")
Back to Journals » Patient Preference and Adherence » Volume 8
Impact of patient satisfaction ratings on physicians and clinical care
Authors Zgierska A, Rabago D, Miller M
Received 12 December 2013
Accepted for publication 23 January 2014
Published 3 April 2014 Volume 2014:8 Pages 437—446
DOI https://doi.org/10.2147/PPA.S59077
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Aleksandra Zgierska,1 David Rabago,1 Michael M Miller2–4
1Department of Family Medicine, University of Wisconsin-Madison, School of Medicine and Public Health, Madison, WI, 2American Society of Addiction Medicine, Chevy Chase, MD, 3Department of Psychiatry, University of Wisconsin-Madison, School of Medicine and Public Health, 4Herrington Recovery Center, Rogers Memorial Hospital, Oconomowoc, WI, USA
Background: Although patient satisfaction ratings often drive positive changes, they may have unintended consequences.
Objective: The study reported here aimed to evaluate the clinician-perceived effects of patient satisfaction ratings on job satisfaction and clinical care.
Methods: A 26-item survey, developed by a state medical society in 2012 to assess the effects of patient satisfaction surveys, was administered online to physician members of a state-level medical society. Respondents remained anonymous.
Results: One hundred fifty five physicians provided responses (3.9% of the estimated 4,000 physician members of the state-level medical society, or approximately 16% of the state's emergency department [ED] physicians). The respondents were predominantly male (85%) and practicing in solo or private practice (45%), hospital (43%), or academia (15%). The majority were ED (57%), followed by primary care (16%) physicians. Fifty-nine percent reported that their compensation was linked to patient satisfaction ratings. Seventy-eight percent reported that patient satisfaction surveys moderately or severely affected their job satisfaction; 28% had considered quitting their job or leaving the medical profession. Twenty percent reported their employment being threatened because of patient satisfaction data. Almost half believed that pressure to obtain better scores promoted inappropriate care, including unnecessary antibiotic and opioid prescriptions, tests, procedures, and hospital admissions. Among 52 qualitative responses, only three were positive.
Conclusion: These pilot-level data suggest that patient satisfaction survey utilization may promote, under certain circumstances, job dissatisfaction, attrition, and inappropriate clinical care among some physicians. This is concerning, especially in the context of the progressive incorporation of patient satisfaction ratings as a quality-of-care metric, and highlights the need for a rigorous evaluation of the optimal methods for survey implementation and utilization.
Keywords: physician satisfaction, quality of care, patient experience of care, health services
Introduction
Patient experience of care, or “satisfaction”, is a crucial element of patient-centered care, the implementation of which has become the focus of wide-scale efforts aimed at improving health and health-care delivery.1–3 Results from patient satisfaction surveys can facilitate positive change and quality improvement (QI) initiatives in health-care delivery that are responsive to patients’ needs. Data support the potential benefits of high patient satisfaction; satisfied patients can have increased treatment adherence and may improve health outcomes.4,5
However, several studies have also raised concerns suggesting the use of patient satisfaction ratings as a quality-of-care marker may be associated with unexpected, undesirable outcomes.6,7 A prospective cohort study of a representative sample of US adults (N=51,946) found that, when compared with those least satisfied, the most satisfied patients had 12% higher odds of hospital admission, 9% greater expenditures for both health services and prescription drugs, and a 26% higher mortality risk, which increased to 44% when additionally adjusted for baseline health status and comorbidities.6 Because patients’ treatment satisfaction may rely more on their perception of met expectations than on objective medical outcomes,7–12 one possible explanation for such findings can be that the pursuit of and incentivizing high survey scores may encourage inappropriate medical practices.13,14
Incentivizing clinicians to meet patient satisfaction score “benchmarks” has become common and stirred heated debates in the professional and lay press.13–25 However, formal evaluation of the effects of patient satisfaction ratings on clinicians and clinical practice patterns is lacking. The goal of this project, therefore, was to assess physicians’ perceptions about the impact of patient experience of care surveys on their job satisfaction and clinical practice.
Methods
Design
This was a cross-sectional electronic survey study, conducted by a state-level medical society. Survey responses were received by the authors as de-identified aggregate data. Because the manuscript preparation did not involve human subjects as defined by federal regulations and the authors were not involved in the design or conduct of this project, the study was determined to be exempt from review by an institutional review board.
Setting and population
Active physician members of a state medical society, regardless of specialty or practice setting, were invited to complete the survey.
Protocol
In 2011, officials in the medical society of a US state noted receiving substantial spontaneous feedback from its members voicing concerns that incorporation of patient experience of care ratings into the “benchmarking” processes (ie, tying them to clinician compensation, bonuses, contract lengths, and even continuation of employment) promoted physician job dissatisfaction and inappropriate clinical practices (personal communication). After a review of existing anecdotal and limited research evidence, the society’s staff and invited consultants developed a 26-question QI survey. Between March and July 2012, the state medical society sent an invitation and six follow-up reminders via email to its approximately 4,000 active physician members to participate in the anonymous online survey hosted by Survey Monkey®. The invitation was also distributed through announcement in a weekly electronic newsletter and a posting on the society’s website and social media sites (Facebook®, Twitter®).
Outcome measures
The 26-item survey inquired about respondents’ demographics and their perceptions about the influence of patient experience of care surveys on job satisfaction and clinical care. Items 1–25 called for demographic information and quantitative responses (“Yes/No/I don’t know” or ordinal response scale answers). Item 26 asked respondents to address the statement: “Please provide us with any additional details that you would like to share.”
Data analysis
The authors adapted a standard method to analyze the first-person qualitative data26 provided in item 26 of the survey. Each respondent’s qualitative comments were reviewed individually by each of the first two authors using a standardized worksheet. They were then discussed by the authors in three meetings over 6 weeks using a consensus approach to identify and code major themes. Disagreements were resolved by consensus. SurveyMonkey® (SurveyMonkey, Palo Alto, CA, USA) was used for data compilation and descriptive statistics. Due to the small sample size and low response rate, no comparisons between subgroups were conducted.
Results
The survey was completed by 155 respondents (response rate 3.9% among the estimated 4,000 active physician members of the society, and 16% among the estimated 551 active emergency medicine physicians in the state in 2012). All respondents completed the demographic portion of the survey; 131 physicians responded to items about the influence of patient satisfaction surveys. Qualitative responses were provided by 52 physicians.
The majority of the 155 respondents were men (84.5%) who were locally practicing physicians (96.1%). Almost all (96.1%) reported that their hospital or employer utilized patient experience of care surveys. Almost half (43.2%) were hospital employed, 34.8% worked in a private group practice, 9.7% in a solo practice, and 14.8% in an academic medical center practice setting (Table 1). The respondents represented multiple specialties. The largest set of respondents comprised emergency department (ED) physicians (56.8% of respondents or 16% of the state’s ED physicians), followed by primary care (16.1%: family medicine, internal medicine, and pediatrics), and obstetrics/gynecology (3.9%). Eleven percent indicated “other medical specialty” and 11% indicated “other surgical specialty” (Table 1).
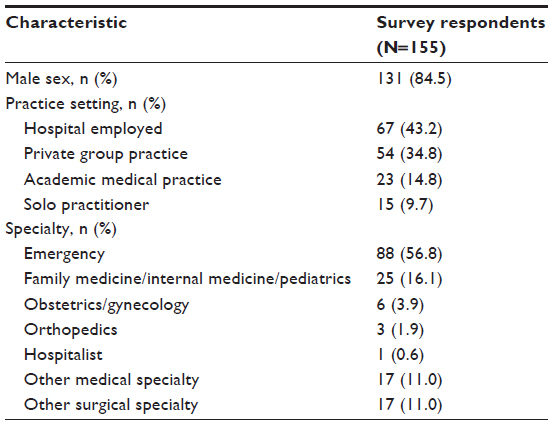 | Table 1 Sample characteristics by sex, practice setting, and specialty |
Fifty-two physicians provided qualitative comments. Analysis identified several themes in these responses, as summarized in Table 2. Six physicians provided neutral (N=3) or positive (N=3) feedback regarding the use of patient satisfaction surveys. The three positive statements noted that written patient comments could be useful but that numerical scores of patient experience of care were not helpful for practice improvement initiatives. The remaining 46 responses presented a negative view of the survey impact on clinicians and their practices, with responses falling into one of five main themes. Theme 1 (N=28) was that patient satisfaction surveys were viewed as a poor surrogate measure of the quality of medical care. Regarding patient satisfaction survey methodology, physicians (N=18) expressed concerns about the validity and reliability of satisfaction surveys due to skewed sampling methods that excluded or potentially over-sampled certain clinical populations (eg, patients admitted from the ED to the hospital did not complete surveys about their ED care; multiple surveys could be completed by those who frequent EDs, with some patients potentially using the surveys as a tool to achieve their goals such as “drug seeking”) or the respondent sample size often being too small to draw statistically meaningful conclusions regarding a particular physician’s care. In addition, physicians believed it was not appropriate for patients to rate the physician’s medical judgment or management (N=6) and that surveys made them feel like “minor service providers” rather than highly trained professionals (N=5). Theme 2 was the physicians’ perception that patient satisfaction surveys promoted inappropriate medical practices (N=16), including inappropriate prescribing of opioids (N=10) and antibiotics (N=4). Theme 3 was that too much weight was placed on patient satisfaction survey results while not enough administrative effort was dedicated toward improving medical care and outcomes (N=13). Although physicians acknowledged that evaluating patient satisfaction is important, they felt “the pendulum had swung too far” (N=9), and expressed frustration about unsatisfactory responses from administrators to physicians’ survey-related concerns (N=8). Theme 4 described physicians’ dilemmas and frustration with a perceived “conflict of interest” (N=12) between the need to generate high satisfaction scores and the need to provide high-quality medical care, especially when clinician salaries were tied to the survey scores, thus potentially promoting inappropriate practices to “boost” satisfaction scores (N=6), or when appropriate medical care may result in an unhappy patient (N=6). Finally, ten respondents viewed patient satisfaction surveys as a “punitive tool” used against physicians (Theme 5), with four respondents expressing fear of losing their job in relation to patient satisfaction survey results.
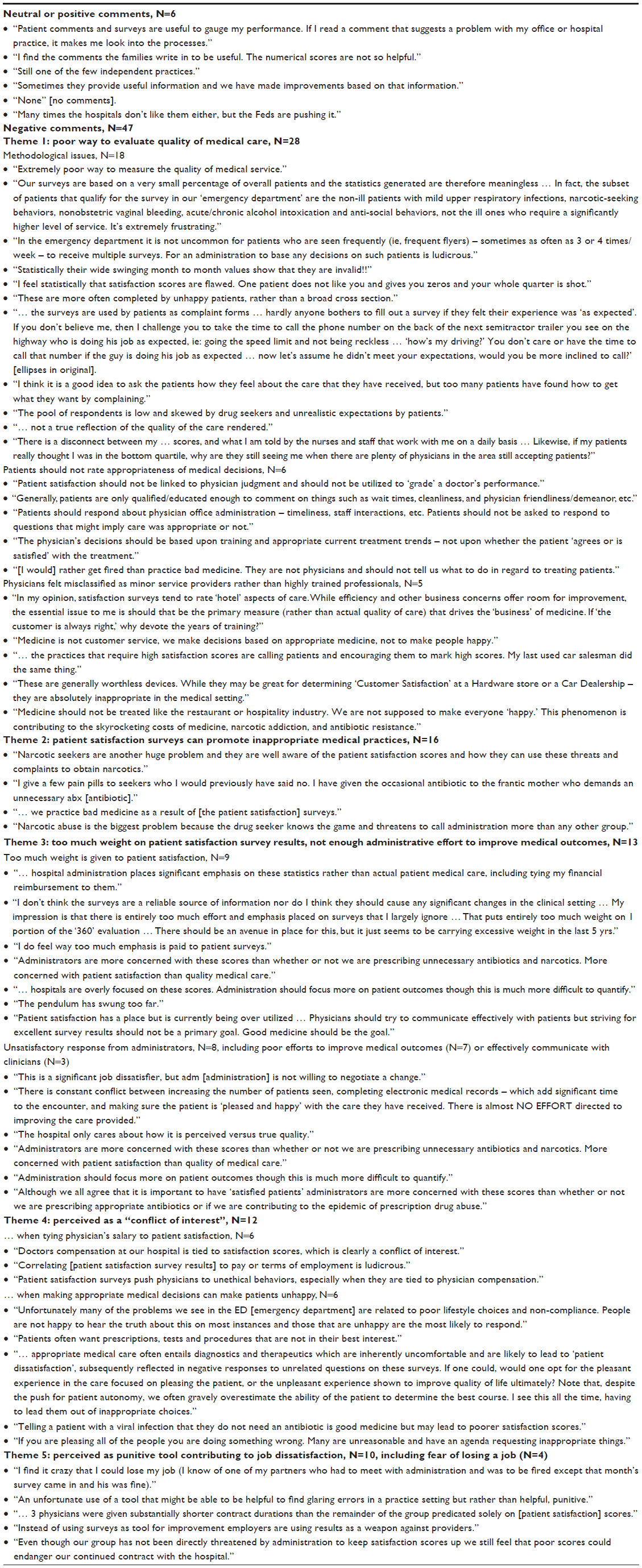 | Table 2 Selected qualitative physician (N=52) responses* to the question: “Please provide us with any additional details you would like to share” |
Table 3 summarizes responses (N=131) regarding the implementation and use of patient satisfaction surveys. When asked how many times in the past 6 months they were provided the results of patient satisfaction surveys, many physicians reported not knowing about such results (45%) or reported receiving summary data pooled from 20 or fewer surveys (29.8%). Most of the respondents (61.8%) did not know the patient satisfaction survey response rate for their hospital or practice. The majority reported not knowing their average “raw score” or percentage rank (62.6% and 53.4%, respectively). Over one-third of clinicians reported not knowing their hospital or practice targets for “excellent” scores or percentile rank for patient satisfaction ratings; almost half of the respondents (44.2%) stated their belief the target was set at 90% or above. Over half (58.8%) reported that part of their compensation was tied to patient satisfaction survey results. Approximately half of respondents also stated they were able to get copies of completed patient satisfaction surveys (48.9%) and had approached their employer in the past to discuss these surveys (56.5%).
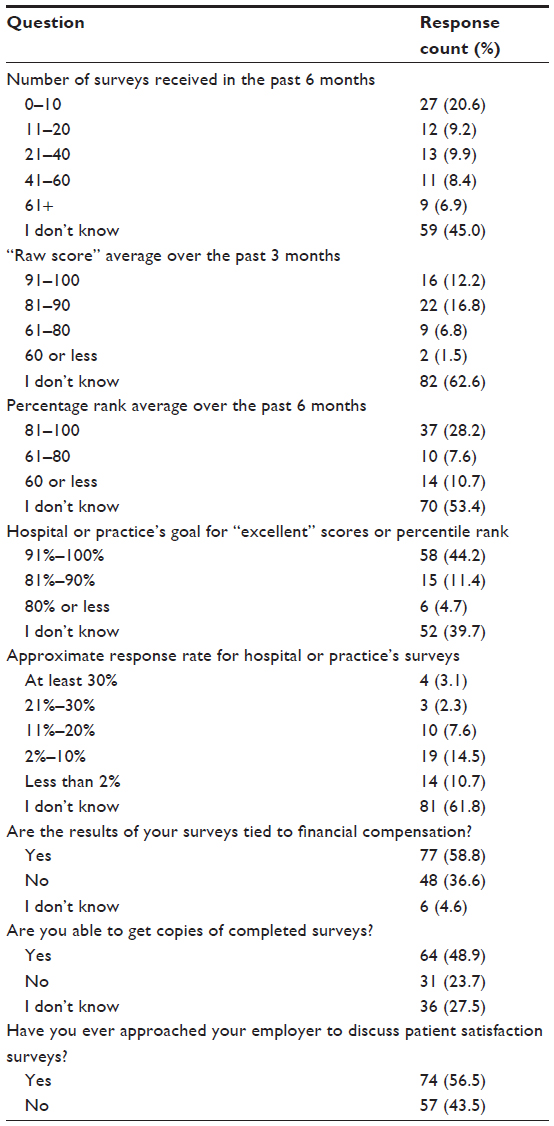 | Table 3 Clinician (N=131) responses to questions related to patient satisfaction survey implementation |
When asked about experiences and perceptions related to patient satisfaction surveys (Table 4; N=131), approximately one-third of the responding physicians reported considering quitting their current job (28.2%) or leaving the profession of medicine (28.2%) because of patient satisfaction survey use in their workplace. Twenty-six physicians (19.8%) reported their employment had been threatened as a direct result of patient satisfaction surveys. The majority (77.9%) felt that patient satisfaction surveys “moderately” or “severely” affected their job satisfaction. About half of clinicians reported ordering an inappropriate test and prescribing inappropriate antibiotic or opioid pain medication as a result of patient satisfaction scores. Some (17.6%) endorsed performing a procedure they believed to be unnecessary and one-third (33.6%) reported they had unnecessarily admitted a patient into the hospital because of patient satisfaction surveys. Almost half (48.1%) felt they had practiced inappropriate patient care as an outcome of patient satisfaction ratings. The vast majority (84.7%) endorsed the statement that their employers support conducting patient satisfaction surveys regardless of concerns raised by physicians.
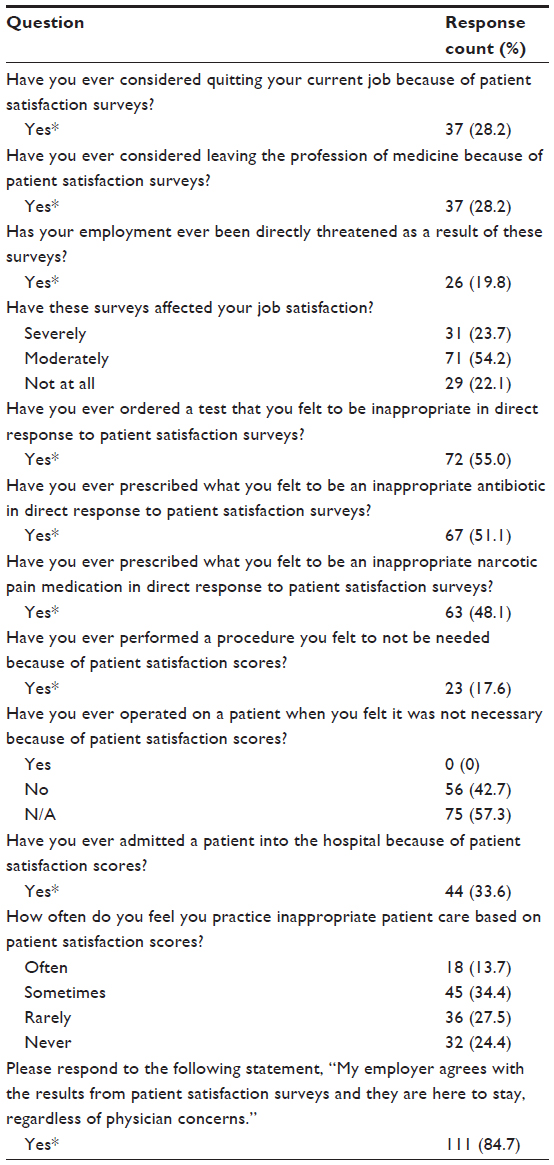 | Table 4 Clinician (N=131) experiences and perceptions related to patient satisfaction surveys |
Discussion
Results from a survey of physicians in a single state in the USA suggest that patient experience of care (“satisfaction”) surveys, as implemented and utilized in the institutions in which they practiced, can lead to physician job dissatisfaction, attrition (exit from the workforce), and inappropriate clinical care, especially if data from patient experience of care surveys are perceived by physicians as a punitive tool regarding compensation or other negative professional consequences. Surveyed physicians also voiced lack of trust in the validity and reliability of survey results, and frustration that administrators did not seem to value their concerns regarding patient satisfaction surveys.
Striving for high patient satisfaction is important, valuable, and a crucial element of patient-centered care. QI initiatives that are responsive to patients’ needs can improve patient satisfaction; in turn, satisfied patients may have better treatment adherence and outcomes.4,5 Interestingly, some studies report that treatment satisfaction may rely more on the patient’s perception of met expectations rather than objective medical outcomes,7–11 and recent publications suggest that utilizing patient satisfaction ratings as a quality-of-care marker may even be harmful.6,13,14 Findings from this pilot study add the perspective of a subset of physicians to this issue and call for the careful evaluation of the effects, especially regarding implementation and utilization, of patient experience of care surveys on clinicians, and clinical care patterns and outcomes.
The most worrisome issue raised by our data is that the use of patient satisfaction surveys may promote, at least among some clinicians and under certain circumstances, a culture of care that can be partially driven by satisfaction score rather than evidence based; this can potentially compromise health-care outcomes as well as violate clinicians’ sense of professional integrity,27 contributing, in turn, to job dissatisfaction. Most of the responding physicians were dissatisfied, with some reporting they were considering leaving medical practice as a result of patient satisfaction surveys. The majority of responding physicians were also concerned that such surveys promoted inappropriate medical practices, including unnecessary antibiotic and opioid pain medication prescriptions, tests, procedures, and hospital admissions. Physicians’ experience of professional roles and their own satisfaction with clinical practice are crucial elements for the stability of physician workforce, an issue which is a component of one of the top three strategic priorities in the American Medical Association’s (AMA) recently revised strategic plan.28 With America facing physician workforce shortages, especially in primary care,29 as well as increasing costs of health care,30 growing antibiotic resistance,31 and an epidemic of prescription drug abuse,32 optimizing system-wide efforts to encourage both evidence-based practice patterns and physician job satisfaction and retention are particularly timely.
These findings are especially important in the context of widespread and broadening utilization of patient satisfaction ratings as an integral element of quality-of-care metrics. Most health-care-related quality metrics assess care processes and health outcomes. With increased emphasis on patient-centered care, patient satisfaction is playing a progressively more prominent role as a surrogate measure of health-care quality. Private sector hospitals, clinics, and health insurance plans collect patient experience of care data for their own use, and many develop initiatives aimed at improving patient satisfaction scores. Reported strategies include incentivizing clinicians by tying physician compensation, academic faculty promotion, or even job retention to patient satisfaction score “benchmarks”. Recently, significant effort and resources have been allocated to patient satisfaction data collection and reporting by the Medicare program33,34 of the federal Centers for Medicare and Medicaid Services (CMS). The CMS’s Hospital Compare and Physician Compare websites publicly report and compare data for hospitals and individual physicians, including cost data, outcome data, and patient experience of care data. Payments to hospitals are now linked to hospital performance not only in generating optimal clinical outcomes and minimizing medical errors but also in creating satisfying experiences for patients, as measured by the CMS’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) initiative. As a result, hospitals encourage their physicians to make decisions facilitating improvement in the hospital’s HCAHPS scores. Our preliminary findings are consistent with the existing limited evidence suggesting that certain methods of implementation and/or utilization of patient satisfaction surveys may have unintended negative consequences. If corroborated, this may have substantial policy- and practice-level implications.
Interestingly, the majority of survey respondents were male physicians, specializing in emergency medicine. Our data do not explain whether or why these physicians may be more dissatisfied or more likely to respond to a survey on patient satisfaction ratings than their counterparts. The higher response rate among ED physicians (16% of the state’s ED physicians in 2012) may, for example, indicate that these physicians are under more scrutiny with respect to patient experience of care measures or may face “tighter” linkages between patient satisfaction scores and professional incentives (financial and emotional rewards from practice). They may also disproportionately find themselves in challenging clinical situations involving patient expectations which – in the physician’s professional judgment – are not aligned with the patient’s best interests. It is also possible that patients may rate ED physicians more “harshly” than they would have rated, under similar circumstances, their continuity clinicians, because the doctor–patient relationship is not as well-established in the acute-care setting. In turn, worse satisfaction ratings may negatively affect the ED clinicians who then voice their dissatisfaction. A study of 7,245 adult Swedish patients from a variety of medical specialty settings found that younger ED patients comprised the least satisfied patient group, and that met expectations were among the top predictors of patient satisfaction.11 Physicians in our study voiced their belief that the use of patient satisfaction ratings had negative effects on their clinical care, especially on opioid prescribing. Issues surrounding opioid prescribing may contribute disproportionately to ED physicians’ dissatisfaction given the clinical challenge of pain-related diagnoses and an epidemic of prescription drug abuse. Provision of adequate analgesia, pain-related communication, and the administration of oral opioids were the main contributors of satisfaction ratings among ED patients with pain.35 The possible negative influence of patient satisfaction-based benchmarks on pain management and opioid prescribing practices has recently been raised by the AMA, whose 2013 report calls for the CMS to suspend the use of HCAHPS-based patient satisfaction ratings on pain management until their validity as a reliable and accurate measure of quality of care is determined.36
Limitations
The survey, developed as a part of a QI project, has a methodological limitation. Its design does not allow us to isolate the effect of patient satisfaction surveys from the potential effect of other factors that may influence physicians’ perceptions and decision making, including, for example, malpractice concerns.
Additionally, the low overall response rate and the relative dominance of ED and male physicians among the respondent pool substantially limit the generalizability of these findings, raising the potential for response bias. However, the consistency of the negative perceptions of patient satisfaction survey impact is compelling and suggests a coherent viewpoint among the responding physicians that is aligned with concerns described in the AMA’s recent report.36 In addition, when estimating the response rate by specialty, ED physician respondents comprised 16% of all practicing ED physicians in the surveyed state in 2012, regardless of their medical society membership. The fact that close to 30% of the surveyed physicians considered not only quitting their current job but also the practice of medicine is worrisome, even in light of the limitations of this study.
Although our data suggest that patient satisfaction surveys may promote inappropriate medical practices among some clinicians, the data may reflect a very different kind of association: it is also possible that our respondents were drawn from a subgroup of clinicians who had provided suboptimal care. If this were the case, it could be that physicians’ practices led to worse patient experience of care ratings which, in turn, resulted in negative consequences for these physicians and, subsequently, increased their likelihood of responding to and airing grievances through an anonymous survey. Thus, responses of the surveyed physicians may represent the voice of a small number of subpar practitioners who were identified via patient experience of care evaluation processes.
Finally, the fact that a large proportion of the surveyed physicians did not know their raw score or percentage rank, both of which make up the “summary scores” of patient satisfaction surveys, may mean that they did not receive feedback on their individual scores; therefore, their perceptions may reflect a general hesitance toward using patient satisfaction data rather than a specific personal experience.
Future directions
These pilot data suggest that current methods of assessment and use of patient satisfaction ratings may, under certain circumstances, have unintended negative consequences for health-care delivery processes and treatment outcomes. They suggest the need for the further investigation of optimal methods to implement and utilize patient experience of care measures to foster patient centeredness, evidence-based clinical practice, and physician job satisfaction.37–39 Examples of such strategies include the provision of regular constructive feedback to individual clinicians; targeted training in communication skills; and venues for open, positive communication between physicians and administration. Identifying subpopulations of patients for whom a different approach to the utilization of patient satisfaction ratings may be warranted (eg, persons with addiction or others seeking opioid prescriptions), could also promote positive change in physicians’ perceptions of the use of patient satisfaction measures.
Conclusion
These state-level data suggest that the system-wide utilization of patient satisfaction surveys may lead to job dissatisfaction and medically inappropriate clinical care among some physicians. These preliminary findings are concerning, especially in the context of the widespread and progressive utilization of patient satisfaction ratings as an integral metric of quality-of-care assessment, and call for a more rigorous evaluation of the use of patient satisfaction surveys and the linkage of data from such surveys to other variables (such as physician compensation, job retention, or job promotion). At the very least, these results are so intriguing that they call for additional investigations of the associations between patient experience of care evaluation activities and physician practice satisfaction.
Acknowledgments
Our thanks to the staff of the state medical society for their assistance with this data.
Disclosure
A Zgierska is supported by grant K23 AA017508 from the National Institute on Alcohol Abuse and Alcoholism at the National Institutes of Health. MM Miller has served on the speakers bureau for Alkermes plc and the physician advisory board for Braeburn Pharmaceuticals, Inc. D Rabago has nothing to disclose.
References
Groene O. Patient centredness and quality improvement efforts in hospitals: rationale, measurement, implementation. Int J Qual Health Care. 2011;23(5):531–537. | |
Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington DC: National Academies Press; 2001. | |
Bertakis KD, Azari R. Patient-centered care is associated with decreased health care utilization. J Am Board Fam Med. 2011;24(3):229–239. | |
Chue P. The relationship between patient satisfaction and treatment outcomes in schizophrenia. J Psychopharmacol. 2006;20(Suppl 6):38–56. | |
Glickman SW, Boulding W, Manary M, et al. Patient satisfaction and its relationship with clinical quality and inpatient mortality in acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2010;3(2):188–195. | |
Fenton JJ, Jerant AF, Bertakis KD, Franks P. The cost of satisfaction: a national study of patient satisfaction, health care utilization, expenditures, and mortality. Arch Intern Med. 2012;172(5):405–411. | |
Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care. Ann Intern Med. 2003;138(4):288–298. | |
Chang JT, Hays RD, Shekelle PG, et al. Patients’ global ratings of their health care are not associated with the technical quality of their care. Ann Intern Med. 2006;144(9):665–672. | |
Schneider EC, Zaslavsky AM, Landon BE, Lied TR, Sheingold S, Cleary PD. National quality monitoring of Medicare health plans: the relationship between enrollees’ reports and the quality of clinical care. Med Care. 2001;39(12):1313–1325. | |
Lee DS, Tu JV, Chong A, Alter DA. Patient satisfaction and its relationship with quality and outcomes of care after acute myocardial infarction. Circulation. 2008;118(19):1938–1945. | |
Rahmqvist M, Bara AC. Patient characteristics and quality dimensions related to patient satisfaction. Int J Qual Health Care. 2010;22(2):86–92. | |
Mold JW, Lawler F, Schauf KJ, Aspy CB. Does patient assessment of the quality of the primary care they receive predict subsequent outcomes?: An Oklahoma Physicians Resource/Research Network (OKPRN) study. J Am Board Fam Med. 2012;25(4):e1–e12. | |
Zgierska A, Miller M, Rabago D. Patient satisfaction, prescription drug abuse, and potential unintended consequences. JAMA. 2012;307(13):1377–1378. | |
Lembke A. Why doctors prescribe opioids to known opioid abusers. N Engl J Med. 2012;367(17):1580–1581. | |
Falkenberg K. Why rating your doctor is bad for your health. Forbes. January 21, 2013. Available from: http://www.forbes.com/sites/kaifalkenberg/2013/01/02/why-rating-your-doctor-is-bad-for-your-health/. Accessed June 6, 2013. | |
O’Reilly KB. Patient satisfaction: when a doctor’s judgment risks a poor rating. American Medical News. November 26, 2012. Available from: http://www.ama-assn.org/amednews/2012/11/26/prsa1126.htm. Accessed June 6, 2013. | |
Sullivan W. Dying for satisfaction. Emergency Physicians Monthly. March 20, 2012. Available from: http://www.epmonthly.com/columns/in-my-opinion/dying-for-satisfaction/. Accessed February 6, 2013. | |
Robbins RA, Raschke RA. A new paradigm to improve patient outcomes: a tongue-in-cheek look at the cost of patient satisfaction. Southwest J Pulm Crit Care. 2012;5:33–35. | |
Press Ganey mantra: suck it up. Emergency Physicians Monthly. January 2, 2013. Available from: http://www.epmonthly.com/whitecoat/2013/01/press-ganey-mantra-suck-it-up/. Accessed February 6, 2012. | |
Elijovich F. Of sommeliers and wine drinkers. Arch Intern Med. 2012;172(14):1111–1112. | |
Friedberg MW, Gelb Safran D, Schneider EC. Satisfied to death: a spurious result? Arch Intern Med. 2012;172(14):1112–1113. | |
Sirovich BE. How to feed and grow your health care system: comment on “The cost of satisfaction”. Arch Intern Med. 2012;172(5):411–413. | |
Maciejewski ML, Harman JS. Patient satisfaction associated with lower emergency department use but more hospitalisations and higher costs and mortality. Evid Based Med. 2013;18(1):e10. | |
Manary MP, Boulding W, Staelin R, Glickman SW. The patient experience and health outcomes. N Engl J Med. 2013;368(3):201–203. | |
Patient expectations regarding opioid prescriptions creating costly conflicts for physicians. The BackLetter. 2012;27(6):67. | |
Crabtree BF, Miller WL. Using Codes and Code Manuals: A Template Organizing Style of Interpretation. In: Crabtree BF, Miller WL, editors. Doing Qualitative Research, 2nd edition. Thousand Oaks, CA: Sage; 1999:163–177. | |
Brett AS, McCullough LB. Addressing requests by patients for nonbeneficial interventions. JAMA. 2012;307(2):149–150. | |
American Medical Association (AMA). Strategic focus [web page on the Internet]. Chicago, IL: AMA; nd. http://www.ama-assn.org/ama/pub/about-ama/strategic-focus.page. Accessed February 25, 2013. | |
Center for Workforce Studies, Association of American Medical Colleges (AAMC). Recent Studies and Reports on Physician Shortages in the US. Washington DC: AAMC; 2012. Available from: https://www.aamc.org/download/100598/data. Accessed May 31, 2013. | |
National Center for Health Statistics. Health, United States, 2011: With Special Feature on Socioeconomic Status and Health. Report No 2012-1232. Hyattsville, MD: US Government Printing Office; 2012. Available from: http://www.cdc.gov/nchs/data/hus/hus11.pdf. Accessed February 2, 2014. | |
Boucher HW, Talbot GH, Bradley JS, et al. Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America. Clin Infect Dis. 2009;48(1):1–12. | |
Executive Office of the President of the United States. Epidemic: Responding to America’s Prescription Drug Abuse Crisis. Washington DC: Executive Office of the President of the United States; 2011. Available from: http://www.whitehouse.gov/sites/default/files/ondcp/issues-content/prescription-drugs/rx_abuse_plan_0.pdf. Accessed February 6, 2012. | |
Meyer Z. Medicare payments tied to patient surveys. U S A Today. December 24, 2012. Available from: http://www.usatoday.com/story/money/business/2012/12/24/hospitals-satisfaction-surveys-medicare/1788833/. Accessed March 1, 2013. | |
Adamy J. US ties hospital payments to making patients happy. Wall Street Journal. October 14, 2012. Available from: http://online.wsj.com/article/SB10000872396390443890304578010264156073132.html. Accessed March 1, 2013. | |
Shill J, Taylor DM, Ngui B, et al. Factors associated with high levels of patient satisfaction with pain management. Acad Emerg Med. 2012;19(10):1212–1215. | |
American Medical Association House of Delegates (A-13). Resolution 18: pain management and the hospital value-based purchasing program.In: Report of Reference Committee G. AMA House of Delegates 2013 Annual Meeting, Chicago, IL, Jun 13–19, 2013. Available from: http://www.ama-assn.org/assets/meeting/2013a/a13-refcomm-g.pdf. Accessed June 30, 2013. | |
Loewenstein G, Volpp KG, Asch DA. Incentives in health: different prescriptions for physicians and patients. JAMA. 2012;307(13):1375–1376. | |
Mannion R, Braithwaite J. Unintended consequences of performance measurement in healthcare: 20 salutary lessons from the English National Health Service. Intern Med J. 2012;42(5):569–574. | |
Rittenhouse DR, Mertz E, Keane D, Grumbach K. No exit: an evaluation of measures of physician attrition. Health Serv Res. 2004;39(5):1571–1588. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.