")
Back to Journals » Cancer Management and Research » Volume 10
Impact of physical activity and sleep quality on quality of life of rural residents with and without a history of cancer: findings of the Day and Night Study
Authors Rafie C , Ning Y, Wang A, Gao X, Houlihan R
Received 21 December 2017
Accepted for publication 1 May 2018
Published 9 November 2018 Volume 2018:10 Pages 5525—5535
DOI https://doi.org/10.2147/CMAR.S160481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Leylah Drusbosky
Carlin Rafie,1,* Yi Ning,2,* Aiping Wang,3 Xiang Gao,4 Robert Houlihan4,5
1Department of Human Nutrition, Foods, and Exercise, Virginia Polytechnic Institute and State University, Blacksburg, VA, USA; 2GlaxoSmithKline Institute of Infectious Disease and Public Health, Beijing, China; 3Apex Life Science, Richmond, VA, USA; 4Department of Nutritional Sciences, Pennsylvania State University, University Park, PA, USA; 5UF Health Cancer Center, University of Florida, Gainesville, FL, USA
*These authors contributed equally to this work
Background: Lifestyle behaviors may impact quality of life (QoL). The relative impact of physical activity and sleep quality on QoL of individuals with and without a history of cancer living in underserved rural communities requires further study to inform health care and public health initiatives.
Methods: Individuals with and without a history of cancer were recruited from rural Virginia. We collected information on physical activity level (PAL), sleep quality (Pittsburgh Sleep Quality Index), and QoL (Short Form-36). Additional dimensions of physical activity and sleep were measured including ambient light exposure and sleep duration via Actiwatch2, and serum vitamin D and urine melatonin, which are markers of outdoor activity and sleep.
Results: A total of 124 cancer survivors and 48 cancer-free individuals were enrolled in the study. Mean age was 59 years, with the majority being women (89%) and Caucasian (76%). Breast cancer was the most common cancer (72%), and mean time from diagnosis to the survey was 8.1 years. Survivors were significantly less active, more likely to be inactive, and had significantly worse sleep quality and physical and mental health relative to cancer-free individuals (P<0.05). Quality of sleep and average sleep time were associated with physical (r=−0.371, P<0.001; r=−0.327, P<0.000) and mental health (r=−0.442, P=<0.001; r=−0.265, P<0.004), as was PAL (r=0.181, P=0.019; r=0.288, P=0.003). Self-reported outdoor activity was associated with mental health (r=0.233, P=0.003) and vitamin D3 (r=0.193, P=0.015). No association was found between melatonin, sleep quality, and QoL. Sleep quality, cancer status, body mass index, and sleep time were predictive of physical health, while sleep quality, sleep time, and outdoor activity were predictive of mental health.
Conclusion: Quality of sleep is a significant predictor of mental and physical health, and important for cancer survivors who experience poorer QoL. Outdoor activity should be encouraged to improve mental health and vitamin D status, and interventions to improve sleep for those with poor sleep quality should be considered in cancer survivorship planning.
Keywords: cancer survivor, quality of life, physical health, mental health, quality of sleep, rural health, survivorship, Actiwatch 2
Introduction
Advances in early cancer detection and treatment have resulted in a steady increase in cancer survival rates.1 The prevalence of cancer survivors in the United States has increased fourfold since 1971, with an expected 20.3 million cancer survivors by 2026.2–4 Substantial epidemiologic and experimental evidence supports the pivotal role of diet and lifestyle in the development and progression of cancer.5 Adherence to healthy lifestyle recommendations including regular exercise, weight maintenance, and a healthy dietary pattern is recommended to reduce cancer risk and improve cancer outcomes and survival.6,7 For cancer survivors, the negative physical and psychological impacts from their disease and its treatment including pain, fatigue, decreased function, anxiety, depression, and cognitive problems has a significant impact on their quality of life (QoL).8–12 As cancer survivors and advocates make their need for posttreatment psychosocial and medical care known, promotion of healthy lifestyles is being recognized as an essential part of cancer survivorship care.13,14
Physical activity is a modifiable lifestyle behavior that has positive physiologic and psychologic health outcomes in cancer survivors.15 It is associated with reduced cancer recurrence and all-cause mortality, as well as improvements in QoL, particularly reported for research of breast cancer and colorectal cancer.16–18 Despite this, it is estimated that <30% of cancer survivors achieve the physical activity recommendations for cancer survivors of the American College of Sports Medicine.19,20 A growing body of evidence implicates the time in sedentary activities as important to health and cancer outcomes, as well.21
Sleep quality is a significant issue for cancer survivors, as well, and is potentially modifiable through lifestyle interventions. Poor sleep quality has been linked to greater fatigue, lower QoL, and poorer clinical outcomes in cancer survivors.22–25 Initial evidence indicates that interventions with cancer patients including physical activity, cognitive behavioral therapy, and mind–body interventions have moderate effectiveness in improving sleep measures and QoL.26
Rural communities have disparities in health care access and health outcomes. In Virginia, the largely rural south and southwest counties have higher cancer mortality rates than the state average. For example, the southwest health districts of Cumberland Plateau and Lenowisco have an all cause cancer mortality rate of 204.8 and 212.4 per 100,000 compared to the state average of 171.2 per 100,000.27 Limited resources for a healthy diet and physical activity, and cultural lifestyle norms may partially explain this disparity.28 The study of lifestyle factors, including diet, physical activity, and sleep in rural cancer survivors are sparse, however. This study evaluated physical activity, and sleep quality among cancer survivors and controls from rural communities in southern Virginia, and investigated the association of lifestyle factors, including outdoor activity and sleep with QoL. In addition, the biomarkers vitamin D and melatonin were evaluated for their utility as surrogate measures of level of outdoor physical activity and sleep quality, respectively.
Materials and methods
A cross-sectional study was conducted to evaluate physical activity and sleep quality and QoL among cancer survivors and individuals without a cancer history. Individuals were recruited from seven rural communities in Southwest and Southern Virginia through collaborative agreements with four hospitals and their oncology practices and through broad multimedia advertising in newspapers and through radio ads in the seven communities. The southwest county where recruitment occurred is in the Appalachian region with a predominantly White population (93%), while the six communities in the south-central region have populations ranging from 30% to 60% Black. All of the communities have lower educational attainment and higher poverty levels than the state average.29 The oncology practices conducted a retrospective review of records to identify patients who were qualified for the study and sent letters of invitation to all the qualified patients from the study team. Interested patients contacted the study team directly. All of the non-cancer patients responded to multimedia advertising, as did 35 cancer patients.
Participants were 18–85 years of age of both genders. Participants without a history of cancer could have no personal history of any cancer type. Cancer survivors could have a history of stage I, II, or III primary breast, colorectal, or prostate cancer and could have had concurrent malignancies only if they were of stage I or II. They must have been at least 6 months from the end of their primary treatment, but could be currently taking hormones or aromatase inhibitors. Individuals who had experienced a recurrence were eligible only if the recurrence was stage I or II. There was no maximum time since diagnosis. The study was approved by the Virginia Commonwealth University Institutional Review Board.
Assessment of exposures (physical activity and sleep quality)
Data on usual dietary intake, sleep quality, overall and outdoor physical activity, and QoL were collected through telephone interview. Standardized and validated surveys were used for this purpose including the Harvard Food Frequency Questionnaire (2007 grid),30 the Pittsburgh Sleep Quality Index (PSQI),31 a modified physical activity questionnaire,32,33 and the RAND 36-Item Health Survey 1.0.34 Demographics, medical history including diabetes and cardiovascular disease, and vitamin supplementation information were collected during the same phone interview.
Physical activity
Multidimensional information on physical activity was gathered through a survey and a wrist-mounted Actiwatch2. A previously described modified physical activity survey provided detailed information of physical activity and sedentary behavior,32 and duration of physical activity in a “typical week” including typical aerobic activities and lower intensity and resistance exercises was queried. The survey asked the usual walking pace outdoors and the number of flights of stairs climbed on a daily basis, followed by the average time per week spent in the past year in eleven different recreational activities (walking, jogging, running, bicycling, racquet games, swimming, aerobics, lower intensity and more vigorous activities, and arm and leg resistance exercises). The survey then queried the hours spent per week in the past year in five more sedentary activities including standing or walking at work and home, sitting or driving to work, sitting at home while watching TV, and while doing other activities.
Questionnaire data were used to calculate physical activity level (PAL) as described by Gerrior et al using metabolic equivalents (METS) from the compendium by Ainsworth et al.35,36 Physical activity was categorized into three categories as inactive (PAL 0.00–1.16), active (PAL 1.17–3.03), and very active (PAL ≥3.04) to evaluate the differences between cancer survivors and those without a history of cancer. These categories were further collapsed into binary groups, combining the active and very active group to look at differences in inactivity and similarly combining the inactive and active group to compare very active behavior. Average daily hours of outdoor activity and days of exercise per week was reported by participants on the physical activity questionnaire.
Ambient light exposure was collected using the Actiwatch2, an actigraphy-based data logger that records gross motor activity and white light exposure (Phillips Healthcare; Respironics Inc., Amesterdam, The Netherlands).37,38 Participants were required to wear the Actiwatch2 for 7 consecutive days and nights and to maintain a diary of times the Actiwatch2 was removed, nap time, bed time and sleep time, and wake time. Calculations of average white light exposure were made from the “daily” exposure data and adjusted according to the time that the Actiwatch2 was not worn which is indicated in the diary. Sleep time was calculated from the “sleep” data, and time to bed and rise recorded in the diary was compared to start and end times of the Actiwatch2 data to confirm concordance, and adjust as appropriate. Data were analyzed using the Actiware 5.0 software program (Respironics Inc.) and the default algorithm. Average daily minutes of white light exposure was generated and used as an estimate of outdoor activity.
Sleep quality
PSQI is a self-rated, validated questionnaire consisting of nine questions, which assesses sleep quality and disturbances over a 1-month period. The questions relate to aspects of sleep during the past month, and relate to sleep duration, disturbance, latency, efficiency, quality, and daytime dysfunction due to poor sleep. Usual bed time, time to fall asleep, wake time, and sleep time are asked in the first four questions. Sources and frequency of sleep disturbance is queried in the fifth, ten-part question, general quality of sleep in the sixth, the use of sleeping medication in the seventh, and impact of lack of sleep on wakefulness and enthusiasm in the last two questions. Sleep quality was scored following the method of Buysse et al.39 The composite sleep quality score has a possible range of 0 (best) to 21 (worst), with a score ≤5 associated with good sleep quality. Average hours of sleep was also calculated from the Actiwatch2.
Assessment of physical activity and sleep-related biomarkers (vitamin D and melatonin)
Participants provided fasting blood and first void morning urine samples at local laboratories contracted for this purpose. Serum 25-hydroxyvitamin D (D2 & D3), urinary 6-sulfatoxymelatonin (aMT6s), and creatinine (Cr) were measured by the University of Minnesota Department of Laboratory Medicine and Pathology. Liquid chromatography tandem mass spectrometry was used for the analysis of vitamin D.40 Urinary concentrations of 6-sulfatoxymelatonin were analyzed using an enzyme-linked immunosorbent assay (IBL International Corp., Toronto, ON, Canada). Urinary Cr was measured by a modified Jaffé method. Urinary 6-sulfatoxymelatonin has been widely used as an estimate of melatonin secretion, and first morning void urinary 6-sulfatoxymelatonin standardized to urinary Cr correlates well with cumulative nocturnal melatonin secretion and is an accurate estimation of nocturnal melatonin secretion.41,42 6-Sulfatoxymelatonin (aMT6s) was standardized to urinary Cr (ie, urinary aMT6s:Cr ratio) for analyses.
Dietary intake
A semi-quantitative, validated food frequency questionnaire, the Harvard Food Frequency Questionnaire, was used to evaluate the usual food and nutrient intake. Average daily calorie, macronutrient (protein, fat, and carbohydrate) and vitamin D intake, including vitamin D supplementation were determined.
Assessment of outcome (QoL)
QoL was evaluated using the RAND-36 Item Health Survey 1.0. The survey consists of 36 items that reflect eight health concepts related to physical health problems, role limitations due to personal or emotional problems, emotional well-being, social functioning, energy/fatigue, general health perception, and one question on change of health status. The first question asks the respondents to rate the health on a 5-point scale from excellent to poor. A series of ten questions ask about the level of limitation of specific physical activities due to health, with response options of “a lot,” “a little,” and “not limited.” Seven questions ask whether specific problems with work or regular activities occurred in the past 4 weeks due to physical and emotional problems, two questions ask about the extent to which physical or emotional problems interfered with social activities, two questions address issues of pain, and the remaining questions ask how often specific emotional and physical feelings occurred in the past 4 weeks. A scoring system consolidates the items into eight scales with scores ranging from 0 to 100 and a high score defining a more favorable health state. The eight scales are aggregated into two composite scores representing physical health and mental health.43
Assessment of potential confounders
The association between physical activity, sleep quality, and QoL was evaluated. The impact of cancer status and potential confounding effects of years since diagnosis, type of cancer, body mass index (BMI), diabetes, and cardiovascular disease were controlled for in multivariate analyses.
Data analysis
Descriptive statistics were used to compare demographic characteristics of cancer survivor and non-survivor study participants. Anthropometrics, dietary intake, physical activity, sleep quality, QoL, serum vitamin D, and urinary melatonin were compared between the two groups using Unpaired two-sample t-test for continuous data and chi-squared test for categorical data. To analyze for differences in relative inactivity, the active and very active categories were combined to form two physical activity categories. Data were evaluated for outliers and normality of distribution and transformed as appropriate. Nonparametric analyses were used for variables without normal distribution and for which transformation was not effective. Mental and physical health were squared; PSQI, physical activity (PAL), and self-reported outdoor physical activity were log10 transformed, and the square root of serum vitamin D3 was calculated to normalize these variables. Correlations were calculated to evaluate the associations between physical activity, sleep quality, and QoL. The associations between light exposure and outdoor physical activity with vitamin D, and sleep quality with urinary melatonin were also evaluated. The significance threshold was set at P<.05.
Linear regression models were constructed to evaluate the predictive value of factors showing a correlation at P<0.10 with the two constructs of QoL, that is, physical health and mental health, and to evaluate the impact of cancer status on these relationships. Age, gender, diabetes, and cardiovascular disease status were entered in both models, in addition to variables found to be confounders in these relationships. Variables with a probability of P≤0.05 were retained in the model.
Results
A total of 172 residents, 124 cancer survivors, and 48 cancer-free individuals were enrolled in the study. Participants were primarily female with a mean age of 59 years (range: 22–84 years). Survivors were significantly older than controls. Race, annual income, education level, and rates of diabetes and cardiovascular disease were not significantly different between the groups (Table 1). Breast cancer was the most prevalent cancer type in survivors (N=95), followed by colon cancer (N=13), prostate cancer (N=8), and lung cancer (N=5). Four participants had “other” cancer types. Twenty-one cancer survivors had been diagnosed with more than one cancer in their lifetime. Mean number of years since cancer diagnosis was 8.1 years (range: 1–49 years, median =5 years). All the participants had completed primary cancer treatment.
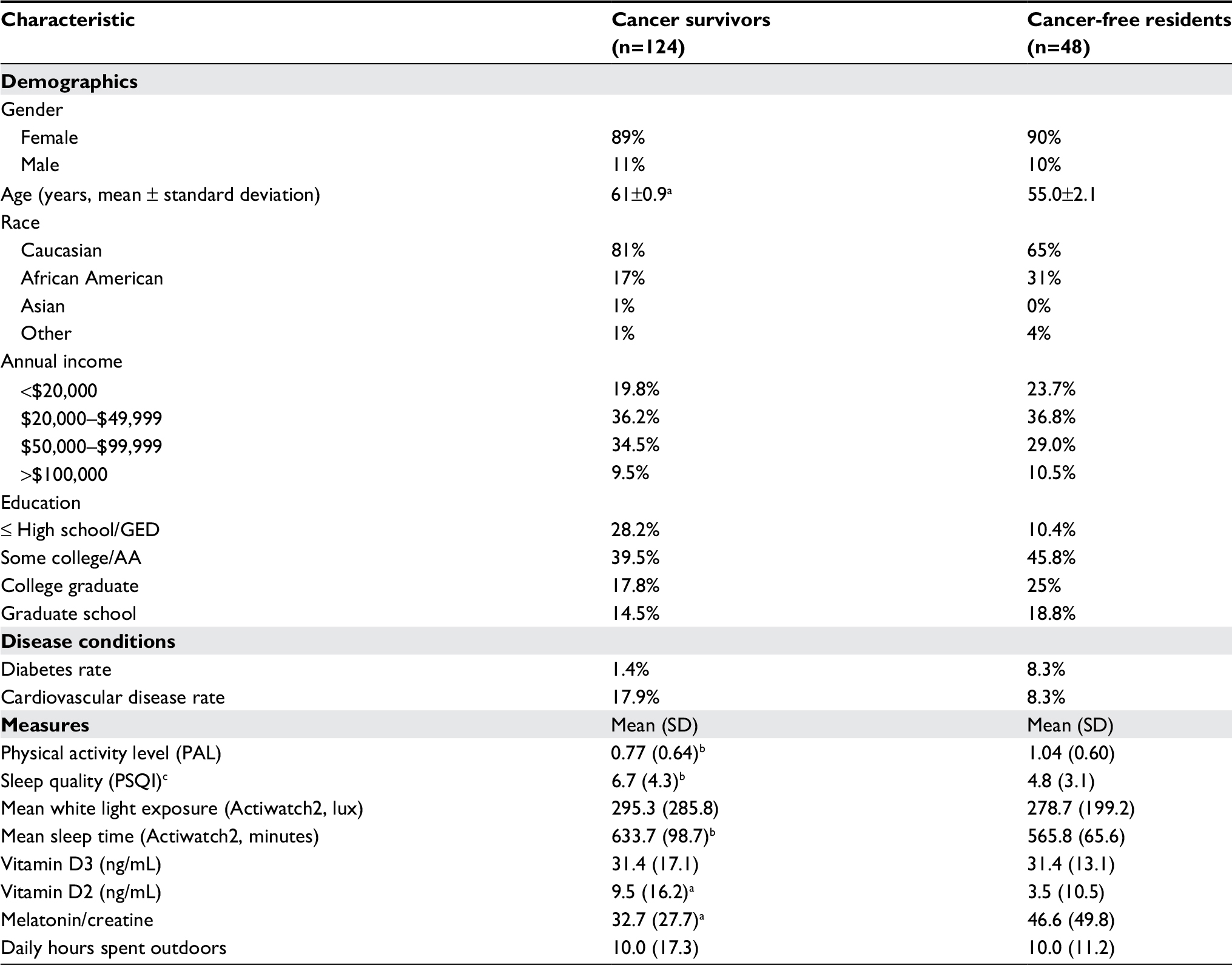 | Table 1 Characteristics of cancer survivors and cancer-free rural residents Notes: aSignificantly different at P<0.002. bSignificantly different at P<0.05. cHigher number signifies worse sleep quality. Abbreviation: PSQI, Pittsburgh Sleep Quality Index. |
Dietary intake results
Dietary intake of calories, protein, carbohydrate, fat, and % calories from fat were not statistically significantly different between cancer survivors and controls, nor was BMI. One hundred and three participants, 83 survivors and 20 controls, were taking vitamin D supplements. The frequency of supplementation was significantly higher for survivors (Pearson’s chi-squared 9.2, P=0.002). Dietary vitamin D intake was not different between survivors and controls; however, cancer survivors consumed a greater quantity of total vitamin D when supplemental vitamin D was included (738, SD=522 vs 565, SD=481 IU, P=0.062). Those taking supplements had significantly higher serum vitamin D2 (11.5, SD=1.80 vs 2.1, SD=0.76, ng/mL, Mann–Whitney U, P=0.011) and D3 (33.69, SD=1.88 vs 27.82, SD=1.30, ng/mL, Mann–Whitney U test, P=0.025).
Physical activity
PAL was significantly different between survivors and controls (Table 1, P=0.023). Cancer survivors were significantly more likely to be inactive compared to residents without a history of cancer (35.5% vs 12.5%, P=0.003) and were also significantly less likely to be very active (29.8% vs 47.9%, P=0.026) (Table 2). There was not a significant difference between survivors and controls for the survey question asking the average number of days of exercise per week.
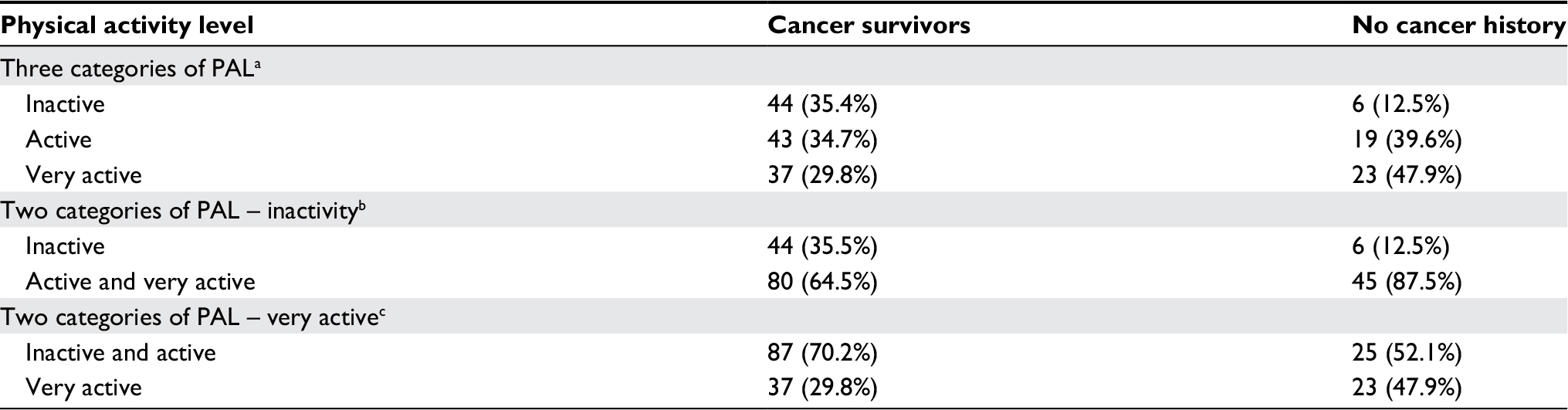 | Table 2 Comparison of categorical physical activity level (PAL) for cancer survivors versus residents with no history of cancer Notes: aPearson’s chi-squared test, df =2, P=0.008. bPearson’s chi-squared test, df =1, P=0.003. cPearson’s chi-squared test, df =1, P=0.026. |
Actiwatch2 data were collected from participants in all four seasons, with 61% of participants wearing the watch in the fall/winter, and 39% wearing the watch in the spring/summer. Participants contributed 816 days of data. Mean daily minutes of light exposure measured by the Actiwatch2 was not different between survivors and controls (295.3, SD =285.5 vs 278.7, SD =199.2; P=0.42). Serum vitamin D3 was not significantly different between the groups; however, serum vitamin D2 was significantly higher in cancer survivors (9.5, SD=1.23 vs 3.55, SD=10.54, ng/mL, I=0.02). However, this was true only for those taking vitamin D supplements. Neither serum vitamin D3 nor D2 were significantly associated with ambient light exposure measured with the Actiwatch2; however, self-reported average weekly hours of outdoor activity was associated with vitamin D3 (r=0.193, P=0.015).
Quality of sleep
Cancer survivors had significantly worse sleep quality compared to those cancer-free (6.73±4.31 vs 4.83±3.14, P=0.006), and urinary melatonin levels were significantly lower in cancer survivors (32.70±27.7 vs 46.6±49.80, ng/mL, P=0.02). Despite this, no significant associations were found between melatonin and sleep time, or quality of sleep, nor was melatonin significantly associated with physical or mental health. Average daily sleep time measured using the Actiwatch2 was significantly lower in cancer survivors, as well (Table 1)
QoL
Cancer survivors had significantly lower QoL scores compared to cancer-free individuals on six of the eight subscales, and the composite scores for physical and mental health (Table 3).
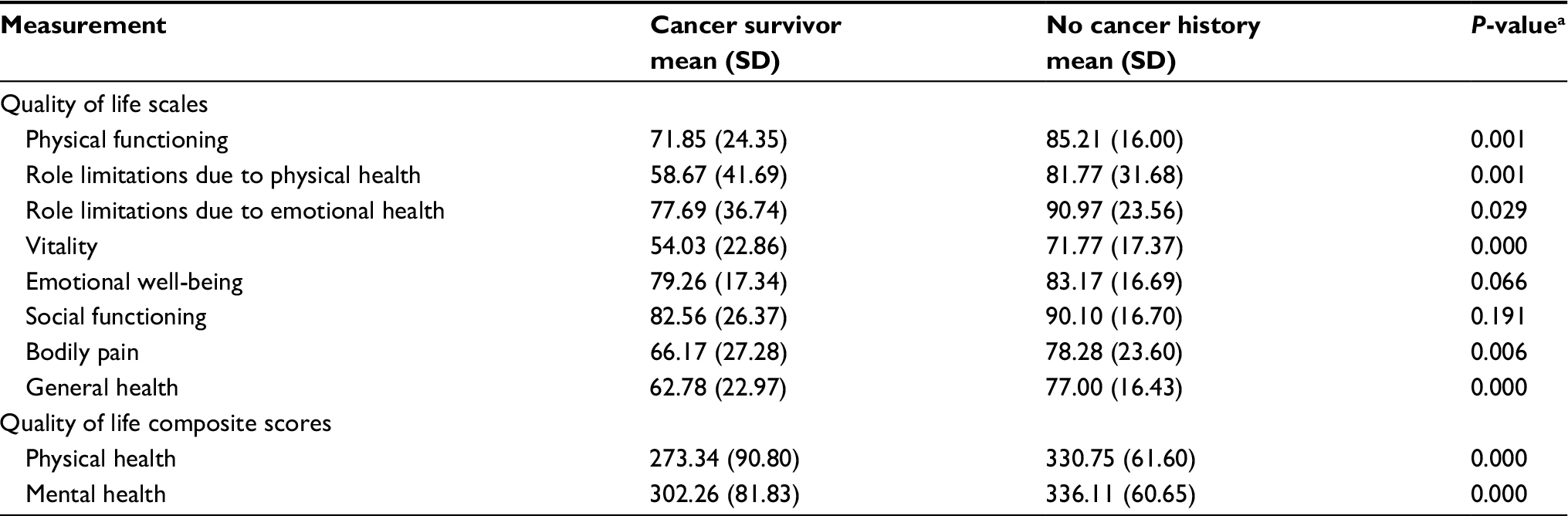 | Table 3 Comparison of quality of life between cancer survivors and cancer-free residents Notes: Significance threshold: P<.05. aMann–Whitney U test. |
Association between physical activity, sleep quality, and QoL
Physical activity (PAL) had significant positive associations with the QoL composite scores of physical and mental health (Table 4), as well as six of the eight QoL subscales (Table 5). When examined in cancer survivors alone, similar but weaker associations were found, with the exception of the association between PAL and role limitations due to physical health, which was stronger in cancer survivors. Self-reported average weekly hours of outdoor activity was significantly associated with mental health (Table 4).
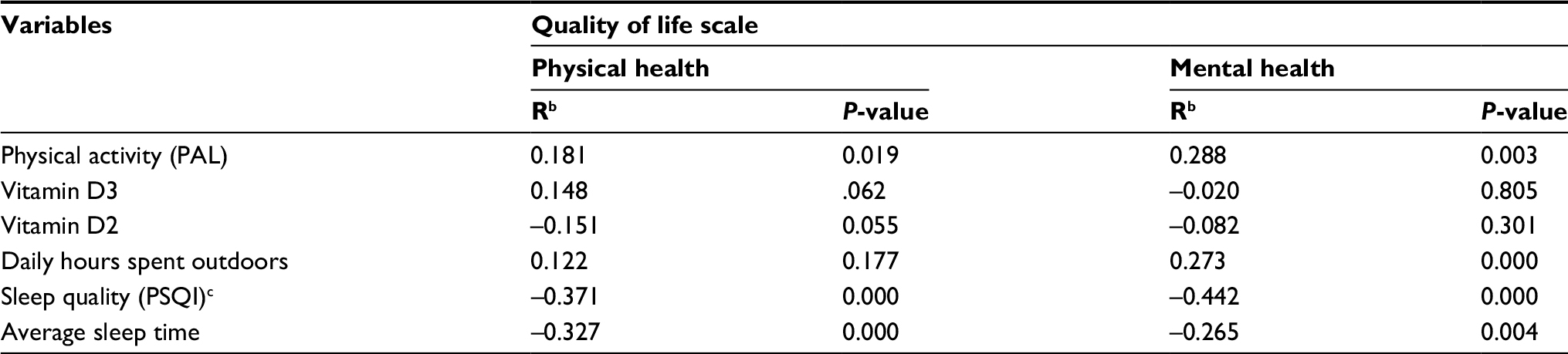 | Table 4 Relationship of physical activity and sleep quality to quality of lifea Notes: Significance threshold: P<.05. aSF-36 physical health and mental health summary scale. bPearson’s correlation coefficient. cSmaller value indicates better sleep quality. Abbreviations: PSQI, Pittsburgh Sleep Quality Index. |
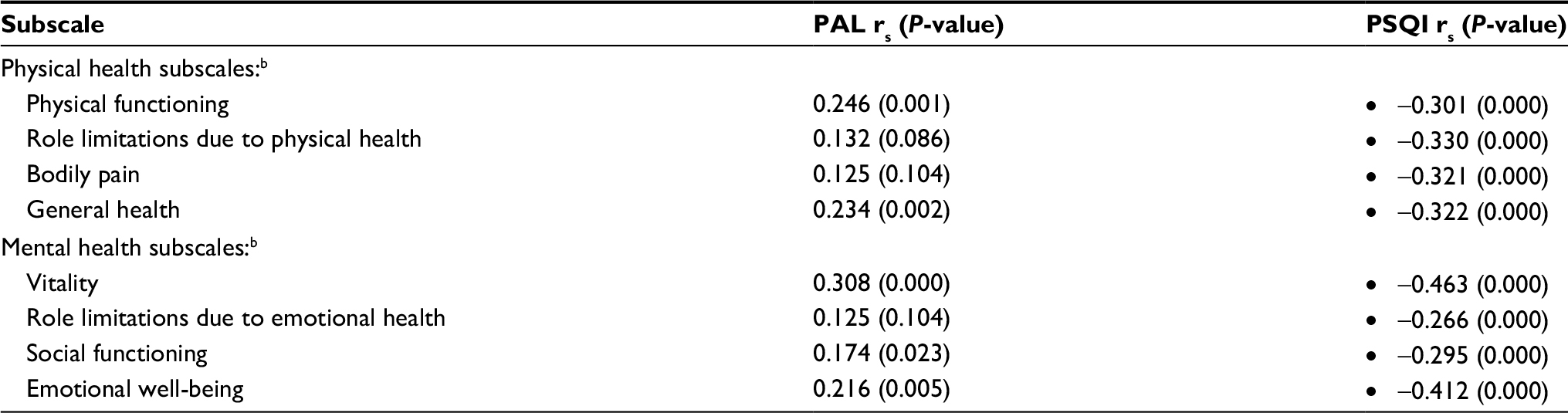 | Table 5 Correlation of quality of life subscalesa with physical activity and sleep quality Notes: Significance threshold: P<.05. aSF-36 physical health and mental health summary and subscales. bSpearman’s correlation coefficient. Abbreviations: PAL, physical activity level; PSQI, Pittsburgh Sleep Quality Index. |
Quality of sleep (PSQI) was strongly associated with both physical health and mental health. Lower values for PSQI were associated with better quality of sleep. The associations between PSQI and physical and mental health were strong inverse associations that were highly significant (Table 4). Strong inverse associations existed with all the sub-scales that make up physical and mental health in the full cohort, as well as in cancer survivors (Table 5).
There was no significant association between physical activity (PAL) and quality of sleep (PSQI). Serum vitamin D3 showed a positive relationship with physical health (r=0.148, P=0.062).
To evaluate the relative impact of cancer status, physical activity, and sleep quality on physical and mental health, as well as other factors found to be related to QoL, stepwise linear regression models were constructed. The predictability of physical health by physical activity (PAL), sleep quality (PSQI), cancer status, serum vitamin D3 and D2 and reported outdoor activity and the predictability of mental health by physical activity (PAL), sleep quality (PSQI), cancer status, reported outdoor physical activity, and sleep time were evaluated. Age, gender, diabetes, and cardiovascular disease were entered in both models, with the addition of BMI in the physical health model. The best fit model for physical health included sleep quality (PSQI), cancer status, BMI, and average sleep time and explained 29.7% of the variance (R2=0.326, F(4,92) =11.14, P=0.000). Sleep quality (PSQI), average sleep time, and BMI significantly predicted the physical health (β=–0.296, P=0.001; β=–0.212, P=0.021; β=–0.270, P=0.003, respectively), as did cancer status (β=0.171, P=0.050). Physical activity (β=0.105, P=0.254), diabetes status (β=0.166, P=0.071), self-reported outdoor activity (β=0.108, P=0.215), and serum vitamin D3 and D2 (β=0.118, P=0.172; β=−0.085, P=0.332) were non-significant contributors to the model and were excluded, as were age, gender, and cardiovascular disease (Table 6).
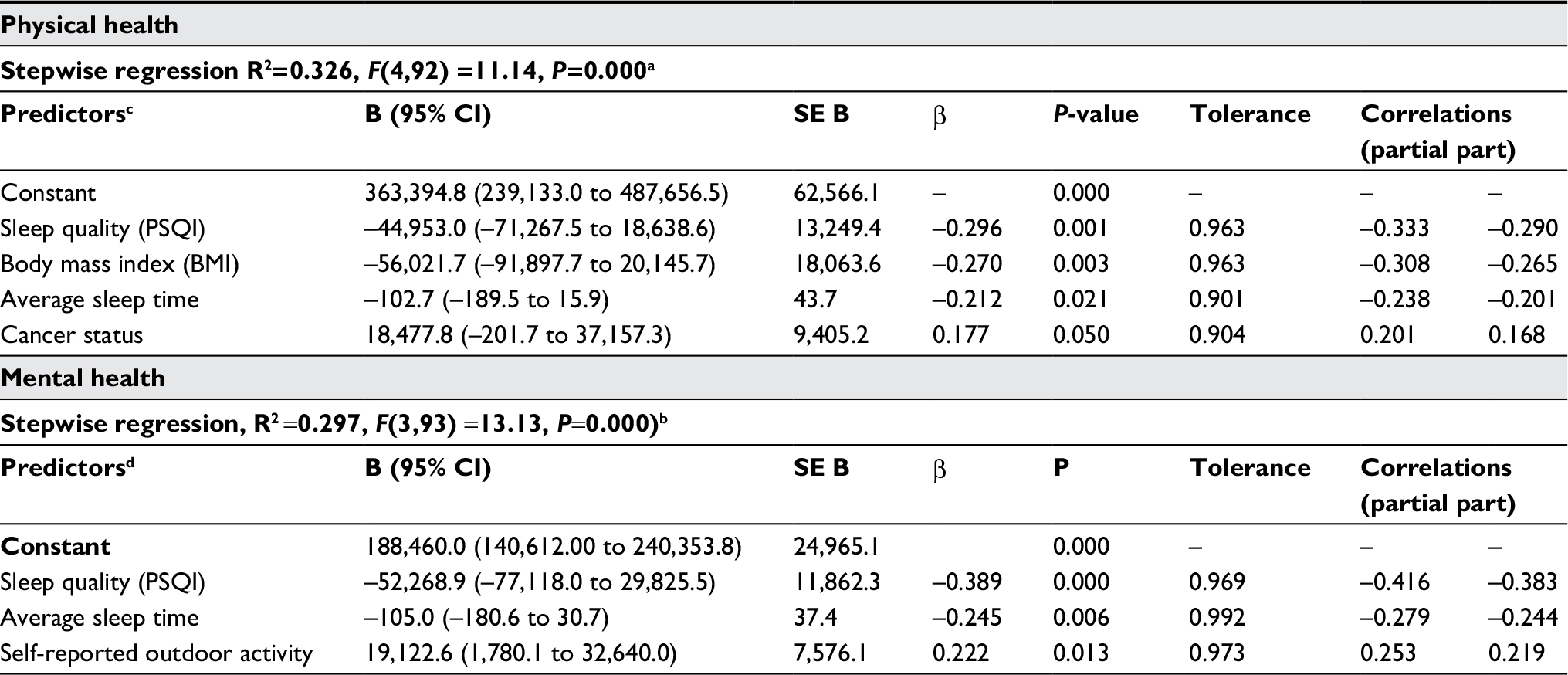 | Table 6 Stepwise regression models for physical health and mental health Notes: aDurbin Watson =1.81. bDurbin Watson = 2.15. cExcluded variables: PAL, vitamin D2 and D3, diabetes, gender, age, CVD. dExcluded variables: PAL, cancer status, diabetes, gender, age, CVD. Abbreviations: CVD, cardiovascular disease; PAL, physical activity level; PSQI, Pittsburgh Sleep Quality Index. |
The best fit model for mental health included only quality of sleep, average sleep time, and self-reported outdoor activity and explained 26.4% of the variance (R2 =0.287, F(3, 93) =12.47, P=0.000). Sleep quality and average sleep time significantly predicted mental health (β=–0.398, P=0.000; β=–0.246, P=0.006, respectively) as did self-reported outdoor activity ((β=0.196, P=0.029). Cancer status (β=0.102, P=0.274), physical activity (PAL) (β=0.097, P=0.312), and diabetes status (β=–0.009, P=0.920) were nonsignificant contributors and were excluded from the model, as were age, gender, and cardiovascular disease (Table 6).
Discussion
We evaluated factors impacting QoL in cancer survivors and cancer-free individuals living in relatively medically underserved rural communities. Cancer survivors had poorer physical and mental QoL, were less physically active, and had poorer quality of sleep. We found a strong relationship between quality of sleep and mental and physical health in this population. Conversely, the relationship between the level of physical activity and QoL was moderate and became insignificant when included in predictive models. Cancer status was predictive of physical health, along with sleep quality, sleep time, and BMI, but was not a significant predictor of mental health. As with physical health, sleep quality and sleep time were predictive of mental health, along with hours of outdoor activity.
The strong association between quality of sleep and both mental and physical health in cancer survivors highlights the potential to improve the QoL of cancer survivors through sleep interventions. Sleep disturbance is common in cancer survivors and is associated with fatigue, symptom burden, mood, and other factors that impact QoL.23,24,27 Sleep quality was associated with all of the subscales of mental and physical health in the cohort as a whole and in cancer survivors, each of which have implications for intervention. Multiple interventions have been tested and show promise to improve sleep quality in cancer survivors.26,27,44
Although we found only moderate associations between physical activity and QoL, there is evidence that moderate increases in physical activity in cancer patients can improve sleep quality and aspects of QoL including emotional distress and fatigue, among others.45–47 Although physical activity was not significantly associated with physical health in the predictive models, physical activity was significantly correlated with the physical health subscales of physical functioning and general health in both cancer survivors and the full cohort and with the emotional health subscale of vitality and emotional well-being. This information may inform aspects of health that impede physical activity in cancer survivors as well as those without a history of cancer, and which may be improved through physical activity interventions. Several recent systematic reviews concluded that exercise improves QoL significantly in patients with cancer during and following medical intervention,48–50 and interventions have been successful at increasing long-term physical activity among cancer survivors.51
Vitamin D was examined in this study, and is available in two distinct forms, ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3). Vitamin D3 is produced from exposure of the skin to ambient light and can also be consumed in the diet. Vitamin D2 is not produced in the human body, but is found in a limited number of foods and is a major component of vitamin D supplements.52 Study participants taking vitamin D supplements had on average five times the level of serum vitamin D2, as those who did not. Vitamin D supplementation was more prevalent among cancer survivors, which may explain the higher serum vitamin D2 levels in survivors compared to controls.
We were interested in comparing serum vitamin D3 status between survivors and controls, as well as testing vitamin D3 as a potential surrogate marker for time spent outdoors. We did not find a difference in vitamin D3 between survivors and controls. Similar to other studies, we did find a weak correlation between serum vitamin D3 and hours spent outdoors daily.34 It is interesting that a significant, moderate correlation existed between hours spent outdoors and mental health and that outdoor activity was predictive of mental health. This suggests the relative importance of mental health to cancer survivor’s and other activities of daily living with potential implications on time spent in inactive behaviors.
Melatonin was also of interest as a potential marker for sleep quality. Urinary melatonin was significantly lower in cancer survivors, and survivors had poorer sleep quality; however there was no significant relationship between melatonin and our measures of sleep time or sleep quality. Of interest, although cancer survivors had poorer sleep quality, they had significantly longer average sleep times, suggesting that their sleep may not be restive.
This study was limited by the cross-sectional nature and relatively small sample size. It was representative of the rural counties in Virginia, however, and may have applicability to other rural communities. Although we used robust instruments to collect information about the physical activity habits and QoL of the rural participants, we did not explore the environmental factors specific to these rural communities that may influence lifestyle behaviors. The living environment is an important determinant of health, and rural communities experience significant health disparities.53
A recent comparison of health outcomes of rural and non-rural US counties showed that a greater proportion of rural counties are in the worst quartile for six indexed health-related domains, and at increased odds of being in the worst quartile for two environmental domains including clinical care and social and economic factors.54 The underserved and under-resourced condition of many rural communities presents challenges for public health initiatives designed to improve the health and QoL of rural residents in general and cancer survivors specifically.
Conclusions
Rural communities have relatively limited cancer treatment facilities, with residents often receiving treatment at distant locations. Posttreatment survivorship care occurs long distance, and survivors may return to environments with limited support services. Our study has highlighted the poorer QoL (physical and mental health) and sleep quality of cancer survivors compared to their neighbors without a history of cancer, and the significant relationship of QoL and sleep. Further study needs to be done on the effectiveness of sleep interventions in improving QoL in cancer survivors. As the cancer care community responds to the expressed need of survivors for posttreatment support by developing survivorship guidelines and quality metrics, QoL and the factors that impact it, particularly sleep quality, should be part of those metrics. Identifying and considering the living environments of rural cancer survivors and the support services available to them should be an integral part of the survivorship care planning. Further research is needed on innovative methods for delivery of effective lifestyle programs that positively impact the factors that influence QoL in rural communities in general and cancer survivors returning to those communities after treatment.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Virginia Commonwealth University Institutional Review Board and with the 1964 Declaration of Helsinki and its later amendments. The study was approved by the Virginia Commonwealth University Institutional Review Board (#052411) and all participants signed informed consent prior to their participation.
Acknowledgments
Significant contributors to the conduct of this study were Susan Mathena and Kristin Herrick. Sincere thanks goes out to the participants in the study, who gave generously of their time and valuable information about themselves. This study was generously funded by the Virginia Tobacco Indemnification and Community Revitalization Commission (grant #2083), awarded to Virginia Commonwealth University Massey Cancer Center. The funder had no role in the conduct of the research.
Disclosure
At the time of this study, Yi Ning was employed by the GlaxoSmithKline Institute of Infectious Disease and Public Health, Beijing, China, and Aipang Wang was employed by Apex Life Science, Richmond, VA, USA. The authors report no other conflicts of interest in this work.
References
Mccabe MS, Bhatia S, Oeffinger KC, et al. American Society of Clinical Oncology statement: achieving high-quality cancer survivorship care. J Clin Oncol. 2013;31(5):631–640. | ||
Aziz NM. Cancer survivorship research: state of knowledge, challenges and opportunities. Acta Oncol. 2007;46(4):417–432. | ||
Aziz NM, Rowland JH. Trends and advances in cancer survivorship research: challenge and opportunity. Semin Radiat Oncol. 2003;13(3):248–266. | ||
American Cancer Society. Cancer treatment & survivorship facts & figures (2016–2017). Available from: http://www.cancer.org/research/cancerfactsstatistics/survivor-facts-figures. Accessed November 14, 2016. | ||
Schottenfeld D, Fraumeni JF, James R. Cancer Epidemiology and Prevention. New York: Oxford University Press; 2006. | ||
Ford ES, Bergmann MM, Kröger J, Schienkiewitz A, Weikert C, Boeing H. Healthy living is the best revenge: findings from the European Prospective Investigation into Cancer and Nutrition-Potsdam study. Arch Intern Med. 2009;169(15):1355–1362. | ||
World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective. Washington DC: AICR; 2007. | ||
Irvine D, Vincent L, Graydon JE, Bubela N, Thompson L. The prevalence and correlates of fatigue in patients receiving treatment with chemotherapy and radiotherapy. A comparison with the fatigue experienced by healthy individuals. Cancer Nurs. 1994;17(5):367–378. | ||
Pozo CL, Morgan MA, Gray JE. Survivorship issues for patients with lung cancer. Cancer Control. 2014;21(1):40–50. | ||
Pinquart M, Duberstein PR. Depression and cancer mortality: a meta-analysis. Psychol Med. 2010;40(11):1797–1810. | ||
Andersen BL, Rowland JH, Somerfield MR. Screening, assessment, and care of anxiety and depressive symptoms in adults with cancer: an American Society of Clinical Oncology Guideline Adaptation. J Oncol Pract. 2015;11(2):133–134. | ||
Ahles TA, Root JC, Ryan EL. Cancer- and cancer treatment-associated cognitive change: an update on the state of the science. J Clin Oncol. 2012;30(30):3675–3686. | ||
Siegel R, Desantis C, Virgo K, et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin. 2012;62(4):220–241. | ||
Bodai BI, Tuso P. Breast cancer survivorship: a comprehensive review of long-term medical issues and lifestyle recommendations. Perm J. 2015;19(2):48–79. | ||
Garcia DO, Thomson CA. Physical activity and cancer survivorship. Nutr Clin Pract. 2014;29(6):768–779. | ||
Ibrahim EM, Al-Homaidh A. Physical activity and survival after breast cancer diagnosis: meta-analysis of published studies. Med Oncol. 2011;28(3):753–765. | ||
Meyerhardt JA, Giovannucci EL, Holmes MD, et al. Physical activity and survival after colorectal cancer diagnosis. J Clin Oncol. 2006;24(22):3527–3534. | ||
Lemanne D, Cassileth B, Gubili J. The role of physical activity in cancer prevention, treatment, recovery, and survivorship. Oncology. 2013;27(6):580–585. | ||
Ottenbacher A, Yu M, Moser RP, Phillips SM, Alfano C, Perna FM. Population estimates of meeting strength training and aerobic guidelines, by gender and cancer survivorship status: findings from the Health Information National Trends Survey (HINTS). J Phys Act Health. 2015;12(5):675–679. | ||
Schmitz KH, Courneya KS, Matthews C, et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc. 2010;42(7):1409–1426. | ||
Blair CK, Robien K, Inoue-Choi M, Rahn W, Lazovich D. Physical inactivity and risk of poor quality of life among elderly cancer survivors compared to women without cancer: the Iowa Women’s Health Study. J Cancer Surviv. 2016;10(1):103–112. | ||
George GC, Iwuanyanwu EC, Anderson KO, et al. Sleep quality and its association with fatigue, symptom burden, and mood in patients with advanced cancer in a clinic for early-phase oncology clinical trials. Cancer. 2016;122(21):3401–3409. | ||
Yennurajalingam S, Chisholm G, Palla SL, Holmes H, Reuben JM, Bruera E. Self-reported sleep disturbance in patients with advanced cancer: frequency, intensity, and factors associated with response to outpatient supportive care consultation – a preliminary report. Palliat Support Care. 2015;13(2):135–143. | ||
Holliday EB, Dieckmann NF, Mcdonald TL, Hung AY, Thomas CR, Wood LJ. Relationship between fatigue, sleep quality and inflammatory cytokines during external beam radiation therapy for prostate cancer: a prospective study. Radiother Oncol. 2016;118(1):105–111. | ||
Innominato PF, Spiegel D, Ulusakarya A, et al. Subjective sleep and overall survival in chemotherapy-naïve patients with metastatic colorectal cancer. Sleep Med. 2015;16(3):391–398. | ||
Dickerson SS, Connors LM, Fayad A, Dean GE. Sleep-wake disturbances in cancer patients: narrative review of literature focusing on improving quality of life outcomes. Nat Sci Sleep. 2014;6:85–100. | ||
Virginia Department of Health. Cancer in Virginia: Overview and Selected Statistics; December 2016. Available from: http://www.vdh.virginia.gov/content/uploads/sites/27/2016/07/Cancer-in-Virginia-2014_Final.pdf. Accessed August 21, 2018. | ||
Meilleur A, Subramanian SV, Plascak JJ, Fisher JL, Paskett ED, Lamont EB. Rural residence and cancer outcomes in the United States: issues and challenges. Cancer Epidemiol Biomarkers Prev. 2013;22(10):1657–1667. | ||
United States Census Bureau. QuickFacts. Available from: https://www.census.gov/quickfacts/fact/table/va,US/PST045217#viewtop. Accessed August 21, 2018. | ||
Rimm EB, Giovannucci E, Stampfer MJ, Colditz GA, Litin L, Willett W. Reproducibility and validity of a self-administered semi-quantitative food frequency questionnaire, and diet records in US men. Am J Epidemol. 1992;135:1114–1136. | ||
Buysse DJ, Reynolds CF, Monk TH, Hoch CC, Yeager AL, Kupfer DJ. Quantification of subjective sleep quality in healthy elderly men and women using the Pittsburgh Sleep Quality Index (PSQI). Sleep. 1991;14(4):331–338. | ||
Kim RB, Phillips A, Herrick K, et al. Physical activity and sedentary behavior of cancer survivors and non-cancer individuals: results from a national survey. PLoS One. 2013;8(3):e57598. | ||
Mccarty CA. Sunlight exposure assessment: can we accurately assess vitamin D exposure from sunlight questionnaires? Am J Clin Nutr. 2008;87(4):1097S–1101S. | ||
Blanchard CM, Côté I, Feeny D. Comparing short form and RAND physical and mental health summary scores: results from total hip arthroplasty and high-risk primary-care patients. Int J Technol Assess Health Care. 2004;20(2):230–235. | ||
Gerrior S, Juan W, Basiotis P. An easy approach to calculating estimated energy requirements. Prev Chronic Dis. 2006;3(4):A129. | ||
Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32(9 Suppl):S498–S516. | ||
Littner M, Kushida CA, Anderson WM, et al. Standards of Practice Committee of the American Academy of Sleep Medicine. Practice parameters for the role of actigraphy in the study of sleep and circadian rhythms: an update for 2002 – an American Academy of Sleep Medicine Report 4. Sleep. 2003;26:337–341. | ||
Pollak CP, Tryon WW, Nagaraja H, Dzwonczyk R. How accurately does wrist actigraphy identify the states of sleep and wakefulness? Sleep. 2001;24(8):957–965. | ||
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. | ||
Enko D, Kriegshäuser G, Stolba R, Worf E, Halwachs-Baumann G. Method evaluation study of a new generation of vitamin D assays. Biochem Med. 2015;25(2):203–212. | ||
Klante G, Brinschwitz T, Secci K, Wollnik F, Steinlechner S. Creatinine is an appropriate reference for urinary sulphatoxymelatonin of laboratory animals and humans. J Pineal Res. 1997;23(4):191–197. | ||
Graham C, Cook MR, Kavet R, Sastre A, Smith DK. Prediction of nocturnal plasma melatonin from morning urinary measures. J Pineal Res. 1998;24(4):230–238. | ||
36-Item Short Form Survey (SF-36) Scoring Instructions. Available from: http://www.rand.org/health/surveys_tools/mos/36-item-short-form/scoring.html. Accessed January 7, 2017. | ||
Mustian KM, Sprod LK, Janelsins M, et al. Multicenter, randomized controlled trial of yoga for sleep quality among cancer survivors. J Clin Oncol. 2013;31(26):3233–3241. | ||
Tang MF, Liou TH, Lin CC. Improving sleep quality for cancer patients: benefits of a home-based exercise intervention. Support Care Cancer. 2010;18(10):1329–1339. | ||
Wenzel JA, Griffith KA, Shang J, et al. Impact of a home-based walking intervention on outcomes of sleep quality, emotional distress, and fatigue in patients undergoing treatment for solid tumors. Oncologist. 2013;18(4):476–484. | ||
Courneya KS, Segal RJ, Mackey JR, et al. Effects of exercise dose and type on sleep quality in breast cancer patients receiving chemotherapy: a multicenter randomized trial. Breast Cancer Res Treat. 2014;144(2):361–369. | ||
Gerritsen JKW, Vincent AJPE. Exercise improves quality of life in patients with cancer: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2016;50(13):796–803. | ||
Mishra SI, Scherer RW, Snyder C, Geigle P, Gotay C. Are exercise programs effective for improving health-related quality of life among cancer survivors? A systematic review and meta-analysis. Oncol Nurs Forum. 2014;41(6):E326–E342. | ||
Mishra SI, Scherer RW, Snyder C, Geigle PM, Berlanstein DR, Topaloglu O. Exercise interventions on health-related quality of life for people with cancer during active treatment. Clin Otolaryngol. 2012;37(5):390–392. | ||
Kanera IM, Willems RA, Bolman CA, Mesters I, Verboon P, Lechner L. Long-term effects of a web-based cancer aftercare intervention on moderate physical activity and vegetable consumption among early cancer survivors: a randomized controlled trial. Int J Behav Nutr Phys Act. 2017;14(1):19. | ||
Houghton LA, Vieth R. The case against ergocalciferol (vitamin D2) as a vitamin supplement. Am J Clin Nutr. 2006;84(4):694–697. | ||
Lutfiyya MN, Mccullough JE, Haller IV, Waring SC, Bianco JA, Lipsky MS. Rurality as a root or fundamental social determinant of health. Dis Mon. 2012;58(11):620–628. | ||
Anderson TJ, Saman DM, Lipsky MS, Lutfiyya MN. A cross-sectional study on health differences between rural and non-rural U.S. counties using the County Health Rankings. BMC Health Serv Res. 2015;15:441. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.