")
Back to Archived Journals » International Journal of Clinical Transfusion Medicine » Volume 8
Impact of Incorporation of Fibrinogen Concentrate in Blood Transfusion Management During Liver Transplantation: An Early Local (Single Centre) Experience
Received 15 November 2019
Accepted for publication 21 January 2020
Published 5 February 2020 Volume 2020:8 Pages 1—5
DOI https://doi.org/10.2147/IJCTM.S238816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Cees Th. Smit Sibinga
Ying Ci Ho, Kai Inn Lim, Fook Onn Lai
Division of Anaesthesiology, Department of Anaesthesia, Singapore General Hospital, Singapore
Correspondence: Ying Ci Ho
Division of Anaesthesiology, Department of Anaesthesia, Singapore General Hospital, Block 6 Level 2, Outram Road, Singapore 169608, Singapore
Email [email protected]
Background: Orthotopic liver transplantation surgery is associated with major bleeding, often requiring transfusions of blood products such as red cell concentrates, plasma, platelets and cryoprecipitate. Fibrinogen concentrate was made available in our institution in January 2017 and is increasingly being used as an alternative strategy to reduce transfusion requirements. Limited literature exists to show the effectiveness of fibrinogen concentrate on blood loss during liver transplantation surgery, as well as its impact on blood transfusion requirements.
Methods: This is a retrospective, observational study conducted at a single, large, tertiary centre in Singapore to evaluate the impact of incorporating fibrinogen concentrate on blood transfusion requirements during orthotopic liver transplantation surgery from January 2014 to December 2018.
Results: A total of 54 patients who underwent liver transplantation during this period were studied. Forty patients did not receive fibrinogen concentrate during the surgery while 14 patients did. No statistically significant difference was detected in the baseline preoperative characteristics of both groups of patients in terms of MELD or preoperative INR. The mean INR in patients who did not receive fibrinogen concentrate was 1.77 while that in patients who received fibrinogen concentrate was 2.21. While not statistically significant, clinically this may be of significance. There was a significant difference in the starting haemoglobin level of the patients, with a lower starting haemoglobin level in patients who received fibrinogen concentrate (p=0.039). No significant difference was noted in the amount of blood loss, amount of red cell transfusions and amount of fresh plasma transfused. Of note, patients who received fibrinogen concentrate had a significantly less amount of cryoprecipitate transfused compared to those who did not (p=0.002).
Conclusion: The intraoperative use of fibrinogen concentrate did not seem to have any statistically significant difference in the amount of blood loss during surgery. However, the amount of cryoprecipitate used was significantly reduced with the introduction of fibrinogen concentrate.
Keywords: fibrinogen concentrate, liver transplantation
Introduction
Orthotopic liver transplantation surgery is associated with major bleeding, often requiring transfusions of blood products such as red cell concentrates, plasma, platelets and cryoprecipitate.1 With improved surgical techniques and more options available for the treatment of coagulation deficiencies, transfusion requirements in liver transplant surgery have started to decrease.
In a review by Saner et al, the most ideal treatment for clinically relevant fibrinogen deficiency was replacement with fibrinogen concentrate.2 Fibrinogen concentrate was made available in our institution in January 2017 and is increasingly being used as an alternative strategy to reduce transfusion requirements.
In a more recent study in 2019 by Hartmann et al, ROTEM guided substitution with fibrinogen concentrates did not negatively affect mortality after liver transplantation while the deleterious effects of platelet concentrates were confirmed. This further encourages the shift towards the use of fibrinogen concentrates as part of our haemostatic strategy. This should be guided objectively by ROTEM analysis.3
Limited literature exists to show the effectiveness of fibrinogen concentrate on blood loss during liver transplantation surgery, as well as its impact on blood transfusion requirements.4 Our study aims to look at the impact of the introduction of fibrinogen concentrate on our blood transfusion management in the local context.
Materials and Methods
This is a retrospective, observational study conducted at a single, large, tertiary centre in Singapore to evaluate the impact of incorporating fibrinogen concentrate on blood transfusion requirements during orthotopic liver transplantation surgery from January 2014 to December 2018.
Waiver of Institutional Review Board Approval was obtained prior to the commencement of this study.
The aim of this study was to pragmatically evaluate the overall impact of fibrinogen concentrate on our practice. As such, we performed a retrospective analysis of all the patients who underwent liver transplantation during the specified period. No patients were excluded and there were no specific inclusion criteria.
Use of blood products and fibrinogen concentrate is guided by ROTEM analysis. ROTEM analysis is a standard of care for all our liver transplant surgeries. Transfusion strategies are left to each individual anaesthetist's discretion but are generally guided by point of care analysis of haemoglobin and largely dependent on the patient’s haemodynamics and ongoing blood losses during surgery. Fluid management and volume transfusion strategies also vary from one anaesthetist to another. Use of fibrinogen concentrate also varied between anaesthetists but was mainly guided by ROTEM, particularly FIBTEM values. Its use was not restricted to any particular group of patients.
As this is a retrospective analysis, there was no standardised protocol of administration of fibrinogen concentrate. Either 1g or 2g of fibrinogen concentrate was administered after ROTEM analysis. As a general guide based on our departmental guidelines, we used the values as follows to guide our haemostatic management: A10 on EXTEM <35mm, A10 on FIBTEM <10mm with normal platelet count to give fibrinogen concentrate with the aim to increase the A10 on FIBTEM to 13mm. In the event of sudden rapid blood loss of more than 1 L, fibrinogen concentrate would be administered at 1g per litre of estimated blood loss and a ROTEM analysis would be performed as soon as possible to target the above values.
A pre-existing database for liver transplantation surgery recipients was used to obtain the raw data required for this study. The data were extracted, anonymized and analysed by independent third parties not involved in this study.
Patients who received fibrinogen concentrate during liver transplantation surgery were compared against those who did not receive fibrinogen concentrate.
Mann–Whitney U-test was used to determine if there was a significant difference in blood loss during surgery, as well as the use of red cell concentrates, fresh plasma and cryoprecipitate in the 2 groups.
Results
From January 2014 to December 2018, there were 54 liver transplants performed in our institution. Since the introduction of fibrinogen concentrate in January 2017, 14 patients who underwent liver transplantation surgery received fibrinogen concentrate.
No significant difference was detected in the baseline preoperative characteristics of the patients in terms of MELD (Model for End-Stage Liver Disease) score (p= 0.296) as well as preoperative INR (International Normalised Ratio) (p=0.091). Though not statistically significant, there does appear to be a difference in the mean INR. Patients who did not receive fibrinogen concentrate had a mean INR of 1.77 while those who did have a mean INR of 2.21. This may be of clinical significance despite not achieving statistical significance (Table 1).
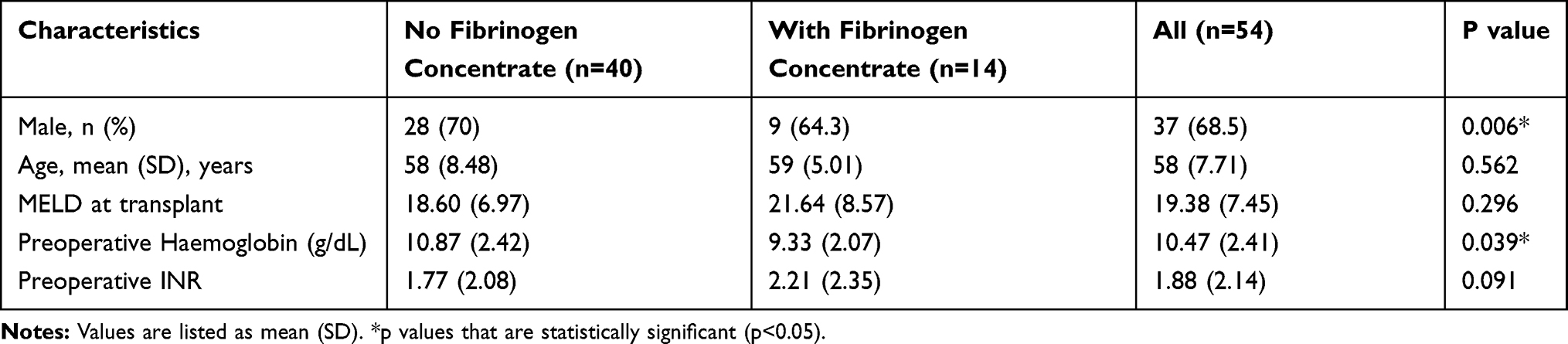 |
Table 1 Baseline Characteristics of Patients Who Received Fibrinogen Concentrate and Those Who Did Not |
There was a significant difference in the starting haemoglobin level of the patients, with a lower starting haemoglobin level in patients who received fibrinogen concentrate (p= 0.039) (Table 1).
No significant difference was noted in the amount of blood loss during surgery (p=0.737), the amount of red cell transfusions (p=0.210) and the amount of plasma transfused (p= 0.559) in both groups of patients (Table 2).
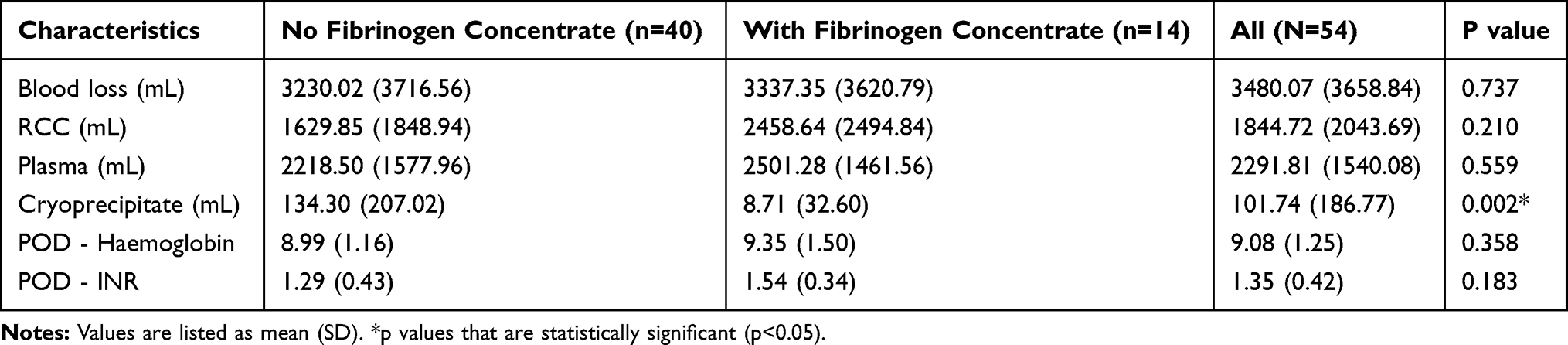 |
Table 2 Table Comparing Postoperative Blood Loss and Laboratory Values of Patients Who Received Fibrinogen Concentrate and Those Who Did Not |
Of note, patients who received fibrinogen concentrate had a significantly less amount of cryoprecipitate transfused compared to those who did not (p=0.002). (Table 2)
No ROTEM values were available on the pre-existing database and hence were not reflected in the results.
Discussion
In the 150 years since Virchow invented the term “fibrinogen” in 1847, the practice of transfusion medicine has further developed, shifting from using whole blood to specific blood components such as red cell concentrates, platelets, and plasma. Further advances have transformed our practice to the use of purified, virus inactivated, plasma-derived products such as factor concentrates.5
Use of fibrinogen concentrate in hemostatic management perioperatively is still in its early years, but studies have shown that its efficacy is consistent. It has a good safety profile with low thrombogenic potential.6 It is also effective in the perioperative management of patients with congenital fibrinogen disorders.7 The way in which fibrinogen concentrate is prepared also carries a lower risk of immunological side effects and reduced risk of viral transmission. There are 5 commercially available preparations of fibrinogen concentrate, namely Haemocomplettan, Fibrinogene T1 and Clottagen, Fibrinogen HT, FibroRAAS and most recently in 2018, FIBRYGA.8 Haemocomplettan is currently the most widely used. It is a human pasteurized, highly purified, plasma-derived product.9 A known amount of factor within each vial as well as lower transfusion volumes allowing for rapid administration help make fibrinogen concentrate an ideal agent to use for haemostasis as compared to the conventional fresh plasma.10
Use of fresh plasma and cryoprecipitate for fibrinogen supplementation has its limitations. Large volumes of transfusions increase the risk of transfusion-related complications such as transfusion-related acute lung injury and viral transmission.9,11 As such, having an alternative replacement to these products that can avoid these adverse effects is desirable.
Few studies describe the impact of the use of fibrinogen concentrate in liver transplantation surgery. Most studies do not focus solely on liver transplantation where pre-existing coagulopathy and potential massive blood loss are major considerations. A retrospective study in 2019 by Hartmann et al described the safety of using fibrinogen concentrates and prothrombin concentrate complexes in liver transplantation.3 In a retrospective cohort studying the use of factor concentrates in liver transplantation, Colevacchia et al noted no significant reduction in transfusion requirements.12 This corresponds to the results of our study done in our local centre.
There may be several reasons for this observation. These reasons are also limitations that we encountered in the conduct of our study. Firstly, the use of fibrinogen concentrate is dependent on the individual anaesthetist and may be reserved for cases in which there is severe intraoperative bleeding not responding to conventional transfusions of fresh plasma and cryoprecipitate. We were unable to tell if the fibrinogen concentrate was given prior to the use of blood products or after from our database. Our transfusion strategy is guided by ROTEM analysis and is a routine for every liver transplantation surgery in our institution. With regard to fibrinogen concentrate, its use is also guided by ROTEM, specifically the FIBTEM component. Our department has developed a simple protocol to follow based on ROTEM analysis. We used the values as follows to guide our hemostatic management: A10 on EXTEM <35mm, A10 on FIBTEM <10mm with normal platelet count to give fibrinogen concentrate with the aim to increase the A10 on FIBTEM to 13mm. This is an abbreviated version as we know that A10 is not the only parameter on ROTEM analysis that is determined by fibrinogen. Other parameters such as maximal clot firmness (MCF), alpha angle and clot formation time (CFT) are also reflective of this. However, to keep the protocol as simple to follow as possible, we have adopted this approach. As fibrinogen concentrate is still fairly new in our practice, there is a learning curve for its usage and hence may impact on its utilisation during this initial introductory phase. Besides, each anaesthetist also has his/her own method of utilising fibrinogen concentrate and may have different aims. Some may use it wholly as a substitute for cryoprecipitate while others may use it to supplement cryoprecipitate use. Unfortunately, this data is not captured on the database owing to the retrospective nature of this study.
Secondly, fibrinogen concentrate is a restricted drug in our hospital and can only be prescribed by certain individuals. Due to the restrictions on prescribing rights, there may be reduced usage of fibrinogen concentrate and a higher tendency to use blood products that are more easily obtained from the blood bank.
Thirdly, there may be a consideration of cost. Ten units of cryoprecipitate (which contains approximately 1g of Fibrinogen) costs SGD$73 and 250mls of fresh plasma (which contains approximately 0.6g of fibrinogen) also cost SGD$73. One vial of Fibrinogen concentrate which contains 1g of fibrinogen concentrate costs SGD$440. As the cost is mainly borne by the patient albeit with subsidies from the government, more cost-conscious anaesthetists may be reluctant to use fibrinogen concentrate instead of the conventional blood products.
This being a retrospective observational study, many limitations exist in our study. Although our centre is one of the two public liver transplantation centres in the country, our numbers are still comparably smaller than in other overseas centres. Small sample sizes, which are an important limitation, may not be reflective of the true effect of fibrinogen concentrate on transfusion requirements.
Inter-individual variation in practice has an impact on the use of fibrinogen concentrate as well. Although fibrinogen concentrate was introduced in January 2017, there was no specific protocol on its use. Hence, anaesthetists who were unfamiliar with its use were less inclined to use it as compared to conventional transfusions of cryoprecipitate. It was only with the introduction of a sample protocol a few months later that its usage picked up.
Pre-emptive use of fibrinogen concentrate to reduce transfusion requirements was previously investigated in 2015 by Sabate et al.13 However, the randomised, double-blind, placebo-controlled trial showed no difference in transfusion requirements. Given the cost involved, we would perhaps adopt a more reactionary approach in our use of fibrinogen concentrate.
Prospective, randomised controlled trials with larger sample sizes should be performed in future to investigate the true impact of using fibrinogen concentrate in liver transplantation surgery. There remains more work to be done to determine the value of fibrinogen concentrate and its subsequent incorporation into our blood transfusion strategy. Perhaps the implementation of a more uniform and aggressive fibrinogen concentrate protocol can eventually help to reduce the amount of blood products required in our transplant surgeries.
Conclusion
The intraoperative use of fibrinogen concentrate did not seem to have any statistically significant difference in the amount of blood loss during surgery in our study. However, the amount of cryoprecipitate used was significantly reduced with the introduction of fibrinogen concentrate. Use of fibrinogen concentrate, guided by point of care coagulation measurement shows tremendous potential as an alternative strategy for coagulation management and should be considered whenever massive blood loss or coagulopathy is expected.
Abbreviations
A10, clot firmness or amplitude obtained after 10 mins beginning from clot formation time (measured in mm); EXTEM, Thromboelastometry that screens for extrinsic hemostatic system via the physiological activator tissue factor; FIBTEM, Fibrin-based extrinsically activated test with tissue factor and platelet inhibitor cytochalasin D; INR, International Normalised Ratio; MELD, Model for End-Stage Liver Disease; POD Haemoglobin, 1st Post Operative Haemoglobin result (g/dL); POD INR, 1st Post Operative International Normalised Ratio; RCC, Red Cell Concentrate; ROTEM, Rotational Thromboelastometry.
Ethics
IRB waiver was obtained from Singhealth (Centralised Institutional Review Board). The reason for the waiver is because the study involves the use of health information that is not individually identifiable. All transplant-related work performed in our institution is done in compliance with the Declaration of Istanbul.
Acknowledgment
This paper has been presented as a poster at the 19th Congress of the European Society for Organ Transplantation, 15–18 September 2019, Copenhagen, Denmark.
Disclosure
The authors declare no conflicts of interest.
References
1. Massicotte L, Denault AY, Beaulieu D, et al. Transfusion rate for 500 consecutive liver transplantations: experience of one liver transplantation center. Transplantation. 2012;93:1276–1281. doi:10.1097/TP.0b013e318250fc25
2. Saner FH, Gieseler RK, Akiz H, Canbay A, Gorlinger K. Delicate balance of bleeding and thrombosis in end-stage liver disease and liver transplantation. Digestion. 2013;88:135–144. doi:10.1159/000354400
3. Hartmann M, Walde C, Dirkmann D, Saner FH. Safety of coagulation factor concentrates guided by ROTEM-analyses in liver transplantation: results from 372 procedures. BMC Anesthesiol. 2019;19:97. doi:10.1186/s12871-019-0767-x
4. Sabate A, Dalmau A. Fibrinogen: a clinical update on liver transplantation. Transplant Proc. 2015;47(10):2925–2928. doi:10.1016/j.transproceed.2015.10.025
5. Costa-Filho R, Hochleitner G, Wendt M, Teruya A, Spahn DR. Over 50 years of fibrinogen concentrate. Clin Appl Thromb Hemost. 2016;22(2):109–111. doi:10.1177/1076029615601494
6. Fominskiy E, Nepomniashchikh VA, Lomivorotov VV, et al. Efficacy and safety of fibrinogen concentrate in surgical patients: a meta-analysis of randomized controlled trials. J Cardiothorac Vasc Anesth. 2016;30(5):1196–1204. doi:10.1053/j.jvca.2016.04.015
7. Simurda T, Kubisz P, Dobrotova M, et al. Perioperative coagulation management in a patient with congenital afibrinogenemia during revision total hip arthroplasty. Semin Thromb Hemost. 2016;42(6):689–692. doi:10.1055/s-0036-1585079
8. Ross C, Rangarajan S, Karimi M, et al. Pharmacokinetics, clot strength and safety of a new fibrinogen concentrate: randomized comparison with active control in congenital fibrinogen deficiency. J Thromb Haemost. 2018;16(2):253–261. doi:10.1111/jth.2018.16.issue-2
9. Franchini M, Lippi G. Fibrinogen replacement therapy: a critical review of the literature. Blood Transfus. 2012;10:23–27. doi:10.2450/2011.0015-11
10. Kozek-Langenecker S, Sørensen B, Hess JR, Spahn DR. Clinical effectiveness of fresh frozen plasma compared with fibrinogen concentrate: a systematic review. Crit Care. 2011;15(5):R239. doi:10.1186/cc10488
11. Goodnough LT, Levy JH, Murphy MF. Concepts of blood transfusion in adults. Lancet. 2013;381:1845–1854. doi:10.1016/S0140-6736(13)60650-9
12. Colavecchia AC, Cohen DA, Harris JE, et al. Impact of intraoperative factor concentrates on blood product transfusions during orthotopic liver transplantation. Transfusion. 2017;57:3026–3034. doi:10.1111/trf.14328
13. Sabate A, Gutierrez R, Beltran J, et al. Impact of preemptive fibrinogen concentrate on transfusion requirements in liver transplantation: a multicenter, randomized, double-blind, placebo-controlled trial. Am J Transplant. 2016;16:2421–2429. doi:10.1111/ajt.13752
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.