")
Back to Journals » Advances in Medical Education and Practice » Volume 11
Impact of Diabetes Continuing Education on Primary Healthcare Physicians’ Knowledge, Attitudes, and Practices
Authors Almetahr H , Almutahar E, Alkhaldi Y , Alshehri I, Assiri A, Shehata S, Alsabaani A
Received 12 August 2020
Accepted for publication 4 October 2020
Published 21 October 2020 Volume 2020:11 Pages 781—790
DOI https://doi.org/10.2147/AMEP.S275872
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Hosam Almetahr,1 Ethar Almutahar,2 Yahia Alkhaldi,3 Ibrahim Alshehri,3 Ali Assiri,3 Shehata Shehata,4,5 Abdullah Alsabaani4
1Preventive Medicine Department, Armed Forces Hospital, Ministry of Defense, Jazan, Saudi Arabia; 2Department of Obstetrics and Gynecology, Abuarish General Hospital, Ministry of Health, Jazan, Saudi Arabia; 3General Directorate of Aseer Health Affairs, Ministry of Health, Abha, Saudi Arabia; 4Family and Community Medicine Department, College of Medicine, King Khalid University, Abha, Saudi Arabia; 5Department of Biostatistics, High Institute of Public Health, Alexandria University, Alexandria, Egypt
Correspondence: Hosam Almetahr Preventive Medicine Department
Armed Forces Hospital, Ministry of Defense, Abuarish, Jazan 45911, Saudi Arabia
Tel +966545919114
Email [email protected]
Background: Little is known about the impact of diabetes mellitus (DM) continuing education (CE) programs on the knowledge, attitudes, and practices of primary healthcare physicians (PHPs) in the Arab world. Accordingly, we aimed to evaluate the effectiveness of a diabetes CE program on the knowledge, attitudes and practices of PHPs in Aseer region, Saudi Arabia.
Methods: This was a quasi-experimental study using a pre-test and post-test design. PHPs attended a three-day diabetes CE session and completed a standardized questionnaire before and after the training session. Also, their practices were assessed by reviewing the records of patients with DM before the CE program and three months later.
Results: A total of 51 PHPs completed the CE program. The sample had a mean (± SD) age of 33.8 ± 6.0 years, and 72.5% were male. The mean knowledge score increased from 14.33 (± 3.37) to 17.61 (± 2.57) (p < 0.001), and the rate of good knowledge increased from 39 (76.5%) before to 51 (100.0%) after (p < 0.001). There was no significant difference in the mean attitude scores before and after the intervention (3.79 vs 3.86; p = 0.10), respectively. Overall, PHPs’ practices related to glycosylated hemoglobin estimation (p = 0.004), foot care (p = 0.02), diet (p < 0.001), exercise (p < 0.001), and weight assessment (p < 0.001) significantly improved following the intervention.
Conclusion: The CE program for PHPs was effective in addressing knowledge gap of PHPs and in improving their practices towards quality patient care.
Keywords: continuing education, diabetes mellitus, knowledge, attitude, practice, primary care physicians
Introduction
Diabetes mellitus (DM) is a metabolic disorder characterized by either lack or insufficient amount of insulin produced from the pancreas, or the body’s inability to utilize insulin.1 Consequently, in uncontrolled DM, there is a persistent elevation of blood glucose, leading to multiple organ damage.1,2 In 2019, nearly 460 million people worldwide were affected by DM, compared to 108 million in 1980.3 In the Arabian Gulf countries, DM is a serious health problem affecting 16.3%, 15.4%, 22.0%, and 15.5% in Bahrain, the UAE, Kuwait, and Qatar, respectively, in 2019.4 In Saudi Arabia, the estimated DM prevalence was 18.3% and it continues to rise over time.4 The rising incidence of DM in Saudi Arabia and other countries in the Arabian Gulf has been attributed to the nutritional transition to Western diets, urbanization, and the sedentary lifestyles that followed the oil boom in the past decades.5,6
The need for quality DM care is well established. Further, and it has been demonstrated that healthcare workers (HCWs) misconceptions regarding DM management may have a negative effect on the quality of services given to affected patients.7,8 Early diagnosis, prompt clinical care, and patient counselling and empowerment through education are the most crucial steps in DM management because they help lower the risk of DM-related complications and help affected individuals to sustain good quality of life.9,10 Easy access to primary healthcare settings that deliver cost-effective interventions for individuals with DM can improve their outcomes. These interventions include a combination of diet, physical activity, medication; and regular screening for complications, which aims to first achieve adequate control of blood glucose and subsequently prevent further complications.6–8 Many studies have evaluated the impact of special DM units, clinics, or services on the quality of care and reducing complications.11,12
Despite the increasing burden of DM, the provision of optimal care and patient education continue to involve substantial problems. Several studies have shown that increased physician knowledge alone does not guarantee improvement in either patients’ or healthcare professionals’ practices and attitudes; however, others have shown improvements in patients’ status with training.11–13 A review revealed that to facilitate increased knowledge and attitudinal changes in patients with DM, it may be necessary for HCWs to undergo specialized DM education and training.14 In addition, an international study conducted in 17 countries showed that HCWs were insufficiently equipped to deliver DM self-management education, including the emotional and psychological aspects of the disease to patients.15 Thus, there is a need to empower HCWs with the skills to address these gaps in DM management.
Little is known about the effectiveness of a diabetes continuing education (CE) program on the knowledge, attitudes, and practices of primary healthcare physicians (PHPs) in Saudi Arabia. Among the limited research on the topic, a study in Al Hasa district revealed the need for improvements in all three domains if physicians are to adequately educate and treat patients with DM.16 Another study conducted in Abha city reported that almost one-third of PHPs were poorly adherent to Saudi DM treatment guidelines.17 Thus, there is a need to address these challenges using diabetes CE programs and to assess their effectiveness with regard to improving the quality of DM care in the country. Therefore, the objective of this study was to evaluate the effectiveness of a CE program with regard to the knowledge, attitudes, and practices of PHPs in Aseer region, Saudi Arabia.
Materials and Methods
Study Design
This was a quasi-experimental study, composed of pre-test post-test uncontrolled experimental design, was conducted from 1st August to 31st October 2019. The protocol was registered at clinicaltrials.gov with the identifier NCT04027062.
Study Population and Setting
The target population for this study included the PHPs registered in the health sector of Abha and Khamis Mushait cities, Aseer region. The study was conducted among physicians working at governmental primary healthcare centers affiliated to the Ministry of Health in the study cities.
Intervention
The diabetes training program was designed to teach participants about DM management and the prevention of complications, as well as to facilitate skill development. This training course served as a basis for health education for physicians and encompassed key health messages for the population about diet, healthy weight, and physical activities. The training program followed the International Curriculum for Diabetes Health Professional Education, which was developed by the International Diabetes Federation.18 In addition, the content of the CE program was designed on the basis of the literature and Saudi national guidelines for DM (Appendix 1).19
DM educators from different professions, such as nurses, dietitians, family physicians, and endocrinologists, were invited to give presentations related to their specialty. The intervention program was implemented as a single-group session over three days. All physicians working in the concerned cities were invited to attend the CE program. At the end of the program, a certificate of completion was awarded to all participants.
Instrument and Assessment
All participants completed a questionnaire before (pre-test) and after (post-test) the intervention. This questionnaire, designed by the authors, was used to gather participants’ demographic characteristics and assess their general knowledge of and attitudes towards DM. This questionnaire consisted of 3 sections: demographic information, knowledge and attitude.
The knowledge section assessed participants’ knowledge before and after the CE program. This section was designed based on Saudi national guidelines for DM, which contains 23 questions covering various aspects of DM.19 Each question had four response options, only one of which was correct based on the adapted program topics. Each correct question was given one point score; otherwise, zero was given. Total scores for knowledge questions were summed. PHPs with a score up to 60% (13 points) of maximum were considered to have poor knowledge level. While PHPs with a score of 60% or more (14–23) were considered to have good knowledge level.
Attitudes were assessed with the most recent version of the Diabetes Attitude Scale 3 (DAS-3) developed by the University of Michigan Diabetes Research and Training Center.20 The DAS-3 is a self-reported instrument consisting of 33 items across five sub-scales. Items are scored on a 5-point Likert scale: 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree. Negatively worded items are reverse scored. A higher score indicates a more positive attitude to DM care. The total score was calculated by dividing the sum of the score by the total number of items in the subscales. Each of the five subscales contains five to eight items addressing topics such as the need for special training, feelings related to the seriousness of type 2 DM, value of tight blood glucose control, psychosocial impact of DM, and patient autonomy. After the pre-test, an interventional CE program was delivered in English language. After the program, all participants completed the same questionnaire (post-test). The study questionnaire was reviewed and validated by three community medicine academic staff at King Khalid University.
The assessment of PHPs’ practices was conducted by reviewing patient records before and after the CE program. Patient files filled by each PHP within three months before and after undertaking the intervention program were reviewed to assess compliance with practice guidelines. The detailed review was based on a checklist of practical aspects related to blood glucose, blood pressure, body mass index, vital signs, HbA1c, and pharmacological and non-pharmacological management.
Pilot Study
We conducted a pilot study with seven PHPs in Abha city whose responses were excluded from the main study. The PHPs were interviewed twice with the same questionnaire two weeks apart. The knowledge section of the questionnaire led to the extraction of five domains, which explained 36% of the total variance (moderate precision). Factor loading for all items ranged from 0.29 for the 8th item of knowledge to 0.99 for the first, which fulfill the required criteria to ensure construct validity of the knowledge tool. Considering Discriminant validity, there was a significant difference in the knowledge scores of the first and last quarters of the samples, which indicate the discriminatory ability of the knowledge items. Regarding reliability, the tool recorded an overall reliability coefficient (KR-20) of 0.78, with none of the items could improve the reliability if removed.
The domains extracted from the attitude section explained 29% of the total variance. Factor loading of the different items ranged from 0.01 for the fifth item to 0.91 for 9th and 10 items revealing good construct validated tool. As for discriminant validity, the tool had a significant difference between the lowest and highest 25% of the samples scores, which confirm the discriminatory ability of the attitude items. Regarding reliability, the tool had an overall alpha Cronbach’s of 0.83, which is very good and no need to remove any item to have better reliability.
Data Analysis
The data were analyzed using IBM SPSS Statistics for Windows, Version 22.0. (Armonk, NY: IBM Corp.). Both descriptive and inferential statistics were used. For the descriptive analysis, results were expressed as numbers and percentages for categorical data and means (± SD and 95% CI) for scale data. The paired t-test and Wilcoxon signed rank test were used to compare the differences between pre-intervention and post-intervention scores. Differences in the mean change in the overall knowledge score according to participants’ sociodemographic characteristics were assessed while adjusting for the effect of pre-test knowledge scores using analysis of covariance.
Ethical Considerations
The Regional Committee for Research Ethics in Aseer region gave approval for the study. All participants provided written informed consent to participate in the study. They also consented to a follow-up visit to assess their practices through their patient records after the intervention.
Results
Sociodemographic Characteristics of the Participants
A total of 51 PHPs completed the CE program. The demographic characteristics of the participants are summarized as shown in Table 1. Participants’ age ranged from 27 to 55 years, with a mean (± SD) of 33.8 ± 6 years; 44 (86.3%) were aged 40 or below. Most of the participants were males 37 (72.5), and 25 (49.0%) were Saudi nationals. The majority of the participants 39 (76.5%) had an MBBS qualification, followed by those with a diploma or master’s 9 (17.6%). Overall, 30 (58.8%) of the physicians had practised for five years or less, and the mean experience in primary healthcare was 5.9 ± 4.2 years. Of the 51 participants, 39 (76.5%) indicated that they had attended a training course about DM in the previous five years.
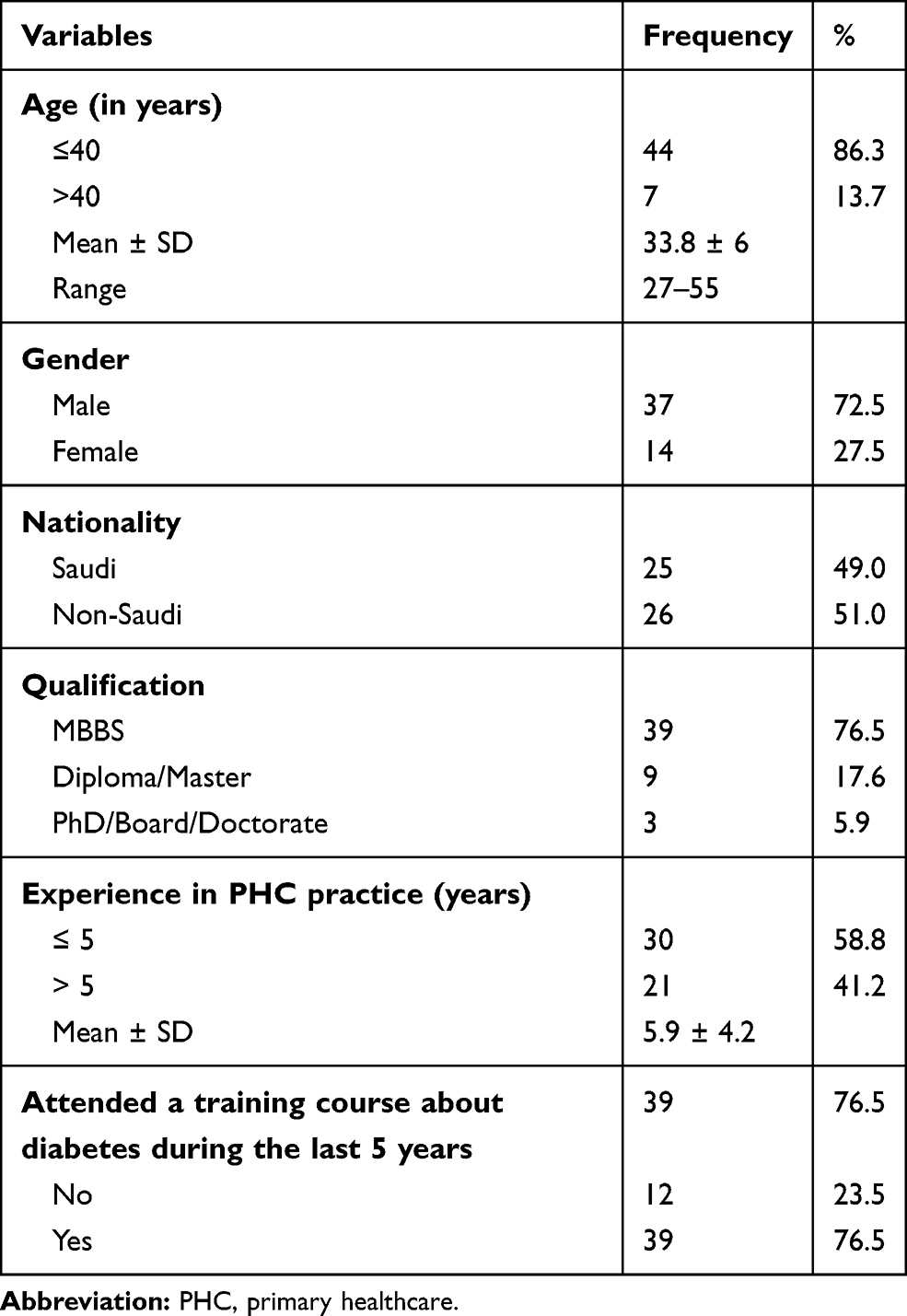 |
Table 1 Sociodemographic Characteristics of the Participants |
Effect of the CE Program Knowledge About DM
The mean (± SD) knowledge domain scores and the pre-post percentage change are shown in Table 2. There was an improvement in the knowledge scores in each domain, with the improvement ranging from 7.4% in the self-management domain to 57.1% in the gestational DM domain. The domains with the most substantial improvement after the intervention were those related to gestational DM with a 57.1% increase (p = 0.005) and DM complications with a 39.7% rise (p < 0.001). However, the increase in the self-management domain was not statistically significant (p = 0.06). The mean scores for all knowledge domains before and after intervention were 14.33 and 17.61, respectively. Thus, there was a 22.8% increase in the overall knowledge score after the intervention (p < 0.001). In total, the overall knowledge level before and after intervention. As depicted, the proportion of participants with good knowledge increased from 39 (76.5%) before the intervention to 51 (100.0%) after the intervention (p < 0.001).
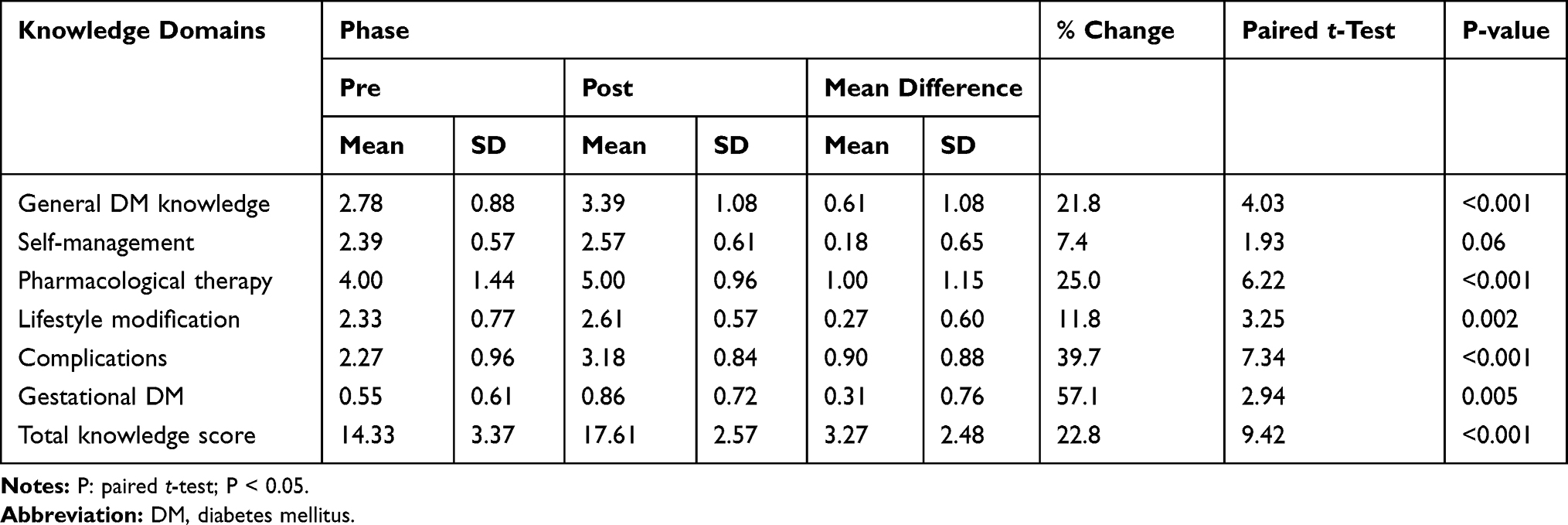 |
Table 2 Change of Knowledge Before and After the Continuing Education Program |
Effect of the CE Program on Attitudes Towards Diabetes
Participants’ attitudes towards diabetes did not substantially change between the pre-intervention period and after completing the CE program (p > 0.05 for all questions). The mean (± SD) attitude domain scores and the pre-post percentage change are shown in Table 3. There was minimal improvement in the attitude scores in each domain, with the change ranging from −0.03% in the value of tight control domain to 2.6% in the patient autonomy domain. The total mean scores for the overall attitude domain before and after the CE program were 3.79 and 3.86, respectively.
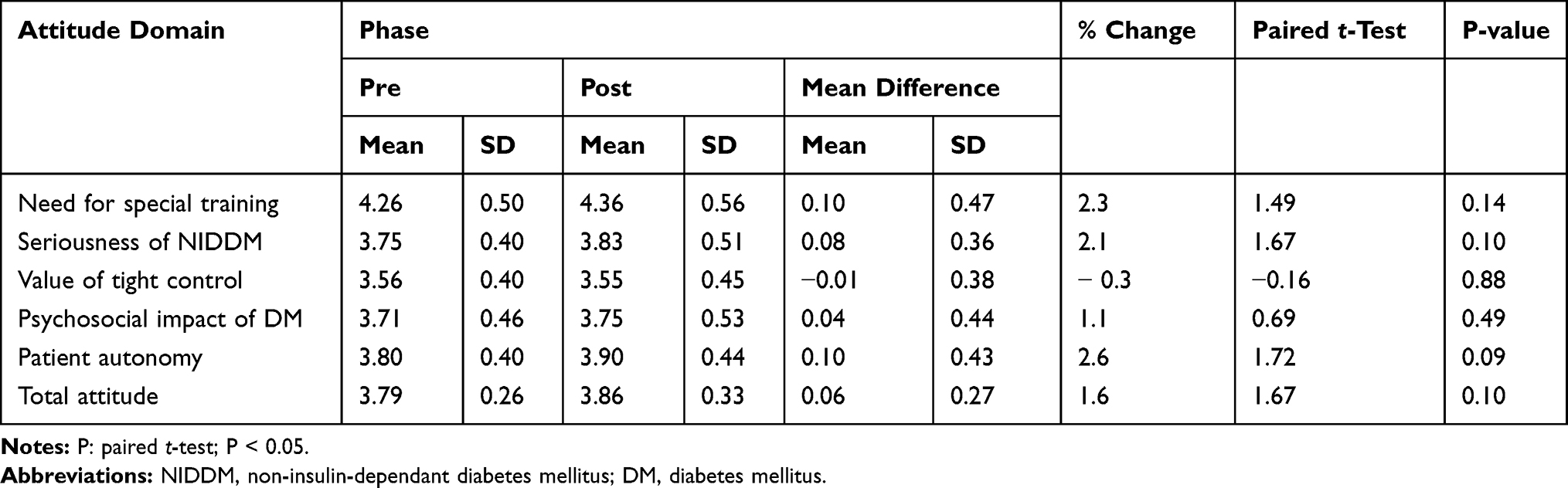 |
Table 3 Change of Attitude of the Participants Before and After the Continuing Education Program |
Factors Associated with Change in Overall DM Knowledge After the Program
The sociodemographic factors associated with change in overall knowledge are summarized in Table 4. There was no significant difference in the mean change in overall knowledge according to participants’ sociodemographic characteristics while adjusting for the effect of pre-test knowledge scores using analysis of covariance (p > 0.05).
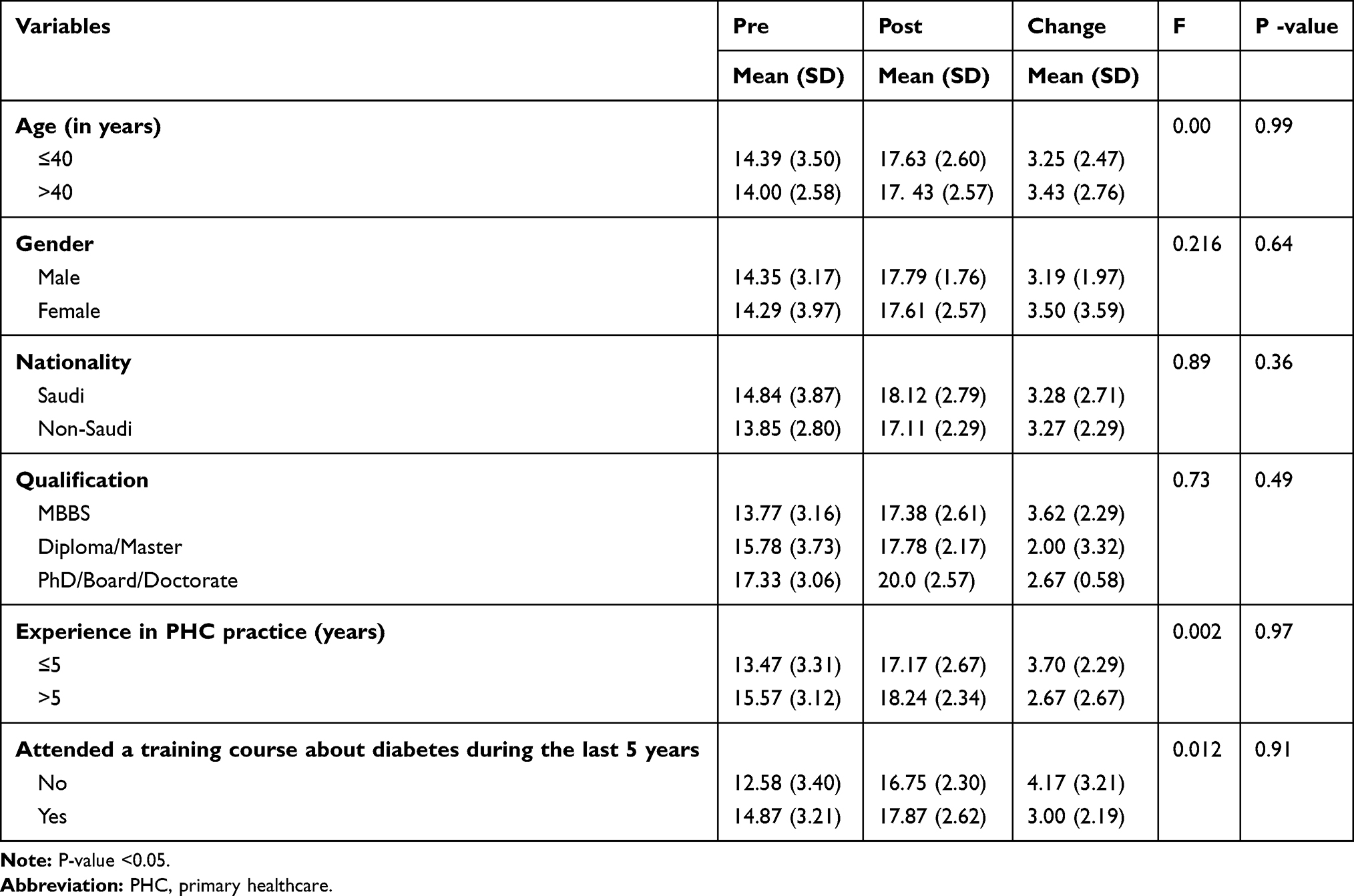 |
Table 4 Factors Associated with Change in Overall Knowledge of Diabetes After the Program |
DM-Related Practices Before and After the Program
For each PHP, the records of four patients with DM were examined in their health facilities before and three months after the CE program. Overall, pre- and post-test practice assessments for 48 PHPs were available, yielding practice records for 192 patients. The practices of the sampled PHPs are shown in Table 5. There were no statistically significant differences in PHPs’ practices related to patient complain assessment (p = 1.00), blood pressure measurement (p = 0.27), and blood glucose estimation (p = 0.27). Overall, their practices related to Hba1c estimation (p = 0.004) and weight measurement (p < 0.001) significantly improved following the intervention. Although the proportions of PHPs with appropriate practices related to foot care, diet, and exercise assessment before and after the intervention were low, there were significant improvements after the intervention (p < 0.05 for each). Although the mean number of referrals to specialized clinics increased from 4.88 pre-intervention to 5.21 post-intervention, the difference was not statistically significant (p = 0.22).
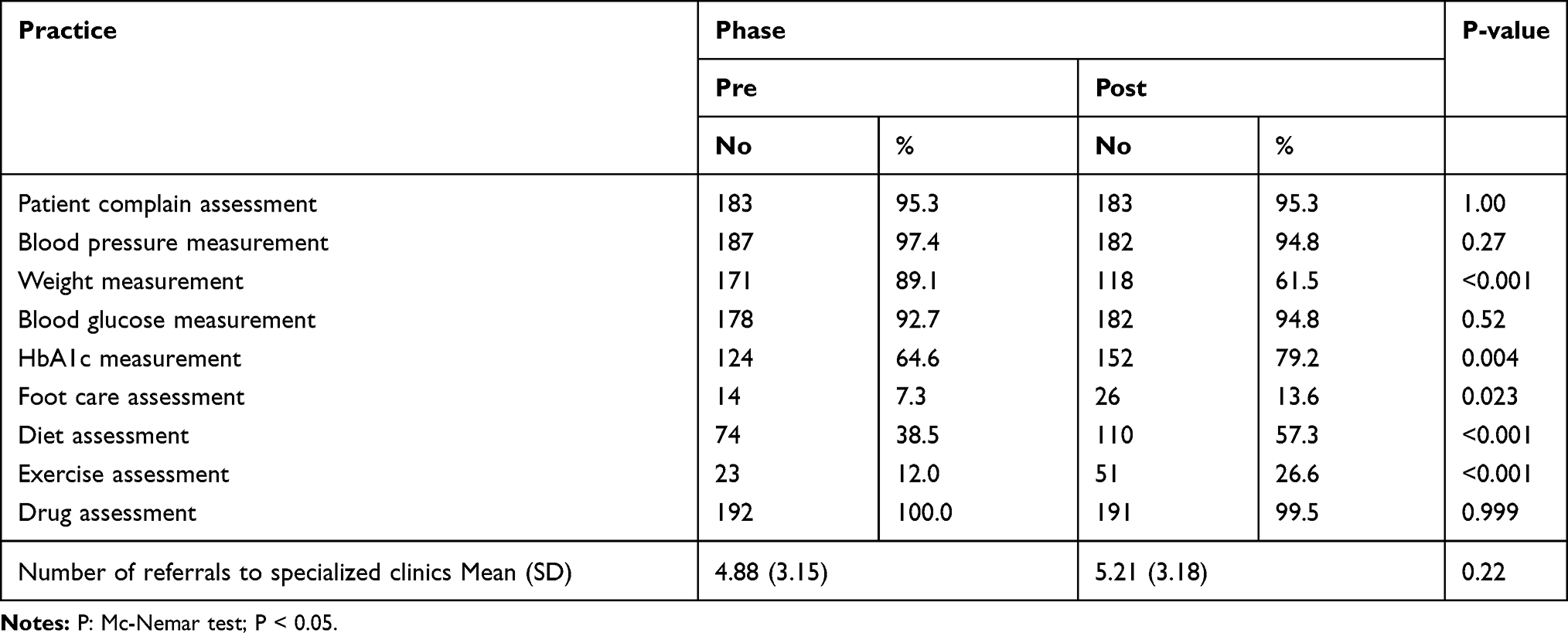 |
Table 5 Practice Among Sampled Physicians Before and After Intervention |
Discussion
PHPs who participated in the training program demonstrated significant improvements in knowledge about DM management. This knowledge was practically applied to DM care as well as other aspects of clinical practice. However, although the findings showed that the participants had higher than neutral attitudes, there were no significant changes in their attitudes towards DM and its management following the CE program.
CE programs for DM are interventions designed to improve PHPs’ knowledge and skills, with the ultimate aim of improving the quality of patient care.21 A meta-analysis of 31 studies showed that CE programs have a moderate effect on physicians’ knowledge; however, there are large variabilities in individual physicians’ practices and patient outcomes.22 Although previous studies in Saudi Arabia have shown that education interventions among patients with DM improved their metabolic parameters and control,23–25 there are no studies known to the authors that assessed the impact of a CE program on PHPs’ knowledge, attitudes, and practices regarding DM care. In this study, the CE program led to a 22.8% increase in the overall knowledge score and ensured that all (100%) participants achieved a good level of knowledge about DM. Also, in the domains concerning knowledge of DM, the change in knowledge increased to over 57% for gestational DM. This indicates that the CE program was generally effective in improving PHPs’ knowledge about DM care.
Our findings on the improvement in PHPs’ knowledge following the CE program are generally consistent with the literature.26–30 A study in the UK showed that the implementation of DM-specific education programs significantly improved patient outcomes as well as trainee doctors’ confidence and knowledge about DM care.26,27 Similarly, a study in the US revealed that a CE program (involving both onsite and online program) led to significant improvements in PHPs’ DM-related knowledge.28 In Malaysia, a CE program on clinical DM care led to significant improvements in DM-related knowledge and clinical skills among general physicians.29 In their analysis of seven practical diabetology courses for multidisciplinary healthcare professionals, Kapur et al reported a significant improvement in knowledge and positive changes in some attitudes.30 A systematic review of 13 studies showed that CE programs led to short-term improvements in PHPs’ knowledge about DM; however, long-term improvements in knowledge or patient outcomes were not demonstrated.13 Thus, although the present study suggests knowledge improvement following the CE program, there is a need to reassess this over a longer period of time. Also, there is a need to develop a standardized instrument to assess PHPs’ knowledge following CE programs in order to allow meaningful comparisons of the effectiveness of such programs across settings.
CE programs that target improvement in PHPs’ attitudes equip them to deliver high-quality DM care.20 In this study, however, there were no significant attitudinal changes following the training. The overall mean attitude score before the CE program was 3.79 out of a maximum of 5. Given that several other studies have also utilized the DAS-3 to assess PHPs’ attitudes, it is possible to make comparisons.14,20,31,32 The overall attitude score in this study is similar to the scores reported from Yemen (3.46), UAE (3.80), and Malaysia (3.98) but lower than the mean score of 4.32 reported from the US.14,31,32 Thus, despite the fact that almost four-fifths of the participants indicated that they had received training on DM in the five years preceding this survey, many had a higher than neutral attitude towards diabetes and its management. The discrepancy between our finding and that of the US study is consistent with earlier arguments that owing to the requirements of regular American certification programs, physicians there tend to have a more positive attitude towards DM care compared to those in developing countries.31
Regarding individual domains, PHPs had a mean attitude score of 4.26 in the need for special training, which increased slightly to 4.36 following the training. This implied that the PHPs placed substantial importance on the need for training on DM care. In the US, Anderson et al reported in a survey of physicians, nurses, and pharmacists a mean score of 4.6 in the need for special training domain.20 Similarly, in their survey of physicians in the same country, Sharp et al found a higher attitude score of 4.66 in the need for special training domain compared to the score of 4.26 in the present study.14 The mean pre-test score in Yemen (4.2) was comparable to our finding but lower than the scores in the UAE (4.6) and Malaysia (4.58).29,31,32 Thus, policies that mandate completing training on DM care as a certification requirement may likely improve PHPs’ attitudes regarding the need for special training in our setting.
Attitudes regarding the severity of DM may inform PHPs’ approach to patient care. PHPs who consider the disease very serious will most likely ensure closer monitoring of patients. In this study, PHPs showed a positive attitude towards the seriousness of DM in the pre-test period with a mean score of 3.75. There was an insignificant increase in this score to 3.81 following the CE program. This indicates that PHPs in Saudi Arabia consider DM a serious disease. This finding is consistent with observations from the US, Malaysia, and the UAE, where high positive mean attitude scores regarding the level of seriousness of DM were reported.14,20,29,32 However, our finding contrasts with those from Yemen, where negative mean attitude scores were reported.31,33 The differences between these studies may be due to variations in PHPs’ experiences with DM care as well as differences in cultural interpretations of the seriousness of DM.
One of the important goals of DM care is to achieve tight blood glucose control. In the United Kingdom Prospective Diabetes Study, patients with DM with tight or intensive glycaemic control had lower microvascular and macrovascular complications as well as better outcomes.34 Thus, there is a need to improve PHPs’ attitudes regarding tight glycaemic control in order to improve patient outcomes. In the present study, participants’ attitudes towards tight glycaemic control were neutral, with a mean score of (3.56 ± 0.40). Also, following the CE program, the mean attitude score in the tight blood sugar control domain decreased slightly to (3.55 ± 0.45). Our pre-test finding for this domain is in accordance with the mean attitude scores reported from Argentina (3.50 ± 0.38), Yemen (3.4 ± 0.65), the UAE (3.68 ± 0.46), and Malaysia (3.79 ± 0.17) but lower than the score reported from the US (4.37 ± 0.50).14,29,32,33,35 This suggests that the PHPs surveyed had a neutral attitude towards maintaining tight blood glucose control in their patients, and this needs to be an important part of future CE training programs.
The fourth domain measured attitudes towards the psychosocial impact of DM on patients. PHPs had a higher than neutral attitude score (pre-test mean = 3.71, post-test mean = 3.75). Thus, the improvement in attitude after the CE program was marginal. This finding is consistent with those of Gagliardino et al, Sales et al, Bani-issa et al, and Lim et al, who reported values of between 3.5 and 4.0.29,31,32,35
The fifth sub-scale measured the participants’ perceptions of patients’ role in their own care, that is, attitudes towards patient autonomy. As per the results, PHPs had a higher than neutral attitude score (pre-test mean = 3.80, post-test mean = 3.90). Thus, there was also a marginal increase in the mean attitude score after the CE program. The positive attitude was demonstrative of PHPs’ agreement with the need to empower patients with DM in order to make appropriate decisions leading to better treatment outcomes. The values obtained in our study were higher than those reported in the UAE, Yemen, and Argentina, where PHPs had a neutral attitude towards patient autonomy with mean scores ranging from 2.79 to 3.40.32,33,35 However, our values are in agreement with findings from the US and Malaysia.14,29
The PHPs’ practices related to HbA1c and weight measurement significantly improved following the intervention. This indicates that the CE program was effective in changing some practices among PHPs, and future training programs need to focus on practices where no substantial improvement was observed. Previous studies utilized variable endpoints to assess the effects of CE programs on PHPs’ practices. The GIANT study, carried out across 10 countries in the Asia-Pacific region, revealed that a structured education program for primary care providers did not improve HbA1c in patients with type 2 DM.36 A randomized controlled trial in Japan showed that the implementation of the “Standard Diabetes Manual” could potentially lead to improved DM management by PHPs.37 The study showed that the proportion of PHPs who adhered to recommendation-concordant measurements of urinary albumin excretion was significantly higher in the intervention group than in the control group (adherence: 17.9% vs 5.3%, p = 0.016). However, other practice parameters were not statistically different between the two groups.37 A systematic review revealed that the delivery of clinical guidelines in conjunction with interactive education did not have an effect on PHP guideline compliance any more than in groups that received guidelines only or usual care; however, when used in conjunction with reminders, guideline recommendations were more likely to be adopted by PHPs at post-intervention compared to those in the usual care group.13 Thus, there is a need for clearly defined short- and long-term practice endpoints of CE programs designed to improve PHPs’ practices. This will help in assessing both the short- and long-term effects of CE programs on PHPs’ practices and allow meaningful comparisons across countries.
This study has some limitations. First is the single-group pre-test and post-test quasi-experimental design, where the participants acted as their own controls. This design poses a threat to internal validity. Second, the study is limited by the small sample size; as we employed convenience sampling and relied on PHPs’ consent during the CE program, adjustments for attrition could not be made. Third, the study assessed neither PHPs’ views on how the CE program could be improved nor the perspectives of the end users (patients) before and after their PHPs participated in the program. The use of a mixed methods design involving qualitative and quantitative aspects will help overcome these limitations.
Conclusion
The CE training program resulted in substantial improvements in PHPs’ DM-related knowledge and clinical practice. However, it had minimal effects on the attitudes towards DM care. Patient perspectives on different aspects of DM care need to be explored and compared with PHPs’ views to determine areas for improvement with regard to patient outcomes. Future CE programs should seek to improve PHPs’ attitudes towards DM care, and clearly defined short- and long-term endpoints of DM-related CE programs with regard to clinical practice need to be developed to facilitate meaningful comparisons across countries and health systems.
Data Sharing Statement
The data that support the findings of the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to thank all of the study participants and the research team who participated in the study for their excellent cooperation. We would like to thank Editage (www.editage.com) for English language editing. This research received no specific grant from any funding agency in the public, commercial, or not for profit sectors.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. Part 1: Diagnosis and Classification of Diabetes Mellitus (WHO_NCD_NCS_99.2-1). World Health Organization; 1999.
2. Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41:255–323. doi:10.1093/eurheartj/eht108
3. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of Type 2 diabetes - global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10:107–111. doi:10.2991/jegh.k.191028.001
4. IDF diabetes atlas – Nineth Edition, 2019 Atlas [Internet]. Available from: http://www.idf.org/diabetesatlas.
5. Alzaman N, Ali A. Obesity and diabetes mellitus in the Arab world. J Taibah Univ Med Sci. 2016;11:301–309. doi:10.1016/j.jtumed.2016.03.009
6. Nasreddine LM, Kassis AN, Ayoub JJ, Naja FA, Hwalla NC. Nutritional status and dietary intakes of children amid the nutrition transition: the case of the Eastern Mediterranean Region. Nutr Res. 2018;57:12–27. doi:10.1016/j.nutres.2018.04.016
7. American Diabetes A. Standards of medical care in diabetes—2015 abridged for primary care providers. Clin Diabetes. 2015;33:97–111.
8. Kloos C, Müller N, Hartmann P, et al. High quality of diabetes care based upon individualised treatment goals – a cross sectional study in 4784 patients in Germany. Exp Clin Endocrinol Diabetes. 2016;124:294–299. doi:10.1055/s-0035-1569380
9. American Diabetes Association. Improving care and promoting health in populations: standards of medical care in diabetes-2020. Diabetes Care. 2020;43:S7–S13. doi:10.2337/dc20-s001
10. Molayaghobi NS, Abazari P, Taleghani F, et al. Overcoming challenges of implementing chronic care model in diabetes management: an action research approach. Int J Prev Med. 2019;10:13. doi:10.4103/ijpvm.ijpvm_485_18
11. Stellefson M, Dipnarine K, Stopka C. The chronic care model and diabetes management in US primary care settings: a systematic review. Prev Chronic Dis. 2013;10:E26. doi:10.5888/pcd10.120180
12. Ricci-Cabello I, Ruiz-Pérez I, Nevot-Cordero A, Rodríguez-Barranco M, Sordo L, Gonçalves DC. Health care interventions to improve the quality of diabetes care in African Americans: a systematic review and meta-analysis. Diabetes Care. 2013;36:760–768. doi:10.1093/eurheartj/eht108
13. Thepwongsa I, Kirby C, Schattner P, Shaw J, Piterman L. Type 2 diabetes continuing medical education for general practitioners: what works? A systematic review. Diabet Med. 2014;31:1488–1497. doi:10.1111/dme.12552
14. Sharp LK, Lipsky MS. Continuing medical education and attitudes of health care providers toward treating diabetes. J Contin Educ Health Prof. 2002;22(2):103–112. doi:10.1002/chp.1340220206
15. Byrne JL, Davies MJ, Willaing I, et al. Deficiencies in postgraduate training for healthcare professionals who provide diabetes education and support: results from the Diabetes Attitudes, Wishes and Needs (DAWN2) study. Diabet Med. 2017;34:1074–1083. doi:10.1111/dme.13334
16. Khan AR, Al Abdul Lateef ZN, Khamseen MB, Al Aithan MA, Khan SA, Al Ibrahim I. Knowledge, attitude and practice of ministry of health primary health care physicians in the management of type 2 diabetes mellitus: a cross-sectional study in the Al Hasa District of Saudi Arabia, 2010. Niger J Clin Pract. 2011;14:52–59. doi:10.4103/1119-3077.79241
17. Somily AA, Khawaji AA, Alsabaani A, Al-Qahtani TAM, Mostafa OA. Adherence of primary health care physicians to Saudi diabetes guidelines. Med J Cairo Univ. 2017;85:2783–2791.
18. International Diabetes Federation. International Curriculum for Diabetes Health Professional Education, 2008. Available from: https://www.idf.org/component/attachments/attachments.html?id=708&task=download.
19. Ministry of Health, Kingdom of Saudi Arabia. National References of Clinical Guidelines for Care of Diabetic Patients in Primary Health Care.
20. Anderson RM, Fitzgerald JT, Funnell MM, Gruppen LD. The third version of the diabetes attitude scale. Diabetes Care. 1998;21:1403–1407. doi:10.2337/diacare.21.9.1403
21. Hayashino Y, Suzuki H, Yamazaki K, Goto A, Izumi K, Noda M. A cluster randomized trial on the effect of a multifaceted intervention improved the technical quality of diabetes care by primary care physicians: the Japan Diabetes Outcome Intervention Trial-2 (J-DOIT2). Diabet Med. 2016;33:599–608. doi:10.1111/dme.12949
22. Mansouri M, Lockyer J. A meta-analysis of continuing medical education effectiveness. J Contin Educ Health Prof. 2007;27:6–15. doi:10.1002/chp.88
23. Tourkmani AM, Abdelhay O, Alkhashan HI, et al. Impact of an integrated care program on glycemic control and cardiovascular risk factors in patients with type 2 diabetes in Saudi Arabia: an interventional parallel-group controlled study. BMC Fam Pract. 2018;19:1. doi:10.1186/s12875-017-0677-2
24. Al-Arifi MN, Al-Omar HA. Impact of a multidisciplinary intensive education program on type 2 diabetes mellitus patients’ glycemic control and cardiovascular risk factors. Saudi Med J. 2018;39:705–710. doi:10.15537/smj.2018.7.22194
25. Ali Dinar NMA, Al Sammouri GAM, Eltahir MA, et al. Effect of diabetes educational program on self-care and diabetes control among type 2 diabetic patients in Al-Baha–Saudi Arabia. AIMS Med Sci. 2009;6:239–249. doi:10.3934/medsci.2019.3.239
26. Taylor CG, Morris C, Rayman G. An interactive 1-h educational programme for junior doctors, increases their confidence and improves inpatient diabetes care. Diabet Med. 2012;29:1574–1578. doi:10.1111/j.1464-5491.2012.03688.x
27. Rajendran R, Kerry C, Round RM, Barker S, Scott A, Rayman G. DICE team impact of the Diabetes Inpatient Care and Education (DICE) project and the DICE care pathway on patient outcomes and trainee doctor’s knowledge and confidence . Diabet Med. 2015;32:920–924. doi:10.1111/dme.12765
28. Lee B, Trence D, Inzucchi S, et al. Improving Type 2 diabetes patient health outcomes with individualized continuing medical education for primary care. Diabetes Ther. 2016;7:473–481. doi:10.1007/s13300-016-0176-9
29. Lim SC, Mustapha FI, Aagaard-Hansen J, Calopietro M, Aris T, Bjerre-Christensen U. Impact of continuing medical education for primary healthcare providers in Malaysia on diabetes knowledge, attitudes, skills and clinical practices. Med Educ Online. 2020;25:1710330. doi:10.1080/10872981.2019.1710330
30. Kapur K, McAleer S, Persson F, Bjerre‐Christensen U. Improving the effectiveness of short-term courses for multidisciplinary health care professionals. Practical Diabetes. 2015;32:80–85. doi:10.1002/pdi.1953
31. Sales I, Babelghaith SD, Wajid S, et al. Impact of diabetes continuing education on health care professionals’ attitudes towards diabetes care in a Yemeni city. Trop J Pharm Res. 2018;17:143–149. doi:10.4314/tjpr.v17i1.20
32. Bani-issa W, Eldeirawi K, Al Tawil H. Perspectives on the attitudes of healthcare professionals toward diabetes in community health settings in United Arab Emirates. J Diabetes Mellitus. 2015;5:1–11. doi:10.4236/jdm.2015.51001
33. Babelgaith SD, Alfadly S, Baidi M. Assessment of the attitude of health care professionals towards diabetes care in Mukalla, Yemen. Int J Public Health Sci. 2013;2:159–164. doi:10.11591/ijphs.v2i4.3842
34. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837–853. doi:10.1016/s0140-6736(98)07019-6
35. Gagliardino JJ, González C, Caporale JE. Diabetes Education Study Group of Argentina. The diabetes-related attitudes of health care professionals and persons with diabetes in Argentina. Rev Panam Salud Publica. 2007;22:304–307. doi:10.1590/s1020-49892007001000002
36. Reutens AT, Hutchinson R, Van Binh T, et al. The GIANT study, a cluster-randomised controlled trial of efficacy of education of doctors about type 2 diabetes mellitus management guidelines in primary care practice. Diabetes Res Clin Pract. 2012;98:38–45. doi:10.1016/j.diabres.2012.06.002
37. Noto H, Tanizawa Y, Aizawa T, et al. Cluster-randomized trial to improve the quality of diabetes management: the study for the efficacy assessment of the standard diabetes manual (SEAS-DM). J Diabetes Investig. 2016;7:539–543. doi:10.1111/jdi.12455
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.