crowe MJ , Malau-Aduli BS
Received 20 June 2022
Accepted for publication 15 September 2022
Published 1 October 2022 Volume 2022:15 Pages 2223—2240
DOI https://doi.org/10.2147/JMDH.S377963
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Louisa M D’Arrietta,1,2 Venkat N Vangaveti,1,3 Melissa J Crowe,4 Bunmi S Malau-Aduli1
1College of Medicine and Dentistry, James Cook University, Townsville, Queensland, Australia; 2Library Services, Townsville University Hospital, Townsville Hospital and Health Service, Townsville, Queensland, Australia; 3Townsville Institute of Health Research and Innovation, Townsville University Hospital, Townsville Hospital and Health Service, Townsville, Queensland, Australia; 4Division of Tropical Health and Medicine, James Cook University, Townsville, Queensland, Australia
Correspondence: Louisa M D’Arrietta, College of Medicine and Dentistry, Division of Tropical Health and Medicine, James Cook University, Townsville, Queensland, 4811, Australia, Tel +61 7 4781 4060, Fax +61 7 4779 6371, Email [email protected]
Background: Clinical research is vital for improved patient health outcomes. However, there has been a decline in the number of new researchers replacing an aging workforce. This is because multiple factors impact on newly graduated health professionals’ (HPs) readiness and motivation to engage with research training and undertake research when taking up hospital clinical roles.
Methods: Drawing on the Expectancy-Value-Cost (EVC) theory, a sequential explanatory mixed methods design involving cross-sectional survey and purposely sampled participant interview data was utilised to investigate the factors that impact on motivation to undertake research for three newly graduated HP groups (allied health, medical and nursing and midwifery). Survey data were subjected to descriptive and inferential statistical analysis, while interview data were thematically analysed to identify recurring themes. Framework analysis was utilised for triangulation of findings.
Results: Participants’ previous exposure to research training influenced their expectancy to undertake research. Participants who had previous research training reported significantly higher (P < 0.001) research confidence (Median (IQR) 3.0 (3.0– 3.0)) compared to those who had no previous research training (Median (IQR) 0.0 (0.0– 1.0)). However, in relation to types of values attached to research, participants who demonstrated intrinsic and attainment values were more engaged and motivated to undertake research despite a myriad of barriers compared to those who demonstrated utility value (P < 0.001). The qualitative data revealed six overarching themes in terms of factors that influence motivation (i) Importance of early immersion into formal research training (ii) Attitude to research (iii) Time constraints (iv) Poor visibility of research training opportunities (v) Lack of organisational support (vi) Low returns on effort.
Conclusion: Research training builds confidence, however, to foster motivation for the uptake and continued engagement with research, educators would need to help new HPs see the intrinsic and attainment values of research as they move through the career pipeline.
Keywords: barriers, facilitators, expectancy-value-cost theory, postgraduate research training
Introduction
Research participation by newly graduated health professionals’ (HPs) when taking up their clinical roles in the hospital environment is largely dependent on whether they are research ready.1,2 Research readiness has traditionally been attributed to having acquired the knowledge and skills required to undertake research.2–4 For HPs, research training has to some degree become a precursor for conducting research; it may be defined as actions aimed at training researchers and includes the process of gaining required skills, knowledge, and information available pertaining to successfully conducting research.5 Interest in research amongst this cohort has traditionally been engendered in their undergraduate curriculum. Although, according to a recent UK study, this is less so in the case of nurses, midwives, and allied health than for medical professionals because of differences in undergraduate training programs.6
Undergraduate medical degrees may include research training which enhances motivation to undertake specialised post-graduate programs.7 For example, a recent Australian study found that 88% of respondents regarded research as a relevant part of medical training; however, only 24% stated that research was included in their undergraduate medical degree.8 Additionally, despite the substantial economic and health benefits realised from medical research with each $1 invested returning an average of $3.90 in health benefits,9 and financial benefit to the economy accounting for Australia’s largest manufacturing export sector worth $8.2 billion in 2019,10 research participation rates among Australian doctors has been declining from 2.1% in 2002 to 1.5% in 201011 and a further decline of 2.3% between 2013 and 201512 with similar declines echoed in the National Health Service (NHS) in the United Kingdom (UK) from 7.5% to 4.2% between 2004 and 2017.13
Nurses, midwives and allied health professionals6 are less likely to encounter and be influenced by research training in their undergraduate experience.14 Nevertheless, once in their clinical positions, they often develop interest in research and research training.6 They then compensate by undertaking formal post-graduate research training, motivated by a desire to improve patient care, career progression, personal development as well as the research capacity and culture of the organisation in which they work.13,15,16 While emerging evidence shows that increasingly organisations are attempting to build the research capacity of allied health professionals by promoting dedicated or embedded research positions,17–19 a recent study has shown that fewer than 1% of allied health professionals in the UK are employed in clinical academic roles,13 and these roles are held by mid/late career HPs with post-graduate research qualifications. Furthermore, the nursing, midwifery, and allied health workforce make up only 1% of the clinical academic workforce in the UK.15 In Australia, 64% of Victorian allied health clinicians perceived lack of access to self-defined “research lead” positions, resulting in blurred career pathways for allied health researchers.15
These challenges pose a clinical academic progression dilemma for newly graduated health professionals who do not have a post-graduate qualification and are unlikely to have research training and experience,16,20 contributing to a decline in the number of new researchers replacing an aging workforce. This has significant ramifications for the whole HP research workforce which has been experiencing a continuing global decline over the last 40 years.21–23 The decline of new researchers epitomises a conundrum that has resulted in a review of the position of research in the HP undergraduate education landscape internationally.24,25 Globally, there is a recognition of the importance of developing formalised research training pathways at junior levels.6 To supplement the “insufficient” coverage of research in undergraduate health curricula,14 new pathways are often developed within the organisations in which HPs work to enable research readiness.3,4,26,27 Nonetheless, this has not translated into an increased uptake of HPs becoming involved in future evidence-based practice or pursuing a research career globally.24,25,28 To stimulate research interest and capacity building, HPs should be provided conducive environment and protected research time to conduct research while in their clinical roles; access to research training opportunities to acquire the required skills, knowledge and information pertaining to successfully conduct research; as well as capability to critically evaluate and apply new developments to their clinical practice.14
To foster an interest in research uptake by HPs, a plethora of initiatives have been introduced at graduate and undergraduate levels.29 A major area of interest is fostering HPs’ motivation to engage in research education.28 Motivation is a human psychological characteristic that contributes to a person’s degree of commitment, it is a predictor of performance, and no task can be performed successfully unless the person involved has both the ability and the motivation towards completing the task.30 The question “could we catch them young”24 has been addressed by some researchers who used the Self-Determination Theory (SDT)24,28,31,32 to investigate if “motivation could be enhanced by building research competence and capability through research training.28,33,34 SDT proposes that people are more motivated to take action when they feel that what they do will affect the outcome.35,36 Studies have shown that desirability to achieve an outcome could be explored using the Expectancy-Value-Cost Model of Motivation (EVC).37,38 Expectancy relates to behaviour that is determined by confidence as well as competence and capability to achieve that outcome and it is traditionally gained by acquiring skills and knowledge.38 Within a research capacity building context, this refers to HPs’ perceived confidence and competence to undertake research successfully.37 Value is interpreted as either attainment value (ie, importance of doing well), intrinsic value (ie, personal enjoyment) and utility value (ie, perceived usefulness for future goals); and the value HPs place on the outcome largely drives their motivation to achieve it.39,40 Cost, on the other hand, pertains to the factors that prevent HPs from investing the time, energy and resources required to achieve the expected outcome of successfully engaging in research.37,38 However, little is known about how the domains within the EVC model interplay in motivating HPs to engage in research.
Our recent systematic review highlighted the significance of investigating HPs’ motivation for research through the EVC model to foster a research culture; it also revealed that attitude to research is a catalyst for motivation or amotivation to engage in research as it directly influences the relevance of barriers.23 Research training has been identified as pivotal to enhancing HPs’ interest to undertake research.41,42 Nonetheless, reduced accessibility to research positions for HPs is further exacerbated in rural and remote settings,23 and draws attention to the importance of building capacity within this context. In this current study, we build upon the initial work by utilising the EVC model to investigate the research training experiences of newly graduated HPs working at a regional university teaching hospital and how this influences their motivation to undertake research. The findings may guide strategies for research capacity building and workforce development. This study aimed to answer the following four specific research questions.
- What factors impact new graduate HPs’ research capabilities?
- What is the influence of confidence and value on motivation to undertake research?
- What are the enablers and barriers to engaging with research/research training?
- How can motivation to engage in research be enhanced?
Methods
Study Design
This study utilised a sequential explanatory mixed methods research design to collect and analyse quantitative cross-sectional survey and qualitative interview data.43 Findings from both phases of the study were triangulated to uncover the best possible explanations for the observed phenomenon.44 The Human Research Ethics Committee (HREC) of Townsville Hospital and Health Service granted approval for this study (Reference number: HREC/2019/QTHS/59607). All participants were provided with an information sheet and consent form that detailed the aims of the study and the ethical obligations of the researchers which included confidentiality and informed consent, including publication of anonymised responses. All these obligations were strictly adhered to during the research process. For the survey, informed consent was implied by submission of either the completed paper-based or online questionnaire. All interview participants were assured of anonymity and they provided verbal consent at the beginning of the interview.
Quantitative Phase
Research questions 1 and 2 were answered in this phase of the study. This phase involved the collection and analysis of survey data on the factors that impact new graduate HPs’ research capabilities, and the influence of confidence and value on their motivation to undertake research.
Survey Instrument Development
The survey instrument (Appendix 1) was adapted from previously validated questionnaires8,45–47 and developed based on the EVC model with a focus on the factors identified from our recent systematic review23 within the three domains: Expectancy for research capacity, Value reflected in attitude, and Cost which relates to barriers. The survey comprised three (3) major parts. Part A focused on the demographics of the participants. Part B had eight sections (total of 54 questions) and utilised 4/5-point Likert scale questions to assess participants’ perceptions of their research training experience, value of research, available time for research, training initiatives to encourage involvement in research, ability to attend research training, and confidence and motivation to undertake research. Part C included four open-ended questions relating to perceived benefits and barriers to research training as well as suggestions for improving research training. The survey was pilot tested by a representative group of 20 HPs of similar backgrounds to those whom the survey was distributed. Content validity was confirmed by three content experts, while inter-item correlations and internal consistency indexes confirmed the reliability of the instruments’ items and scales. The survey instrument had an acceptable reliability with an overall Cronbach’s alpha score of 0.848.
Participant Recruitment and Data Collection
All 236 new graduate HPs (medical interns, allied health and nursing and midwives) to the Townsville Hospital and Health Service (THHS) in January/February 2020 were invited to participate in this study. Sample size was calculated by hypothesising that 50% of the participants were motivated to undertake research and a minimum of 98 responses were required to achieve 80% power for detecting a medium-sized effect at a 0.05 level of statistical significance. The sample size was calculated using OpenEpi version 3. The first named author (LMDA) sent the survey link or paper copies (if preferred) through the new graduates’ co-ordinators to participants. Anonymous survey responses were collected via online Survey Monkey® (by SVMK Inc.) and Remark Office OMR from January 2020 to April 2020. Reminders increased the response rate. Interview participants were recruited through the final question on the survey. Thirteen out of the 14 who indicated availability were able to be contacted.
Quantitative Data Analysis
Quantitative data were analysed using SPSS software version 26. Numerical data were presented as means and standard deviations or median and interquartile range, while categorical data were presented as frequencies and proportions. Likert scale items were treated as ordinal. However, to assess the influence of the variables on motivation for research, a total score which is the sum of the item scores was calculated for each item. While these total scores are discrete and not continuous, under the Likert perspective, these total scores were treated as ordinal approximation of a continuous variable48,49 Nonetheless, non-parametric (Mann–Whitney U or Kruskal Wallis H) univariate analysis was undertaken. Correction for multiple testing was undertaken by performing Bonferroni correction. P value of ≤0.05 was considered statistically significant.
Qualitative Phase
The qualitative phase answered research questions 3 and 4. Purposive sampling of consenting participants from the survey was undertaken and semi-structured questions utilised for the collection of individual telephone/face-to-face interview data. Each interview lasted approximately 30 minutes and allowed participants to freely share their research training experiences and perceptions about research.50 The interview questions sought to explore participants’ experiences of enablers and barriers to engaging with research and their perceived views on how motivation to engage in research can be enhanced. The interview/discussion guide (Appendix 2) was developed from the responses to the survey questionnaire and was pilot tested before final use. Different sets of questions were developed for participants who had previously participated in research training and those who had not. For those who had participated in research training, the focus was on their perceptions and experience of the training and exploring the concepts of the impact of the training on their interest and motivation in undertaking future research, the barriers they encountered and their recommendations for future effective training programs to foster engagement in research. For participants who had not participated in research training, the conversation attempted to probe the reasons as to why they had not done so, including explicit barriers they had encountered or perceived they would encounter in future engagement in research training and whether research training would influence their motivation for research.
Interview Protocol and Data Collection
Three pilot telephone interviews were conducted by author LMDA and the recordings were reviewed by author BSMA to ensure clarity of questions and accuracy of data. Trustworthiness and shared understanding were fostered through member-checking (summarising interview accounts with each participant whilst still on the phone or in the interview room in person).51 Interviews continued until data saturation was reached.52
Qualitative Data Analysis
Interviews were audio-recorded, transcribed verbatim (by a professional transcriber) and de-identified before data analysis.53 All data were imported into QSR International’s NVivo version 12 Plus to facilitate storage, coding, and theme development.54 Inductive thematic analysis55 was used to identify emerging themes which were independently confirmed by LMDA and BSMA. A consensus meeting of team members resolved any discrepancies. Illustrative quotes were presented verbatim. To maintain confidentiality participants were assigned with pseudonyms. The consolidated criteria for reporting qualitative research (COREQ) checklist56 was utilised to guide the procedures for the qualitative phase (see Appendix 3 for a detailed COREQ protocol).
Triangulation of Findings
Triangulation of the quantitative and qualitative findings was conducted using framework analysis. This involved the application of the EVC37,38 theory of motivation to integrate, synthesise, and interpret the results from both phases of the study.
Results
Quantitative Phase
Characteristics and Research Experience of Participants
Out of a total population of N = 236 new graduates, including allied health n = 15 (6.36%), medical n = 71 (30.08%), nursing and midwifery n = 150 (63.56%), there were one hundred and fourteen (114) survey responses, all of which were complete and analysed giving a response rate of 48.3%. This group was representative of the whole population and all subgroups were well represented. Table 1 portrays the demographic characteristics of the participants. Respondents were predominantly females, Australian citizens/Permanent residents and held undergraduate qualifications. Respondents were in the early stages of their careers and their ages ranged from 20 to 57 years of age of whom 40.4% were up to 23 years, 28.9% from 24 to 28 years and 30.7% were 29 years and above. The majority of the participants (85.8%) had not worked in major city hospitals.
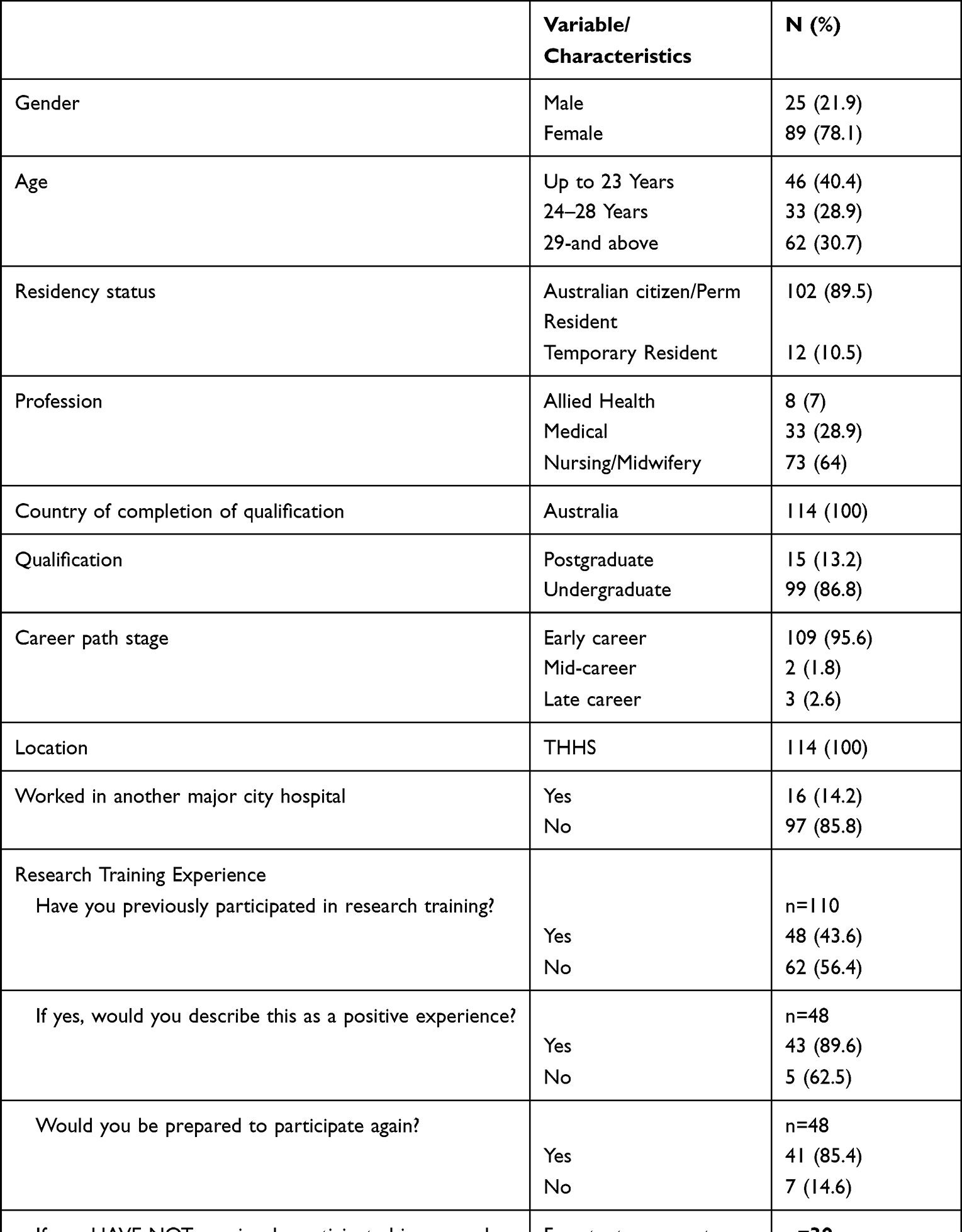 |
Table 1 Characteristics and Research Training Experience of Participants* |
As shown in Table 1, over half (56.4%) of the participants had not participated in research training. Of those who had been involved in research training previously, 89.6% had found it a positive experience and would be prepared to participate again (85.4%). About one-third of the participants (34.2%) responded to the open-ended question as to why they had not participated in research training with just under half indicating it was either because of lack of opportunity (46.2%), had never been asked (28.2%), did not know it existed (17.9%) or because of lack of time/interest (7.7%).
Factors That Impact on Research Capabilities
As shown in Table 2, participants’ previous exposure to research training influenced their reported research experience and confidence to undertake research. Participants who had previous research training reported significantly higher (P < 0.001) research experience (Median (IQR) 3.0 (3.0–3.0)) compared to those who had no previous research training (Median (IQR) 0.0 (0.0–1.0)). They also had higher (P < 0.004) confidence levels to undertake research (Median (IQR) 29.0 (23.8–36.0)) compared to those who had no previous research training (Median (IQR) 25.0 (20.0–30.8)). Younger participants reported significantly higher (P < 0.005) research experience (Median (IQR) 2 (0–3.0)) than their older counterparts (Median (IQR) 1 (0–3.0)). Male participants reported significantly higher research experience (P < 0.002) Median (IQR) 3 (1–3) vs Median (IQR) 1 (0–3) and motivation to undertake research (P < 0.044) Median (IQR) 29.0 (26.5–33.5) vs Median (IQR) 27.0 (24.3–30.3) than their female counterparts. The nursing and midwifery group reported significantly lower (P < 0.034) Median (IQR) 1 (0–2.3) research experience than the medical (IQR) 3 (0 −0.3.0) and allied health (IQR) 2 (0.5 −0.3.0) professional groups. Overall, previous research training improved participants’ research experience and increased their confidence levels to undertake research, particularly for younger male HPs and the medical professional group.
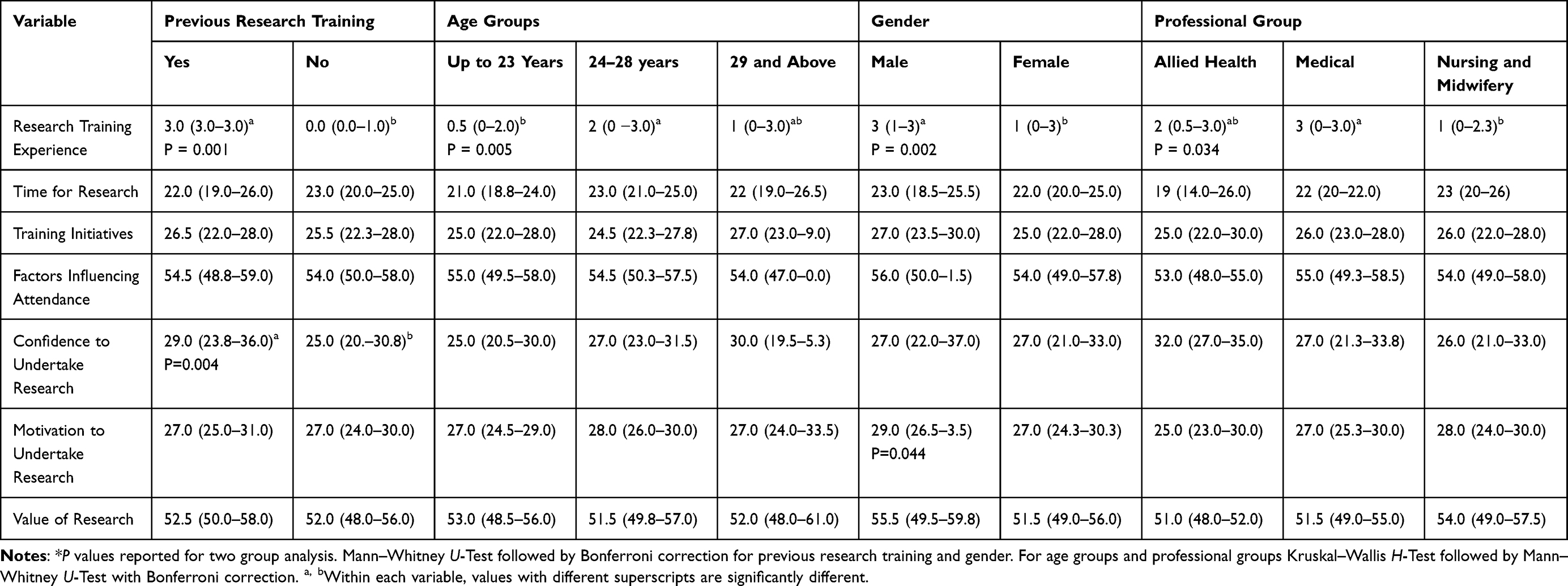 |
Table 2 Influence of Demographics on Participants’ Research Capabilities* |
Influence of Confidence and Value on Motivation
Table 3 portrays the influence of confidence and value attributed to research on motivation to undertake research. There was no significant difference in the confidence levels of participants who had low motivation levels (Median (IQR) 25.0 (24.0–27.0)) and those who had high motivation levels (Median (IQR) 31.0 (30.0–34.0)). Interestingly, for overall value, participants with high motivation levels attributed significantly higher (P < 0.001) value to research (Median (IQR) 30.0 (29.0–33.3)) than those who had low motivation levels (Median (IQR) 25.0 (24.0–27.0)). Motivation was also significantly influenced by type of value; attainment and intrinsic values were significant at P < 0.001 while utility value was significant at P < 0.003. Overall, it is not the confidence gained from research training, but rather the value attributed to research, that significantly influences motivation to undertake research.
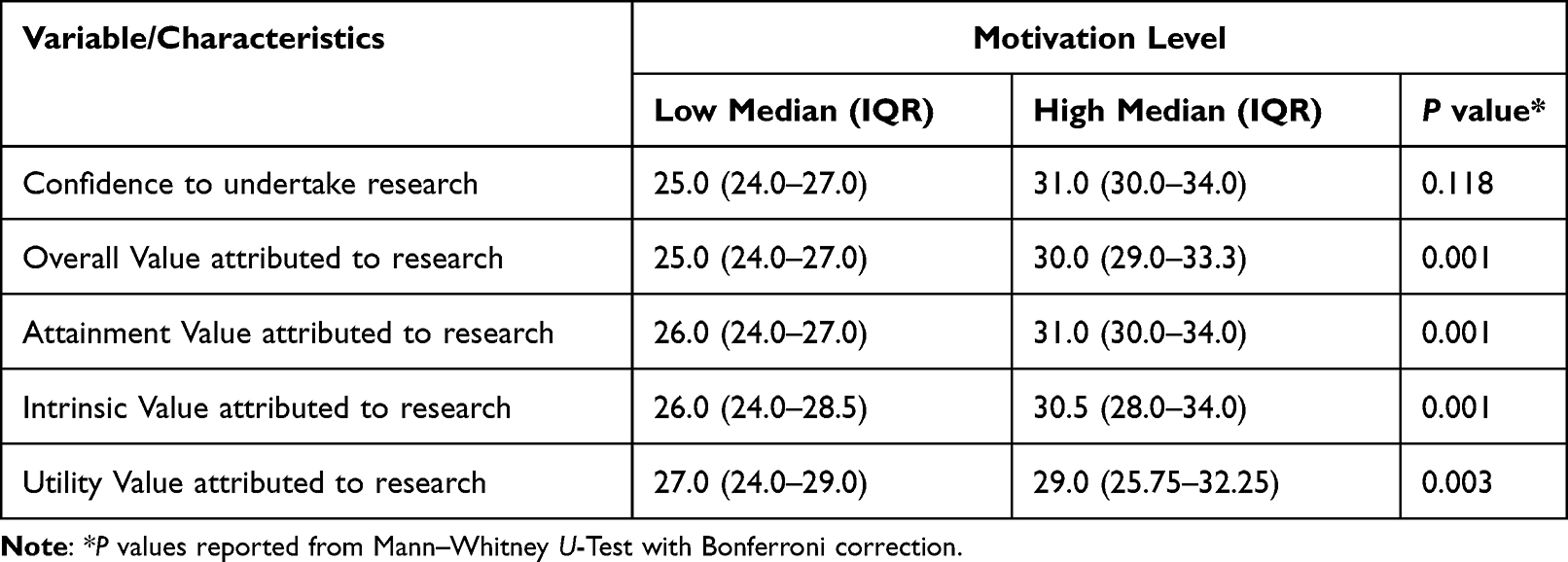 |
Table 3 Influence of Confidence and Value on Motivation to Undertake Research |
Qualitative Phase
Thirteen participants were involved in the qualitative interviews, comprising 7 females (63.8%) and 6 males (46.2%) (Medical N = 6, males n = 3, females n = 3; Nurses and Midwives N = 7, males n = 3, females n = 4). No Allied Health new graduates responded to the invitation to participate in an interview. Six overarching themes emerged in relation to research question 3. Two of these themes were enablers to engaging with research: (i) importance of early immersion into formal research training and (ii) attitude to research. The remaining four themes were barriers to undertaking research: (iii) time constraints, (iv) poor visibility of research training opportunities, (v) lack of organisational support, (vi) low returns on effort. Four themes emerged as recommendations for motivation to engage in research: (1) organisational support, (2) appropriate timing for research training, (3) protected time for research, (4) supervision and support. A detailed description of the themes is provided below. Illustrative quotes are presented and affixed with participants’ interview number and demographic profiles. For example, P13 MN refers to Participant 13, Male, Nurse.
Enablers to Undertaking Research/Research Training
The interviewees reported (i) importance of early immersion into formal research training and (ii) attitude to research as two major enablers to engaging with research.
Importance of Early Immersion into Formal Research Training
All participants emphasised the importance of early immersion into formal research training at the undergraduate level. Participants who had not previously been involved in research training reported lack of confidence in doing research. They also expressed that research training would provide the guidance needed to assist with their confidence and competence to successfully undertake research. They reported that research training could alleviate some of their concerns about the difficulty of research. Regardless of whether or not interviewees had undertaken prior research training they were able to see the value in doing research and were willing to explore opportunities for future participation.
I wish that I had done more formal research training. That would have given me a little bit more confidence and I guess having more confidence and more structure in what I could offer to the team definitely would have been beneficial, I think. (P2 FI)
Definitely necessary, because I mean I know that leaving university I had no real understanding of how to do research of my own, so it would be valuable. Well, I guess I would be hoping if I was going to research training that they might be able to guide me through a little bit and teach me the process. Hopefully, develop a little bit of confidence that I would be able to undertake it and, yeah, that it would be possible, because right now I wouldn’t really know where to start. (P13 MN)
Attitude to Research
All participants from both the medical and nursing professions expressed a positive attitude to research and research training and acknowledged the importance of participating in both for the benefit of their patients and their careers. Those who had been previously involved in research were mostly doctors and they emphasised the importance of research for career progression.
For me, personally, what drives me is that I do see a lot of value in research and would like to explore how I could participate in that. I know that training would be the way for me to explore those avenues. (P11 FN)
I think it’s largely intrinsic for me. I’m passionate about it and I do find adding value to or finding some knowledge or answer questions like that is quite interesting. I think it adds another dimension to my work and my learning as well. (P7 MI)
Barriers to Undertaking Research/Research Training
Interviewees from both the medical and nursing groups reported that there were major challenges that limited their ability to engage in research. These challenges included time constraints, poor visibility of research training opportunities, lack of organisational support and low returns on effort.
Time Constraints
Participants were acutely aware of constrictions on their time to do research or engage in research training while working full-time as clinicians. They felt that research would be time consuming and given that they were in the early stages of their career, they wanted to focus on the specialty training program.
I personally haven’t thought too much about research training. I suppose, in my phase of career it’s just a bit too busy at the moment. I’ve just started becoming a nurse. Maybe when I have a bit more time, so maybe the research might be time consuming, and that could be a barrier. I would take it on maybe next year. This year is just very, very hectic for me, and especially with the graduate program, I have assignments and things like that, I have to do. Yes, and the timing. But I would definitely in the future, once I upgrade my skills in nursing and become a bit more confident in myself, I’ll definitely take part in something like that. (P1 FN)
Poor Visibility of Research Training Opportunities
Respondents from the nursing group reported that they had little or no exposure to research in their undergraduate years while the medical group lamented that it was either overshadowed or introduced near the end of their medical degree. The participants also complained that despite the fact that there were multiple resources from an educational institution, academic institution, and also a professional body and corporation such as the hospital, they were mostly inexperienced. They also indicated they had little or no knowledge of research training opportunities available to them and that where they did, they often found little opportunity to participate.
It wasn’t offered, and I really hadn’t been exposed to it at the university. But I was aware that there were research groups that were happening out of Townsville. It’s just a little bit hard in your first year, in your grad year. (P3 MN)
I think just being informed about it would be a good start. I think if you were introduced to the idea by your lecturers, so if it was just brought into attention time and again, I think that would motivate a lot of people. I think a lot of us have the idea that we needed to do an Honours program or some kind of research as regards to doing the medical degree. So we did start probably like halfway through; everyone started to look at opportunities. So, I think that should have been introduced to us earlier as well. (P7 MI)
Lack of Organisational Support
Participants reported lack of organisational support as another significant constraint to research involvement. Participants indicated that the lack of support stemmed from the fact that they were new graduates and their advisors recommended they concentrate on their clinical roles before considering further study or research.
I think because I’m so fresh out of uni, and I have mentioned to my manager that I was intending on doing my Honours myself and was advised not to do that just yet, to try and find my feet before I get back into the research and study. I’ve been knocked off my pedal a couple of times just by other people saying, oh you know, I think that’s probably something that you shouldn’t be looking into just yet. So yes, I mean, that’s sort of taken my motivation down a little bit but I’m still very passionate about my topic. So it is something that I will endeavour to pursue. (P5 FN)
Low Returns on Effort
In terms of return on time and effort invested, respondents were also ambivalent as to the outcome of their efforts in this area. They felt the effort put into research was not easily rewarded and did not easily translate into measurable personal outcomes. This indicated that they did not see any personal value in undertaking research.
I had no intention of completing an Honours project while I was at university, because I didn’t find any interest that the university created for research. I think at the end of the day, there’s a number of cases that have been published from Honours projects. It’s probably like eight per cent or something like that. very small amount that have actually reached publication. It’s a lot of stress for students to take on, a lot of work to take on, and the reward is not always there for the amount of effort - it doesn’t translate from effort to rewards sometimes. (P7 MI)
Recommendations for Promoting Motivation to Engage in Research
Participants identified and recommended four areas for improvement to promote a research culture that fosters motivation to engage in research: organisational support, appropriate timing for research training, protected time for research and supervisor/mentor support.
Organisational Support
The participants reported that they had applied to work at their organisation because of its reputation for promoting a strong research culture. However, they felt there was a need for more organisational support to increase the visibility and accessibility of available research/training opportunities.
I mean, just seeing how they work, like the research team at the hospital, that was something when I looked at applying for the job that was part of the reason for applying to Townsville, was knowing that there was a research group within the hospital. I haven’t heard any bad thing about it. When I was researching to see what was available at the hospital and what initiatives the hospital was taking as a result of research, it was quite mind blowing, and I was like I want to be a part of that and obviously getting the grad program to come over as well. But during my orientation there was only me and one other person who put our hands up to say that we were interested in undertaking further research. (P5 FN)
The interviewees provided some insight on how to inculcate a research culture into the organisation from the ground up to make it more inclusive on an ongoing basis. Ideas included publicising research training opportunities, providing examples of research translated into practice throughout the organisation and inclusion of research training in the new graduate program orientations. Participants reported that if research training was embedded as part of continuing professional development, and advertised/promoted at events such as orientation programs, many of them would be inclined to participate.
I think if it was part of a continued professional development, I think that would be really beneficial because you’re actually contributing. It would encourage a lot more people on a broader spectrum to attend. Also, I think good examples of research done in the institution to show that it is possible for junior practitioners and new clinicians in the workplace to perform it, yeah, because it can be quite far removed from practice in some circumstances. But when it’s more present in the workplace and in every day, I guess, is a more active part of practice. It’s more motivating to other clinicians that it is possible and available to them rather than a distant idea of what you can do. (P6 MN)
I think perhaps making it I suppose more noticeable, more at the forefront I really haven’t heard about any other than the first session that we did with XXX, I’ve not really heard much about research, other than the survey that I filled out earlier in the year. I would have loved to have been involved. (P12 FN)
Appropriate Timing for Research Training
Participants had numerous suggestions for, when where and how research training could be provided including during undergraduate, postgraduate education and in the workplace nominating after hours, face-to-face/on-line options delivery modes. Interviewees most frequently mentioned a preference for research training during their undergraduate education. Interviewees from both the medical and nursing groups overwhelmingly nominated including research training in their undergraduate degrees so they are research ready once they take up their clinical roles.
I think a good introduction to it would be in any undergraduate degree. We may not have to undergo a whole research thesis or a proposal but at least if they did something small to encourage us to learn and how to apply those skills, it could serve as an introduction for us to start thinking about it for the future, especially once we enter our fields, that we find areas that we may want to research. We would have a foundation to start with. (P11 FN)
The participants also proposed that research training during the postgraduate phase would have a more immediate benefit for them being research ready in terms of competency and motivation to engage in research especially if it was included in the program for graduate nurses commencing at the hospital.
I think in an undergraduate year, we are told the importance of research but it’s hard to imagine research coming to light when we don’t have too much clinical experience yet. Starting as an intern this year, I’m starting to realise why it’s so important to have ongoing research that continue to explore and ask questions. So, I would say intern year would probably be one of the best times for research training, because now we’ve passed medical school and they’ve given us our little doctor lanyard. (P2 FI)
As part of the undergraduate degree would be fantastic. Also, as part of the graduate program, because I suppose the idea of research as a nurse is not really - it’s not brought up a lot during your undergraduate degree. So, we had one session on it in the graduate program, it doesn’t pique everyone’s interest, and some of us go, oh wow, that sounds very interesting. Then we hear nothing more about it, - so during the undergraduate degree, I think, and then also during the graduate program, I think would maybe make research less of an abstract concept to us. (P 12 FN)
The interviewees had views on when and how research training could be delivered including during and after hours, face-to-face/on-line, varied considerably impacted by time taken by their work-life commitments. While some interviewees stated that they preferred face-to-face training, others acknowledged that was not always possible due to their work schedules which often put them at a disadvantage of attending scheduled face-to-face training sessions. Interviewees acknowledging the difficulty of attending face-to-face training suggested that on-line training might be a viable alternative to accommodate them.
Online access would be a great motivator. I think the ability to access training when I have the time would be fantastic. Whether that means it’s a fully online package or just the ability even to dial in and watch a live session but from wherever I am, I think that would be a huge motivator, because it makes it significantly easier to work it around my set hours. (P12 FN)
Self-paced learning or training embedded in the formal onboarding of new graduates was suggested by interviewees especially those who were remote from the hospital as remoteness of physical connection to the hospital was a consideration for rural HPs who felt isolated.
I think that the best way in the workplace would be to have it available in person or even recorded sessions that people could follow along with. As a nurse, I can find sometimes on my night shift that I have a lot of time that I could do things. So, if there was recorded things I could watch that would walk me through how to do research, and things that I could do and tasks that I could undertake to practice, I could do those on my night shift. Then there could also be options to attend workshops for people who that’s an option for. (P11 FN)
Protected Time for Research
Interviewees expressed a desire for protected time to facilitate research/training. However, they acknowledged that due to the nature of their job, having protected research time has not been as pragmatic as desired.
It’s also protected intern teaching time, which makes us feel supported. But I think if there’s protected time for research training, that would definitely help in the years to come. I think probably in the resident years it would be beneficial too, to have a little bit of protected time. (P2 FI)
Supervisor/Mentor Support
The medical doctors expressed the need for practical guidance by supervisors/mentors in the research/training journey. These participants also felt some supervisors needed upskilling on how to train and engage their juniors in research, implying the need for a “teach the teacher” program.
Do you think there would be any benefit for supervisors out there to undergo training on how to train juniors, because I think there are a lot of supervisors who assume that the juniors know how to do basic programs or basic Excel but some of us do not have that IT experience [laughs]. Do you find that it would be helpful for supervisors to know how to train the juniors, or are they inherently good at teaching? (P2 FI)
Triangulation/Integration of Findings
Integration and synthesis of the qualitative interview findings and quantitative survey results as aligned with the EVC theoretical framework is summarised in Table 4. In relation to expectancy of involvement in research, the quantitative data showed that participants who had prior research training experience were more confident to undertake research compared to those who had no previous research training. This was confirmed in the interviews and highlights the pivotal role of research training in inspiring confidence to undertake research. There was consonance between the survey and interview findings in relation to the importance of value attributed to research in fostering motivation to undertake research at the individual, team, and organisational levels. The interview participants also corroborated the survey findings as they emphasised the implications of unprotected research time and lack of organisational and financial support on motivation to engage in research.
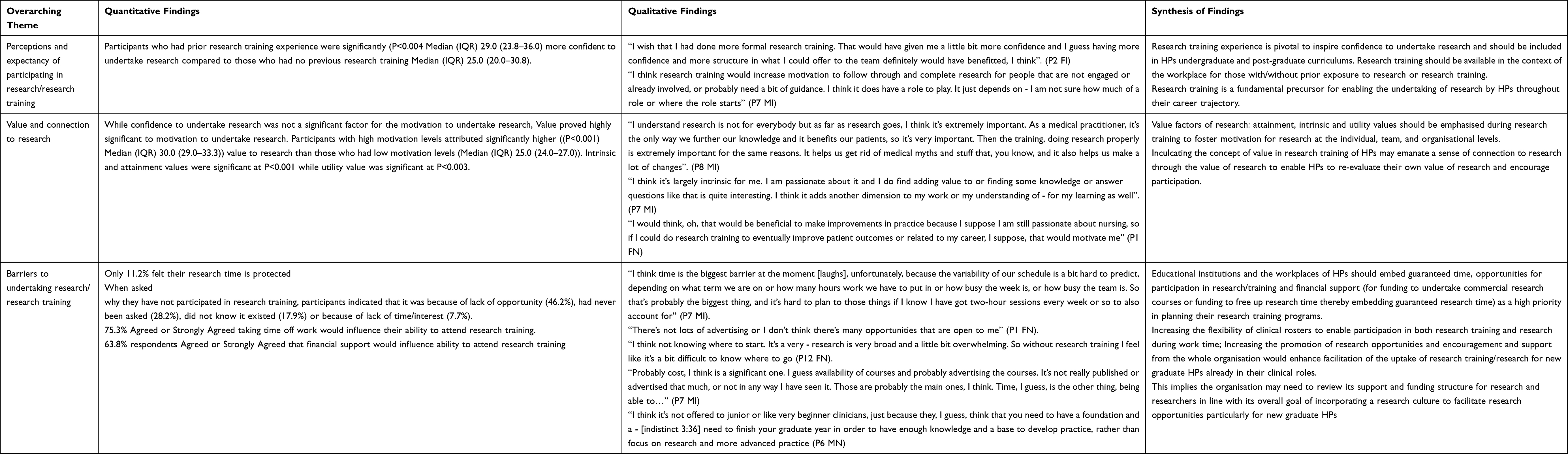 |
Table 4 Triangulation of Study Findings Using the Expectancy + Value – Cost = Motivation Model |
Discussion and Conclusions
Discussion
This study adds to previous work by adopting a theoretically informed mixed methods design to investigate newly graduated HPs’ perspectives about the impact of research training on their motivation to undertake research. The novelty of this study is based on the utilisation of the EVC theory to better understand the factors that influence newly graduated HPs’ research capabilities and their motivation to engage with research. Both the quantitative and qualitative phases of this study highlighted the influence of confidence and value on motivation to do research and undertake research training.57–60
The study findings showed that participants who had prior research training were more confident than those who had not been previously exposed to training. Previous research training was viewed positively by respondents and significantly influenced their expectations about participating in research. This result has been reported in previous studies13,41,61–65 and confirms that research training is pivotal to inspiring confidence. Therefore, it behooves educational institutions to establish research training opportunities early in the curricula in undergraduate HP programs. By embedding research training into the undergraduate program, new graduates will gain confidence to undertake research when they take up their clinical positions in the hospital environment. Nonetheless, confidence levels did not influence the participants’ motivation and willingness to undertake research.
Motivation to undertake research is underpinned primarily by the value and connection attributed to research15 and to a lesser degree by the confidence in the expectancy of being able to successfully engage in undertaking research.24,66 This implies that emphasis at all stages of research/training trajectory should focus on the value of research, particularly attainment and intrinsic values to imbue a sense of worth to the research/training endeavour at the individual and organisational level. Regular exposition of research values (attainment, intrinsic and utility) throughout the undergraduate and into the postgraduate phases of education and embedding into the culture of the organisation may add a whole new paradigm for research and training.6,7,66
Nonetheless, there are factors that can potentially inhibit the uptake and continuing engagement with research and training. Our study participants perceived little or no return on time and effort invested in their expectations of research outcomes because of barriers including lack of time, poor visibility of training opportunities, lack of visible and inherent organisational support vis-a-vis mentors, supervisors and the organisational structure as deterrents to engaging with research.23,25,34,66,67 Respondents revealed that the cost of participating in research and training particularly that of time for research would be in competition with their other goals including work-life balance, clinical time, financial benefits and organisational expectations.18,20,23,67–72
Our study findings indicate that there are significant challenges for HP undergraduates, particularly for those in nursing and allied health who are less likely than medical undergraduates to have the opportunity to be exposed to research training in their undergraduate curriculum. Therefore, there is need to make greater provision for research training to support research readiness for when these HPs take up their clinical roles in public hospitals after graduation. Additionally, the reported lack of organisational support confirmed by previous studies6,15,16,72,73 indicates that for those new graduates taking up clinical roles, the benefit of having had research training in their undergraduate years would have attenuated some of the concerns expressed in our current study about their confidence and competence to undertake research in their new work areas. Inculcating the values of research and embedding them in research training in undergraduate curricula and in the early postgraduate phase after taking up clinical roles in their health organisation would contribute substantially to the research readiness of new graduates.
The competing demands on newly graduated HPs as they settle into their clinical work roles highlight the challenging intersect between individual capability and capacity. This substantiates the need for research capacity building interventions that address both individual training needs and organisational bottlenecks. At the individual level, it is important to increase research training opportunities for HPs with emphasis on attainment and intrinsic value attributed to research. At the organisational level, attention should be given to strengthening of organisational research culture and the development of research support networks and partnerships. New graduates in our study taking up clinical roles in the hospital expressed the desire to be able to enter into an inclusive organisational environment where research is pivotal and embedded in quarantined time, allowing for professional development and research training opportunities. Furthermore, the respondents in our study echoed what other studies have previously identified as the provision of a variety of flexible research training modules including face-to-face and online26 opportunities for engagement in research that is supported by suitably skilled research supervisors/mentors within the constructs of the work experience.27,74 Such training opportunities should be accessible to all, notwithstanding their physical location, to overcome a sense of lack of connection experienced by rural HPs who felt isolated due to the remoteness of their location.45
Engaging HPs in research training facilitates research endeavours and successful outcomes that translate to dollar savings in patient care both directly and indirectly through applying research findings to the treatment and management of diseases.23 Investing in research and research training may be a cost-efficient strategy/initiative for both educational institutions and health-care organisations to mitigate the decline in research participation.27 By emphasising the attainment, intrinsic and utility value of research during research training for newly graduated HPs, the organisation can increase its research capability and capacity to maximise health-care outcomes.
Strengths and Limitations
The strengths of this study include the use of a sequential explanatory mixed methods design and theory-driven conceptual framework in rethinking the impact of training on the motivation of new HP graduates to undertake research. Nonetheless, generalisability of the findings may have been limited by participants’ self-reported responses and sample bias which relates to the chance that people who volunteered to participate in our research had a positive attitude or interest in research as opposed to those who did not participate. Additionally, the study design restricted opinions to new graduate HPs from only three HP groups, within one rural/remote organisational setting. Furthermore, the perspective of the Allied Health group was not represented in the qualitative findings as they were not available to participate in the interviews.
Conclusion
This study has demonstrated that newly graduated HPs are generally interested in undertaking research as part of their career trajectory and it has provided a lens with which to reconsider research training by using the EVC model with a particular focus on the value concepts: attainment, intrinsic and utility values and how they influence current and future attitude to the uptake and continuance of research/training. Promoting awareness of the vital role of connectivity and value attributed to research through research training/education may facilitate readiness and motivation of newly graduated HPs to undertake research in their clinical roles. Research training facilitators as well as educational institutions, workplace organisations, accrediting professional associations and funding bodies could translate these findings into practice. Future studies could explore the concept of value (attainment, intrinsic, utility) attributed to research at different HP career stages.
Abbreviations
EVC, Expectancy-Value Cost Theory; SDT, Self-Determination Theory; HPs, Health professionals; COREQ, Consolidated criteria for reporting qualitative research.
Acknowledgments
This research was supported by a research grant from the Study, Education and Research Trust Account (SERTA), Townsville Hospital and Health Service (SERTA 2019_17).
Disclosure
The authors report no conflicts of interest in this work.
References
1. McMaster R, Jammali-Blasi A, Andersson-Noorgard K, Cooper K, McInnes E. Research involvement, support needs, and factors affecting research participation: a survey of mental health consultation liaison nurses. Int J Ment Health Nurs. 2013;22(2):154–161.
2. Lopez-Bushnell K. Get research-ready. Nurs Manage. 2002;33(11):41–44. doi:10.1097/00006247-200211000-00018
3. Central Queensland Hospital and Health Service. Research program to transform CQ healthcare. Queensland Helath; 2018. Available from: https://www.health.qld.gov.au/cq/about/news/articles/research-program-to-transform-cq-healthcare.
4. University of Queenaland Rural Clinical School. The research ready grant program University of Queensland; 2021. Available from: https://rcs.medicine.uq.edu.au/research/research-events.
5. Ángel MD-V. Teaching digital competence and scholarly communication: ten years moving researchers to digital scholarship at Pablo de Olavide University. In: Viviana F-M, Llarina G-S, editors. Cases on Research Support Services in Academic Libraries. Hershey, PA, USA: IGI Global; 2021:142–165.
6. Avery M, Westwood G, Richardson A. Enablers and barriers to progressing a clinical academic career in nursing, midwifery and allied health professions: a cross‐sectional survey. J Clin Nurs. 2022;31:406–416. doi:10.1111/jocn.15673
7. Smith M, Patel J, Gay S, Davison I, Buckley S. Clinical scientists’ early career choices and progression: an exploratory mixed methods study. BMC Health Serv Res. 2021;21(1):1–9. doi:10.1186/s12913-021-07064-1
8. Mills JMZ, Januszewski AS, Robinson BG, Traill CL, Jenkins AJ, Keech AC. Attractions and barriers to Australian physician-researcher careers: physician-researcher influences. Intern Med J. 2019;49(2):171–181. doi:10.1111/imj.14086
9. Association of Australian Medical Research Institutes, KPMG. Economic impact of medical research in Australia. KPMG; 2018. Available from: https://aamri.org.au/wp-content/uploads/2018/10/Economic-Impact-of-Medical-Research-full-report.pdf.
10. Association of Australian Medical Research Institutes. Health and medical research in Australia. Association of Australian Medical research Institutes (AAMRI); 2022. Available from: https://www.aamri.org.au/health-medical-research/fast-facts-on-medical-research/.
11. Australian Institute of Health and Welfare. Medical workforce 2010. Australian institute of health and welfare. National health workforce series No. 1. Cat. No.: HWL 47 web site; 2012. Available from: https://www.aihw.gov.au/getmedia/75c1aba7-71b3-4844-bd8c-9afad41e8287/14055.pdf.aspx?inline=true.
12. Deloitte Access Economics. Australia’s health and medical research workforce: expert people providing exceptional returns; 2016. Available from: https://www2.deloitte.com/au/en/pages/economics/articles/australias-health-and-medical-research-workforce.html.
13. Cordrey T, King E, Pilkington E, Gore K, Gustafson O. Exploring research capacity and culture of allied health professionals: a mixed methods evaluation. BMC Health Serv Res. 2022;22(1):85. doi:10.1186/s12913-022-07480-x
14. King O, West E, Lee S, et al. Research education and training for nurses and allied health professionals: a systematic scoping review. BMC Med Educ. 2022;22(1):385. doi:10.1186/s12909-022-03406-7
15. Brandenburg C, Ward EC. ”There hasn’t been a career structure to step into”: a qualitative study on perceptions of allied health clinician researcher careers. Health Res Policy Syst. 2022;20(1):1–17. doi:10.1186/s12961-021-00801-2
16. Trusson D, Rowley E, Bramley L. A mixed-methods study of challenges and benefits of clinical academic careers for nurses, midwives and allied health professionals. BMJ Open. 2019;9(10):e030595. doi:10.1136/bmjopen-2019-030595
17. Wenke R, Mickan S. The role and impact of research positions within health care settings in allied health: a systematic review. BMC Health Serv Res. 2016;16:355. doi:10.1186/s12913-016-1606-0
18. Paget SP, Lilischkis KJ, Morrow AM, Caldwell PH. Embedding research in clinical practice: differences in attitudes to research participation among clinicians in a tertiary teaching hospital. Intern Med J. 2014;44(1):86–89. doi:10.1111/imj.12330
19. Slade SC, Philip K, Morris ME. Frameworks for embedding a research culture in allied health practice: a rapid review. Health Res Policy Syst. 2018;16:1. doi:10.1186/s12961-018-0304-2
20. Alison JA, Zafiropoulos B, Heard R. Key factors influencing allied health research capacity in a large Australian metropolitan health district. J Multidiscip Healthc. 2017;10:277. doi:10.2147/JMDH.S142009
21. McKinney RE
22. Wyngaarden JB. The clinical investigator as an endangered species. N Engl J Med. 1979;301(23):1254–1259. doi:10.1056/NEJM197912063012303
23. D’Arrietta LM, Vangaveti VN, Crowe MJ, Malau-Aduli BS. Rethinking health professionals’ motivation to do research: a systematic review. J Multidiscip Healthc. 2022;15:185–216. doi:10.2147/JMDH.S337172
24. Ommering BWC, van Blankenstein FM, Waaijer CJF, Dekker FW. Future physician-scientists: could we catch them young? Factors influencing intrinsic and extrinsic motivation for research among first-year medical students. Perspect Med Educ. 2018;7(4):248–255. doi:10.1007/s40037-018-0440y
25. Stone C, Dogbey GY, Klenzak S, Van Fossen K, Tan B, Brannan GD. Contemporary global perspectives of medical students on research during undergraduate medical education: a systematic literature review. Med. 2018;23(1):1537430.
26. McNab M, Berry A, Skapetis T. The potential of a lecture series in changing intent and experience among health professionals to conduct research in a large hospital: a retrospective pre-post design. BMC Med Educ. 2019;19(1):124. doi:10.1186/s12909-019-1548-4
27. Brown A, Pain T, Edelman A, Larkins S, Harvey G. Linking Research Investment and Input with Impact: A Research Impact Evaluation at the Townsville Hospital and Health Service (Final Report). Townsville: Townsville Hospital and Health Service; 2020.
28. Orsini C, Binnie VI, Wilson SL. Determinants and outcomes of motivation in health professions education: a systematic review based on self-determination theory. J Educ Eval Health Prof. 2016;13:19. doi:10.3352/jeehp.2016.13.19
29. Jain MK, Cheung VG, Utz PJ, Kobilka BK, Yamada T, Lefkowitz R. Saving the endangered physician-scientist - a plan for accelerating medical breakthroughs. N Engl J Med. 2019;381(5):399–402. doi:10.1056/NEJMp1904482
30. Ryan RM, Deci EL. Intrinsic and extrinsic motivations: classic definitions and new directions. Contemp Educ Psychol. 2000;25(1):54–67. doi:10.1006/ceps.1999.1020
31. Kusurkar RA, Ten Cate TJ, van Asperen M, Croiset G. Motivation as an independent and a dependent variable in medical education: a review of the literature. Med Teach. 2011;33(5):e242–e262. doi:10.3109/0142159X.2011.558539
32. Rosenkranz SK, Wang S, Hu W. Motivating medical students to do research: a mixed methods study using self-determination theory. BMC Med Educ. 2015;15(1):95. doi:10.1186/s12909-015-0379-1
33. Stewart D, Cunningham S, Strath A, et al. A theoretically informed survey of the views and experiences of practicing pharmacists on research conduct, dissemination and translation. Res Social Adm Pharm. 2019;15(11):1298–1308. doi:10.1016/j.sapharm.2018.12.005
34. Marais DL, Kotlowitz J, Willems B, Barsdorf NW, van Schalkwyk S. Perceived enablers and constraints of motivation to conduct undergraduate research in a faculty of medicine and health sciences: what role does choice play? PLoS One. 2019;14(3):e0212873. doi:10.1371/journal.pone.0212873
35. Ryan R. Self determination theory and well being. Soc Psychol. 2009;84(822):848.
36. Ryan RM, Deci EL. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness. New York: Guilford Press; 2017.
37. Eccles JS, Adler TF, Futterman R, et al. Expectancies values and academic behaviors. In: Spence J, editor. Achievement and Achievement Motives. San Francisco, CA: W H Freeman; 1983:74–146.
38. Eccles JS, Wigfield A. Motivational beliefs, values, and goals. Annu Rev Psychol. 2002;53(1):109–132. doi:10.1146/annurev.psych.53.100901.135153
39. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68–78. doi:10.1037/0003-066X.55.1.68
40. Deci EL, Olafsen AH, Ryan RM. Self-determination theory in work organizations: the state of a science. Annu Rev Organ Psychol Organ Behav. 2017;4:19–43. doi:10.1146/annurev-orgpsych-032516-113108
41. Hall AK, Mills SL, Lund PK. Clinician-investigator training and the need to pilot new approaches to recruiting and retaining this workforce. Acad Med. 2017;92(10):1382–1389. doi:10.1097/ACM.0000000000001859
42. Hay-Smith EJ, Brown M, Anderson L, Treharne GJ. Once a clinician, always a clinician: a systematic review to develop a typology of clinician-researcher dual-role experiences in health research with patient-participants. BMC Med Res Methodol. 2016;16:95. doi:10.1186/s12874-016-0203-6
43. Creswell JW, Clark VLP. Designing and Conducting Mixed Methods Research.
44. Yardley L, Bishop F. Mixing qualitative and quantitative methods: a pragmatic approach. In: Willig C, Rogers WS, editors. The Sage Handbook of Qualitative Research in Psychology. Thousand Oaks: SAGE; 2008:352–370.
45. Pain T, Plummer D, Pighills A, Harvey D. Comparison of research experience and support needs of rural versus regional allied health professionals. Aust J Rural Health. 2015;23(5):277–285. doi:10.1111/ajr.12234
46. Robinson GF, Switzer GE, Cohen ED, et al. Shortening the work preference inventory for use with physician scientists: WPI-10. Clin Transl Sci. 2014;7(4):324–328. doi:10.1111/cts.12132
47. Amabile TM, Hill KG, Hennessey BA, Tighe EM. The work preference inventory: assessing intrinsic and extrinsic motivational orientations. J Pers Soc Psychol. 1994;66(5):950–967. doi:10.1037/0022-3514.66.5.950
48. Norman G. Likert scales, levels of measurement and the ”laws” of statistics. Adv Health Sci Educ. 2010;15(5):625–632. doi:10.1007/s10459-010-9222-y
49. Sullivan GM, Artino AR
50. Sofaer S. Qualitative methods: what are they and why use them? Health Serv Res. 1999;34(5p2):1101.
51. Shaw R. Embedding reflexivity within experiential qualitative psychology. Qual Res Psychol. 2010;7(3):233–243. doi:10.1080/14780880802699092
52. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
53. Plano Clark VL, Creswell JW. Student Study Guide to Accompany Creswell’s Educational Research: Planning, Conducting, and Evaluating Quantitative and Qualitative Research / Vicki L. Plano Clark.
54. Jackson K, Bazeley P. Qualitative Data Analysis with NVivo.
55. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
56. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
57. STARSurg Collaborative. Medical research and audit skills training for undergraduates: an international analysis and student-focused needs assessment.[erratum appears in postgrad med j. 2018 feb; 94 (1108):86note: evans, david [added]; pmid: 29378916], [erratum appears in postgrad med j. 2018 jun; 94 (1112):324; pmid: 29853557]. Postgrad Med J. 2018;94(1107):37–42. doi:10.1136/postgradmedj-2017-135035
58. Al-Busaidi IS, Tarr GP. Dissemination of results from medical student public health research training and factors associated with publication. Postgrad Med J. 2018;94(1112):330–334. doi:10.1136/postgradmedj-2017-135361
59. Klimas J, McNeil R, Ahamad K, et al. Two birds with one stone: experiences of combining clinical and research training in addiction medicine. BMC Med Educ. 2017;17(1):22. doi:10.1186/s12909-017-0862-y
60. Dicianno BE, Glick RM, Sowa GA, Boninger ML. Processes and outcomes from a medical student research training program in integrative, complementary, and alternative medicine. Am J Phys Med Rehabil. 2016;95(10):779–786. doi:10.1097/PHM.0000000000000508
61. Yano EM, Resnick A, Gluck M, Kwon H, Mistry KB. Accelerating learning healthcare system development through embedded research: career trajectories, training needs, and strategies for managing and supporting embedded researchers. Healthcare. 2021;8(Supplement 1):100479. doi:10.1016/j.hjdsi.2020.100479
62. Purnell M. Findings from a training needs analysis survey to support health professionals across the research lifecycle. Health Info Libr J. 2020;37(2):118–127. doi:10.1111/hir.12303
63. Lyle D, Greenhill J. Two decades of building capacity in rural health education, training and research in Australia: university departments of rural health and rural clinical schools. Aust J Rural Health. 2018;26(5):314–322. doi:10.1111/ajr.12470
64. Harding CV, Akabas MH, Andersen OS. History and outcomes of 50 years of physician-scientist training in medical scientist training programs. Acad Med. 2017;92(10):1390–1398. doi:10.1097/ACM.0000000000001779
65. Jones AA, Ng E, Deguise MO, et al. Md/PhD training in Canada: results from a national trainee and program director review. Clin Invest Med. 2016;39(4):E132–139. doi:10.25011/cim.v39i4.27092
66. Sarwar MR, Saqib A, Riaz T, Aziz H, Arafat M, Nouman H. Attitude, perception, willingness, motivation and barriers to practice-based research: a cross-sectional survey of hospital pharmacists in Lahore, Punjab, Pakistan. PLoS One. 2018;13(9):e0203568. doi:10.1371/journal.pone.0203568
67. Pain T, Petersen M, Fernando M. Building allied health research capacity at a regional Australian hospital: a follow-up study. Internet j Allied Health Sci Pract. 2018;16(4):1–10.
68. Borkowski D, McKinstry C, Cotchett M, Williams C, Haines T. Research culture in allied health: a systematic review. Aust J Prim Health. 2016;22(4):294–303. doi:10.1071/PY15122
69. Harvey D, Plummer D, Nielsen I, Adams R, Pain T. Becoming a clinician researcher in allied health. Aust Health Rev. 2016;40(5):562. doi:10.1071/AH15174
70. Hiscock H, Ledgerwood K, Danchin M, Ekinci E, Johnson E, Wilson A. Clinical research potential in Victorian hospitals: the Victorian clinician researcher needs analysis survey. Intern Med J. 2014;44(5):477–482. doi:10.1111/imj.12396
71. Marshall AP, Roberts S, Baker MJ, et al. Survey of research activity among multidisciplinary health professionals. Aust Health Rev. 2016;40(6):667–673. doi:10.1071/AH15156
72. Wenke R, Noble C, Weir KA, Mickan S. What influences allied health clinician participation in research in the public hospital setting: a qualitative theory-informed approach. BMJ Open. 2020;10(8):e036183. doi:10.1136/bmjopen-2019-036183
73. Crombie A, Borkowski D, Gardner M, Masman K, Howlett O. Understanding the research capacity and culture of a regional allied health workforce. Aust J Prim Health. 2021;27(5):397–403. doi:10.1071/PY20260
74. Noble C, Billett SR, Phang DTY, Sharma S, Hashem F, Rogers GD. Supporting resident research learning in the workplace: a rapid realist review. Acad Med. 2018;93:1732–1740. doi:10.1097/ACM.0000000000002416
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.