")
Back to Journals » Nature and Science of Sleep » Volume 11
Impact Of Phenotypic Heterogeneity Of Insomnia On The Patients’ Response To Cognitive-Behavioral Therapy For Insomnia: Current Perspectives
Authors Galbiati A, Sforza M, Fasiello E, Castronovo V, Ferini-Strambi L
Received 6 July 2019
Accepted for publication 22 October 2019
Published 29 November 2019 Volume 2019:11 Pages 367—376
DOI https://doi.org/10.2147/NSS.S198812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sutapa Mukherjee
Andrea Galbiati,1,2 Marco Sforza,1,2 Elisabetta Fasiello,1 Vincenza Castronovo,1 Luigi Ferini-Strambi1,2
1IRCCS San Raffaele Scientific Institute, Department of Clinical Neurosciences, Neurology – Sleep Disorders Center, Milan, Italy; 2Faculty of Psychology, “Vita-Salute” San Raffaele University, Milan, Italy
Correspondence: Andrea Galbiati
Department of Clinical Neurosciences OSR-Turro, Neurology – Sleep Disorders Center, Università Vita-Salute San Raffaele, Milan, Italy
Tel +39 0226433397
Email [email protected]
Abstract: Insomnia is one of the most common mental disorders and the most frequent sleep disorder encountered in clinical practice, with a prevalence of about 7% in the European population. Insomnia Disorder (ID) is defined as a disturbance of sleep initiation or maintenance, followed by a feeling of non-restorative sleep and several diurnal consequences ranging from occupational and social difficulties to cognitive impairment. Cognitive-Behavioral Therapy for Insomnia (CBT-I) is considered the first-choice therapy for this disorder because its effectiveness has been proven to be greater in the long term with fewer side effects in comparison to pharmacotherapy. Although its effectiveness has been well established, it has been reported that nearly 40% of patients do not achieve remission after treatment. This finding could be the consequence of heterogeneity of ID between patients. It has been proposed that this heterogeneity might be ascribable to indices that are not related to sleep quality and quantity, such as comorbidities, life events, and personality traits. However, several works focused on the role of sleep markers, in particular objective total sleep time, for the phenotypization of ID and treatment response. The aim of this work is to summarize the available scientific literature regarding the impact of ID subtype on CBT-I response.
Keywords: cognitive-behavioral therapy for insomnia, polysomnography, insomnia disorder, subtype, objective sleep duration
Introduction
Insomnia Disorder (ID) is one of the most common mental disorders and the most frequent sleep disorder encountered in clinical practice, with a prevalence of about 7% in the European population.1 It is defined as a disorder of sleep initiation or maintenance, followed by a feeling of non-restorative sleep and several diurnal consequences ranging from occupational and social difficulties to cognitive impairment.2 Notably, the diagnosis is based only on the clinical assessment of subjective symptoms according to the most recent versions of the two principal nosological classifications of mental and sleep disorders: the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and the third version of the International Classification of Sleep Disorder (ICSD-3).2,3 Polysomnographic (PSG) evaluation in ID patients is used only to exclude the presence of another sleep disorder.
An important aspect of insomnia is its association with mental disorders; in particular, patients with ID have a twofold risk of developing depression over the course of the disease.4 Hence, an efficacious and timely treatment is of the utmost importance.
According to the most recent guideline for ID management, Cognitive-Behavioral Therapy for Insomnia (CBT-I) is considered the first-choice therapy for this disorder because its effectiveness has been proven to be greater in the long term with fewer side effects in comparison to pharmacotherapy.5,6 CBT-I is a multicomponent approach that encompasses psychoeducation/sleep hygiene, relaxation training, stimulus control, sleep restriction, and cognitive therapy. It is usually delivered face to face, both individually or in a group, by a trained clinician.
Although its effectiveness has been well established, it has been reported that up to 40% of patients do not achieve remission after treatment.6–8 This lack of effectiveness could be the consequence of poor adherence to the treatment program or the patient having a type of insomnia for which CBT-I is not sufficient. With respect to adherence to CBT-I, less attention has been paid than might be expected for a therapeutic program.9 For instance, there is no agreed definition of adherence to CBT-I. It is possible that heterogeneity of ID between patients explains why some patients do not achieve remission of insomnia with CBT-I.9
In recent years, ID heterogeneity has gained more attention. Of note, it has been proposed that the characterization of ID types should be based on more than the usual indices of sleep quality and quantity and include a variety of dimensions, such as mental and physical health, childhood trauma and other life events, fatigue, sleepiness, hyperarousal, hyperactivity, lifetime sleep history, chronotype, depression, anxiety, mood, quality of life, personality, happiness, worry, rumination, and self-consciousness.10 However, several studies have investigated the value of objective sleep markers, in particular objective Total Sleep Time (TST),11 for phenotyping ID and its response to treatment. This approach challenges the current guidelines that PSG assessment is not useful in the evaluation of ID, only being of value in excluding another sleep disorder.
The aim of this narrative review is to summarize the available scientific literature about the impact of ID subtype on CBT-I response. The review is divided into two parts: the first on insomnia subtyping in general; the second on sleep and non-sleep features that predict response to CBT-I. The overall aim is to identify indices able that will predict CBT-I outcomes.
Insomnia Subtyping: State Of The Science
As noted above, ID is a chronic clinical syndrome based on symptoms of difficulty with sleep despite adequate opportunity for sleep together with daytime dysfunction. Although used in the past, there is little evidence to support the classification into sleep onset insomnia, sleep maintenance insomnia, and early awakening. Given the diagnosis on subjective complaints, the current recommendation is that objective sleep studies, such as actigraphy and PSG, are not used unless there are grounds to exclude another sleep disorder. However, there is valuable information about sleep studies in patients with ID that might inform better selection for CBT-I.
Objective measures derived from PSG recordings often show variations of minor significance between good sleepers (GS) and people with ID defined by self-reported subjective complaints about sleep quality and quantity. A meta-analysis showed that, compared to GS, insomnia patients had longer Sleep Latency (SL), shorter TST, reduced Sleep Efficiency (SE) below the accepted threshold of “good sleep” of 85%,12 decreased slow-wave sleep and decreased Rapid Eye Movements (REM) sleep.12
More in-depth methods to characterize sleep electrophysiology have identified further differences between these two groups.13 ID patients have increased instability of non-REM (NREM) and REM sleep13,14 and an increase in electroencephalographic (EEG) fast frequencies, that can be interpreted as a marker of cortical hyperactivity.15–20 This hyperactivity is also reflected in Event-Related Potentials (ERPs) studies, which show an increased sensitivity to auditory stimuli in ID patients.21–24 In addition, EEG features of sleep stage 2, such as Sleep Spindles (SS) and K-Complexes, have been found to be different between ID and GS.25–27 However, up until now, PSG data have not been sensitive enough for either the diagnosis of insomnia or for phenotyping it. Furthermore, as noted above, even the classical insomnia complaints of difficulty initiating sleep, difficulty maintaining sleep, and early morning awakening, as well as the common classification into idiopathic, psychophysiological, and paradoxical insomnia,28,29 do not have adequate validity and reliability for diagnostic purposes.30 Therefore, ICSD-3 and DSM-5 did not include additional subtyping of chronic insomnia.2,3
Following the decision by DSM-5 and ICSD-3 not to subtype ID, in particular the conclusion that sleep outcomes are not sufficient to describe the heterogeneity of insomnia patients, the focus of investigations has been on non-sleep-related characteristics. Benjamins et al.10 reviewed the literature on psychometric aspects of ID to complement other meta-analyses and systematic reviews. They concluded that inconsistencies in studies on subtyping ID arise from the limited value of sleep-related variables and that non-sleep variables (personality traits, history of disease, and life events) can discriminate between patients with and without ID. In further exploration of this hypothesis, several authors have attempted to subtype the ID population by using sophisticated methodologies such as Latent Class Analysis (LCA), Latent Profile Analysis, and Network Analysis. The patient data used were on one hand sleep variables such as insomnia symptoms, severity, and sleep disturbance,31,32 and on the other hand non-sleep variables, such as functional impairment and comorbid condition,31 socioeconomic state and gender,33 level of distress32–34 and personality traits including neuroticism,35 response to pleasurable emotions and level of reactivity to life events.34
Overall, the balance of these recent studies support the hypothesis that sleep outcomes are not sufficient to describe ID heterogeneity. However, further studies are needed to confirm the hypothesis. Finally, an important approach to subtyping a syndrome such as ID is whether to do so on diagnostic, demographic, and pathogenetic data or to subtype on response to treatment. In the case of ID, it would be valuable to have it subtyped into categories that are likely to respond or not to CBT-I, the first-choice treatment.
Can Sleep And Non-Sleep Features Predict CBT-I Outcome?
Objective Sleep Duration (OSD)
Most of the studies that support the value of objective sleep indices to predict the CBT-I outcomes are focused on OSD at the baseline. This index seems useful to assess the biological severity of ID and to distinguish two insomnia subtypes: patients with Short Sleep Duration (SSD: < 6 h per night) and patients with Normal Sleep Duration (NSD: > 6 h per night).11 Using this subtyping, several studies report that SSD may be a marker of a blunted CBT-I response.36–38 This result could be explained by SSD patients not being able to benefit from sleep restriction, which is the primary intervention in behavioural sleep treatments. Patients with SSD have high rates of comorbidity,39–44 an association with cognitive, emotional, physiological, and cortical hyperarousal,45,46 and seem to be more susceptible to pharmacological therapies that aim to decrease physiological hyperarousal and to increase OSD.11,47 Conversely, patients with NSD, characterized by sleep misperception, anxious-ruminative traits,48 cognitive and emotional hyperarousal, but not by physiological hyperarousal,49,50 seem to respond better to behavioural strategies.11
Even though this OSD biomarker looks promising, there are other studies,51–53 that report no group significant difference in response to CBT-I between SSD and NSD phenotypes.
In summary, OSD has been found to be an inconsistent marker to predict CBT-I outcome (Table 1).
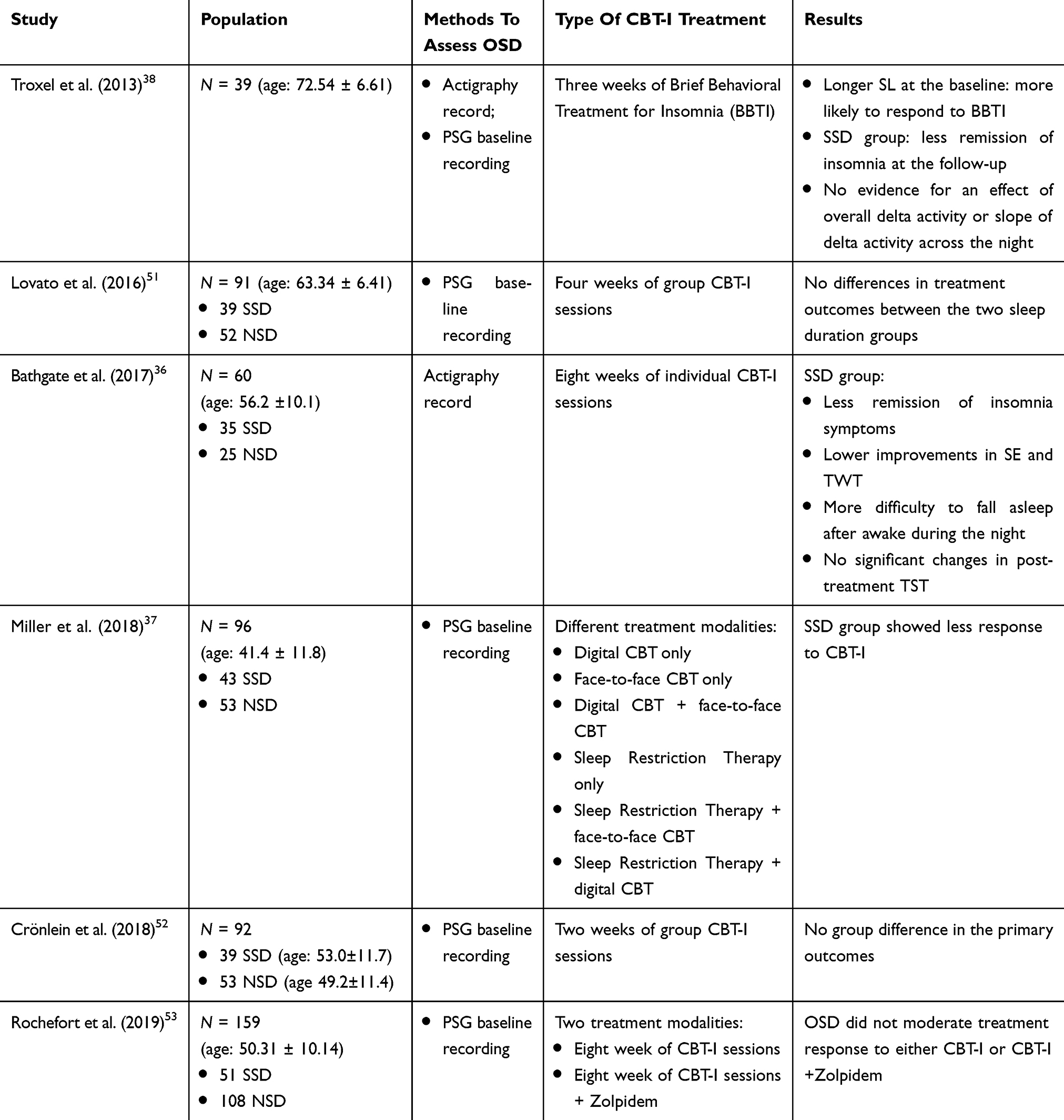 |
Table 1 Studies Evaluating OSD In CBT-I |
Subjective Sleep Duration
With respect to subtyping by subjective sleep duration as a predictor of CBT-I efficacy, a recent study by our group54 demonstrated that short sleepers showed a boosted response to CBT-I. Chiu et al.55 report a similar finding with CBT-I treatment for ID in patients with schizophrenia and related psychoses. On the other hand, patients with shorter TST were reported to be more likely to drop-out prior to the fourth session, but there are inconsistencies across studies.56–58 In summary, subjective sleep duration has been found to be an inconsistent predictor of CBT-I outcomes.
Sleep Variability
ID is often characterized by night-to-night fluctuations in the quantity and quality of sleep. In other words, insomnia sufferers show some nights of poor sleep quality, typically followed by good ones, and vice versa.59 Because sleep variability may be one of the most distressing aspects of insomnia, it is relevant to assess its impact for ID patients, especially its relationship to the efficacy of treatments.
However, there are only a few studies60–62 on sleep variability measures as prognostic indices of therapeutic response. The results show that improvements in SL, SE, Wake After Sleep Onset (WASO) and TST with CBT-I were higher in ID patients who had increased rates of sleep variability at the baseline compared with those who had lower variability.60–62 As suggested by Chan et al.,61 patients with high variability may be more motivated to improve their sleep because they are more aware of what a good sleep is like and hence adhere more to the treatment. It is important to note that the presence of sleep variability with night-to-night fluctuations in the quantity and quality of sleep in ID patients makes it questionable to make a clear distinction between subjects with NSD and SSD, especially the current strict cut-off of 6 hrs TST.
PSG/EEG Features
There are three aspects of PSG/EEG results in ID patients. The first is whether there are differences in the PSG/EEG between ID patients and GS. The second is whether successful CBT-I changes the PSG/EEG. The third is whether there are features on the baseline PSG/EEG that predict a successful response to PSG. With respect to the impact of CBT-I, PSG indices such as spending excessive Time in Bed (TIB) and napping are targets of CBT-I and likely to improve with successful CBT-I. One of the proposed mechanisms of CBT-I is that it may increase the homeostatic pressure of sleep. This is supported by the results of Cervena et al., where CBT-I resulted in a more rapid decline in EEG NREM delta power during the night.63
With respect to PSG/EEG markers of response to CBT-I, Krystal et al.64 investigated the relationship between NREM EEG spectral measures and CBT-I response. They demonstrated that lower peak delta power in the first NREM period and a slower decline in peak delta power over the night were associated with greater subjective improvement after treatment.64 These results support the hypothesis of an impaired homeostatic function in ID patients that can be restored throughout CBT-I.
It is interesting to note that ID patients with misperception of sleep duration had decreased NREM EEG delta and elevated alpha, sigma, and beta powers, compared with both control subjects and insomnia sufferers who accurately estimated their sleep times.65 This result suggests that alterations in NREM EEG frequencies are associated with a perception of wakefulness and/or a sense of impaired sleep that is not detected by the traditional scoring of PSG.
A few studies have investigated sleep-microstructure and specific EEG elements as biomarkers to predict CBT-I outcomes. A pilot study showed that basal differences in SS density (SSD) were associated with some measures of response to CBT-I, both in the short and long term.66 As there is evidence suggesting a protective role of SS in maintaining sleep, lower SSD might represent an individual EEG marker for the development of ID.67–69
In summary there are complex relationships between PSG/EEG, ID and its response to CBT-I. Future investigations should explore how interventions, especially CBT-I, might be tailored for individual patients by taking into account specific sleep EEG properties.
Clinical/Demographic Characteristics
At present, the criteria for the diagnosis of ID are symptoms frequency and duration, all subjective criteria70 with no reference to pathogenesis or likelihood of response to treatment. Nevertheless, we will focus on clinical/demographic features that could predict the effect of CBT-I. In this section efficacy refers to the performance of CBT-I under the ideal, controlled conditions of a clinical trial and effectiveness refers to its performance under “real-world” conditions.
Drop-Out, Adherence, And Attendance Predictors
The reduced effectiveness of CBT-I compared to its efficacy in clinical trials can be explained in part by drop-out, poor adherence, and reduced attendance at sessions.
With respect to drop-out, adherence, and attendance percentage, Perlis et al.56 showed that shorter TST and greater number of awakenings were associated with drop-out prior to the fourth session. Consistent with these results, Ong et al.57 reported that shorter TST and greater severity of depression at the baseline were related to drop-out prior to the fourth session. In contrast, Yeung et al.58 showed that longer TST (TST ≥ 6.82h), lower Insomnia Severity Index (ISI) total score (ISI < 13) and higher depression score (Hospital Anxiety and Depression Scale depression score ≥ 9) predicted drop-out in 207 insomnia subjects. However, the difference in the results may be due to different forms of CBT-I. Face-to-face CBT-I was provided in the first two studies compared to internet-based self-help CBT-I in the third. However, taken together, these findings suggest that depression severity, rather than TST, may be an informative predictor of drop-out.
Adherence to a treatment such as CBT-I is a very important determinant of its effectiveness. For example, Ludwin et al.71 assessed adherence to sleep restriction, not CBT-I, through differences in prescribed versus self-reported TIB, variability of TIB, and percentage of completed sleep diaries.72 They reported no significant relationships among the adherence measures and sleep outcomes. The authors interpreted this lack of association with the possible presence of some confounding factors, such as comorbidities with other psychiatric disorders. In addition, the sample size was small, with only 22 volunteers completing the study. Cui and Fiske73 evaluated the prediction of both adherence and attendance in 108 adults with ID. An association between older age and better attendance (in terms of presence at three or more sessions) and adherence (in terms of consistent bedtime and waketime) was found. In addition, symptoms of anxiety and depression were associated with less attendance, and depression was linked to more inconsistent wake times. The authors recommend a tailored-approach CBT-I, in which anxiety and depression are managed before or during the CBT-I combined with addressing the needs of different age groups.
In conclusion, comorbidities, especially depression, seem to be a consistent predictor of drop-out, attendance, and adherence.
Sleep And Non-Sleep Predictors Of CBT-I Outcomes
The prediction of CBT-I efficacy can be investigated not only through predictors of drop-out, adherence and attendance, but also with subjective sleep or non-sleep indicators useful for subtyping ID population in accordance with treatment efficacy.
Indeed, comorbidities could be added to the list of CBT-I outcomes’ predictors. Chiu et al.55 investigated sleep subtypes in schizophrenia and related psychoses as well as response to CBT-I. Sleep subtypes were based on self-reported sleep outcomes from the Pittsburgh Sleep Quality Index (PSQI) assessed at the baseline. Data-driven exploratory LCA of PSQI variables identified three classes: classic severe insomnia; insomnia with normal sleep duration; and insomnia with hypersomnia. All three clusters showed significant improvements in sleep and clinical symptoms after CBT-I, specifically psychological distress, anxiety, and depression subscale scores were no longer at clinical levels at the end of CBT-I. However, no statistical differences were found in improvements of comorbid symptoms across the three classes. Although all three classes showed improvements in sleep indicators at the end of the treatment, there were differences between the classes. Patients with classic severe insomnia symptoms (SSD, poor SE, and prolonged SL) showed the greatest benefit from CBT-I. On the other hand, insomnia with NSD had a blunted response, with improvements in daytime functioning and TST, but no changes in SE.
Another study by Bei et al. investigated the heterogeneity in long-term trajectory of depression following CBT-I in 148 adult patients with combined Major Depression Disorder (MDD) and ID.74 Using data from 2-year follow-up after CBT-I, statistical modeling identified latent trajectory classes. The three trajectory classes based on depression severity were: partial responders (68.9%), initial responders (17.6%), and optimal responders (13.5%). Although the three classes had reduced insomnia severity during and immediately after CBT-I treatment, they differed on insomnia-related measures after treatment began, with the optimal responders reporting the lowest insomnia severity at all time periods and at 2-year follow-up.
These studies highlighted the complex, potentially bi-directional, relationship between ID and mental health disorders, with the conclusion that treatment should be directed to both.
With respect to a general population with insomnia, Sánchez-Ortuño et al.75 investigated the patterns of unhelpful beliefs about sleep in insomnia patients and whether those patterns could predict treatment responses. Four empirically derived age-matched subgroups were determined which differed in terms of insomnia severity, use of prescribed medication for sleep, depression and anxiety symptoms, and daytime sleepiness: “worried and medication-biased”; “worried and symptom-focused”; “mild sleep worries”; and “low endorsement.” The group with more severe insomnia and specific sleep-related worry exhibited the greatest reduction on the Insomnia Symptoms Questionnaire (ISQ) scores at the 6-month follow-up after CBT-I. On the other hand, patients with most extreme view in endorsing statements about medication such as “I’d better take sleeping pills” had scores on the worry/helplessness scale that still remained above the norm after treatment. These results demonstrated that dysfunctional beliefs about sleep might contribute to subtyping ID patients into subgroups that respond differently to CBT-I.
The most comprehensive study to date, which investigated predictors for the effectiveness of CBT-I efficacy through subtyping both sleep and non-sleep measures, is that of Blanken et al. mentioned above34. In addition to the identification of five insomnia subtypes, they developed and tested a new questionnaire (Insomnia Type Questionnaire) to enable recognition of the five classes in clinical practice, with the ultimate aim of predicting treatment response. The study attempted to assess the value of the subtypes for predicting response to online CBT-I provided for a subsample of 42 ID patients compared with 26 patients in a waitlist control group. Unfortunately, the sample size was inadequate for identifying three out of five subtypes. In subjects classified as “moderately distressed but with intact responses to pleasurable emotions”, CBT-I lead to a large decrease in ISI score and in SL. On the other hand, in subjects classified as “slightly distressed with high reactivity to their environment and life events” ISI score was decreased, but SL showed no improvement.
In conclusion, there is an increasing body of evidence that ID can be subtyped or phenotyped using sleep parameters, mental health status, grade of distress, worry and beliefs about sleep to identify better those who will respond well to usual CBT-I, those who will require a highly tailored program, and those for whom other treatments are first-line (Table 2).
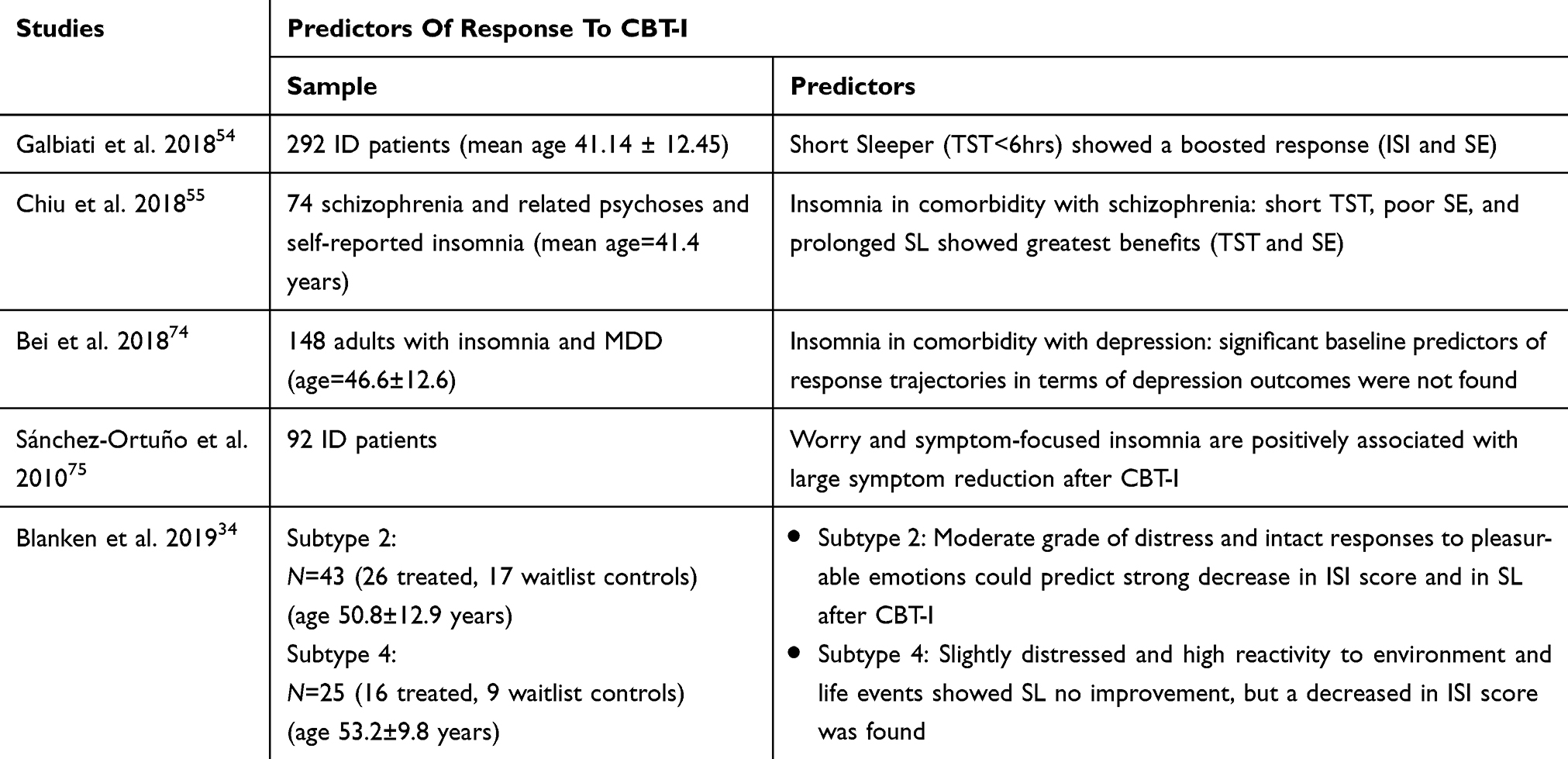 |
Table 2 Subjective Sleep And Non-Sleep Predictors Of CBT-I Outcomes |
Conclusion
There is substantial concern that the high efficacy of CBT-I for ID reported in clinical trials has not been translated into effectiveness, with up to 40% of patients not achieving remission. The evidence from this narrative review indicates that there is an urgent need for high-quality translational research to ensure that patients with ID have the best opportunity for improvement with CBT-I and other treatments.
There are several issues to be considered when evaluating the effectiveness of CBT-I or any other treatment for ID. The first is that there is clarity, ideally standardization, about the intervention. This is a potential problem for ID, because the studies considered in this review have a broad range of “CBT-I” with durations from 2 weeks to 10 weeks, from face-to-face to internet-based self-help, from individual to groups, and from highly experienced clinical psychologists with extensive sleep experience to recent psychology graduates. It is acknowledged that there are limited resources for high-quality face-to-face CBT-I and that alternative forms of delivery, such as internet self-help, are important, but they should be standardized and reproducible. In addition, there is a lack of consensus for the definition and the evaluation of both remission and response after treatment that complicates the interpretation when comparing different studies. Furthermore, adherence to therapy and attrition have received limited attention or have been inadequately addressed. With respect to identifying the predictors of response to treatment, they range from subjective diary and questionnaire reports to objective measures from PSG and actigraphy. Finally, the predictors vary from simple measures such as OSD to highly complex statistical analyses to produce subclasses of ID. Given these challenges, it is important that a consensus is built about how to study the translation of highly efficacious interventions such as CBT-I into real-world practice.
The application of a strict cut-off value (6 hrs) for the distinction between SSD and NSD has produced conflicting results in respect to CBT-I outcomes. Furthermore, the presence of night-to-night fluctuations in the quantity and quality of sleep in ID patients challenges the validity of OSD as a marker. Up to now, there is evidence for a homeostatic dysfunction in these patients76 ; however, its relevance on treatment outcomes needs to be further investigated. Clinical indices, especially those not related to sleep, including the presence of comorbidities, life events, dysfunctional beliefs, grade of distress and emotional regulation skills, are promising factors in predicting CBT-I effectiveness, but their reliability in clinical practice needs to be addressed.
In conclusion, future studies should carefully take into account a combination of both objective and subjective sleep- and non-sleep-related variables in order to identify those patients who may benefit from a specific component of the CBT-I repertoire. For example, patients characterized by increased pre-sleep arousal might benefit from interventions mainly focused on reducing arousal such as meditation, relaxation, and cognitive techniques, whereas patients presenting a homeostatic dysfunction may be more suitable to a sleep restriction protocol. Importantly, recent research has been focused on other interesting constructs that may account for ID symptomatology, for example emotional dysregulation. It has been demonstrated that dysfunction in emotion regulation is present in ID patients,77 but no specific intervention has been developed. Future studies should carefully investigate features of ID symptomatology in order to develop and test new interventions. While the development and dissemination of internet-based CBT-I is fundamental to reach those patients who do not have access to face-to-face treatment, it remains a challenge to identify other patients who might benefit from such an automated intervention compared to conventional delivery78. In summary, although there is clearly phenotypic heterogeneity of ID, the limited number of studies and the methodological variability do not allow a strong conclusion about how to subtype or phenotype ID in a way that will predict confidently the success of CBT-I or any other treatment.
Disclosure
Luigi Ferini-Strambi reports personal fees from Philips-Respironics, UCB Pharma, Lundbeck, Pfizer, Valeas, Italfarmaco, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Wittchen HU, Jacobi F, Rehm J, et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol. 2011;21:655–679. doi:10.1016/j.euroneuro.2011.07.018
2. American Academy of Sleep Medicine. International Classification of Sleep Disorders (ICSD-3).
3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
4. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135:10–19. doi:10.1016/j.jad.2011.01.011
5. Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. Sleep Res. 2017;26(6):675–700.
6. Castronovo V, Galbiati A, Sforza M, et al. Long-term clinical effect of group cognitive behavioral therapy for insomnia: a case series study. Sleep Med. 2018;47:54–59. doi:10.1016/j.sleep.2018.03.017
7. Riemann D, Nissen C, Palagini L, et al. The neurobiology, investigation, and treatment of chronic insomnia. Lancet Neurol. 2015;14(5):547–558. doi:10.1016/S1474-4422(15)00021-6
8. Morin CM, Vallières A, Guay B, et al. Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial. JAMA. 2009;301(19):2005–2015. doi:10.1001/jama.2009.682
9. Matthews EE, Arnedt JT, McCarthy MS, Cuddihy LJ, Aloia MS. Adherence to cognitive behavioral therapy for insomnia: a systematic review. Sleep Med Rev. 2013;17(6):453–464. doi:10.1016/j.smrv.2013.01.001
10. Benjamins JS, Migliorati F, Dekker K, et al. Insomnia heterogeneity: characteristics to consider for data-driven multivariate subtyping. Sleep Med Rev. 2017;36:71–81. doi:10.1016/j.smrv.2016.10.005
11. Vgontzas AN, Fernandez-Mendoza J, Liao D, et al. Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev. 2013a;17(4):241–254. doi:10.1016/j.smrv.2012.09.005
12. Baglioni L, Regen W, Teghen A, et al. Sleep changes in the disorder of insomnia: a meta-analysis of polysomnographic studies. Sleep Med Rev. 2014;18:195–213. doi:10.1016/j.smrv.2013.04.001
13. Feige B, Baglioni C, Spiegelhalder K, et al. The microstructure of sleep in primary insomnia: an overview and extension. Int J Psychophysiol. 2013;89:171–180. doi:10.1016/j.ijpsycho.2013.04.002
14. Riemann D, Spiegelhalder K, Nissen C, et al. REM sleep instability: a new pathway for insomnia? Pharmacopsychiatry. 2012;45(5):167–176. doi:10.1055/s-0031-1299721
15. Freedman RR. EEG power spectra in sleep-onset insomnia. Electroencephalogr Clin Neurophysiol. 1986;63(5):408–413. doi:10.1016/0013-4694(86)90122-7
16. Perlis ML, Smith MT, Andrews PJ, et al. Beta/gamma EEG activity in patients with primary and secondary insomnia and good sleeper controls. Sleep. 2001;24(1):110–117. doi:10.1093/sleep/24.1.110
17. Feige B, Al-Shajlawi A, Nissen C, et al. Does REM sleep contribute to subjective wake time in primary insomnia? A comparison of polysomnographic and subjective sleep in 100 patients. J Sleep Res. 2008;17(2):180–190. doi:10.1111/j.1365-2869.2008.00651.x
18. Terzano MG, Parrino L, Spaggiari MC, et al. CAP variables and arousals as sleep electroencephalogram markers for primary insomnia. Clin Neurophysiol. 2003;114(9):1715–1723. doi:10.1016/S1388-2457(03)00136-6
19. Chouvarda I, Mendez MO, Rosso V, et al. CAP sleep in insomnia: new methodological aspects for sleep microstructure analysis. Conf Proc IEEE Eng Med Biol Soc. 2011;2011:1495–1498.
20. Chouvarda I, Mendez MO, Rosso V, et al. Cyclic alternating patterns in normal sleep and insomnia: structure and content differences. IEEE Trans Neural Syst Rehabil Eng. 2012;20(5):642–652. doi:10.1109/TNSRE.2012.2208984
21. Yang CM, Lo HS. ERP evidence of enhanced excitatory and reduced inhibitory processes of auditory stimuli during sleep in patients with primary insomnia. Sleep. 2007;30(5):585–592. doi:10.1093/sleep/30.5.585
22. Bastien CH, St-Jean G, Morin CM, et al. Chronic psychophysiological insomnia: hyperarousal and/or inhibition deficits? An ERPs investigation. Sleep. 2008;31(6):887–898. doi:10.1093/sleep/31.6.887
23. Kertesz RS, Cote KA. Event-related potentials during the transition to sleep for individuals with sleep-onset insomnia. Behav Sleep Med. 2011;9(2):68–85. doi:10.1080/15402002.2011.557989
24. Turcotte I, Bastien CH. Is quality of sleep related to the N1 and P2 ERPs in chronic psychophysiological insomnia sufferers? Int J Psychophysiol. 2009;72(3):314–322. doi:10.1016/j.ijpsycho.2009.02.001
25. Besset A, Villemin E, Tafti M, et al. Homeostatic process and sleep spindles in patients with sleep-maintenance insomnia: effect of partial (21 h) sleep deprivation. Electroencephalogr Clin Neurophysiol. 1998;107(2):122–132. doi:10.1016/S0013-4694(98)00048-0
26. Bastien CH, St-Jean G, Turcotte I, et al. Sleep spindles in chronic psychophysiological insomnia. J Psychosom Res. 2009;66(1):59–65. doi:10.1016/j.jpsychores.2008.05.013
27. Forget D, Morin CM, Bastien CH. The role of the spontaneous and evoked k- complex in good-sleeper controls and in individuals with insomnia. Sleep. 2011;34(9):1251–1260. doi:10.5665/SLEEP.1250
28. Bastien CH, Vallieres A, Morin CM. Precipitating factors of insomnia. Behav Sleep Med. 2004;2(1):50–62. doi:10.1207/s15402010bsm0201_5
29. American Academy of Sleep Medicine. The International Classification of Sleep Disorders (ICSD-2): Diagnostic and Coding Manual.
30. Edinger JD, Wyatt JK, Stepanski EJ, et al. Testing the reliability and validity of DSM-IV-TR and ICSD-2 insomnia diagnoses: results of a multitrait-multimethod analysis. Arch Gen Psychiatry. 2011;68(10):992–1002. doi:10.1001/archgenpsychiatry.2011.64
31. Foley KA, Sarsour K, Kalsekar A, et al. Subtypes of sleep disturbance: associations among symptoms, comorbidities, treatment, and medical costs. Behav Sleep Med. 2010;8(2):90–104. doi:10.1080/15402001003622842
32. Crawford MR, Chirinos DA, Iurcotta T, et al. Characterization of patients who present with insomnia: is there room for a symptom cluster-based approach? J Clin Sleep Med. 2017;13(7):911–921. doi:10.5664/jcsm.6666
33. Green MJ, Espie CA, Benzeval M. Social class and gender patterning of insomnia symptoms and psychiatric distress: a 20-year prospective cohort study. BMC Psychiatry. 2014;14(1):152. doi:10.1186/1471-244X-14-152
34. Blanken TF, Benjamins JS, Borsboom D, et al. Insomnia disorder subtypes derived from life history and traits of affect and personality. Lancet Psychiatry. 2019;6(2):151–163. doi:10.1016/S2215-0366(18)30464-4
35. Dekker K, Blanken T, Van Someren E. Insomnia and personality-a network approach. Brain Sci. 2017;7(3):28. doi:10.3390/brainsci7030028
36. Bathgate CJ, Edinger JD, Krystal AD. Insomnia patients with objective short sleep duration have a blunted response to cognitive behavioral therapy for insomnia. Sleep. 2017;40:1.
37. Miller CB, Espie CA, Bartlett DJ, et al. Acceptability, tolerability, and potential efficacy of cognitive behavioural therapy for insomnia disorder subtypes defined by polysomnography: a retrospective cohort study. Sci Rep. 2018;8(1):6664. doi:10.1038/s41598-018-25033-3
38. Troxel WM, Conrad TS, Germain A, et al. Predictors of treatment response to brief behavioral treatment of insomnia (BBTI) in older adults. J Clin Sleep Med. 2013;9(12):1281–1289. doi:10.5664/jcsm.3270
39. Fernandez-Mendoza J, Vgontzas AN, Liao D. Insomnia with objective short sleep duration and incident hypertension: the Penn State Cohort. Hypertension. 2012b;60(4):929–935. doi:10.1161/HYPERTENSIONAHA.112.193268
40. Bathgate CJ, Edinger JD, Wyatt JK, et al. Objective but not subjective short sleep duration associated with increased risk for hypertension in individuals with insomnia. Sleep. 2016;39(5):1037–1045. doi:10.5665/sleep.5748
41. Vgontzas AN, Liao D, Pejovic S, et al. Insomnia with objective short sleep duration is associated with type 2 diabetes: a population-based study. Diabetes Care. 2009;32(11):1980–1985. doi:10.2337/dc09-0284
42. Fernandez-Mendoza J, Calhoun S, Bixler EO, et al. Insomnia with objective short sleep duration is associated with deficits in neuropsychological performance: a general population study. Sleep. 2010;33(4):459–465. doi:10.1093/sleep/33.4.459
43. Vgontzas AN, Liao D, Pejovic S, et al. Insomnia with short sleep duration and mortality: the Penn State cohort. Sleep. 2010;33(9):1159–1164. doi:10.1093/sleep/33.9.1159
44. Bertisch SM, Pollock DB, Mittleman MA, et al. Insomnia with objective short sleep duration and risk of incident cardiovascular disease and all-cause mortality: sleep Heart Health Study. Sleep. 2018;41:6. doi:10.1093/sleep/zsy047
45. Bonnet MH, Arand DL. Clinical effects of sleep fragmentation versus sleep deprivation. Sleep Med Rev. 2003;7(4):297–310. doi:10.1053/smrv.2001.0245
46. Vgontzas AN, Zoumakis E, Bixler EO. Adverse effects of modest sleep restriction on sleepiness, performance, and inflammatory cytokines. J Clin Endocrinol Metab. 2004;89(5):2119–2126. doi:10.1210/jc.2003-031562
47. Rodenbeck A, Cohrs S, Jordan W, et al. The sleep-improving effects of doxepin are paralleled by a normalized plasma cortisol secretion in primary insomnia. A placebo- controlled, double-blind, randomized, cross-over study followed by an open treatment over 3 weeks. Psychopharmacology (Berl). 2003;170(4):423–428. doi:10.1007/s00213-003-1565-0
48. Harvey AG, Tang NK. Mis)perception of sleep in insomnia: a puzzle and a resolution. Psychol Bull. 2012;138(1):77–101. doi:10.1037/a0025730
49. Vgontzas AN, Tsigos C, Bixler EO, et al. Chronic insomnia and activity of the stress system: a preliminary study. J Psychosom Res. 1998;45(1):21–31. doi:10.1016/S0022-3999(97)00302-4
50. Bonnet MH, Arand DL. 24-hour metabolic rate in insomniacs and matched normal sleepers. Sleep. 1995;18(7):581–588. doi:10.1093/sleep/18.7.581
51. Lovato N, Lack L, Kennaway DJ. Comparing and contrasting therapeutic effects of cognitive-behavior therapy for older adults suffering from insomnia with short and long objective sleep duration. Sleep Med. 2016;22:4–12. doi:10.1016/j.sleep.2016.04.001
52. Crönlein T, Wetter T, Rupprecht R, et al. Cognitive behavioral treatment for insomnia is equally effective in insomnia patients with objective short and normal sleep duration. Sleep Med. 2018;
53. Rochefort A, Jarrin DC, Bélanger L, et al. Insomnia treatment response as a function of objectively measured sleep duration. Sleep Med. 2019;56:135–144. doi:10.1016/j.sleep.2019.01.016
54. Galbiati A, Sforza M, Poletti M, et al. Insomnia patients with subjective short total sleep time have a boosted response to cognitive behavioral therapy for insomnia despite residual symptoms. Behav Sleep Med;2018. 1–10. doi:10.1080/15402002.2018.1545650
55. Chiu VW, Ree M, Janca A, et al. Sleep profiles and CBT-I response in schizophrenia and related psychoses. Psychiatry Res. 2018;268:279–287. doi:10.1016/j.psychres.2018.07.027
56. Perlis M, Aloia M, Millikan A, et al. Behavioral treatment of insomnia: a clinical case series study. J Behav Med. 2000;23(2):149–161. doi:10.1023/A:1005413117932
57. Ong JC, Kuo TF, Manber R. Who is at risk for dropout from group cognitive-behavior therapy for insomnia? J Psychosom Res. 2008;64(4):419–425. doi:10.1016/j.jpsychores.2007.10.009
58. Yeung WF, Chung KF, Ho FYY, et al. Predictors of dropout from internet-based self-help cognitive behavioral therapy for insomnia. Behav Res Ther. 2015;73:19–24. doi:10.1016/j.brat.2015.07.008
59. Perlis ML, Swinkels CM, Gehrman PR, et al. The incidence and temporal patterning of insomnia: a pilot study. J Sleep Res. 2010;19:31–35. doi:10.1111/jsr.2010.19.issue-1-Part-I
60. Sánchez-Ortuño MM, Edinger JD. Internight sleep variability: its clinical significance and responsiveness to treatment in primary and comorbid insomnia. J Sleep Res. 2012;21(5):527–534. doi:10.1111/jsr.2012.21.issue-5
61. Chan WS, Williams J, Dautovich ND, et al. Night-to-night sleep variability in older adults with chronic insomnia: mediators and moderators in a randomized controlled trial of Brief Behavioral Therapy (BBT-I). J Clin Sleep Med. 2017;13(11):1243–1254. doi:10.5664/jcsm.6790
62. Suh S, Nowakowski S, Bernert RA, et al. Clinical significance of night-to-night sleep variability in insomnia. Sleep Med. 2012;13(5):469–475. doi:10.1016/j.sleep.2011.10.034
63. Cervena K, Dauvilliers Y, Espa F, et al. Effect of cognitive behavioural therapy for insomnia on sleep architecture and sleep EEG power spectra in psychophysiological insomnia. J Sleep Res. 2004;13(4):385–393. doi:10.1111/jsr.2004.13.issue-4
64. Krystal AD, Edinger JD. Sleep EEG predictors and correlates of the response to cognitive behavioral therapy for insomnia. Sleep. 2010;33(5):669–677. doi:10.1093/sleep/33.5.669
65. Krystal AD, Edinger JD, Wohlgemuth WK, et al. NREM sleep EEG frequency spectral correlates of sleep complaints in primary insomnia subtypes. Sleep. 2002;25(6):630–640.
66. Dang-Vu TT, Hatch B, Salimi A, et al. Sleep spindles may predict response to cognitive-behavioral therapy for chronic insomnia. Sleep Med. 2017;39:54–61. doi:10.1016/j.sleep.2017.08.012
67. Schabus M, Kerstin H, Thomas P, et al. Interindividual sleep spindle differences and their relation to learning-related enhancements. Brain Res. 2008;1191:127–135. doi:10.1016/j.brainres.2007.10.106
68. Fogel SM, Smith CT. The function of the sleep spindle: a physiological index of intelligence and a mechanism for sleep-dependent memory consolidation. Neurosci Biobehav Rev. 2011;35(5):1154–1165. doi:10.1016/j.neubiorev.2010.12.003
69. Dang-Vu TT, McKinney SM, Buxton OM, et al. Spontaneous brain rhythms predict sleep stability in the face of noise. Curr Biol. 2010;20(15):R626–7. doi:10.1016/j.cub.2010.06.032
70. Buysse DJ, Ancoli-Israel S, Edinger JD, et al. Recommendations for a standard research assessment of insomnia. Sleep. 2006;29(9):1155–1173. doi:10.1093/sleep/29.9.1155
71. Ludwin BM, Bamonti P, Mulligan EA. Program evaluation of group-based cognitive behavioral therapy for insomnia: a focus on treatment adherence and outcomes in older adults with co-morbidities. Clin Gerontol. 2018;41(5):487–497. doi:10.1080/07317115.2017.1399190
72. Riedel BW, Lichstein KL. Strategies for evaluating adherence to sleep restriction treatment for insomnia. Behav Res Ther. 2001;39(2):201–212. doi:10.1016/S0005-7967(00)00002-4
73. Cui R, Fiske A. Predictors of treatment attendance and adherence to treatment recommendations among individuals receiving cognitive behavioral therapy for insomnia. Cogn Behav Ther. 2019;1–7. doi:10.1080/16506073.2019.1586992
74. Bei B, Asarnow LD, Krystal A, et al. Treating insomnia in depression: insomnia related factors predict long-term depression trajectories. J Consulting Clin Psychol. 2018;86(3):282–293. doi:10.1037/ccp0000282
75. Sánchez-Ortuño MM, Edinger JD. A penny for your thoughts: patterns of sleep-related beliefs, insomnia symptoms and treatment outcome. Behav Res Ther. 2010;48(2):125–133. doi:10.1016/j.brat.2009.10.003
76. Neu D, Mairesse O, Le Bon O. What about sleep homeostasis in insomnia? Comment on the European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):701. doi:10.1111/jsr.2017.26.issue-6
77. Palagini L, Moretto U, Dell’Osso L, Carney C. Sleep-related cognitive processes, arousal, and emotion dysregulation in insomnia disorder: the role of insomnia-specific rumination. Sleep Med. 2017;30:97–104. doi:10.1016/j.sleep.2016.11.004
78. Zachariae R, Lyby MS, Ritterband LM, O’Toole MS. Efficacy of internet-delivered cognitive-behavioral therapy for insomnia – A systematic review and meta-analysis of randomized controlled trials. Sleep Med Rev. 2016;30:1–10. doi:10.1016/j.smrv.2015.10.004
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.