")
Back to Journals » Patient Preference and Adherence » Volume 16
Impact of Personal, Cultural and Religious Beliefs on Medication Adherence among Patients with Chronic Diseases at University Hospital in Northwest Ethiopia
Authors Kasahun AE , Sendekie AK , Mekonnen GA , Sema FD , Kemal LK , Abebe RB
Received 10 April 2022
Accepted for publication 12 July 2022
Published 27 July 2022 Volume 2022:16 Pages 1787—1803
DOI https://doi.org/10.2147/PPA.S370178
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Asmamaw Emagn Kasahun,1 Ashenafi Kibret Sendekie,2 Gizework Alemnew Mekonnen,2 Faisel Dula Sema,2 Leila Kenzu Kemal,2 Rahel Belete Abebe2
1Department of Pharmaceutics and Social Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Rahel Belete Abebe, Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia, Tel +251 924538037, Email [email protected]
Background: Subjective beliefs about chronic disease conditions and their drug management are among factors determining adherence to medications that are amenable to interventions. Patient-level factors such as personal, cultural, and religious beliefs about diseases, and medication use may have a significant impact on medication adherence. The purpose of this study was to assess the impact of personal, cultural and religious beliefs on medication adherence behavior among patients with chronic follow-up.
Patients and Methods: An institutional-based cross-sectional study design was conducted among chronic ambulatory patients from July to August 2021. The data was collected through an interviewer administered questionnaire. Initially stratified sampling technique was used to include proportional participants from different disease conditions, and systematic random sampling was employed to enroll eligible patients from each subgroup. Descriptive statistics such as frequencies and percentages were computed for categorical variables and mean with (standard deviation ±SD) used for continuous variables. Logistic regression model was employed to determine variable with poor adherence. A 95% confidence interval with P-value ≤ 0.05 was used to declare statically significance.
Results: Among the 404 participants, more than half (51%) were males. The mean (±SD) age of the patients was 47.8 ± 14.8 years. Patients with strong belief in the harm of medications were found 4 times more likely to have poor medication adherence than those with weak belief in the harm of medications (AOR = 4.027, 95% CI:1.232– 13.161, P = 0.021). In contrast, having strong personal belief regarding the necessity of medications were found to be less likely to have poor medication adherence (AOR = 0.368, 95% CI: 0.220– 0.615, P < 0.001).
Conclusion: This study generalized that most of the patients were poor adherent to their medications. Personal beliefs were found to influence medication adherence of the patients. Future studies could be needed to explore and identify how these factors affect patients’ medication adherence.
Keywords: chronic illnesses, cultural beliefs, personal beliefs, medication adherence, religious beliefs
Introduction
Adherence to properly prescribed medications is critical for patients with chronic disease conditions in order to prevent illness progression and death.1 According to the World Health Organization (WHO), only about half of all chronic disease patients take their medications adherently.2 Adherence to a medication regimen is usually defined as the extent to which patients take medications as recommended by their health care providers or when a person’s behavior is in line with medical advice.3 Since adherence to medications is a multifaceted behavioral process, it is critical that providers identify all potentially modifiable risk factors for low adherence.4 Many factors influence medication adherence, including patient demographics, treatment complexity, and disease conditions.5 Furthermore, psychological factors such as patients’ perceptions of medications and chronic conditions, such as disease severity, as well as social factors such as religious and cultural beliefs, may influence medication adherence behavior.1
Medication non-adherence is a worldwide challenge, with up to half of patients prescribed a medication for a chronic condition failing to take it as agreed with their doctor.2,6,7 Non-adherence to medication is the leading cause of preventable medical costs globally, and it is projected that people could save 4.6% of global healthcare costs (or $US 269 billion) if they adhere to their medication regimen.8
There is significant evidence that too many individuals with chronic illnesses, such as diabetes, hypertension, HIV/AIDS and asthma struggle to adhere to their prescribed regimens causing, the illness to be managed and controlled in a less than optimal manner.2
Adherence among chronic disease patients in developed nations is only 50% on average.9,10 Poor adherence is expected to have a greater impact in developing countries like Ethiopia due to a lack of health resources and inequities in access to health care.11 Beliefs about medicines are considered to play an important role in medication adherence; understanding an individual’s beliefs about their medicines, illness, and the controllability of their health offers a promising way to better comprehend non-adherence in patients with chronic diseases.12
Despite the fact that the importance of treatment adherence has been studied in Ethiopia, a review of the literature reveals several factors, such as age, income, race/ethnicity, health literacy, education, access/cost, and others may be associated with nonadherence. These factors, however, may not fully explain the variation in adherence. As a result, adherence research is focusing on other patient-level factors, such as personal, cultural, and religious beliefs about diseases, as well as the impact of medication-taking behaviors.
The patient-level factors impact on adherence was hardly studied in Ethiopia, to the best of the authors’ knowledge and search, especially in the study setting, and data are scarce. As a result, the goal of this study was to assess the impact of personal, cultural and religious beliefs on medication adherence among patients with chronic diseases that has follow-up at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. The finding may also help as a baseline and provide insight for further studies related to the impact of personal, culture and religion beliefs on medication adherence.
Material and Methods
Study Design and Setting
An institution-based cross-sectional study was conducted at the University of Gondar comprehensive specialized hospital (UoGCSH) from July to August, 2021. The UoGCSH is one of the country’s largest hospitals, and it is located in Gondar, about 750 km northwest of Addis Ababa (the capital city of Ethiopia). It has been serving more than 9 million populations with its catchment area including chronic care for patients with chronic illness.
Study Participants and Inclusion Criteria
All adult (age ≥18) patients with chronic disease attending at the chronic ambulatory units in UoGCSH were the source population, while all adult patients with chronic disease who were under follow-up during the data collection period at UoGCSH were in the study populations.
All adult patients with a chronic disease diagnosis confirmed by patients and verified by medical records, and who had been receiving pharmacologic treatment for at least 3 months, were included in the study, while patients with cognitive impairments that could interfere with communication or comprehension of the questions, patients with significant hearing impairments, and mentally ill or psychiatric patients were excluded. In addition, patients with more than one chronic illness with medications for each chronic illness were also excluded from the study.
Sample Size Determination and Sampling Techniques
A single population proportion formula was used to calculate the sample size. The following factors were considered when determining the sample size: Because no similar study had been conducted in the study area, 50% proportion (p = 0.5) of the prevalence of the outcome was considered in addition 95% confidence interval and margin of error 5% (d = 0.05) were used.

Where: n = sample size; p = prevalence of nonadherence, we use positive prevalence estimated, to maximize sample size. Negative prevalence = 1–0.5 = 0.5, d = degree of accuracy desired (margin of sampling error tolerated that is 5% (0.05)); Z = the standard normal value at a confidence interval of 95%=1.96; Computing with the above formula gives a total sample size of 384. The study enrolled 422 chronic disease patients after accounting for a 10% contingency for possible non-respondents.
Initially stratified sampling technique was used to include proportional participants from various chronic disease conditions, and then the study participants who met the inclusion criteria from each subgroup were chosen using a systematic random sampling technique with a lottery method. The expected number of chronic patients at chronic illness follow-up care during the average of the 3 months preceding the study was estimated to determine the number of participants in each stratum. A total of 2210 patients were estimated to have chronic illness follow-up care in the hospital in the 3 months prior to the study, with 900 on antihypertensive treatment, 700 on diabetes mellitus (DM) treatment, 400 on cardiac treatment (ischemic heart disease (IHD), heart failure (HF), stroke), 90 on chronic liver disease (CLD) treatment, 50 on chronic kidney disease (CKD) treatment, 50 on asthma treatment, and 20 on neurologic (Eg, Epilepsy) treatment. Based on this information, the required number of participants was selected proportionally and calculated as ni = Ni*n/N, where ni = disease condition required sample size; Ni = disease condition source sample size; n = total sample size; N = total population. As a result, 172 (40.8%) patients with HTN, 133 (31.5%) patients with DM, 76 (18%) patients with cardiac, 17 (4%) patients with CLD, 10 (2.4%) patients with asthma and CKD, and 4 (0.9%) patients with Neurology disorders were approached. The “K” value for the sampling interval was calculated as K = N/n, where “N” is the expected number of chronic patients’ average follow-up per month and “n” is the required final sample size. Since the data collection period was for one month after substituting 2210 for N, we find a sampling interval of five. As a result, participants were selected in every five-number intervals from the eligible individuals based on the patients’ record order as a sampling frame, which was listed in the follow-up appointment.
Dependent Variable and Independent Variables
Adherence of patients to their medications was the dependent variable whereas personal beliefs, cultural beliefs, religious beliefs, sociodemographic variables, like (sex, age, place of residence, marital status, ethnicity, educational status, income, occupational status, health insurance), and health-related variables, including (number of prescription pills per day, use of injection and inhalation routes of administration, duration of follow-up care, communication with the health providers, quality of health care, interference of medication in daily life), and patient-related variables, including (number of comorbidities and treatment duration of chronic disease, social drug use, adherence to exercise, level of independency, reminder type for drug dosing, knowledge about using medications) were independent variables.
Operational Definitions
Adherence: Adherence is the extent to which patients take medications as prescribed by their health care providers. In this study, adherence is categorized as an optimal or good adherence, when a total score of the seven-item Adherence to Refills and Medications Scale (ARMS-7) is equal to 7, while any score greater than 7 shows some degree of nonadherence or poor adherence.13
Personal belief: It is the extent of personal view or belief about medications they take. Personal belief questionnaire had four parts: the general overuse belief and the general harm belief, both of which contained four statements and the necessity and the concern beliefs, both of which contained five statements. Participants in this study were classified as having strong general-overuse medication belief, strong general harm belief, strong necessity belief, and strong concern belief if they scored above the mean on the general overuse medication belief, general harm belief, necessity belief, and concern belief, respectively, and weak believers were defined as participants who scored less than or equal to the mean for each type of belief.14
Cultural belief: is a set of behavioral patterns relating to attitudes, manners, and acts that members of society have embraced and handed on to generation after generation. The study participants’ cultural beliefs were assessed using a five-item Likert scale with nine statements adopted from various literatures.
Participants with a score of less than 50% were considered to be weak believers, while those with a score of 50–75% and greater than 75% were considered to have fair and strong cultural beliefs, respectively.
Family support: is a helpful hand provided by a family member to a relative suffering from a chronic disease. Family support is present if family members can assist by providing medical information, making time for emotional sharing, and preparing financial resources for disease treatments.15
Independent daily activity: is the ability to perform basic or personal care activities such as eating and drinking, dressing/undressing, using toilets, walking unassisted, going to bed/getting up, bathing/showering, as well as instrumental activities such as telephone use, mobility (travel), shopping, meal preparation, housework, medication management, and money management. Individuals who require assistance with some or all activities or who require some support from another person on a regular basis will be classified as dependent on daily living activities.16,17
Self-perceived quality of health care: is patient’s sense of obtaining proper health-care services in a technically competent manner, with effective communication, collaborative decision-making and cultural sensitivity while avoiding harm.18
Patient-provider communication: is present when patients perceive a mutually understood and shared transmission of information with their health-care practitioner whether verbally or nonverbally.19
Self-Perceived Quality of Life: Patients’ subjective judgment or perception of overall happiness or satisfaction with life.20
Religious belief: Participants who scored higher than the mean on religious belief statements of the Spiritual Perspective Scale (SPS) were considered to have strong religious beliefs, while those who scored lower or equal to the mean were considered to have weak religious beliefs.21
Data Collection Procedure and Quality Control
Data Collection Tools and Procedures
A pretested, structured, interviewer-administered questionnaire was used to collect the data. Data collection tool was prepared from previewed journals and it had 4 parts. Part one of the tool included the participants’ socio-demographic characteristics such as age, gender, residence, religion, ethnicity, income, marital status, educational status, occupational status, and health insurance status. The second part addressed patient clinical characteristics that are related to therapy and health. The patient-related variables include social drug use, alcohol consumption, cigarette smoking, exercise, level of independency, reminder type for drug dosing, knowledge about using medications and self-perceived overdosing and quality of life. The third section contained the seven-item Adherence to Refills and Medications Scale (ARMS-7) to determine the participants’ level of medication adherence; participants were asked to report on the medications they had been taking for at least three months to treat their chronic medical condition. The tool is used to assess the medication adherence regardless of the types of medications the patient is taking. The level of drug adherence was classified as either good or poor. Participants who scored seven out of seven items had good medication adherence, while those who scored more than seven had poor medication adherence. The fourth part of the data collection tool includes questioners about personal, cultural and religious beliefs. All personal, cultural, and religious beliefs were evaluated on a 5-point Likert scale, with 1 to 5 points denoting strongly disagree, disagree, neutral, agree, and strongly agree.
Data Quality Assurance
The investigators developed the questionnaire in English, and then local language translation was done by Amharic and English-speaking individuals to ensure consistency. On the basis of the translation, necessary changes were made to the instrument. The questionnaire’s completeness and readiness were pretested before the actual data collection began. Three graduating pharmacy students who were trained on the data collection tool, questionnaire technique, and ethical issues collected the data. The questionnaire’s quality was assured by having the data collector check the questionnaire’s completeness and consistency at each step of the data collection process, as well as during data entry. Prior to the actual data collection, the questionnaire was pretested on 5% of the study subjects to assess its clarity and socio-cultural compatibility. The results of the pretest were not used in the final study. The internal consistency of the adherence questionnaire was validated and had a Cronbach’s alpha of 0.802. Moreover, the internal consistency and reliability of the personal, cultural and religious beliefs questioners were examined and resulted in a Cronbach’s alpha of 0.81, 0.72 and 0.75, respectively.
Data Processing and Analysis
After the collected data was cleaned, coded and entered analysis was carried out using statistical package for social science (SPSS) version 25 software. Frequency and percentage were computed for categorical variables and mean with standard division was used for continuous variables. Some continuous variables were changed into categorical variables either aimed at good presentations for the reader or to measure the association of their categories with outcome variables. For instance, age, monthly income, number of prescriptions and comorbidities were categorized based on the cut points of previous literatures. Bivariate and multivariate logistic regression analyses were used to determine variables associated with poor adherence of medications. Variables with P≤ 0.2 in the bivariate analysis were entered into multivariables for further analysis to identify associated factors of medication adherence. Then, the findings represent the association after controlling for the other variables. An adjusted odds ratio (AOR) at 95% confidence interval (CI) with P-value ≤0.05 was considered to be statistically significant. To determine the model fit of each variable in a logistic regression model, the Hosmer and Lemeshow goodness-of-fit test was used.
Ethical Considerations
The study was carried out in line with the Helsinki Declaration. All participants were given written informed consent after the study’s nature properly explained verbally, and participation was voluntary. The Institutional Review Board of the University of Gondar College of Medicine and Health Sciences granted ethical clearance with the reference number of SOP/272/2013. Furthermore, the confidentiality and privacy of the information obtained from the patient’s records were actively protected.
Results
Socio-Demographic Characteristics and Enrollment of the Study Participants
Out of the 422 approached patients with chronic disease, 404 participants took part in the final study with a response rate of 95.7% (Figure 1). More than half (51%) of the participants were males with the mean (±SD) age of 47.9 (±14.8) years. Around two third of the study participants (64.9%) resided in urban areas. Regarding a stream of the education level, close to one-third (31.2%) of the respondents were unable to read and write and at least 8 out of 10 respondents were Orthodox Christian. Moreover, below one-third (29%) of participants were private workers and a higher proportion of the study participants (27.7%) had monthly income less than 1500 Ethiopian birr (Eth. birr) (Table 1).
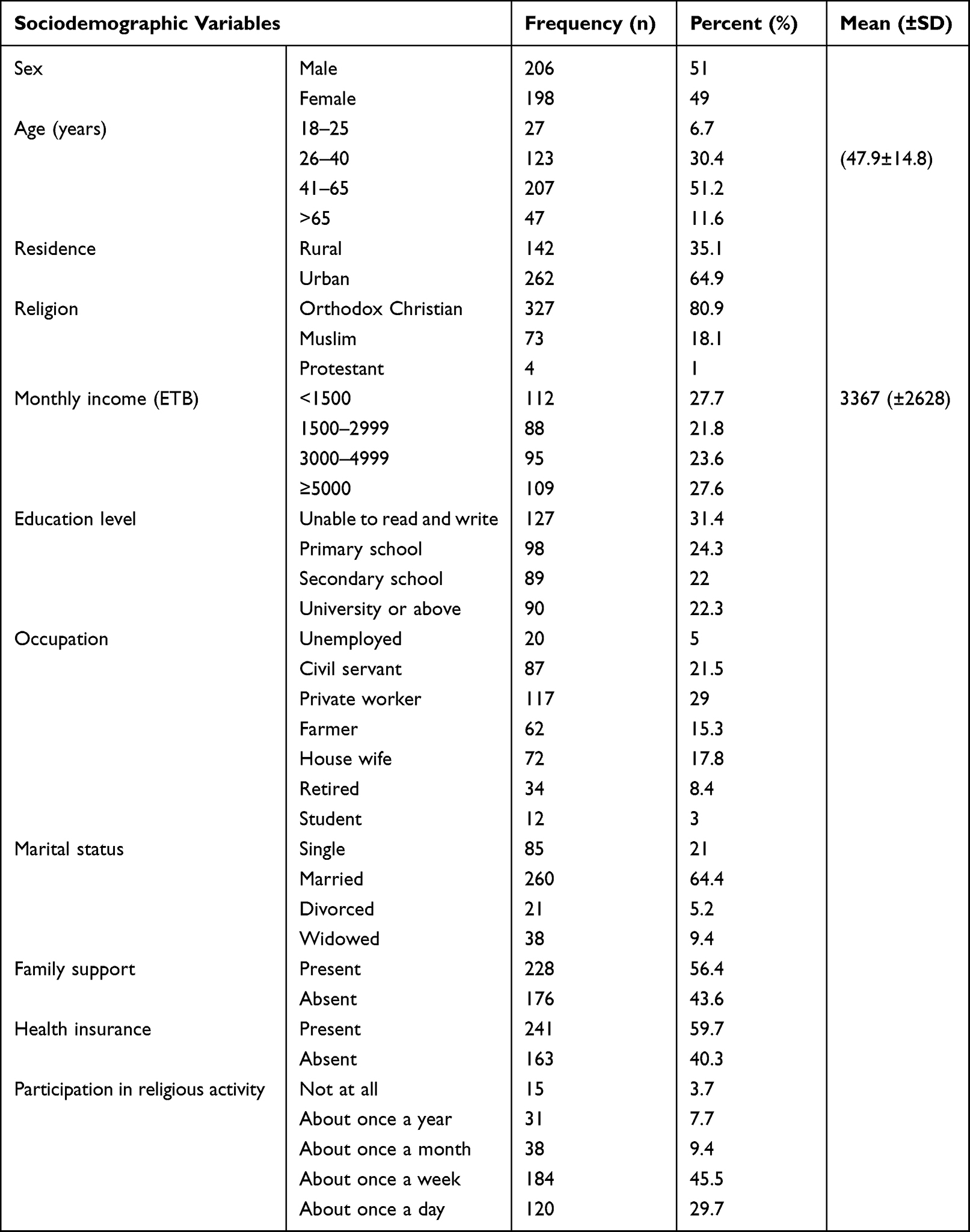 |
Table 1 Sociodemographic Features of Patients Attending Chronic Care Clinic at UoGCSH, North West Ethiopia, 2021 (N = 404) |
 |
Figure 1 The sampling procedures of study participants from different chronic disease conditions attending chronic care follow up at University of Gondar Comprehensive and Specialized Hospital, North West Ethiopia. |
Study Participants’ Personal and Clinical Characteristics
Most of the study participants (92.3%) were nonsmoker and more than two-thirds (69.8%) did not drink alcohol. The majority of the participants were capable of doing their daily activity independently. Almost 60% of the participants did not use any kind of medication reminder. The majority of study participants (68.1%) had a single chronic disease, with hypertension (41.1%) being the most common. More than half of the participants had a disease duration of less than 5 years (range: 1–32 years). The mean duration of treatment was 7.1± (5.9) year (range, 1–32 years). Majority of the respondents (72.5%) received 1–2 medications (range 1–6) per day. Around two-thirds of the patients (64.1%) had monthly treatment follow-up. In terms of patient-provider communication, nearly all patients (96%) reported to have good communication and a positive perception of the quality of care (Table 2).
 |
Table 2 Patient and Therapy Related Clinical Characteristics of the Study Participants Attending Chronic Care Clinic at UoGCSH, North West Ethiopia |
Personal, Cultural and Religious Beliefs Towards Medication Adherence
From the perspective of general overuse belief, the mean (±SD) belief score was 2.4 (±0.6) on a 5-point Likert scale. Higher proportions of participants disagreed (61.9%) and strongly disagreed (16.1%) in that doctor use too many medicines. From the general harm beliefs, the mean (±SD) score was 1.9 (±0.7) out of 5 points. In regard to the necessity beliefs, the mean (±SD) score was 3.7 (±0.8) out of 5 points and most (60.6%) of patients agreed in the statement that my health at present depends on my medicines. The mean (±SD) score was 3.0 (±0.8) out of 5 points for the concern belief and near half (49.3%) disagreed on the statement that having to take these medications worries me and about 43.6% worried on the long-term effects of their medicines (Table 3). Overall, the majority of the participants had weak belief towards general overuse (85.1%), general harm belief (95%) and concern belief (61.6%) about their medications. But most of the participants (78.8%) believed strongly regarding necessity belief of medications.
 |
Table 3 Personal Beliefs of Chronic Disease Patients Attending Chronic Care Clinic at UoGCSH, North West Ethiopia |
The mean (±SD) score of respondents for cultural belief towards their medication was 2.5 (±0.5) on 5-point Likert scale with most (81.7%) of the participants had weak cultural belief, and 2.7% and 15.6% had fair and strong beliefs, respectively. Majority (55%) of the respondents were agreed on following doctor’s order is the best way to keep disease condition from getting any worse and most of the patients (58.9%) do not believe in the effectiveness of traditional medicines for their disease. And the majority of the patients had weak beliefs that disease condition is a punishment for bad behaviors and illness will improve by casting spells on food, drink or other objects (Table 4).
 |
Table 4 Cultural Beliefs on Their Medications Among Chronic Disease Patients Attending UoGCSH, North West Ethiopia |
The majority of the participants (93.8%) had strong religious belief with the mean (±SD) score of 3.9 (±0.5) on 5-point Likert scale. A greater portion of the patients agreed and/or strongly agreed on statements of religious beliefs (Table 5).
 |
Table 5 Religious Beliefs on Their Medications Among Chronic Disease Patients Attending UoGCSH, North West Ethiopia |
Level of Adherence Among the Study Participants
Overall, the majority of study participants (59.4%) had good adherence to their medications in this study, while others were depicted under poor medication adherence (Figure 2) (Table 6).
 |
Table 6 Level of Adherence Among the Study Participants |
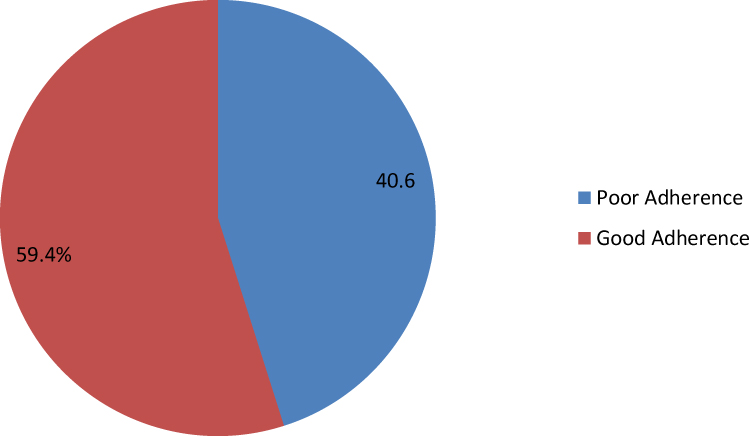 |
Figure 2 Level of Adherence among patients attending chronic care clinic at University of Gondar Comprehensive and Specialized Hospital, North West Ethiopia. |
Association of Personal, Cultural and Religious Belief with Medication Adherence
The multivariable logistic regression model revealed that patients having strong belief on harm of medications were found to be four times more likely to have poor medication adherence than those having weak belief on harm of medications (AOR=4.027, 95% CI:1.232–13.161, P = 0.021). In contrast, patients who had a strong personal belief regarding the necessity of medications were found to have a significantly lower likelihood of poor medication adherence (AOR = 0.368, 95% CI: 0.220–0.615, P < 0.001) (Table 7).
 |
Table 7 Association of Personal, Cultural and Religious Beliefs with Medication Adherence |
Association of Socio-Demographic and Clinical Factors with Medication Adherence
According to the multivariable logistic regression model, patients who were female, and had quarterly follow-up frequencies, good communication with health providers and were active on physical exercise had a significantly lower likelihood of poor medication adherence than those who were male, had monthly follow-ups, poor communication, and were not active towards physical exercise, respectively (Table 8).
 |
Table 8 Association of Socio-Demographic and Clinical Characteristics with Medication Adherence |
Discussion
The study was intended to investigate the impact of personal, cultural and religious beliefs on medication adherence among chronic disease patients. Additionally, this study demonstrated the association of patient socio-demographic and clinical characteristics with level of adherence. This study revealed that 40% of the participants were poor adherent to their medications, which is lower than the worldwide estimate of 50% put forward by the WHO.10,14 Our findings suggest that the majority of chronic disease patients who take their medications as prescribed believe they are necessary; strong belief in medication necessity is linked to good adherence in this patient population. This finding was similar to previous studies that suggest people who do not perceive a need for medication or who have strong reservations about taking it are more likely to forget to take it and become less adherent.22–24
In this study, there was a significant association of general-harm beliefs about medicines with medication adherence; the patients with a high score of general harm beliefs had more negative views about medicines as a whole and a tendency to see medicines as fundamentally harmful and addictive poisons, and they were more likely nonadherent to their medications, which is consistent with other study done in Palestine.22 This suggests that certain personal beliefs and aspects might affect harm beliefs and thereby influence medication adherence.
Non-adherence of medications in chronic illness patients was linked to patients who were more concerned about their medications in a Chinese study.24 Similar findings were found in Kuwait, which showed that negative beliefs about medications have a significant negative impact on chronically ill patients’ adherence to their treatment regimen.22 However, our findings showed that there is no significant association between specific concern and medication adherence, in contrast to those findings.
Concerns about the negative effects of anti-diabetic medications, as well as beliefs that medicines in general are essentially harmful, were found to be significantly associated with non-adherence in a study conducted in Palestine.23 Similar to these findings, patients with a strong belief about the harmful effects of medicines were found to be less adherent in our study than those with a weak belief in harm.
In our study, culture had no significant association with medication adherence, this may be due to the fact that perceived cultural beliefs were measured only by general statements, such as “Luck plays a big part in determining how my disease condition improves” and adapted from the 7 items Traditional Chinese Health belief which were not specific to treatment seeking and/or medication taking behaviors.25 The study’s findings, however, do not imply that there is no relationship between culture and medication adherence; cultural beliefs may influence medication adherence behavior in different populations depending on the culture involved.
In addition, patients with stronger beliefs in the effectiveness and safety of traditional Medication and traditional health beliefs were found to be less likely to be adherent to their medication, this is similar with another study investigating Asian Asthmatic perception behaviors and the association with medication adherence, which found patients with low adherence were more likely to believe that using traditional herbal medicines is safer than inhalers.26
Even if there is no significant relationship between cultural beliefs and medication adherence, the majority of patients who scored high in the cultural questions had poor medication adherence 138 (84.1%). Those who scored low had a high level of medication adherence 209 (87.1%). This could be because many patients agreed that they sought treatment and took medication according to a doctor’s orders, and many who do not believe that traditional medicines are more beneficial than modern medicines are more likely to be adherent.
In our study almost half (49.5%) of respondents were attending church at least once a week, but high religious score or reading spiritually related material had no association with medication adherence. In line with this finding, a study carried out in the USA, focusing on Christian black women, found that attending church, praying and reading Bible/religious material, and having strong religious beliefs were not significantly associated with medication adherence.27 In contrast to this finding in relation to spiritual beliefs, a study conducted in Ethiopia, report that the healing potential of holy water was associated with non-adherence to ART.28 A similar study from Ghana found that in hypertensive patients, religiosity was associated significantly with medication nonadherence.21 Similarly, according to a study carried out in Saudi Arabia, people who reported that they could follow their medication regimen and perceived that God controls their health and illness, were found to have good adherence to taking their medication.29
The current study also demonstrated the association of socio-demographic and clinical characteristics of the patients with medication adherence. In consistent with the previous study,30 female patients were found to be less likely to have poor medication adherence than male patients. This could be because, according to previous studies, men are more prone to forgetting to their medications, which could make it more difficult to remember and take medications as prescribed for a long time. There was no age difference observed in the effect of adherence in the current study. Other socio-demographic characteristics were also not associated with medication adherence level in this study.
Our findings also revealed that patients who received biannual or quarterly follow-up care were less likely to be nonadherent to their medications than those who received monthly follow-up care. This could be due to the fact that patients who visit the hospital on a monthly basis have serious complications and a low quality of life, and they may not take their medications appropriately as directed. Moreover, patients who had good communication with health care providers were found to be less likely to have poor medication adherence. The finding is in agreement with studies that stated communication between patients and healthcare providers aids in the formation of positive beliefs about treatment options.31,32 This could be due to enhancement of patients’ involvement in decision-making, and taking into account patients’ preference to improve medication adherence. This allows health care professionals and patients to identify gaps, misunderstandings, and misconceptions in the patient’s perceptions. Patients who have faith in their healthcare provider are unlikely to believe that the medication is being misused.
The current study has some limitations. Firstly, due to the cross-sectional nature of the study, different beliefs were studied as reported by the patients, which reflected the responses could be subjected to recall and social desirability bias. Furthermore, the study uses patients’ self-report to evaluate medication adherence, which may be affected by recall bias and could introduce an under- or over-reported rate of medication adherence.
Generally, the current study highlighted the impact of personal, cultural and religious beliefs towards medication adherence in patients with chronic illness. Indeed, the findings of this study may have significant implications for focusing on patients’ personal beliefs in order to improve adherence, particularly for chronic disease patients with poor medication adherence. Additionally, it also examined the association of certain socio-demographic and clinical characteristics with medication adherence. The findings may be helpful for tailored interventions considering patients' personal, cultural and religious beliefs in conjunction with socio-demographic and clinical variables. Furthermore, the study may be a benchmark for future researchers in the area with a prospective approach in large-sized sample population.
Conclusion
This study concluded that the overall medication adherence in chronic patients is low. Personal beliefs were significantly associated with level of medication adherence. Indeed, the findings of this study may have significant implications for focusing on patients’ personal beliefs in order to improve adherence, particularly for chronic disease patients with poor medication adherence. Future research could look into the association between the level of medication adherence and predictor subjective belief variables in patients with chronic illnesses.
Abbreviations
ARMS, adherence to refills and medications scale; BMQ, Beliefs about Medicines questionnaire; CKD, Chronic kidney disease; CLD, Chronic liver disease; HTN, Hypertension; UoGCSH, University of Gondar Comprehensive and Specialized Hospital; WHO, World Health Organization.
Data Sharing Statement
All necessary data are available from the manuscript. We will share the available dataset if required.
Acknowledgments
The authors would like to thank the data collectors and the study participants, as well as the University of Gondar’s college of medicine and health science, for providing and approving the study’s ethical clearance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Hatah E, Lim KP, Ali AM, Shah NM, Islahudin F. The influence of cultural and religious orientations on social support and its potential impact on medication adherence. Patient Prefer Adherence. 2015;9:589. doi:10.2147/PPA.S79477
2. Sabaté E, Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003.
3. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
4. Brown MT, Bussell J, Dutta S, Davis K, Strong S, Mathew S. Medication adherence: truth and consequences. Am J Med Sci. 2016;351(4):387–399. doi:10.1016/j.amjms.2016.01.010
5. Gellad WF, Grenard JL, Marcum ZA. A systematic review of barriers to medication adherence in the elderly: looking beyond cost and regimen complexity. Am J Geriatr Pharmacother. 2011;9(1):11–23. doi:10.1016/j.amjopharm.2011.02.004
6. Bender BG, Rand C. Medication non-adherence and asthma treatment cost. Curr Opin Allergy Clin Immunol. 2004;4(3):191–195. doi:10.1097/00130832-200406000-00009
7. Fischer MA, Stedman MR, Lii J, et al. Primary medication non-adherence: analysis of 195,930 electronic prescriptions. J Gen Intern Med. 2010;25(4):284–290. doi:10.1007/s11606-010-1253-9
8. Aitken M, Gorokhovich L. Advancing the responsible use of medicines: applying levers for change. SSRN Electron J. 2012. doi:10.2139/ssrn.2222541
9. Haynes RB, McDonald HP, Garg A, Montague P. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. 2002;2. doi:10.1002/14651858.CD000011
10. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:1–12. doi:10.1155/2015/217047
11. Horne R. Compliance, adherence, and concordance: implications for asthma treatment. Chest. 2006;130(1):65S–72S. doi:10.1378/chest.130.1_suppl.65S
12. LaBine N. Teaching the Spiritual Dimension of Nursing Care: A Survey of Associate Degree Nursing Programs in the Southeast United States. East Tennessee State University; 2015.
13. Kripalani S, Goggins K, Nwosu S, et al. Medication nonadherence before hospitalization for acute cardiac events. Journal of Health Communication. 2015;20(sup2):34-42. doi:10.1080/10810730.2015.1080331
14. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86:304–314. doi:10.4065/mcp.2010.0575
15. Kamaryati NP, Malathum P. Family support: a concept analysis. Pac Rim Int J Nurs Res. 2020;24(3):403–411.
16. PoplasSusič A, Klemenc-Ketiš Z, Blagus R, RužićGorenjec N. Factors that determine dependence in daily activities: a cross-sectional study of family practice non-attenders from Slovenia. PLoS One. 2021;16(1):e0245465. doi:10.1371/journal.pone.0245465
17. Rubio E, Lázaro A, Sánchez-Sánchez A. Social participation and independence in activities of daily living: a cross sectional study. BMC Geriatr. 2009;9(1):1–11. doi:10.1186/1471-2318-9-26
18. Weigl M, Schneider A. Associations of work characteristics, employee strain and self-perceived quality of care in emergency departments: a cross-sectional study. Int Emerg Nurs. 2017;30:20–24. doi:10.1016/j.ienj.2016.07.002
19. Patak L, Wilson-Stronks A, Costello J, et al. Improving patient-provider communication: a call to action. J Nurs Adm. 2009;39(9):372. doi:10.1097/NNA.0b013e3181b414ca
20. N’Goran AA, Déruaz-Luyet A, Haller DM, et al. Comparing the self-perceived quality of life of multimorbid patients and the general population using the EQ-5D-3L. PLoS One. 2017;12(12):e0188499. doi:10.1371/journal.pone.0188499
21. Kretchy I, Owusu-Daaku F, Danquah S. Spiritual and religious beliefs: do they matter in the medication adherence behaviour of hypertensive patients? Biopsychosoc Med. 2013;7(1):1–7. doi:10.1186/1751-0759-7-15
22. Lemay J, Waheedi M, Al-Sharqawi S, Bayoud T. Medication adherence in chronic illness: do beliefs about medications play a role? Patient Prefer Adherence. 2018;12:1687. doi:10.2147/PPA.S169236
23. Sweileh WM, Sa’ed HZ, Nab’a RJA, et al. Influence of patients’ disease knowledge and beliefs about medicines on medication adherence: findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. BMC Public Health. 2014;14(1):1–8. doi:10.1186/1471-2458-14-94
24. Wei L, Champman S, Li X, et al. Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: a cross-sectional study in China. BMJ open. 2017;7(10):e017293. doi:10.1136/bmjopen-2017-017293
25. Eh K, McGill M, Wong J, Krass I. Cultural issues and other factors that affect self-management of type 2 diabetes mellitus (T2D) by Chinese immigrants in Australia. Diabetes Res Clin Pract. 2016;119:97–105. doi:10.1016/j.diabres.2016.07.006
26. Chiu K-C, Boonsawat W, Cho S-H, et al. Patients’ beliefs and behaviors related to treatment adherence in patients with asthma requiring maintenance treatment in Asia. J Asthma. 2014;51(6):652–659. doi:10.3109/02770903.2014.898772
27. Abel WM, Greer DB. Spiritual/religious beliefs & medication adherence in black women with hypertension. J Christ Nurs. 2017;34(3):164–169. doi:10.1097/CNJ.0000000000000333
28. Tymejczyk O, Hoffman S, Kulkarni SG, et al. HIV care and treatment beliefs among patients initiating antiretroviral treatment (ART) in Oromia, Ethiopia. AIDS Behav. 2016;20(5):998–1008. doi:10.1007/s10461-015-1184-x
29. Albargawi M, Snethen J, Al Gannass A, Kelber S. Relationship between person’s health beliefs and diabetes self-care management regimen. J Vasc Nurs. 2017;35(4):187–192. doi:10.1016/j.jvn.2017.07.002
30. Gadkari AS, McHorney CA. Unintentional non-adherence to chronic prescription medications: how unintentional is it really? BMC Health Serv Res. 2012;12(1):1–12. doi:10.1186/1472-6963-12-98
31. Butow P, Sharpe L. The impact of communication on adherence in pain management. Pain®. 2013;154:S101–S7. doi:10.1016/j.pain.2013.07.048
32. Delamater AM. Improving patient adherence. Clin Diabetes. 2006;24(2):71–77. doi:10.2337/diaclin.24.2.71
33. Gökdoğan F, Kes D. Validity and reliability of the Turkish Adherence to Refills and Medications Scale. nt J Nurs Pract. 2017;23(5):e12566. doi:10.1111/ijn.12566.33
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.