")
Back to Journals » Clinical Interventions in Aging » Volume 15
Impact of Metabolic Syndrome Components in High-Risk Cardiovascular Disease Development in Older Adults
Authors Gustavo de Sousa Barbalho Y , Morato Stival M , Ramos de Lima L , Cristina Rodrigues da Silva I , de Oliveira Silva A , Vieira Gomes da Costa M , Cristina Morais Santa Barbara Rehem T, Schwerz Funghetto S
Received 5 March 2020
Accepted for publication 25 July 2020
Published 18 September 2020 Volume 2020:15 Pages 1691—1700
DOI https://doi.org/10.2147/CIA.S252589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Yuri Gustavo de Sousa Barbalho, 1 Marina Morato Stival, 1 Luciano Ramos de Lima, 1 Izabel Cristina Rodrigues da Silva, 1 Alessandro de Oliveira Silva, 2 Manoela Vieira Gomes da Costa, 1 Tania Cristina Morais Santa Barbara Rehem, 1 Silvana Schwerz Funghetto 1
1Graduate Department of Health Sciences and Technologies, University of Brasilia (UnB), Brasilia, Federal District, Brazil; 2Physical Education Department, University Center of Brasilia, Brasilia, Federal District, Brazil
Correspondence: Yuri Gustavo de Sousa Barbalho Tel +55 61 9 9112-7116
Email [email protected]
Objective: Analyze the influence between the components of metabolic syndrome and the independent risk for cardiovascular disease (CVD) in the elderly.
Methods: A descriptive cross-sectional study was carried out with 205 older adults from a primary healthcare unit of the Federal District, Brazil. The cardiovascular risk was determined by the Framingham Risk Score (FRS). The National Cholesterol Evaluation Program for Adult Treatment Panel III 2001 (NCEP-ATP III) criteria were considered to analyze metabolic syndrome (MS) diagnoses.
Results: There was a strong association between MS and high cardiovascular risk (OR = 8.86). The univariate analysis main findings revealed that male gender, diabetes, smoking habit, systolic blood pressure, HDL level, high blood glucose, glycated hemoglobin, and LDL level were associated with high cardiovascular risk. FRS increases significantly with the presence of four or more MS components (by 30%, if 4 components are present, and by 40%, if 5 components) when compared with the presence of three or fewer components (P < 0.001). A logistic regression analysis of high-risk predictors was described to reduce the effects of confounding and bias factors.
Conclusion: The identification of MS associated with high FRS values represents a cascading of adverse effects on the population’s aging process.
Keywords: aged, metabolic syndrome, cardiovascular system, aging population
Introduction
The impact of the aging population is noticeable in several fields of society, especially in the healthcare area. The continuing increase in the aging population’s longevity rates has become a challenge for public health care, primarily due to an increase in the number of chronic non-communicable diseases (NCDs) and the complications of multifactorial etiology.1 Brazil is among the six countries with the largest aging population in the world. This population is expected to exceed 26.2 million individuals, equivalent to approximately 12.4% of the total Brazilian population, by 2020.2 According to the Brazilian Society of Geriatrics and Gerontology, in the year 2032, there will be roughly 32.5 million Brazilians older adults.3
The development of poor habits in the aging population exponentially increases the risk of metabolic syndrome (MS), which, in turn, may trigger or exacerbate NCDs and cardiovascular disorders.4 The Brazilian Guideline on the Diagnosis and Treatment of Metabolic Syndrome defines the disease as a set of cardiovascular and metabolic factors.5 In the international scenario, it is estimated that 25% of the population has components indicative of MS diagnosis,6 which may lead to 7% of deaths. Furthermore, data suggest that 17% of the cardiovascular system deaths occur due to MS.7 Evidence in the literature indicates that the MS prevalence increases with age, representing an increase of 2.5 times that of cardiovascular diseases (CVD) risk.8 In this respect, the literature has a large number of studies attesting the relationship between MS and its prevalence in older adults.8–11 A specific study revealed that by 2012 more than a third of the US adult population met the definition and criteria for MS.12
Cardiovascular risk classification is a follow-up strategy and indicator of the quality of treatment implemented in individuals belonging to a high-risk group. The Framingham Risk Score (FRS) is one of the main cardiovascular risk stratification methods recommended by the Brazilian Ministry of Health. In the literature, the results of its use have been of utmost importance in CVD primary prevention.13,14
Therefore, the present study aims to analyze the influence between the MS components and the independent risk for CVD in older adults. The initial hypothesis was that older adults with a higher number of MS components have a higher risk of developing CVD.
Method
Subjects
The participants ‘designation flowchart in the study is displayed in Figure 1. A descriptive cross-sectional study with a quantitative approach carried out in a primary healthcare unit (UBS, per its Portuguese) of the Federal District (FD), Brazil. The study population was composed of older adults who met the following inclusion criteria: being 60 years or older (considered an older adult in Brazil), receiving monitoring in the UBS, and a sound mind. The study sample was of 205 participants, with a 5% margin of error and a 95% confidence level.
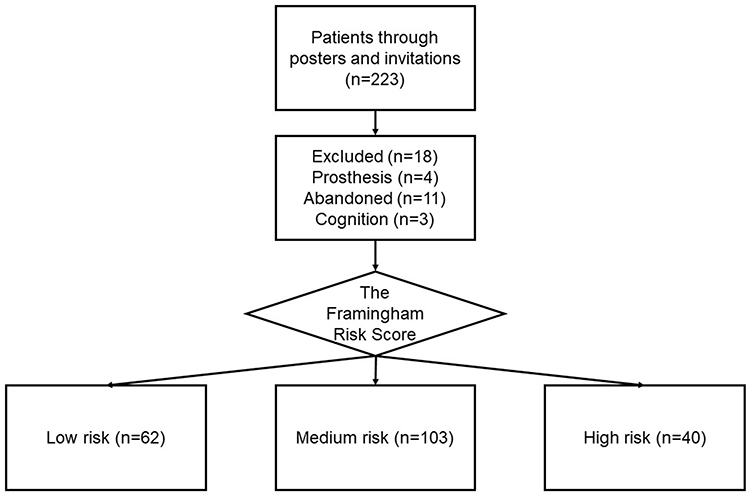 |
Figure 1 The participants’ designation flowchart in the study. Brasília, 2019. |
Individuals with a previous cardiac event, informed at the time of the interview, were excluded from this study. The following exclusion criteria were considered: having a score ≤9 points on the Mini-Mental Health Examination (MMSE) test and having a pacemaker or metallic prosthesis. The Secretariat of Health of the Federal District research ethics committee approved this study (protocol 1.355.211/2017). All information was collected after a written consent document was obtained from all participants. It followed the principles of the National Research Council according to legislation in force in Brazil provided for in the Resolution n° 46 (2012) and according with the Declaration of Helsinki.
Study Presentation
The data collection stages occurred after signing an informed consent form (ICF), from February to June 2019. Each item was properly clarified, and ethical aspects established within the national territory were respected. The responsible researchers were readily available for possible events.
Collection
The first step was a blood sample collection after a fasting period. Approximately 15 mL of venous blood from the cubital vein region were collected, followed by food provision for diabetic patients. The second step was the application of a structured data collection survey for evaluation of patients’ demographic and socioeconomic profiles, constituted by closed questions concerning gender, age, education level, retirement, income, life habits (smoking), clinical conditions (hypertension or diabetes mellitus diagnosis), and medication use (type and administration route). This stage’s objective was to characterize the population involved; researchers also addressed questions and clarified possible doubts. This research was conducted in the FD region with the lowest education and human development index rates. The population studied is also part of the FD densest population mass and is close to the largest slum (favela).
Cardiovascular Data and Anthropometric Measurements
Blood pressure (BP) was measured following the criteria established by the Brazilian Guideline on Hypertension.15 Regarding the anthropometric measurements evaluation, weight and height were determined using a measuring tape and scale (SANNY brand), and the body mass index (BMI) was calculated implementing the weight/height2 formula. Previously trained evaluators obtained the measurements with the application of Lohman’s techniques (1988). The following BMI reference values were considered: normal (22.0 kg/m2 to 27.0 kg/m2) and overweight (>27 kg/m2). Body composition was evaluated employing a dual-energy X-ray absorptiometry examination (DXA, model 8548 BX1L, Lunar DPX type, software Encore 2005, GE Healthcare Europe GmbH Freiburg, Germany).16
The Framingham Risk Score (FRS) was used to determine cardiovascular risk, where each variable presented value ranges with specific positive or negative scores. The total score was calculated by applying the following variables: age, gender, smoking, diabetes mellitus (DM), HDL, total cholesterol (TC), systolic blood pressure (SBP), and diastolic blood pressure (DBP). The resulting score corresponds to a probability percentage of coronary artery disease (CAD) occurrence in the next ten years. The use of FRS to determine cardiovascular risk is presented by Simão et al5 as an economically viable and efficient strategy for tracking patients at high risk and a more careful managing of the risk factors.
The FRS classification is thus determined: low, if risk <10% in 10 years; intermediate, if between 10–20%; and high, if >20%. Hence, patients are considered at high cardiovascular risk when FRS >20%.
Metabolic Syndrome
The Brazilian Society of Cardiology criteria were used to analyze the MS diagnoses that followed the Brazilian Guideline on the Diagnosis and Treatment of Metabolic Syndrome. This Guideline does not require insulin measurement and adopts the National Cholesterol Evaluation Program for Adult Treatment Panel III 2001 (NCEP-ATP III) as a clinical criterion. The following components were evaluated: waist circumference (WC) >88 cm for women and >102 cm for men; BP ≥130x85mmHg or the use of an antihypertensive; fasting glucose ≥110mg/dL or a DM type 2 diagnosis; triglyceride (TG) ≥150mg/dL; and HDL-c <40mg/dL for men and <50mg/dL for women. The presence of at least three components is required for an MS diagnose.17
Statistical Analysis
A database was created using the Statistical Package for the Social Sciences 20 (SPSS). Foremost, relative and absolute frequencies, dispersion measures, mean, and standard deviation were calculated. The Kolmogorov–Smirnov test was applied to analyze the variables’ normality. The t-test and the ANOVA test were employed to compare differences among groups. The Spearman correlation coefficient was performed for the correlations analysis of numerical variables. P-values of <0.05 were considered statistically significant.
Regression analysis was employed to reduce the effects of confounding and bias factors. To determine the logistic regression mathematical model, the criteria of Hair et al (2005), which includes 20 cases for each predictor variable and a minimum of 5 cases, was adopted.18
Results
Two-hundred five older adults participated in the study. Most were women, aged between 60 and 64, with one to four years of education, not retired, and with a monthly income of less than or equal to one minimum wage. Some variables, such as educational level, retirement, and income, collected did not present a significant association with the presence of high cardiovascular risk.
For the selection of possible candidate variables to predict high cardiovascular risk according to the FRS classification criteria, a univariate association analysis was first performed, as described in Table 1. It was noted that the variables males (p=0.001); Metabolic Syndrome (MS) presence (p<0.001); Diabetes Mellitus (DM) presence (p<0.001); smoking (p=0.027); altered systolic blood pressure - SBP (p<0.001); altered diastolic blood pressure -DBP (p=0.008); low HDL levels (p<0.001); high blood glucose (p<0.001); elevated glycated hemoglobin (p<0.001); high LDL levels (p=0.007); and CVD risk (p<0.001) were associated as risk factors for cardiovascular risk (OR>1.0).
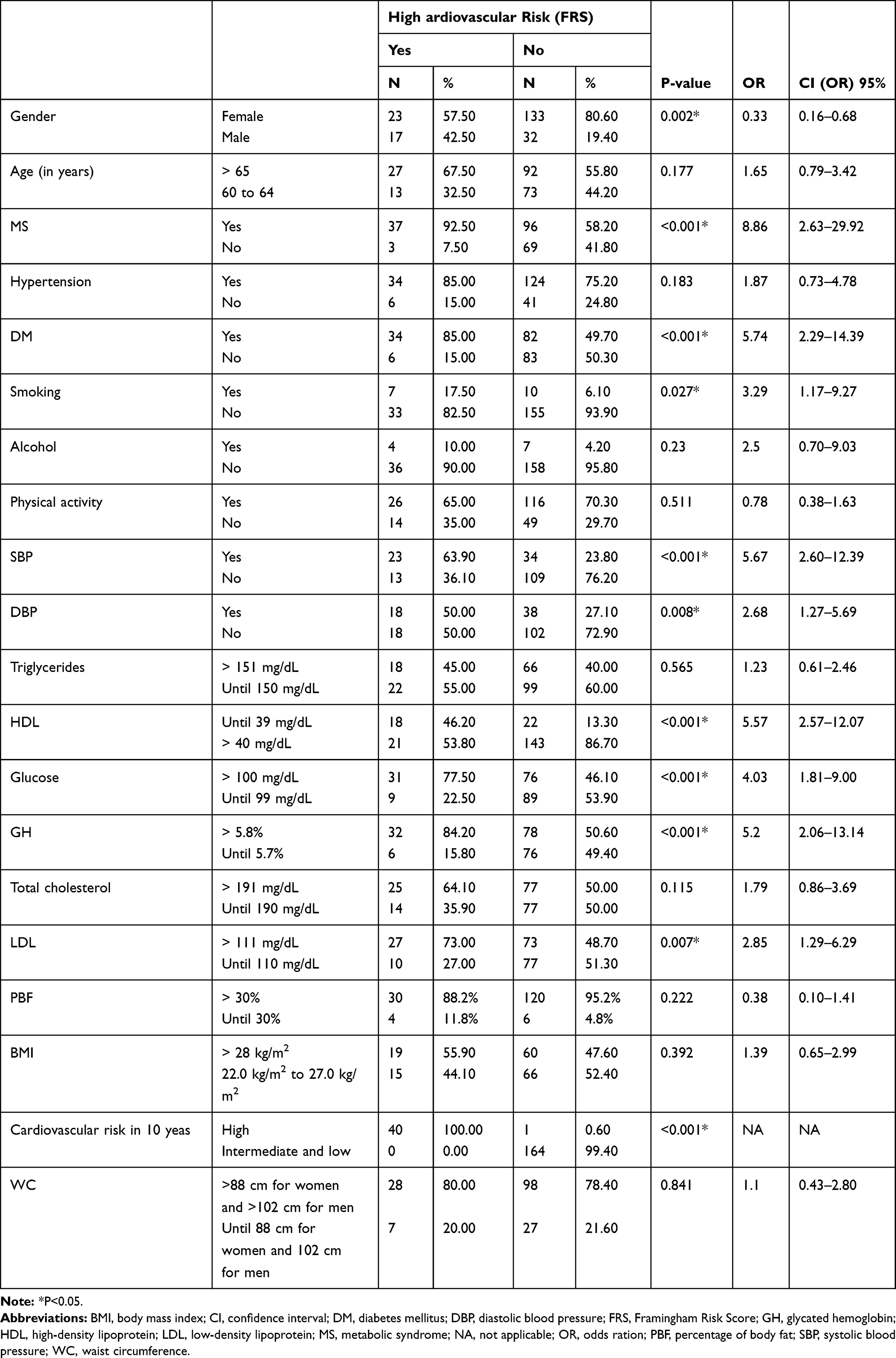 |
Table 1 High-Risk Category to the Framingham Risk Score (FRS) in Older Adults According to Demographic, Anthropometric, Biochemical, Clinical, and Socioeconomic Variables. Brasilia, 2020 |
As the MS presence was strongly associated with high cardiovascular risk (OR = 8.86), it was decided to investigate further this connection. The median FRS difference was evaluated under different combinations of MS components. FRS had a significant median increase of 30% and 40% in the presence of 4 and 5 included components, respectfully, when compared to the presence of 1 to 3 components (P<0.001; Figure 2). Thus, FRS increases significantly in the presence of at least four MS components. Nonetheless, these FRS median did not differ between low numbers (1, 2, or 3) or high numbers (4 or 5) of components.
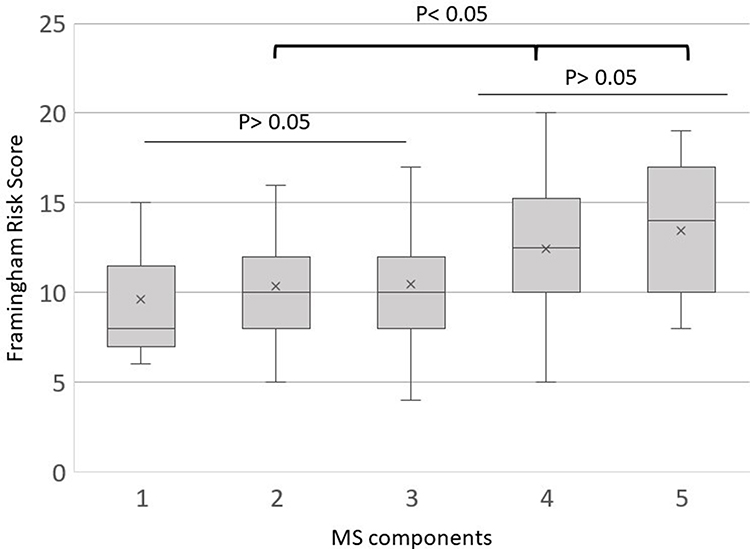 |
Figure 2 Effect of Metabolic Syndrome (MS) components on Framingham Risk Score (FRS) values. Brasilia, 2019 (n=205). Kruskal–Wallis´: p<0.001; Bonferroni correction test comparison of the FRS median of four or five components with one, two, or three are statistically significant (P<0.050). The “x” mark on the boxplot denotes the data mean. |
The other variables that were statistically associated with the high FRS value were eligible for the logistic regression model. The results showed that the model composed of these variables was significant (p<0.01) for the explanation of the variable criterion “Cardiovascular risk,” measured in terms of the proportion of the high FRS category presence. The model’s adjustment was expressive, and adequately classified 87.1% of the individuals present in the sample. Table 2 presents the results of the logistic return analysis, in which return coefficients are: not standardized (B), meaning level (sig.), odds ratios for the predictors (Exp(B)), and the intercept (constant). Thus, predictors for high cardiovascular risk are altered SBP, male gender, DM presence, smoking habit, and alteration in HDL and LDL biochemical components.
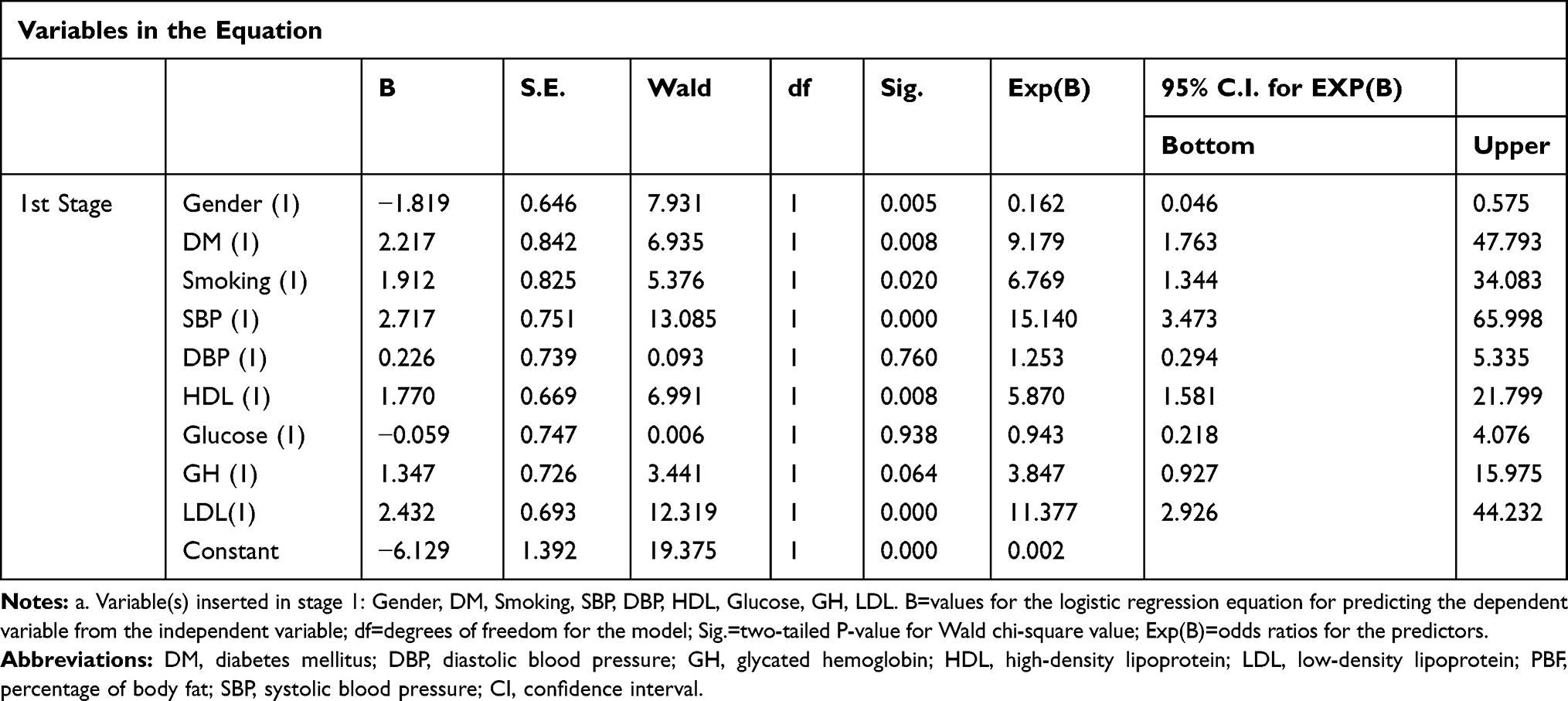 |
Table 2 Logistic Regression of Predictors of High Cardiovascular Risk. Brasilia, 2020 (n=205) |
Finally, for a better comprehension of the body and biochemical composition in the different FRS categories, Table 3 was constructed. In the comparison among risk groups, higher mean values were found in the high-risk group, such as triglycerides and BMI, compared with the moderate and low-risk group (P =0.003 and P = 0.036, respectively). Likewise, when comparing blood glucose, glycated hemoglobin, waist circumference (WS), SBP, DBP, and HDL, higher mean values were found in the high-risk group when compared with the moderate and low-risk group which had similar mean values (Table 3).
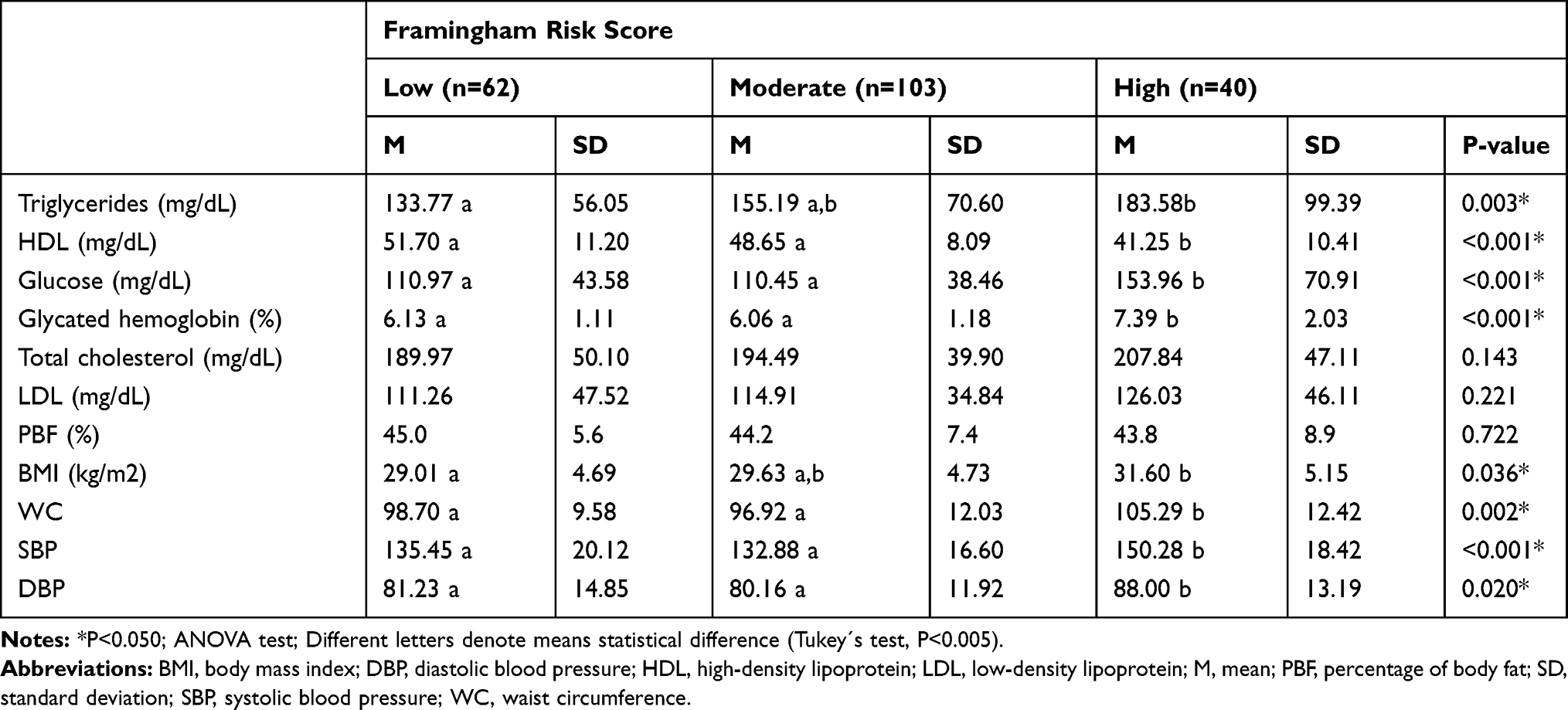 |
Table 3 Framingham Risk Score of Older Adults According to Biochemical and Nutritional Variables. Brasilia, 2018 (n=205) |
Discussion
This study analyzed the influence between the metabolic syndrome (MS) components and the independent risk for cardiovascular disease (CVD) in older adults confirming the initial hypothesis that individuals with a higher number of MS components have a higher risk for developing CVD. Furthermore, a quarter of the older adults with MS had a high risk of developing CVD compared to those without MS. Though it is important to note that old adults with diabetes mellitus (DM), increased systolic blood pressure (SBP), smoking habit, and a high LDL level demonstrated a high cardiovascular risk regardless of having MS.
MS seems to increase cardiovascular risk while also carrying other commodities. Mansourian et al19 claim that MS individuals have twice as much risk compared to the general population. MS represents a condition that deserves attention due to the complexity of components and risk factors.20 For a better comprehension of its influence, analyzing the current diagnoses are essential. Many studies investigate specific clinical conditions, such as the impairment of the cardiovascular system, yet clinical conditions depend on the prevalence of the number of MS components and the associated risk factors.21,22
The statistics on the present study sample indicate that increased cardiovascular risk is closely associated with older adults who have more MS components. The presence of 4 MS components increases cardiovascular risk by 30%, while 5 components increase the risk by 40%, compared to the elderly with 3 or fewer components. A study found that MS individuals had an increased prevalence of coronary heart disease and stroke, illustrating the link between health conditions.23
The biochemical profile showed significant metabolic alterations in old adults who met the high cardiovascular risk criteria. The prevalence of changes in lipid, glycemic, and BMI profiles causes several associated systemic diseases. Factors related to abdominal fat accumulation and increased waist circumference (WC) are associated with the lipid process, which, when increased releases inflammatory mediators into the bloodstream.24 Lack of glycemic control activates hepatic mechanisms that rise lipoprotein synthesis, increasing LDL levels, and reducing HDL levels. These factors are strongly associated with cardiovascular risk,23,25 which supports the metabolic results of this study. Results similar to these were found in our previous study, revealing that a more meticulous analysis of biochemical components allows a better comprehension of the MS progression status in the elderly population.26
Factors involving lipids are present in the pathological process of obesity. Although these lipid profile factors do not affirm the obesity diagnosis, they alert to patterns that expose the risk of obesity development. These patterns reaffirm inflammatory conditions that, when associated with the increased life expectancy, have a high potential for cognitive impairment and decreased quality of life.27
In our previous study, a correlation between the inflammatory process and the anthropometric state was evidenced.28 This inflammatory process begins with the lipoproteins agglomeration in the vessel walls and is related to adipokines’ function as proinflammatory mediators.24,29
Our results reveal an association between decreased HDL levels and high cardiovascular risk. This result confirms previous studies that connected low HDL levels to alterations that represent cardiovascular complications, presenting HDL levels as an independent predictive variable for MS.30 It is important to remember that cholesterol is an essential molecule for the proper functioning of homeostasis. The distinct types of cholesterol perform specific functions within the body, with HDL molecule being responsible for eliminating the cholesterol accumulation in the walls of the vessels and arteries, thus preventing complications. Hence, when HDL levels are below optimum, the higher risk for CVD development.
Table 2 also presents the correlation between LDL levels and high cardiovascular risk. LDL molecule is responsible for transporting the cholesterol deposited in the liver to the arteries, and when accumulated may form an obstruction. Increases in LDL levels may be associated with behavioral factors such as inadequate nutrition, use of specific medications, and intrinsic factors, eg, overweight and genetics. The LDL role associated with cardiovascular impairment may trigger CVD development, and this association may be enhanced by factors such as a smoking habit, DM, and hypertension.23,25,31
DM was identified in this study as predictive of high cardiovascular risk and is one of the factors involved in the MS process. Some studies cite MS as a predictor for the DM diagnosis.32–34 Despite this association, the literature has also described DM as an insufficient predictor of cardiovascular impairments.35,36 Yet, many other studies associate DM with the appearance of complications in the cardiovascular system.37–39 Therefore, DM is a potential predictor, knowing that it may cause impairment of the vascular system walls, in addition to carrying other clinical factors such as obesity, physical inactivity, and dyslipidemia.40,41
The overall diabetic population is denoted at high cardiovascular risk. Relevant to underline that these conditions have treatment and control, and it is possible to stabilize them, as long as there are adequate monitoring and access to treatment.42 These responsibilities fall on primary health care for it has higher power for direct monitoring.14 Studies carried out in line with the Cardiovascular Health Study (CHS) corroborate data from past and current decades, showing that CVD and MS have a favorable prognosis with the early recognition of the risk and adherence to the treatment plan.43
Regarding blood pressure, this study presents similar results to those found in literature, demonstrating a correlation between the set of MS components and the CVD risk. A review study conducted in Japan showed MS as a potential predictor of mortality from CVD associated complications.32 In the USA, a cohort study revealed that MS patients are 30% more likely to develop CVD.44 When studying CVD according to the MS risk factors, an Iranian study45 revealed that the highest number of MS components is associated with the highest risk of cardiovascular complications. This association of component numbers may be related to the systemic repercussion of each of the MS risk factors and components. These include insulin resistance, which, in turn, is related to the increase in circulating glucose and DM diagnosis. Other complications related to this health condition, such as vasoconstriction and sodium retention, generate an intimate connection with blood pressure variations, especially the systolic.45
There is a considerable prevalence of smoking habits in cardiovascular risk assessment studies.46–48 There is a considerable prevalence of smoking habits in cardiovascular risk assessment studies. 46–48. The effect of tobacco within the organism occurs through nicotine. Its action prevents vasodilation of blood vessels and capillaries, remaining in a state of vasoconstriction, which increases blood pressure and compromises the arrival of oxygen molecules required in places such as the myocardium. In addition to cardiovascular implications generated from endothelial dysfunction, smoking can also influence the atherosclerosis process.49
Limitations of the Study
Due to the cross-sectional design of the study, it was impossible to obtain temporal information, such as in prospective studies. Further studies must be performed to obtain more accurate results regarding the association of these variables as these are still scarce in the literature, especially in regards to older adults.
Conclusion
The results of the present study provide convincing evidence that older adults with MS have high FRS values, and that the more MS components present, the higher the cardiovascular risk, which, in turn, may negatively affect the aging process of this population. The predictors of high cardiovascular risk are as follows: altered systolic blood pressure, male gender, diabetes mellitus presence, smoking habit, and alteration in HDL and LDL biochemical components.
It is worth remembering the background in which this study was conducted. The studied population resides in an underdevelopment region of the city that has a high population density. The factors cited as predictive of cardiovascular risk are amenable to the identification and multi-professional intervention and may be used by primary health care teams for monitoring, treatment, and prevention. Establishing these therapeutic approaches for health promotion and prevention carries a high potential for improving the aging process of the population, therefore aiming for a better quality of life and healthy aging conditions.
Further studies must investigate the chronic effects of MS on cardiovascular risk and their clinical impact, specifically in the older population of developing countries, where public healthcare systems are not prepared to meet their needs.
Acknowledgments
We would like to offer thanks to all people who accepted to participate in this study. We also thank the Foundation of Support to Research of the Federal District (FAP-DF) and National Council for Scientific and Technological Development (CNPq), Coordination for the Improvement of Higher Education Personnel (CAPES), and the University of Brasilia which have supported this research.
Disclosure
The authors declare no conflicts of interest in the present study.
References
1. Souza JD, Martins MV, Franco FS, Martinho KO, Tinôco AL. Dietary patterns of the elderly: characteristics and association with socioeconomic aspects. Rev Bras Geriatr Gerontol. 2016;19(6):970–977. doi:10.1590/1981-22562016019.160035
2. Bortoletto MSS, Souza RKT, de Cabrera MAS, González AD. Metabolic syndrome, components, and associated factors in adults aged 40 years or older from a city in southern Brazil. Cad Saúde Coletiva. 2016;24(1):32–40. doi:10.1590/1414-462x201600010123
3. Brazilian Society of Geriatrics and Gerontology. WHO discloses targets for 2019; challenges impact the lives of the elderly; 2019. Available from: https://sbgg.org.br/oms-divulga-metas-para-2019-desafios-impactam-a-vida-de-idosos/.
4. Matos De Pinho P, Maria L, Machado M, et al. Metabolic syndrome and its relationship with cardiovascular risk scores in adults with non-communicable chronic diseases. Rev Soc Bras Clin Med. 2013;12(1):22–30. doi:10.5151/biochem-jaibqi-0090
5. Simão AF, Precoma DB, Andrade JP, et al. 1st Brazilian cardiovascular prevention directive. Arq Bras Cardiol. 2013;101(6 SUPPL.2):1–63. doi:10.5935/abc.2013S012
6. Nolan PB, Carrick-Ranson G, Stinear JW, Reading SA, Dalleck LC. Prevalence of metabolic syndrome and metabolic syndrome components in young adults: a pooled analysis. Prev Med Rep. 2017;7:211–215. doi:10.1016/j.pmedr.2017.07.004
7. Garcia Lira Neto JC, Almeida Xavier M, Pereira Borges JW, Moura de Araújo MF, Coelho Damasceno MM, Freire de Freitas RWJ. Prevalence of metabolic syndrome in people with type 2 diabetes mellitus. Braz J Nurs. 2017;70(2):282–287.
8. Auxiliadora Nogueira Saad M, Perez Cardoso G, de Andrade Martins W, Guillermo Coca Velarde L, Antunes da Cruz Filho R. Prevalence of metabolic syndrome in elderly and agreement among four diagnostic criteria. Arq Bras Cardiol. 2014;102(3):263–269. doi:10.5935/abc.20140013
9. Dada A, Ajayi D, Areo P, et al. Metabolic Syndrome and Framingham Risk Score: observation from Screening of Low-Income Semi-Urban African Women. Medicines. 2016;3(2):15. doi:10.3390/medicines3020015
10. Rocha FL, de Melo RLP, de Menezes TN. Factors associated with metabolic syndrome among the elderly in the northeast of Brazil. Rev Bras Geriatr Gerontol. 2016;19(6):978–986. doi:10.1590/1981-22562016019.160046
11. Zoraski H, Fiametti M, Santos Dos R, de Gregoletto MLO, Cremonese C. Metabolic syndrome in elderly from Nova Roma do Sul, RS: prevalence and associated factors. ABCS Heal Sci. 2017;42(3). doi:10.7322/abcshs.v42i3.955
12. Moore J, Chaudhary N, Akinyemiju T. Metabolic syndrome prevalence by race/ethnicity and sex in the United States, national health and nutrition examination survey, 1988–2012. Rev Chronic Dis. 2017;14(3). doi:10.5888/pcd14.160287
13. Applebaum J, Harun A, Davis A, Hillel AT, Best SRA, Akst LM. Geriatric Dysphonia: characteristics of Diagnoses in Age-Based Cohorts in a Tertiary Voice Clinic. Ann Otol Rhinol Laryngol. 2019;128(5):384–390. doi:10.1177/0003489419826133
14. de Sousa NP, De Sousa MF, de Araújo DER, Santos WS, de Lima LR, Rehem TCMSB. Cardiovascular risk stratification in primary care according to Framingham’s score. Tempus Actas De Saúde Coletiva. 2016;10(1):157. doi:10.18569/tempus.v10i1.1862
15. Malachias MVB, Souza WKSB, Plavnik FL, et al. 7th Brazilian Guideline of Arterial Hypertension: presentation; 2016. Available from: www.arquivosonline.com.br.
16. de Souza WC, de Lima VA, França SN, Rebesco DB, Leite N, Mascarenhas LPG. Association of body mass index with dual-energy X‐ray absorptiometry (DEXA) in type 1 diabetics. Rev Cuba Med Mil. 2019;48(2):224–237.
17. Catelli De Carvalho MH. 1st Brazilian guideline for the diagnosis and treatment of metabolic syndrome. Arq Bras Cardiol. 2005;84(SUPPL. 1):1–28. doi:10.1590/s0066-782x2005000700001
18. Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., & Tatham, R. L. Analysis multivariate of date. Bookman editora, 2009.
19. Mansourian M, Babahajiani M, Jafari-Koshki T, Roohafza H, Sadeghi M, Sarrafzadegan N. Metabolic syndrome components and long-term incidence of cardiovascular disease in Eastern Mediterranean Region: a 13-year population-based cohort study. Metab Syndr Relat Disord. 2019;17(7):362–366. doi:10.1089/met.2018.01367
20. Hosseini N, Talaei M, Dianatkhah M, Sadeghi M, Oveisgharan S, Sarrafzadegan N. Determinants of incident metabolic syndrome in a Middle Eastern population: Isfahan cohort study. Metab Syndr Relat Disord. 2017;15(7):354–362. doi:10.1089/met.2016.0156
21. Oliveira JS, Narriman R, De Oliveira S. An integrative review of associations between polymorphic variants and the metabolic syndrome. J Vasc Bras. 2018;7301(2):141–147. doi:10.1590/1677-5449.007917
22. Azambuja CR, Farinha JB, Rossi DS, Spohr CF, Dos Santos DL. Diagnosis of metabolic syndrome analyzed under different definition criteria. Rev Baiana Saúde Pública. 2015;39(3):482–496. doi:10.5327/z0100-0233-2015390300002
23. Li W, Song F, Wang X, et al. Relationship between metabolic syndrome and its components and cardiovascular disease in middle-aged and elderly Chinese population: a national cross-sectional survey. BMJ Open. 2019;9(8):e027545. doi:10.1136/bmjopen-2018-027545
24. Mota AVH, Cruz JF, Santana JT, Martins BM, Dantas JGL, Lima SO. Correlation of anthropometric indicators of obesity and prevalence of non-alcoholic hepatic steatosis diagnosed by ultrasound. J Braz Soc Clin Med. 2018;16(2):85–88.
25. Soltani A, Argani H, Rahimipour H, Soleimani F, Rahimi F, Kazerouni F. Oxidized LDL: as a risk factor for cardiovascular disease in renal transplantation. J Bras Nefrol. 2016;38(2):147–152. doi:10.5935/0101-2800.20160023
26. Silva a de O, Tibana RA, Karnikowski MGO, Funghetto SS, Prestes J. Inflammatory status in older women with and without metabolic syndrome: is there a correlation with risk factors? Clin Interv Aging. 2013;8:361–367. doi:10.2147/CIA.S39899
27. Arnoriaga-Rodríguez M, Fernández-Real JM. Microbiota impacts on chronic inflammation and metabolic syndrome-related cognitive dysfunction. Rev Endocr Metab Disord. 2019;20(4):473–480. doi:10.1007/s11154-019-09537-5
28. Funghetto SS, De Oliveira Silva A, De Sousa NMF, et al. Comparison of percentage body fat and body mass index for the prediction of inflammatory and atherogenic lipid risk profiles in elderly women. Clin Interv Aging. 2015;10:247–253. doi:10.2147/CIA.S69711
29. Ramires EKNM, de Menezes RCE, Longo-Silva G, Dos Santos TG, Marinho P de M, da Silveira JAC. Prevalence and factors associated with metabolic syndrome among Brazilian adult population: national health survey – 2013. Arq Bras Cardiol. 2018;110(5):455–466. doi:10.5935/abc.20180072
30. Hosseinpanah F, Nazeri P, Ghareh S, Tohidi M, Azizi F. Predictors of the incident metabolic syndrome in healthy obese subjects: a decade of follow-up from the Tehran lipid and glucose study. Eur J Clin Nutr. 2014;68(3):295–299. doi:10.1038/ejcn.2013.142
31. Meireles-Brandão JA, Meireles-Brandão LR, Coelho R, Rocha-Gonçalves FR. Lipoprotein(a) in the evaluation of cardiovascular risk in the portuguese population. Acta Med Port. 2019;32(3):202–207. doi:10.20344/amp.10251
32. Watanabe J, Kotani K. Metabolic syndrome for cardiovascular disease morbidity and mortality among general Japanese people: a mini-review. Vasc Health Risk Manag. 2020;16:149–155. doi:10.2147/VHRM.S245829
33. Nieto CIR, Pérez JDM, Freire LM, Morales KR de P, Vicente ERC. Prevalence of metabolic syndrome and associated risk factors in Ecuadorian university students. Nutr Hosp. 2015;31(4):1574–1581. doi:10.3305/nh.2015.31.4.8371
34. Carvajal C. Metabolic syndrome: definitions, epidemiology, etiology, components, and treatment. Med Perna Costa Rica. 2017;34(1):175–193.
35. Hosseini-Esfahani F, Bahadoran Z, Moslehi N, et al. Metabolic syndrome: findings from 20 years of the Tehran lipid and glucose study. Int J Endocrinol Metab. 2018;16(4 Suppl). doi:10.5812/ijem.84771
36. Ren J, Anversa P. The insulin-like growth factor I system: physiological and pathophysiological implication in cardiovascular diseases associated with metabolic syndrome. Biochem Pharmacol. 2015;93(4):409–417. doi:10.1016/j.bcp.2014.12.006
37. Silva-E-Oliveira J, Amélio PM, Abranches ILL, Damasceno DD, Furtado F. Heart rate variability based on risk stratification for type 2 diabetes mellitus. Einstein (Sao Paulo). 2017;15(2):141–147. doi:10.1590/S1679-45082017AO3888
38. Alcocer-Gamba MA, Gutiérrez-Fajardo P, Sosa-Caballero A, et al. Recommendations for the care of patients with diabetes mellitus with risk factors or established cardiovascular disease and SARS-CoV-2. Arch Cardiol Mex. 2020;90:77–83. doi:10.24875/ACM.M20000074
39. Chmelík Z, Vaclová M, Lánská V, Laštůvka J, Vrablík M. Analysis of incidence and prevalence of cardiovascular risk factors and evaluation of their control in the epidemiological survey in the Czech Republic. Cent Eur J Public Health. 2020;28(2):114–119. doi:10.21101/cejph.a5730
40. Cuevas MA, Alonso KR. Diabetic Dyslipidemias. Rev Médica Clínica Las Condes. 2016;27(2):152–159. doi:10.1016/j.rmclc.2016.04.004
41. Silveira EA, Vieira LL, de Souza JD. High prevalence of abdominal obesity among the elderly and its association with diabetes, hypertension, and respiratory diseases. Cien Saude Colet. 2018;23(3):903–912. doi:10.1590/1413-81232018233.01612016
42. Aguiar C, Duarte R, Carvalho D. New approach to diabetes care: from blood glucose to cardiovascular disease. Rev Port Cardiol. 2019;38(1):53–63. doi:10.1016/j.repc.2018.03.013
43. Closs VE, Feoli AMP, Schwanke CHA. Metabolic syndrome in elderly from tertiary health care in Porto Alegre, Rio Grande do Sul, Brazil: association with the Healthy Eating Index. Sci Med (Porto Alegre). 2016;26(3). doi:10.15448/1980-6108.2016.3.23422
44. McNeill AM, Katz R, Girman CJ, et al. Metabolic syndrome and cardiovascular disease in older people: the cardiovascular health study. J Am Geriatr Soc. 2006;54(9):1317–1324. doi:10.1111/j.1532-5415.2006.00862.x
45. Khosravi-Boroujeni H, Ahmed F, Sadeghi M, et al. Does the impact of metabolic syndrome on cardiovascular events vary by using different definitions? Chronic Disease Epidemiology. BMC Public Health. 2015;15(1). doi:10.1186/s12889-015-2623-3
46. Fernandes PV, de Castro MM, Fuchs A, et al. Predictive value of the Framingham risk score in identifying high cardiovascular risk. Int J Cardiovasc Sci. 2015;1(1). doi:10.5935/2177-7772.20150002
47. Cichocki M, Parron Fernandes K, Cristhine Castro-Alves D, Vinicius de Matos Gomes M. Physical activity and modulation of cardiovascular. Rev Bras Med Esporte. 2017;23(1):21–25. doi:10.1590/1517-869220172301159475
48. Menezes MH, Reis VHS, Dantas DBG, et al. Hypertension and cardiovascular events in the state of Tocantins, Brazil. Rev Patol Do Tocantins. 2017;4(2):50. doi:10.20873/uft.2446-6492.2017v4n2p50
49. Brandão JM, Fernandes C Dos S, Barroso SG, Rocha G de S. Association of fiber intake and cardiovascular risk in elderly patients. Int J Cardiovasc Sci. 2015;28(6):464–471.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.