")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Impact of Prior Digestive System Disease on In-Hospital Gastrointestinal Bleeding in Patients with Acute Myocardial Infarction
Authors Liu Y, Wang LF, Liu LH, Yang XC, Ren ZH, Li KB, Chen ML, Wang HS, Zhong JC, Xu L, Ni ZH, Li WM, Xia K, Zhang DP, Sun H, Guo ZS, Chi YH, He JF, Zhang ZY, Jiang F
Received 29 December 2020
Accepted for publication 24 February 2021
Published 22 March 2021 Volume 2021:14 Pages 1233—1239
DOI https://doi.org/10.2147/RMHP.S299169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Yu Liu,1 Le-Feng Wang,1 Li-Hong Liu,1 Xin-Chun Yang,1 Zheng-Hong Ren,2 Kui-Bao Li,1 Mu-Lei Chen,1 Hong-Shi Wang,1 Jiu-Chang Zhong,1 Li Xu,1 Zhu-Hua Ni,1 Wei-Ming Li,1 Kun Xia,1 Da-Peng Zhang,1 Hao Sun,1 Zong-Sheng Guo,1 Yong-Hui Chi,1 Ji-Fang He,1 Zhi-Yong Zhang,1 Feng Jiang1
1Heart Center & Beijing Key Laboratory of Hypertension, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2School of Public Health, Peking University Health Science Center, Beijing, People’s Republic of China
Correspondence: Le-Feng Wang
Heart Center & Beijing Key Laboratory of Hypertension, Beijing Chaoyang Hospital, Capital Medical University, No. 8 of Gongtinan Road, Chaoyang District, Beijing, People’s Republic of China
Tel/Fax +86 10 85231173
Email [email protected]
Objective: Patients presenting with acute myocardial infarction (AMI) with prior digestive system disease are more likely to suffer from gastrointestinal (GI) bleeding than those without these diseases. However, few articles reported how the different conditions of the digestive tract produced different risks of GI bleeding.
Methods: A single-center study on 7464 patients admitted for AMI from December 2010 to June 2019 in the Beijing Chaoyang Heart Center was retrospectively examined. Patients with major GI bleeding (n = 165) were compared with patients without (n = 7299). Univariate and multivariate logistic regression models were constructed to test the association between GI bleeding and prior diseases of the digestive tract, including gastroesophageal reflux disease, chronic gastritis, peptic ulcer, hepatic function damage, diseases of the colon and rectum, and gastroenterological tract tumors.
Results: Of the 7464 patients (mean age, 63.4; women, 25.6%; STEMI, 58.6%), 165 (2.2%) experienced major GI bleeding, and 1816 (24.3%) had a history of digestive system disease. The risk of GI bleeding was significantly associated with peptic ulcer (OR = 4.19, 95% CI: 1.86– 9.45) and gastroenterological tumor (OR = 2.74, 95% CI: 1.07– 7.04), indicated by multivariate logistic regression analysis.
Conclusion: Preexisting peptic ulcers and gastroenterological tract tumors rather than other digestive system diseases were indicators of gastrointestinal bleeding in patients with AMI who undergo standard antithrombotic treatment during hospitalization.
Keywords: gastrointestinal bleeding, digestive system disease, acute myocardial infarction, peptic ulcer, gastroenterological tract tumor
Introduction
Acute myocardial infarction is acute and persistent myocardial necrosis caused by ischemia and hypoxia of the coronary artery. The treatment of acute myocardial infarction (AMI) has concentrated on the recanalization of the culprit coronary artery and the prevention or minimization of ischemic complications with antithrombotic treatments and catheter-based interventions.1–3 Many reviews recognize that antithrombotic treatment or primary PCI for patients with AMI has been supplemented with an increased risk of bleeding,4,5 and this adverse occurrence is correlated with a significant impact on clinical outcomes.6,7 Previous studies reported that the gastrointestinal (GI) tract was the most common organ source of hemorrhage compared with any other part of the body, with an incidence of 31.5–70%.8–13 Previous studies also recognize that the risk of GI bleeding converged on specific diathesis as the history of GI bleeding, anticoagulant therapy, chronic non-steroidal anti-inflammatory drugs/corticosteroid (NSAIDs) user, and ≥2 or more of the following: Age ≥65, dyspepsia, gastroesophageal reflux disease (GERD), H. pylori infection, and chronic alcohol use.14,15
In 1992, Beijing Chaoyang Hospital developed the first PCI center in China. It has collected one of the largest AMI data sets to reflect regional patient characteristics. The Statistical Department of the Beijing Chaoyang Hospital also provided the consecutive diagnostic information of patients with AMI. In this retrospective study, we proposed that different digestive system diseases have a diverse impact on in-hospital GI bleeding in patients with AMI undergoing standard antithrombotic treatment.
Patients and Methods
Study Population
A single-center cohort of 7464 cases admitted for AMI from December 2010 to June 2019 in the Beijing Chaoyang Heart Center was retrospectively examined. The clinical diagnosis of coronary and digestive system disease included ST-segment elevation myocardial infarction (STEMI, I21, and I23), non-ST-segment elevation myocardial infarction (NSTEMI, I21, and I23), hemorrhage of the digestive tract (K27.404, K92.204, K92.207, and K92.208), and reflux esophagitis (RK21), reflux gastritis (RG, K29.701), chronic gastritis (CG, K29.502), peptic ulcer (PU, DA61), colitis and polyp of the colon (K51, K63), hepatic function damage (R94, K72, K71, K76), and gastroenterological tract tumor (GT, Z85, D37). In this study, the Statistical Department of the Beijing Chaoyang Hospital provided all the information on patients with AMI, according to the medical records during an 8.5-year screening span, except for names and addresses, which were confidential. The Department of Pharmacy of the Beijing Chaoyang Hospital provided all the medication information. Dual antiplatelet therapy (DAPT) was used at admission for all subjects unless contraindications existed.
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University (NO.2019-5-1). Participant informed consent was not obtained because the study involved using patient data that were anonymized before the research team received it.
We classified the irregular digestive system disease of the cases into six types: 1. GERD; 2. Chronic gastritis (CG); 3. Peptic ulcer (PU); 4. New diagnosis of hepatic function damage (HFD); 5. Disease of the colon and rectum (DCR); and 6. Gastroenterological tract tumor (GET). HFD was named as both alanine aminotransferase (ALT) and aspartate aminotransferase (AST) exceeding the upper normal value by 3, and an ALT/AST of >1.1. Patients with major GI bleeding (n = 165) were compared with those without (n = 7299), and the association between major GI bleeding and the six types of digestive system disease was examined. In our study, patients diagnosed with CG, GERD, GI tract tumor, or disease of the DCR were confirmed by the prior endoscopic examinations and not current admission.
The Main Observation Indicators and Definitions
We defined major bleeding using an adjustment of the International Society on Thrombosis and Hemostasis definition.9 This included fatal bleeding, hemodynamic instability and the need for a transfusion, symptomatic bleeding into adjusting the regime of antiplatelet therapy, bleeding in a critical organ, bleeding in a surgical site requiring reoperation, and bleeding leading to unplanned and prolonged hospitalization. Major GI bleeding was defined as major bleeding in the gastroenterological tracts such as the esophagus, stomach, duodenum, small intestine, colon, and rectum. Any bleeding that did not meet the definition for major bleeding was defined as minor and not considered an endpoint occurrence.
Statistical Analyses
The analyses were performed using SPSS software, version 26 (IBM SPSS Statistics 26.0). The continuous variables of normal distribution were expressed as mean ± standard deviation, the continuous variables of non-normal distribution were expressed as median (interquartile range [IQR]), and the categorical variables were expressed as frequency (percentage [%]). Univariate logistic regression analysis (p < 0.05) and then multivariate stepwise logistic regression analysis were performed. We assessed the association between major GI bleeding (GIB) and six types of digestive system diseases using logistic regression models. The GI bleeding occurrence was modeled as a dependent variable and digestive system disease as covariates. A two-sided value of P < 0.05 was considered statistically significant.
Results
The Baseline Characteristics
A total of 7464 patients were enrolled, including patients with STEMI (n = 4205) and NSTEMI (n = 3259). Of the 7464 patients, 232 (3.1%) experienced serious bleeding and underwent a modified anticoagulation regime. Among the 232 cases of bleeding in patients, 165 (2.2%) occurred in the gastroenterological tracts and 67 (0.9%) in sites other than the peptic system, including intracranial bleeding (n = 32), subarachnoid hemorrhage (n = 3), fundus hemorrhage (n = 7), nasal hemorrhage (n = 3), urinary tract bleeding (n = 17), retroperitoneal hemorrhage (n = 3), and postoperative hemorrhage (n = 2). Among the 165 patients with GI bleeding, 37 (22.4%) were diagnosed with stress ulcers.
When we compared the baseline characteristics of the 165 patients who experienced in-hospital major GI bleeding and the 7299 patients who did not, we found that both groups had a similar age distribution and gender ratios, with no significant differences. The former was more likely to have a history of diabetes mellitus and renal dysfunction. These patients also had a higher incidence of pulmonary edema (Killip 3) and cardiogenic shock (Killip 4). Patients with major GI bleeding were more likely to have a history of digestive tract diseases. The details are presented in Table 1.
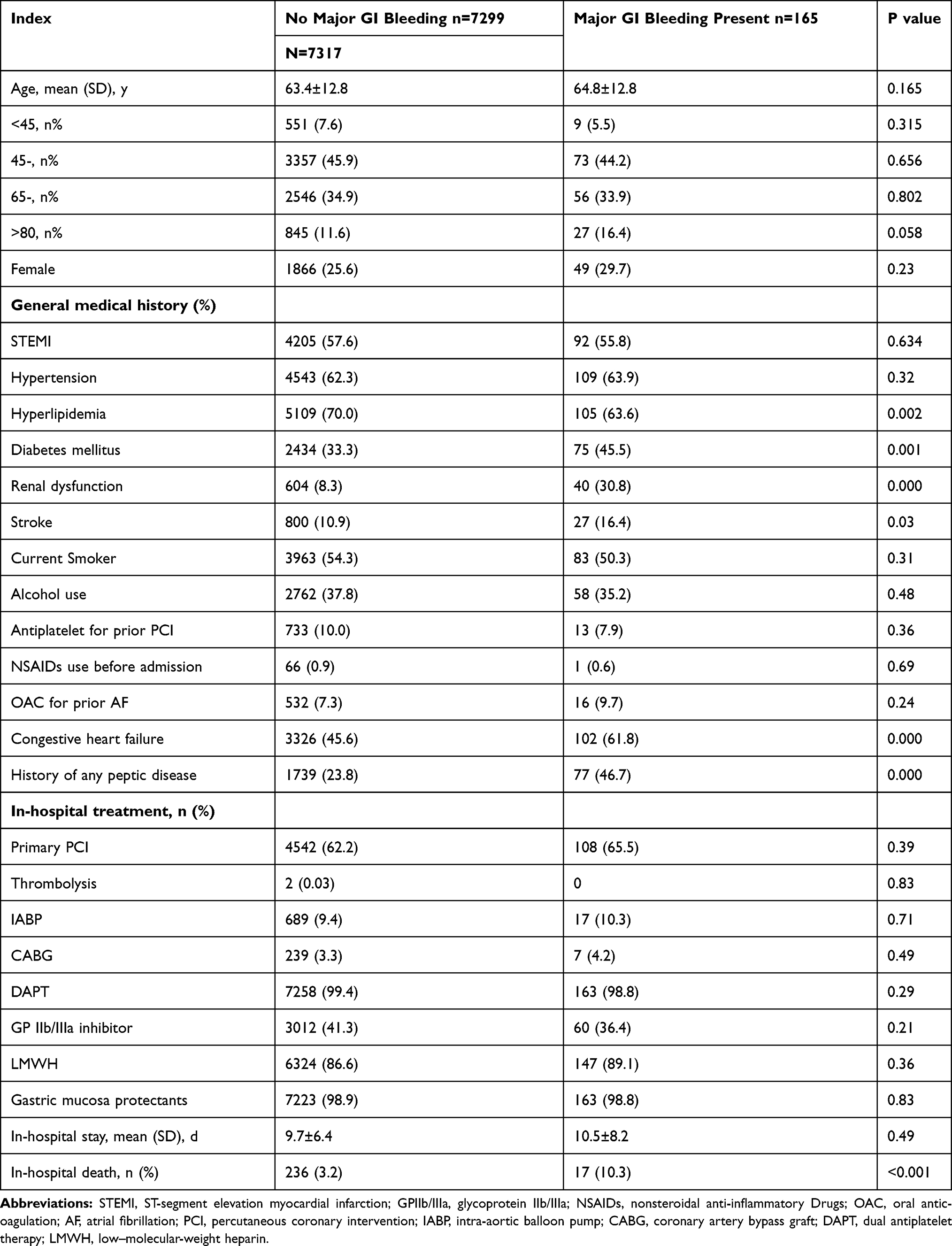 |
Table 1 Baseline Characteristics |
A History of Digestive System Disease
Of the 7464 patients, 1816 (24.3%) had a history of one or more of the six types of digestive system disease. Of these 1816 patients, 268 had a history of peptic reflux diseases, including reflux esophagi (RK21, n = 265) and reflux gastritis (K29.701, n = 3); 554 had a history of CG, including chronic gastritis (K29.500 and K29.502, n = 504), chronic superficial gastritis (K29.300 and K29.303, n = 33), and chronic atrophic gastritis (K29.401 and K29.451, n = 17); 294 had a history of peptic ulcers, including gastric ulcers (K25, n = 125), duodenal ulcers (K26, n = 107), peptic ulcers (K27, n = 48), and complex ulcers (K27.900, K27.901, K27.902, n = 14); 662 had a history of a new diagnosis of hepatic function (HFD), including hepatic function damage (R94.500, R94.501, n = 592), hypohepatia (K72.905, K76.806, n = 66), and hepatic failure (K72.001, K72.901, n = 4); 88 had a history of colon and rectum diseases, including ulcerative colitis (K51, n = 8), polyps of the colon (K63, n = 9), chordapsus (K51.904, K51.905, n = 27), and hemorrhoids (184.101, 184.102, 184.152, 184.202, 184.154, n = 44); 66 had a history of gastroenterological tumors, including esophagus cancer (Z85.051, n = 5), gastric cancer (D37.101, D37.203, C16.906, n = 18), gastric cardia cancer (D37.103, n = 2), duodenum tumors (D37.203, n = 2), colon tumors (D37.401, D37.403, D37.405, D37.407, D45.411, D45.414, n = 25), and rectum tumors (D37.501, 48.351, n = 14). Of the 1816 patients, 1601 (88.2%) had one type of peptic disease, 205 (11.3%) had two types, nine (0.5%) had three types, and one (0.06%) had four types. None of the patients exceeded five types.
The Association Between In-Hospital Major GI Bleeding and the Diagnosis of Digestive System Disease
Logistic regression was performed with whether GI bleeding was the dependent variable and six types of gastroenterological diseases as covariates. There were significant correlations between in-hospital major GI bleeding with peptic ulcers (OR = 4.19, 95% CI: 1.86–9.45) and gastroenterological tumors (OR = 2.74, 95% CI: 1.07–7.04). There were no significant correlations between in-hospital major GI bleeding with diseases of the colon and rectum (OR = 0.68, 95% CI: 0.24–1.97); neither with CG (OR = 0.59, 95% CI: 0.31–1.14) nor HFD (OR = 0.66, 95% CI: 0.35–1.24) nor GERD (OR = 0.34, 95% CI: 0.11–1.09) (Table 2).
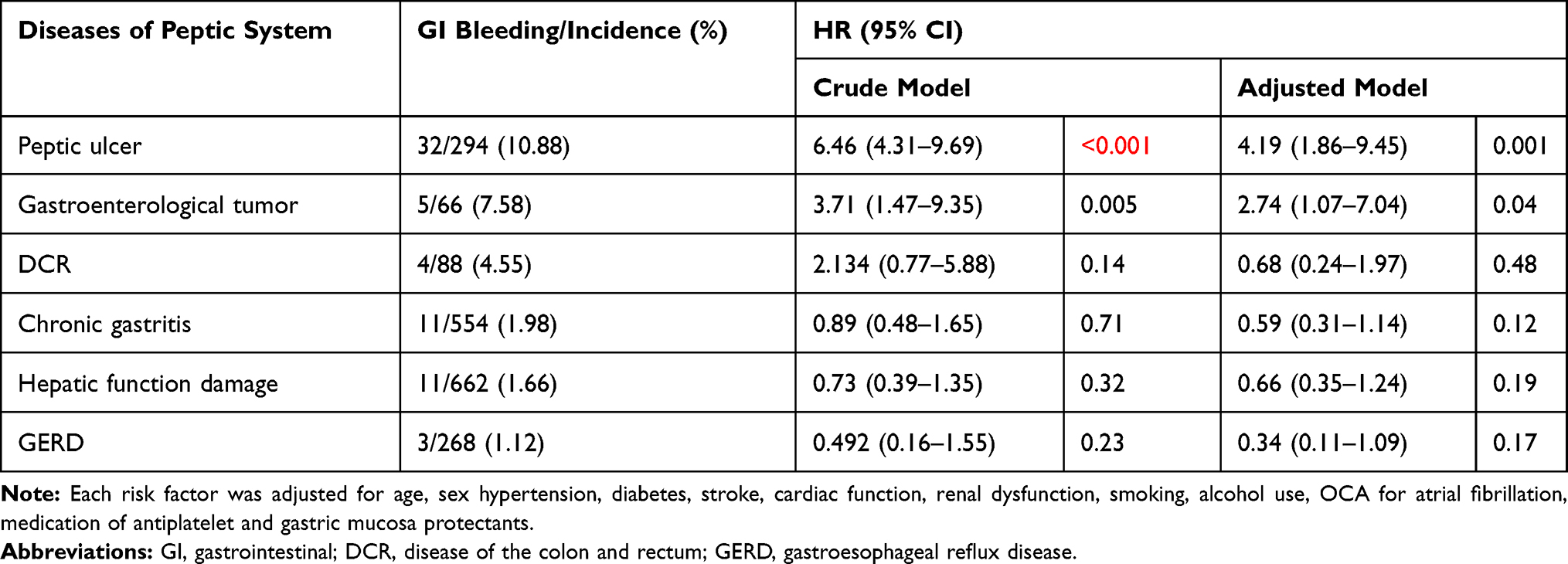 |
Table 2 The Crude and the Adjusted Relationship Between In-Hospital Major GI Bleeding and Prior Peptic Diseases |
Discussion
In our study, 1816/7464 (24.3%) of the patients admitted with AMI had accompanying digestive system diseases. Among these patients, 1601 (88.2%) had one type of digestive system disease and 215 (11.8%) had two or more types, as defined. The results of the diseases were as follows: HFD (36.5%, n = 662), CG (90.3%, n = 551), peptic ulcer (17.2%, n = 294), GERD (14.7%, n = 268), DCR (4.8%, n = 88), and gastroenterological tumor (3.6%, n = 66).
All 232 (3.1%) of the patients who experienced major bleeding had to stop one of the antiplatelet medications, including aspirin and clopidogrel, during hospitalization. The GP IIb/IIIa inhibitor and LMWH were discontinued before aspirin or clopidogrel. Of the 232 patients, 165 (71.1%) had major bleeding events in the GI tract, and 132 of the 165 (80%) had bleeding in the upper gastrointestinal tracts. The incidence of major GI bleeding in patients with a history of any peptic disease is significantly higher than those without (46.7% vs 23.8%, P < 0.001). However, not all preexisting digestive system diseases are linked with AMI in-hospital major GI bleeding. In our study, we tested the six most common conditions in clinical settings. We found that history of peptic ulcer and gastroenterological tract tumors were indicators of gastrointestinal bleeding in patients with AMI who underwent standard antiplatelet treatment during hospitalization, rather than those with other types of digestive system disease. When we restricted our analysis to a concrete diagnosis of digestive system disease, peptic ulcers were associated with a 4.19-fold higher hazard for GI bleeding, and gastroenterological tumors were associated with a 2.74-fold higher hazard for GI bleeding. In our logistic model, preexisting GERD, CG, and diseases of the colon and rectum did not present a close association with in-hospital major GI bleeding.
In this study, we also found in-hospital deaths in the GI bleeding group were significantly higher than those without GI diseases. The GI bleeding group had a higher proportion of congestive heart failure, diabetes mellitus, renal dysfunction, and stroke. All these risk factors, together with GI bleeding, increased the AMI mortality, as had been pointed out by previous guidelines.1,2
Many factors increase the major GI bleeding for patients with AMI (eg, age, sex, renal disease, liver disease, active cancer, stroke, prior bleeding, smoking, alcohol intake, DAPT, and oral anticoagulants [OAC] use).16 The mixed features constitute the individual bleeding diathesis.17 We compared the baseline characteristics and found that the proportion of the treatment of primary PCI, CABG, and long- and short-term medication in the two groups was similar. These medications included NSAIDs, OAC before admission, aspirin, P2Y12 receptor inhibitors, LMWH, GP IIb/IIIa receptor inhibitors, gastric mucosa protectants including PPI, and H2RA after admission. Therefore, the different in-hospital major GI bleeding between the two groups is caused by reasons other than medication.
In our study, we found that the use of gastric mucosa protectants was over 98%, which reflects that patients with AMI may have been overusing this type of medication in the past 8.5 years. Our study helps to distinguish patients at stratified risk with a history of digestive tract diseases. For low-risk patients, the use of gastric mucosal protectants should be meticulous.18,19
HFD in some patients was preexisting. A large part of the associated pathological morbidity developed with the AMI process,20 particularly in cases accompanied by right ventricle infarction and subsequent hepatic congestion.21 This pathological morbidity often recovered after the treatment of congestive right ventricle failure. Our study did not identify a strong and specific association between major GI bleeding and HFD.22,23
In this retrospective clinical data analysis, we found that for patients with AMI who were admitted to hospital, preexisting peptic ulcers and gastroenterological tract tumors were indicators of major gastrointestinal bleeding that required a change in the therapeutic strategy of antiplatelet drugs. However, GERD and CG did not lead to major GI bleeding, even though a high incidence rate was present.24
This study had several limitations. First, it was retrospective. We found that several digestive system diseases could indicate major GI bleeding, but this needs to be tested further by a randomized control trial. Second, there is evidence that Helicobacter pylori (HP) infection is a risk factor for GI bleeding. We did not test the association between GI bleeding and HP infection since the carbon 13 urea breath test was not a routine lab test for patients with AMI in our hospital. However, previous studies showed that the incidence of HP infection is high in Chinese people. Therefore, the potential association between GI bleeding and HP infection also needs to be tested by a randomized control trial. Third, few patients underwent endoscopy examinations unless an urgent need arose during their hospitalization. Endoscopy was avoided due to complications such as aggravating heart failure and gastrointestinal mechanical injury.
Conclusions
Preexisting peptic ulcers and gastroenterological tract tumors, rather than other digestive system diseases, are indicators of gastrointestinal bleeding among patients with AMI who undergo typical antiplatelet treatment during hospitalization.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University (NO.2019-5-1). Participant informed consent was not obtained because the study involved using patient data that were anonymized before the research team received it.
Consent for Publication
Participant informed consent was not obtained because the study involved using patient data that were anonymized before the research team received it.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Funding
This study was funded by the Beijing Municipal Administration of Hospitals Digest Collaborative Center major project (XXZ0607) and National Key R&D Program of China (2016 YFC1301102). The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declare that they have no competing interests.
References
1. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. doi:10.1093/eurheartj/ehx393
2. Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:267–315. doi:10.1093/eurheartj/ehv320
3. Aslanabadia N, Safaiea N, Talebib F, Dousti S, Entezari-Maleki T. The streptokinase therapy complications and its associated risk factors in patients with acute ST elevation myocardial infarction. Iran J Pharm Res. 2018;17:53–63.
4. Desai NR, Kennedy KF, Cohen DJ, et al. Contemporary risk model for inhospital major bleeding for patients with acute myocardial infarction: the acute coronary treatment and intervention outcomes network (ACTION) registry?–Get With The Guidelines (GWTG)? Am Heart J. 2017;194:16–24. doi:10.1016/j.ahj.2017.08.004
5. Ameloot K, Daemen J, Mieghem N. PCI strategies in acute myocardial infarction with cardiogenic shock. N Engl J Med. 2018;378:1360–1361.
6. Attar R, Wester A, Koul S, Eggert S, Andell P. Peripheral artery disease and outcomes in patients with acute myocardial infarction. Open Heart. 2019;6:e001004. doi:10.1136/openhrt-2018-001004
7. Ndrepepa G, Schuster T, Hadamitzky M, et al. Validation of the bleeding Academic Research Consortium Definition of bleeding in Patients With Coronary Artery Disease Undergoing Percutaneous Coronary Intervention. Circulation. 2012;125:1424–1431. doi:10.1161/CIRCULATIONAHA.111.060871
8. Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med. 2006;355:2203–2216. doi:10.1056/NEJMoa062437
9. Kaatz S, Ahmad D, Spyropoulos AC, Schulman S. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in nonsurgical patients: communication from the SSC of the ISTH. J Thromb Haemost. 2015;13:2119–2126. doi:10.1111/jth.13140
10. Rao SV, O’Grady K, Pieper KS, et al. Impact of bleeding severity on clinical outcomes among patients with acute coronary syndromes. Am J Cardiol. 2005;96:1200–1206. doi:10.1016/j.amjcard.2005.06.056
11. Rao SV, Eikelboom JA, Granger CB, Harrington RA, Califf RM, Bassand J. bleeding and blood transfusion issues in patients with non–ST segment elevation acute coronary syndromes. Eur Heart J. 2007;28:1193–1204. doi:10.1093/eurheartj/ehm019
12. Spencer FA, Moscucci M, Granger CB, et al.; GRACE Investigators. Does comorbidity account for the excess mortality in patients with major bleeding in acute myocardial infarction? Circulation. 116;2007:2793–2801. doi:10.1161/CIRCULATIONAHA.107.694273
13. Ng FH, Lam KF, Wong SY, et al. Upper gastrointestinal bleeding in patients with aspirin and clopidogrel co-therapy. Digestion. 2008;77:173–177. doi:10.1159/000141264
14. Costa F, Tijssen JG, Ariotti S, et al. Incremental value of the CRUSADE, ACUITY, and HAS-BLED risk scores for the prediction of hemorrhagic events after coronary stent implantation in patients undergoing long or short duration of dual antiplatelet therapy. J Am Heart Assoc. 2015;4:
15. Agewall S, Cattaneo M, Collet JP, et al.; ESC Working Group on Cardiovascular Pharmacology and Drug Therapy and ESC Working Group on Thrombosis. Expert position paper on the use of proton pump inhibitors in patients with cardiovascular disease and antithrombotic therapy. Eur Heart J. 2013;34:
16. Urban P. Defining High bleeding Risk in Patients Undergoing Percutaneous Coronary Intervention. A Consensus Document From the Academic Research Consortium for High bleeding Risk. Circulation. 2019;140:240–261. doi:10.1161/CIRCULATIONAHA.119.040167
17. Chhatriwalla AK, Amin AP, Kennedy KF, et al. Association between bleeding events and in-hospital mortality after percutaneous coronary intervention. JAMA. 2013;309(10):1022–1029. doi:10.1001/jama.2013.1556
18. Krag M, Perner A, Wetterslev J, et al. Prevalence and outcome of gastrointestinal bleeding and use of acid suppressants in acutely ill adult intensive care patients. Intensive Care Med. 2015;41:833–845. doi:10.1007/s00134-015-3725-1
19. Wang Y, Ye ZK, Ge L, et al. Efficacy and safety of gastrointestinal bleeding prophylaxis in critically ill patients: systematic review and network meta-analysis. Br Med J. 2020;368:1–12.
20. Hasanzadehmoghadam M, Khademansari MH, Farjah GH, et al. Hepatoprotective effects of betaine on liver damages followed by myocardial infarction. Vet Res Forum. 2018;9:129–135. doi:10.30466/vrf.2018.30834
21. Guo RQ, Song CF. Two-dimension speckle tracking assessment of right ventricle in patients with acute inferior myocardial infarction and after PCI. Ultrasound Med Biol. 2013;39:S6. doi:10.1016/j.ultrasmedbio.2013.02.045
22. Lofthus DM, Stevens SR, Armstrong PW, et al. Pattern of liver enzyme elevations in acute ST-elevation myocardial infarction. Coron Artery Dis. 2012;23:22–30. doi:10.1097/MCA.0b013e32834e4ef1
23. Alexander M, Loomis AK, van der Lei J, et al. Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: findings from matched cohort study of 18 million European adults. BMJ. 2019;367:l5367. doi:10.1136/bmj.l5367
24. Keskin M, Hayıroğlu Mİ, Uzun AO, et al. Effect of nonalcoholic fatty liver disease on in-hospital and long-term outcomes in patients with ST-segment elevation myocardial infarction. Am J Cardiol. 2017;120:1720–1726. doi:10.1016/j.amjcard.2017.07.107
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.